cysts and cyst like lesions of the jaw
1/94
Earn XP
Description and Tags
lecture given 4/30/2026- i tried to include all pics so sorry if this is the most annoying knowt ever
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
what are the keys to radiographic interpretation?
clinical exam, quality of the diagnostic images, number and type of diagnostic images, viewing conditions, image analysis
what factors should you use to systematically analyze intraosseous lesions?
location of the abnormality, periphery of the lesion and internal contents, effects on surrounding structures, radiographic interpretation
what are the types of acquired abnormalities?
cyst, benign neoplasia, malignant neoplasia, inflammatory lesion, bone dysplasia, vascular anomaly, metabolic disease, trauma
cyst
a pathologic cavity that is filled with fluid, lined by epithelium, and surrounded by definite connective tissue wall
development requires presence of epithelium in deep tissues and proliferative stimulus
what differentiates a pseudocyst from a cyst?
it lacks epithelial lining
what is the pathology of a cyst?
exact pathogenesis remains somewhat unknown
theories regarding that factors that influence formation and growth
exact mechanism is likely a combination of developmental and inflammatory influences unique to the cyst
what are the clinical features of a cyst?
swelling, lack of pain unless infected, interruption in the eruption of teeth
what are radiographic features of cysts?
located in mandible or maxilla
well defined and corticate if infected
round or oval
internal structure is radiolucent, can have dystrophic calcification and septation
what effects can cysts have on surrounding structures?
