Intro to the Liver
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
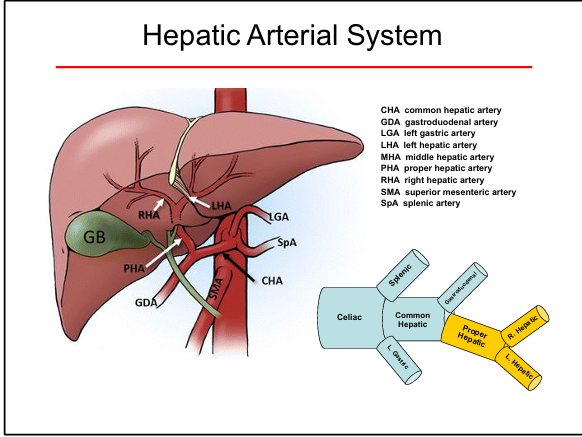
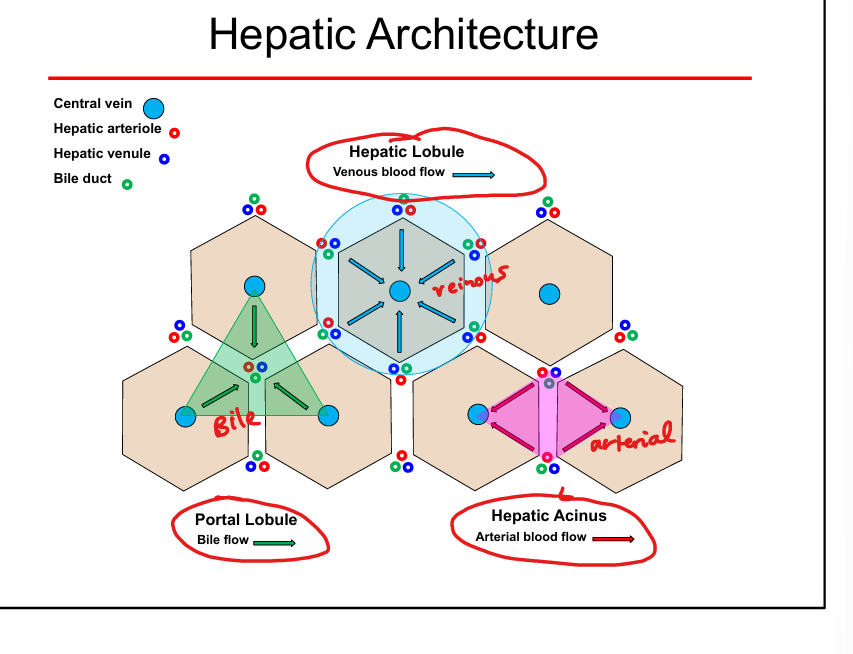
Liver blood supply
Dual supply: hepatic artery (oxygenated) + portal vein (nutrient-rich)
Portal triad components
Portal venule, hepatic arteriole, bile duct
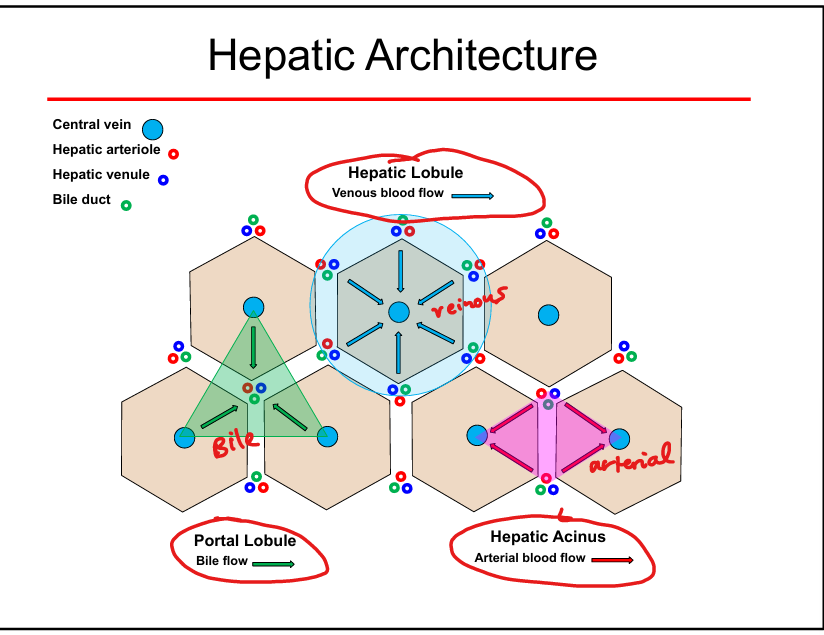
Hepatic lobule blood flow direction
From portal triad → sinusoids → central vein
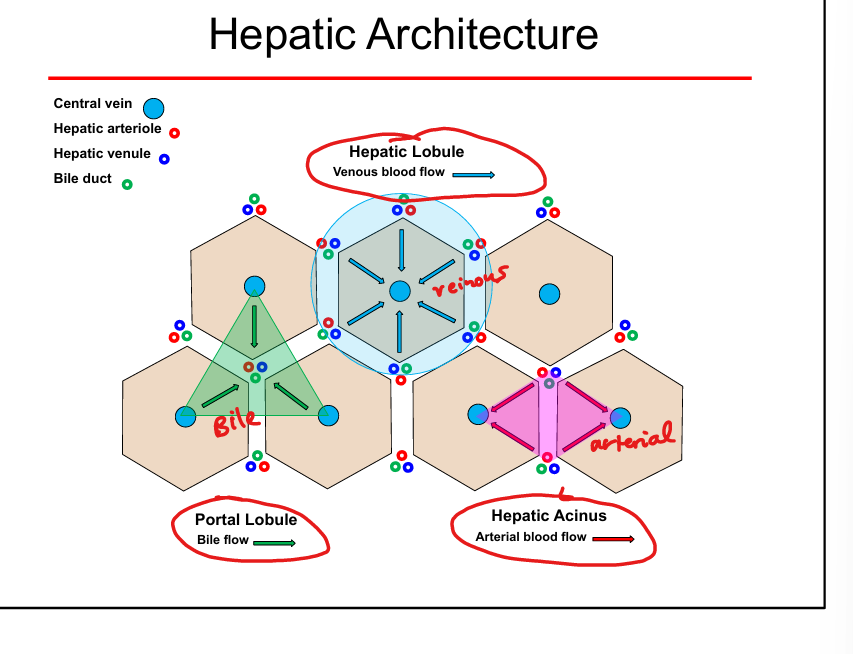
Bile flow direction
From hepatocytes → canaliculi → bile ducts (opposite blood flow)
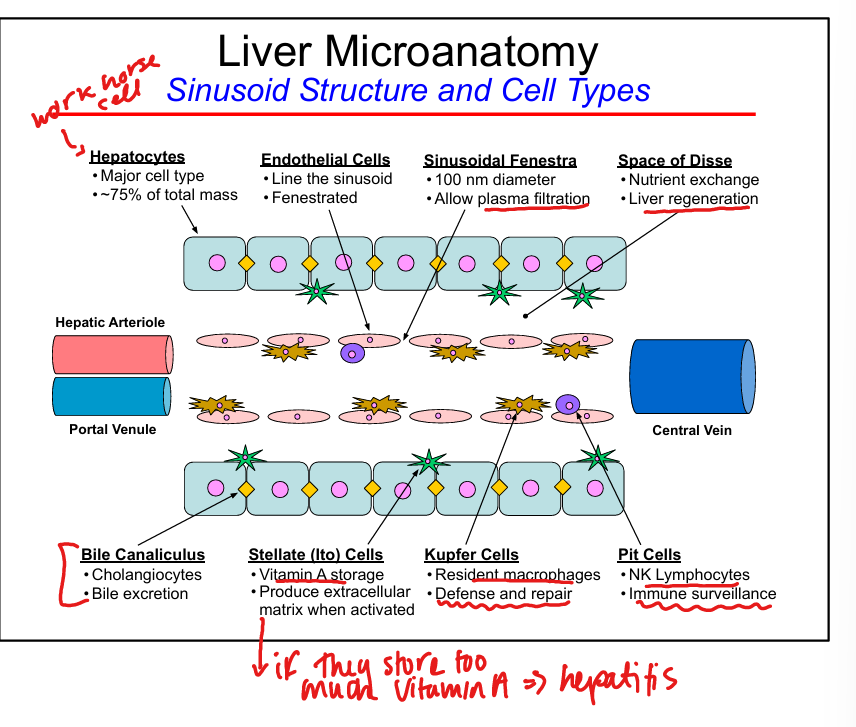
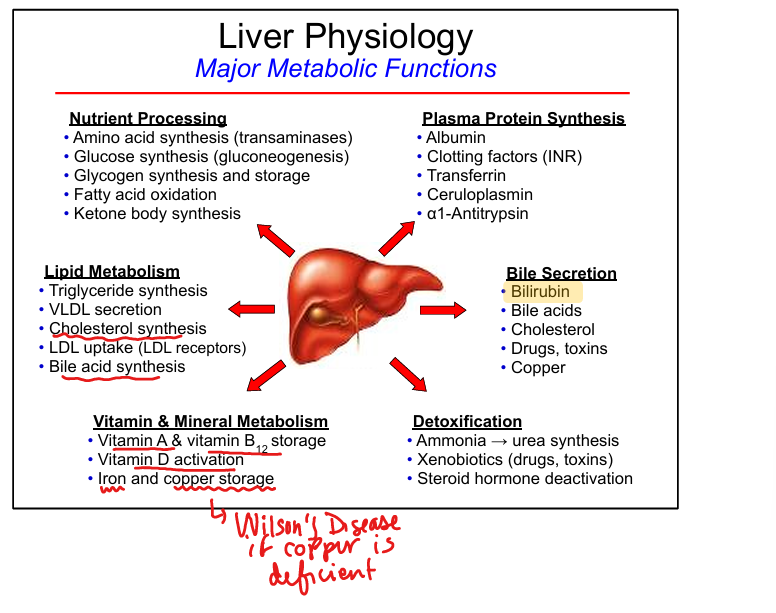
Hepatocyte functions
