Blood and Immune
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
the simplest and most successful form of life on earth
consists of DNA/RNA genome, lipid and protein coat
viruses cannot replicate themselves so must invade cells to multiply
billions of different viruses — infects all living things from bacteria to humans
intracellular pathogens
they need the cellular machinery (ribosomes and protein synthesis) so they need a way of getting inside a cell
outline viruses
bacteria are prokaryotes — no nucleus or organelles but a well-organised soup
10x the size of a virus
replicate rapidly by themselves and evolve
quickly by mutation and/or gene swapping
extracellular pathogens (mostly)
they grow outside cells, defence is primarily mediated by innate mechanisms and phagocytosis
outline bacteria
plant-like multicellular eukaryotic organisms
outline fungi and yeasts
complex multicellular organism too large to be eaten by phagocytes
outline parasites
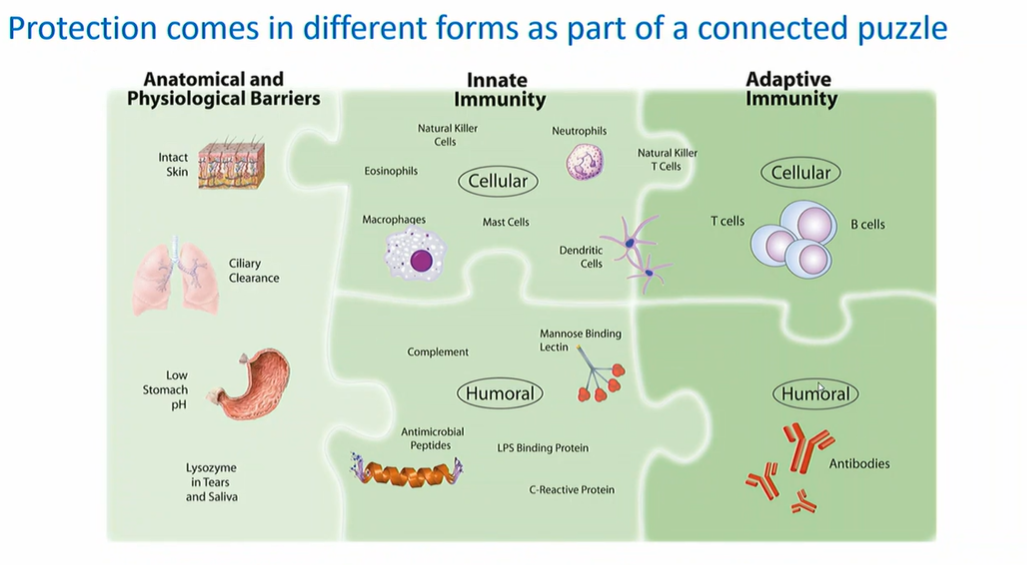
anatomical and physiological barriers
intact skin
ciliary clearance
low stomach pH
lysozome in tears and saliva
innate immunity
cellular:
neutral killer cells
neutrophils
neutral killer T cells
eosinophils
macrophages
mast cells
dendritic cells
humoral:
complement
mannose binding lectin
antimicrobial peptides
LPS binding protein
C-reactive protein
adaptive immunity:
cellular:
T cells
B cells
humoral:
antibodies
how does our body protect against pathogens
distribute oxygenated blood to tissues
what is the role of the heart in the circulatory system
arteries:
thick, muscular, elastic
carry blood away from heart
maintain back pressure for even flow
veins:
thinner walled
carry blood back to heart
have valves to prevent backflow
large vessels near heart = high volume/low flow; capillaries in tissue = low volume/high flow
describe the different blood vessels and their roles
120 = systolic (LV contracting); 80 = diastolic (heart at rest)
hypotension (too low) → blood can’t reach capillaries → fatigue, fainting
hypertension (too high) → capillary damage, abnormal clotting, stroke risk
outline blood pressure (120/80)
oxyhaemoglobin (bright red) → lungs to tissue via arteries
