High Acuity Final Exam
1/109
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
110 Terms
explain the practice of critical care nursing
Care of pts with life threatening conditions that require complex assessment, advanced technology, and rapid decision making. It is holistic, interdisciplinary collaboration, patient-and-family centered care integrating physiologic, psychosocial, ethical, and cultural needs in a high acuity environment.
management of pain
subjective and objective pain score, can use BPS (behavioral pain scale) for nonverbal patients
management of agitation
could be hyperactive psychomotor functions such as tachycardia, hypertension, movement, sedate to limit these functions (low dose)
management of delirium
acutely changing mental status, inattention. Can be hyperactive, hypoactive, or mixed. For preventing delirium ABCDE bundle, medications
ABCDE delirium bundle
awakening, breathing, coordination, choice of sedation, delirium monitoring, early ambulation, and excerise
1st line treatment for delirium
haloperidol
informed consent
patients include receiving adequate information, understanding the risks, benefits and alternatives, making a voluntary decision and having decision making capacity
intubation informed consent
if patient is awake and alert - provider explains need for ventilator, risks (aspiration, infection), alternatives (BiPAP), and outcomes, nurse verifies understanding and witness consent. If the patient is unconscious or unstable - implied consent applies (life saving emergency), nurse documents condition and urgency
brain injury with surgery needed informed consent
assess if patient has capacity, if not identify healthcare proxy / POA. Provide information to surrogate for consent (nurse advocates if family is confused or pressured.
advanced directives
living will, durable power of attorney for healthcare (DPOA), DNR/DNI orders, POLST/MOLST.
indications for calling a rapid response
Respiratory: rate < 8 or > 28, oxygen saturation < 90% despite oxygen, new onset respiratory illness, increased work of breathing, cyanosis.
Cardiovascular: systolic BP < 90 mmHg or a significant drop from baseline, HR < 40 or > 130, new chest pain, s/s shock (cool, clammy, altered mental status)
Neurologic: acute change in mental status, new confusion, agitation, or lethargy, unresponsiveness, seizure activity.
Other triggers: staff or family concerned about patient condition, significant change in urine output, uncontrolled bleeding, or clinical deterioration that does not meet code criteria but is concerning.
key functions rapid response team
prevent cardiac arrest, ICU transfer, or death by intervening early. This includes rapid bedside assessment of the patient, identifying causes of deterioration, stabilizing patients, collaborating with the primary care team, determining whether a patient needs ICU transfer, providing support and education to bedside nurses, preventing future deterioration through early intervention before full code is needed.
formula for cardiac output
heart rate x stroke volume
assessment and preparation for diagnostic purposes in cardiology
Review patient history, allergies (especially to contrast), and current medications (e.g., anticoagulants).Provide clear patient education to reduce anxiety and improve cooperation.