Protein synthesis, metabolism, detoxification, bile formation
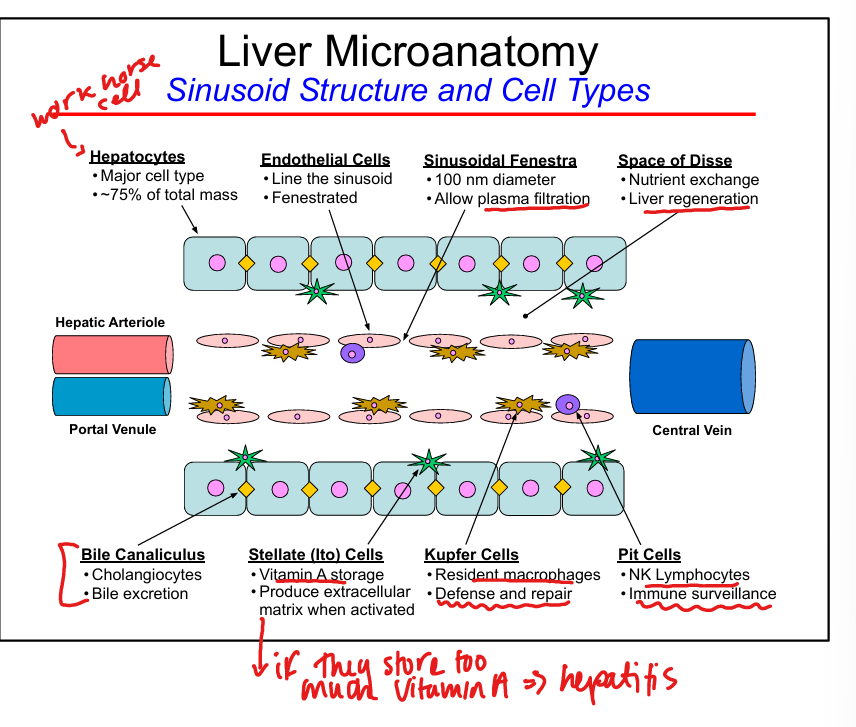
Endothelial cell features
Fenestrated, allow plasma filtration into Space of Disse
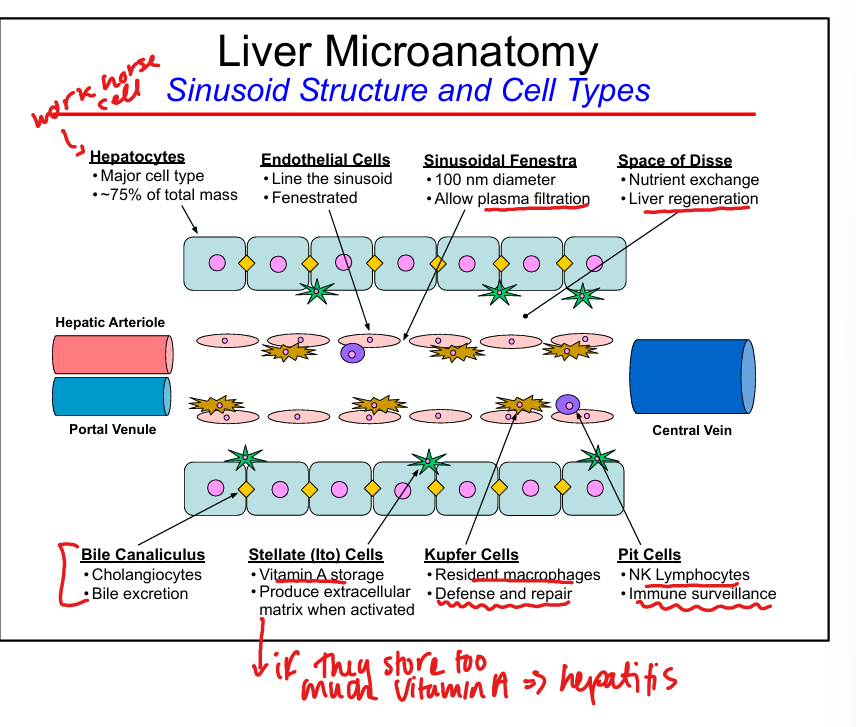
Kupffer cell function
Resident macrophages, phagocytosis, immune surveillance
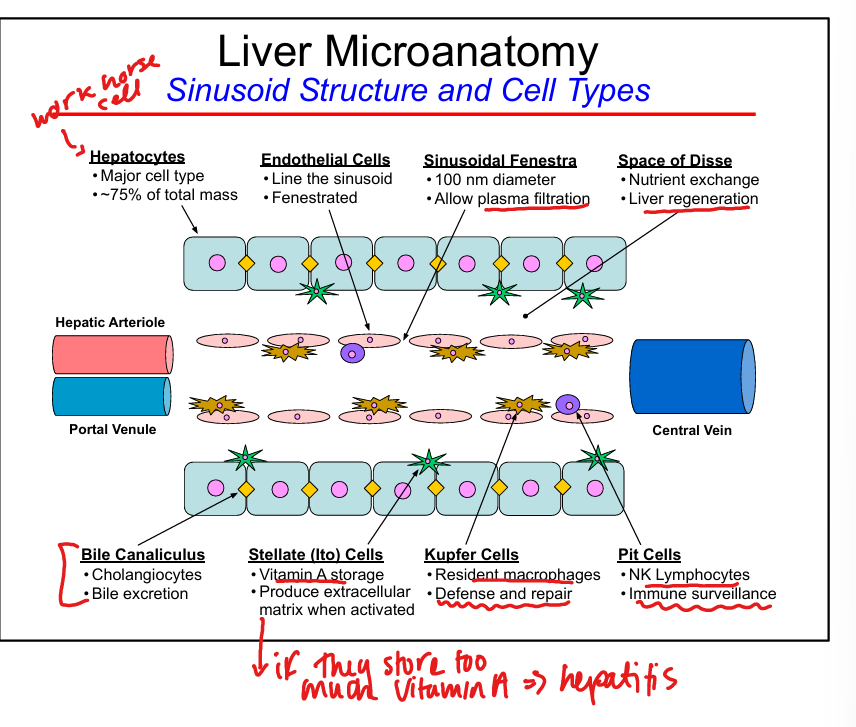
Stellate (Ito) cell function
Vitamin A storage
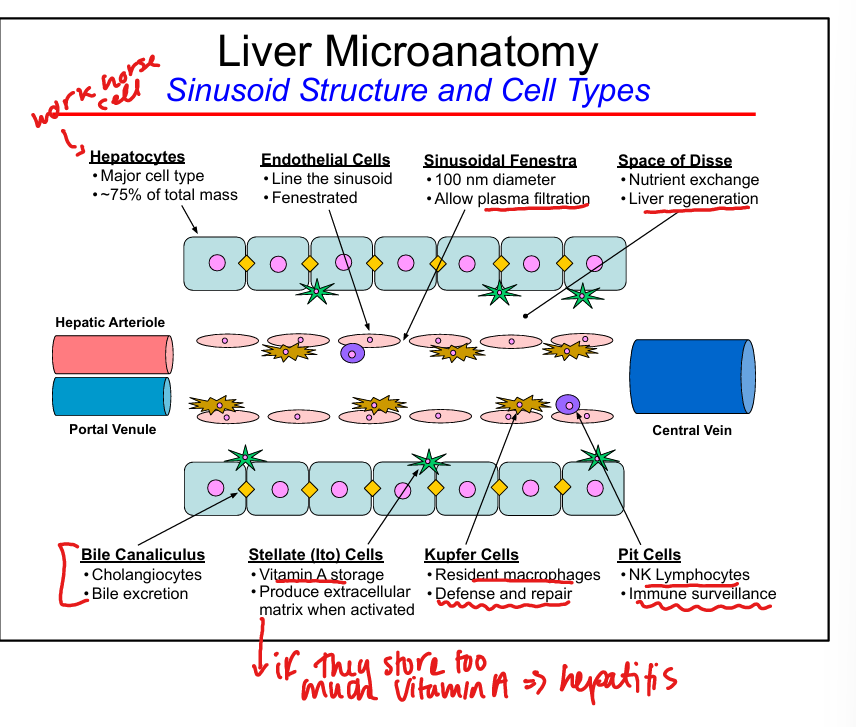
Pit cell function
NK lymphocytes for immune surveillance
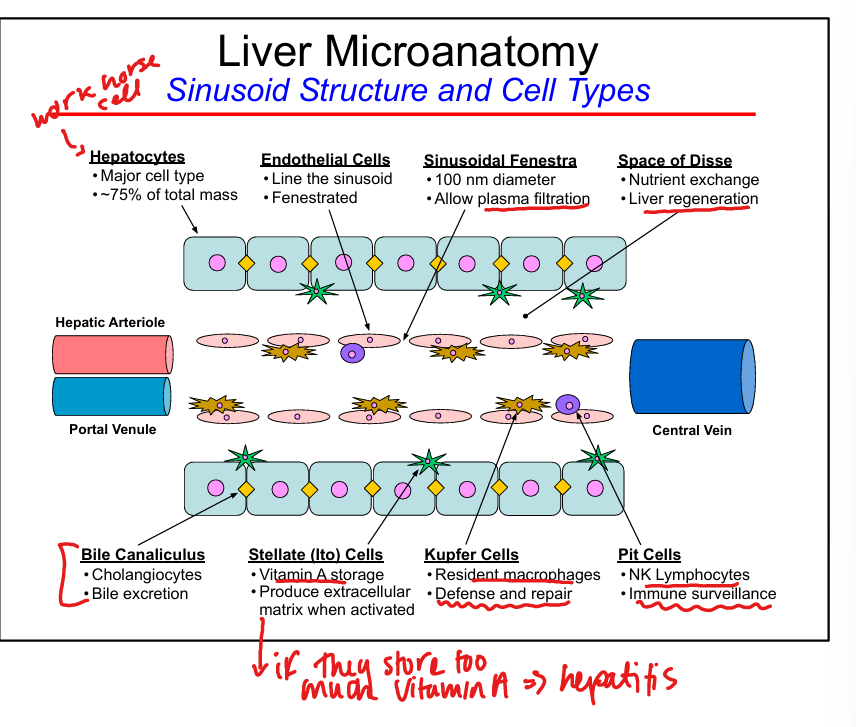
Space of Disse
Site of nutrient exchange between blood and hepatocytes, liver regeneration
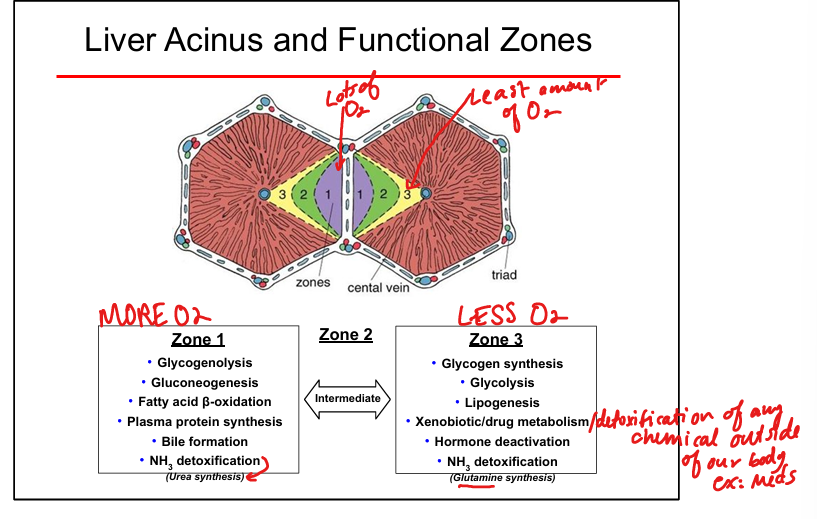