carbaminohaemoglobin (dark red) → tissue back to lungs via veins
exchange happens at lung alveoli (vast surface area)
outline the haemoglobin cycle in the transport of oxygen and CO2 transport
O2 binds/releases based on partial pressure (pO2):
Location | pO₂ (mmHg) | pCO₂ (mmHg) |
|---|---|---|
Air | 160 | 0.3 |
Lung alveoli | 100 | 35 |
Arterial blood | 80–100 | 40 |
Venous blood | 20–40 | 50 |
O2 associates in the lungs (high pO2), dissociates in tissue (low pO2) — CO2 is the reverse
cyanide and carbon monoxide can displace O2 from haem (cherry red/pink appearance)
outline how haem and partial pressure causes O2 to bind/release
Component | Examples & Notes |
|---|---|
Cells | Erythroid (O₂ transport), Myeloid (innate immunity), Lymphoid (adaptive immunity), Platelets (clotting) |
Proteins | Albumin (~50% of blood protein; pH/osmolarity balance), Haemoglobin (O₂/CO₂ transport), Fibrinogen (coagulation), Immunoglobulins (antibodies), Complement (innate defence) |
Lipids | Carried in lipoproteins — HDL (good), LDL (bad), VLDL |
Electrolytes | HCO₃⁻, Na⁺, Cl⁻, Ca²⁺, Mg²⁺, K⁺ |
Other | Vitamins, hormones, glucose |
outline the major components of blood
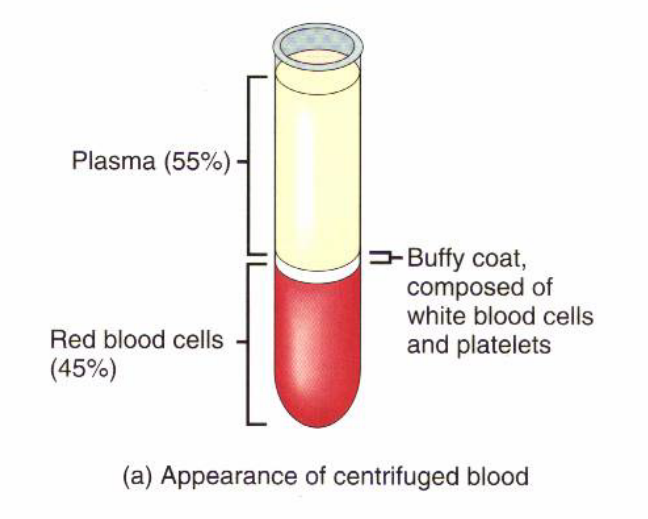
plasma (55%) — top layer; liquid fraction; still contains fibrinogen (needs anticoagulant, e.g. heparin)
buffy coat — thin middle layer; white blood cells + platelets
red blood cells (45%) — bottom layer
serum = what remains after clotting (no fibrinogen)
what does blood separate into when centrifuged
all cells originate from CD34+ haematopoietic stem cells (HSC) in thebone marrow (1 in 10,000 white cells)
CD = “cluster of differentiation” — cell surface markers used to identify cell types via monoclonal antibodies (mAbs)
outline what CD34+ is
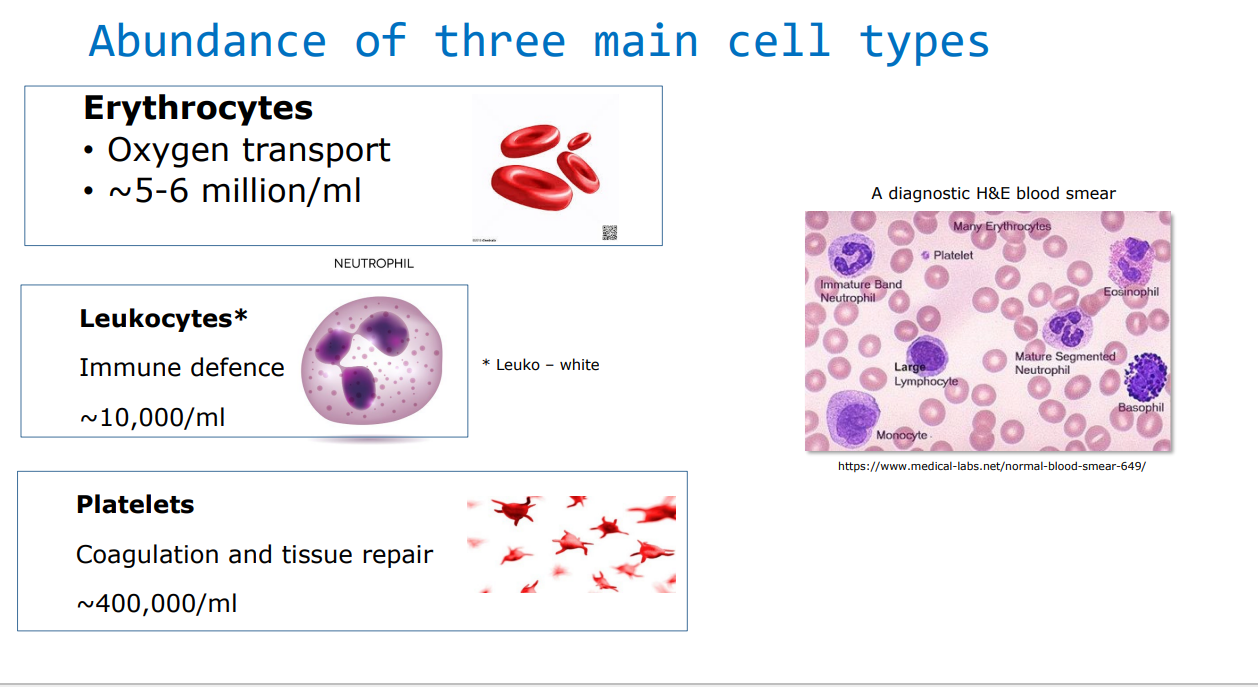
Cell Type | Function | Count/mL |
|---|---|---|
Erythrocytes (RBCs) | O₂ transport | ~5–6 million |
Leukocytes (WBCs) | Immune defence | ~10,000 |
Platelets | Coagulation & repair | ~400,000 |
outline the function and abundance of each blood cell type
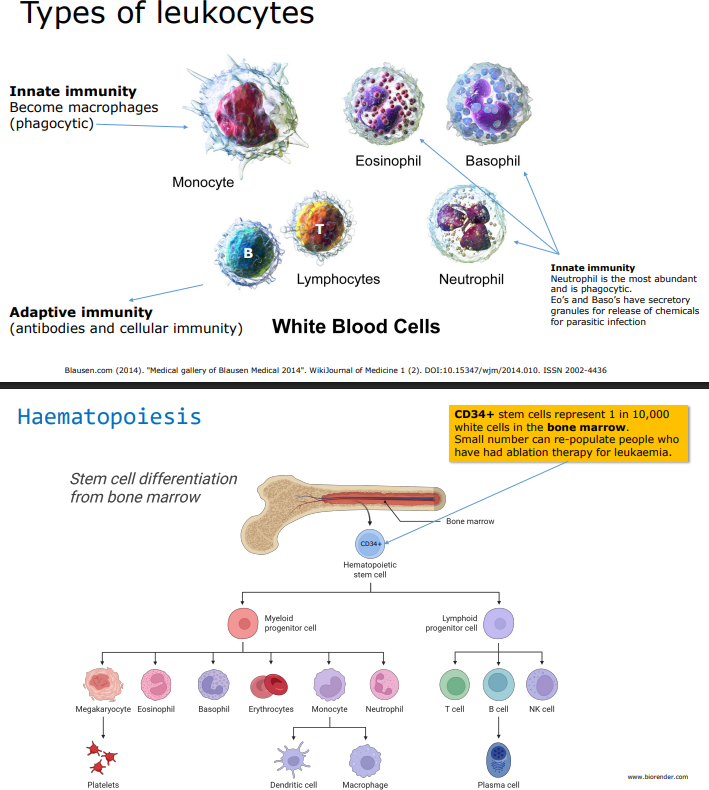
Innate immunity (fast, non-specific):
neutrophil — most abundant, phagocytic
eosinophil and basophil — secretory granules; fight parasitic infection