displacement, resorption of roots, expansion of cortical plates, IAC displacement (inferiorly), displacement of maxillary antrum

what is this?
cyst
types of odontogenic cyst
radicular, residual, dentigerous, buccal bifurcation, keratocystic odontogenic tumor, basal cell nevus syndrome, lateral periodontal, glandular odontogenic
types of nonodontogenic cysts
nasopalatine duct cyst, nasolabial
cyst like lesion
simple bone cavity, stafne defect
radicular cyst
most likely due to epithelial cells undergoing proliferations and degeneration due to inflammation
synonyms: periapical cyst, apical periodontal cyst, dental cyst
what are clinical features of radicular cysts?
*most common type of cyst in the jaw, arise from non-vital teeth
can be asymptomatic unless secondarily infected
incidence is greater in pts 30-60 y/o, shows a slight male predominance
60% found in maxilla, esp incisors and canines
what are the radiographic features of radicular cysts?
the periphery usually has a well defined cortical border- but if secondarily infected may lose cortex
typically radiolucent- dystrophic calcification may develop in long standing cysts
displacement and resorption of roots may occur
typical hydraulic (circular) shape in the periapical region of the tooth
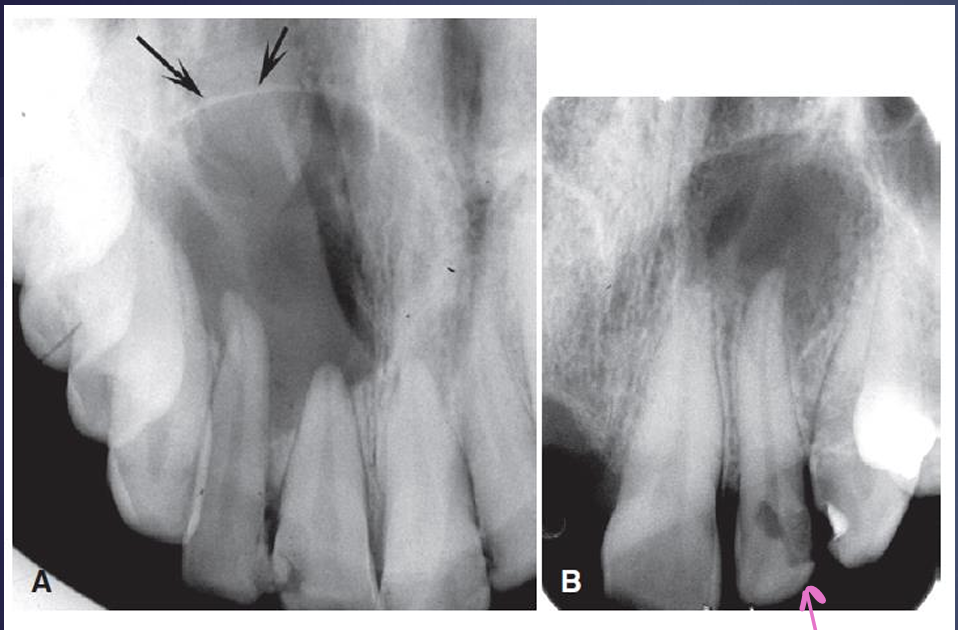
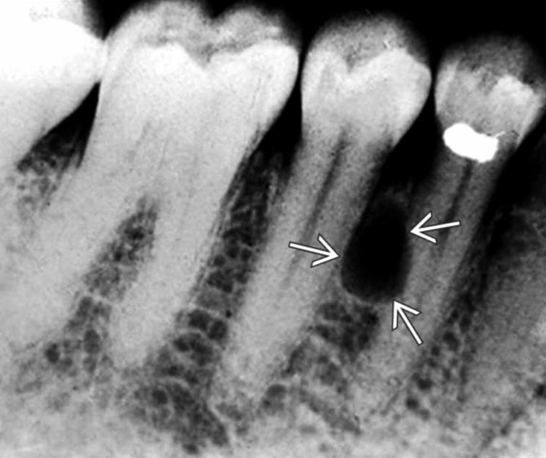
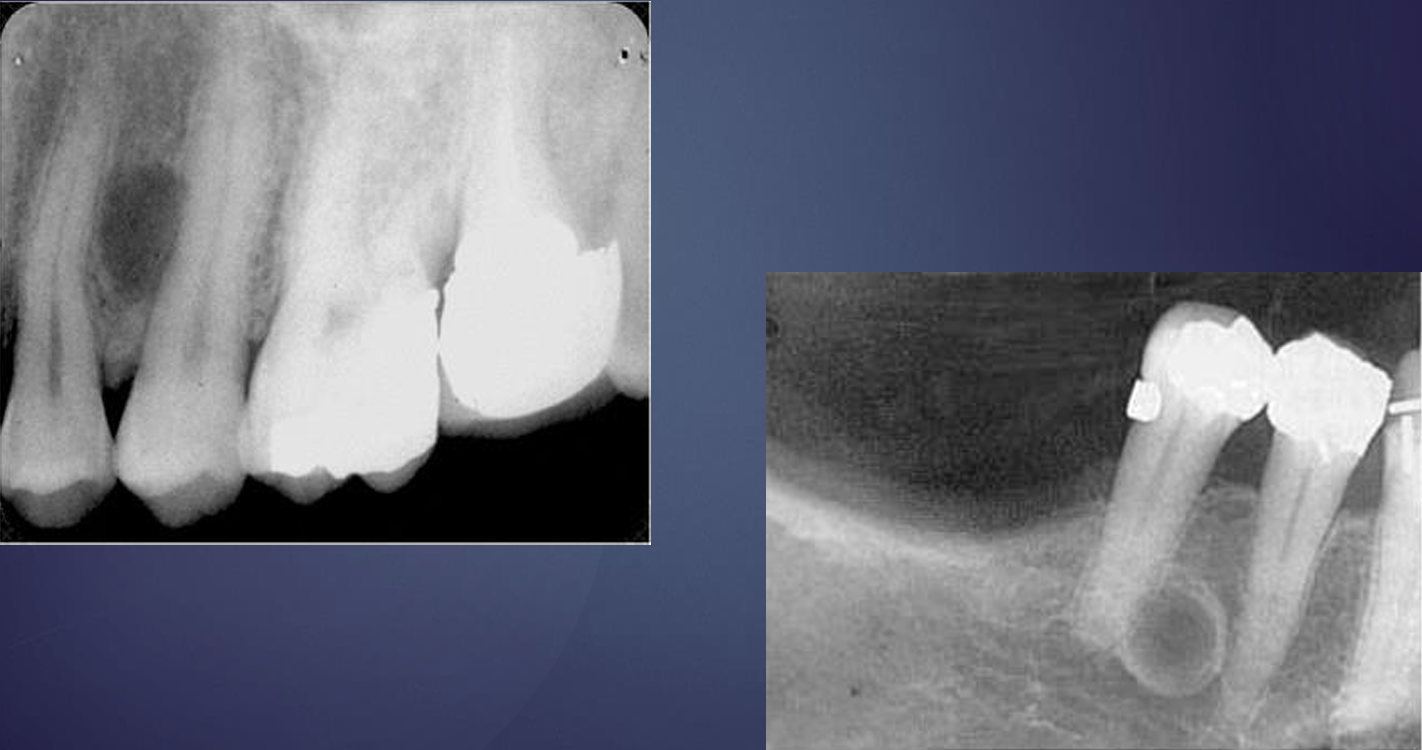
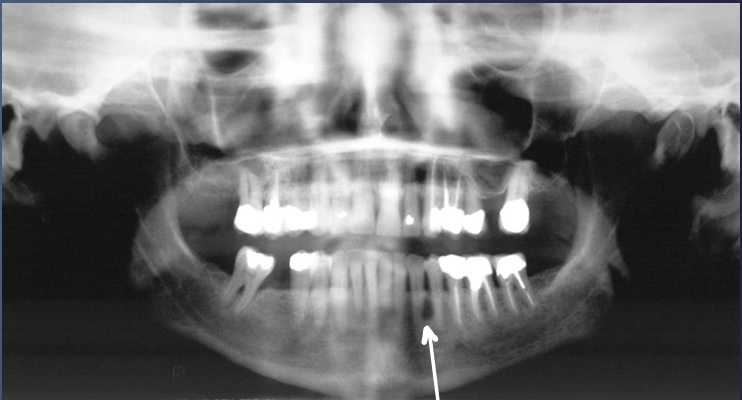
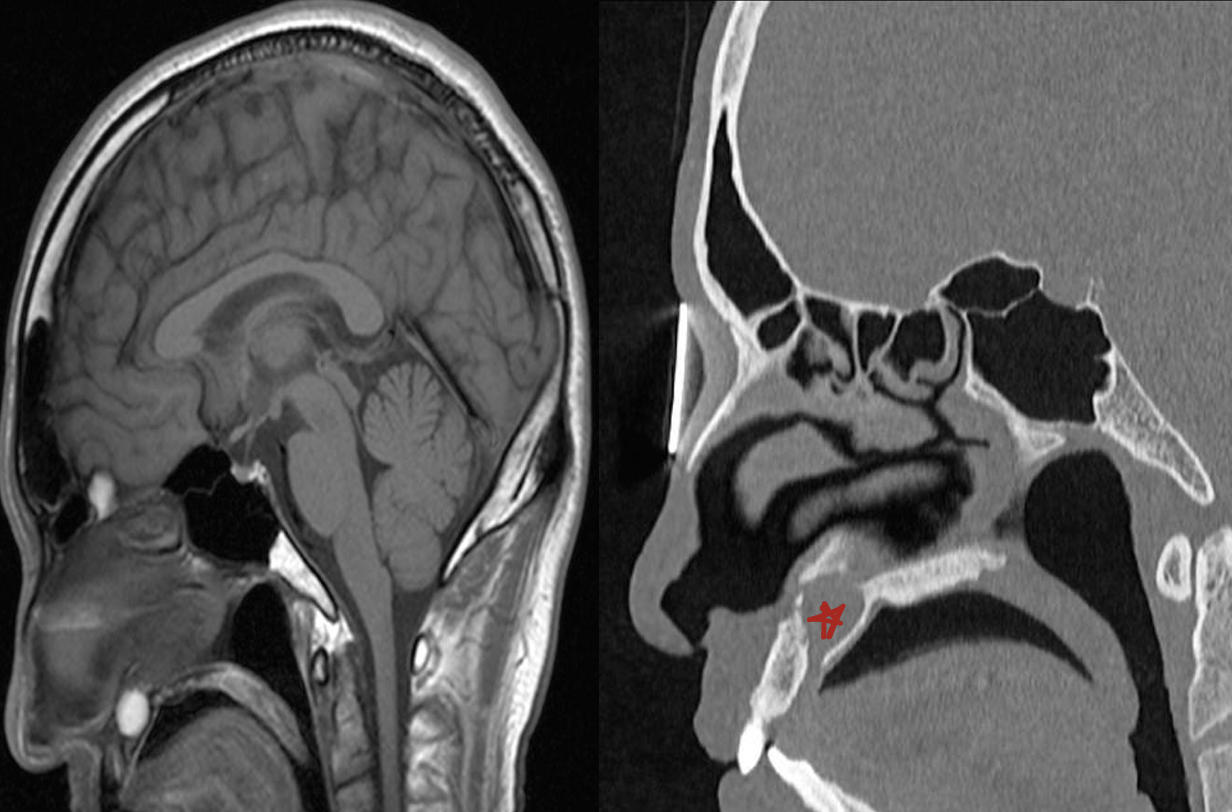
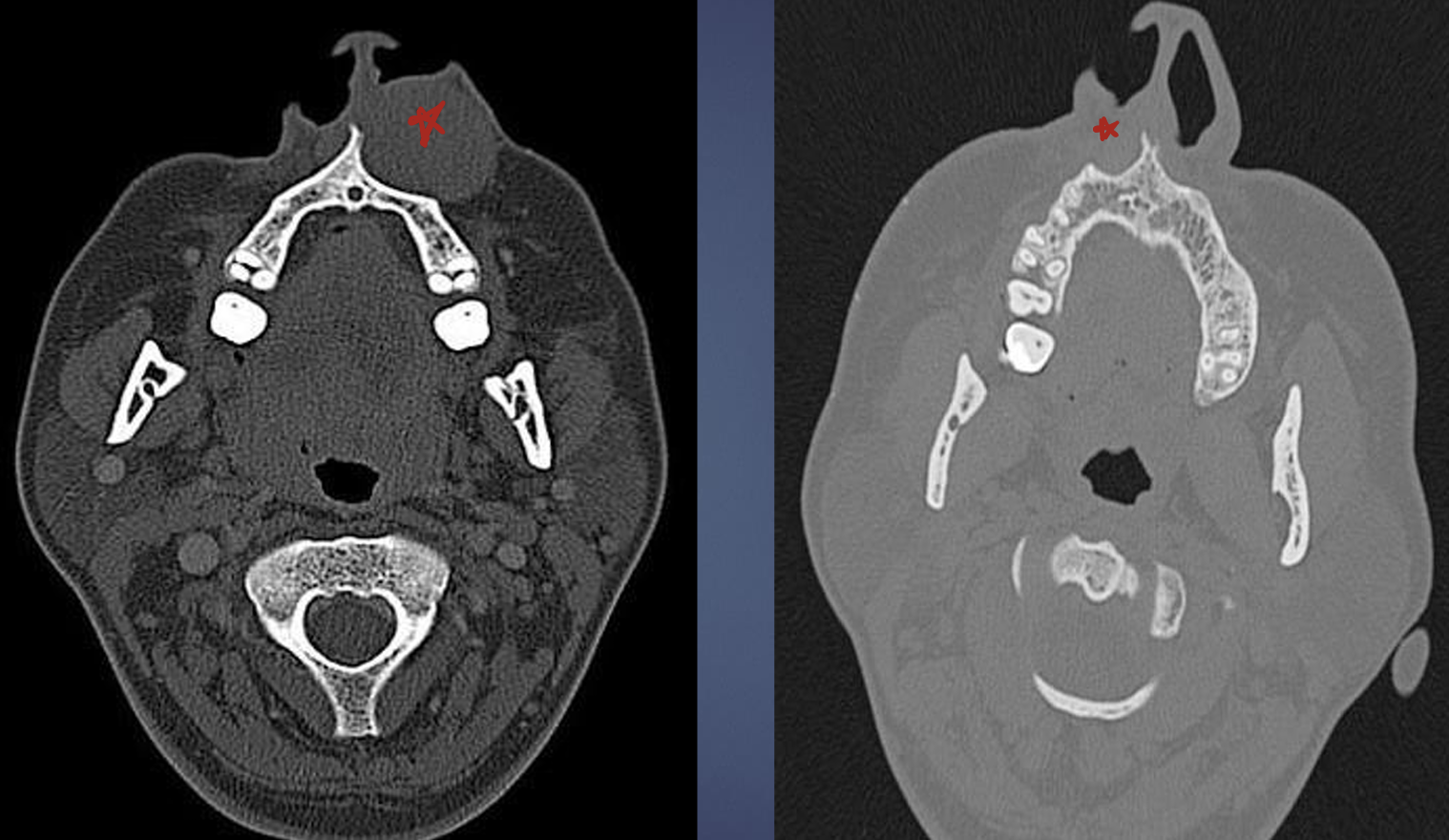
what is this, and what is the pink arrow pointing at?
radicular cyst
the likely reason for the lesion (okay dr. seuss)

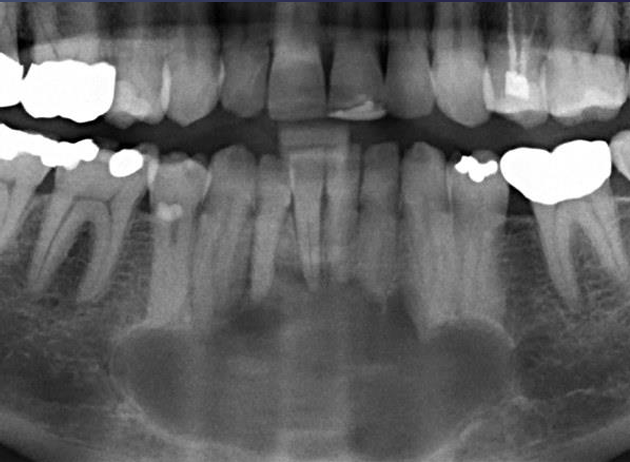
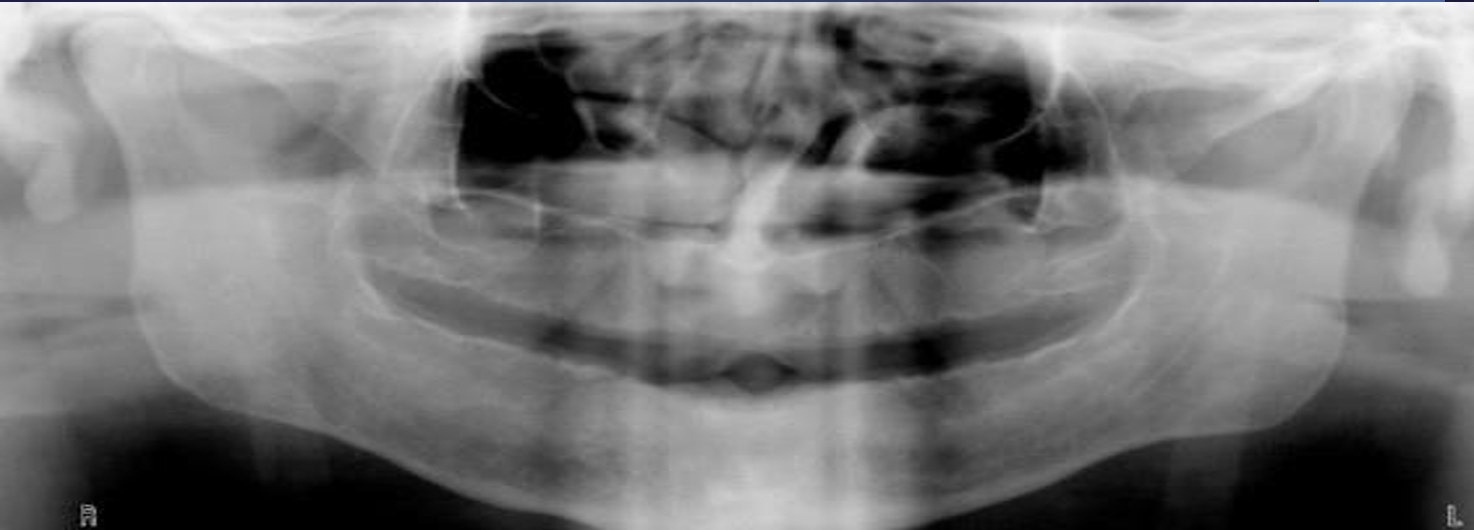
what is this?
radicular cyst

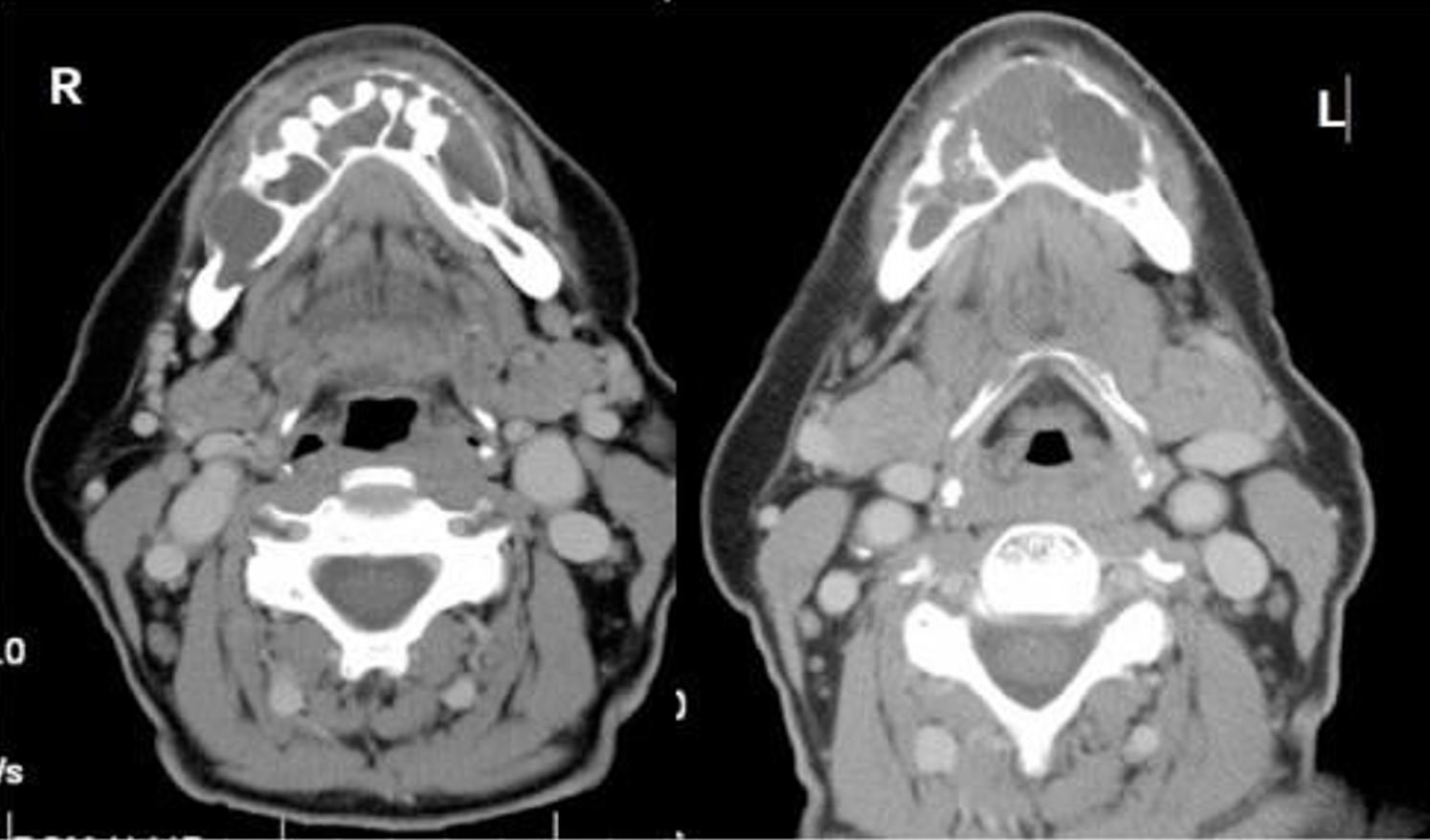
what is this, and what is happening?
