antimicrobial pharmacology
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
what are antibiotics
evolved by bugs to fight each other
hijacked by man and now an arms race - resistance develops, new substances evolve
Man has synthesised new versions and developed ways to block resistance
Bugs fight back
More use = more selection pressure = more resistance
some are completely synthetic = completely chemical synthesised
substance produced by bugs/plants which are then modified to alter properties
pharmokinetics
action of animal on drug
pharmacodynamics
action of drug on animal
antibiotics = on the bacteria
mechanism of action
aim to prevent growth and/or survival of invading organisms while causing minimal damage to host
using specific pathways that a mammal doesn’t have so doesn’t kill a mammal
selective toxicity = magic bullets
tend to target receptors or pathways unique to prokaryote cells
how do antibiotics work
distrupt cell wall production or function
beta-lactams, penicillins, cephalosporins
distrupts cell membrane function
ionophores
distrupts DNA function
potential sulphonamides, fluroroquinolones, aminocoumarins
distrupt protein synthesis
aminoglycosides, tetracyclines, macrolides, florphenicol
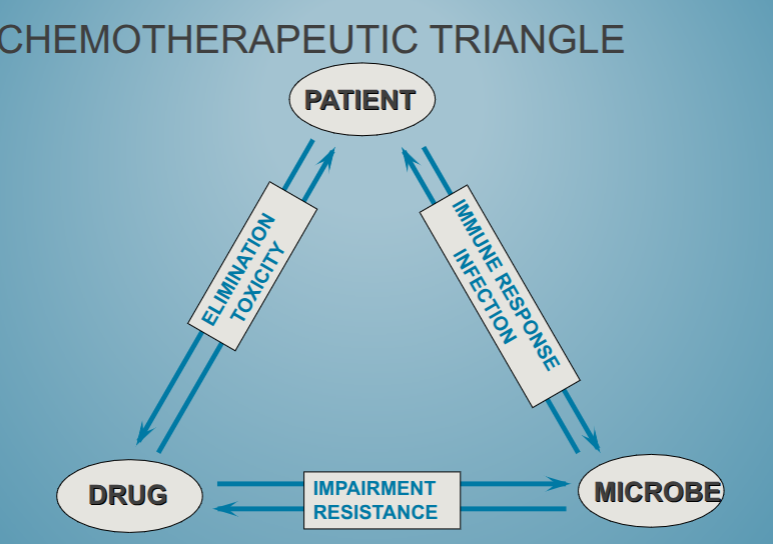
chemotherapeutic triangle
antibiotic classifications
how they affect bacteria - bacteriostatic or bacteriocidal
range of bacteria they affect
post-antibiotic effect
whether they are concentration or time dependent in how they kill bacteria
chemical structure and properties e.g molecular size, lipid solubility
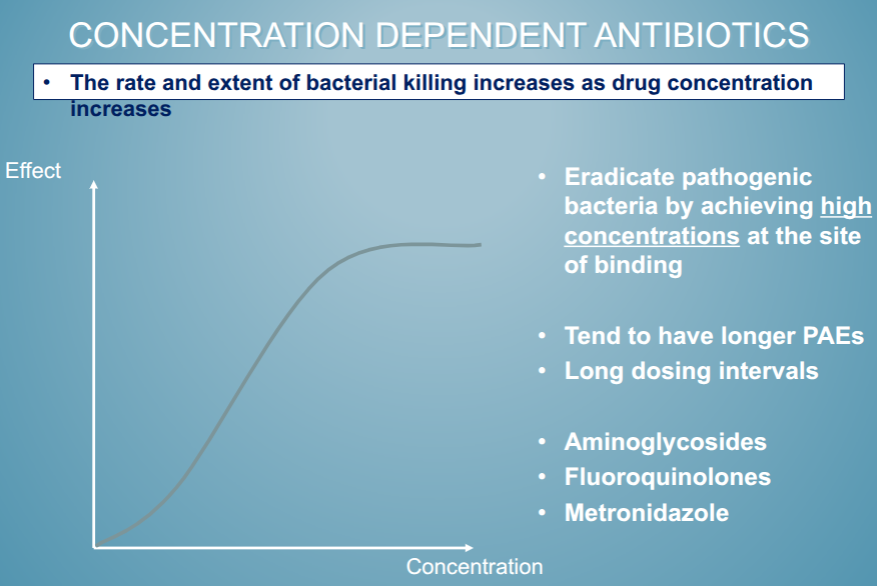
Depend on concentration
Gentamicin can be static, but cidal at 2-4x higher concentration
Tetracyclins would be toxic given at bacteriocidal concentrations, so used at static dose.