safety monitoring for diagnostic purposes in cardiology
Continuously monitor vital signs during stress tests, sedation, or invasive procedures. Observe allergic reactions, especially with contrast agents. Manage patient discomfort, pain, or anxiety proactively.
patient education diagnostic purposes in cardiology
Explain purpose, process, and expected sensations for each test. Instruct about activity restrictions, fasting requirements, and device care. Clarify when to seek urgent care post-procedure (e.g., severe chest pain, bleeding).
documentation and communication diagnostic purposes in cardiology
Record baseline and post-test vitals, symptoms, and any abnormalities. Communicate findings promptly to the care team to support diagnosis and treatment planning.
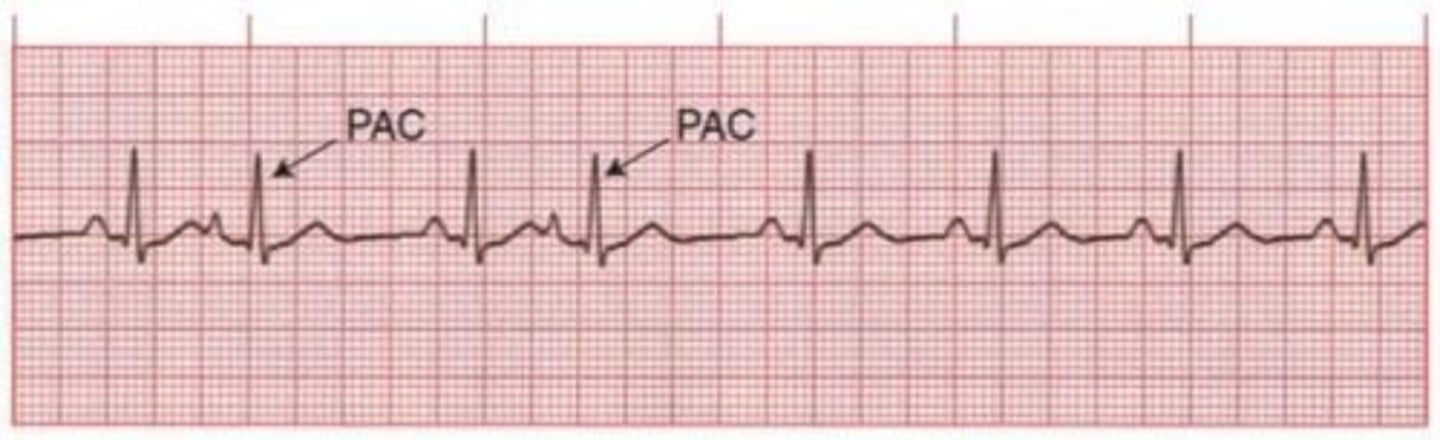
Premature Atrial Contractions (PACs)
usually common and benign
triggers: stress, caffeine, alcohol, and tobacco
can signal atrial irritability which may precede to a-fib, flutter, or SVT
s/s skipped beat
tx: usually none but continue to monitor and treat underlying cause
not usually an emergency unless frequent or symptomatic
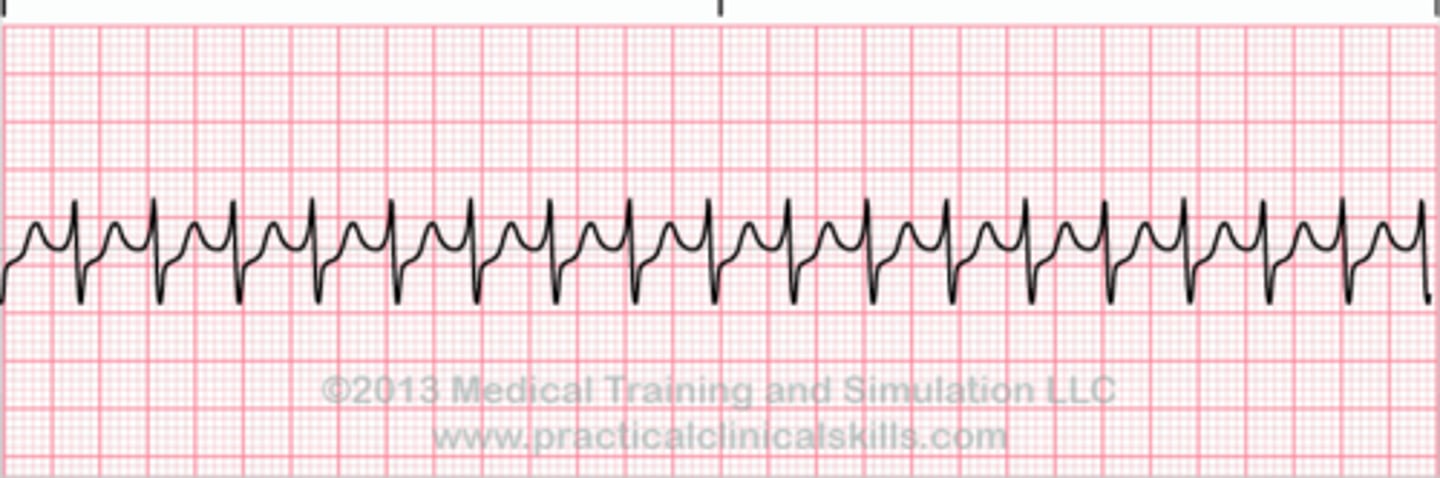
Paroxysmal Supraventricular Tachycardia (PSVT) same as (SVT)
sudden fast regular rhythm
causes: stress, hypoxia, and metabolic disorders
often in healthy hearts
s/s palpitations, dizziness, decreased CO if sustained
tx: first line vagal maneuvers
second: beta blockers, calcium channel blockers, or adenosine
third: cardioversion if unstable
Atrial Flutter
sawtooth flutter waves, more regular pattern, seen with CAD and rheumatic disease
key problems: loss of atrial kick, decreased CO, and thromboembolism risk
tx: rate control or rhythm conversion by AV node slowing meds, synchronized cardioversion (prompt treatment), and anticoagulation is greater than 72 hours.
For synchronized cardioversion, pt should be NPO before procedure and receive sedation.
If needed long term management, radio frequency ablation, pacing, and implantable devices.
Flutter = regular rhythm but still high stroke risk

a-fib
Irregularly irregular
Common with HF, CAD, valve disease and other underlying heart diseases.
Major concern: rate of ventricular response meaning if the ventricular rate is too fast, end diastolic filling time is decreased and CO is compromised. If too slow, CO also decreased.
Major risks: loss of atrial kick → ↓CO, stroke, and emboli
Tx: priorities are rate control, anticoagulation, and cardioversion if unstable or symptomatic.
If needed long term management, ablation, pacing, and implantable devices - just like flutter.
AF = anticoagulant NEEDED

premature ventricular contractions
Most common ectopic beats can occur with or without heart disease in any age group.
Causes: ischemia, hypokalemia, catecholamines.
Concern: frequent PVCs → ventricular tachycardia and VF.
Tx: treat cause and monitor.
PVCs + hypokalemia = replace potassium

ventricular tachycardia
Most often occurs after MI
Rare in normal hearts
Serious as it is a precursor to v-fib
If the rate is fast or sustained, hemodynamic compromise.
s/s: hypotension, ischemic chest pain, pulmonary edema, ↓ LOC/unconsciousness.
Tx: stable - amiodarone, unstable - cardioversion, pulselessness - defib + cpr, long term - ICD.