radicular cyst
elevation of the maxillary antrum
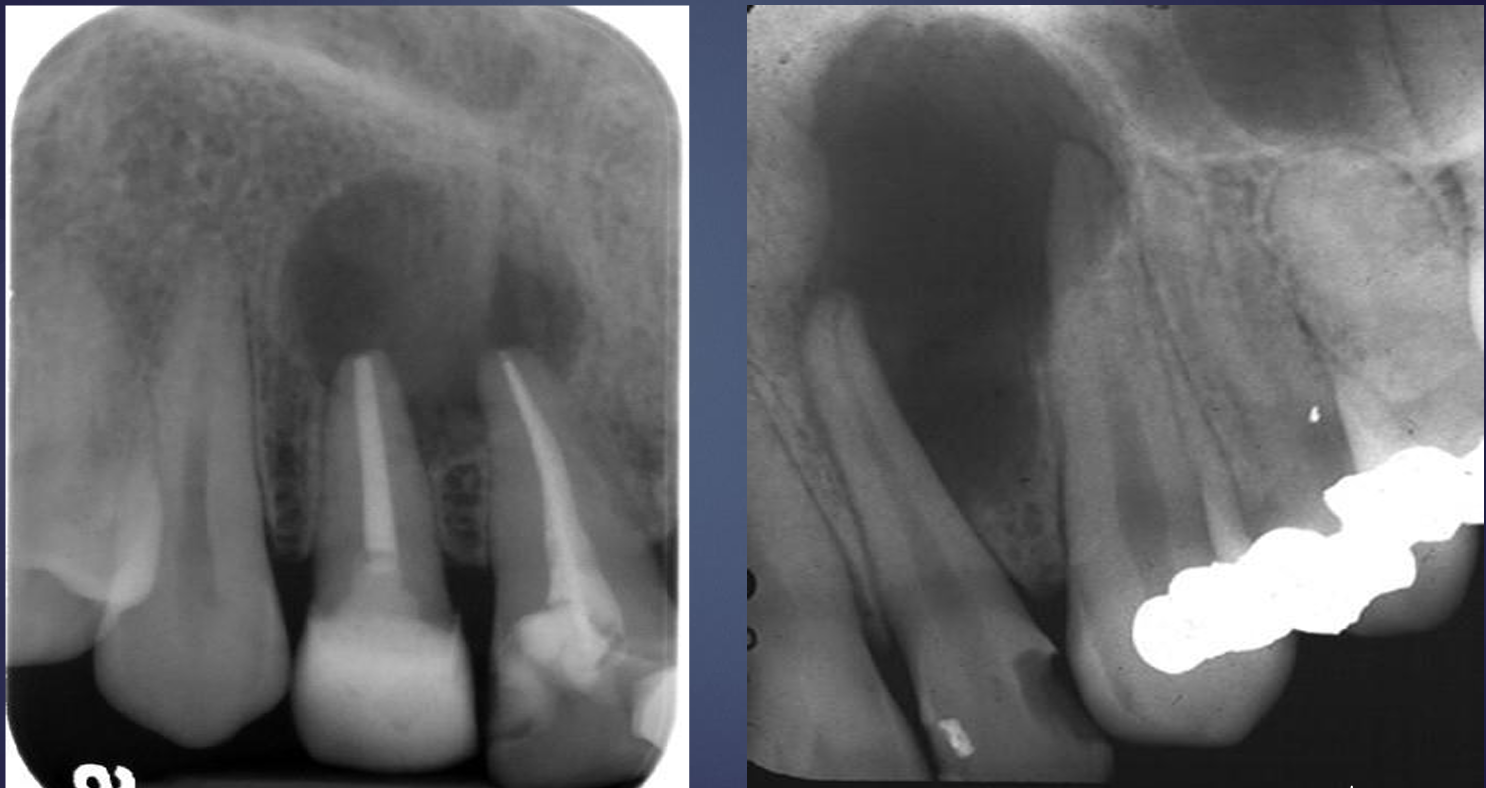
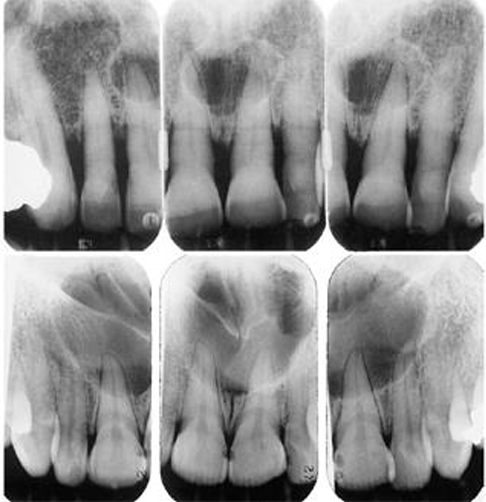
what is this, and what is happening?
radicular cyst
blunting of roots and splaying of teeth
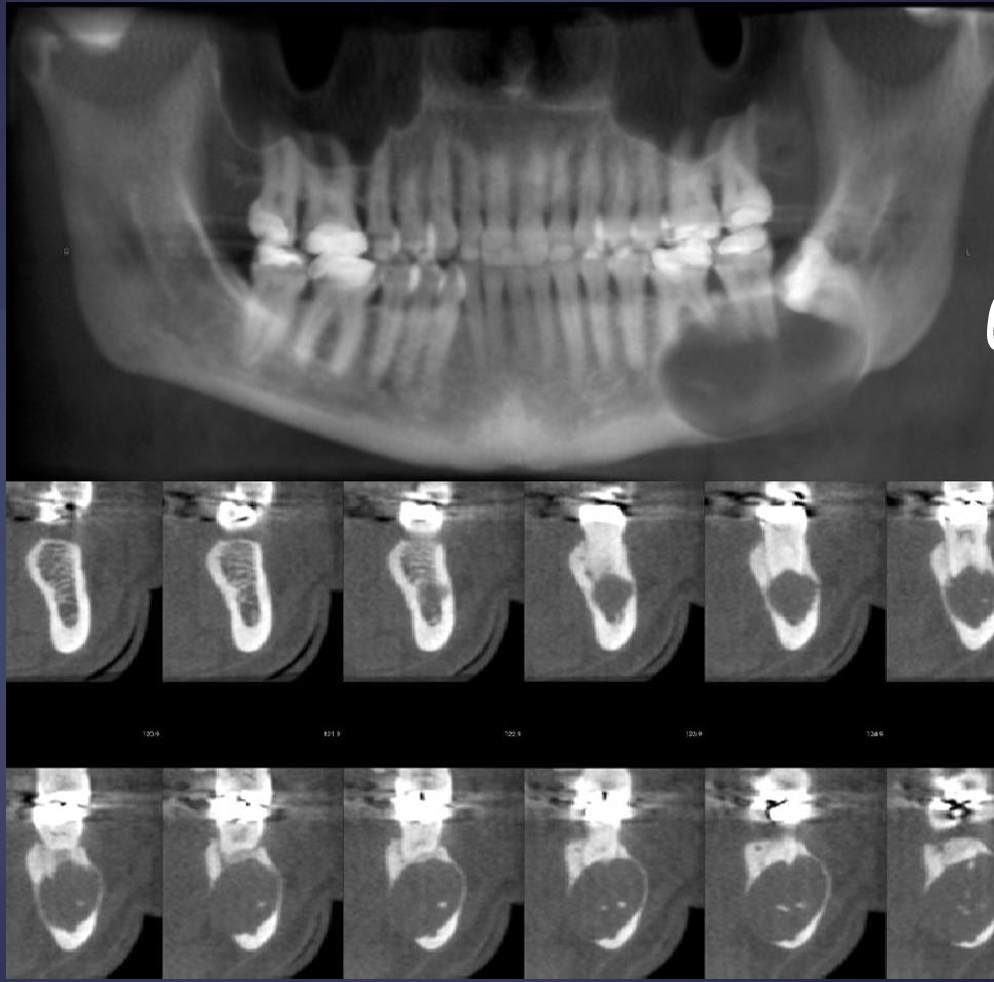
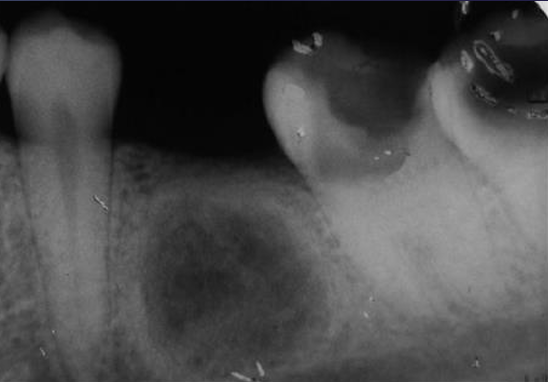
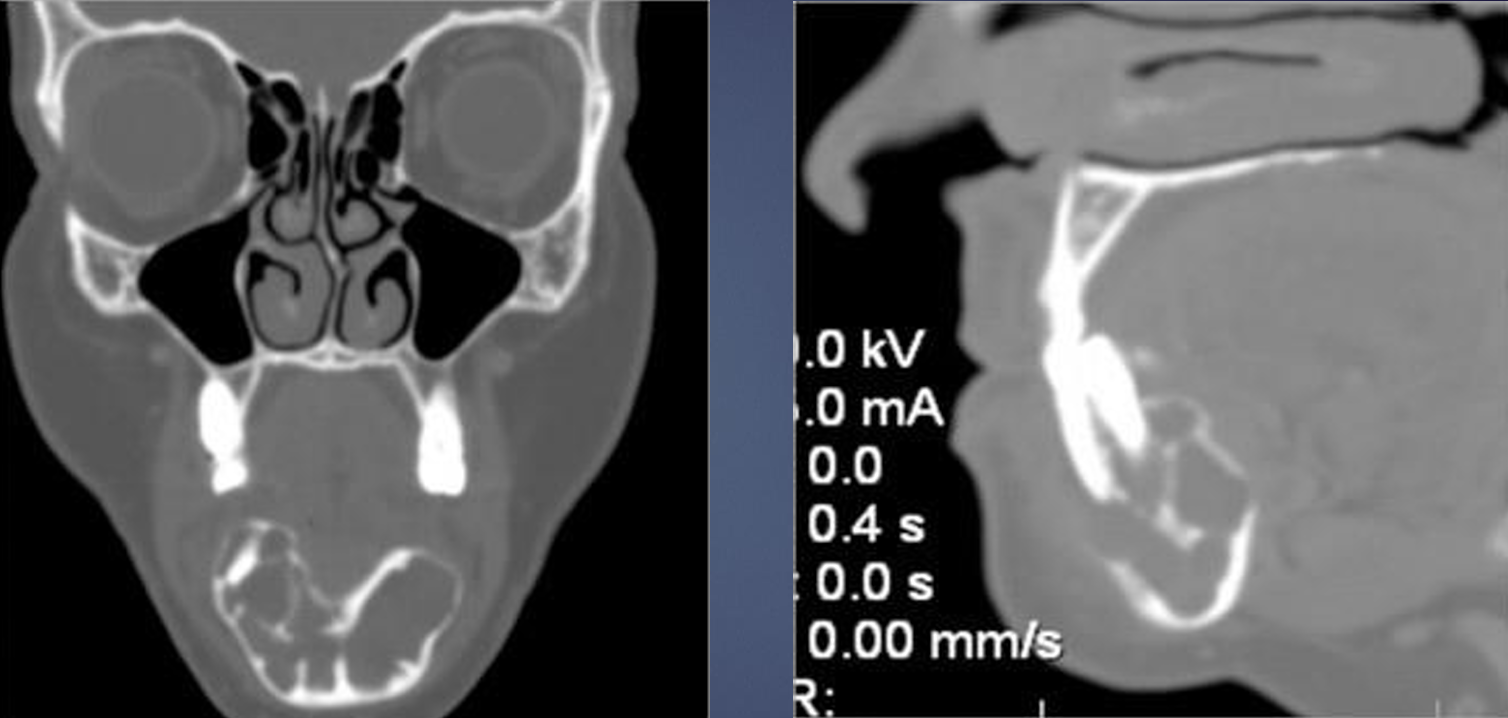
what is this and what phenomena can be seen in the lower row?
