Renal Anatomy and Absorption Control
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
kidneys
pair of retroperitoneal organs that filter waste from the blood
stones can manifest as back pain
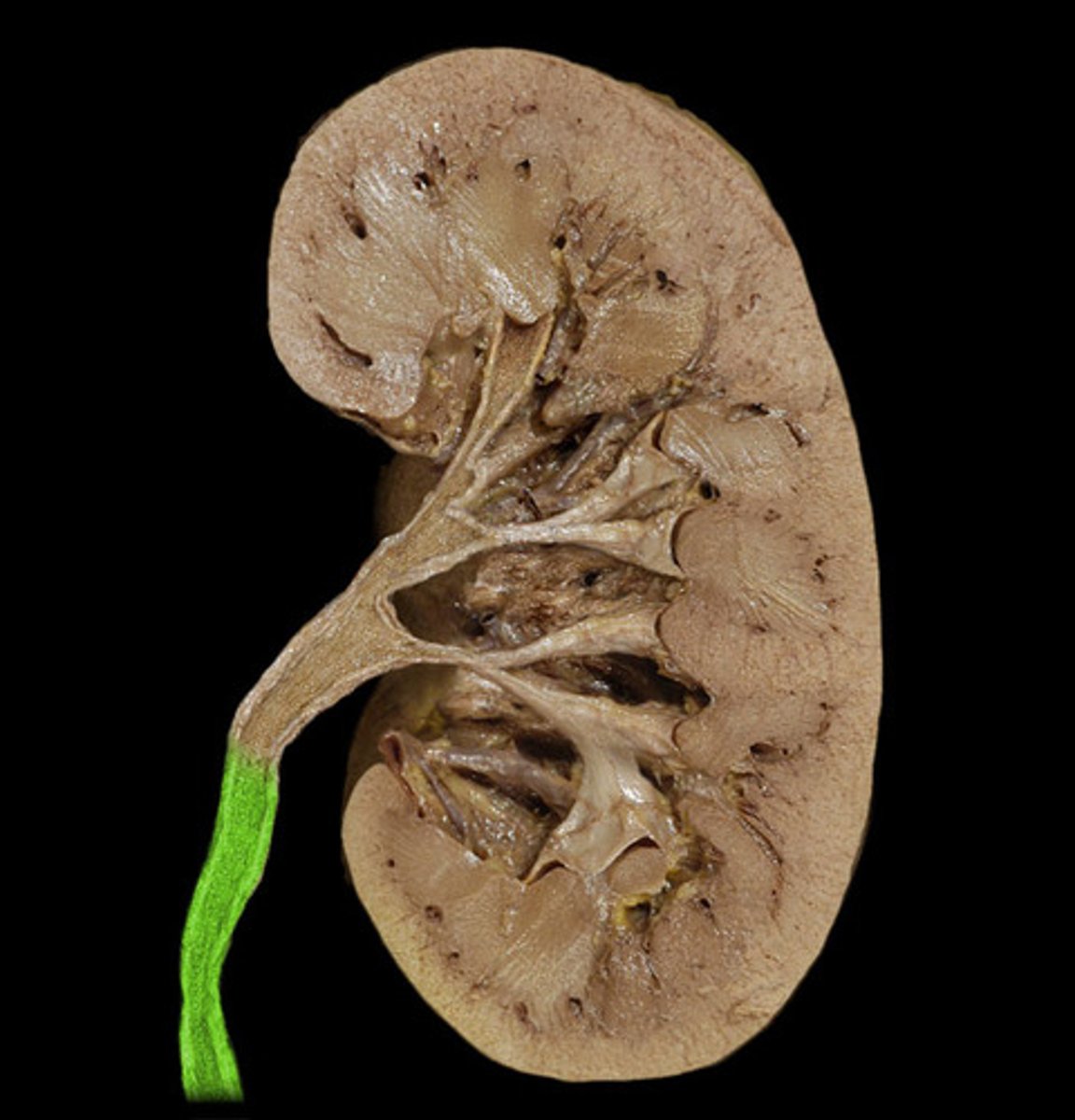
ureter
tube that carries urine from the kidney to the urinary bladder
urinary bladder
temporarily stores urine
urethra
tube that carries urine from the bladder to the outside of the body for excretion
excretion: metabolic end products, drugs, and other exogenous compounds
regulation: filtering blood → regulates essential substances like ions, osmolarity, pH, arterial BP (homeostasis by selectively absorbing/secreting and altering their concentrations)
secretion: renin, EPO, and activates vitamin D
