Biology 30 AP - Reproduction & Development
1/114
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
115 Terms
Male reproductive system flow chart
primary reproductive organs (gonads) → testes → produce sperm
Male gonads function
secret sex hormones → testosterone
puberty (point where reproduction is possible) → males must be able to produce and ejaculate semen
controlled by specific hormones
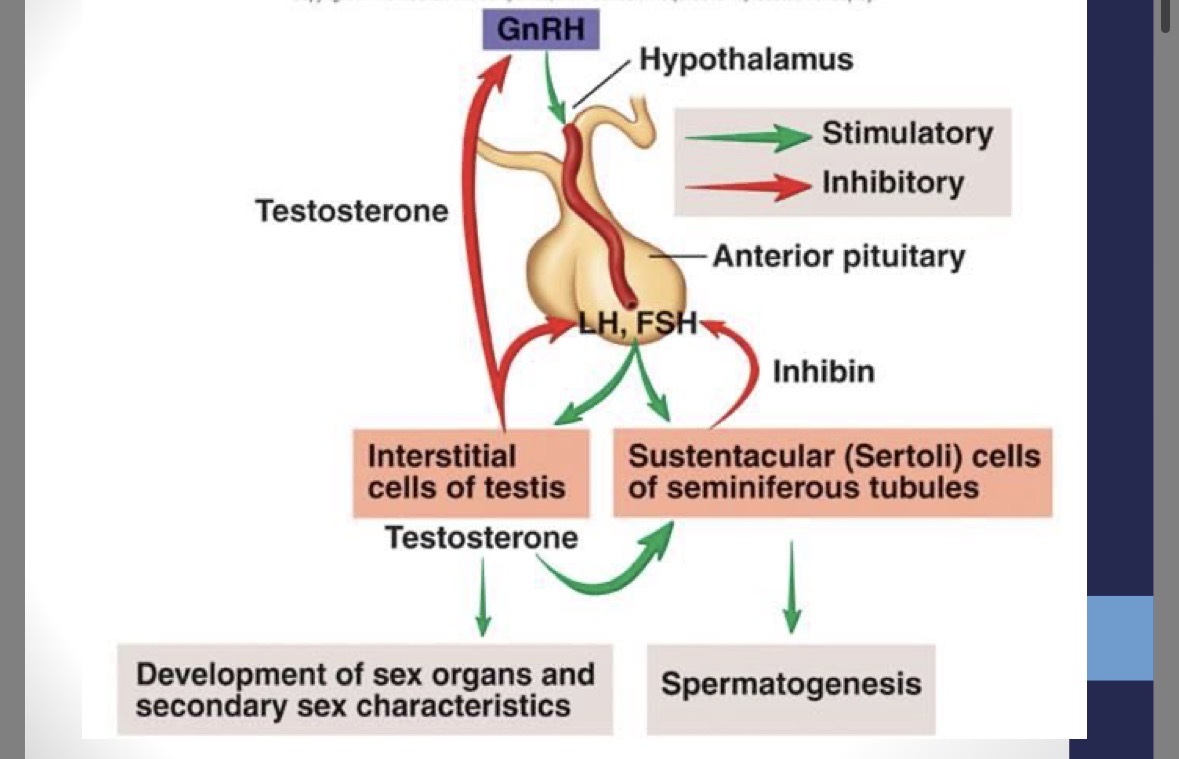
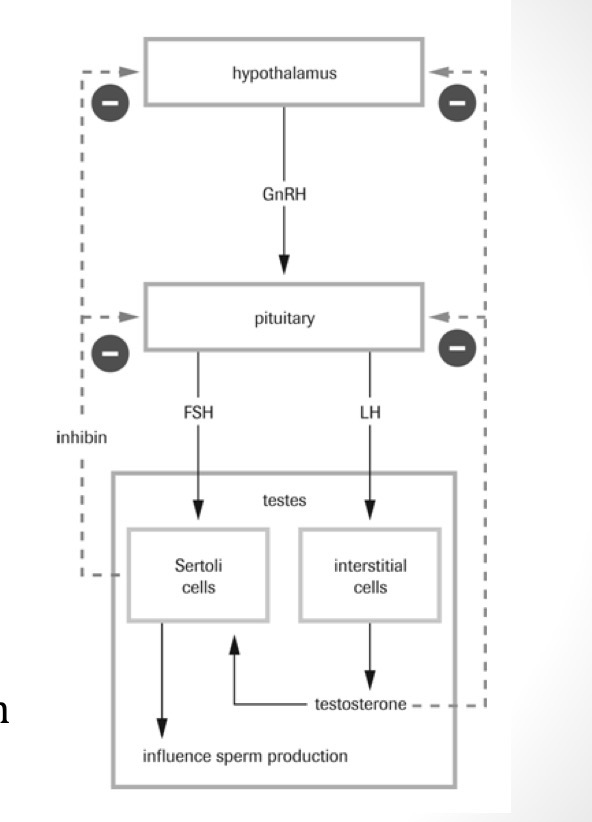
Hypothalamus secretions
GnrH (gonadotropin releasing hormone)
Anterior pituitary secretions (male)
FSH (follicle stimulating hormone) → simulates sperm production in seminiferous tubules
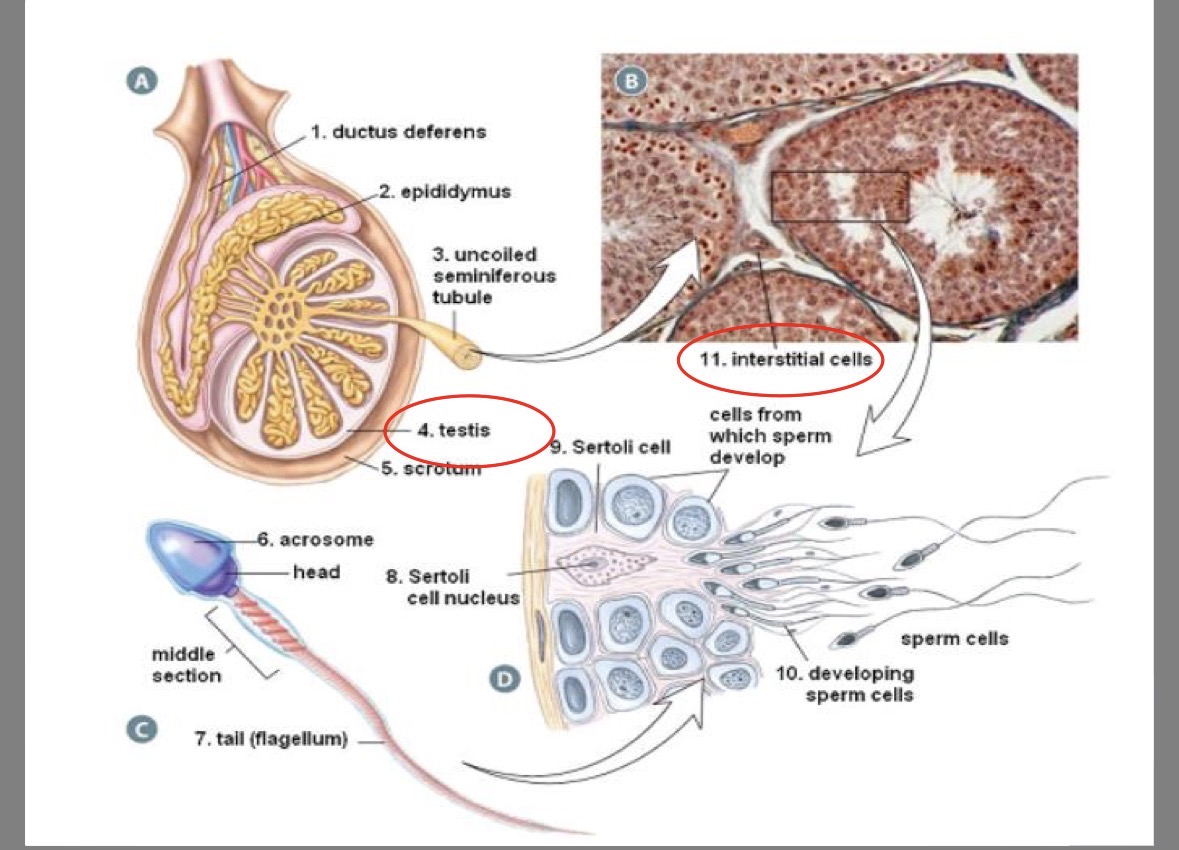