VT = wide QRS, regular rhythm, always assess pulse and stability FIRST

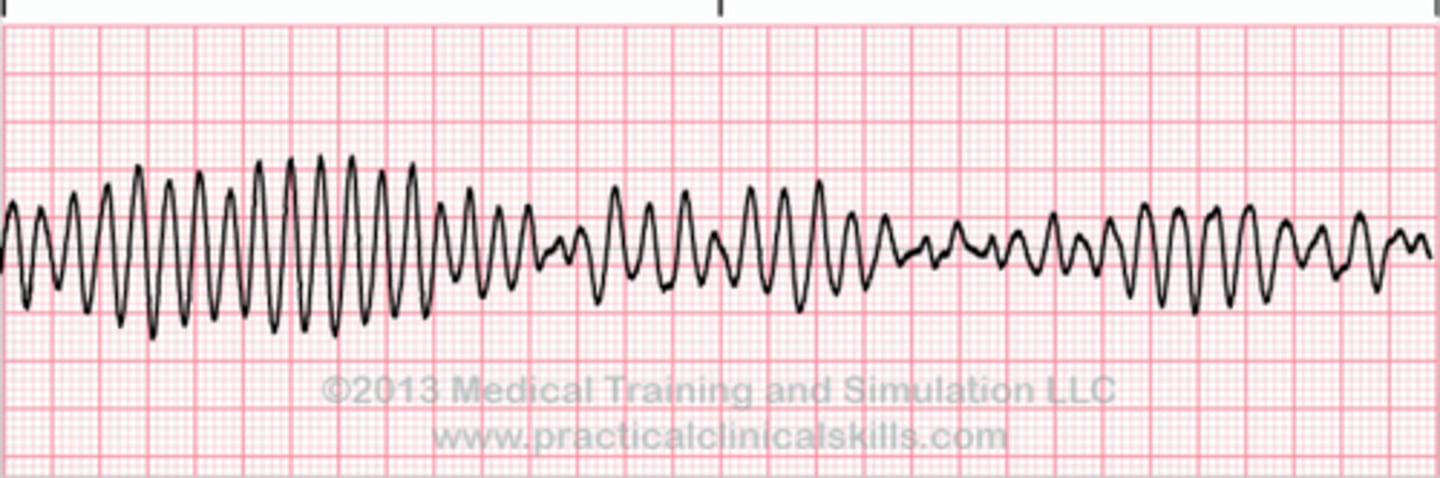
torsades de pointes
Polymorphic VT associated with prolonged QT interval, can be self-terminating or progress to v-fib
causes: electrolyte imbalance (hypokalemia, hypomagnesia, hypocalcemia), QT prolonging drugs (especially classes IA antiarrhythmics), severe brady, and congenital long QT syndrome.
Tx: first line - MAGNESIUM SULFATE
Magnesium is almost always the answer
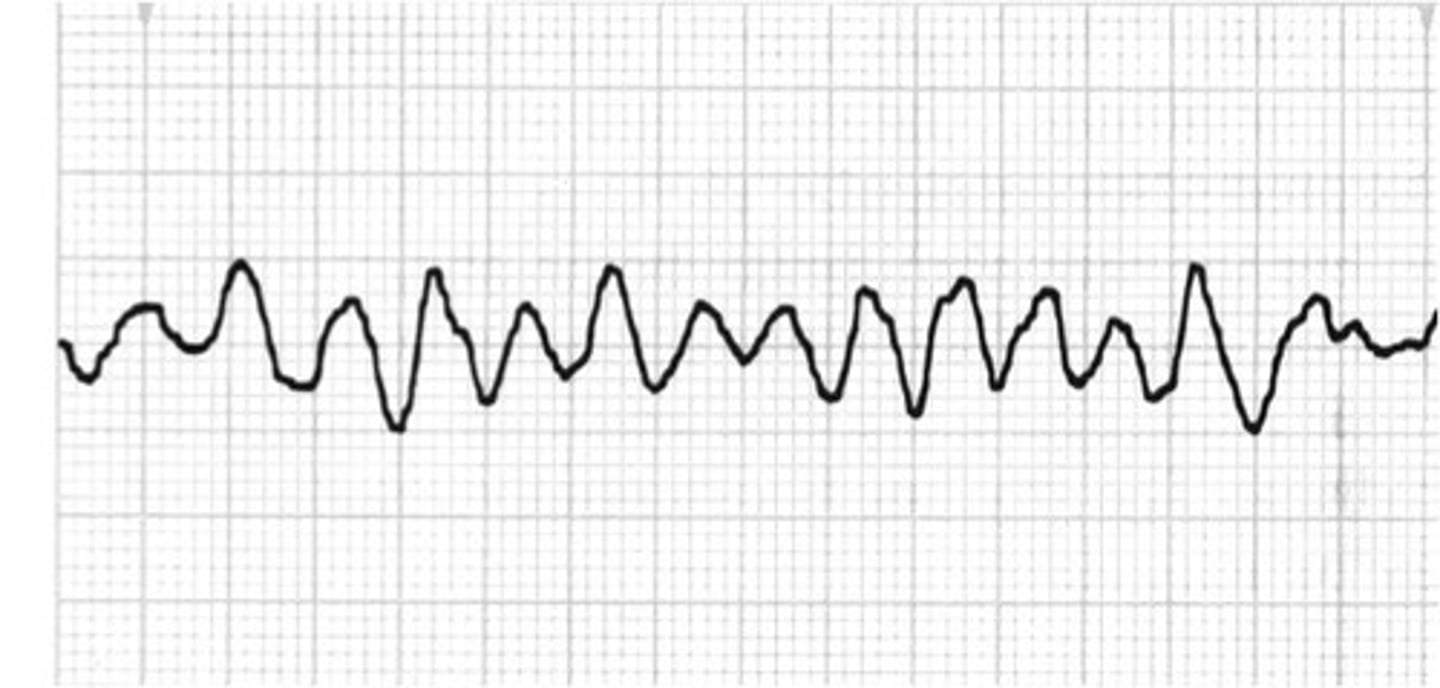
ventricular fibrillation
Chaotic ventricular rhythm → no CO, no pulse
Most common cause of sudden cardiac death
Fatal without immediate intervention
Causes: acute MI or ischemia, prolonged QT interval, electrocution, ventricular catheter manipulation, end stage circulatory failure.
s/s: immediate loss of consciousness, pulseless, and apneic.