what functions is the urinary system responsible for?
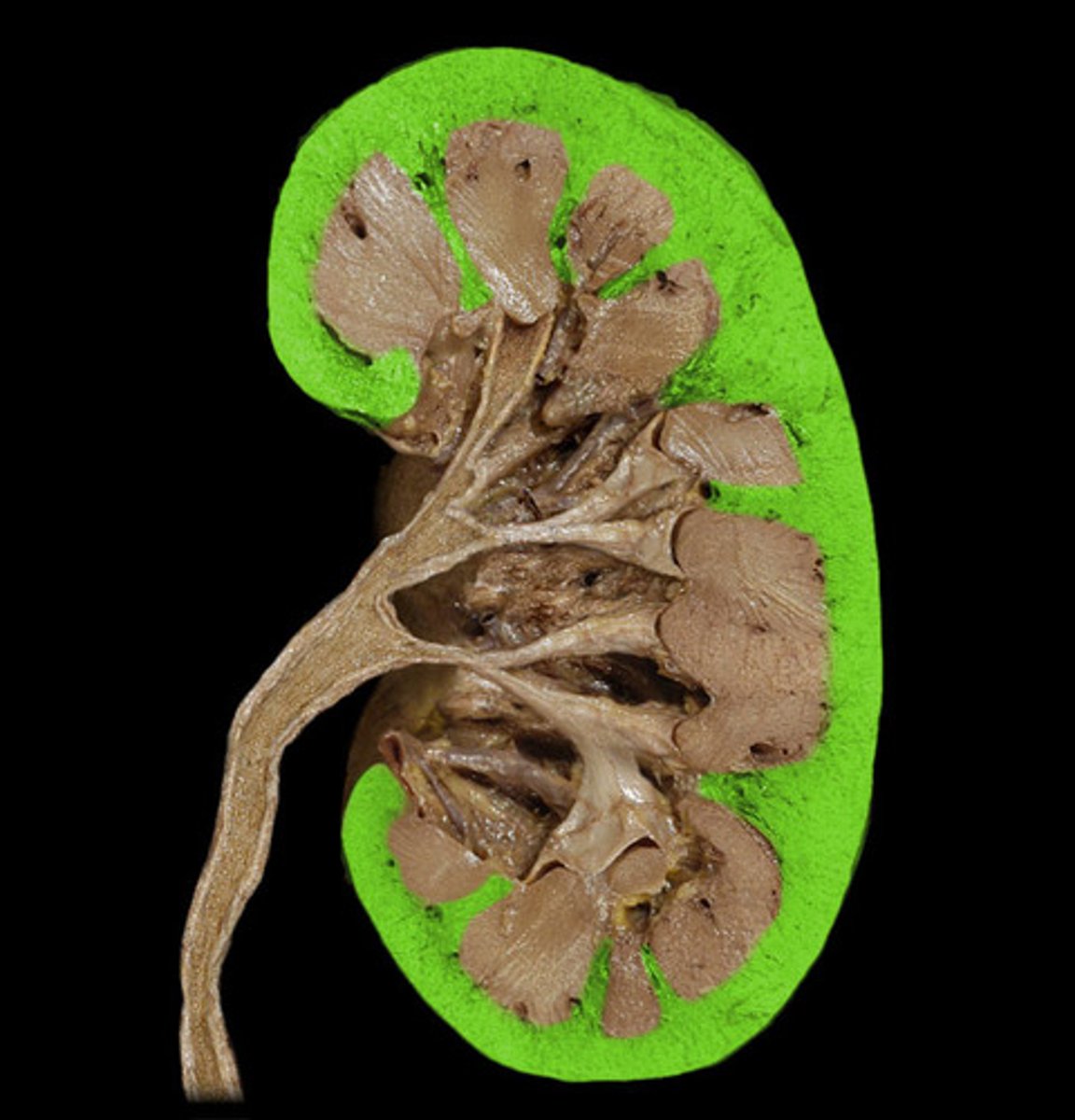
cortex
outer layer of the kidney
medulla
inner part of the kidney

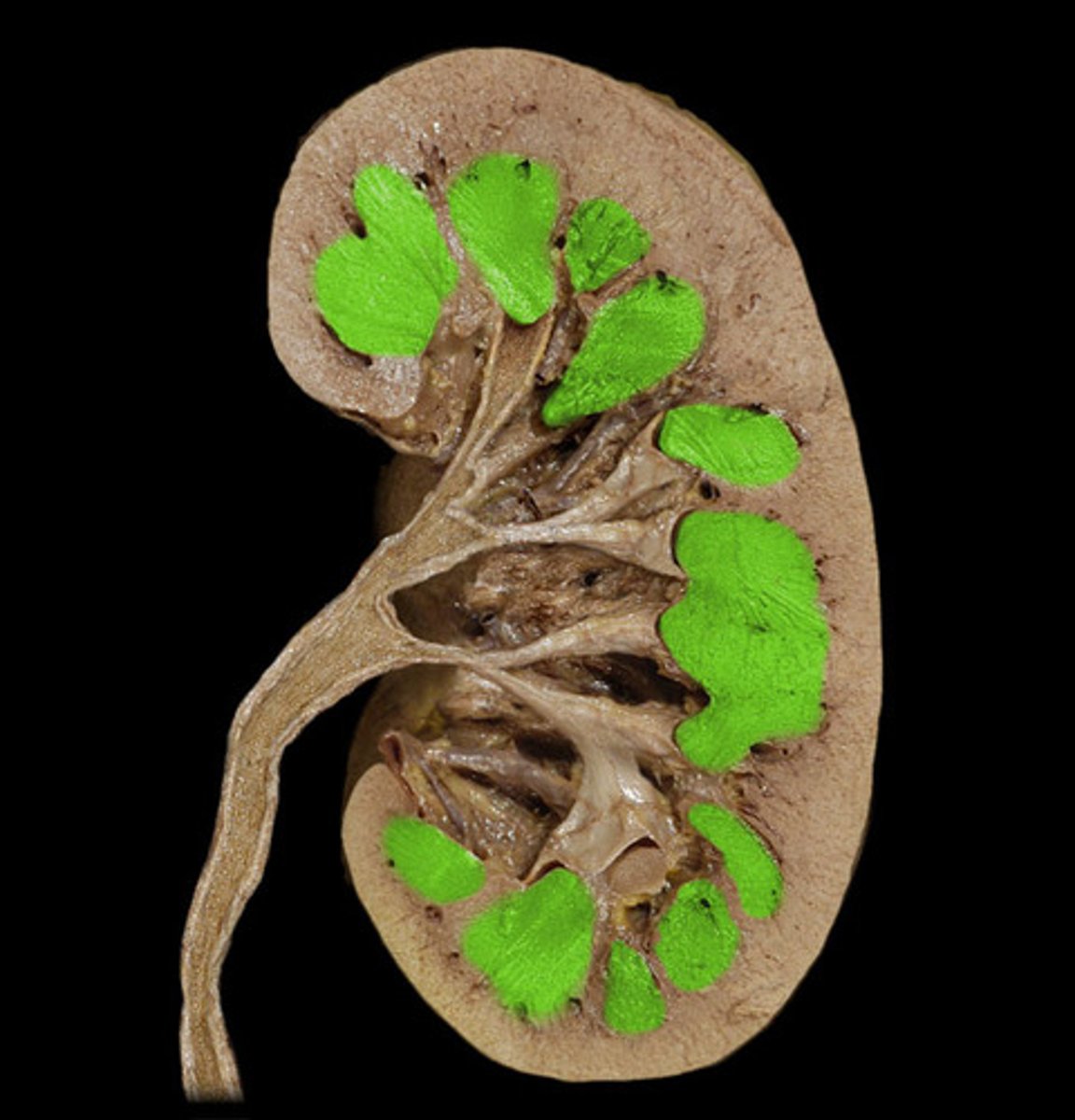
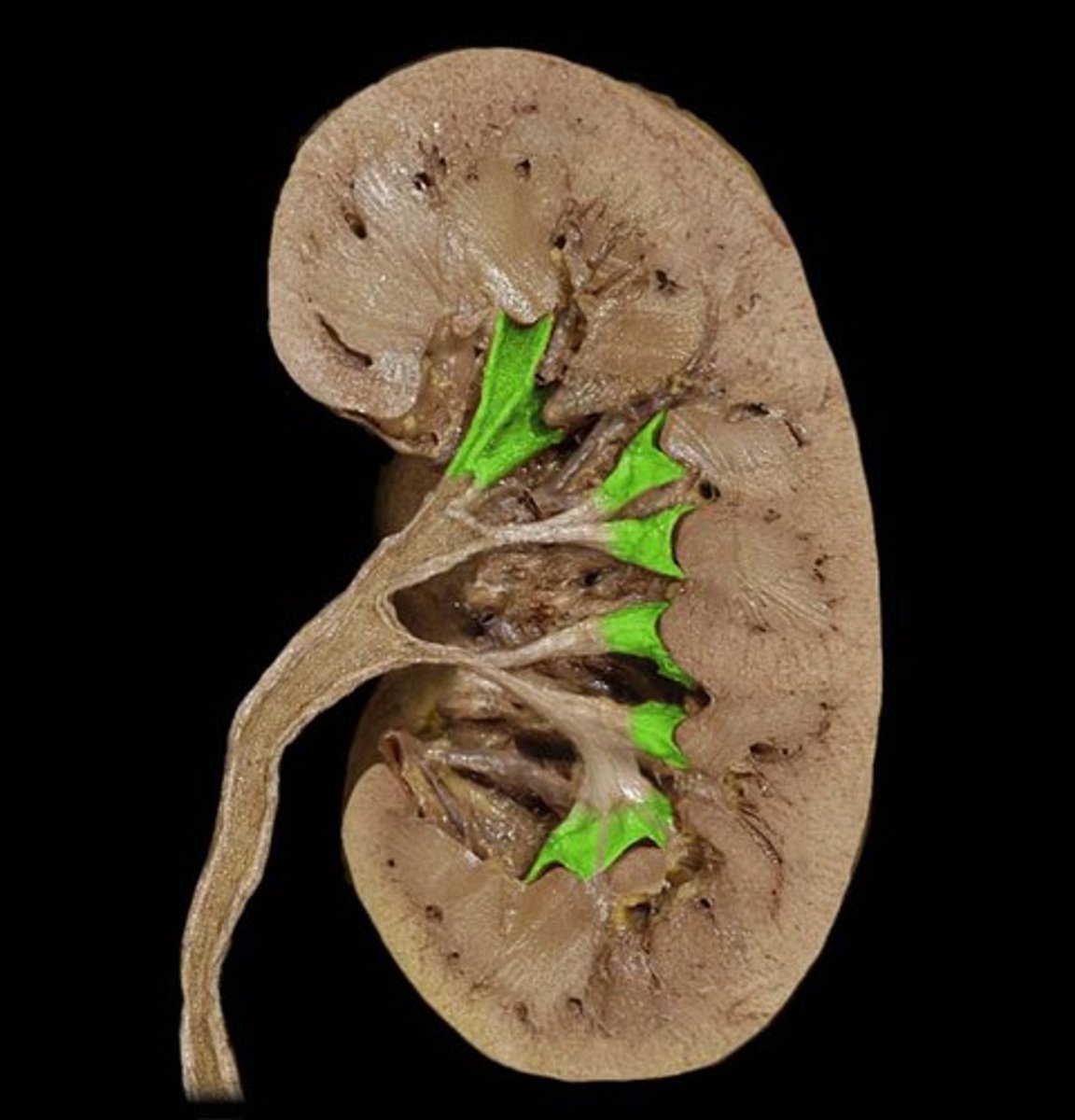
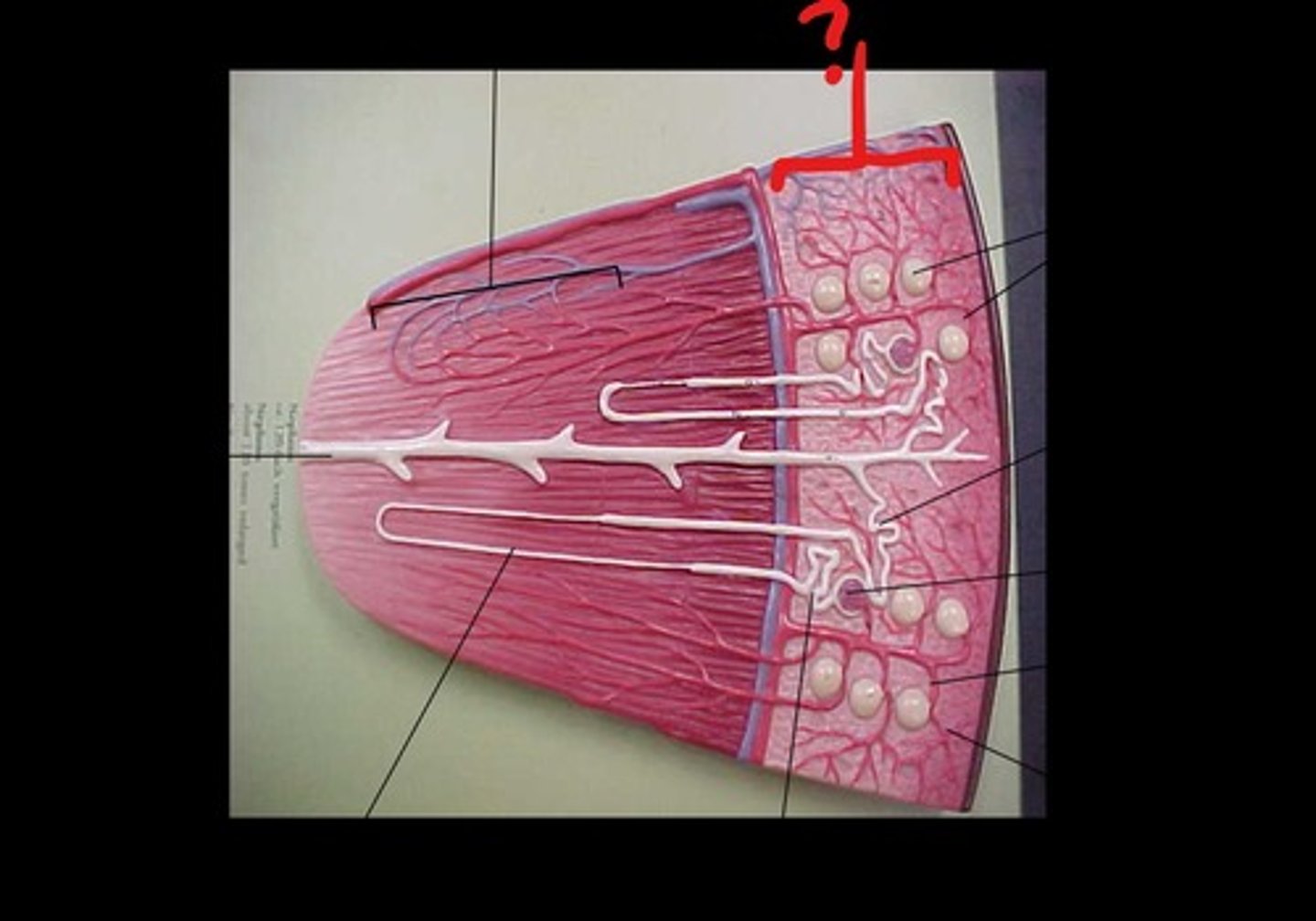
renal pyramids
triangular-shaped areas of tissue in the medulla of the kidney where many nephrons are found (in the tip)
papillae
tip/apex of renal pyramid where nephrons are "funneled" in/drain (contains terminal portions of nephron collecting ducts)

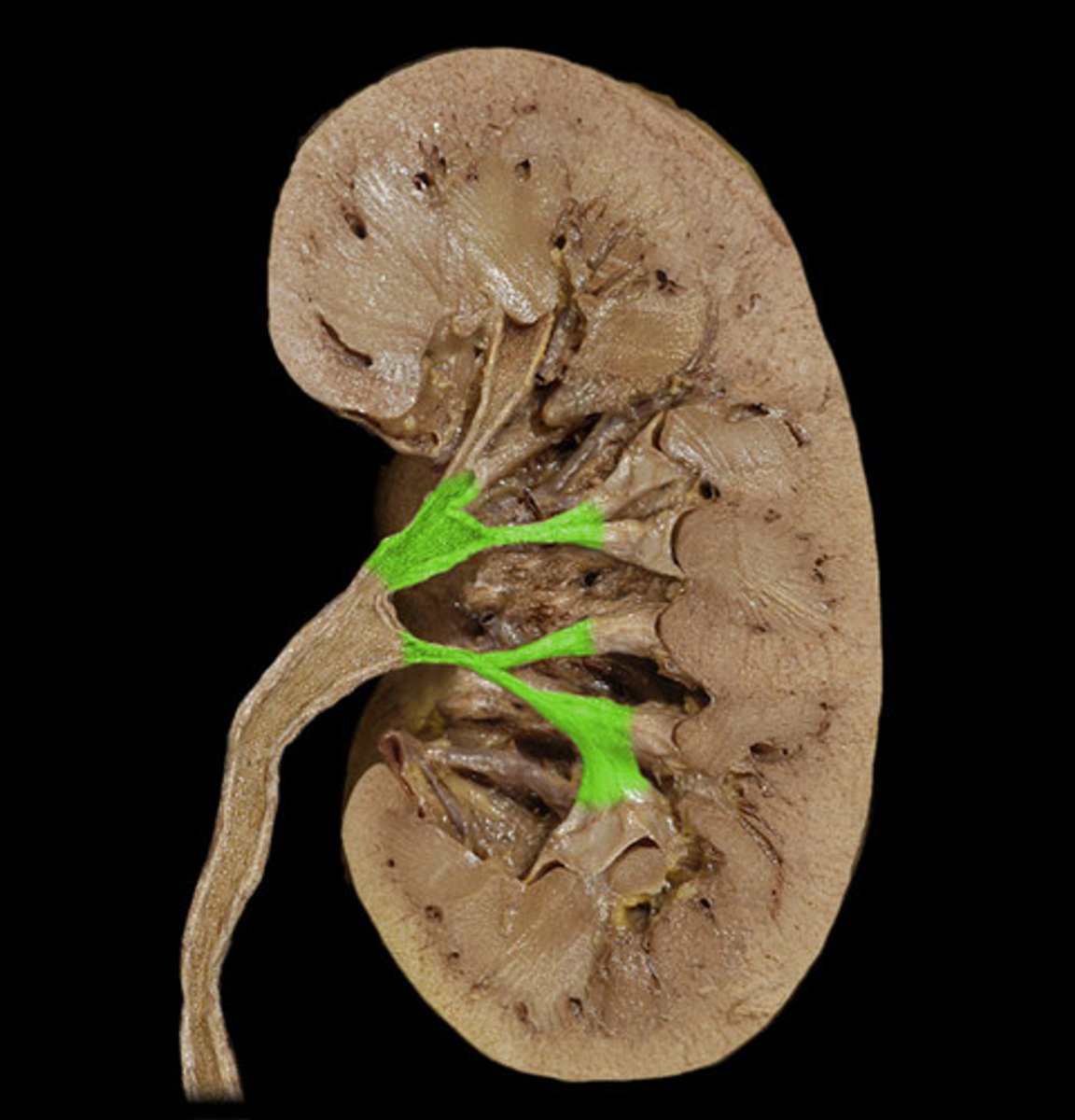
minor calyx
where papillae extend into
major calyx
where minor calyces converge into to form the renal pelvis
nephron
functional unit of the kidney; two types (cortical and juxtamedullary)