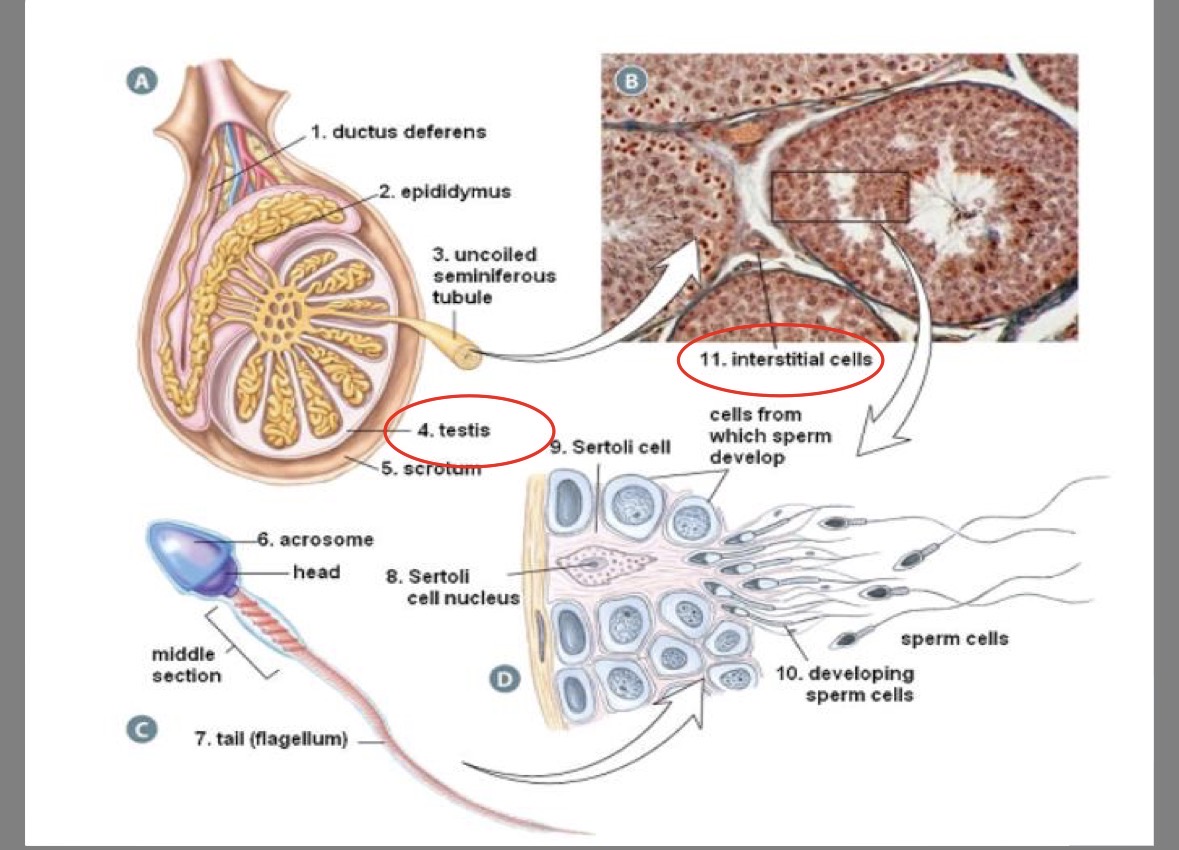
LH (luteinizing hormone) → stimulates testosterone production in interstitial cells
Male secondary sex characteristics
caused by testosterone
development of pubic and facial hair
maturation of internal and external genitalia
increase in shoulder width and muscle mass