monocyte → becomes Macrophage (phagocytic) or Dendritic cell
Adaptive immunity (slow, specific):
B cells → become Plasma cells (produce antibodies); marker: CD19+
T cells (CD3+) → CD4+ (helper) or CD8+ (cytotoxic); marker: CD3+
NK cells
outline the different leukocyte types
AIDS → very low CD4+ + T cell count
Neutropenia → low myeloid count (signals infectionor cancer)
what are the clinical uses of immunophenotyping
Core concept: a proteolytic cascade — each factor activates the next (zymogen → active protease), with amplification at each step
Two activation pathways:
Pathway | Trigger | Key Factors |
|---|---|---|
Intrinsic (Contact) | Contact with activating surface (e.g. glass, prosthetic valve) | XII, XI, IX, VIII |
Extrinsic (Tissue Damage) | Cut, bruise, infection; platelet aggregation | Tissue Factor, V, VII, |
Both converge on Factor X → Xa, then:
Factor Xa → Prothrombin → Thrombin → Fibrinogen → Fibrin → CLOTcalcium is essential at multiple steps — remove it and blood won’t clot
plasminogen → plasmin disolves the fibrin clot (thrombolysis)
TPA (tissue plasminogen activator) used clinically for stroke, MI, DVT, PE — must be given early
Anticoagulants:
Herparin — inhibits thrombin
Hirudin — from leeches; also targets thrombin
Key clinical points:
haemophilia — genetic defect in a clotting factor; most common is X-linked VIII Factor deficiency
many blood-feeding parasites produce anticoagulants targeting the thrombin step
Outline the the coagulation cascade
Purpose: First-line innate defence — rapidly coats and destroys pathogens
9 major proteins (C1-C9) attach to bacteria in a proteolytic cascade
3 Activation Pathways (all converge on C3):
Pathway | Trigger |
|---|---|
Classical | Antibodies (IgM/IgG) binding to microbe → C1 |
Lectin | Complement recognises unique sugars on bacteria |
Alternative | Direct C3 activation on bacterial surface (most important — self-amplifying loop) |
Key steps and Terms:
C3 — most abundant complement protein in blood; activated C3b binds covalent to bacterial surface (opsonisation)
Convertases — stable enzyme complexes formed on bacteria surface; irreversibly bound; amplify cascade