Bacteriostatic may have a slow onset of “action” and require good host immune response as the drug do not clear the infection, the body does.
Should not give static drugs with cidal, as many cidal drugs require active growing cells. Will only get the static action.
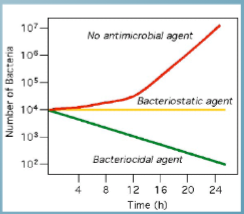
bacteriostatic antibiotics
antibiotics that prevent replication but don’t kill susceptible bacteria
number of organisms will stay the same
e.g tetracyclines, macrolides, sulphonamides alone
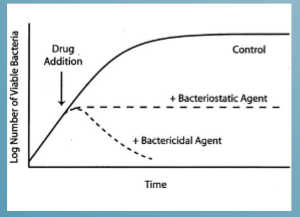
bacteriocidal
antibiotics that kill susceptible bacteria
number of organisms will go down
e.g fluroquinolones, B-lactams, trimethoprim, potantiated sulphonamides
spectrum of activity
broad spectrum
no need to diagnose
select for resistance in wide population of organisms
narrow spectrum
greater chance of failure
will not select for resistance in enteric gram -ve organisms when treating gram +ve disease
penicillins = narrow spectrum
fluroquinolones = broad spectrum
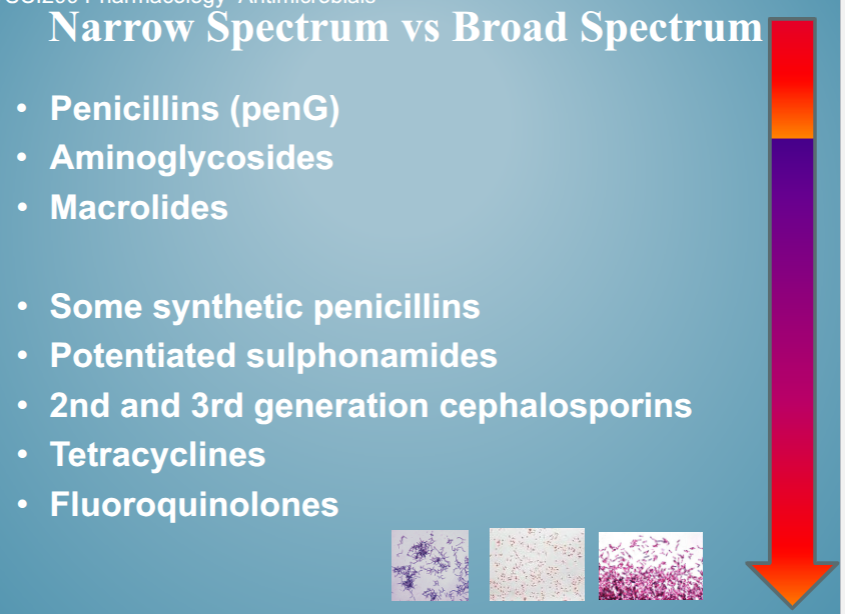
broad vs narrow spectrum
empiric therapy
infecting organisms not yet identified
more broad spectrum use
definitive
organisms identified and specific therapy chosen
more narrow spectrum
prophylactic (preventative)
prevent an initial infection or its recurrence after infection
currative treatment
treatment of sick animal or group of animals following diagnosis of infection and/or clinical disease
prophylactic treatment
veterinary medicines regulations 2024
Prophylactic use is defined as =
‘the administration of a medicinal product to an animal or group of animals before clinical signs of disease in order to prevent the occurrence of disease or infection.’