voice → larynx enlarges, vocal cords thicken and lengthen
skin → sebaceous gland secretion thickens and increases (acne)
mental → increased aggression, sex drive
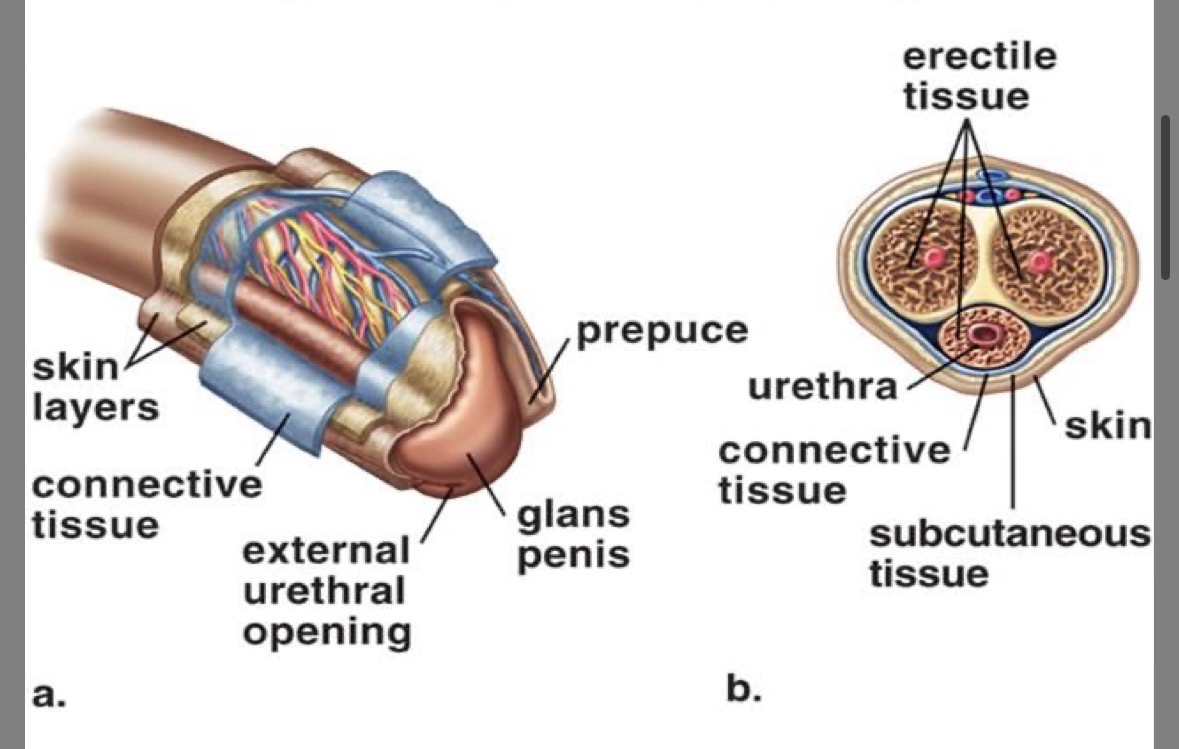
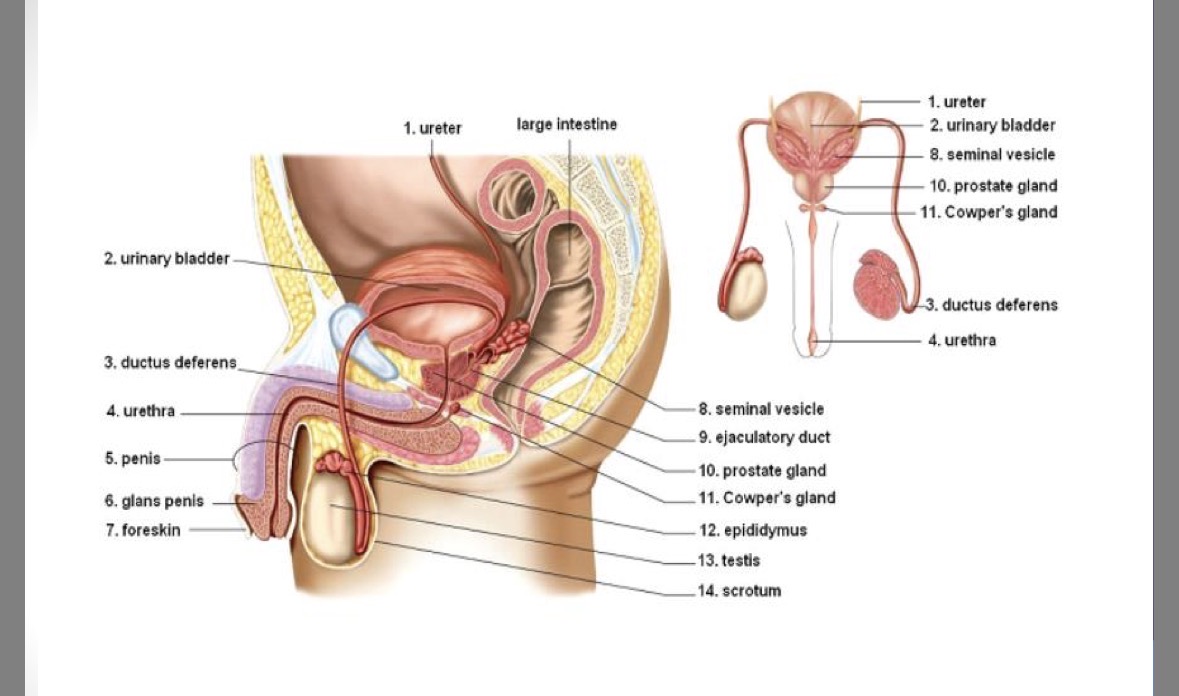
Prepuce (foreskin)
serves a protective function
sometimes removed in circumcision)
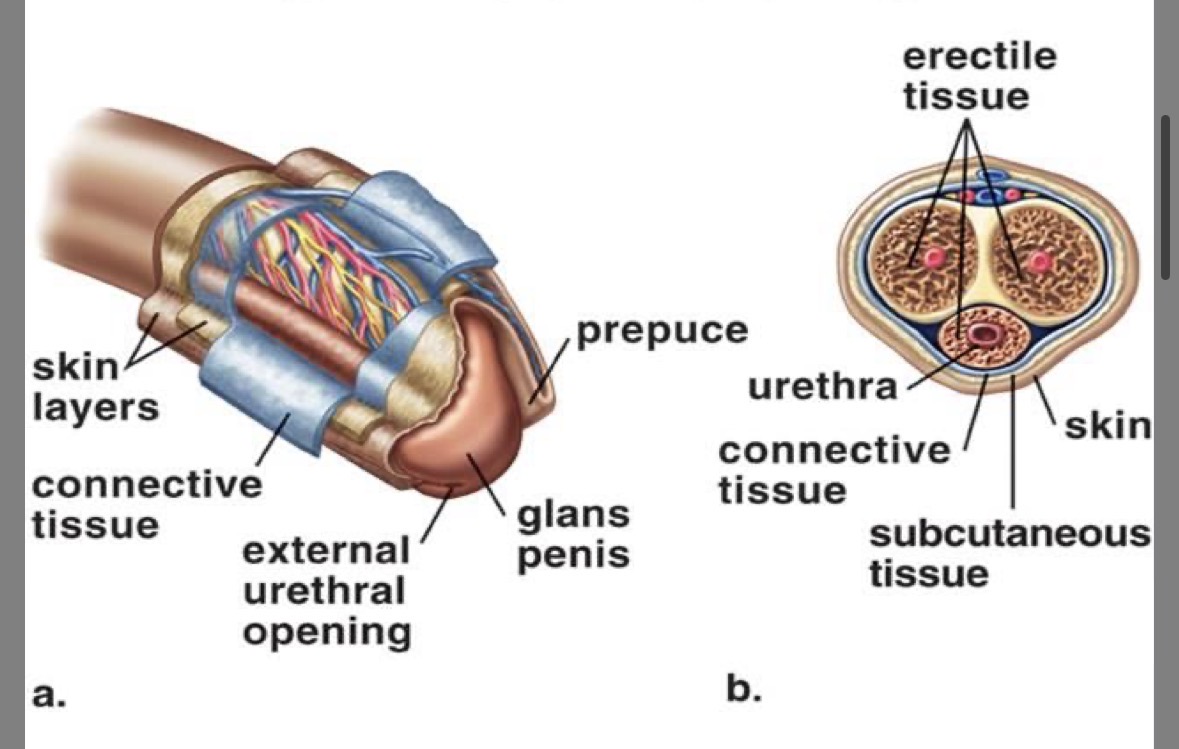
Glans