Sinusoidal oxygen gradient
Highest O₂ in Zone 1, lowest in Zone 3
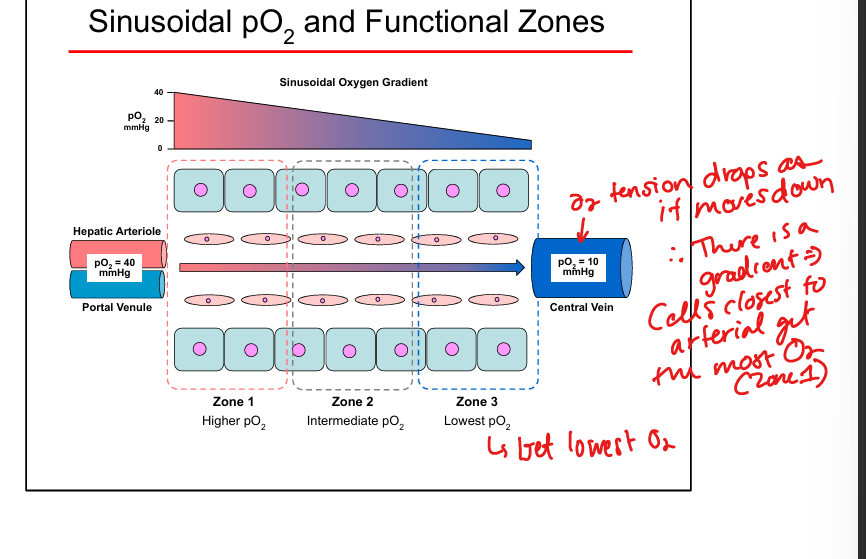
Zone 1 functions
Gluconeogenesis, glycogenolysis, fatty acid β-oxidation, urea cycle(NH3 detox), protein synthesis, bile formation
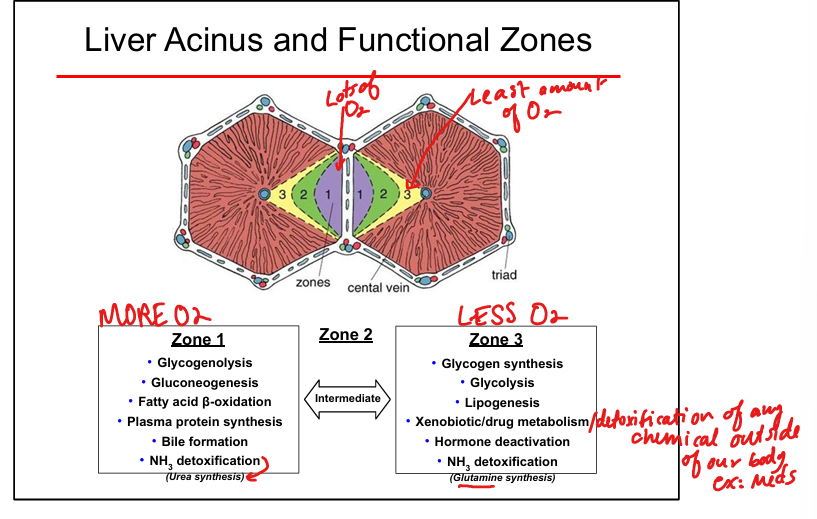
Zone 3 functions
Glycogen synthesis, Glycolysis, lipogenesis, drug metabolism (CYP450), glutamine synthesis, hormone deactivation
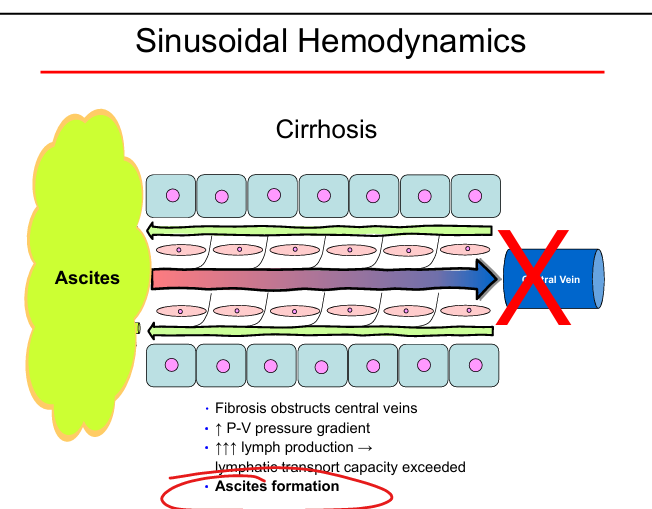
Portal hypertension mechanism
Fibrosis → ↑ portal–venous gradient → ↑ lymph → ascites
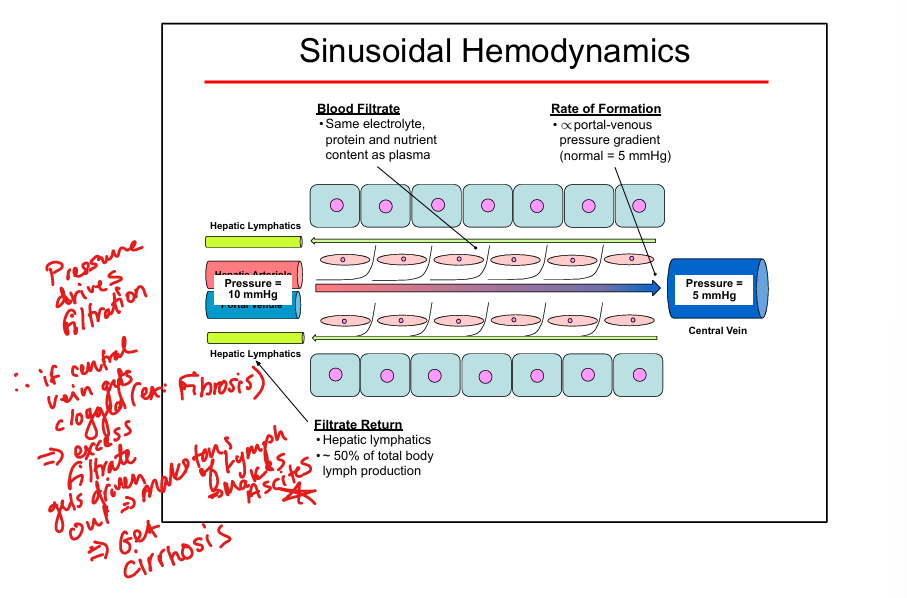
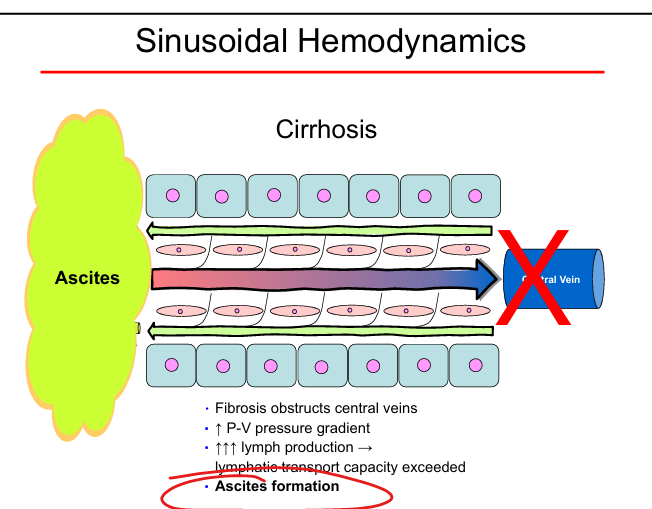
Ascites formation
