4. Advanced Simulation: Promoting Adherence to New Medicines
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
3 Phases of Medication Adherence
1. Initiation = Does the patient start the medicine?
2. Implementation = Does the patient take it correctly?
3. Persistence = Does the patient continue for the full duration?
Difference between 3 Phases of Medication Adherence
1. Initiation = Does the patient actually take the medicine?
2. Implementation = Does the patient take the medicine correctly?
3. Persistence = Does the patient continue taking the medication for the full duration?
Primary Non-Adherence
When a medicine is prescribed, but the patient does not obtain or start the medication within an acceptable time.
Why is Treatment Initiation a "Critical Period"?
Patients are forming first impressions about the medicine, including whether they think it is needed, effective, safe and worth continuing.
What might happen after the First Dose of a New Medicine?
Patients may become more aware of bodily sensations, side effects may appear before benefits, and beliefs about the medicine may be reinforced or changed.
Why are Preventative Medicines at high risk of Early Non-Adherence?
The patient may not feel immediate benefit, but may notice side effects early, e.g. statins or antihypertensives.
What Model can be used to Understand the Reasons behind Non-Adherence?
COM-B Model
- Capability
- Opportunity
- Motivation
- Behaviour
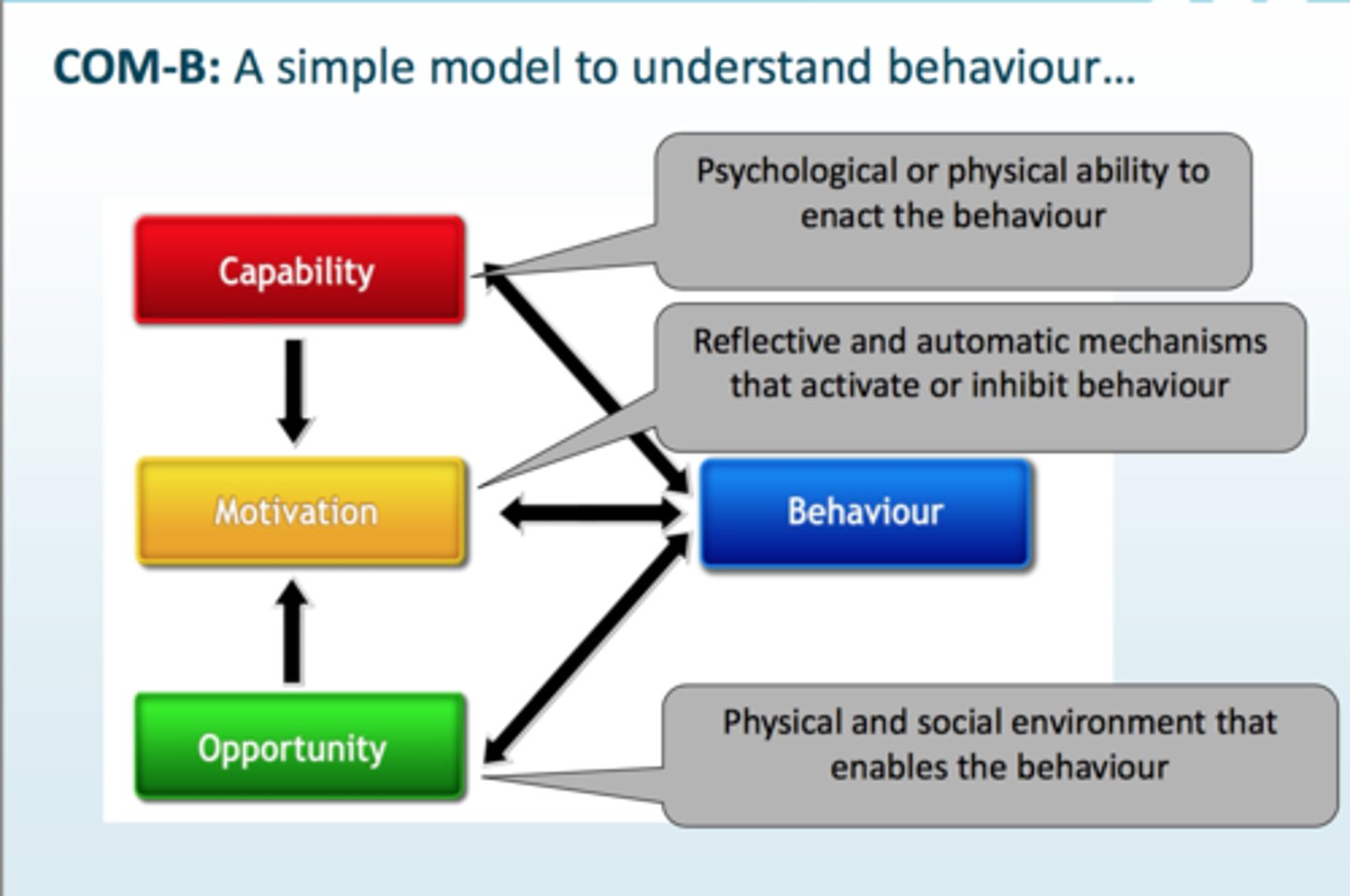
2 Types of Capability in the COM-B Model
Psychological Capability = Does the patient understand and remembers why/how to take the medicine?