Anaphylatoxins (C3a, C4a, C5a) — small fragments released during cascade; powerful chemoattractants for neutrophils
MAC (Membrane Attack Complex) — terminal pore formed by C5b-C9; lyses some bacteria
Clincial Points:
complement deficiency → susceptibility to chronic infections
many microbes produce virulence factors that inhibit complement
Outline the Complement System
There are three interconnected layers of defense against pathogens:
Layer | Examples |
|---|---|
Anatomical & Physiological Barriers | Intact skin, ciliary clearance in lungs, low stomach pH, lysozyme in tears/saliva |
Innate Immunity | Complement, neutrophils, macrophages, NK cells, PRRs, antimicrobial peptides |
Adaptive Immunity | T cells, B cells, antibodies |
Outline the layers of defense
Feature | Innate | Adaptive |
|---|---|---|
Speed | Immediate (minutes) | Slow (days–weeks) |
Specificity | Broad (recognises patterns) | Highly specific (recognises antigens) |
Memory | No memory | Forms memory |
Age | Ancient — found in all living things | Appeared ~300 million years ago |
key point: innate immunity provides the first-line response, it also acts as the alarm switch tht activates the adaptive response
Comapre Innate immunity to Adaptive immunity
Pathogen | Location | Defence Strategy |
|---|---|---|
Viruses | Intracellular | Mainly adaptive (cellular immunity + antibodies) |
Bacteria | Mostly extracellular | Innate + adaptive (complement, phagocytosis, antibodies) |
Fungi/Yeast | Extracellular | Innate + adaptive |
Parasites | Multicellular, extracellular | Innate + adaptive (eosinophils important) |
outline the different types of pathogens and the respetive immune strategies that are used to combat them
How neutrophils travel from blood vessels to the site of infection
Activation
chemoskines released by opsonisation/tissue injury activate nearby capillary endothelial cells
Tethering
neutrophil loosely attaches to the capillary wall — mediated by selectins (on endothelial cells) binding sialyl Lewis X (sLex) (on neutrophil surface)
Adhesion
strong binding between neutrophil integrins and ICAM-1 on the endothelium
neutrophil flattens and immobilises
Diapadesis
neutrophil squeezes between endothelial cells into the interstitial space (tissue)
