NURS 3070: ADH1: MODULE 4: Gastrointestinal Disorders PRT 1
1/190
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
191 Terms
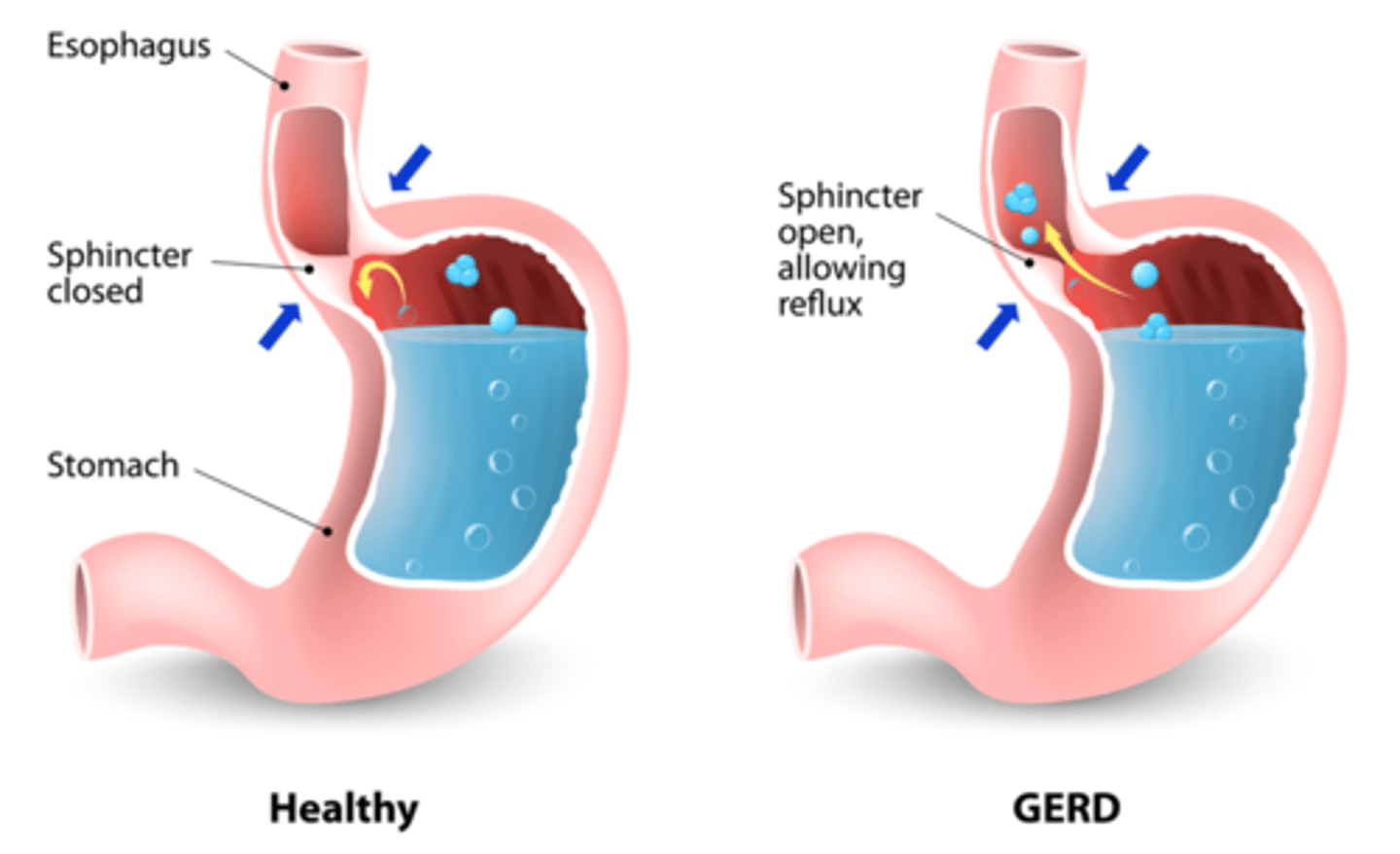
What does GERD stand for?
Gastroesophageal Reflux Disease
What happens in GERD?
Backflow of gastric and duodenal contents into the esophagus
What causes GERD?
Incompetent lower esophageal sphincter, pyloric stenosis, hiatal hernia, and motility disorders
What symptom does an incompetent lower esophageal sphincter cause?
Burning pain from acid reflux
What is pyloric stenosis?
Narrowing of the opening between the stomach and small intestine
How does a hiatal hernia contribute to GERD?
The stomach pushes through the diaphragm into the chest, allowing acid reflux
What diagnostic tests are used for GERD?
Endoscopy, barium swallow study, and wireless capsule or transnasal catheter placement
What is the gold standard test for GERD diagnosis?
Transnasal catheter placement
What are common risk factors for GERD?