Tx: immediate defib (treatment of choice), CPR + ACLS medications, long term ICD placement.
VF = defib immediately
No cardioversion because no organized rhythm.
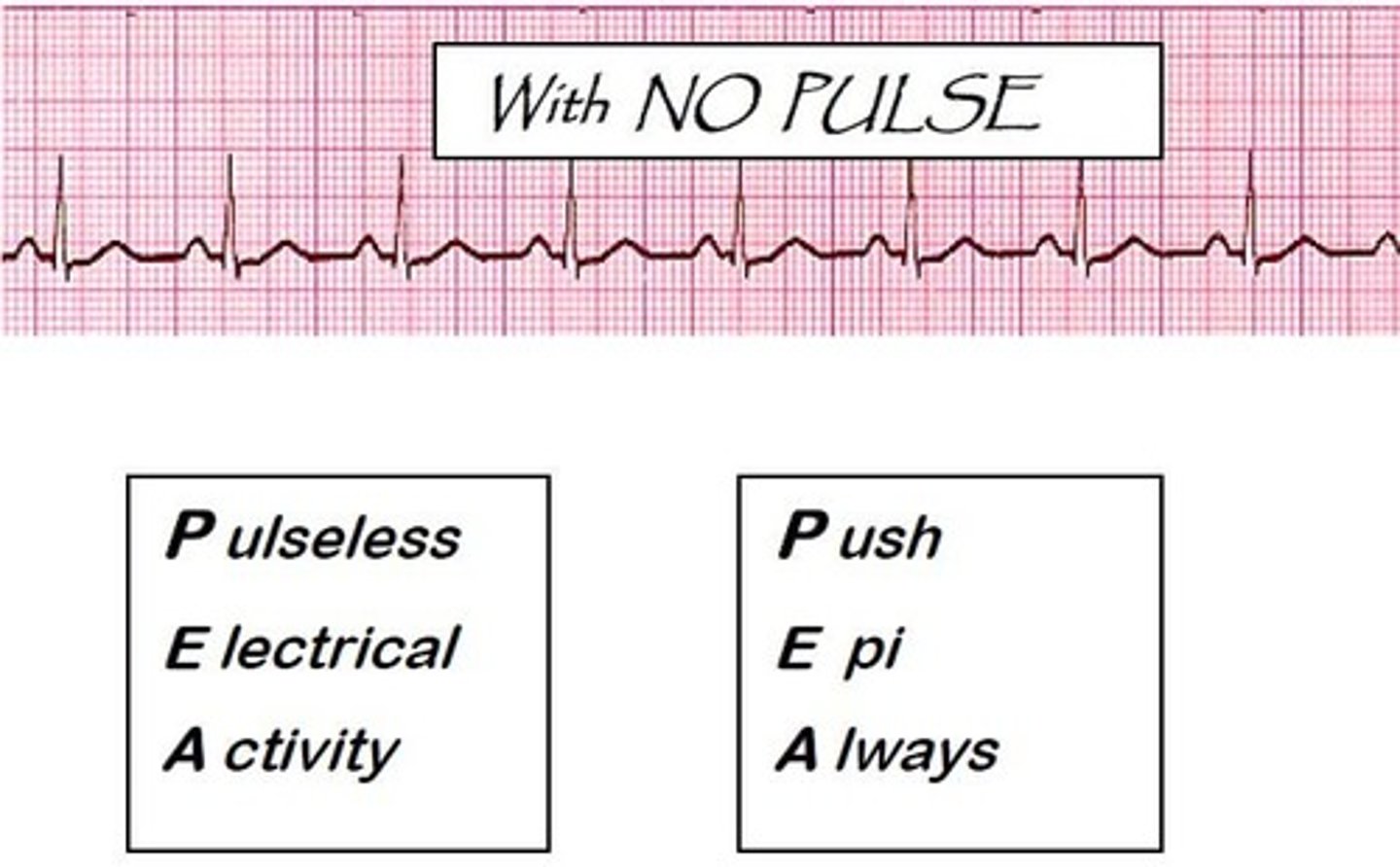
pulseless electrical activity
Minimal electrical activity with NO PULSE, often bradycardic.
Commonly the initial arrest rhythm.
Assess the H's and T's Hypovolemia, Hypoxia, hydrogen ions (acidosis), hyper/hypokalemia, hypoglycemia, and hypothermia. T's- Toxins, Tampanode, Tension pneumothorax, Thrombosis, and Trauma.
Initiate CPR, epinephrine, ACLS algorithm.
DO NOT SHOCK
system components required to monitor hemodynamic pressure
Indwelling cath is attached by the pressure tubing to a transducer which is connected to the amplifier/monitor that visually shows waveforms and systolic and diastolic mean pressure values.
The system is composed of a flush solution under a pressure infuser, a continuous flush device and series of stopcocks; the pressured bag solution infusion is 300 mmHg with continuous flow of 3 to 5L/hr to prevent backflow of blood and to maintain system patency
the stopcock closest to insertion site is used for blood draws and the stopcock located nearest to the transducer is used for zeroing
Right ventricular pressure
Systolic 20-30 mmHg
Diastolic 0-5 mmHg
PA systolic pressure
15-30 mmHg
PA diastolic pressure
8-12
central venous pressure
2-6
complications with a PA cath
pneumothorax, infection, vent. dysrhythmias, PA rupture, perforation, and air embolism.
