Uworld: Surgery Rotation
1/216
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
217 Terms
Good and bad days, navigation problems, frequent falls, initially no short term memory loss dx:
Lewy body dementia
lewy body dementia symptoms
hallucinations, good and bad days, navigation issues (early), frequent falls/motor manifestations, memory problems (late), visuospacial deficits (clock drawing problems)
dementia before parkinsons
Lewy body dementia
loud noises cause myoclonus dx:
Startle myoclonus due to Prion-related dementias like Creutzfeld-Jakob disease
Primitive reflexes (rooting, sucking, glabellar) + dementia
Frontotemporal dementia
medications associated with drug induced pancreatitis
thiazides, ACE inhibiotrs
Indications for ERCP
Cholangitis-visibile common bile duct dilation/obstruction or increasing liver enzyme levels
Indications for endoscopic ultrasonography in setting of cholangitis
Patient that has cholangitis (dilated common bile duct) on U.S. but no increase in LFTs --> instead ERCP they can get endoscopic ultrasonography to see if there are stones in CBD and then remove gall bladder
Indications for hepatobiliary iminodiacetic acid (HIDA)
For evaluating the presence of cholecystitis in patients with no gall bladder wall thickening or signs of biliary obstruction on U.S. Procedure- nuclear tracer that is excreted in bile-->failure to see it in gall bladder suggests obstruction
Gall stone pancreatitis treatment
cholecystectomy after being medically stable enough for srugery
ALT>150U/L, nausea, vomiting, gall stones suggests
Gall stone pancreatitis
early onset arthroplasty infection (first 3m) symptoms
wound drainage, erythema, swelling and fever
arthroplasty infection (e.g. prosthetic knee joint inf) within the first 3m is due to which organisms
S. aureus, or gram neg anaerobes
treatment of prosthetic knee infection within first 3m due to wound
implant removal or change, or debridement and implant retention
persistent joint pain, implant loosening or sinus tract infection in first 3m after knee replacement can be due to which organisms
Coag neg staph (staph epi), propionibacterium species (enterococci)
treatment for infection in person with knee replacement >3m ago
implant removal, or exchange
Post Gastrectomy hypotension, nausea, vomiting, tachycardia, diaphoresis 20-30min post food
Dumping syndrome
Mechanism of Dumping Syndrome post gastrectomy
damage to pyloric sphincter during surgery or surgical bypass of the sphincter leading to rapid emptying of hypertonic gastric content into the duodenum and SI-->fluid shifts from intravascular space to the small intestine-->hypotension, ANS stimulation-->vasoactive peptide release
Dumping syndrome treatment
change diet: more fibers, more complex carbs, more small meals
Motor vehicle accident + lower extremity fractures + scalp lacerations+ abdominal bruising+ shortness of breath + low bp that became high and pulse that went from high to low after fluids and then development of progressive weakness on the right side of his body. What does the patient have? and what CN may be injured? What artery may be injured?
Due to right sided weakness but left sided injury, there may be Uncal Herniation due to middle meningeal artery rupture-->expanding hematoma. Cushing reflex occurs because the expanding hematoma + fluid recussitation causes there to be elevated intracranial pressure--> constriction of arterioles-->cereberal ischemia-->brain senses inc pCO2 and dec pH--> central reflex sympathetic to increase perfusion pressure + hyperventillate-->hypertension because brain thinks patient is hypptensive--> reflex bradycardia due to strestching of baroreceptors. CN 3 injury occurs due to uncal herniation-->down and out pupil
occlusion of PICA causes damage to which CN
Accessory 11
jugular foramen syndrome(posterior fossa tumor) causes damage to which nerve
Glossopharyngeal nerve (CN IX) --> loss of gag reflex, loss of taste and sesnation on posterior 1/3 of tongue, loss of pharyngeal sensation and dysfxn of carotid sinus reflex leading to inc risk of syncope
transtenorial herniation can lead to
ipsilateral hemiparesis, ipsilateral mydriasis and strabismus, contralateral hemianopsia and AMS (altered mental status)
Lesion compressing the contralateral crus cerebri against the tentorial edge causes
ipsilateral hemiparesis
compression of ipsilatearl CNIII by herniated uncus causes
loss of parasympathetic innervation causing mydraisis (occurs early); loss of motor innervation causes ptosis and a downa nd out gaze of ipsilateral pupil due to unopposed CNIV and VNVI action
compression of reticular formation causes
AMS and coma
fever, dysphagia, odynophagia, drooling and redness near submandibular and sublingual area can suggest
Ludwig angina = rapidly progressive bilateral cellulitis of submandibular and sublingual spaces usually due to an infected mandibular molar
tachypnea, tachycardia, hypoxia within first 24h after blunt injury with rib fractures suggests, chest wall bruising, decreased breath sounds on side of injury
pulmonary contusion (bruised lung parenchyma)
chest x-ray shows rib fractures and patchy irregular infiltrate in a tachypneaic, tachycardic, hypoxemic patient -- diagnosis
pulmonary contusion
ARDS vs Pulmonary contusion
ARDS8 occurs within first 24-48 h whereas pulm contusion* occurs in first 24h. Bilateral lung involvement is in ARDS.