Tobacco use, alcohol, caffeine, H. pylori infection, and obesity
What can happen if GERD is left untreated?
Mucosal injury to the esophagus and complications such as PUD, IBS, or airway disorders
Gastroesophageal Reflux Disease (GERD)
Q: What are common clinical manifestations of GERD?
Heartburn (pyrosis), epigastric pain, dyspepsia, nausea, regurgitation, and pain or difficulty swallowing
What are the hallmark symptoms of GERD?
Pyrosis (Heartburn/Burning sensation) and regurgitation
What does hypersalivation mean in GERD?
Increased production of saliva
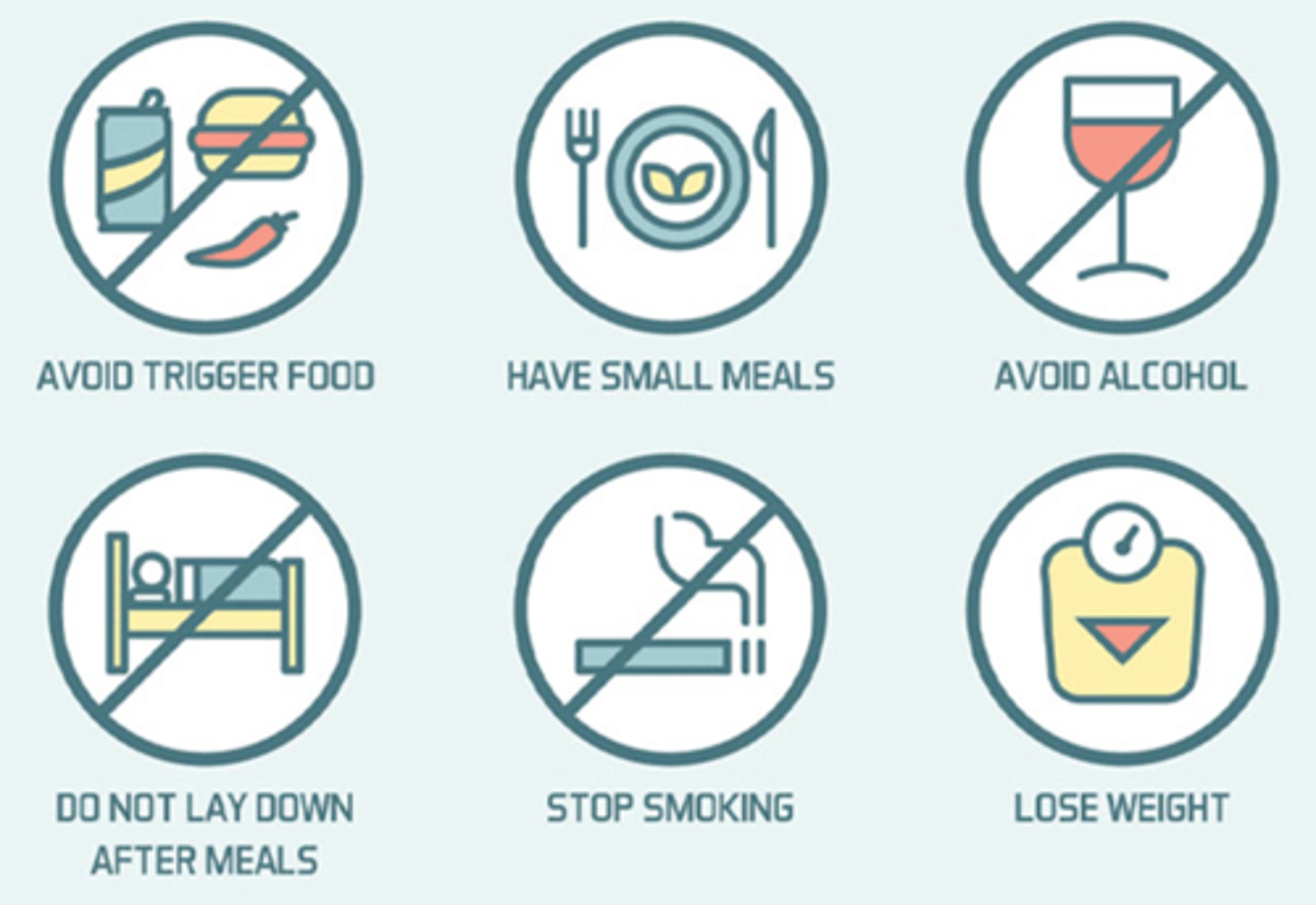
What are key lifestyle modifications for GERD?
Avoid caffeine, tobacco, alcohol, or carbonated beverages; avoid fried or fatty food; avoid peppermint or chocolate; do not lie down directly after eating.
What should GERD patients avoid consuming?
Caffeine, tobacco, alcohol, carbonated beverages, fried or fatty foods, peppermint, and chocolate.