Physical Capability = Does the patient have the dexterity to actuate an inhaler? Can the patient physically take/use the medicine, e.g. swallow tablets, open bottles, use inhalers.
2 Types of Opportunity in the COM-B Model
Physical Opportunity = Does the patient have the practical access to get the medicine? Can they access a pharmacy nearby? Can they afford the medication?
E.g., pharmacy access, affordability, storage, delivery.
Social Opportunity = Does the patient have the support of family in taking the medication? Is there a stigma attached to taking the medication? What is the patient's relationship with their prescriber like?
E.g., support, stigma, cultural beliefs, family/friend influence, prescriber relationship.
2 Types of Motivation in the COM-B Model
Reflective Motivation = Patient understands why they need to take their medication, e.g. “I need this statin.”
Automatic Motivation = Patient has incorporated the medication into their routine, e.g., they take it after dinner without thinking twice.
Examples of Motivational Barriers to Starting a Medicine
- Doubts that the medicine is needed
- Concerns about side effects
- Belief that lifestyle changes are enough
- Doubts that the medicine will work
- Belief the condition is not serious
Examples of Opportunity Barriers to starting a Medicine
- Distance from pharmacy
- Cost/co-payments
- Stigma
- Lack of social support
- Poor shared decision-making with prescriber
Examples of Capability Barriers to starting a Medicine
- Forgetting information
- Not understanding instructions
- Difficulty travelling to the pharmacy
- Difficulty planning medicine-taking into daily life
Habit
A habit is a learned cue-response association where a cue automatically triggers a behaviour.
How do Habits form?
Through repeated performance of a behaviour in the same context, linked to a regular cue.
What makes a Good Cue for taking Medicine?
A good cue is...
- Consistently present
- Easy to notice
- Linked to an existing routine
- Occurs at the right time for the dose
"Piggybacking" in Adherence Support
Linking a new medicine-taking habit to an existing routine, e.g. brushing teeth, breakfast, bedtime or morning coffee.
Key Purpose of "Action Planning"
To help the patient make a specific plan for when, where and how they will take their medicine, so it becomes part of a routine.
"Action Planning"
A behaviour change technique (BCT) where the patient makes a specific plan for when, where and how they will take their medicine.
When should you use Action Planning?
When the patient thinks they may struggle to get into a routine with a new medicine.
Ideal Format for an Action Plan
An if-then plan, e.g. “If I have brushed my teeth at night, then I will take my tablet.”
What should you ask when helping a Patient create an Action Plan?
Ask what regularly happens in their day that they could link the medicine to, rather than immediately giving your own suggestions.
What should you do after the Patient creates an Action Plan?
Ask them to evaluate whether it will work in real life, then encourage them to record it, e.g. write it down or put it in their phone.
What if a Patient cannot think of when to take their Medicine?
Ask them to talk through their typical day around the time the dose is due, so they can identify their own possible cue.
What if a Patient takes Multiple Daily Doses?
Create a separate action plan for each dose, e.g. morning, lunchtime and evening.
What if a patient's routine varies between workdays and weekends?
Create different action plans for different routines, e.g. one for workdays and one for weekends.
"Righting Reflex"
The urge to immediately fix the patient's problem by giving advice or solutions before fully understanding their situation.
Why can the righting reflex reduce adherence support?
It can make patients feel misunderstood, disempowered or resistant because the solution has been imposed on them.
How can you Avoid the "Righting Reflex"?
Pause, ask open questions, use empathy, reflect what the patient says, and help the patient find their own solution.
Shared Decision-Making
Patients are more likely to start and continue treatment when they feel involved, informed and listened to.
2 Types of "Expert" in Shared Decision-Making
The clinician is the expert in clinical evidence. The patient is the expert in their own life, values, priorities and preferences.
DECIDE Model
- Define the decision
- Explain the situation
- Consider the options
- Invite views
- Decide together
- Evaluate the decision
When is the DECIDE Model used?