hemothorax on CXR is detected as
pleural effusion with hypotension if its significant
thrombocytopenia, petechiae, mental changes, hypotension tachypnea, tachycardia following trauma suggest
bone fat embolism
GCS factors
1. ability to open eyes 2. motor response 3. verbal response (e.g. oriented, disoriented, confusion8
GCS is calculated when?
For all trauma patients in order to triage based on severity and prognosis of coma
anterior mediastinal mass DDX
Four Ts Thymoma, Teratoma, Terrible lymphoma, Thyroid neoplasm
Germ cell tumor types
Seminomatous - Elevated Beta HcG in 1/3 of cases but normal AFP. Non-seminomatous = yolk sac tumor, choriocarcinoma, embryonal carcinoma, Mixed germ cell tumor = mix of non-seminomatous germ cell tumors. Non-semis have elevated AFP but often also elevated BHCG
arteries damaged in hemothorax
MC due to laceration of lung parenchyma or damage to intercostal or internal mammary arteries
flaccid paralysis and diminished pain and temp sensation but preserved vibration post thoracic aortic aneurysm repair is due to
ischemia to anterior spinal artery that supplies (branches from artery of Adamkieqicz and other radicular arteries of the thoracic aorta) the anterior 2/3 of the psinal cord. The ischemia is due to either cross clamping or hypotension from bleeding.
Nasogastric tube in chest x-ray above diaphragm =
diaphragmatic hernia
Diaphragmatic hernia caused by trauma mechanism
trauma causes increased abdominal pressure that makes diaphragm explode and intestine or stomach go through it
vitals of diaphragmatic hernia
stable
diaphragmatic hernia CXR

tension pneumothorax vitals
unstable (hypotensive)
three or more adjacent rib fractures that break in 2 places + create an unstable chest wall segment that moves in a paradoxical motion with respiration (during inspiration it contracts instead of bulging out and bulges out during expiration when it normally should retract) is consistent with
flail chest
diaphragmatic hernia is usually on which side
left because right side is protected by liver
CXR of diaphragmatic hernia description
deviation of mediastinal contents to opposite side; elevation of hemidiaphragm; nasogastric tube in pulmonary cavity or intestines there
nausea, abdominal distention, obstipation, hypoactive bowel sounds that persist for >3-5days post-op
Post-operative ileus
etiologies of Post Op Ileus
increased splanchnic nerve sympathetic tone following peritoneal instrumentaton, local release of inflammatory mediators and post operative opiate analgesics (dec. motility)
preventative measures to prevent Post Op ileus
epidural anesthesia, minimal invasive surgery, judicious perioperatve use of I.V. fluids to minimize gastrointestinal edema
MCC of mechanical bowel obstruction in U.S.