Lymph production exceeds lymphatic drainage due to cirrhosis
Vitamin storage in liver
Vitamins A, D, B12
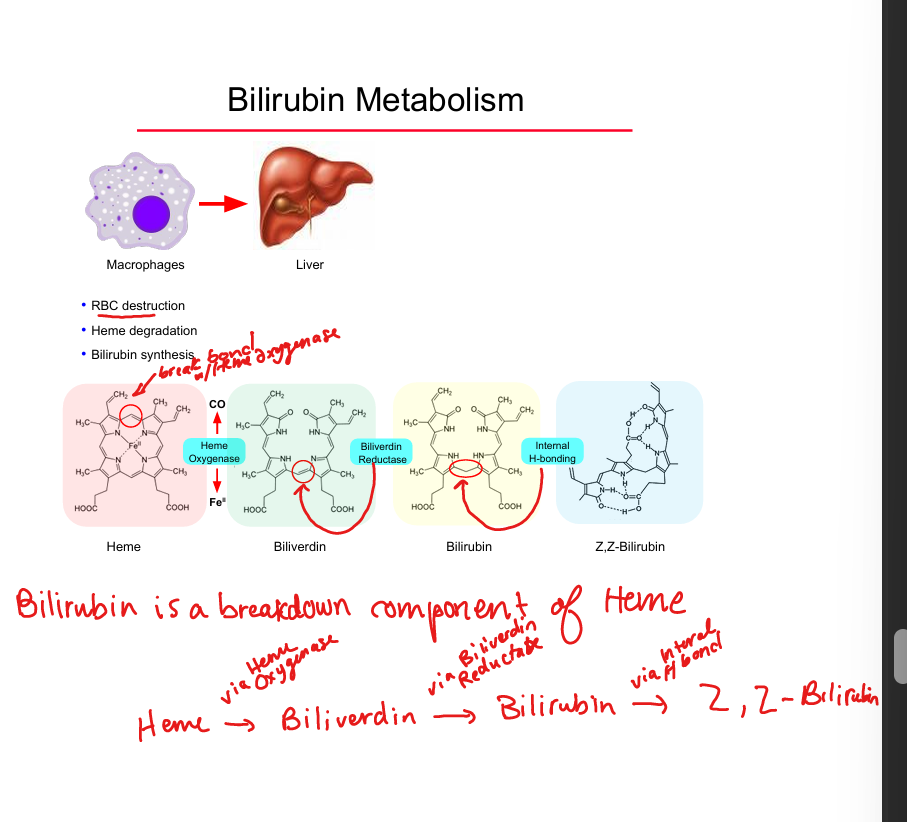
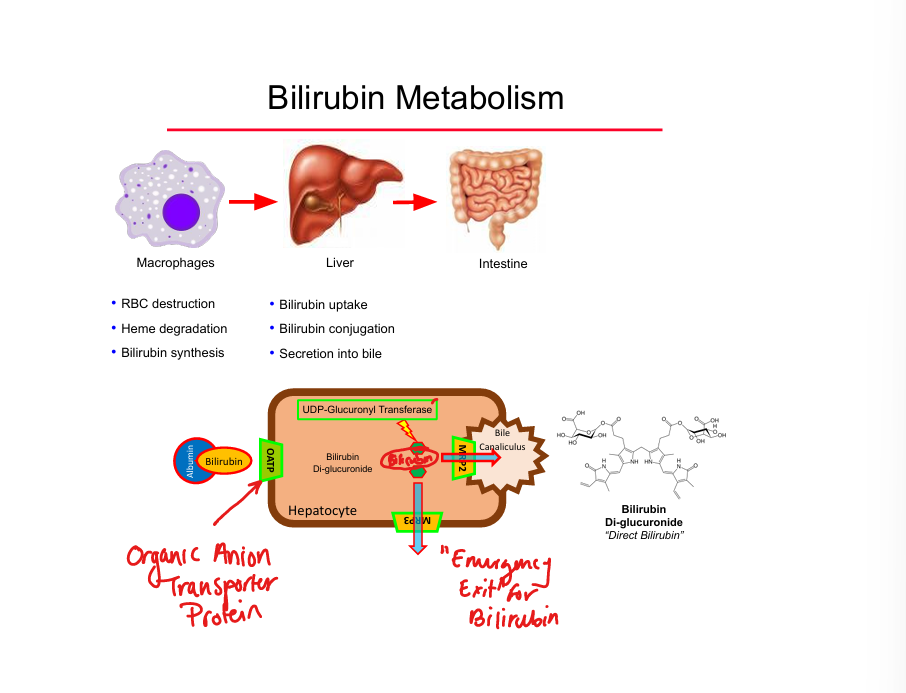
Bilirubin source
Breakdown of heme from senescent RBCs
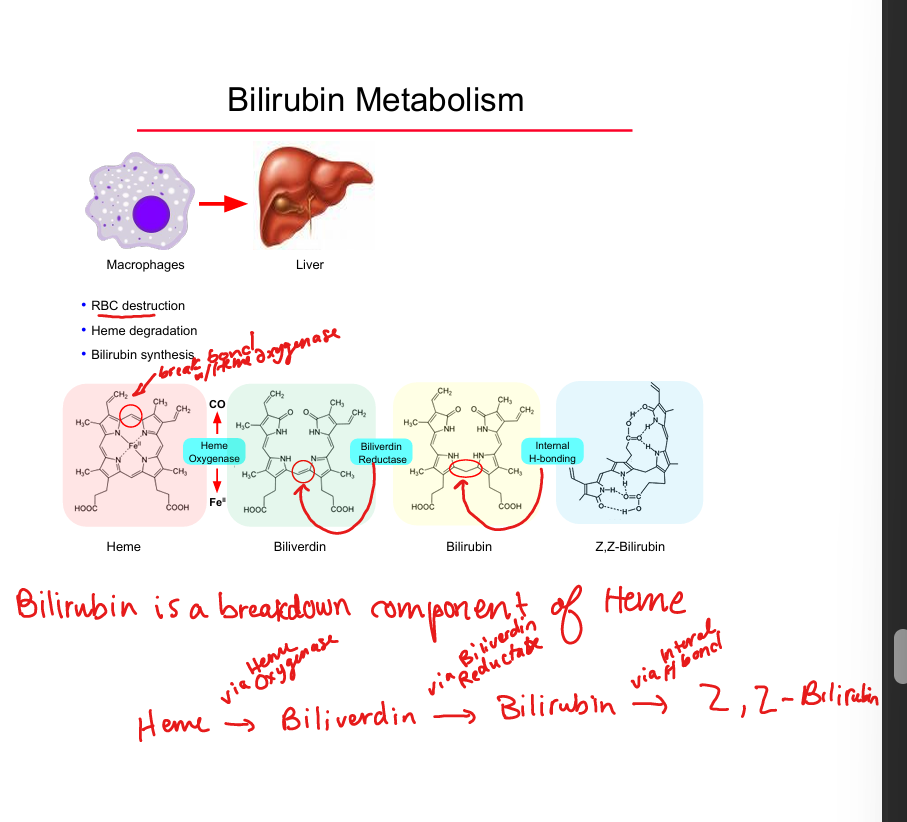
Heme → biliverdin enzyme
Heme oxygenase
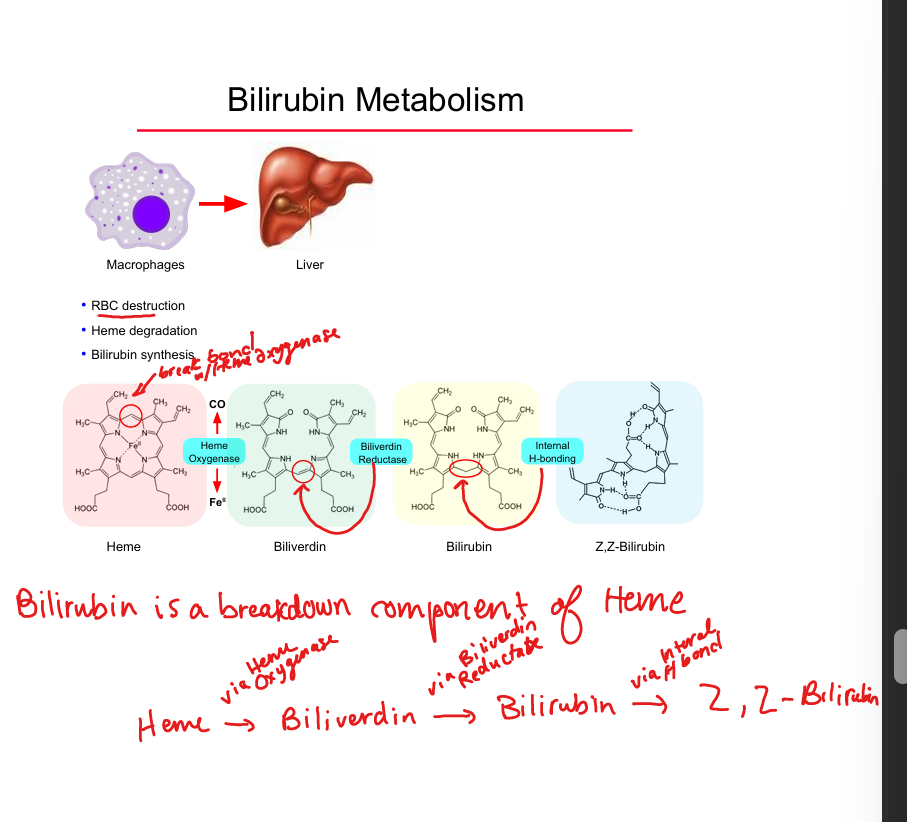
Biliverdin → bilirubin enzyme
Biliverdin reductase
Unconjugated bilirubin transport
Bound to albumin in plasma
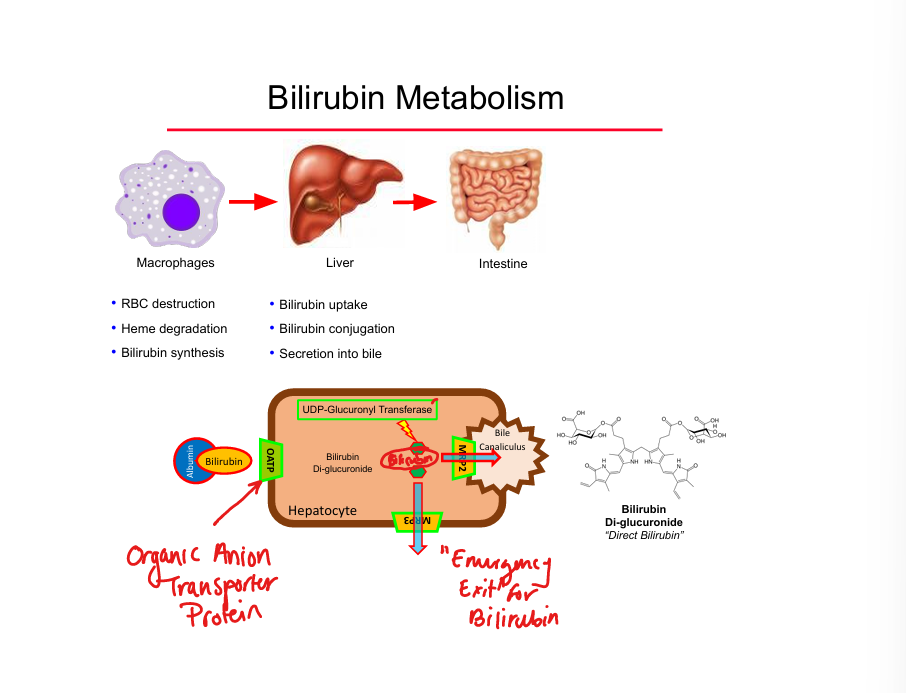
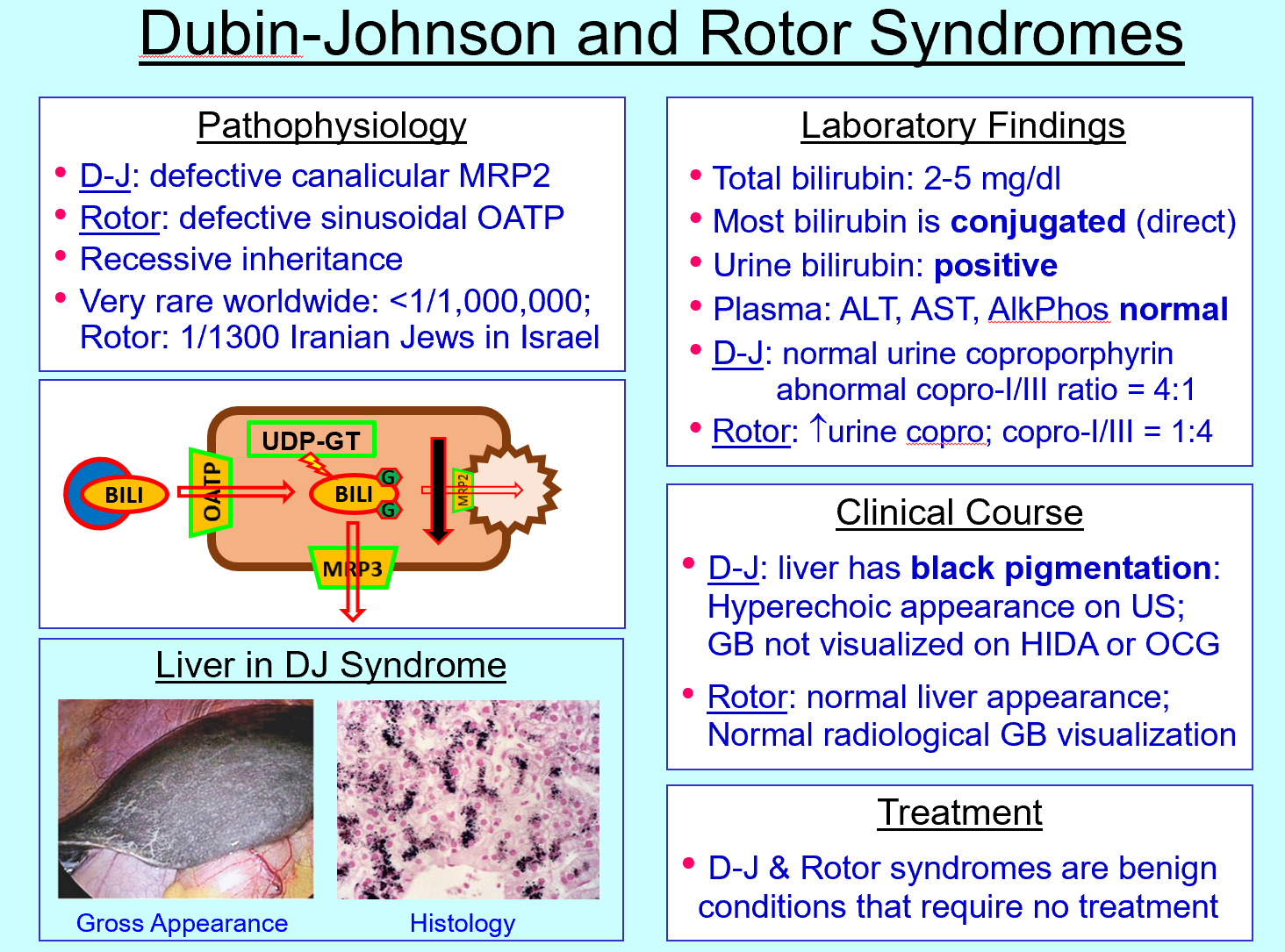
Bilirubin conjugation enzyme
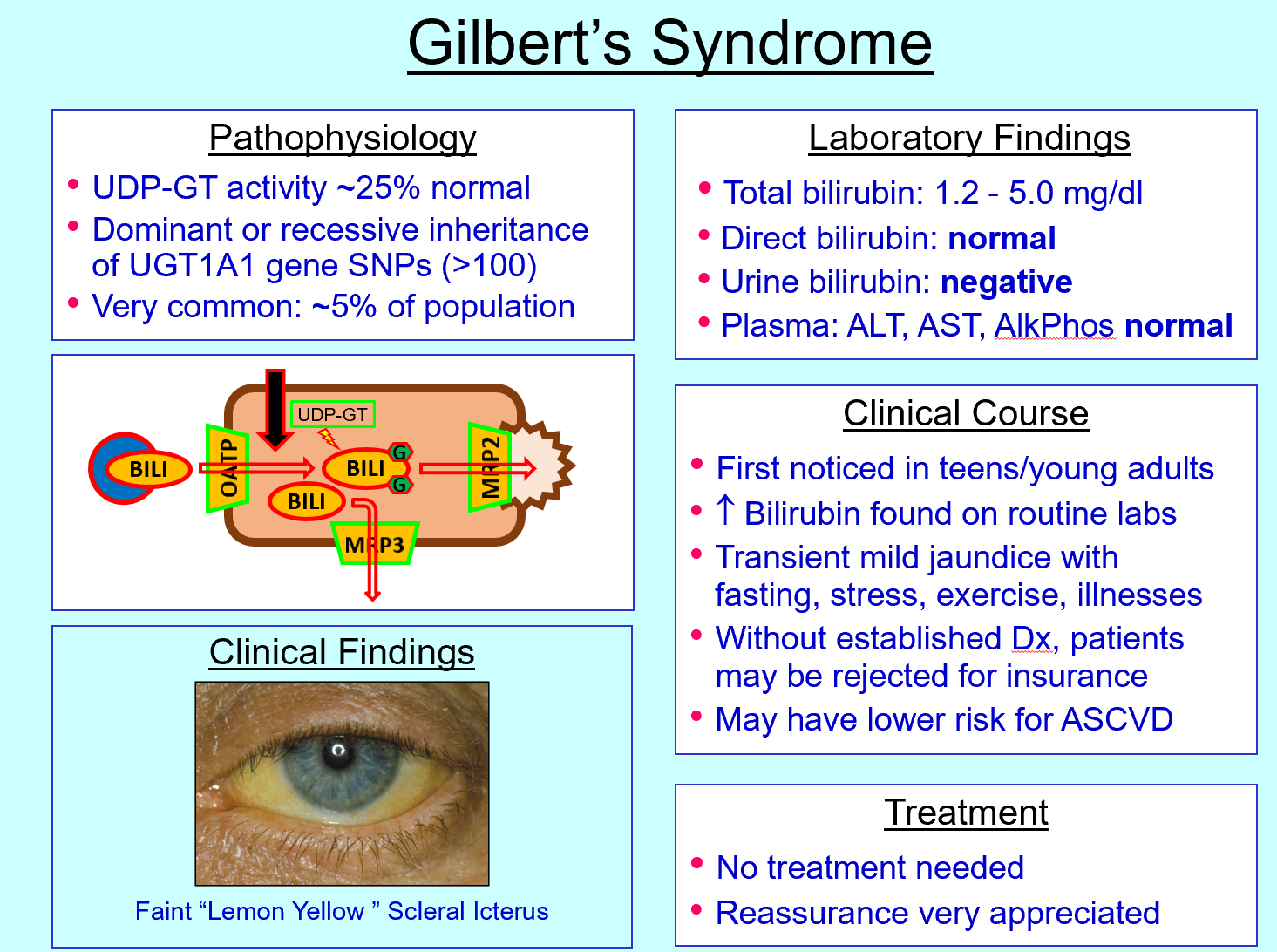
UDP‑glucuronyl transferase (UDP‑GT)