radicular cyst
partial volume averaging
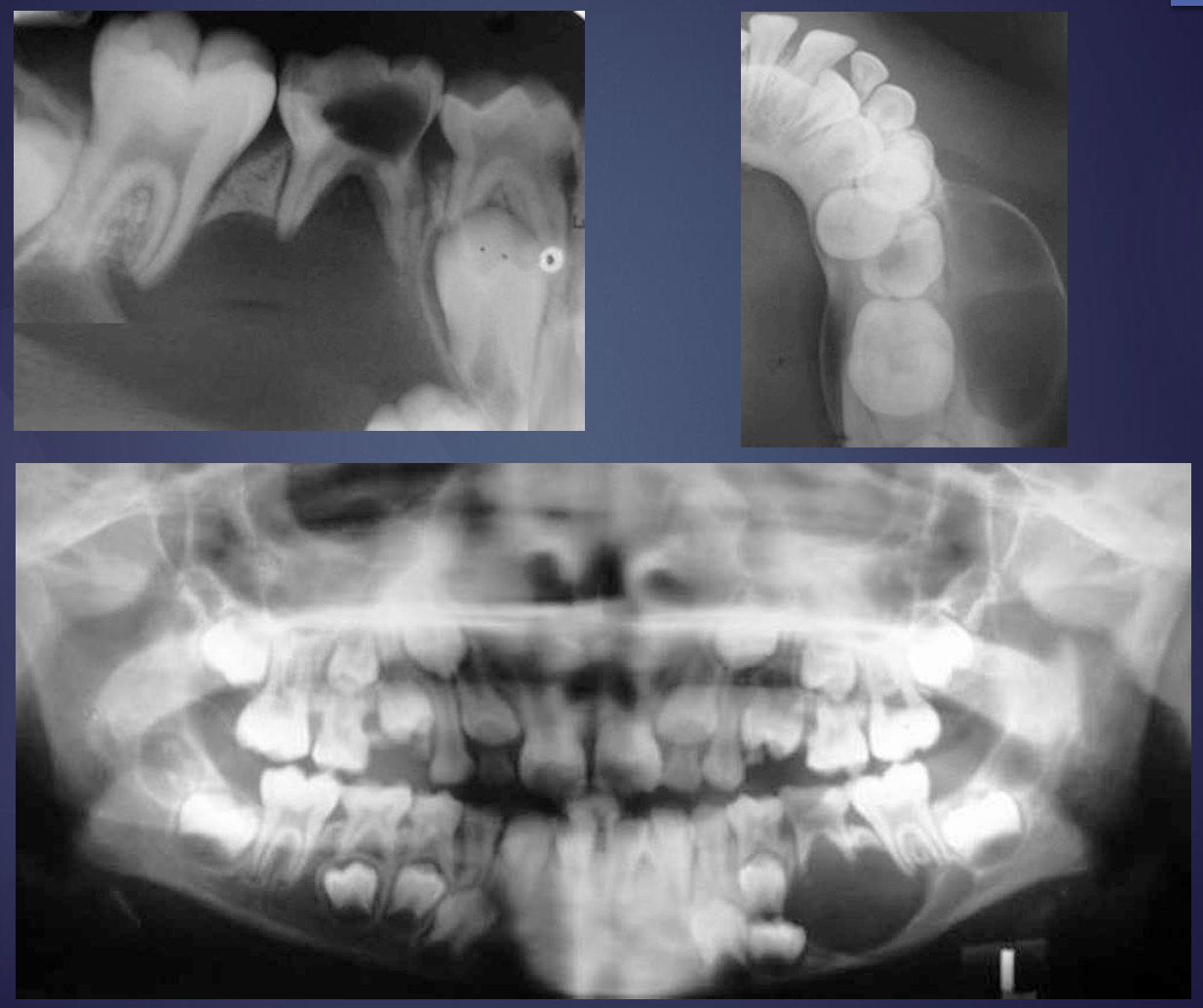
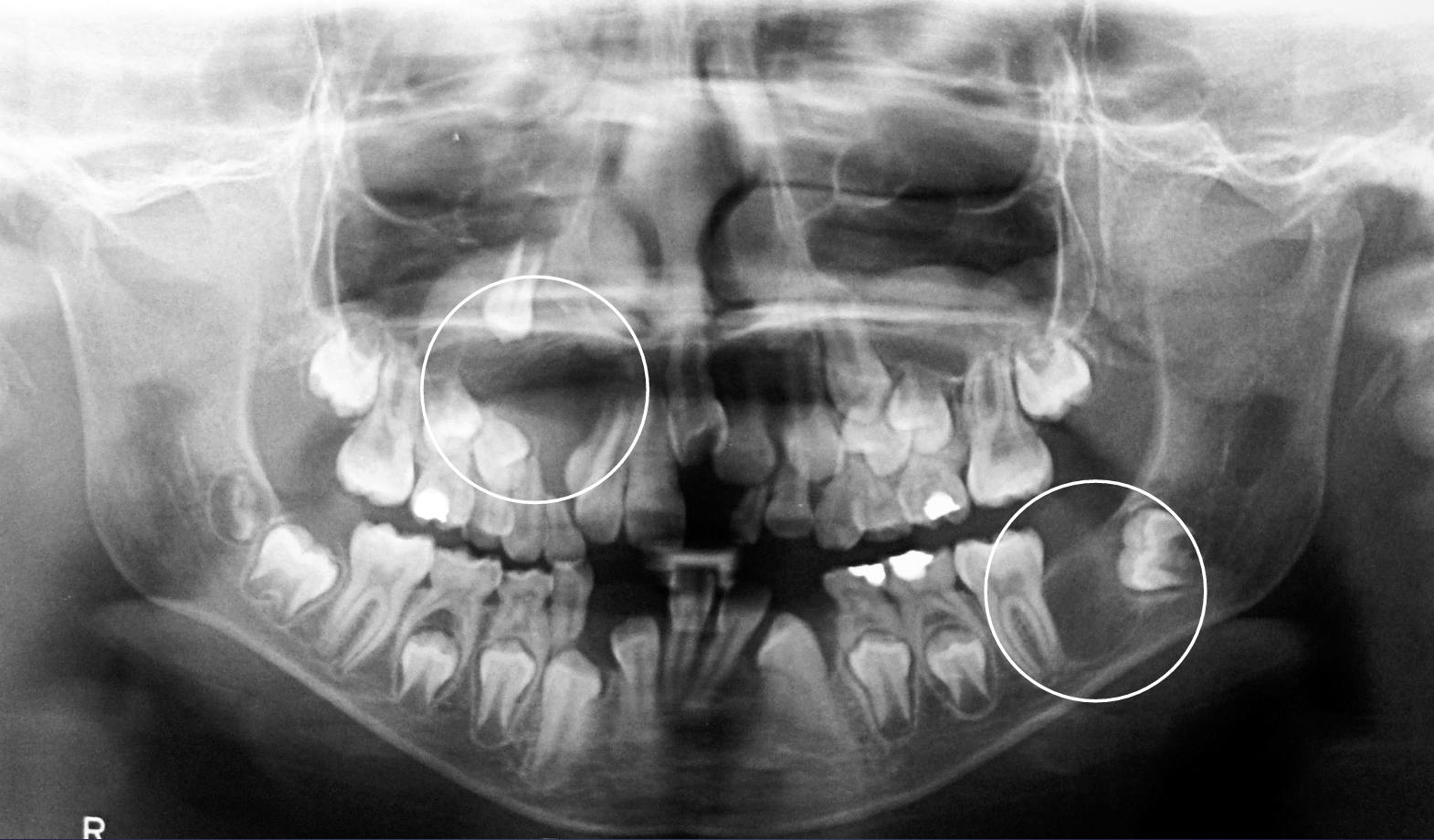
what is this?
a baby with a radicular cyst
what are the differential diagnoses for a radicular cyst?
apical granuloma/abscess
fibrous healing of endodontically treated tooth (clinical evaluation may help differentiate)
early stage of periapical osseous dysplasia (vitality testing may help differentiate)
lateral periodontal cyst (vitality testing may help differentiate)
OKC if small and unilocular
how are radicular cysts managed?
vitality testing, CBCT if very large or encroaches on adjacent structures, removing the source of infection (endo or extraction)
if there is healing within a radicular cyst after it is treated, where does the healing start?
in the periphery, then fills in the center
what are the clinical features of a residual cyst?
inflammatory odontogenic cyst formed after incomplete removal of original radicular cyst following tooth extraction
more common in males
unilocular, round, well corticated radiolucency
maxilla more common than mandible
above IAC in posterior mandible
can extend into maxillary sinus
usually asymptomatic- asymptomatic tend to decrease in size due to epithelial atrophy, enlargement due to persistent presence of an inflammatory stimulus
symptomatic more common in anterior maxilla, and may be less corticated
*seen at edenulous spaces
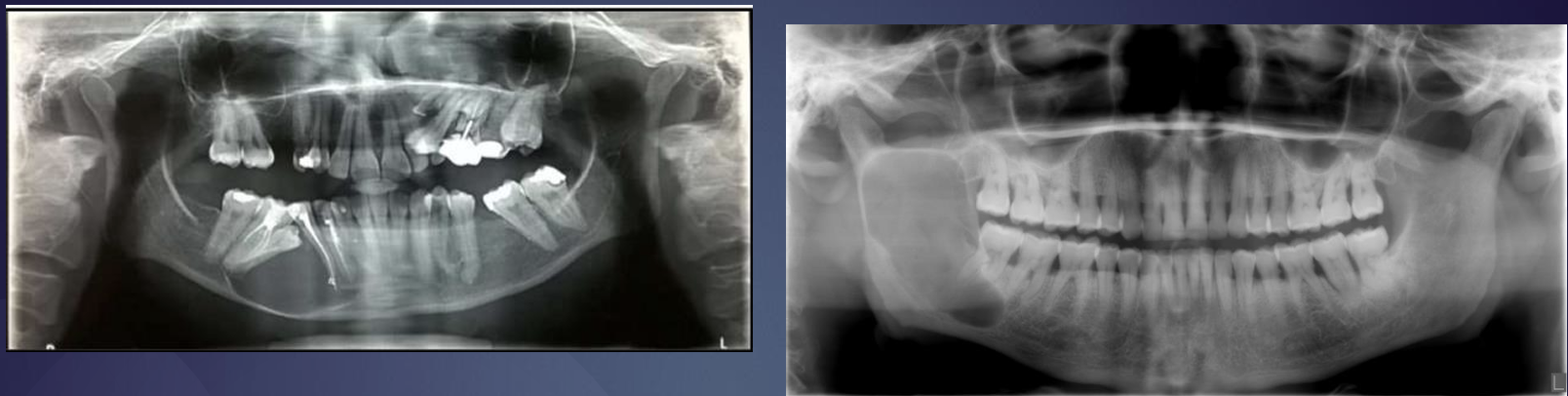
what is this?
residual cyst

what are these?
residual cysts
what is this?
residual cyst
what are the differential diagnoses for residual cysts?
