Health and disibility final exam prep
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
Controlling costs – Health expenditures as % of GDP, how much of the gdp are attributed to healht expenditures
how has this changed with time? 2020, 1980, now (2026)
why are these expendatures so high
Health care expenditures are approximately 20% of U.S. GDP [edit: clarified “GDP” means total market value of all goods and services produced in a country in a given year].
Timeline: In 1980: 9.2%,
in 2020: 19.7%.
Projected for 2026: $16,167 per person (vs. ~$1,100 in 1980s).
Why are expendatures so high: Growth due to..
high prices,
lack of standardization,
lack of transparency,
low-value care,
minimal government regulation,
high physician wages,
complex patient care,
and paying for social determinants of health.
Health costs and outcomes model
Healthcare costs and outcomes model
Use? -
Provides a framework for discussion, analysis, and decision making
The relevant outcome of interest is the overall population vs an individual
Results that spending more money does not improve outcomes
Strategies for cost control – Painless methods
Control provider fees/incomes,
cut drug/supply prices ([edit: U.S. prescription drugs ~50% higher than other countries]),
reduce administrative waste,
unnecessary interventions/technologies,
increase preventive services to lower hospitalizations.
Where U.S. health care money goes
~⅔ from rising prices faster than other sectors,
~¼ from increased quantity of services. More specialists = higher costs.
Financing vs. reimbursement controls
Financing: flow of money from individuals/employers to health plans.
Reimbursement: money flowing from health plans to providers.
Stratagies for cost control: Financing controls – regulatory vs. competitive
Financing controls
Regulatory: limits on taxes or premiumas
Competitive
Stratagies for cost control: Reimbursement controls –
uses price controls
regulatory or competative
Price controls (regulatory or competitive), quantity controls (aggregate payment units, patient cost sharing, utilization management, supply limits), and mixed controls.
Stratagies for cost controls: utilization
defined as quantity controls
aggregating units of payment
payment cost sharing
utalization management
supply limits
Use and Drawbacks of financing controls: regulatory and competative stratages
Regulatory
The government’s regulation of taxes = control over public expenditures
Drawback: increasing taxes is a political process + inadequate support = larger budget deficits
Competitive strategies
Health insurance plans compete based on price and are rewarded for lower costs
Drawbacks: us is not very good at controlling costs = higher premium plans
Cost containment – controlling quantity. How do you do it? what polcicies should we focus on? hint ther are 5
Changing the unit of payment (global cost containment tools)
More aggregated units of payment to counter cost inflation due to provider pressure to increase quanity
More risk shifted to the provider- fee schedules or expenditure caps
Paintent cost sharing
Point of service” utalization
Individuals with cost sharing plans ⅓ fewer office visits and hospitalized ⅓ less times - leads to a reduction of preventative services
Us has one of the highest leves of cost sharing of any nation but hte highest overall costs
utilization management
Insururser examine physician behaior and use of services and apply a micromanagement approach .
Looking more at the entire practice
supply limits
puts a limit on the number of providers + material resouces
requires physccicans to prioritze services on the approprieatents and urgency of patient need
controling supply limits
control the number of genralists vs specialsits
overgenralization
Micromanagement of capacity and budgets
Global cost containment tools - paying by capitation or aggregated methods, limiting size and speciality mix of providers, concentrating high-tech services regionally
Global cost containment tools to use (similar to quantity controls)
Capitation or aggregated payments, limiting provider numbers/specialty mix, regionalizing high-cost services.
Affordable Care Act – 4 main components
1) Insurance market reforms (no preexisting condition denials, no lifetime/annual caps, coverage until age 26, essential benefits)
cannot deny based on preexisting conditions
ended lifteime/anual caps
standardized essential bennefits.
2) Public program expansion (Medicaid up to 138% FPL).
if you are up to that level of the fedral poverty line
3) Health insurance marketplaces (buy plans if 138–400% FPL with subsidies).
you can buy your own plan if you do not qualify for any of those meausres
if you are between 138-400% of the income line the govnerment subsitizes some of this for you
4) Individual mandate ([edit: repealed in 2017]).
you have to have insurance or else you pay a fine
What are some of the levels of the health insurance market places
Do not qualify above? You can buy your won plan if you make between 138-400% of the fpl (government will substidise part of it for you)
Bronze – you receive minimal credible coverage. The plan covers 60% of the benefit costs of your plan.