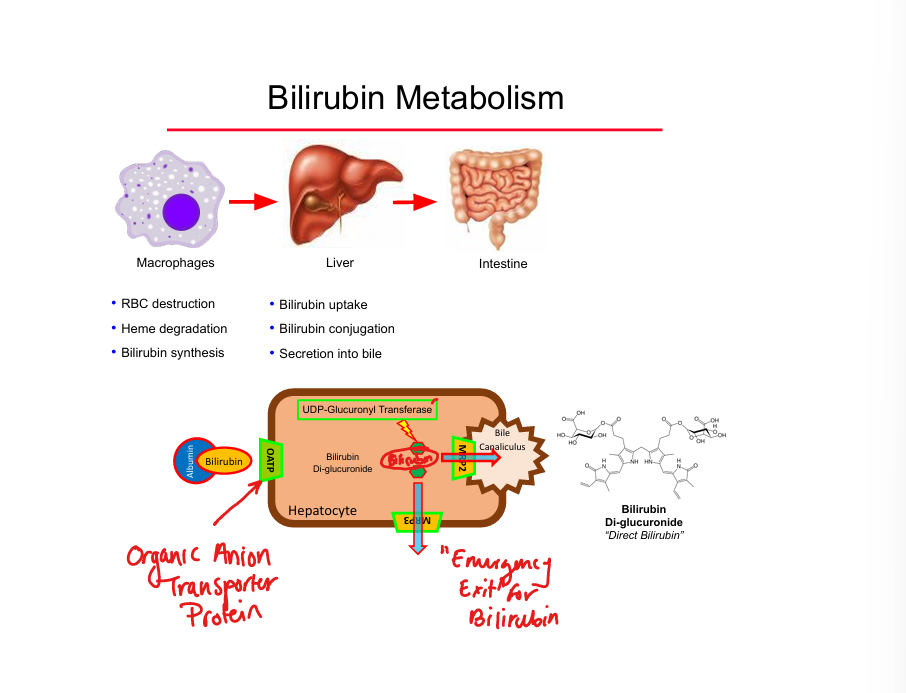
Conjugated bilirubin transporter into bile
MRP2
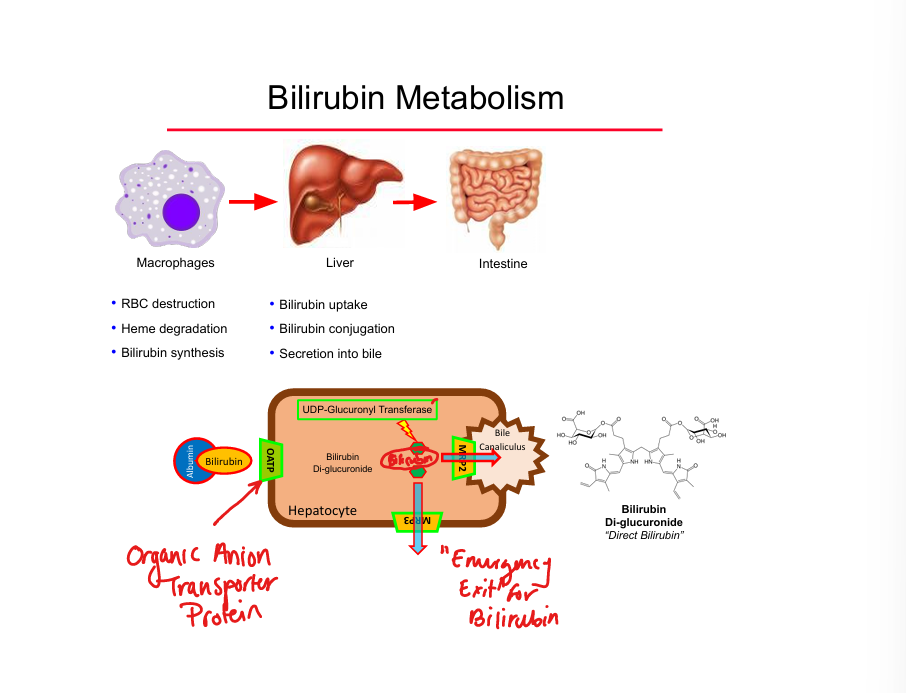
Emergency bilirubin efflux transporter
MRP3
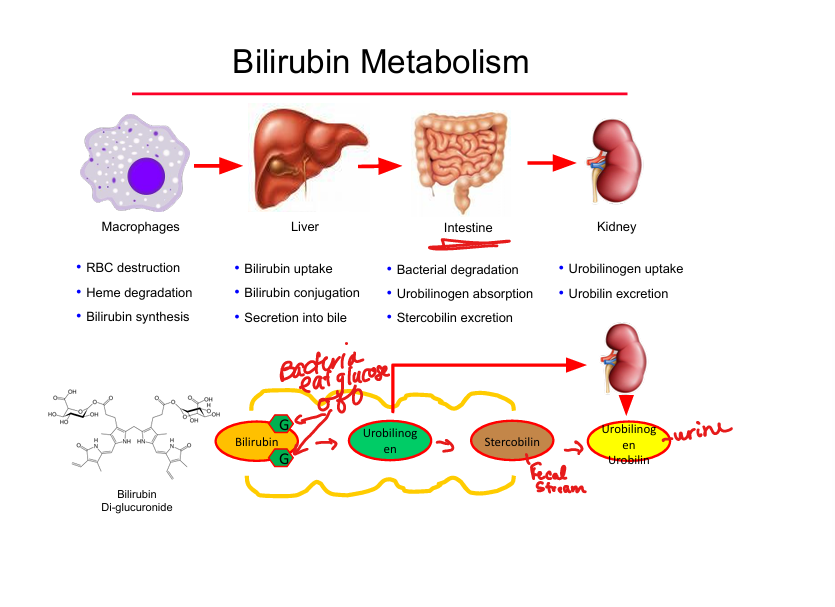
Bilirubin → urobilinogen location
Intestinal bacterial metabolism of glucose on the bilirubin
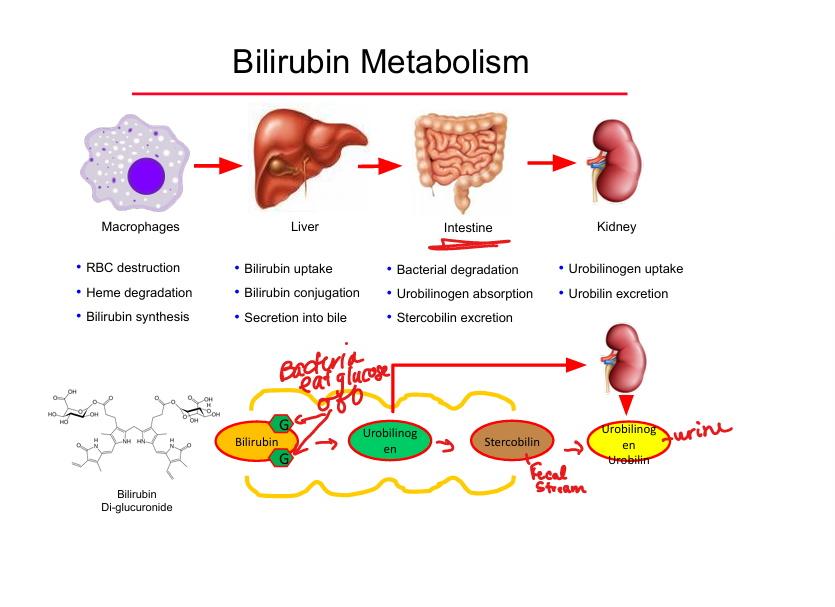
Urobilinogen fates
Reabsorbed → urine (urobilin) OR feces (stercobilin)
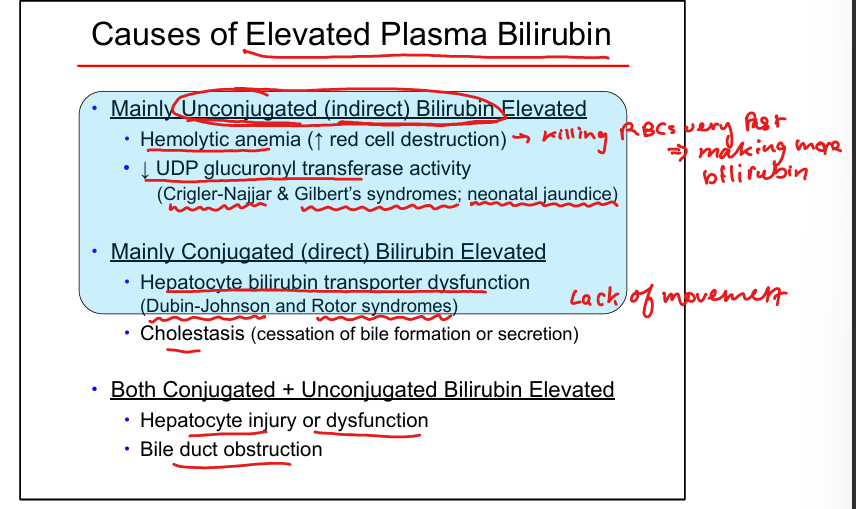
Unconjugated hyperbilirubinemia causes
Hemolysis, Gilbert syndrome, Crigler‑Najjar, neonatal jaundice
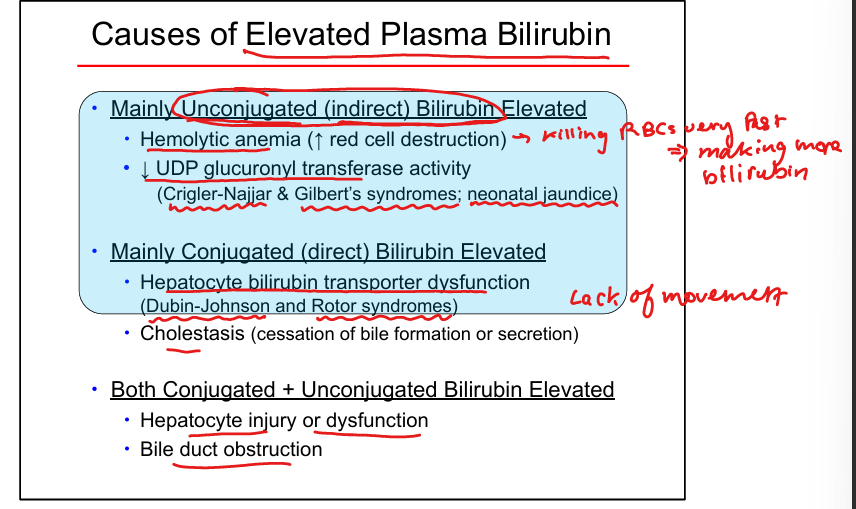
Conjugated hyperbilirubinemia causes
Dubin‑Johnson, Rotor, cholestasis