adhesions--following previous abdominal surgeries
difference between mechanical vowel obstruction vs post-op ileus
Bowel sounds hyperactive bowel sounds in mechanical bowel obstruction vs hypoactive in post op ileus. MBO- have temporary return of bowel fxn prior to symptom onset (think of daniel...patient who went home and came back). X-ray -both have dilated loops of bowel but compared to PPI, x-rays in MBO are more likely to have air- fluid levels and clear transition points of the bowel
burn victims - initial management
1. ABC-- secure airway by giving oxygen first and ventillating if there is evidence the airway was burned/damged thermally (>10% carboxyhemoglbin level, tridor, carbenaceous sputum, burns to face, oropharyngeal inflam) etc. intubate sooner than later due to increasing edema in airway post burn
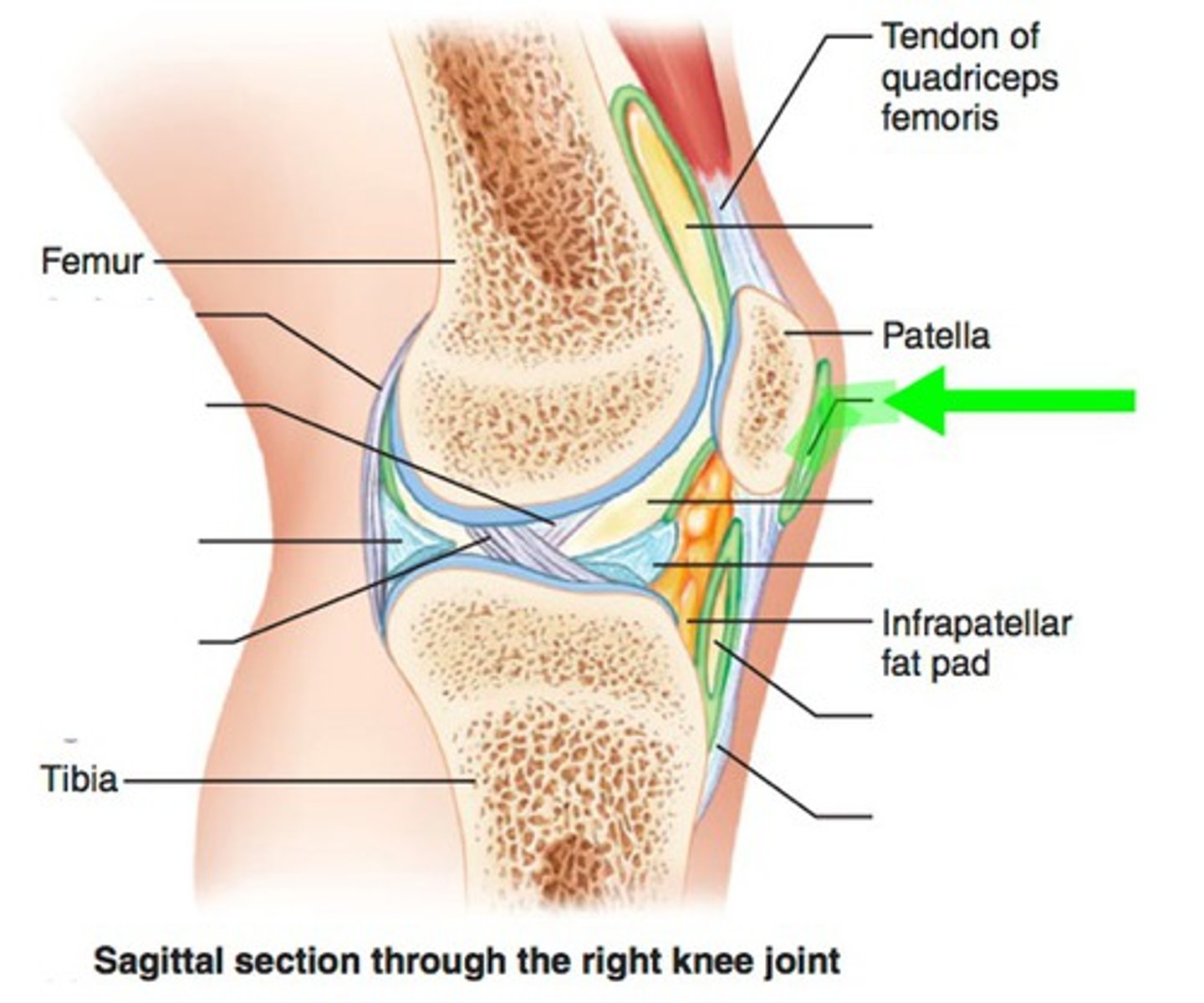
inability to extend knee, acute swelling, tenderness of patella region after falling or direct blow to knee =
fracture of patella
episodic pain and tenderness at inferior patella and pateller tendon usually seen in atheletes in jumping sports or in occupations with repetitive forceful knee extension
patellar tendenitis
chronic anterior knee pain that is MC in women, presents with peripatellar pain worsened by activity or prolonged sitting
patellofemoral pain syndrome
anterior knee pain, tenderness, erythema, localized swelling, MC in occupations requiring repetitive kneeling (housewives, plumbers), Often due to S.aureus which can infect the bursa from penetrating trauma or repetitive friction or extension of local cellulitis =
prepatellar bursitis
prepatellar bursa
high riding prostate on DRE, blood in urethra, inability to void post car accident, scrotal or perineal hematomas suggests
posterior urethral injury
suspected posterior urethral injury management
1. Retrograde urethrogram prior to insertion of a Foley catheter because you can increase the urethral tear or cause infection of the periurethral hematoma
Anterior urethral injury management
1. Immediate surgical repair (ocassionally) 2. Treat with urinary diversion via suprapubic catheter while the primary injuries/hematomas heal. 2. Once healing is over, urethral stricture/residual damage is assessed and repaired
diagnosis of bladder injury
retrograde cystogram
fever, sore throat, difficulty swallowing, muffled hot potato voice, uvula deviation awaya from enlarged tonsil and pooling of saliva =
peritonsillar abscess ( acute bacterial inf between tonsil and pharyngeal muscles)
treatment for peritonsillar abscess
needle aspiration or incision and drainage + antibiotic therapy to cover Group A hemolytic strep and respiratory anaerobes
fever, pharyngeal pain, earache and deviation of uvula to oppositve side of swollen tonsil =
peritonsillar abscess
compartemnt syndrome etiology
direct trauma or prolonged compression of an extremity or revascularization of an acutely ischemic limb
excruciating pain worsened on passive range of motion that does not respond well to narcotics after trauma or prolonged compression of an extremity =
compartment syndrome
Early paresthesia from sensory nerve ischemia after trauma to the leg + later neuro defecits (sensory loss, motor weakness) suggests
compartment syndrome
compartment syndrome treatment
Immediate fasciotomy!!!