Clinical signs of disease include visible outward signs of disease as well as sub-clinical disease detected through laboratory testing, for example, somatic cell counts in milk and/or other pathology testing
routine use as - repeated, habityal use such as treating every batch of animals without attempts to reduce ongoing use of sntibiotics and/or without a proper evidence/ risk based assessment to determine whether antibiotic use is necessary
mataphylaxis treatment
Metaphylaxis treatment – which is mostly equivalent in human
medicine to “group prophylaxis”
“means the administration of the veterinary medicinal product to a group of animals after a diagnosis of clinical disease in part of the group has been established, with the aim of treating the clinically sick animals and controlling the spread of the disease to animals in close contact and at risk and which may already be sub-clinically infected
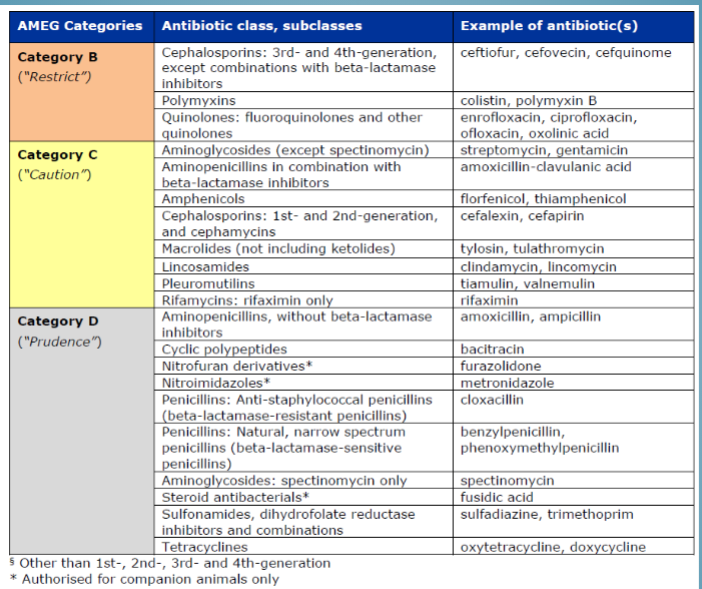
antibiotic classes and examples of antibiotics
try to use class D
how long does it need to be there for
mode of action
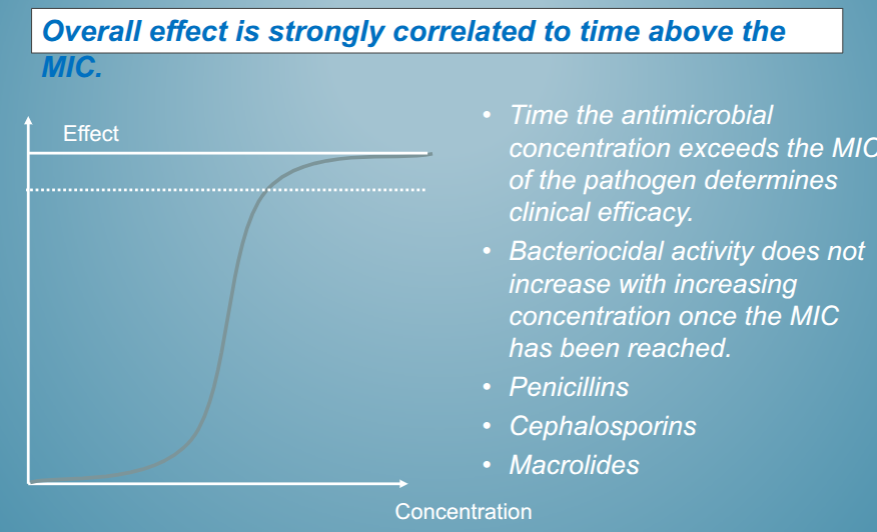
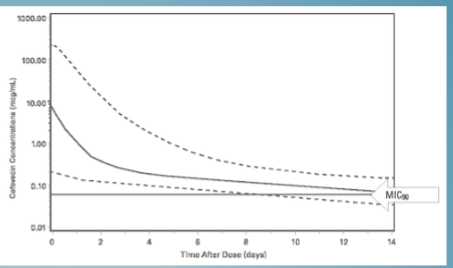
time over MIC(minimal inhibitory concentration) dependent - peniclinis, cephalosporins, tetracyclines, macrolides
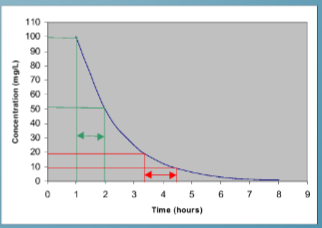
concentration dependent - aminoglycerides
area under curve dependent - fluroquinolones
ratio of plasma to tissue distrubution may not matter as long as enough gets to where it is needed - judged by MIC of organism
post-antibiotic effect - PAE
the ability of a drug to suppress or kill bacteria after the drug concentration has dropped below the MIC
highly dependent on antimicrobial and the pathogen
concentration dependent antibiotics
plateaus when you have maximium amount of antibiotic that you need
time dependent antibiotics
have to get it over a certain concentration for a certain amount of time
if you don’t then you have no effect
systemic availability of the drug
dosage
route of administration
dosing rate - some need to be spread out across multiple sites to work
access to site of infection
injectables
used for treatment of severe infections
may depend on availability and toxicity
advantages
used for drugs poorly absorbed, inactive or inefective if given orally due to action of GI tract - poor blood supply, immunocompressed, dehydrated, GI infection
IV route provides immediate onset of action and may get higher initial concentrations depending on tissue
IM and SC routes may slow or delay onset of action - but can stay for longer
client training and compliance to give injection
disadvantages
can be painful
cost
aseptic technique required
side effects - higher initial concentration in heart and other tissues
must be soluble prep
needle stick injury, sharps disposal safety and cost
intravenous administration
total dose enters systemic circulation
high concentration quickly declines
high concentration gradient from plasma to tissue
Drug molecules penetrate cellular barriers and enter cells via passive diffusion