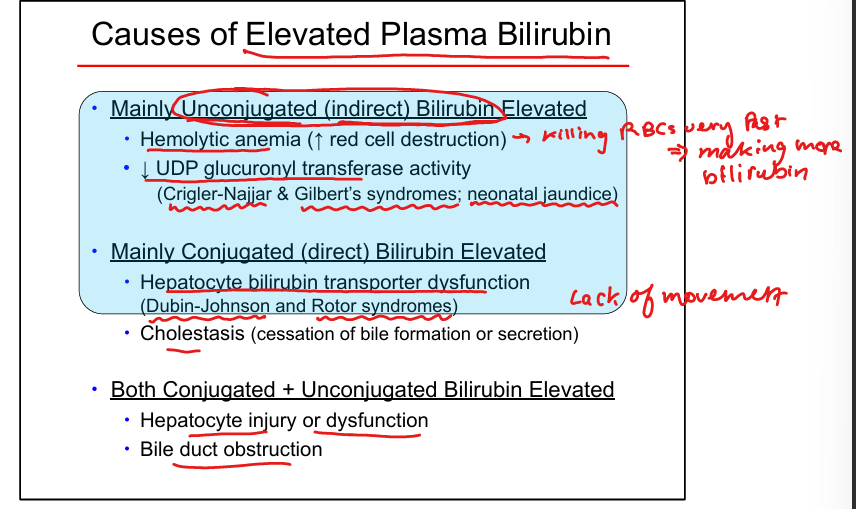
Mixed hyperbilirubinemia causes
Hepatocellular injury, bile duct obstruction
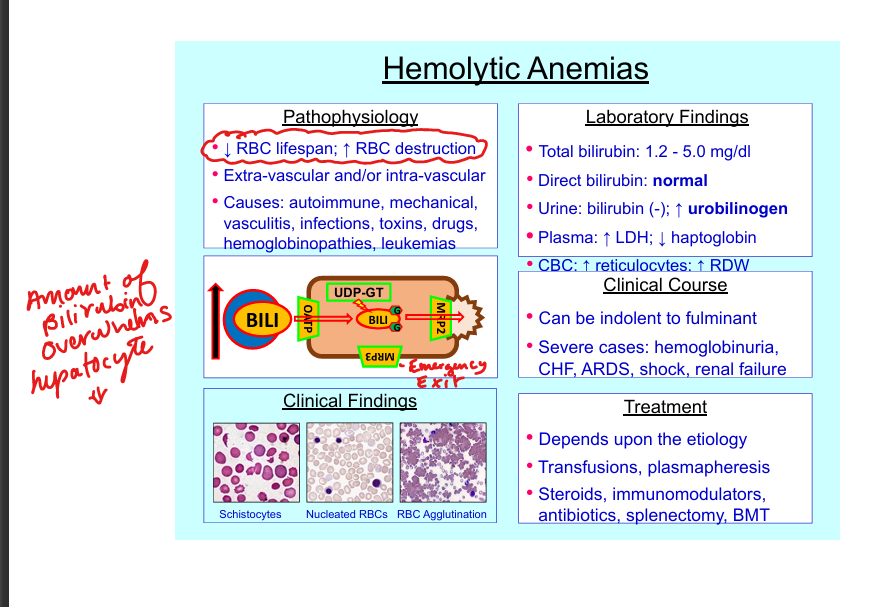
Hemolytic anemia bilirubin pattern + cause
↑ total bili, normal direct, ↑ urobilinogen, no urine bilirubin; all caused by a decreased RBC lifespan and inc RBC destruction
Gilbert syndrome defect
↓ UDP‑GT activity (~25% normal)
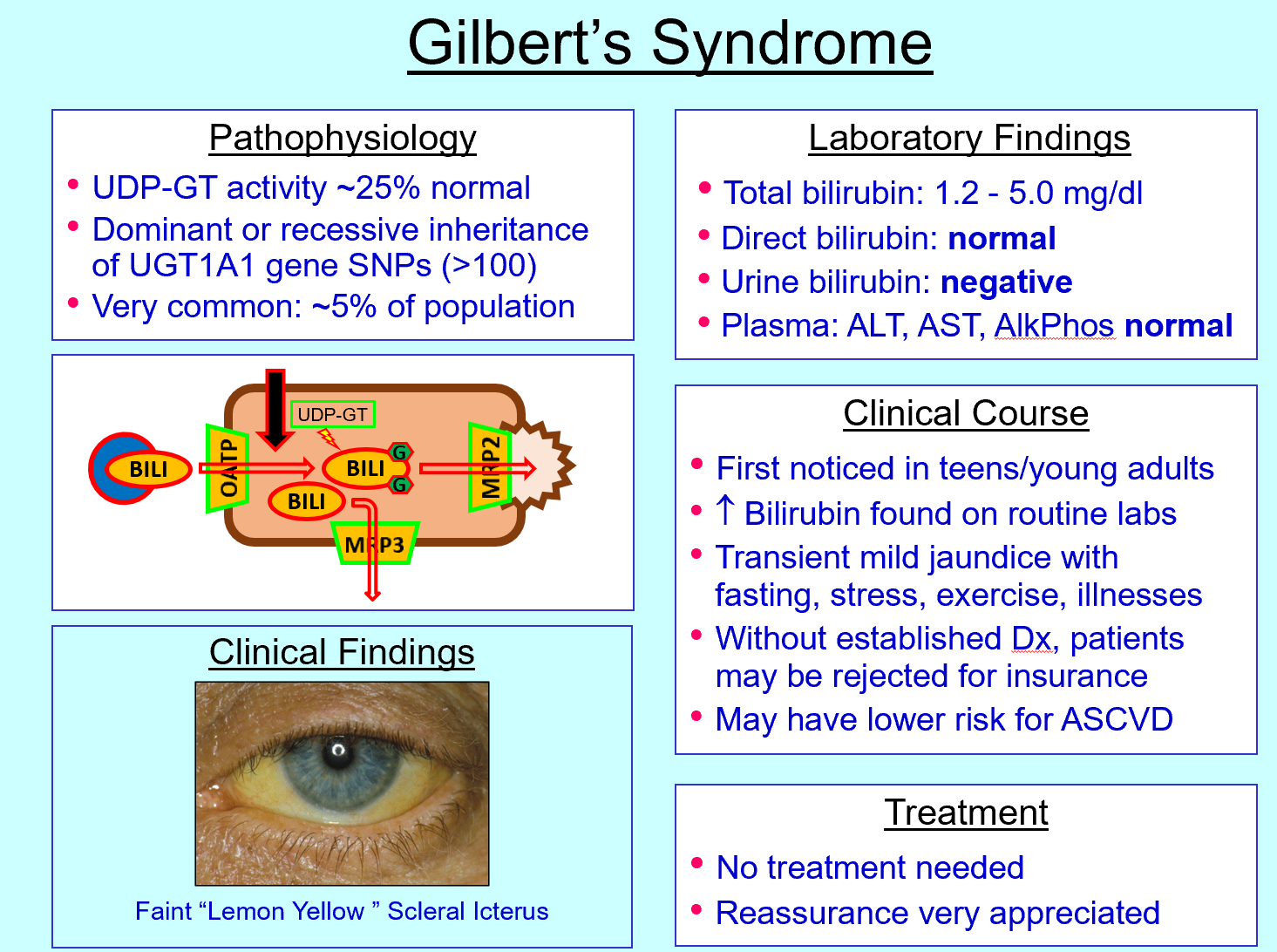
Gilbert syndrome features
Mild jaundice during stress/fasting
Crigler‑Najjar type I defect
Absent UDP‑GT
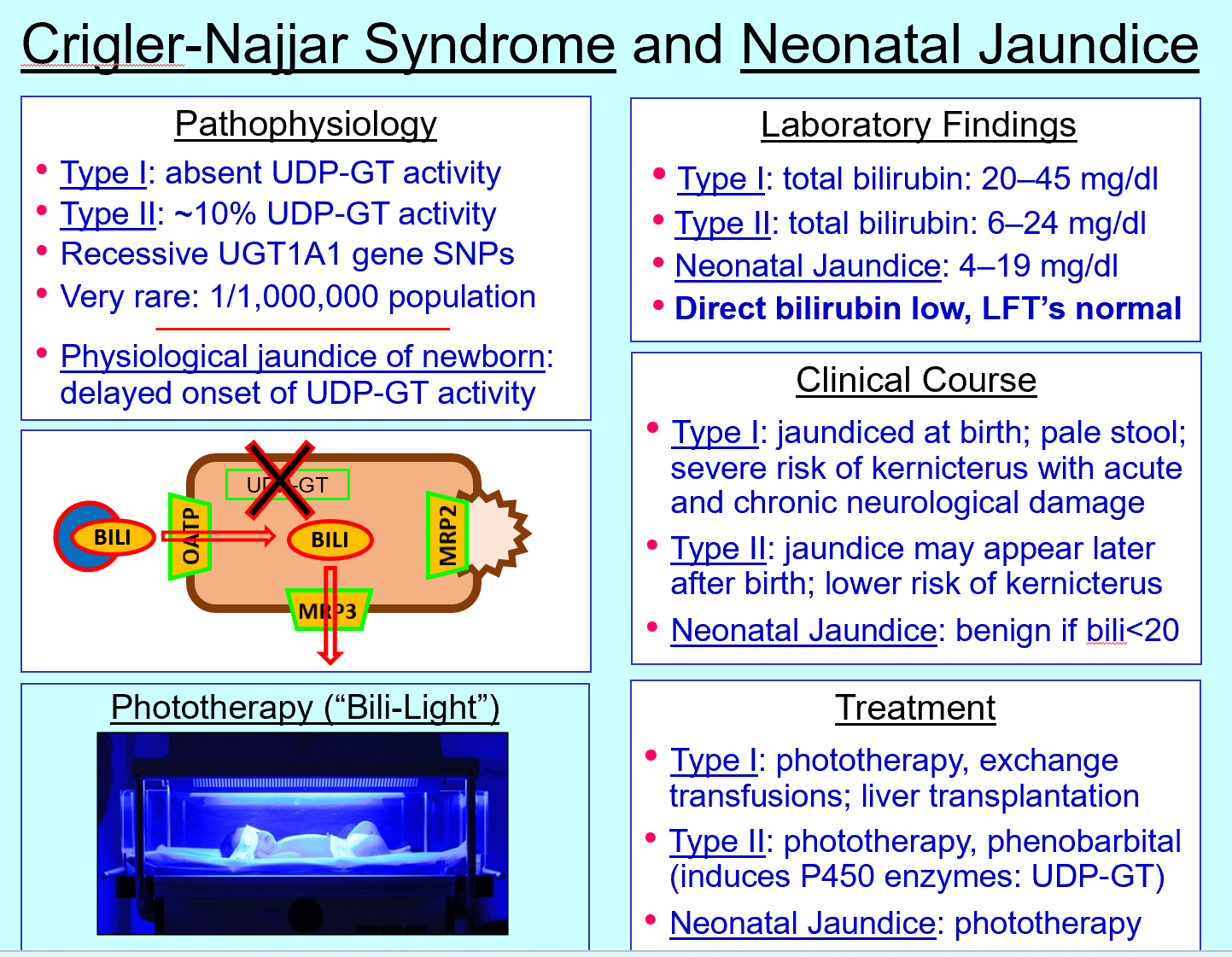
Crigler‑Najjar type I features
Severe unconjugated hyperbilirubinemia, kernicterus risk