OKC- esp in the maxilla where expansion can be more hydraulic and uniform as opposted to anterio-posterior expansion pattern in mandible, residual cyst has more potential for expansion, OKC is more common in 20-30 y/o and in the posterior body of the mandible
stafne defect- will not grow (static), can occur below IAC
dentigerous cyst
second most common type of cyst in the jaws, associated with the crown of an unerupted tooth
synonyms: follicular cyst
what are the clinical features of dentigerous cysts?
missing tooth, swelling, facial asymmetry, painless unless secondarily infected
what is the location of dentigerous cysts?
most commonly 3rd molars or maxillary canines (supernumeraries, esp mesiodens)
*attaches at the CEJ
can grow to side of the crown rather than directly above it (lateral dentigerous cyst)
maxillary 3rd molar dentigerous cysts can grow into the antra and mandibular ones can extend considerably into the ramus
what are radiographic features of dentigerous cysts?
*epicenter is just above the crown of the impacted tooth
well defined, corticated unless infected
radiolucent with the crown within the lesion
displaces and resorbs teeth, can expand cortical boundaries, IAC displacement (usually inferior), can encroach into the maxillary sinus

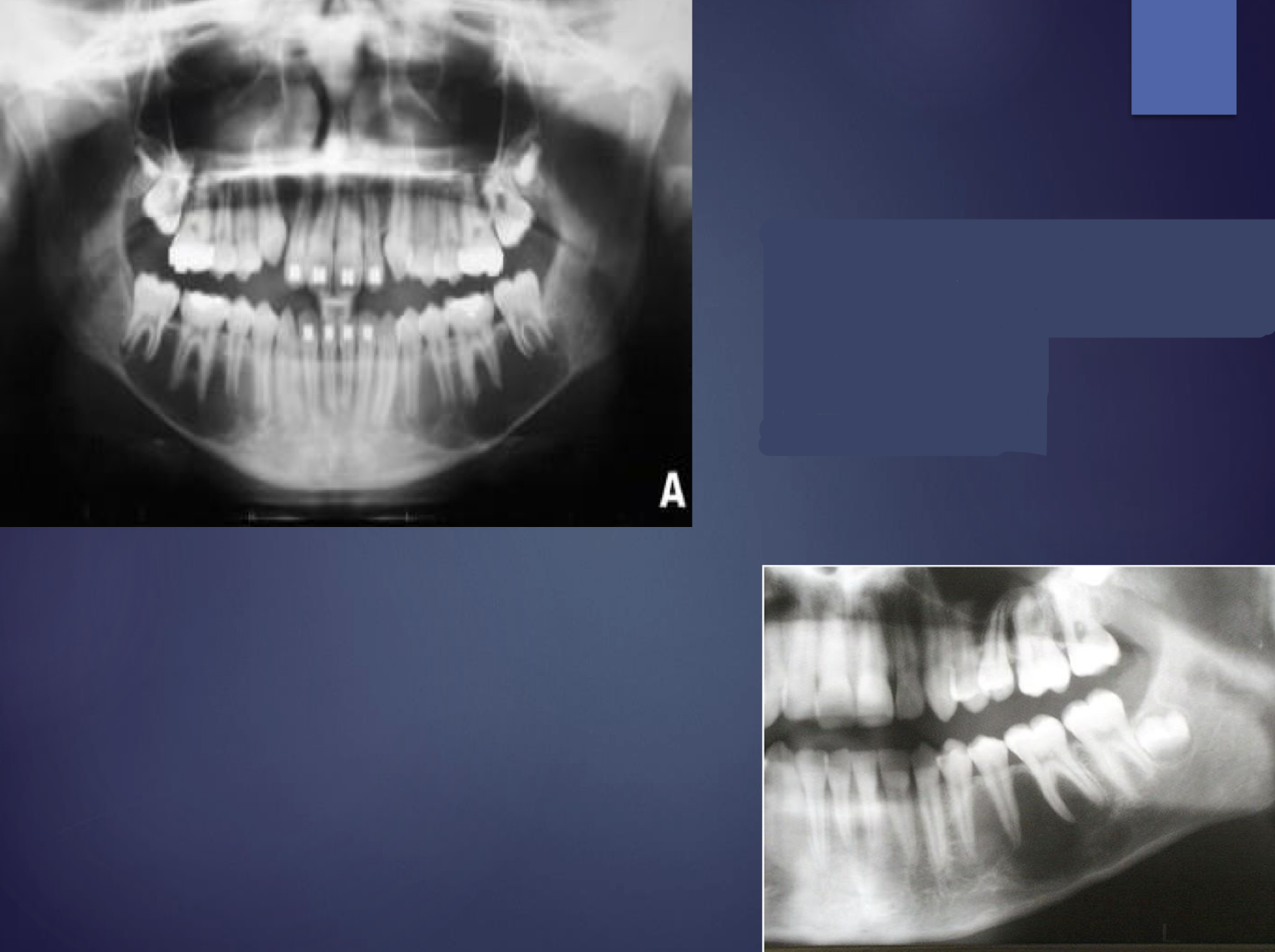
what is this?
dentigerous cyst

what is this?
dentigerous cyst

what is this?
dentigerous cyst
what is this?
dentigerous cyst
what is this?
dentigerous cyst
what are the differential diagnoses for dentigerous cysts?
normal folluclar space (2-3mm), follicular hyperplasia (3-5mm)
odontogenic keratocyst- tends to not enlarge as much as dentigerous cysts
ameloblastic fibroma
unicystic ameloblastoma
adenomatoid odontogenic tumor- uncommon, may have internal calcifications
radicular cysts of primary tooth- can appear in similar pericoronal position in regards to developing permanent tooth
how are dentigerous cysts managed?
yank that tooth
buccal bifurcation cyst
molar may be missing, or have abnormally protruding lingual cusps through the mucosa
*tipping of occlusal table is a key diagnostic feature
1st molar > 2nd molar, rare in maxilla
vital teeth
may have firm buccal swelling
age range of first 2 decades
what are radiographic features of buccal bifurcation cysts?
PDL and lamina dura intact
occasionally bilateral
radiolucent
tipping of the involved molar- root tips are pushed into the lingual cortical plate of the mandible
is large enough it can displace and resorb adjacent teeth and cause a considerable amount of smooth expansion of the buccal cortical plate
if the cyst is secondarily infected, the periosteal new bone formation is seen on the buccal cortex adjacent to the involved tooth
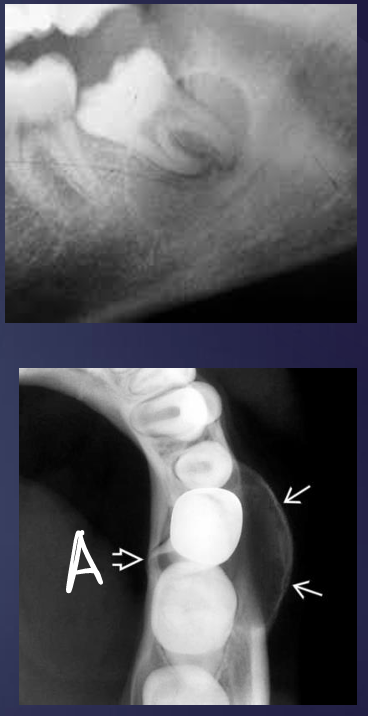
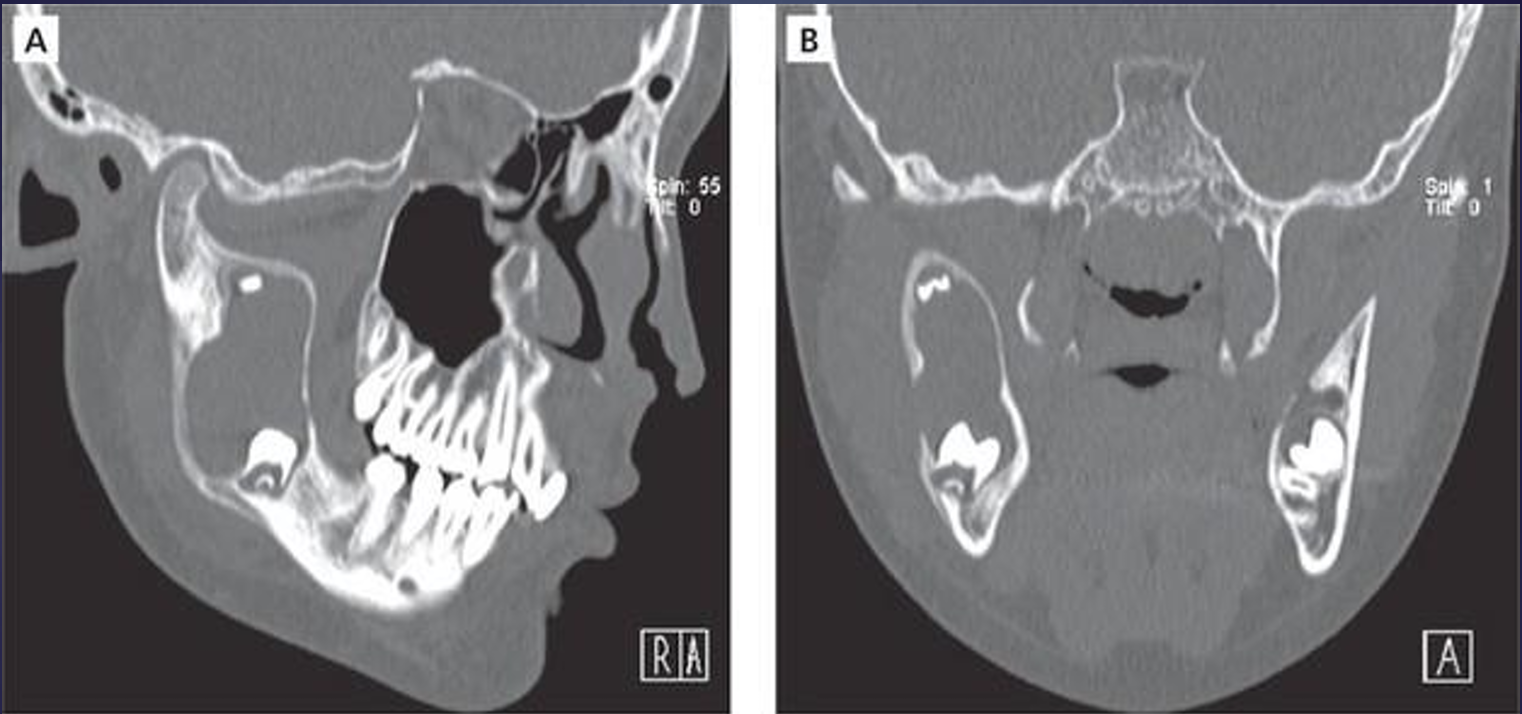
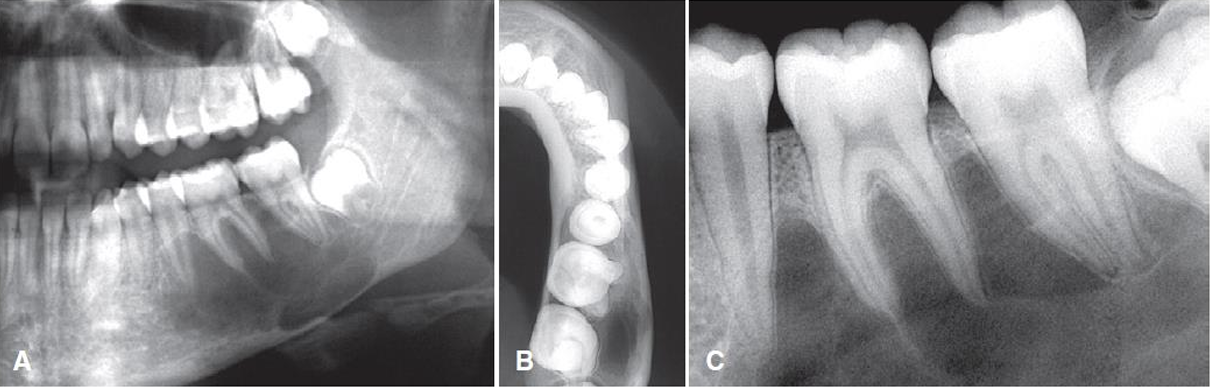
what is this and what is A pointing to?