Chemotaxis
neutrophil follows a chemokine gradient (e.g. C5a) to migrate toward infection site
The entire process takes only minutes from initial infection
Outline Neutrophil extravasation
chemoattractants (e.g. C5a) radiate outward from bacteria
neutrophil senses gradient at its leading edge
moves via actin polymerisation at leading edge and depolymerisation at trailing edge
outline how neutrophils find bacteria
bacteria coated in C3b via complement (opsonisation)
neutrophil complement receptors (CR1, CR2, CR3, CR4) bind C3b
CR1 is the main receptor
cross-linking of surface CRs → triggers phagocytosis
C5a receptor also activates the neutrophil further
outline how phagocytosis is triggered by the complement receptor
antibodies (IgM or IgG) bind bacteria surface antigens → Fc region exposed
neutrophil Fc receptors (FcR) bind the multivalent Fc regions
triggers phagocytosis
outline how phagocytosis is triggered by Fc receptors
Capture — neutrophil adheres to bacterium
Invagination — membrane engulfs bacterium, forming a phagosome
Phagosome/lysosome fusion → phagolysosome
Killing — phagolysosome acidifies; superoxides and digestive enzymes destroy the bacterium
Exocytosis — waste expelled from cell
Outline the general steps of phagocytosis
PAMPs — what PRRs recognise
PAMPs = Pathogen-Associated Molecular Patterns
molecules unique to microbes (not found on human cells)
structural complex (e.g. LPS) and evolutionary stable — don’t change much
PRRs bridge innate and adaptive immunity — they tell the immunity system if pathogen is present and what type it is
outline Pattern Recognition Receptors (PRRs)
most well-known class of PRR
rich in leucine repeats (coiled-spring shape)
bind many different PAMPs; often work together
activation → signalling cascade via NFkB (nuclear factor) → strong innate immune response
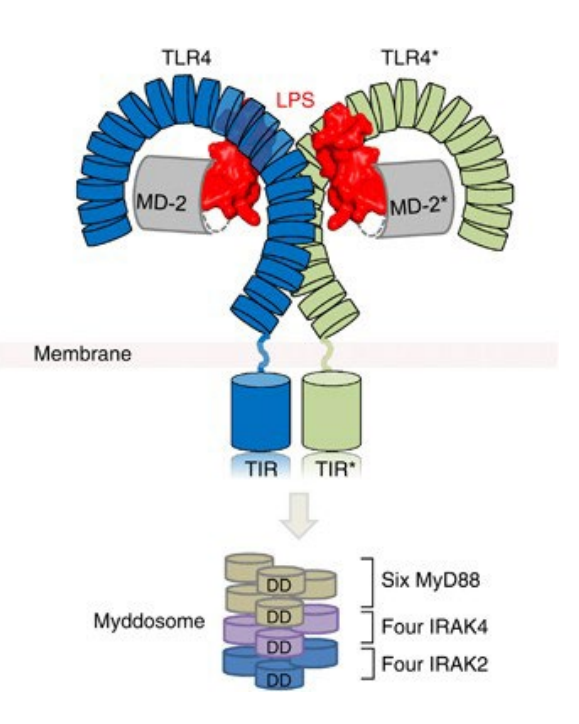
outline Toll-Like Receptors (TLRs)
LPS (Lipopolysaccharide):
a membrane component of all gram-negative bacteria
extremely complex molecule; only a small part (lipid A) is recognised by TLR4
acts as a pyrogen — tiny amounts in the bloodstream cause rapid fever
must be removed from any injectable pharmaceutical products (common contaminant)