What dietary pattern is recommended for GERD?
Low-fat, high-fiber diet.
When should GERD patients avoid lying down?
Directly after eating.
What are examples of lifestyle changes to manage GERD?
Avoid trigger foods, eat small frequent meals, avoid alcohol, stop smoking, lose weight.
What body position is recommended for GERD management?
Semi-Fowler's position (head of bed at 30 degrees).
What type of clothing should GERD patients avoid?
Tight clothes.
What is the purpose of maintaining normal body weight in GERD?
To decrease pressure on the lower esophageal sphincter.
How should meals be structured for GERD patients?
Smaller, more frequent meals (may not be necessary with medications).
GERD nursing interventions
What should patients with GERD avoid before bedtime?
Drinking or eating 2 hours before bedtime
What medications should be avoided with GERD?
NSAIDs (ibuprofen, Motrin) and medications that contain acetylsalicylic acid
What is a recommended nursing intervention for GERD at night?
Elevate the head of bed at night
What medications are used to manage GERD?
Antacids, H2 receptor antagonists, and proton pump inhibitors
Where can medication management for GERD be found in the textbook?
Table 39-4, p. 1258 (15th edition)
What are additional lifestyle education points for GERD management?
Avoid trigger foods, eat small meals, avoid alcohol, do not lie down after meals, stop smoking, and lose weight
Gastritis (picture)

What is gastritis?
Inflammation of the gastric or stomach mucosa.
What causes the irritation and inflammation in gastritis?
Disruption of the mucosal barrier that normally protects the stomach tissue from digestive juices.
What happens when the mucosal barrier is disrupted in gastritis?
Corrosive acid (pepsin) and other irritants can irritate the gastric mucosa, causing inflammation.
Is gastritis a common gastrointestinal problem?
Yes, it is a common GI problem that affects men and women equally.
Can gastritis be acute or chronic?
Yes, gastritis may be acute or chronic.
What are the clinical manifestations of acute gastritis?
Epigastric or abdominal pain/discomfort
Dyspepsia (indigestion)
Anorexia, nausea, and vomiting
Hiccups
Reflux
Erosive gastritis may cause bleeding
Melena or hematochezia (bright red blood)
How is the onset and duration of acute gastritis typically described?
Usually transient, rapid onset, and self-limiting — lasting hours to days
What are the risk factors for acute gastritis?
NSAIDs/aspirin (Motrin), corticosteroids, H. pylori infection, binge drinking, spicy or irritating foods, gastric radiation, acute illnesses/injuries (burns, severe infections)
What are the two main types of acute gastritis based on cause?
Erosive: caused by local irritants (NSAIDs, corticosteroids, alcohol, gastric radiation); Non-erosive: caused by gram-negative bacterium H. pylori
What are the treatments for acute gastritis?
Eliminate the cause, NPO until no symptoms, supportive medications (treat nausea/vomiting & anxiety, pain relief), IV fluids if persistent, may need NG tube, monitor for bleeding
How does the gastric mucosa heal after an acute episode of gastritis?
It can repair itself, typically taking about one day to recover, with appetite returning in 2-3 days.
What supportive measures may be needed for fluid replacement in acute gastritis?
2-3 liters of fluid and electrolyte replacement.
Why might a patient with acute gastritis require an NG tube?
To help remove gastric secretions and monitor for bleeding.
What are the clinical manifestations of chronic gastritis?
Fatigue, pyrosis (heartburn) after eating, belching, sour taste in the mouth, halitosis (bad breath), early satiety (feeling full after small meals), anorexia, nausea, and vomiting.
What causes chronic gastritis?
Repeated exposure to irritating agents and reoccurring episodes of acute gastritis.
What happens to the stomach in chronic gastritis?
Inflammation and atrophy of the gastric mucosa occur, leading to diminished intrinsic factor production.
Why can chronic gastritis cause vitamin B12 deficiency?
Because of loss or atrophy of parietal cells, which decreases intrinsic factor production.
What condition can result from vitamin B12 deficiency due to chronic gastritis?
Pernicious anemia.
What are the risk factors for chronic gastritis?
NSAIDs, H. pylori, drinking, smoking, reflux, dietary habits, autoimmune disorders
What are the treatments for chronic gastritis?
Modify diet, promote rest and decrease stress, avoid alcohol, tobacco, and NSAIDs, supportive medications, treat H. pylori with amoxicillin and a proton pump inhibitor (PPI), initiate medications
What are some long-term causes of chronic gastritis?
Recurrent episodes of acute gastritis, prolonged exposure to irritants, long-term NSAID use, autoimmune disorders (e.g., Hashimoto's, Addison's, Graves' disease)
What is the treatment regimen for H. pylori infection in chronic gastritis?
Amoxicillin, clarithromycin, and pantoprazole (PPI)
Why is pain relief important in chronic gastritis?