head of all of these is located in the the cortex
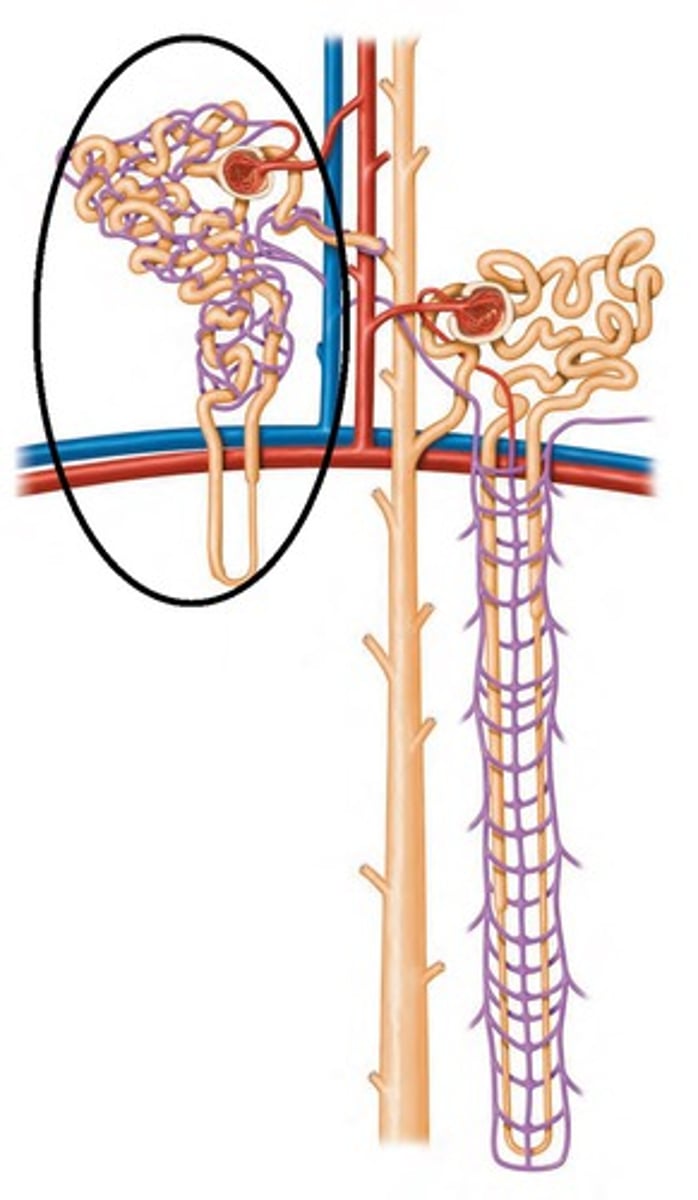
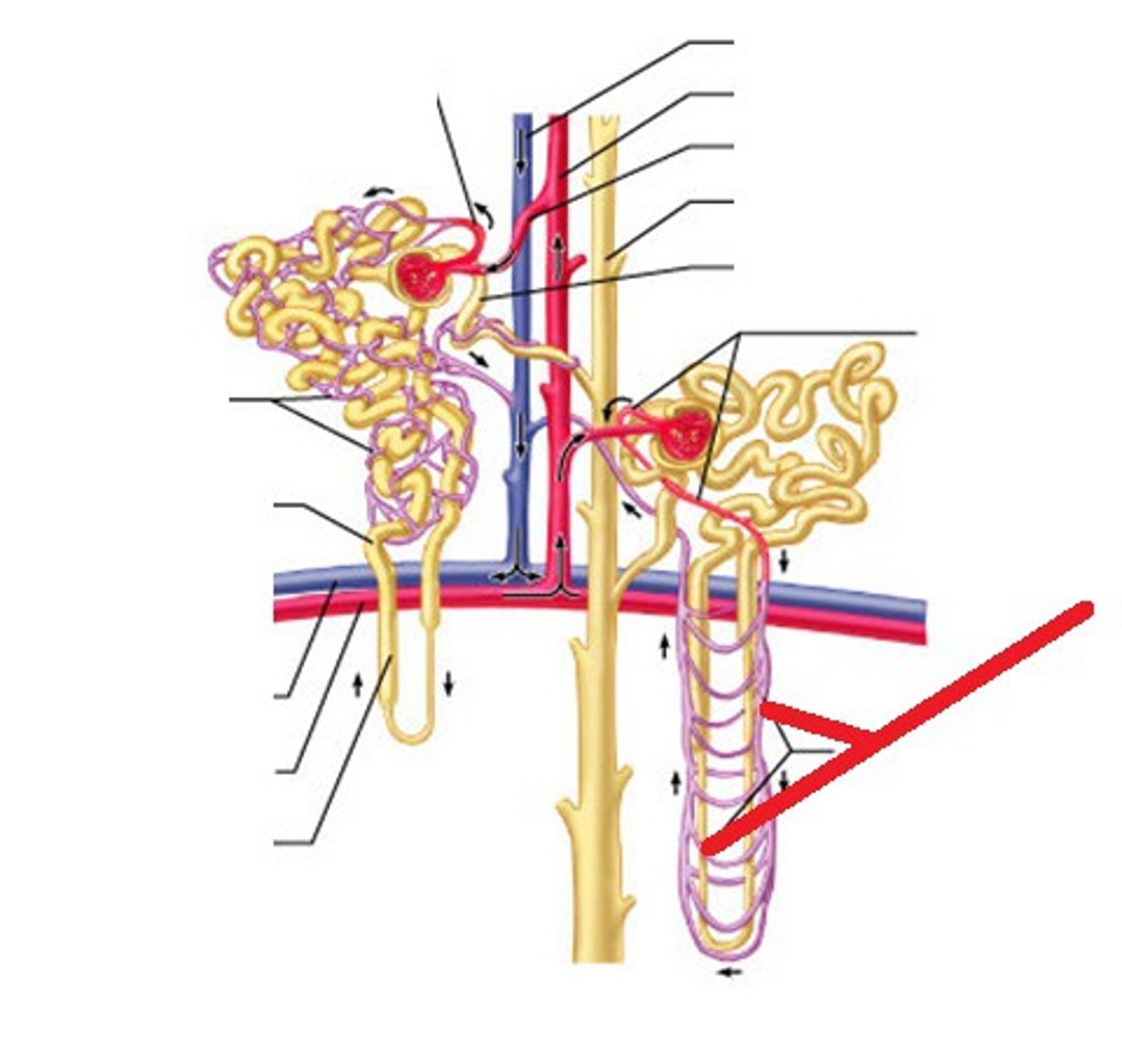
cortical nephron
nephrons with a shorter loop of henle responsible for filtration, reabsorption, and secretion
surrounded by peritubular capillaries
85% of nephrons
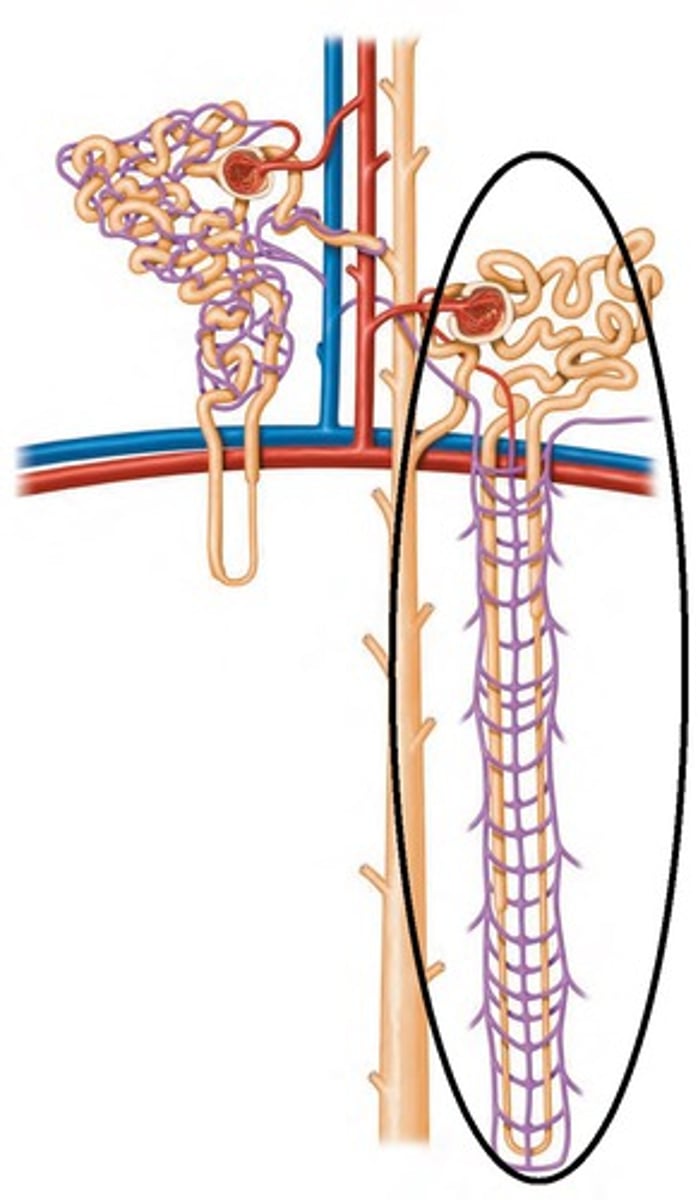
juxtamedullary nephron
nephrons with a long loop of hence that extended deeper in to the medullar responsible for concentrating urine
establish concentration gradient from cortex to deeper medulla; build osmolarity diff
surrounded by vasa recta and peritubular capillaries
peritubular capillaires
capillaries that surround the tubules of a nephron; site of secretion/reabsorption (nephrons are in very close contact with blood in vessels)