buccal bifurcation cysts
lingual cortical plate
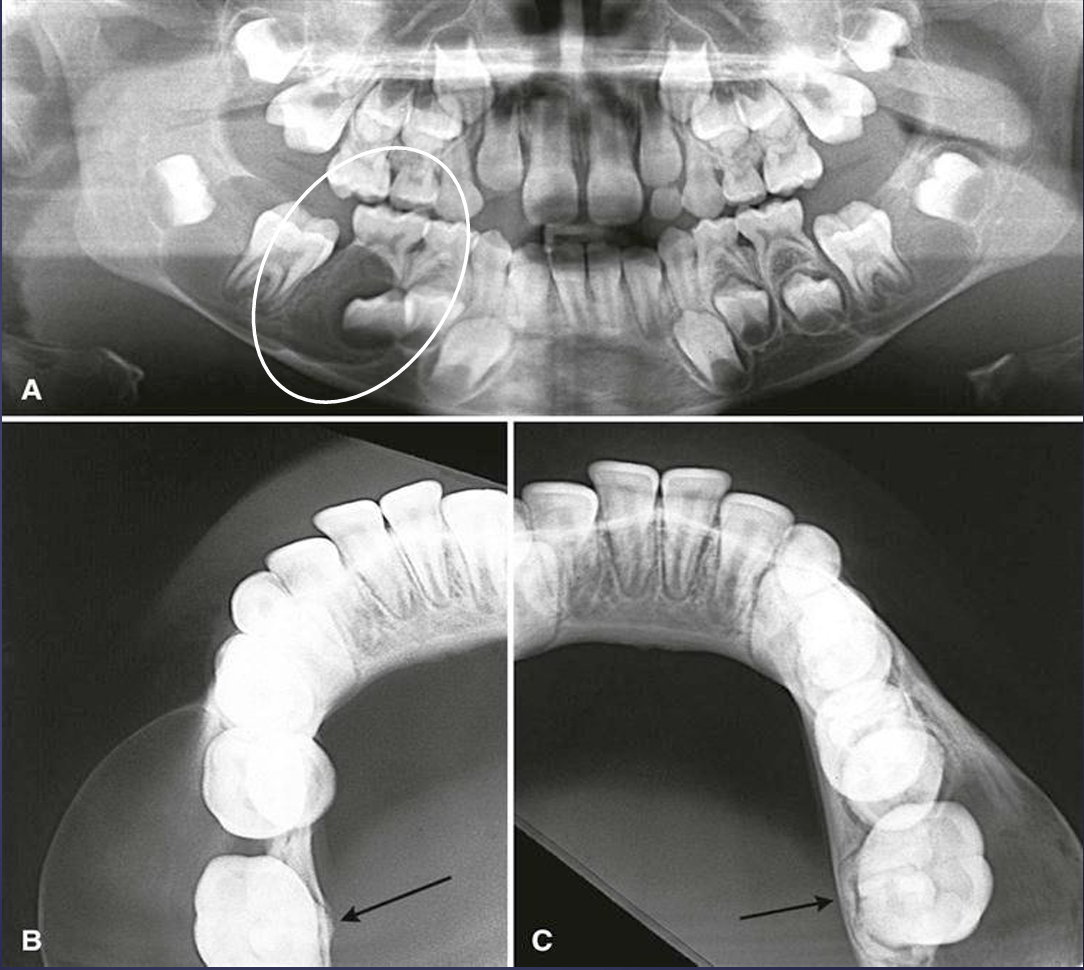
what is this?
buccal bifurcation cyst
what is this?
buccal bifurcation cyst
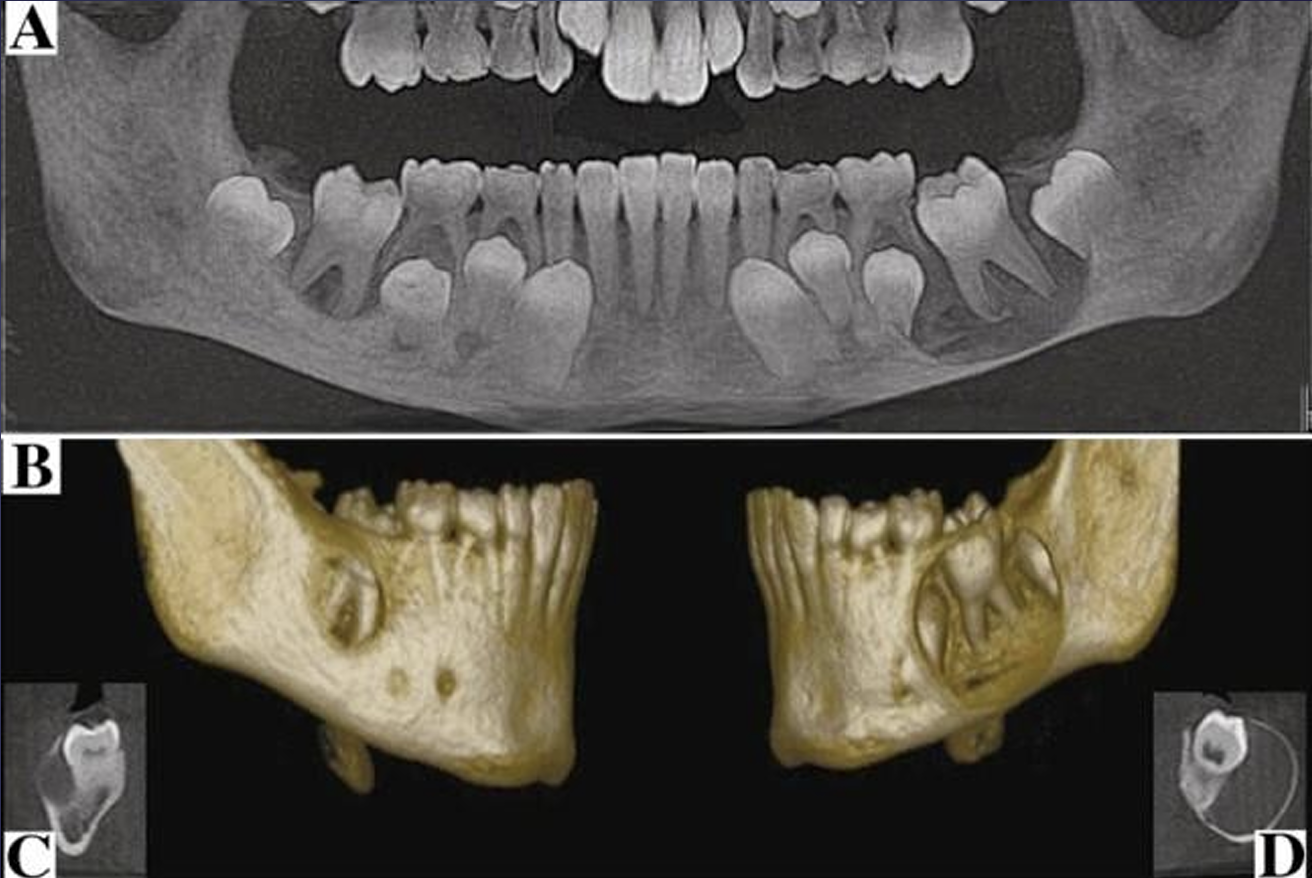
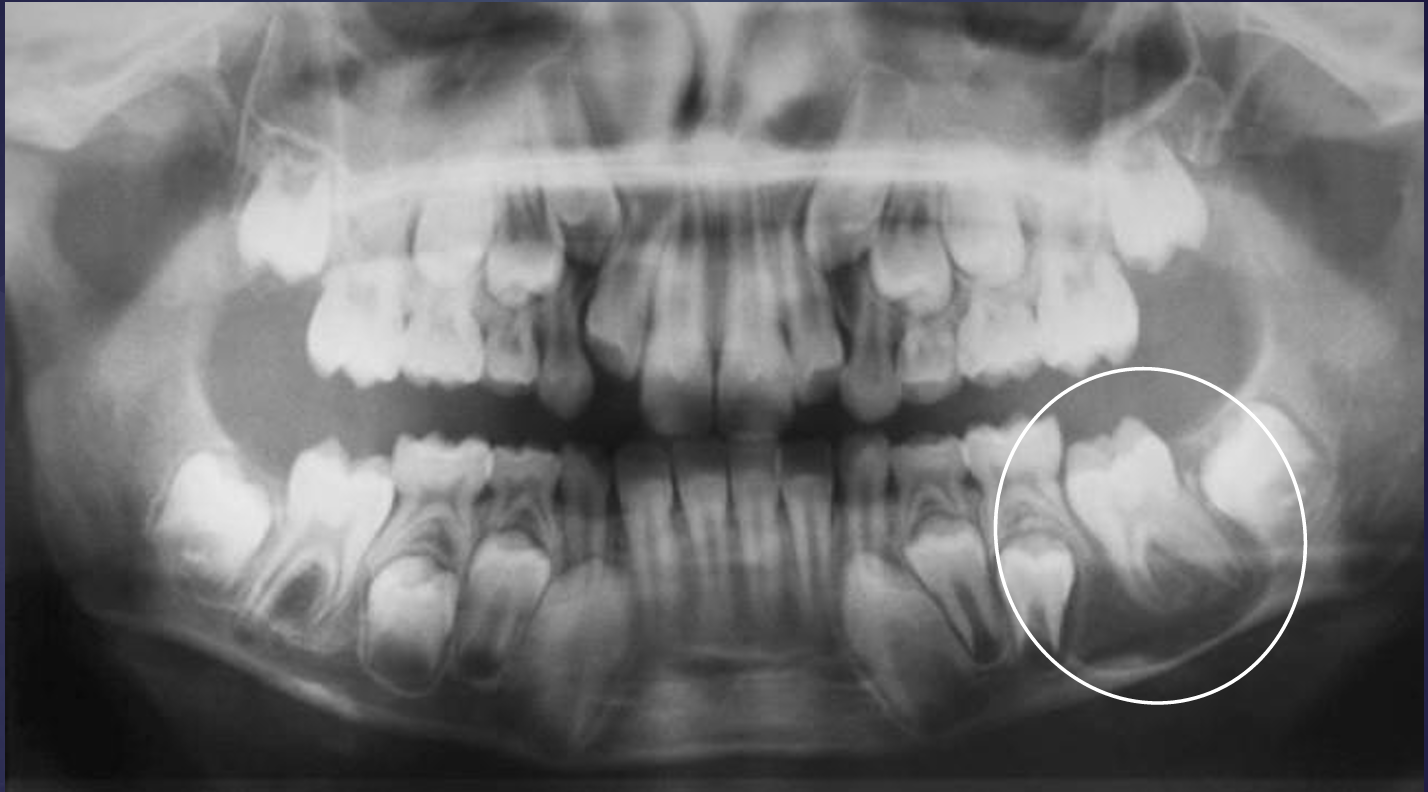
what is this?