The DECIDE model helps structure shared decision-making so patients understand their options, express their values, and make an informed treatment choice, which can improve autonomy, trust and adherence.
It stops the consultation from becoming:
“I’m the clinician, this is the medicine, take it.”
Instead, it becomes:
“Here are the options, here are the benefits and risks, what matters to you, and let’s decide together.”
That matters because patients are more likely to start and continue a medicine if they feel involved, understand why it is needed, and feel the decision fits their life and priorities.
What does “Define the Decision” mean in DECIDE?
Make it clear that a decision is being made together, e.g.“Today we’re deciding together whether starting a statin is right for you.”
What does “Explain the Situation” mean in DECIDE?
Find out what the patient already knows, their concerns, priorities and questions before presenting options.
What should you do if a Patient is stuck at the "Decide Together" stage?
Ask permission before suggesting a way forward, e.g."Would it help if I suggested an option and explained why?"
BRAN
Benefits
Risks
Alternatives
Nothing
How should Statin S/E risk be explained in the BRAN Model?
Use absolute numbers, e.g."About 2 in 100 people may get mild muscle pain. Severe muscle damage is very rare, around 3 in 10,000."
How should Risk and Benefit statistics be Communicated?
Use absolute numbers and consistent denominators, e.g. “12 in 100 people” rather than switching between percentages and fractions.
Why Should you Explain how a Medicine works?
A concrete explanation helps patients understand why the medicine is needed and may improve adherence if they choose to take it.
What does “Invite Views” mean in DECIDE?
Ask what matters to the patient after discussing options, e.g.“What feels most important to you when thinking about these options?”
What does “Decide Together” mean in DECIDE?
Use the patient's priorities and the clinical options to agree on the best way forward together.
What does “Evaluate the Decision” mean in DECIDE?
Check the patient is happy with the decision, understands what it means, and knows they can think about it or revisit it later.
Key Exam Phrase for Adherence Support
Use shared decision-making to support motivation and action planning to help patients build a medicine-taking routine.
Difference between Primary Non-Adherence and Poor Implementation
Primary Non-Adherence = Patient does not start/obtain the medicine.
Poor Implementation = The 2nd phase of medication adherence where the patient starts taking the medication but does not take it correctly, e.g. missed doses, wrong timing, wrong method.
Why is early Non-Adherence important?
Early patterns can continue long term.
- If a patient does not start well, they may be more likely to remain non-adherent later.
Examples of Early Non-Adherence Rates
Approximate primary non-adherence rates...
- Statins = 25%
- Osteoporosis Medicines = 25%
- Antidepressants = 12%
What Motivational Barriers can stop someone starting a Medicine?
- Doubts about need
- Doubts about effectiveness
- Fear of side effects
- Belief the condition is not serious
- Preference for lifestyle change only.
What is the difference between DECIDE and BRAN?
DECIDE structures the whole shared decision-making conversation.
BRAN sits inside "Consider the options" and explains Benefits, Risks, Alternatives and Nothing.
Why use Shared Decision-Making for New Medicines?
It supports autonomy, builds trust, addresses concerns, and makes the patient more likely to start and continue the medicine.
A 56-year-old man is prescribed atorvastatin after a QRISK3 assessment. Two weeks later, the pharmacy record shows the prescription was issued but never collected. When contacted, he says, “I’m not against tablets, but I thought I’d try diet first and see if my cholesterol improves.”
Which type of adherence problem is this?
A. Poor implementation due to incorrect dose timing
B. Non-persistence after adverse effects
C. Primary non-adherence during initiation*
D. Intentional dose experimentation after collection
E. Automatic motivation failure after habit formation
*The patient was prescribed atorvastatin but never collected or started it. That is primary non-adherence, which happens in the initiation phase.
----------------------------------------------------------
A = Poor implementation means the patient has started but takes it incorrectly.
B = Non-persistence means stopping after starting.
D = Dose experimentation would require the patient to collect and partially take it.
E = Automatic motivation/habit failure happens after a routine has begun forming.
A patient collects a new antihypertensive but takes it only on days when they “feel their blood pressure is high.” They have not experienced side effects and understand the label directions.
Which phase of adherence is mainly affected?
A. Initiation
B. Implementation*
C. Persistence
D. Dispensing
E. Prescriber-related adherence
*The patient collected and started the antihypertensive but is taking it incorrectly - only when they “feel” BP is high. That is poor implementation.
--------------------------------------------------------
A = Initiation has already happened.
C = Persistence is about continuing for the intended duration, not incorrect timing.
D = Not a recognised adherence phase.
E = Vague and does not describe the phase affected.
A patient is prescribed an antidepressant but says, "I'm worried it will change my personality. I don't really think I need it because I can manage this myself."