vasa recta
vessels that extend from peritubular capillary that accompanies the long loop of henle
corpuscle (bowman's capsule + glomerulus) and renal tubule (50 mm length)
Bowman's capsule → proximal convoluted tubule → loop of henle (hairpin/U-shaped structure) → distal convoluted tubule → collecting duct → drains into tip of medulla
what structures make up a nephron? list them in order
filtration, reabsorption, and secretion
excretion = filtration - reabsorption + secretion
urinary excretion of a substance depends on its ___? give the formula to determine this
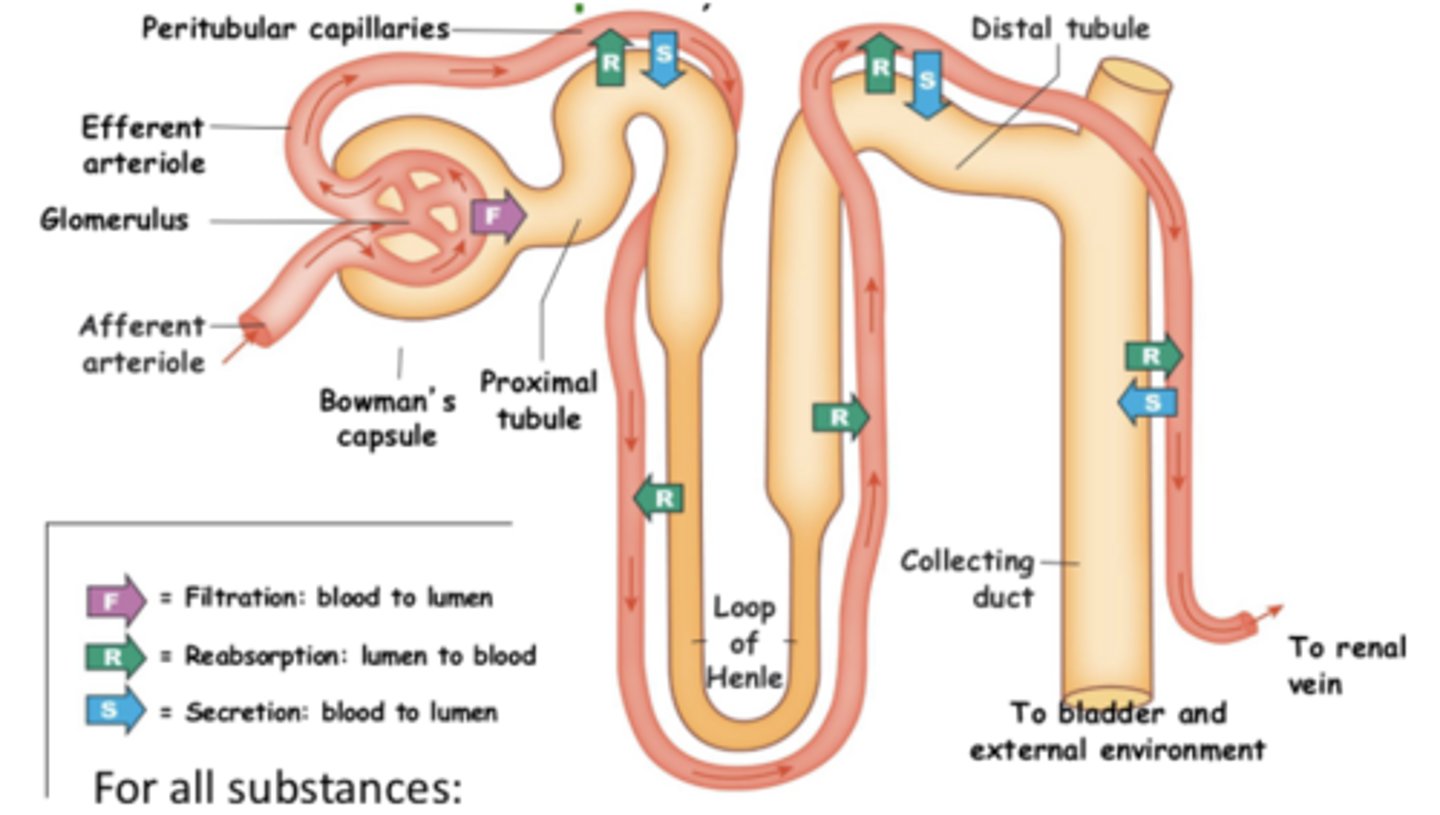
excretion
how much filtration from capillary bed (glomerulus) into Bowman's space there is