complications with a central venous cath
infection, thrombosis, air embolus, (CLABSI)
complications with an indwelling arterial cath
infection, accidental blood loss, impaired circulation to extremity. Check Allen's test
causes of cardiopulmonary arrest
V fib, v tach with pulselessness, shock, trauma, asystole, PEA, acute MI,HF, coronary vasospasm, cardiac tamponade, respiratory failure, airway obstruction, PE, pulmonary artery cath, cardiac cath, surgery, hypoxia, electrolyte imbalances, severe acidosis, and drug toxicity.
steps of CPR and role of each member of the resusciation team
COMPRESSION, AIRWAY, BREATHING
Check for responsiveness and pulse, call for help/activate code, high quality chest compressions, airway management, breathing (bag-mask or advanced airway), defibrillation when indicated, medication administration, identify and treat reversible causes (Hs and Ts)
Roles: team leader, compressors, airway manager, medication nurse, recorder, defibrillator operator.
indications, procedures, and nursing management for electrical cardioversion
Indications: monomorphic v tach with pulse, a flutter, a fibrillation
Procedure: give adenosine, synchronize, pain meds and or sedatives
Nursing management: must have IV, VS, pulse ox, continuous monitoring of ABCs, monitor heart rhythms, and document the procedure.
pre op CABG or valve surgery
patient education, baseline labs and diagnostics (CBC, BMP, coag.), skin preparation, anxiety reduction
post op CABG or valve surgery
temporary pacing, mediastinal chest tubes, pleural chest tubes, cardiac and hemodynamic monitoring, manage hypothermia by core temp monitoring and rewarming, prevent shivering, pain control.
nursing interventions preventing complications after cardiac surgery
under anesthesia so not awake, expected GCS = 3 when come back, must have vent in place, central line, PIV, incision on chest glued shut, bone will be wired shut, 5 lead EKG, need monitor for BP/HR/O2/RR/CVP/PAP/radial art line q15mins, may have pacer wires (2) make sure dressing in place and look to see what's under dressing when they come back, if pacer wires cap do not let them touch or put them on pacer box, chest tubes (at least 2; mediastinal and plural) output q15mins (1st hour 300, 200 in 2nd), for chest tube backs up can cause tamponade, DO NOT FLUSH TUBES but can strip and milk tubes, foley for urine output and temp, SCDs, warm them up, this surgery hurts really bad cannot get rid of pain but will try best to control pain, labs and get glucose, meds (IV fluid, anticoag, packed RBC (check H&H and platelets), pain meds, nitroprusside, levophed, orders to replace potassium, if need insulin regular IV (blood sugar q15 if on insulin), stool softeners after surgery.
Early ambulation, do not lift or put arms above head, strict I&O monitoring, infection prevention, DVT prophylaxis.
Respiratory acidosis
PaCO2 greater than 45, and a pH less than 7.35 - inadequate elimination of carbon dioxide by the lungs and may be a result of inefficient pulmonary function or excessive production of carbon dioxide.
respiratory acidosis causes
COPD, opioids/sedation, respiratory failure, obstruction
respiratory acidosis s/s
hypoventilation, hypoxia, rapid shallow respirations, decreased BP, dyspnea, headache, hyperkalemia, drowsiness, dizziness, muscle weakness, hypereflexia, dysrhythmias
respiratory alkalosis
PaCO2 less than 35 and pH greater than 7.45 - excessive elimination of carbon dioxide from the serum.
respiratory alkalosis causes
anxiety/panic attacks, pain, fever, early hypoxia, mechanical over ventilation.
respiratory alkalosis s/s
seizures, deep rapid breathing, hyperventilation, tachycardia, low or normal bp, hypokalemia, lethargy and confusion, N/V, light headedness
metabolic alkalosis
bicarbonate level greater than 29 and a pH greater than 7.45 - excessive loss of nonvolatile acids or excessive production of bicarbonate.
metabolic alkalosis causes
vomiting, NG suction, diuretics, antacids, hypokalemia
metabolic alkalosis s/s
restlessness followed by lethargy, confusion, N/V/D, tremors, muscle cramps, tingling of fingers and toes, dysrhythmias, tachycardia, compensatory hypoventilation
metabolic acidosis
bicarbonate level less than 22 and a pH less than 7.35 - excessive production of nonvolatile acids or an inadequate concentration of acid within the serum.
metabolic acidosis causes
DKA, lactic acidosis, renal failure, diarrhea, and shock.
metabolic acidosis s/s
headache, decreased BP, muscle twitching, warm flushed skin, N/V/D, changes in LOC, kussmaul respirations
analyzing ABGs
pH: acid or base? Acid = lower, base = higher
PaCO2: respiratory
HCO3: metabolic
Determine compensation
Example: pH 7.28 / PaCO₂ 55 / HCO₃⁻ 26 → Uncompensated respiratory acidosis
pH
7.35-7.45
acid base balance
PaCO2
35-45
ventilation (lungs)
Bicarb/HCO3
22-26
metabolic control (kidneys)
PaO2
80-105
oxygenation
Sp02
95-10
oxygen saturation
nursing management of patients with a chest tube drainage system
keep system below chest, assess tidaling and air leaks, do not clamp, able to milk and strip tubing, have emergency supplies at bedside.