To reduce irritability and anxiety in patients
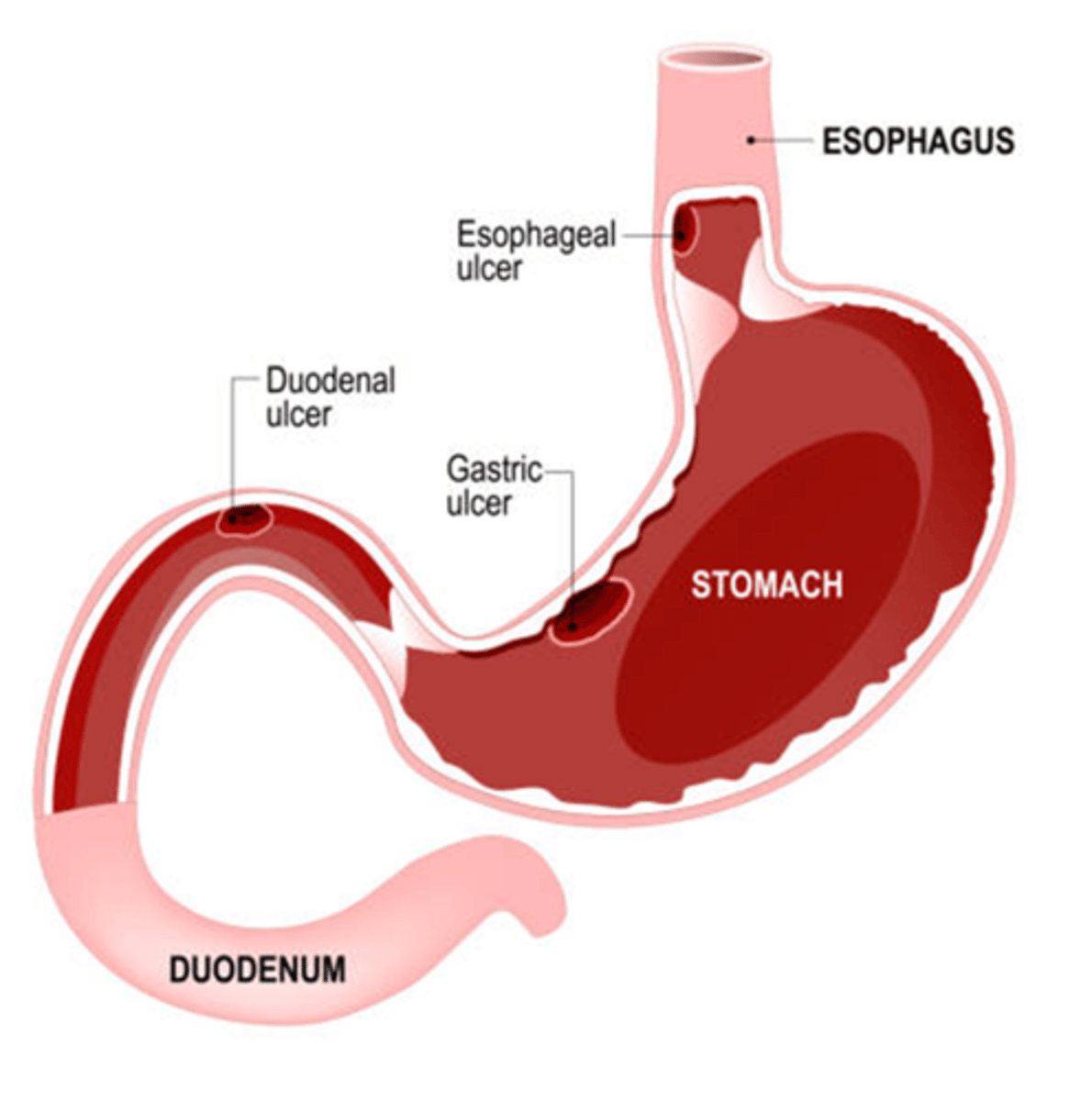