Clinical significance:
gram-negative bacterial infection → LPS release → massive TLR4 activation → septic shock
septic shock = life-threatening, systemic inflammatory response
outline TLR4 and LPS
Feature | Gram-Positive | Gram-Negative |
|---|---|---|
Cell wall | Thick peptidoglycan layer | Thin peptidoglycan + outer membrane containing LPS |
Gram stain | Purple | Pink/red |
LPS present? | No | Yes |
Septic shock risk | Lower | Higher (due to LPS) |
compare gram negative bacteria to gram positive bacteria
protective immunity that develops after exposure to infection or vaccination
unlike innate immunity, it adapts over time — responds faster and more effectively with each encounter
can provide lifelong protection (e.g. measles)
relies on billions of naive B and T lymphocytes, each with a unique antigen specificity, generated randomly before birth
diversity come from random gene rearrangement in BCR and TCR loci — the only region in your genome that does this
what is adaptive immunity
transposition is a gene changing location within a genome
two essential elements of transposition:
transpoease (recombinase) — enzyme that cuts and repositions DNA; in B/T cells these are RAG1 and RAG2 (only active in B and T lymphocytes)
recognition signal sequences (RSS) — short conserved sequences (7 or 9bp) at the end of each segment, recognised by RAG1/2 which then cuts and rejoins segments that can be millions of base pairs apart
outline transposition
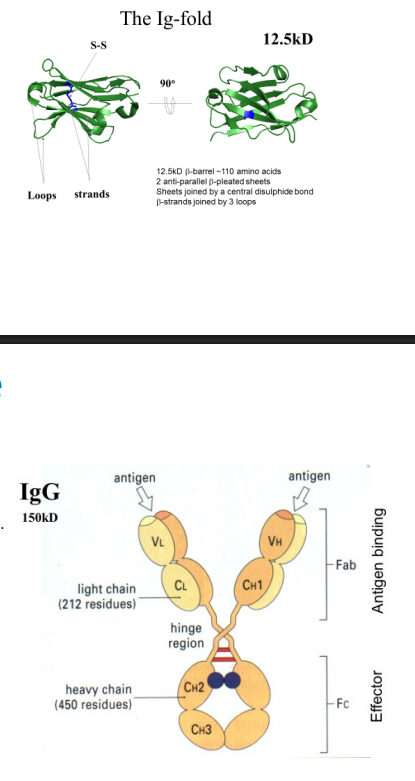
The Ig domain (building block):
~110 amino acids in length; ~12.5kD
structural shape: β-barrel fold — two anti-parallel β-pleated sheets (like two cupped hands)
held together by a central covalent disulphide bond
three unconstrained loops join the sheets — these loops can vary greatly in amino acid sequence without disrupting the overall structure → this is where diversity arises
Overall Antibody structure
made of 2 protein chain types: Heavy (H) chains and Light (L) chains, both built from repeated Ig domains
assembly: L—S-S—H—S-S—H—S-S—L (connected by disulphide bonds)
shape: Y-shaped
Region | Location | Function |
|---|---|---|
Variable domain (Fab) | Tips of the two arms | Antigen binding; where all diversity occurs |