Volume assist control (V-A/C)
delivers a set tidal volume, pt can trigger breaths but every breath is full volume, guarantees minute ventilation, best for COPD, anesthesia, and pneumonia. key risks - barotrauma if lungs are stiff - A/C = always complete breaths
Full support
Pressure assist control (P- A/C)
delivers breaths to a set pressure, set rr, volume varies based on lung compliance, lung protective, best for poor lung compliance, increased risk of barotrauma. key risks - tidal volume can drop leading to hypoventilation - pressure control protects the lungs
Full support
Synchronized intermittent mandatory ventilation (SIMV)
set number of mandatory breaths, pt can breathe spontaneously in btwn, often paired with pressure support, best for weaning, pts who can breath on their own, stable COPD patients. key risk - fatigue if support is too low - SIMV = some from vent, some from me
Partial support
Pressure regulated volume control (PRVC)
95% of pts, targets a set volume, uses lowest pressure possible, automatically adjusted breath to breath. key benefit - combines safety of pressure + guarantee of volume - PRVC = pressure smart volume control
"Smart" pressure control
Pressure support (PS)
patient initiates every breath, vent only adds extra pressure, no set rate or volume, best for weaning, post op, awake and cooperative pts. key requirement - pt must be breathing independently - pressure support = ventilator gives a boost.
Spontaneous
Continuous positive airway pressure (CPAP)
no mandatory breaths, keeps alveoli open, best for obstructive sleep apnea, CHF with pulmonary edema, weaning trials - CPAP = continuous pressure, pt breathes alone
spontaneous
High frequency oscillatory ventilation (HFOV)
very tiny tidal volumes, extremely fast rates (300 - 420), maintains constant lung inflation. best for severe ARDS, covid pts, refractory hypoxemia, neonates, requires sedation/paralysis - HFOV = fast, tiny, last resort lungs
Tiny rapid breaths (300-420)
Noninvasive positive pressure ventilation (NPPV)
BiPAP/CPAP, delivers pressure without intubation, pt must be alert and protecting airway, best for COPD exacerbation, sleep apnea, do not use if decreased LOC, vomiting, facial trauma - NPPV = no tube, needs alert pt
No tube
maximize oxygen delivery with the goal of achieving a nontoxic FiO2 setting
Target FiO2 60% or greater
Use: peep, positioning prone, recruitment maneuvers, and prevent oxygen toxicity.
mechanical ventilation strategies used to prevent ventilator-induced lung injury
Low tidal volume (6 mL/kg) to prevent barotrauma
Limit plateau pressure ≤30 cm H₂O
PEEP to prevent alveolar collapse
Permissive hypercapnia (allow mild ↑ CO₂ to reduce ventilator injury)
Prone positioning improves oxygenation
Avoid excessive FiO₂ to prevent oxygen toxicity
ARDS causes
sepsis (most common), pneumonia, aspiration, trauma, burns, pancreatitis, drug overdoses, or near drowning.
ARDS assessment findings
acute onset (within week), severe dyspnea, tachypnea, hypoxemia, bilateral pulmonary infiltrates on CXR or CT, decreased lung compliance leading to stiff lungs, accessory muscle use, cyanosis, confusion, and fatigue.
ARDS outcomes and complications
high risk of morbidity and mortality in critically ill, risk of multi-organ failure, prolonged ICU stay, long term pulmonary dysfunction, shunt.
Barotrauma (pneumothorax, subcutaneous emphysema) reduces pressures
Volutrauma (alveolar distention) use low tidal volumes
Oxygen toxicity maintain FiO2 greater than 60% if possible
Multi organ failure monitor labs, hemodynamics, renal/liver support and function.
ARDS bundle
VAP prevention bundle: HOB ↑ 30-45°, oral care, suctioning
Sepsis bundle: Early recognition & antibiotics
Sedation & weaning bundle: Daily sedation vacation, spontaneous breathing trials
Early mobility: Reduce ICU-acquired weakness
concussion
temporary neurologic dysfunction, loc may or may not occur, headache, confusion, dizziness, usually no structural injury on CT.
contusion
bruising of brain tissue, focal deficits possible, edema may worsen over 24 to 72 hours.
epidural hematoma
arterial bleed, brief LOC leading to lucid interval leading to rapid deterioration, requires emergency surgery.
subdural hematoma
venous bleed, gradual neurological decline, common in elderly anticoag pts.
diffuse axonal injury
shearing injury for rapid acceleration/deceleration, immediate unconsciousness, poor prognosis.
importance of serial neurological assessment in the patient with TBI
TBI patients can deteriorate quickly, the purpose is to detect subtle changes early, identify rising ICP, guide interventions.
Neuro checks: level of consciousness (GCS), pupils, motor function, vital signs, should be every 15 minutes initially then hourly as stated.
nursing management with a TBI
Primary goals: maintain oxygenation, maintain cerebral perfusion pressure (60 - 70), prevent increased ICP, prevent secondary injury.
Airway and oxygenation: intubate if less than 8, maintain PaO2 above 60, avoid hypercapnia.
Blood pressure management: prevent hypotension, maintain adequate MAP.
ICP control: HOB 30 degrees, neutral head alignment, sedation, mannitol or hypertonic saline, CSF drainage.
Temp control by preventing hyperthermia
Glucose control.
Seizure prophylaxis.
Nutrition: early enteral feeding within 24 - 48 hours.
Spinal shock
temporary loss of all reflexes below injury, flaccid paralysis, no bowel/bladder tone, resolves when reflexes return, neurologic phenomenon.
Neurogenic shock
injury above T6, loss of sympathetic tone, hypotension and bradycardia, warm dry skin, hemodynamic emergency.
Orthostatic hypotension
BP drops when upright, due to impaired vasoconstriction, common during rehab.
Autonomic dysreflexia (T6 and above)
medical emergency caused by noxious stimulus below injury.
s/s: severe hypertension, pounding headache, flushing above injury, bradycardia, sweating.