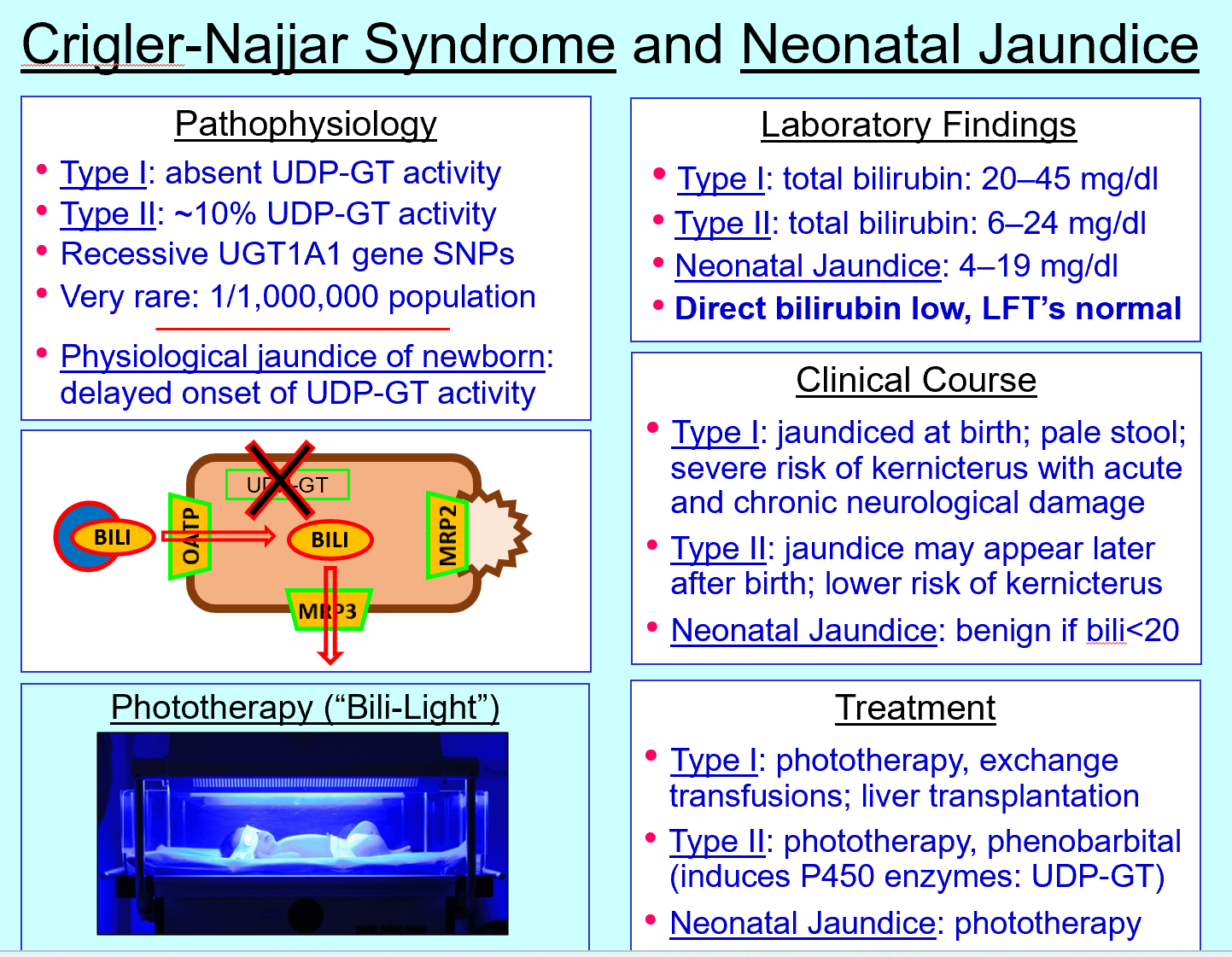
Crigler‑Najjar type II defect
~10% UDP‑GT activity
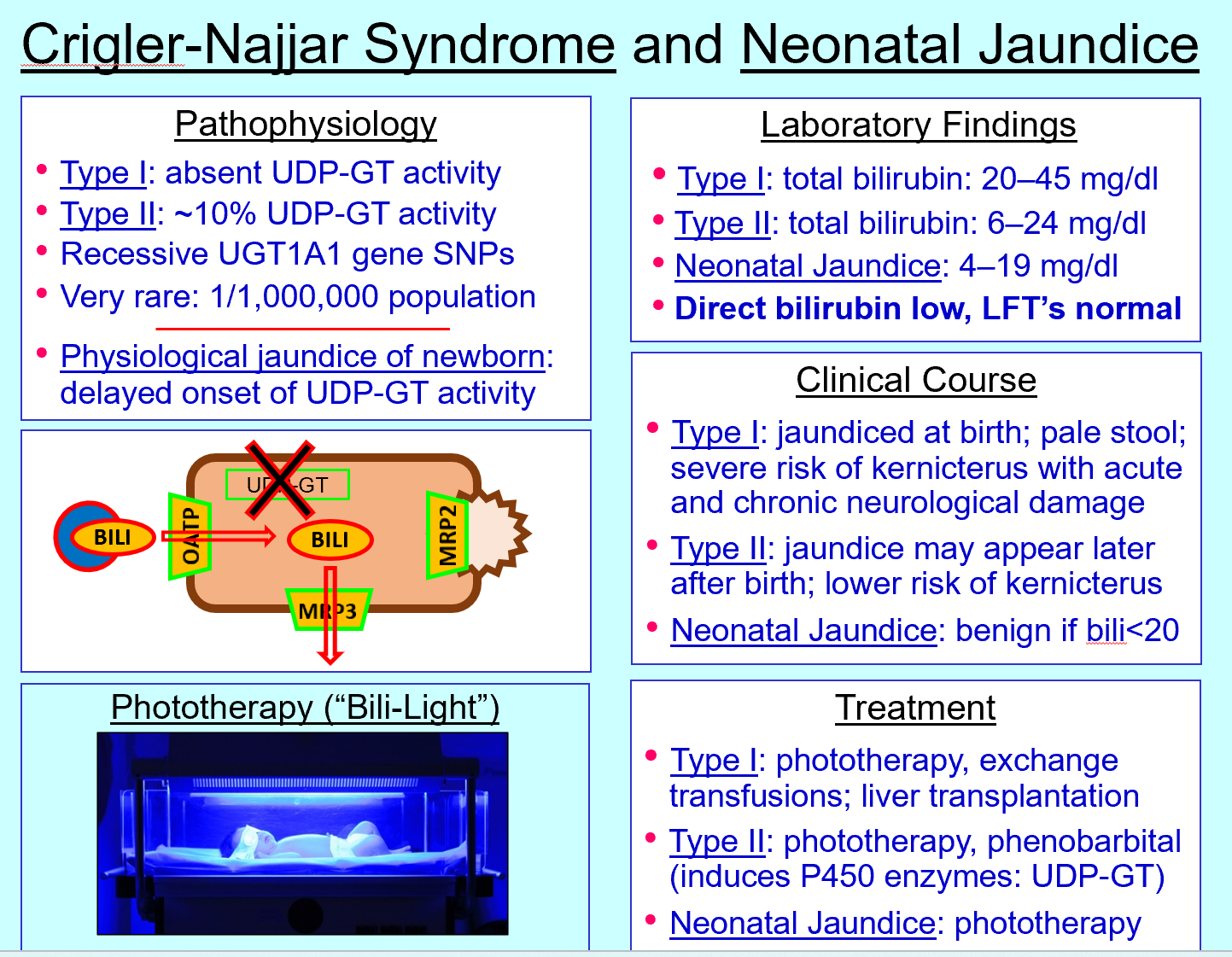
Crigler‑Najjar type II treatment
Phenobarbital (induces UDP‑GT) + phototherapy
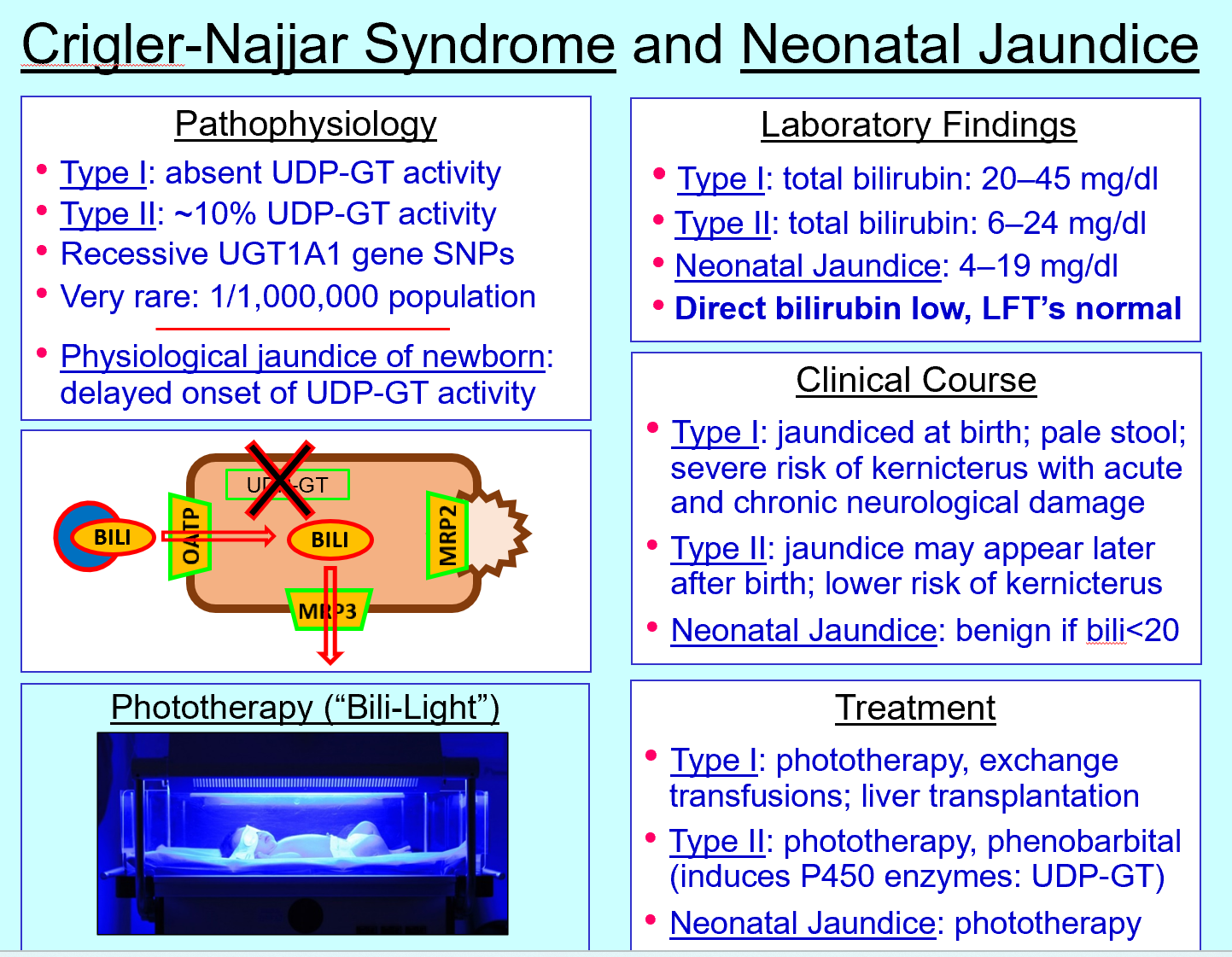
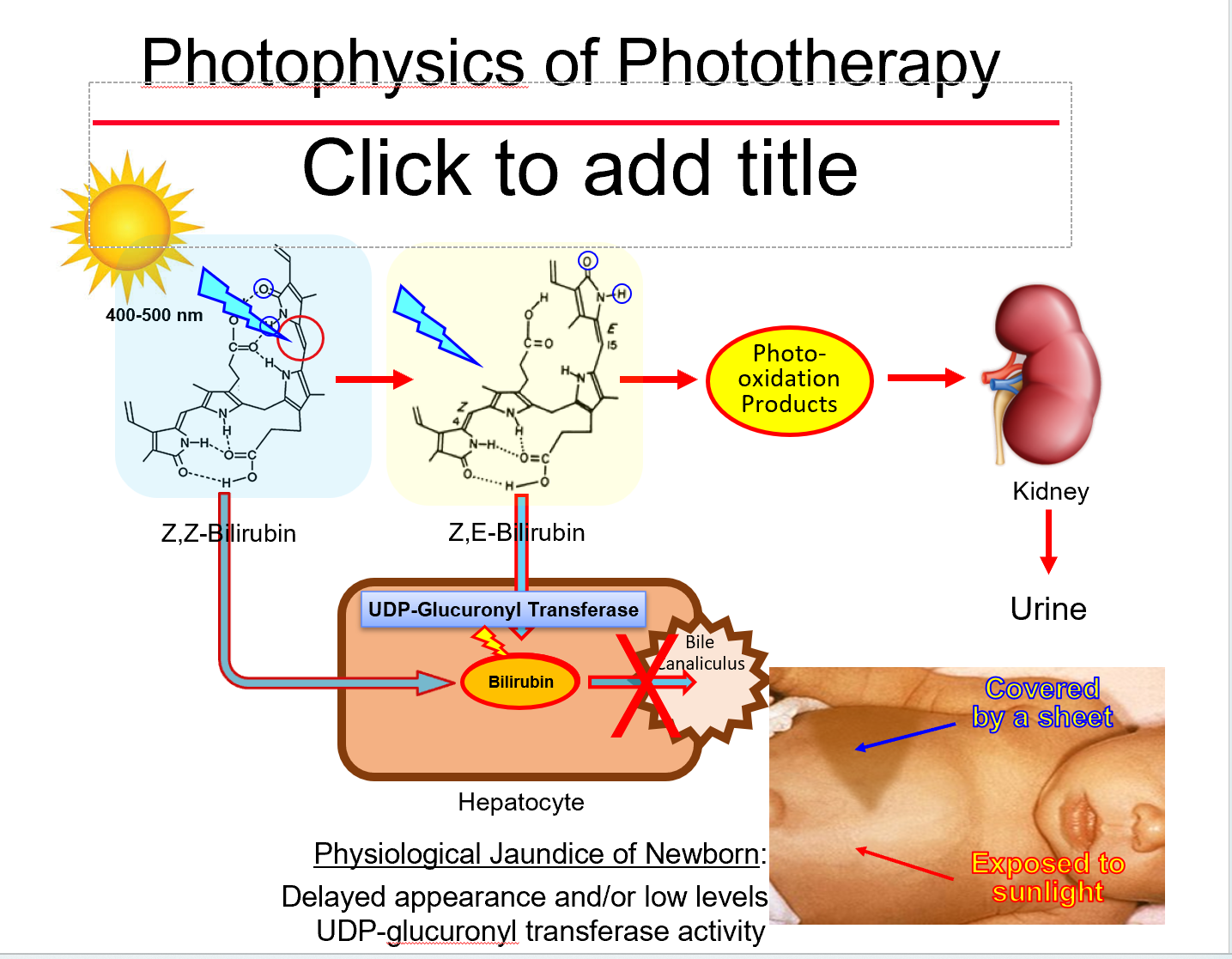
Neonatal jaundice cause
Delayed UDP‑GT activity
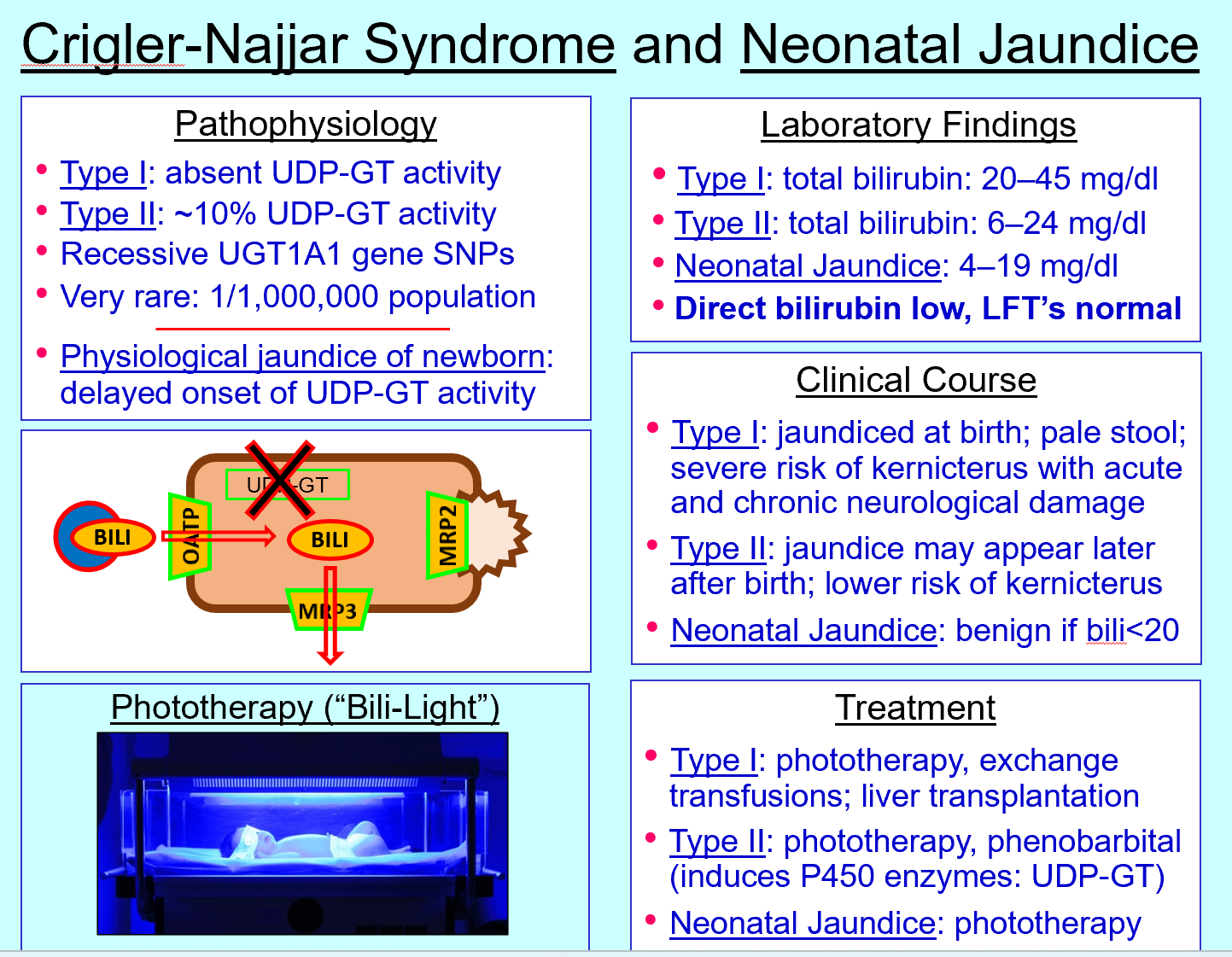
Phototherapy mechanism
Converts bilirubin to water‑soluble isomers excreted without conjugation
Dubin‑Johnson syndrome defect
MRP2 transporter deficiency
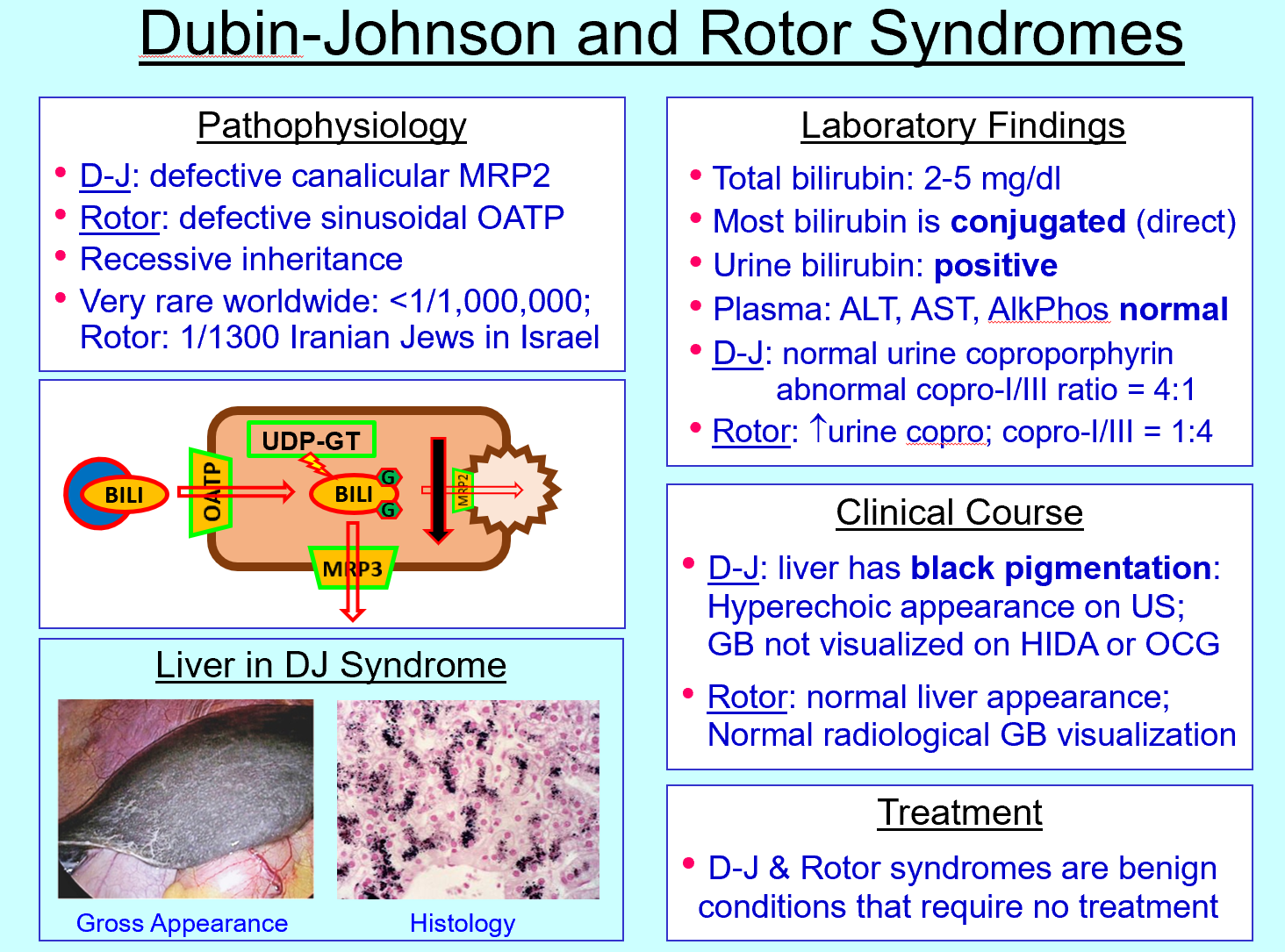
Dubin‑Johnson features
Conjugated hyperbilirubinemia, black liver, benign