Labs for Acute mesenteric ischemia
1. elevated wBC, hemoglbin, amylase, metabolic acidosis, inc lactate
Patient had MI in past and now has leukocytosis, elevated amylase + phosphate levels, metabolic acidosis (inc lactate, elevated hemoglobin and pain out of proportion to examination findings on abdominal P.E. =
Acute mesenteric ischemica
diagnosis of acute mesenteric ischemia
CTangio (preferred), or MRI angiography, Mesenteric angiography if diagnosis is unclear
treatment of Acute mesenteric ischemia
1. either embolectomy with vascular bypass or endovascular thrombolysis 2. Broad spectrum antibiotics 3. anti-coagulants to reduce risk of clot expansion (unless contraindicated)
penis is deviated to right after sex with female on top- whats the initial management
1. Retrograde urethrogram followed by surgical exploration of penis
diagnosis of fat embolism
fat droplets in urine or intraarterial fat globules on fundoscopy
timeline for fat embolism
12-72h post injury
air embolism etiology
subclavian vein access or trauma patient on respirator
sudden upward pulling on the arm can cause
injury to lower brachial plexes (C8-T1) causing Klumpy's palsy. which causes Injury to ulnar nerve --> atrophy of interosseous and hypothenar muscles--> claw hand
humeral neck fracture presents as
swelling, ecchyosis, crepitus over a fracture--axillary nerve injury may be present
pain after femoral embolectomy in right calf with burning sensation =
compartment syndrome-- ischemia-reperfusion syndrome
compartment syndrome is associated with
long bone fractures or traumatic injuries of the extremities; any condition that causes increased pressure in a confined tissue space and compromises blood flow
diagnosis of compartment syndrome
Compartment pressure>30mmHg or delta pressure (diastolic bp- compartment pressure) <20-30mmHg
treatment of compartment syndrome
if compartment pressures improve rapidly, observe them and if not do fasciotomy
Homan sign =
pain with passive stretching of calf --> indicative of DVT
eschar formation in a burn suggests
Acute compartment syndrome with so much edema that there is tissue ischemia and venous and lymphatic compromise -->eschar (third degree burn)
treatment of acute compartment syndrome
fasciotomy or escharotomy (think of the syrian patient)
crutches can cause
radial nerve injury
fraction of humeral shaft causes
radial nerve injury
blocking a basketball shot can cause
anterior shoulder dislocation and axillary nerve injury
symptoms of radial nerve injury
wrist drop and sensory loss on posterior arm, forearm and lateral dorsal hand
fracture of medial epicondyle injures
ulnar nerve
symptoms of ulnar nerve injury
claw hand, sensory loss of dorsal and ventral aspects of hand
Uncomplicated vs Complicated Diverticulitis
Uncomplicated = 75% diverticulitis with no abscess, occurs in stable patients and can be treated with bowel rest, oral antibiotics, observation, hospitalize + I.V. antibiotics are needed for elderly, immunocomp, high fever or significant leukocytosis patients. Complicated = 25% diverticulitis + abscess, perforation, obstruction or fistual formation.
Complicated Diverticulitis + <3cm fluid collection treatment
I.V. antibiotics + observation
Complicated diverticuliits + abscess >3cm treatment
CT-guided percutaneous drainage and surgical if it fails
If symptoms of complicated diverticulitis are not controlled by the 5th day - treatment?
surgical drainage and debridement
when should sigmoid resection be done in diverticulitis patients?