Silver – covers 70% of the benefit costs of your plan
Gold – covers 80% of the benefit costs of your plan
Platinum – covers 90% of the benefit costs of your plan. \
ACA – Key coverage measuresy
High-risk pools for uninsured with preexisting conditions;
dependent coverage to age 26;
no lifetime caps;
no denial for children with preexisting conditions;
Medicare Part D coverage gap reduction;
Medicaid expansion to 133–138% FPL;
insurance exchanges; employer mandate (>50 employees must provide insurance).
Employer “Pay or Play” mandate
- employers with more than 50 employees have an approximately $2000/ employee penalty if they do not offer an employer sponsored plan to atleast 95% of full time employees
ACA financing reforms
Higher-income individuals pay more into Medicare; excise tax on high-cost employer plans;
fees on pharma/insurance companies;
more generic drugs;
reduced Medicare payments to hospitals with excess readmissions.
private insurance
no refusals for coverage due to preexisting conditions
no mor elife tieme limits
children now covered until 26
state responsiblity
states are responsible for enrolling newly eligable medicare beneficiaries
medicare payments were reduced to hospitals that had excess admisssions
the approval of more generic drugs
ACA quality improvement measures
Bundled Medicare payments;
performance-based Medicare payments to hospitals;
reduced malpractice litigation;
funding for preventive services with no copays.
for screenigns for gestational diabees, cervical cancer, breastfeeding support, domestic violence, contraceptives, or chekcups
4 ways to get insurance under ACA
Employment-based – for those who work for an employer that has more than 50 employees, your employer must offer you health insurance
Medicare – If you are over 65, have chronic renal disease, ALS, or are disabled, you qualify for Medicare
Medicaid – when the ACA was signed into law, you qualified for Medicaid if your income was below 133% of the FPL. Now the income qualification is up to 138% of the FPL.
Health Insurance Marketplace Exchanges - If you do not qualify for any of the above, you may buy your own health insurance plan. In all but 19 states if you make between 138-400% of the FPL the government will subsidize part of the premium for your health insurance. It was up to each individual state to decide if they wanted to expand Medicaid up to 400% of the FPL. Some decided to and some did not.
National health insurance – common features of the ACA
Benefit package includes hospital, doctor visits, imaging, rehab, prescriptions ([edit: excludes long-term care and dental]);
covers baseline needs
minimal patient cost sharing;
a single payer system (national heaht insurance plan would minimize patient cost sharing. helps minimize people bing underinsure
cost containment via global budgets and fee regulation.
global budget and have regulation on fees
Primary reasons why quality is lacking in U.S. health care
Lack of access to care, (these are the primary causes
not all people have acces to the same services
practice variations and defects, (primary causes
overuse of services,
underuse of effective care,
underuse of generic drugs= things costing too much
and misuse/errors.
inefficiecny and wastes
long delays and waits for services
lack of communication between different hospitals
Never events (serious hospital errors not reimbursed)
Surgery on the wrong body part or wrong patient
Wrong surgery on a patient
Foreign object left in a patient after surgery
Death/disability associated with intravascular air embolism, incompatible blood, or hypoglycemia
Stage 3 or 4 pressure ulcers after admission (these occur when a patient is left in one position for an extended period— the skin breaks down and an ulcer develops).
Death/disability associated with electric shock, a burn incurred within a facility, or a fall within a facility.
Donabedian’s quality assessment model
hree central things influence outcomes
Structure, process, are influencing outcomes
Structure (source inputs)
Facilities
Must be licenced and accredited to make sure standards are met
Joint commissions accredits hospitals
The commission on accreditation of rehabilitation facilities (CARF) accredits rehab
Equipment
Equipment in hospitals and rehab facilies needs to be up to date
Staffing levels
Proper staff and adiquae levels
Staff qualifications
Qualified staff
Delivery system
Distribution of beds and staff
Process (actual delivery of services)
Interpersonal aspects of care (how patients are treated. How things are communitcated. Empathy and wahtnot)
To improve you much touch upon all aspects
Common HEDIS indicators? definition
healthcare effectiveness data and information set
What indicators does it includ
Children immuninized
Mammograms
Pap smears
Prenatal exams
Eye exams for diabetic patients
Osteroperosis screaning
bmi
Methods to achieve malpractice reform
Tort reform (limits on awards to patients for malpractice),
alternative dispute resolution (mediation/arbitration),
substituting mediation and arbatrition for jury truals
use of practice guidelines to assess negligence,
no-fault reform (compensation without proving negligence),
providing copensation to paitens suffering medical injury regardless of negligance or not
enterprise liability (institutions responsible for compensation).
making institutions responsible for cpomensations to improve quality of care need
What are some Proposals to improve quality of healhtcare outside of cost? who does this
Continuous Quality Improvement (CQI) that allows providers to explain mistakes instead of immediate punishment; quality report cards;
Electronic Health Records (EHRs);
Artificial Intelligence (AI).