Peptic Ulcer Disease (picture)
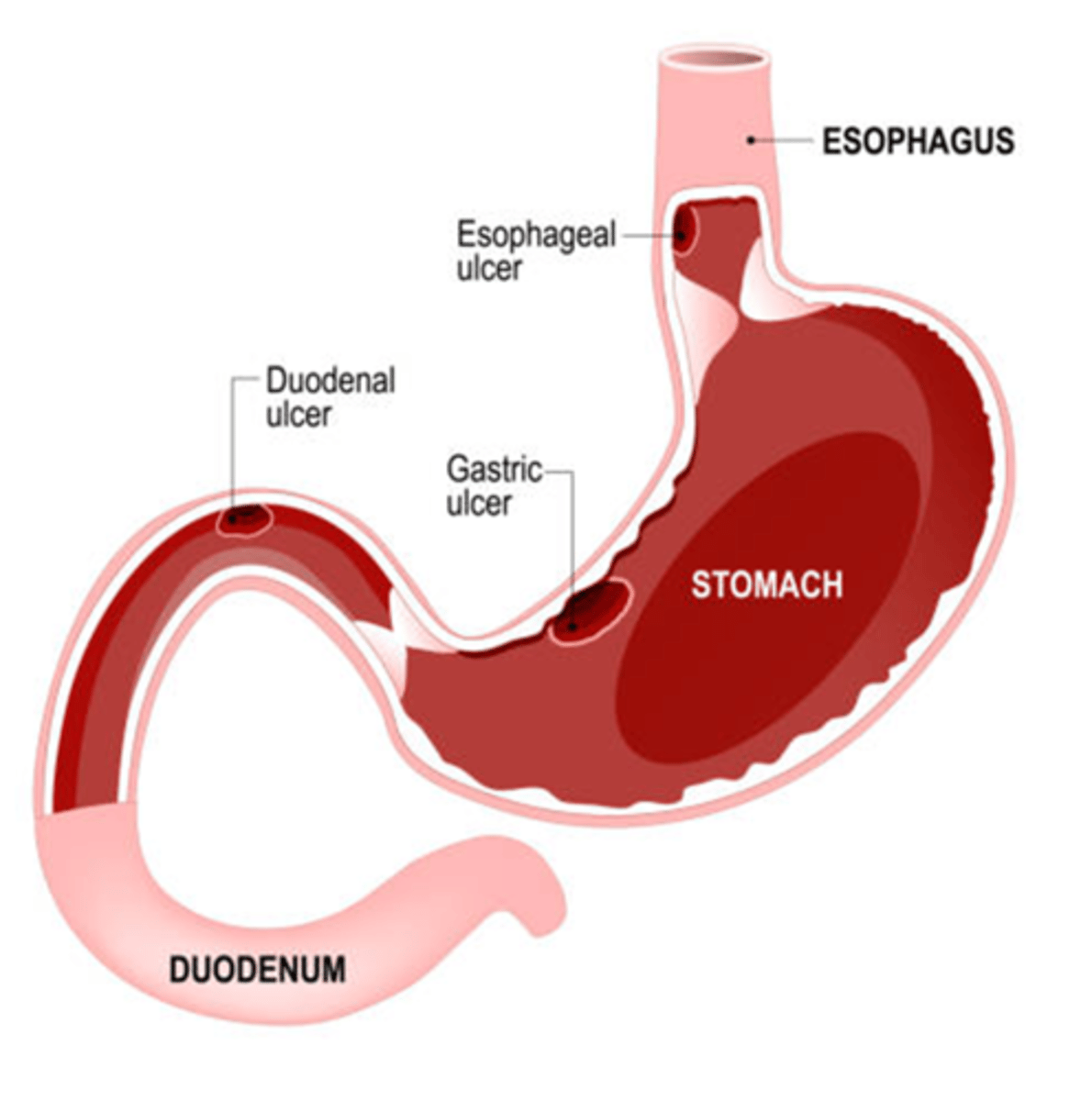
Peptic Ulcer Disease (picture) 2