Fistulas, perforation with peritonitis, obstruction, recurrent attacks of diverticulitis
pain, edema or erythema spreading beyond surgical site infection suggests
necrotizing surgical site infection
symptoms of necrotizing surgical site infection
1) Pain, edema, or erythema spreading beyond surgical site 2) systemic signs such as fever, hypotension, tachycardia 3) paresthesia or anesthesia at the edges of the wound 4) purulent, cloudy gray discharge (dishwater drainage) 5) subcutaneous gas or crepitus
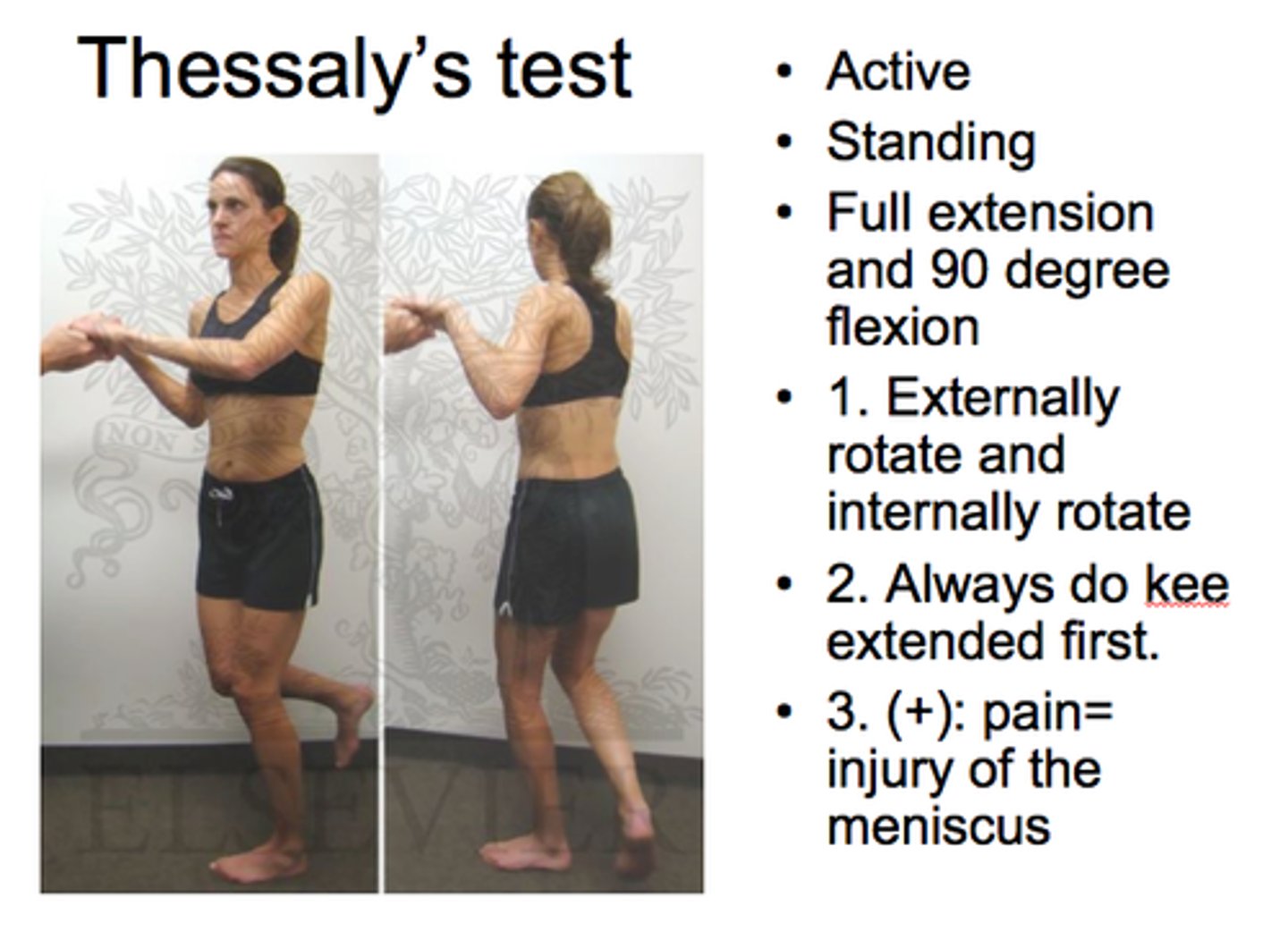
testing for meniscus tears
Thessaly and McMurray test
Thessaly test