National commits for quality assurance (NCQA)
Created healthcare effectiveness data and Information Amset (HEIDS)
Goal = compare performace and publicize that information to help improve clinical care
Role of EHRs and AI in quality improvement
HITECH Act (2009) led to EHR adoption in ~90% of hospitals, streamlining patient care but sometimes reducing interpersonal communication
takes up more time to doccument too
. AI helps organize large data sets, reads digital images, and can outperform human pathologists.
Components of high-quality care
adequate access to care
Competent healthcare providers
Adequate scientific knowledge
Money and quality of care
Organization of health insitutions (being able to have information transformed easily)
Who would qualify for what: Rehabilitaiton, skilled nursing, nursing home - custodial only, hospice and home care
Hospital care: used for acute conditions with a one or shorter effects or for chronic conditions
Rehabilitation facilities: complex medical management or intense rehabilitation services. You have to be able to withstand 3 hours of therapy per day. Ex stroke patient tin recovery to bring them back to normal affairs
Skilled nursing Facility: offers skilled nursing and rehabilitative services
Used for patients who are not able to withstand 3 hours of therapy but still need therapy (medicare covers 100 days
Maintenance care (not covered)- assisting with daily living or activities
Like elderly care homes
Nursing home
Provide only custodial care (maintenance) - just help with daily living. You just live there not expecting to leave
Hospice:
Covered if you are terminally ill adn have les than 6 monyhs
The following things are covered
Intermittent nursing care, physical therapy, occupational therapy and speech therapy.
Doctors’ services
Medications including outpatient drugs for pain relief
Home health aide/homemaker
Medical social services
Medical supplies
Counseling
Unfortunatley there are significant gaps in coverage
Home care:
When proviers come to your home to provider care to you
What do you need for medicare to cover this
Patient needs intermittent skilled nursing, physical therapy, occupational therapy or speach therapy
Patient is home bound
Physician must certify that there is reasonable cause for improvement
Medicare does not cover custodial care.
Most pay out-of-pocket until Medicaid eligible.
have to run out of a good portion of life savings
Private LTC insurance exists but is expensive/high deductible; ~13% of costs out-of-pocket.
PACE Program (On Lok Model)? when was it started? who finances it? what does it manage/ who does it help? purpose
Community-based care for 55+ to avoid nursing homes. Financed by Medicare/Medicaid. Manages multiple chronic conditions and ADL dependencies to keep elders in community.
Combines all the necessary care needs for an elderly person
started in the 70s
assumes financial risk for frail individuals
These programs try to keep people out of nursing homes and hospital facilites
Money Follows the Person (MFP)? How does it work?
Medicaid program helping nursing home residents transition to community living with flexible service funding and home modifications.
How does mfp work
Allows for flexible funding helping states develop the infrastructure and process needs for transitions
Provides financial assistance for particiipatns
Medical Home
Primary care model with coordinated team managing all aspects of patient care to improve quality and outcomes.
it is an apporach to providng comprehensive primary care… not an actual place lol. it extends outside of the hospital
Continuous process: assess community needs → develop policy → assure services → reassess.