Physiochemical properties, lipid solubility, degree of ionization (weak acids/bases) determine concentration obtained in the tissues, transcellular fluids (CSF, synovial and ocular) and glandular secretions (milk, saliva, prostatic)
Often in the form of a salt (pH varies) at high concentration = IV preparations must be given slowly or via infusion
route of administration
IM or SC
absorption following injection
formulation of drug - concentration is important
vascularity of injection site - lateral neck preffered site in large animals - consider scaring and meat quality
physiochemical properties
>20ml volumes should not be used in one site of a cow
rapidly absorbed with peak plasma levels ~1hr
route of administration - injectables
IM or SC
withdrawl periods
varies with formulation of drug and between animal species due to metabolism
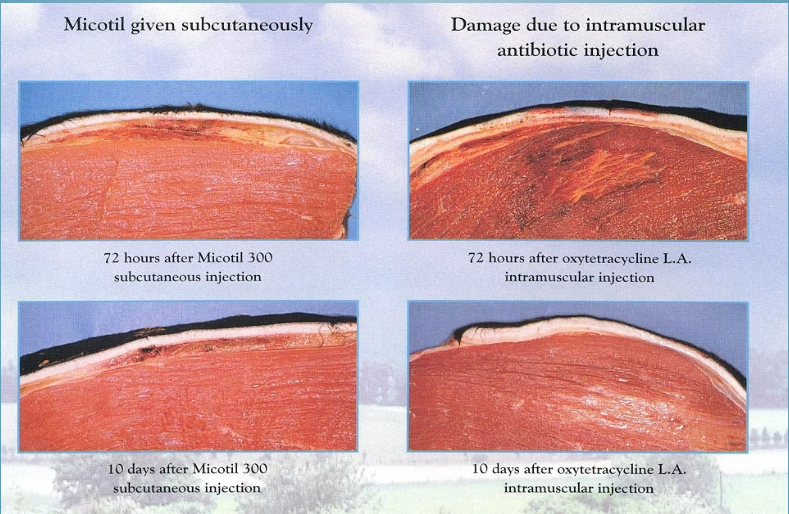
parental preps should be formulated to not cause local tissue damage when given IM = tissue damage may lead to persistence of drug residues, hide damage
tissue damage at injection site
route of administration - oral administration
lots of dosage forms - incl medicating water and feed
dissolution will dictate rate of drug absorption
monogastric versus ruminants - diluted rumen and may be metabolised by organism/ select for resistance/kill them
systemic availability
fraction of dose which reaches systemic circulation unchanged - bioavailability
influenced by - stability in gastric contents, susceptibitlity to inactivation, physiochemical properties(passive diffusion across epithelial barrier)
drugs then go into hepatic portal venous blood to liver which is main organ for drug metabolism
metabolism of drug before it reaches systemic circulation
pre-systemic metabolism = 1st pass effect
gut lumen - bacterial
mucosal epithelium
liver
effect of liver blood flow and metabolic rate
important for activating some drugs
other factors
presence of food or binding to food can affect it
decreases systemic availability for following drugs - most penicillins, oral sephalosporins, trimethroprim/sulphonamide combinations, tetracyclines
doxycycline and erythrocoplasmacin systemi availability increased after food in dogs
in horses systemic availability for drugs decreased by feeding therefore recomended to not feed for up to 2 hrs following administration
drug distribution systemically
determined by blood flow to tissues
ability to penetrate cellular barriers
rate is dependent upon
perfusion - lipophilic drugs - fluroquinolones, macrolides, lincosamides
diffusion - ionised or polar drugs
binding of drug to plasma protein also limits immediate availability
selective binding e.g aminoglycerides to phospholipid rich inner ear and kidney cortex tissues = small fraction of total drug but can result in toxicity
volume distribution
= reflection of amount left in blood stream after drug has been absorbed
if drug held in blood stream it will have a small volume of distribution
if very little drug remains in blood stream has a large volume of distribtuion
plasma protein binding
can affect
tissue penetration
volume of distribution
half-life
elimination
reduces free fraction of drug available for bacterial killing