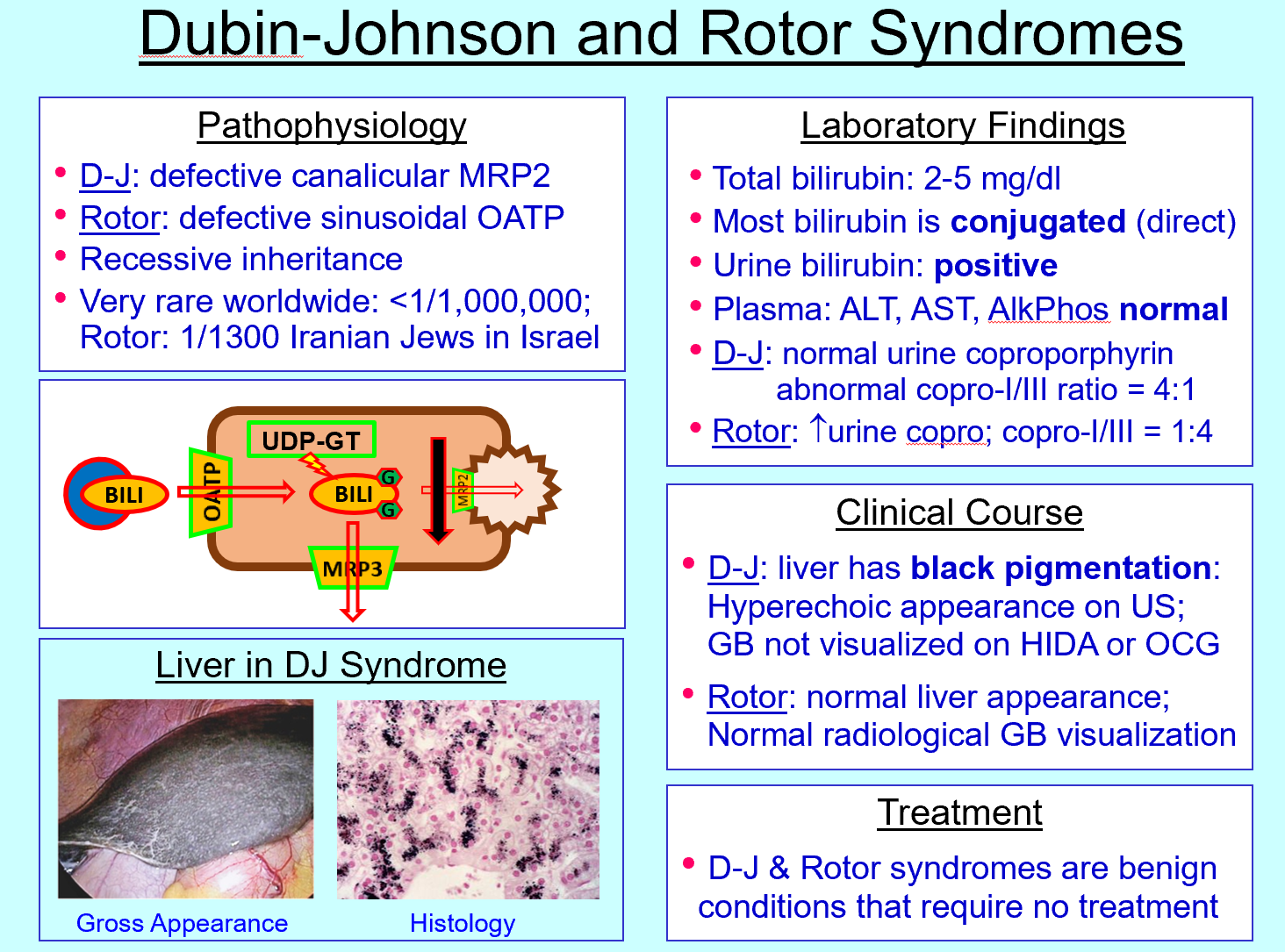
Rotor syndrome defect
OATP transporter defect (sinusoidal uptake)
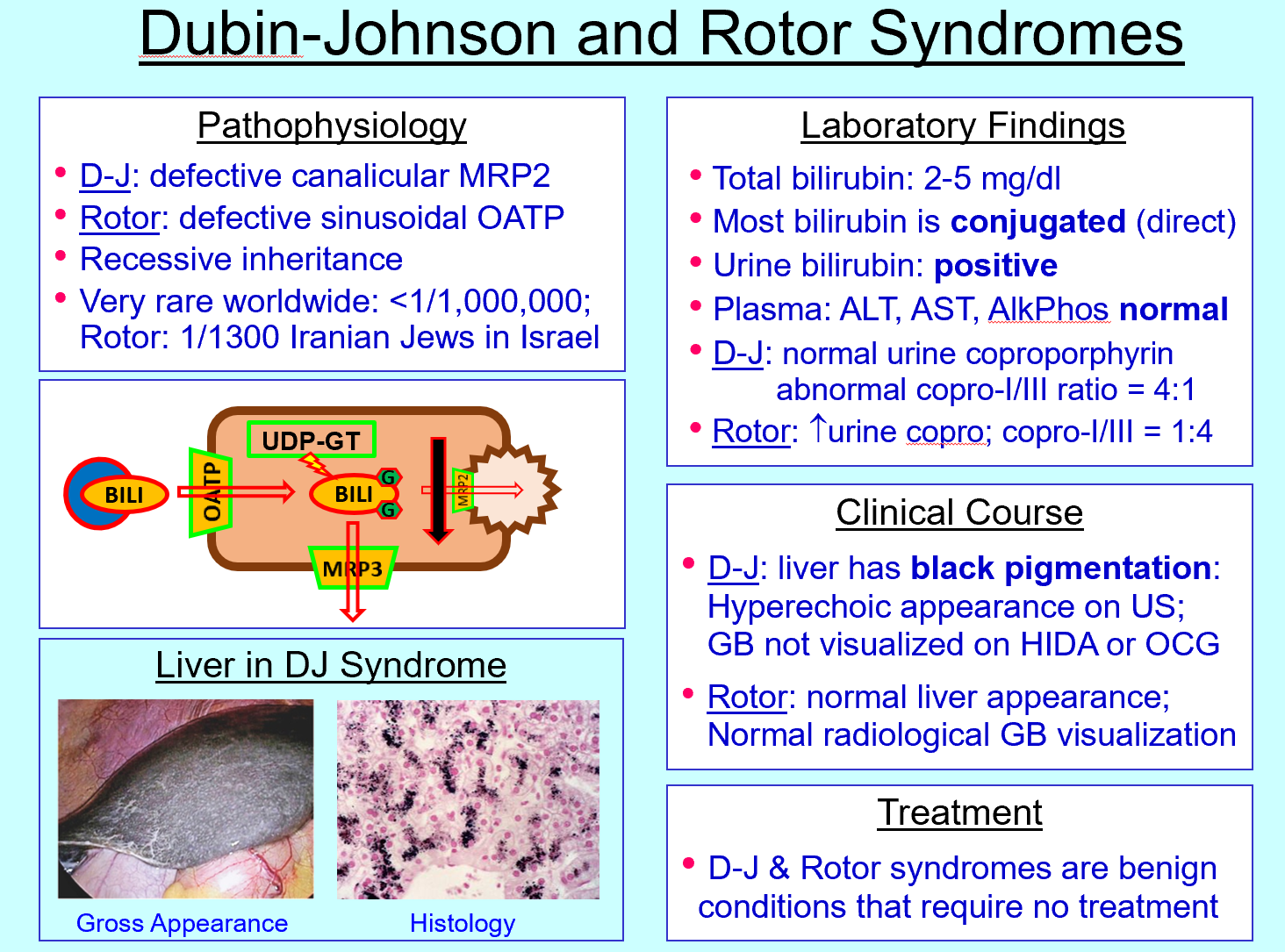
Rotor syndrome features
Bilirubin has difficulty getting into and stored in liver cell via OATP “door” defect» will travel to blood stream »Conjugated hyperbilirubinemia, normal liver pigmentation
Urine bilirubin significance
Indicates conjugated bilirubin (water‑soluble)
Urine urobilinogen significance
Elevated in hemolysis
Cholestasis bilirubin pattern
↑ direct bilirubin, pale stools, dark urine
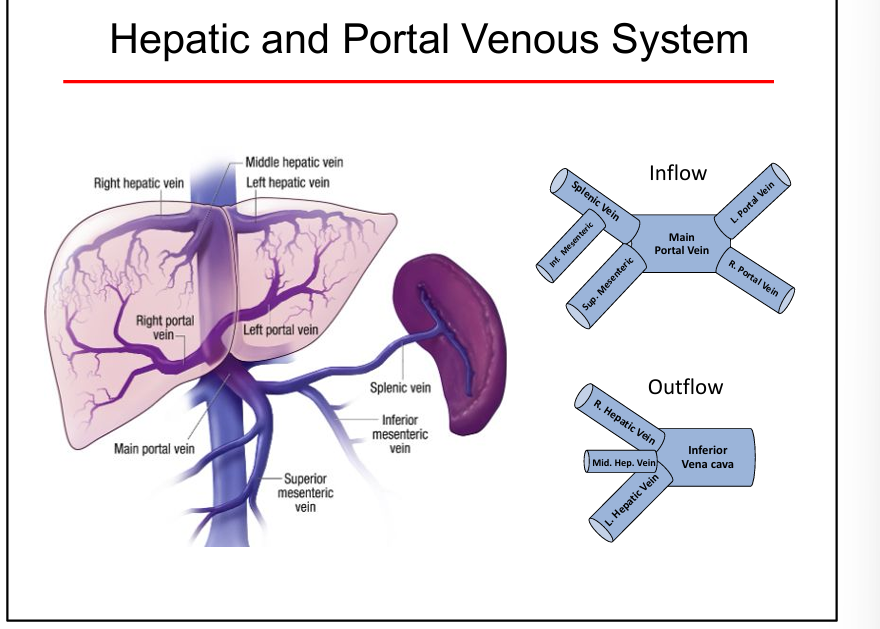
Portal vein function
Delivers nutrient‑rich blood from GI tract to liver