expanded tip of the penis
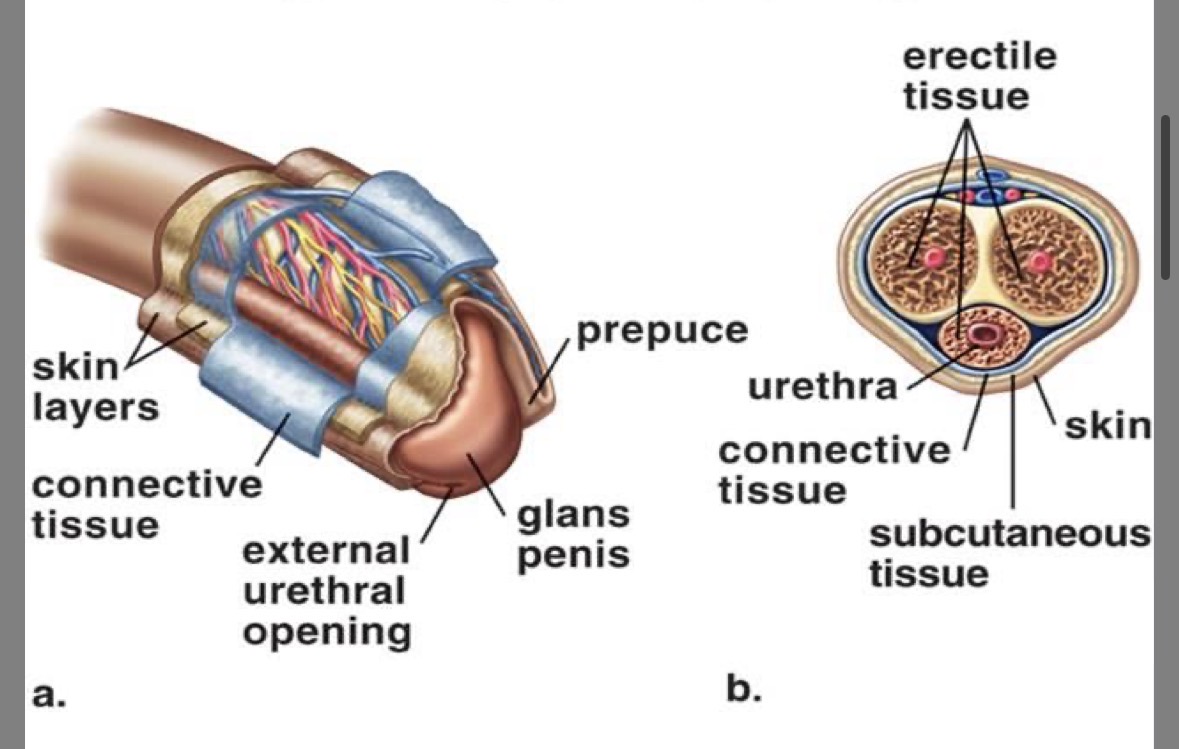
Corpus cavernosa
erectile tissue
fills with blood thus producing an erection
Corpus spongiosa
soft erectile tissue
Urethra
carries sperm and urine (NEVER AT THE SAME TIME)
sphincter controls urine excretion
Erection
produced by trapping of blood in corpus cavernosa in response to stimulation of parasympathetic nervous system