Which COM-B component is the most relevant barrier?
A. Physical capability
B. Psychological capability
C. Physical opportunity
D. Reflective motivation*
E. Automatic motivation
*The patient is making a conscious judgement: "I don’t think I need it" and "I’m worried it will change my personality." These are beliefs, concerns and doubts, so this is reflective motivation.
-------------------------------------------------------
A = They are not physically unable to take it.
B = They do not lack understanding of instructions; they have concerns and beliefs.
C = Access or cost is not the barrier.
E = Automatic motivation is about habit/emotion-driven routines, not conscious reasoning.
A patient says they want to take their new inhaler but cannot press the canister and breathe in at the same time because of poor hand strength and coordination.
Which COM-B component is most directly implicated?
A. Physical capability*
B. Psychological capability
C. Reflective motivation
D. Social opportunity
E. Automatic motivation
*The patient cannot physically coordinate pressing the inhaler and breathing in. This is a physical ability problem.
----------------------------------------------------------
B = They may understand the instructions but cannot physically perform them.
C = This is not about beliefs.
D = Stigma/social support is not the issue.
E = This is not about habit formation.
A patient wants to start a new medicine but says the nearest pharmacy is difficult to reach because they have limited mobility and no transport.
Which COM-B component is most directly implicated?
A. Psychological capability
B. Physical opportunity
C. Social opportunity
D. Reflective motivation
E. Automatic motivation
*The patient wants to start the medicine but cannot easily access the pharmacy due to transport and mobility barriers. That is a physical opportunity issue because the environment is preventing medicine access.
-------------------------------------------------------
A = The problem is not memory or understanding.
C = The issue is not stigma or social support.
D = The patient is motivated.
E = The medicine is not yet part of a habit.
A patient is prescribed a new medicine for osteoporosis. They say, “I know I should take it, but I keep forgetting because my mornings are chaotic.” They ask for advice about building it into their routine.
Which intervention is MOST suitable?
A. Repeat the dosing instructions several times
B. Use action planning to link the medicine to a consistent cue in their daily routine*
C. Advise them to take it whenever they remember
D. Tell them non-adherence will increase fracture risk
E. Ask their GP to switch to a different medicine immediately
*The patient wants to take the medicine but struggles with routine. Action planning helps them link medicine-taking to a regular cue, which supports habit formation. Action planning is helping the patient plan when and where to take the medicine, often using an existing routine or cue.
--------------------------------------------------------
A = Repeating instructions does not create a routine.
C = Unsafe because “whenever you remember” is vague.
D = May increase fear or guilt but does not solve the routine problem.
E = Unnecessary unless there is a medicine-specific problem.
You are using action planning with a patient who takes a new medicine twice daily. They work shifts, so their wake-up and meal times vary between workdays and non-workdays.
What is the most appropriate approach?
A. Tell them to take both doses with breakfast and dinner
B. Create one fixed clock-time plan for every day
C. Create separate action plans for different routine patterns, such as workdays and non-workdays*
D. Avoid action planning because it only works in patients with fixed routines
E. Ask them to rely on the label instructions instead
*If routines vary, you may need different action plans, for example one for workdays and one for non-workdays.
--------------------------------------------------------
A = Too prescriptive and may not fit shift work.
B = Unrealistic if wake-up and meal times change.
D = Action planning can still work with more than one plan.
E = Insufficient because label instructions do not solve the routine barrier.
A patient cannot think of any routine to link their medicine to. The pharmacist immediately says, “Why don’t you just take it after brushing your teeth?”
Why is this NOT the best action-planning technique?
A. Toothbrushing is never an appropriate medication cue
B. The pharmacist has used the righting reflex rather than helping the patient generate their own plan*
C. Action planning should only use clock times
D. Action planning should not involve existing routines
E. The patient should not be involved in generating the plan
*The pharmacist jumps in with their own solution instead of helping the patient generate one. That is the righting reflex. Avoid jumping in with advice and instead use open questions/empathy so the patient creates their own plan.
---------------------------------------------------------
A = Toothbrushing can be a good cue.
C = Action planning can use routines, not just clock times.
D = Existing routines are ideal cues.
E = Patient involvement is central to action planning.
Which of the following is the best example of an action plan?
A. “I will try harder to remember my tablets.”
B. “I will take my medicine whenever I get time.”
C. “If I sit down for the 6 pm news in the living room, then I will take my tablet from the side table.”*
D. “I understand the medicine is important.”
E. “I will take the medicine because my pharmacist told me to.”
*It is specific: if a regular cue happens, then the patient takes the medicine, with a location included.
------------------------------------------------------
A = Too vague.