filtration - reabsorption + secretion
reabsorption
once a substance has entered tubule, going back into the blood
lots throughout path of renal tubule
secretion
when a substance from the blood joins the renal tubule
mostly in proximal and distal tubules/collecting duct
glomerular filtration rate (GFR)
amount of plasma filtered from the glomeruli into Bowman's space (amount of filtrate formed) per unit time; volume/time
key indicator of kidney health → in average adult, average is about 125 mL/min or 180 L/day (entire plasma can be filtered by kidneys ab 60x/day)
20% of plasma is filtered each time by renal tubule, 80% bypasses it
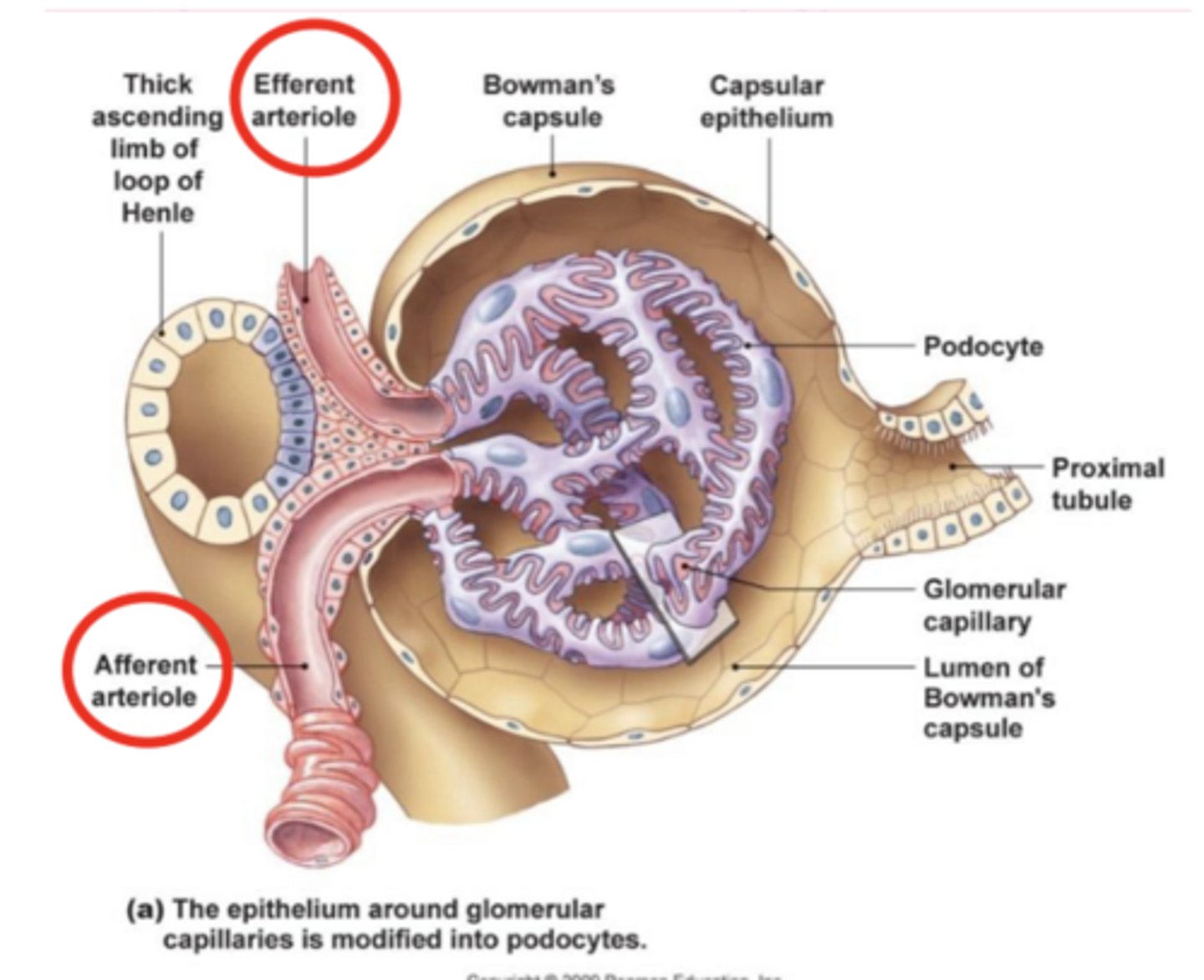
glomerulus
capillary network encased in the upper end of a nephron where filtration of blood takes place