Immediate nursing actions: sit out upright IMMEDIATELY, loosen tight clothing, assess bladder (most common cause) so check catheter and straight cath is needed, assess bowel for impaction, remove triggering stimulus, admin antihypertensive is BP remains elevated, do not leave pt flat.
primary survey trauma
A: airway with cervical spine protection
B: breathing
C: circulation and hemorrhage control
D: disability (neurological status)
E: exposure and environmental control
Goal is to identify immediate life threats
resuscitation phase trauma
Simultaneous with primary survey, includes oxygen, IV access, fluids, blood products, controlling bleeding.
secondary survery trauma
- AMPLE history
- rapid but thorough head-to-toe exam
- examine each region systematically
- non-critical injuries identified
- injuries found on primary survey are re-assessed
- set priority for care
- include resuscitation and frequent monitoring of vital signs
tertiary survey trauma
happens when the pt gets to the ICU, full head to toe assessment
thoracic trauma
pneumothorax, hemothorax, flail chest, cardiac tamponade. Nursing care - oxygen therapy, chest tube management, pain control, monitor respiratory status.
abdominal trauma
organs commonly affected are liver, spleen, kidneys, and bowel. Nursing care - monitor for internal bleeding, serial abd scans, fluid resuscitation, prepare for surgery if needed.
musculoskeletal trauma
fractures, compartment syndrome, crush injuries. Nursing care - immobilization, neurovascular checks, pain control, monitor for fat embolism.
maxillofacial trauma
airway obstruction, bleeding, facial fractures. Nursing care - airway management, suction, cervical spine protection, nutritional support.
nursing management principles for patients with shock, SIRS, and MODS
Continuous monitoring of vital signs, urine output, lactate levels, hemodynamics
Maintain perfusion with fluid resuscitation, vasopressors, oxygen therapy
Prevent complications with DVT prophylaxis, pressure injury prevention, glycemic control, nutritional support
Early recognition early intervention greatly improves survival
SIRS
Criteria are temp abnormality, tachypnea, tachycardia, abnormal WBC count. Can progress to sepsis or MODS
MODS
Progressive failure of two or more organ systems