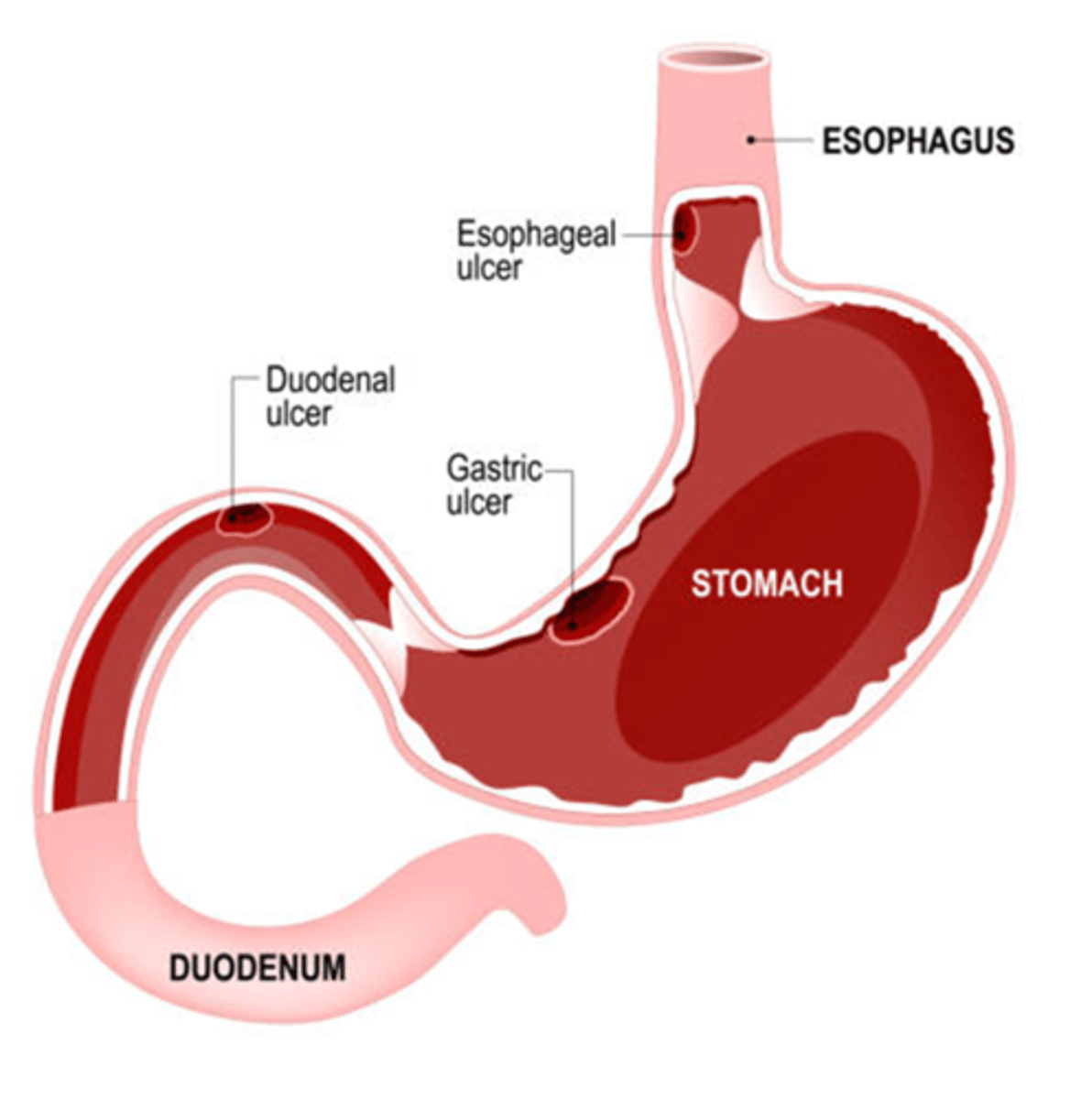
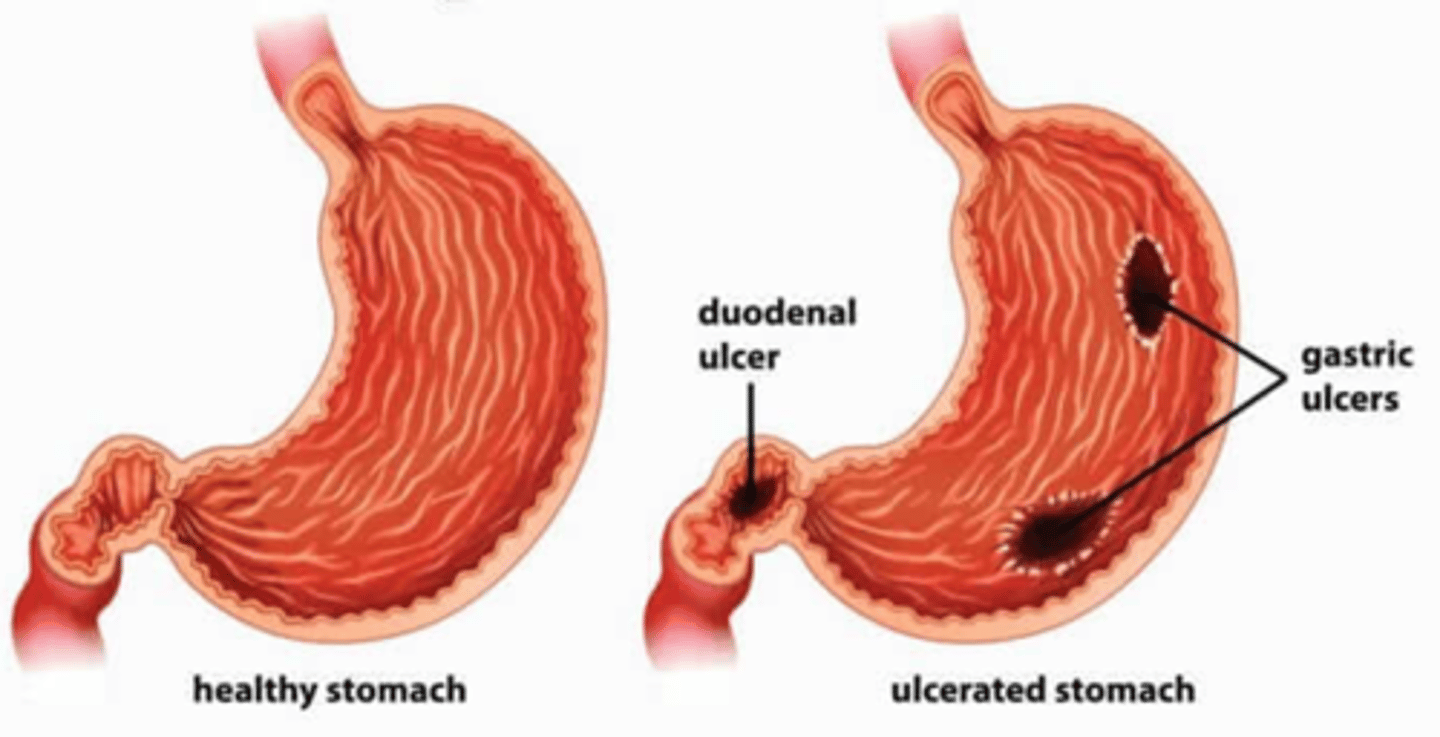
What is peptic ulcer disease?