buccal bifurcation cysts
odontogenic keratocyst
10% of all cystic jaw lesions
occurs at any age and at all locations
asymptomatic unless secondarily infected
*high recurrence rate due to small satellite cysts or residual epithelium left after removal
aspirations may reveal a thick, yellow, cheesy material (keratin)
what are the radiographic features of odontogenic keratocyst?
located in posterior body of the mandible
well defined unless secondarily infected
corticated, smooth, round/oval shaped or scalloping outline
mostly radiolucent, with occasional radiopacities seen, internal septa
what is this?
odontogenic keratocyst

what is this?
odontogenic keratocyst

what is this?
odontogenic keratocyst
how are odontogenic keratocysts managed?
high recurrence rate- resection, curettage, or marsupialization (basically drain it but suture it so it has a permanent hole in it, don’t look it up)
periodic post-treatment clinically and radiographic examinations to detect any recurrence is recommended
typically every 6 months for first year and then yearly for the next 10 years
*basal cell nevus syndrome
aka gorlin-goltz syndrome, nevoid basal cell carcinoma syndrome
*inherited autosomal dominant
starts to appear early in life, usually after 5 y/o and before 30
what are clinical features of basal cell nevus syndrome?
OKC’s appear in multiple quadrants and earlier in life than solitary OKCs
high recurrence rate
skin lesions- small, flattened, flesh colored or brown papules occurring anywhere on the body but especially prominent on the face/neck/trunk
skeletal anomalies include bifid rib (most common)
calcification of the falx cerebri
what is the differential diagnosis for basal cell nevus syndrome?
cherubism
what are common characteristics (not all dental) of patients with basal cell nevus syndrome?
skin growths, jaw cysts, elevated scapula, chest/pectus deformity, enlarged head circumference, syndactyly, pitting of soles/palms, spine misalignment
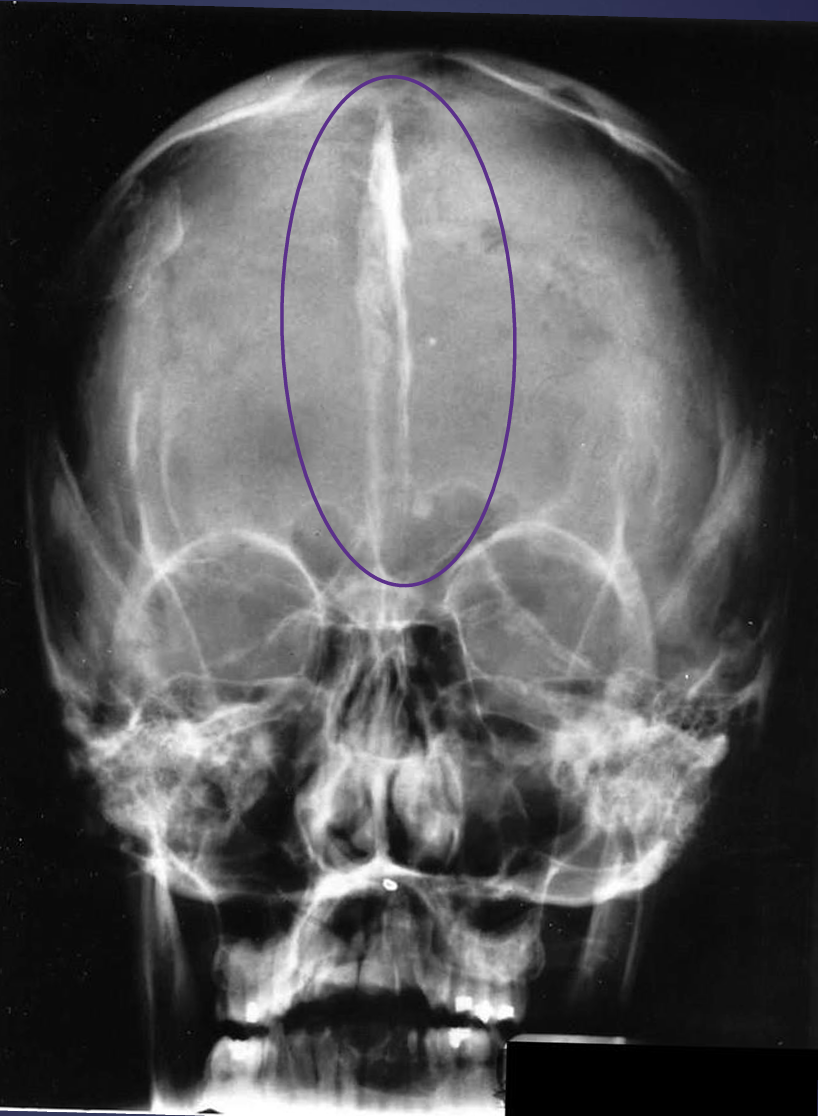
what’s going on here?
calcified falx cerebri- potentially basal cell nevus syndrome
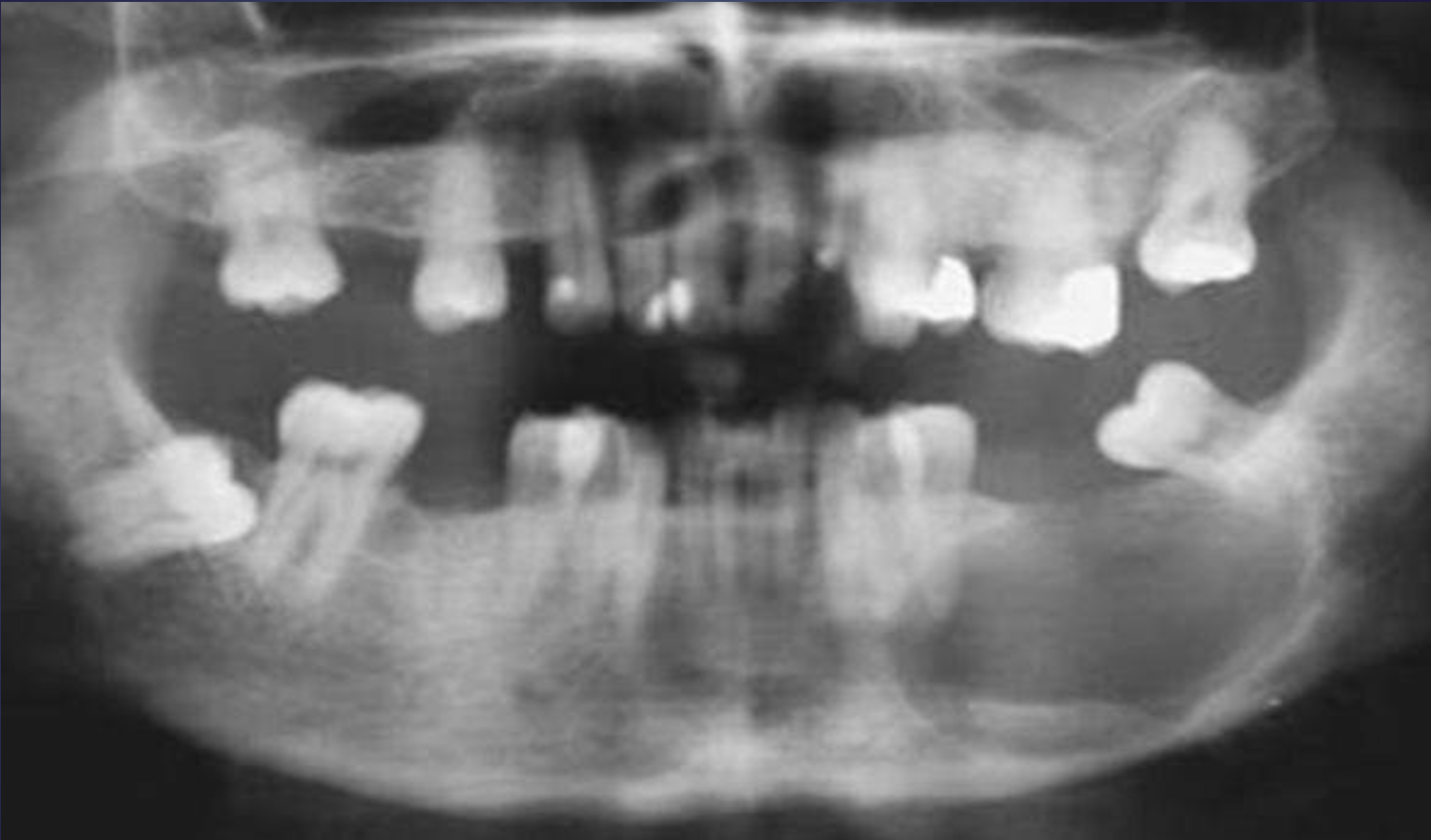
what is this?
basal cell nevus syndrome
lateral periodontal cyst
usually asymptomatic and less than 1cm in diameter
no sex or age predilection
vital tooth
if these cysts become secondarily infected, they mimic a lateral periodontal abscess
what are the radiographic features of lateral periodontal cysts?