reveraible
PP binding important for some drugs and allows them to be long acting - good for B-lactams
cefovecin ~97% PP binding in dogs and 99% in cats
excreted unchanged in urine - only unbound fraction
halflife of antimicrobials
time required for plasma concentration to half after reaching pseudo-equilibrium distribution
The larger the volume of distribution, the longer it takes to clear the drug, at a constant rate of clearance
important for dosing intervals
synergism
= potentiation of 1 drug action by another
may be due to preventing drug metabolism or blocking bacterial metabolism in different ways
concentration deendent
do pharmo-kinetics match in theses species
phase of bacterial of bacterial life cycle when active
growth
biofilms
possible antagonism if concentrations wrong
inhibition of L-form to enable activity
they have just a cell membrane and no cell wall
half life vs clearnace
clearance = ability to eliminate drug
half-life - overall elimination during terminal phase which depends on both clearance and distrubtuion
drug elimination
various routes by which drugs can be eliminated
most important = kidney, liver
less important = bile, sweat, milk, faeces for oral antibiotics with poor absorption
drug clearnace
most drugs are cleared from plasma in 2 ways by metabolism in liver and by being eliminated(unchanged) through kidneys
fraction unchanged(fu) represents the proportion cleared by kidneys while 1-fu represents fraction cleared by metabolism
drug elimination via liver
depends on
blood flow to liver
activity of enzyme in liver - influenced by milk yield or work animal is doing
liver enzymes will chemically alter the drug to form metabolites which may
inactivate
equally or more active than the parent
Metabolites are eventually eliminated via the kidney as they are usually more water soluble
Factors which may reduce elimination via the liver
elderly have poorer blood flow
neonates have a low liver enzyme activity
some drugs reduce liver enzyme activity
extensive liver damage (cirrhosis, liver fluke)
antibiotics mechanisms of action
cell wall inhibitors - penicillins, cephalosporins, polymixins, bacitracin
protein synthesis inhibitors - aminoglycerides, macrolide, tetracyclines
DNA metabolism - sulfonamides, potentiated sulfonamides, fluroquinolones, metronidazole
penicillins classes of agents
1. Natural: penicillin G, penicillin V
2. ß-Lactamase Resistant: cloxacillin
3. Aminopenicillins: amoxicillin, ampicillin
4. Extended Agents: ticarcillin, carbenicillin
5. Augmented Agents: amoxicillin + clavulanate
penicillins common properties
1. cleared by kidneys (filtered + tubule transport)
2. does NOT enter CNS (meningitis)
3. weak acids; 50% plasma protein bound
penicillins side effects
Immune-mediated reactions: autoimmune haemolytic anemia and immune-mediated thrombocytopenia (Type II hypersensitivities), anaphylaxis (Type I hypersensitivity).
Procaine reactions (e.g. CNS stimulation). hyperexcitability , muscle tremors, ataxia, apnea and cardiac arrest. No treatment.
Can inhibit protein binding or renal excretion of other acidic drugs