B = Too vague and unreliable.
D = Knowledge, not an action plan.
E = Motivation/compliance language, not a practical routine.
A patient with newly diagnosed hypertension says they are unsure about starting treatment. The pharmacist says, “Today we’re deciding together whether starting a blood pressure medicine is the right option for you.”
Which stage of the DECIDE model is this?
A. Define the decision*
B. Explain the situation
C. Consider the options
D. Invite views
E. Evaluate the decision
*The pharmacist frames the consultation as a decision to be made together: whether to start a BP medicine. That is Define the decision.
-----------------------------------------------------
B = Would involve exploring what the patient already knows and their concerns.
C = Would involve discussing options and BRAN.
D = Would involve asking the patient’s views after options.
E = Would involve checking the final decision and understanding.
During a statin consultation, the pharmacist asks, “Can you tell me what you already know about statins, and whether you have any worries or questions about them?”
Which stage of DECIDE does this best represent?
A. Define the decision
B. Explain the situation*
C. Consider the options
D. Decide together
E. Evaluate the decision
*The pharmacist is asking what the patient already knows and whether they have concerns. That fits Explain the situation in DECIDE.
-------------------------------------------------------
A = Only framing that there is a decision.
C = Discussing benefits/risks/options.
D = Agreeing the option together.
E = Checking whether the patient is happy with the final decision.
A pharmacist explains statin treatment to a patient with a QRISK3 score of 20%.
Which explanation best follows the communication principles of BRAN?
A. “A statin reduces your relative risk by about a third, so you should take it.”
B. “Without a statin, 20 in 100 people like you may have a heart attack or stroke over 10 years; with a statin, about 13 in 100 may.”*
C. “Your risk falls from 20 in 100 to 1 in 8, so the numbers are much better.”
D. “Most people benefit from statins, but some people get side effects.”
E. “Statins prevent heart attacks, but the exact numbers are too complicated to explain.”
*It uses absolute risk and keeps the denominator consistent: 20 in 100 without statin, 13 in 100 with statin. Your slides specifically say to use frequencies, keep denominators consistent, and use absolute rather than relative risk.
----------------------------------------------------------
A = Uses relative risk and sounds directive.
C = Switches denominator style, making it harder to compare.
D = Too vague.
E = Avoids giving useful risk information.
A patient with raised cardiovascular risk says, “I don’t want to take a statin. I’d rather make lifestyle changes.” The pharmacist has not yet discussed the likely benefits, risks, alternatives or what happens if no action is taken.
Which is the best next step?
A. Respect the refusal and end the consultation immediately
B. Explain that lifestyle changes are ineffective compared with medicines
C. Use BRAN to discuss benefits, risks, alternatives and doing nothing before inviting the patient’s views*
D. Prescribe the statin anyway because QRISK is above 10%
E. Tell the patient they can only choose lifestyle changes after trying a statin
*The patient has expressed a preference, but the pharmacist still needs to support an informed decision by discussing Benefits, Risks, Alternatives and Nothing.
--------------------------------------------------------
A = Ends the consultation before informed decision-making.
B = Dismisses the patient’s preference.
D = Undermines autonomy by prescribing anyway.
E = Falsely suggests lifestyle change is only allowed after a statin trial.
A patient is concerned about muscle pain from statins.
Which response best reflects shared decision-making?
A. “That side effect is rare, so you don’t need to worry.”
B. “Most patients take statins, so you should too.”
C. “Let’s discuss how likely that is, how serious it could be, and what we could do if it happened.”*
D. “We should avoid discussing side effects because it may reduce adherence.”
E. “Lifestyle change is safer, so we should not consider tablets.”
*This validates the concern and gives balanced information. It supports shared decision-making and avoids dismissing the patient.
----------------------------------------------------------
A = Dismisses the concern.
B = Applies pressure rather than shared decision-making.
D = Avoids side-effect discussions and can reduce trust.
E = Jumps to one option without exploring risks/benefits.
A pharmacist and patient decide together to start atorvastatin. The pharmacist says, “So you’ve decided to try atorvastatin because reducing your heart attack and stroke risk matters to you, but you want to review side effects in 8 weeks. Are you clear what this means, and are you happy with that plan?”
Which DECIDE stage is this?
A. Define the decision
B. Explain the situation
C. Consider the options
D. Invite views
E. Evaluate the decision*
*The pharmacist summarises the decision, checks the patient understands it, and confirms they are happy with the plan. That is Evaluate the decision.
--------------------------------------------------------
A = Happens at the start.
B = Explores prior knowledge and concerns.
C = Discusses options.
D = Invites the patient’s views before the final decision.