ASSURANCE GOES TO ASSESMENT WHICH INFLUENCE PPOLICY DEVELOPMENT AND IT GOES INTO A CIRCLE
How is this working
Public health officials begin with assessing community nees
Passing initiates should be next to promote teofrm
Ex food pyramid to base nutrition
Prevention (two components)
Primary prevention
Preventing the first occursnde (ex immunizations)
Secondary prevention
Early detection of sisease (ex mammogram)
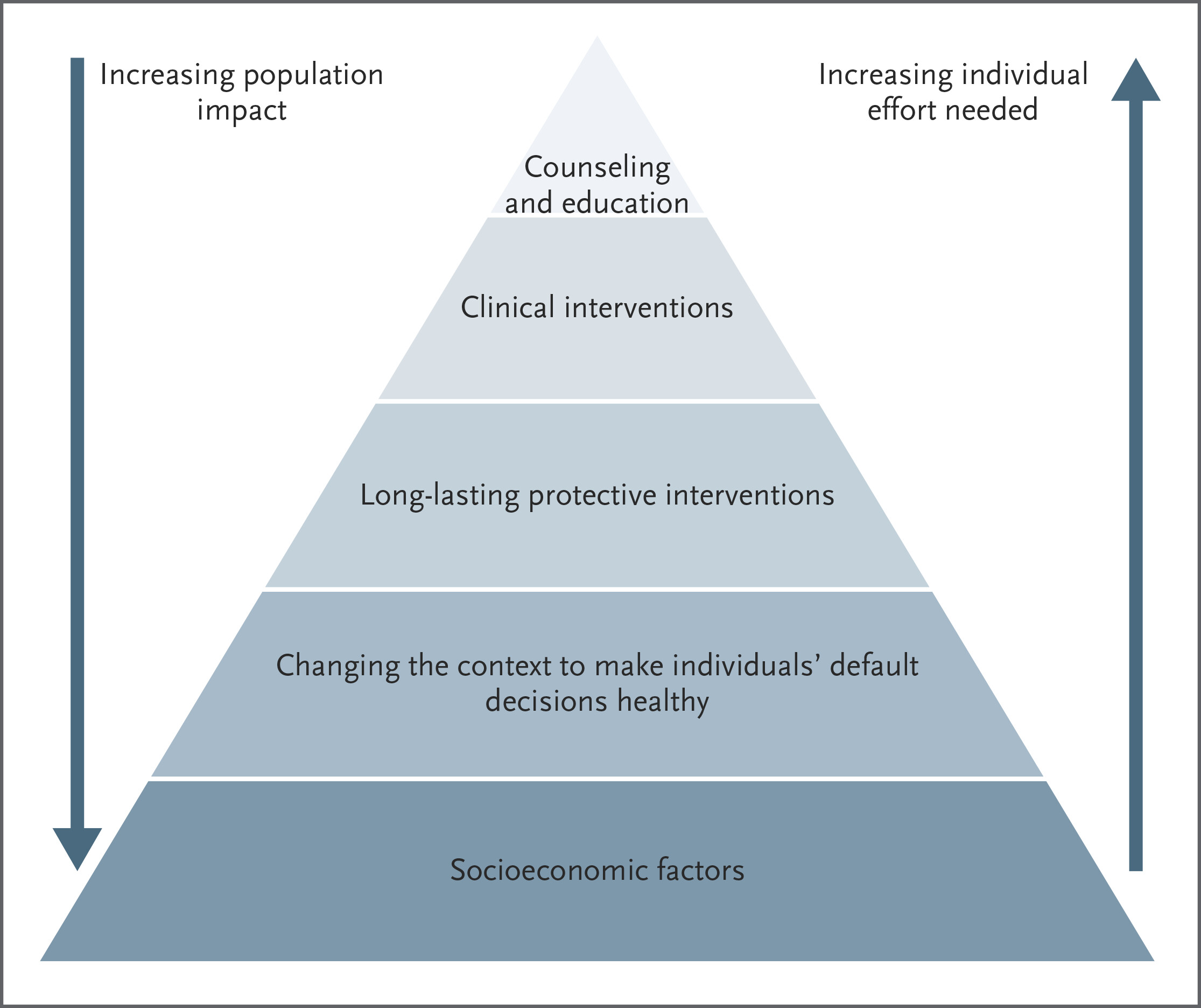
5 levels of intervention (bottom to top)
Socioeconomic factors (baseline needs)
Indiciduality
Long lasting preventing conditions.
Clinical interventions
Counseling and intervention (topeteor needs like malows hierarchy of needs)
Levels of Intervention (triangle graph:hint)
Socioeconomic factors → Changing context (policy/environment) → Long-lasting protections (vaccines) → Clinical interventions → Counseling/education. Population impact decreases from broad to individual.
How is the NHS funded? How do hospitals and doctors get paied
Funded by taxes (single-payer).
uses a single payer (hospital) for healthcare
What does it cover?
coveres nearly all care
no cost for transport or seeing a doctor for the country
Who has access
everyon regarlesss of profession through a pcp
How does the cost of care and outcomes compare to the Us
better life expectancy and lower the costs than the us
Covers nearly all care. Universal access via PCP. Better life expectancy & lower costs than US. Weakness: long waits for disability/chronic care.
Public insurance (Medicare) funded by taxes, for citizens/permanent residents. Private insurance offers faster care/perks
note private care may be better for those with chronic conditions or non urgent conditions
. Government sets drug/treatment prices. Strain from people dropping insurance → rising costs.
Universal healthcare system with no public/private split.
Strengths: coordinated resources, hospitals not overwhelmed during COVID.
Gaps: LTC, mental health, financial aid, tech delays.