Bowman's capsule
beginning of tubule; cup-shaped strucutre of the nephron that encloses the glomerulus where filtration takes place
has parietal and visceral epithelium

parietal (outer) and visceral (inner) epithelium
visceral is in contact with capillaries and where filtration occurs
what are the two layers of Bowman's capsule?
renal corpuscle
glomerulus and bowman's capsule
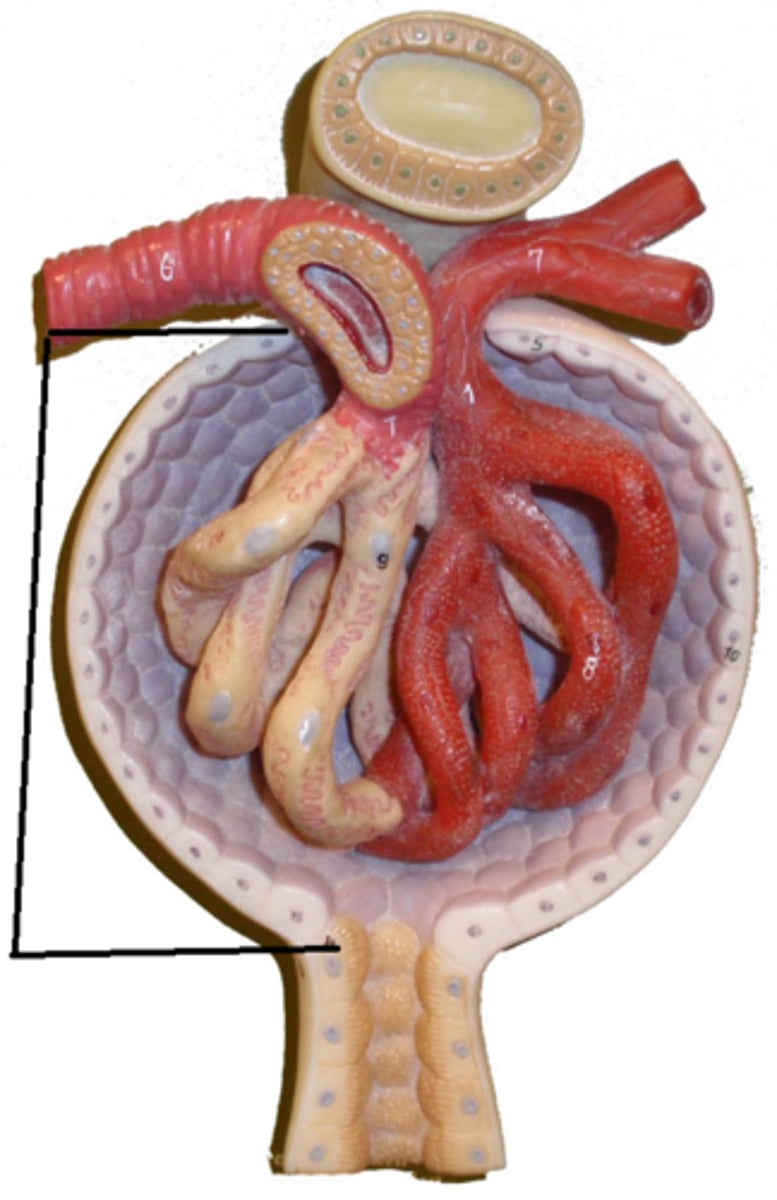
the afferent arteriole brings blood in, the efferent arteriole is where blood exits (80% of blood leaves through here)
how does blood enter and leave the glomerulus?
filtration barrier
fenestrated capillary epithelium and basement membrane (basal lamina)
pores formed by podocytes, and leaky bc they are not in close contact with each other
podocytes
epithelial cells in the glomerulus that wrap around blood vessels and form a filtration barrier; make up visceral epithelium
resulting filtrate is protein-free dialysate of plasma; only RBCs and large proteins are left behind in blood during filtration
plasma inside capsule has ions, nutrients, etc.
what substances are found in the filtrate in nephron?
how much gets filtered depends on pressure; net glomerular filtration pressure = PH - Pfluid - π
favor filtration: PH (glomerular capillary hydrostatic pressure)
oppose filtration: Pfluid (Bowman's hydrostatic pressure) and π (colloid osmotic pressure)
what factors affect GFR? what is the equation for net glomerular filtration pressure?