Common organs affected are lungs, kidneys, liver, cardiovascular system.
Management is treating the underlying cause, organ support, preventing further injury.
plan of care for a patient who has sustained a burn injury
Airway: intubate early if inhalation injury suspected
Breathing: oxygen and ABGs
Circulation: control bleeding and IV fluids
Disability: neuro status
Exposure: remove clothing and assess burns
Fluid resuscitation for the first 24 hrs (critical), wound care such as debridement and dressings, pain management, infection prevention, nutritional support with high calorie and high protein, physical therapy if able, and psychosocial support.
pathology, assessment, and management of DIC
Patho: systemic activation of clotting cascade, formation of microthrombi leading to organ ischemia, clotting factors consumed = bleeding.
Assessment: bleeding (gums, IV sites, petechiae), organ dysfunction (kidneys, lungs, brain), labs (low platelets, high PT/INR, high aPTT, low fibrinogen, high D-dimer)
Management: treat underlying cause (sepsis, trauma, cancer), blood products (platelets, fresh frozen plasma, and cryoprecipitate), heparin, and supportive ICU care.
indications, assessment, and management CRRT
Indications: hemodynamically unstable, severe fluid overload, AKI with sepsis or shock, when slow, continuous is needed.
Assessment and management: continuous monitoring (ICU setting), frequent labs, strict I&O hourly, maintain catheter patency, anticoagulation monitoring to prevent filter clotting.
Complications: hypothermia, infection, electrolyte imbalances, filter clotting, hypotension
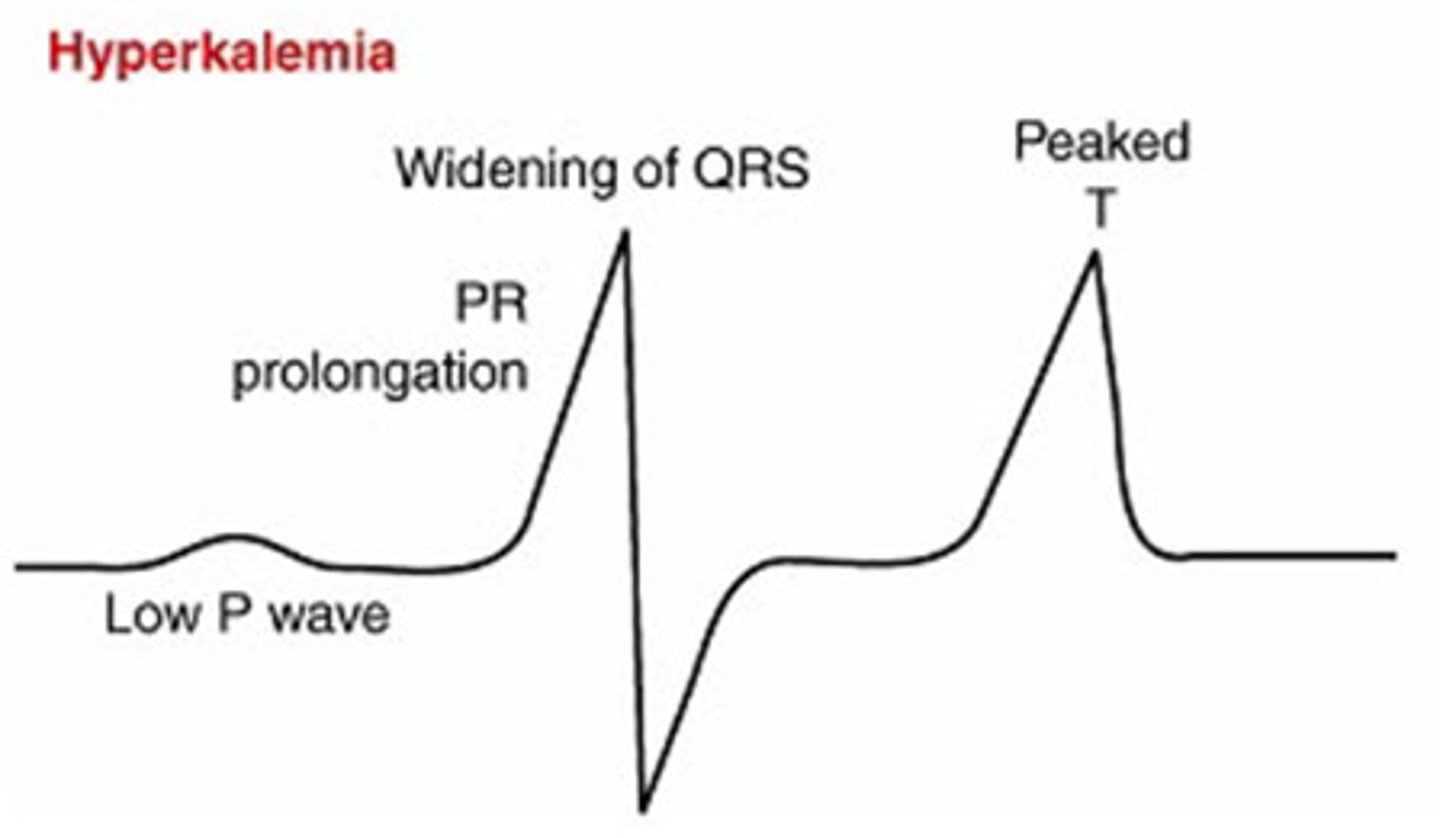
Hyperkalemia
life threatening cardiac arrhythmias, management - cardiac monitoring, administration of insulin + glucose, calcium gluconate, loop diuretics or dialysis, restrict potassium intake.
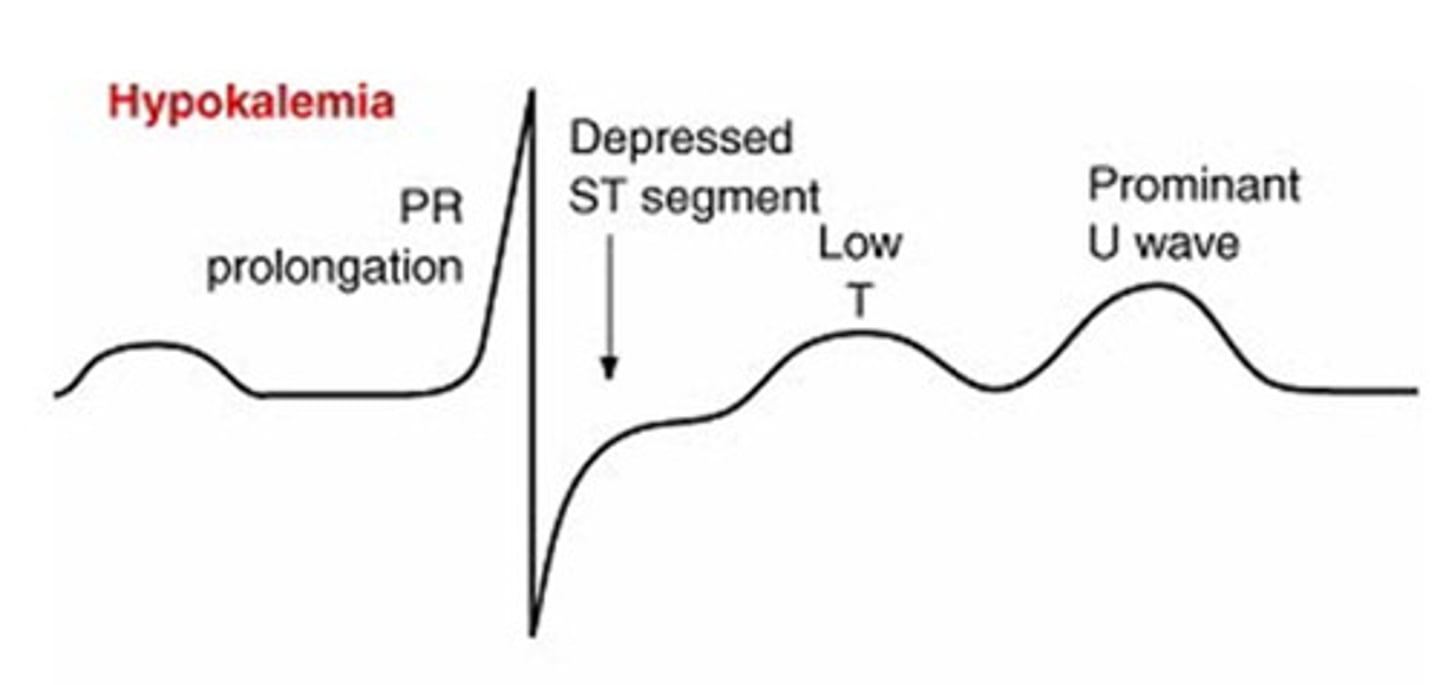
Hypokalemia
dysrhythmias and muscle weakness, management - replace potassium, never IV push, monitor ECG, encourage potassium rich foods.
Hyponatremia
neuro changes, confusion and seizures, management - fluid restriction, hypertonic saline (extreme cases), seizure precautions.
Hypernatremia
risk for cellular dehydration, management - gradual fluid replacement, hypotonic fluids, monitor neuro status.