50-75% in mandible
<1cm with round/teardrop shape
well defined radiolucency with a prominent cortical boundary and a round or oval shape
internal aspect is radiolucent
small cysts may efface the lamina dura of the adjacent root
large cysts can displace adjacent teeth
large cysts have similar growth pattern to OKC (minimum expansion)
how are lateral periodontal cysts managed?
excision
what is this?
lateral periodontal cyst
what are these?
lateral periodontal cysts
what are the differential diagnoses for lateral periodontal cysts?
small odontogenic keratocyst- OKC may have a more aggressive pattern of enlargement
simple bone cysts- scalloped between roots
lateral radicular cyst- non-vital tooth
small neurofibroma
mental foramen
glandular odontogenic cyst
cyst derived from odontogenic epithelium with characteristics of salivary gland features- mucus producing
aka sialo-odontogenic cyst
aggressive behvaior with recurrence
what are the radiographic features of glandular odontogenic cyst?
most common in anterior mandible and in maxilla
usually a cortical border that may be smooth or scalloped
both unilocular and multilocular appearances of this cyst have been reported
expansion of the outer cortical plates of the jaws with regions of perforation through the cortex has been reported
displacement of teeth is a common feature
what is this?
lateral peridontal cyst
what is this?
glandular odontogenic cyst

what is this?
glandular odontogenic cyst
what is this?
glandular odontogenic cyst
what is this?
glandular odontogenic cyst
what are the differential diagnoses for glandular odontogenic cyst?
ameloblastoma
OKC- younger age group
CGCG- younger age group
central mucoepidermoid carcinomas
how are glandular odontogenic cysts managed?
high rate of recurrence; aggressive treatment, including resection may be considered
follow up with periodic radiographic examinations to assess for recurrence
nasopalatine duct cysts
well defined, corticated, and is circular or oval in shape
shadow of the nasal spine may superimpose on the cyst, giving it a heart shape
usually totally translucent- rarely may have internal dystrophic calcifications, which may appear as ill-defined, amorphous, scattered radiopacities
PDL and lamina dura intact, rare for root resorption or root displacement
the cyst may expand in to the labial cortext and the palatal cortex
the floor of the nasal fossa may be displaced in a superior direction
what is this?
nasopalatine duct cyst
what are the differential diagnoses for nasopalatine duct cyst?
large nasopalatine fossa/foramen- typically non corticated, compare with prior or future images
periapical or residual cyst- non vital teeth
CGCG- younger age group, more common in mandible
dentigerous cyst of impacted mesiodens
adenomatoid odontogenic tumor

what is this?
nasopalatine duct cyst
what is this?
nasopalatine duct cyst
what is this?
nasopalatine duct cyst
what is the management of nasopalatine duct cyst?
enucleation, preferably from the palate to avoid the nasopalatine nerve and biopsy
recurrence 2%, paresthesia <10%
if uncertain as to if there is a cyst, can make serial radiographs in ~6 mo to assess for enlargement
nasolabial cyst
aka nasoalveolar cyst
unknown origin
unilateral swelling of the nasolabial fold, pain, or discomfort may be there
soft tissue cyst
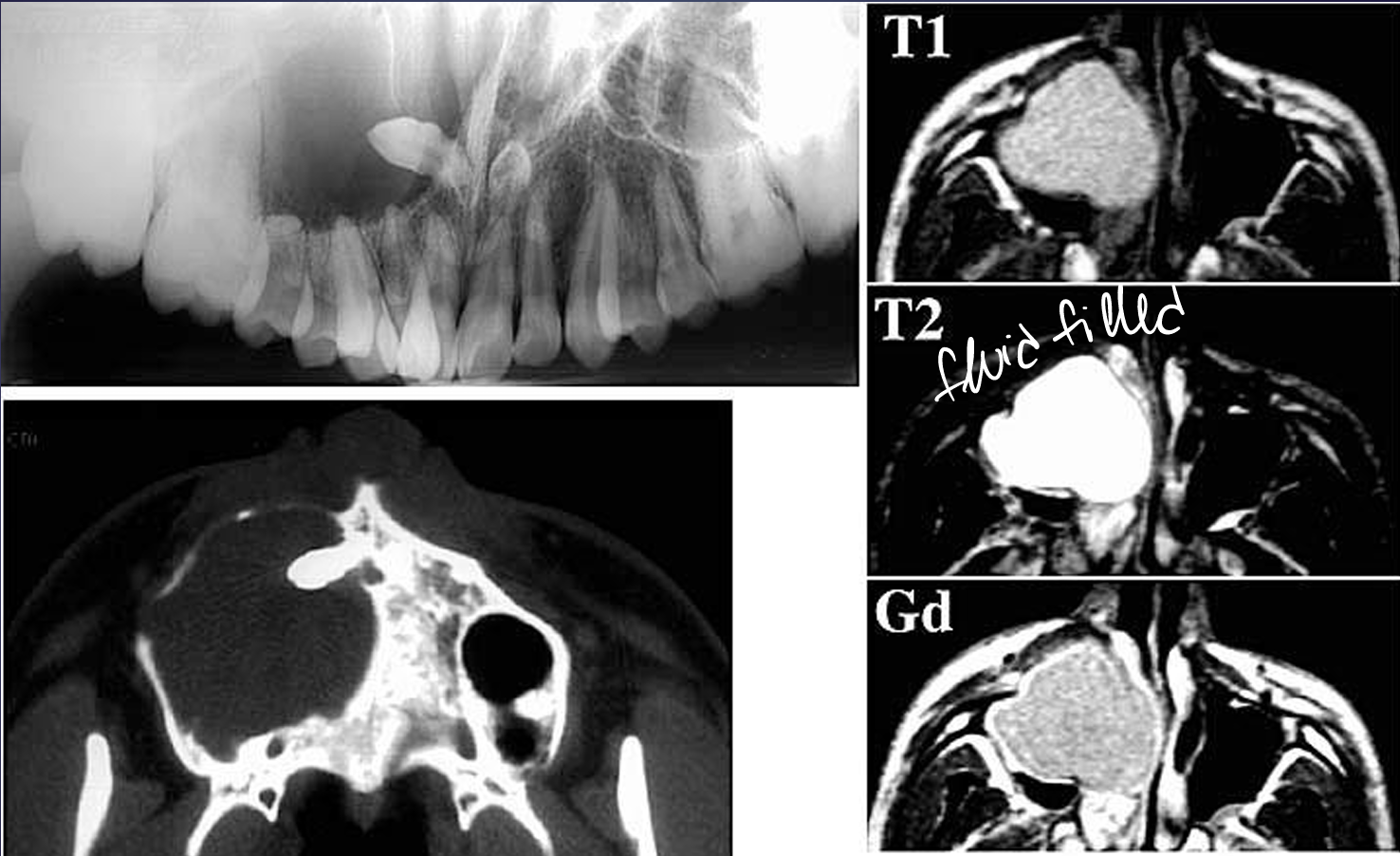
what are radiographic features of nasolabial cysts?
soft tissue lesions seen apical to incisors, best modalities to image are CT or MRI
circular or oval with peripheral enhancement with contrast
homogenous in relation to the surrounding soft tissue
can cause erosion of the underlying bone
what are the differential diagnoses of nasolabial cysts?
nasal furuncle, mucous extravasation cyst or cystic salivary adenoma
what is this?
nasolabial cyst
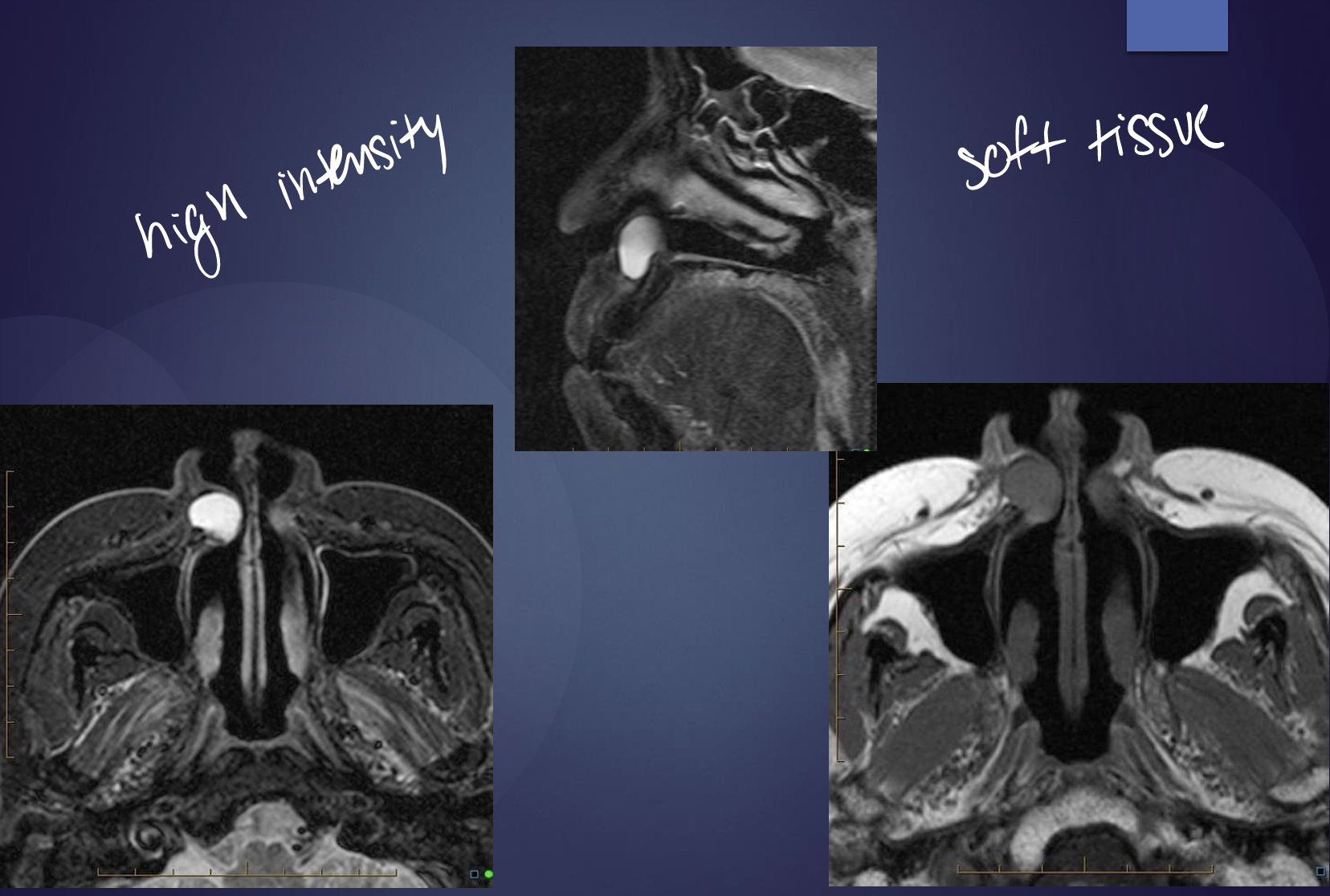
what is this?
nasolabial cyst
simple bone cavity
no epithelial lining- not a true cyst
>males ~17, >females ~42 w pain or tenderness
*w > cemento-osseous dysplasia
aka traumatic bone cyst, hemorrhagic bone cyst, solitary bone cyst
what are imaging features of simple bone cavity?
borders vary from a well defined, delicate cortext to an ill-defined border without a cortext that blends into the surrounding bone
the shape most often is smooth and curved, similar to a cyst, with an oval or scalloped border
internal structure is radiolucent
it may appear multilocular although the lesion does not usually contain true septa
*no effect on surrounding teeth!
lamina dura intact or only partially disrupted
SBCs also have a tendency to grow along the long axis of the bone, causing minimal expansion
what is this?
simple bone cavity

what is this?
simple bone cavity
what is this?
simple bone cavity
what are the differential diagnoses of a simple bone cavity?
odontogenic keratocyst- resorbs and displaces teeth
diagnosis primarily relies on radiographic and surgical observations- at biopsy usually open lesion to reveal hollow non-lined cavity
what is the management of simple bone cavity?
a conservative opening into the lesion and careful curettage of the lining- this usually initiates bleeding and subsequential healing
spontaneous healing has been reported
periodic radiographic examinations are advisable, esp if the pt declines treatment
these lesions can recur but rare

what is this?
stafne defect

what is this?
stafne defect