Ulceration of the mucosal wall of the stomach, pylorus, duodenum, or esophagus.
What may the ulcer in peptic ulcer disease be referred to as?
Gastric, duodenal, or esophageal ulcer.
What causes the mucosal tissue damage in peptic ulcer disease?
The mucosal tissue cannot withstand the digestive action of gastric acid and pepsin, leading to damage and inability to secrete enough protective fluids.
What results from the mucosa's inability to act as a barrier to digestive juices in peptic ulcer disease?
Normal digestive acids and juices corrode the stomach or duodenal lining, causing ulcer formation.
How do esophageal ulcers develop in peptic ulcer disease?
From the backward flow of acid from the stomach up into the esophagus.
What is the preferred method of diagnosing peptic ulcer disease?
Endoscopy.
What are the main risk factors for peptic ulcer disease (PUD)?
NSAIDs; potentially corticosteroids, H. pylori infection, stress and anxiety, smoking and alcohol use, history of gastritis, family history of gastric ulcers, Zollinger-Ellison Syndrome (ZES)
What is Zollinger-Ellison Syndrome (ZES)?
A rare condition involving benign or malignant tumors in the pancreas or duodenum that secrete excessive amounts of gastrin, increasing gastric acidity and causing severe PUD.
What age group is at higher risk for developing peptic ulcer disease?
Adults greater than 65 years old.
Gastric Ulcers (picture)
Where is the pain located in a gastric ulcer?
Sharp pain in or to the left of the mid-epigastric region.
How is the pain described in gastric ulcers?
Burning or gaseous.
When does gastric ulcer pain typically occur?
Immediately up to 1 to 2 hours after a meal.
What effect does food have on gastric ulcer pain?
Food will exacerbate the pain.
Which is more common in gastric ulcers — hematemesis or melena?
Hematemesis is more common than melena.
What additional symptoms may occur with gastric ulcers?
Nausea and vomiting.
How long can gastric ulcer symptoms last?
Days, weeks, or even months.
What provides relief for gastric ulcer pain?
Antacids.
What type of stool may be seen in gastric ulcer patients?
Black, tarry stools.
What type of vomit may be seen in gastric ulcer patients?
Bloody vomit (hematemesis).
Duodenal Ulcers (picture)
Where does pain occur with duodenal ulcers?
Burning pain occurs in the mid-epigastric area or back.
How is duodenal ulcer pain described?
Burning or cramp-like.
What effect does food have on duodenal ulcer pain?
Food buffers the acid and provides relief.
When does duodenal ulcer pain typically occur?
2 to 4 hours after a meal and during the night.
What symptom often awakens clients with duodenal ulcers?
Pain that occurs 2-4 hours after eating or during the night.
Which is more common in duodenal ulcers — melena or hematemesis?
Melena is more common than hematemesis.
What other symptoms may occur with duodenal ulcers?
Nausea and vomiting.
What type of stool is more common in duodenal ulcers?
Black, tarry stools.