Effector region (Fc) | Stem (CH2 + CH3) | Binds Fc receptors and complement C1; defines antibody class and function |
Hinge region | Junction of arms and stem | Flexibility |
describe the immunoglobulin (Ig) structure
each antibody has two identical antigen binding sites (one per arm)
each site is made up of 6 loops total — 3 from the L-chain + 3 from the H-chain
these loops are the hypervariable regions = complementarity determining regions (CDRs): CDR1, CDR2, CDR3
CDR3 (the VDJ join loop) is the most variable and contributes most to antibody diversity
outline the antigen binding site
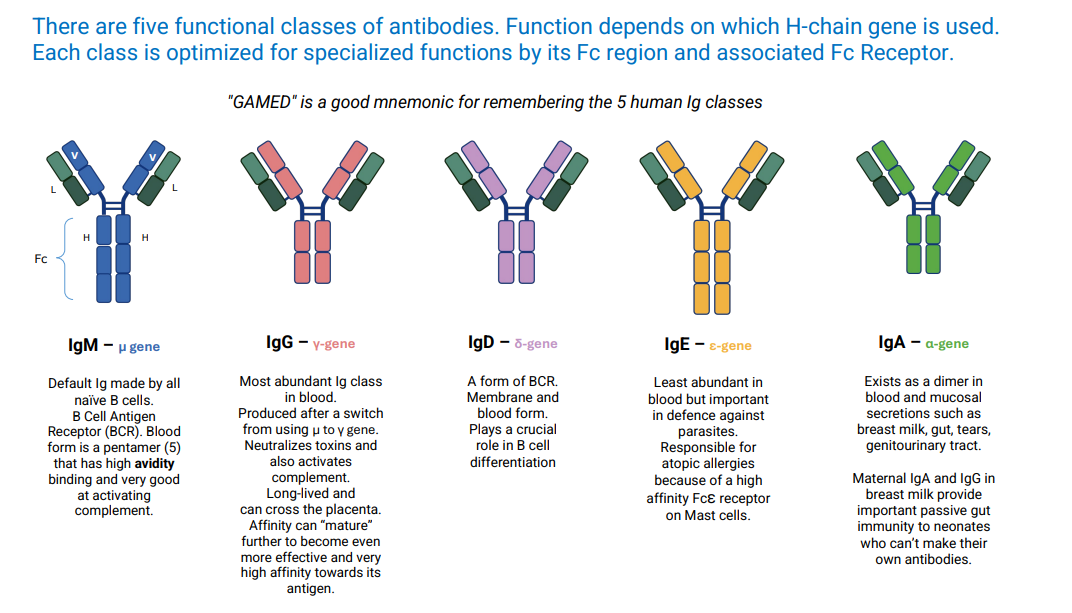
Class | Gene | Form | Key Functions |
|---|---|---|---|
IgG | γ | Monomer | Most abundant in blood; neutralises toxins; activates complement; crosses placenta; long-lived; undergoes affinity maturation |
IgA | α | Dimer | Found in mucosal secretions (breast milk, gut, tears, genitourinary tract); passive gut immunity to neonates |
IgM | μ | Pentamer (blood) / Monomer (BCR) | Default Ig of naïve B cells; 10 antigen binding sites; high avidity; excellent at activating complement (classical pathway) via 5 Fc regions |
IgE | ε | Monomer | Least abundant; defence against parasites; causes atopic allergies via high-affinity FcεR on mast cells |
IgD | δ | Monomer | BCR form; role in B cell differentiation |
outline the five antibody classes
the strength of binding between a single antibody binding site and its antigen — sum of attractive forces exceeding repulsive forces
example: high affinity IgG after maturation
what is affinity
combined binding strength from multiple simultaneous weak contacts — orders of magnitude stronger than single affinity
example: IgM pentameter with 10 binding sites — like Velcro
key point: avidity allows naive, low-affinity antibodies (like IgM) to still effectively bind pathogen surfaces before affinity maturation has occurred
what is avidity
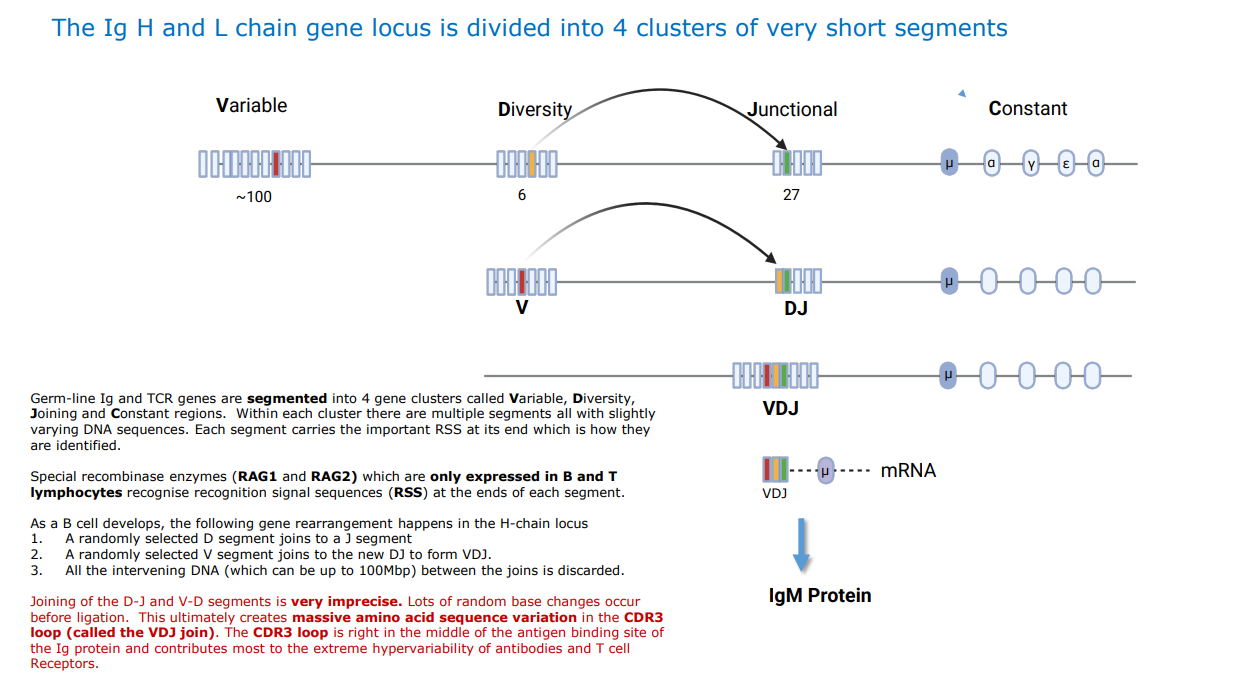
the Ig H-chain gene locus is divided into four clusters:
Segment
Name
Number of variants
V
Variable
~100
D
Diversity
6
J
Junctional
27
C
Constant
Defines antibody class (μ, α, γ, ε, δ)
what are the 4 gene segments (V-D-J-C)