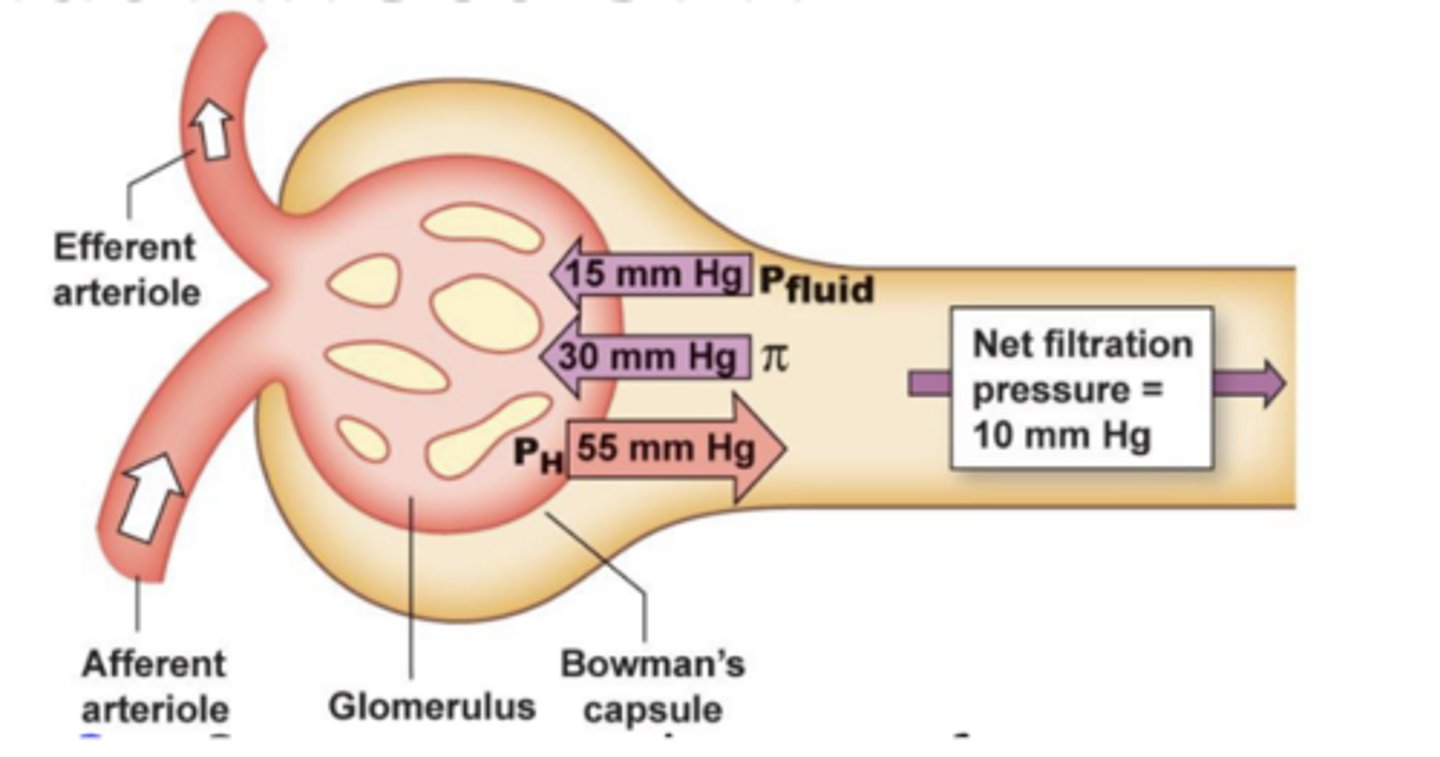
PH (glomerular capillary hydrostatic pressure)
blood coming in from capillaries; very little pressure in Bowman's space normally, but glomerulus does have pressure from fluid
driving force of filtration by acting as primary mechanism for physiological regulation of GFR (increase in this = increase in GFR)
Pfluid (Bowman's hydrostatic pressure)
once fluid moves into Bowman's space, it creates pressure opposing original fluid that came in
π (colloid osmotic pressure)
protein left behind in blood creates osmotic pressure gradient that drives fluid back into the capillaries (glomerulus)
arterial pressure (systemic BP, buffered by autoregulation), afferent arteriole resistance (blood coming in), and efferent arteriole resistance (blood going out)
what are the 3 factors that influence PH?
autoregulation of GFR
maintains GFR despite (wide range of) changes in systemic BP; even if systemic BP (MAP) changes, GFR will be buffered and not change as much bc of myogenic response, TGF, and hormones (RAAAS)
afferent: less blood flow in → hydrostatic pressure in glomerulus (PH) and thus GFR will decrease → renal blood flow (blood flow to kidneys) will also decrease bc less input = less output → more blood will flow to other organs
efferent: more blood flow in (less out) → PH and thus GFR will increase
renal blood flow will still decrease if both efferent and afferent are restricted an equal amount
how would constricting the afferent and/or efferent arterioles affect PH?
myogenic response
increase in renal BP (stretch in arteriole) = constrict smooth muscle in afferent arteriole to oppose it (and vice/versa)
stretch from increased BP → Ca in → activate calmodulin and MLCK → contraction
similar to autoregulation in other systemic arterioles
tubuloglomerular feedback (TGF)
paracrine control/feedback; increase in GFR → increasing NaCl (osmolarity in renal tubule) sensed by macula densa → send signals to juxtamedular cells → smooth muscle of afferent arteriole contracts
macula densa
osmoreceptors in distal tubule; modified epithelial cells that detect osmolarity change and send signals based on that to granular cells
granular cells (juxtaglomerular cell)
modified smooth muscle of afferent arteriole that receive signals from macula densa cells and act accordingly
secrete renin (paracrine signal from NO)
GFR increase → flow through tubule increases → flow past macula densa increases → paracrine signals from macula densa go to afferent arteriole (granular cells) → granular cells contract (afferent arteriole constricts) → resistance in afferent arteriole increase → hydrostatic pressure in glomerulus decreases → GFR decreases
describe the feedback loop of TGF of lowering GFR in response to an increase in it
use adenosine: if you have too much GFR, you constrict afferent arteriole to decrease how much blood gets through
Adenosine causes vasoconstriction and NO causes vasodilation. When GFR increases, the macula densa cells will release which paracrine signal as part of the TGF response?
renin
hormone secreted by the kidney that raises BP and converts angiotensinogen into angiotensin I
secreted in response to BP drop, sympathetic activation, and low osmolarity of tubular fluid (through macula densa) from granular cells
angiotensin-converting enzyme (ACE)
converts angiotensin I to angiotensin II, made by lung endothelial cells
angiotensin II
increases BP by causing arteries to constrict, increases CO, and triggers secretion of ADH (hypothalamus) and aldosterone
decreases GFR → water retention (not excreted in urine) → higher BP from higher blood volume
made by liver and causes thirst as well
aldosterone
triggered by angiotensin II, causes nephron to reabsorb more Na → increase blood volume and maintain osmolarity
from adrenal glands (kidneys), increases BP
antidiuretic hormone (ADH)
increases water reabsorption (insertion of aquaporins into nephron)
from posterior pituitary (made in hypothalamus), increases BP
atrial natriuretic peptide (ANP)
dilates afferent arterioles to increase GFR and inhibit renin secretion in response to high BP (antagonist of RAAAS)
increases excretion of Na in urine; increases GFR and decreases reabsorption of Na by nephrons
from heart (atrial myocytes)
correct answer is E because aldosterone secretion is suppressed, not increased
answer the question and explain your answer