PUD Peptic Ulcer Disease (picture)
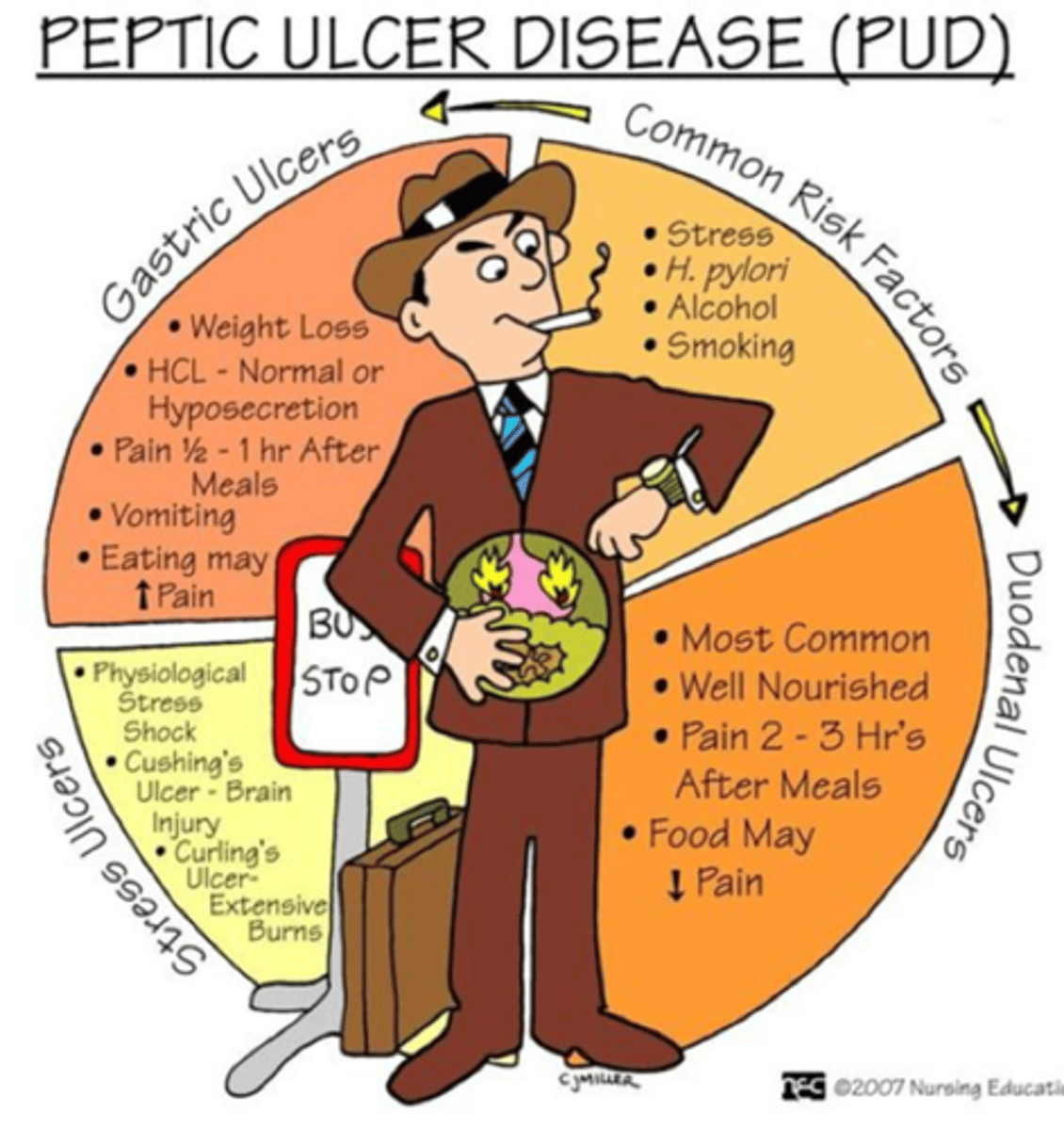
What are the common risk factors for Peptic Ulcer Disease (PUD)?
Stress, H. pylori infection, alcohol use, and smoking.
What are key characteristics of gastric ulcers?
Associated with weight loss, HCl levels are normal or low (hyposecretion), pain occurs ½ to 1 hour after meals, vomiting may occur, eating increases pain.
What are key characteristics of duodenal ulcers?
Most common type of ulcer, patients are usually well-nourished, pain occurs 2 to 3 hours after meals, food may decrease pain.
What are key characteristics of stress ulcers?
Caused by physiological stress or shock, may occur with Cushing's ulcers (brain injury) or Curling's ulcers (extensive burns).
What is another name for a stress ulcer caused by a brain injury?
Cushing's ulcer.
What is another name for a stress ulcer caused by extensive burns?
Curling's ulcer.
What causes stress ulcers?
Physiological stress, shock, extensive burns, and multiple organ dysfunction.
What is given in the hospital to prevent stress ulcers?
Prophylactic medications.
What are examples of prophylactic medications used for stress ulcer prevention?
Omeprazole, pantoprazole, Pepcid, and Phenergan (photonics).
Why are prophylactic medications given to prevent stress ulcers?
To prevent heartburn and complications that can mimic symptoms of a myocardial infarction (MI), such as chest pain and anxiety.
What type of patients are most at risk for stress ulcers?
Critically ill patients experiencing physiological stress, shock, burns, or multiple organ failure.
What percentage of peptic ulcer disease (PUD) patients experience hemorrhage?
27-40%
What type of GI bleed is most common in PUD complications?
Upper GI bleed
What color may emesis appear in a PUD hemorrhage?
Bright red or dark coffee-ground emesis