arteries dilate (increased blood flow in)
veins constrict (decreased blood flow out)
Prostate gland
produces mucous for lubrication and buffer to protect sperm from acidic vagina
Vas deferens
ductus deferens
tube that carries sperm from testes to urethra
Seminal vesicle
sacs under bladder
secret fructose (food for sperm) & prostaglandins (stimulates uterine contractions → helps sperm move up uterus)
60% of total semen volume
Ejaculatory duct
connects vas deferens to urethra
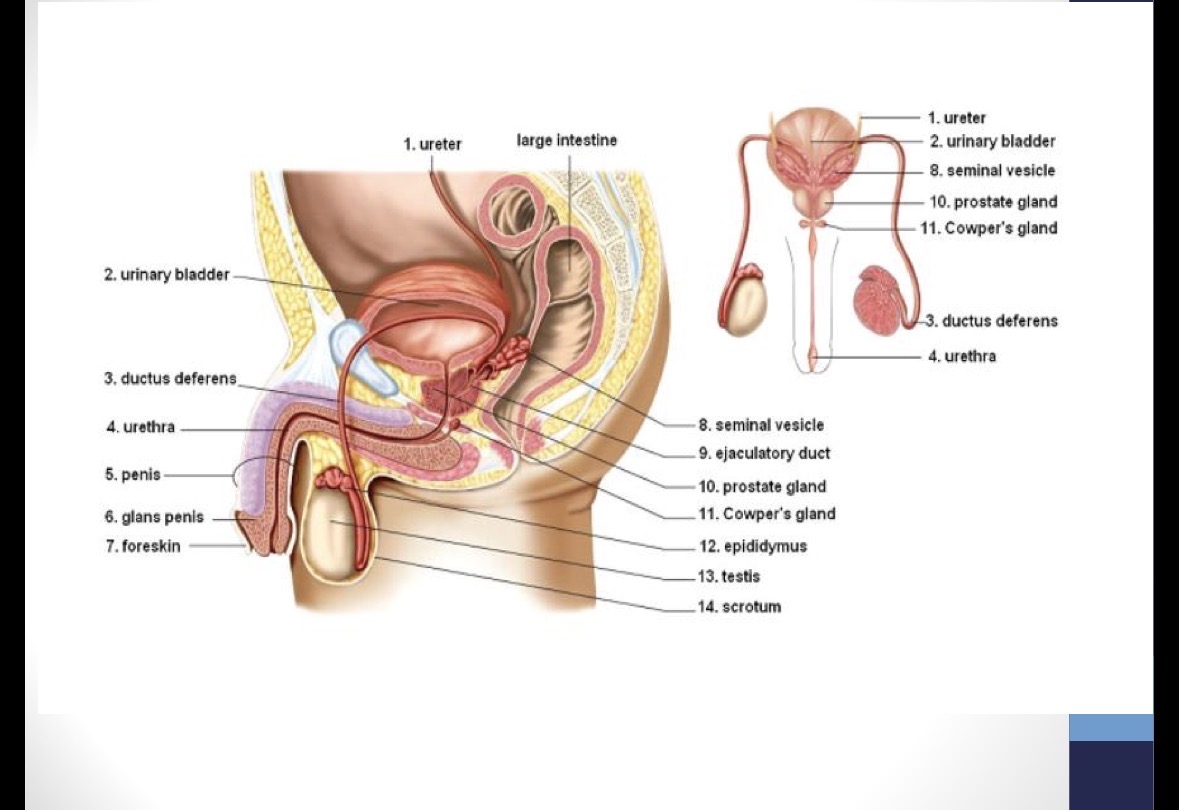
Cowper’s gland (bulbourethral) gland
secretes clear, salty mucous for lubrication and neutralizes acidic male urethra and vagina
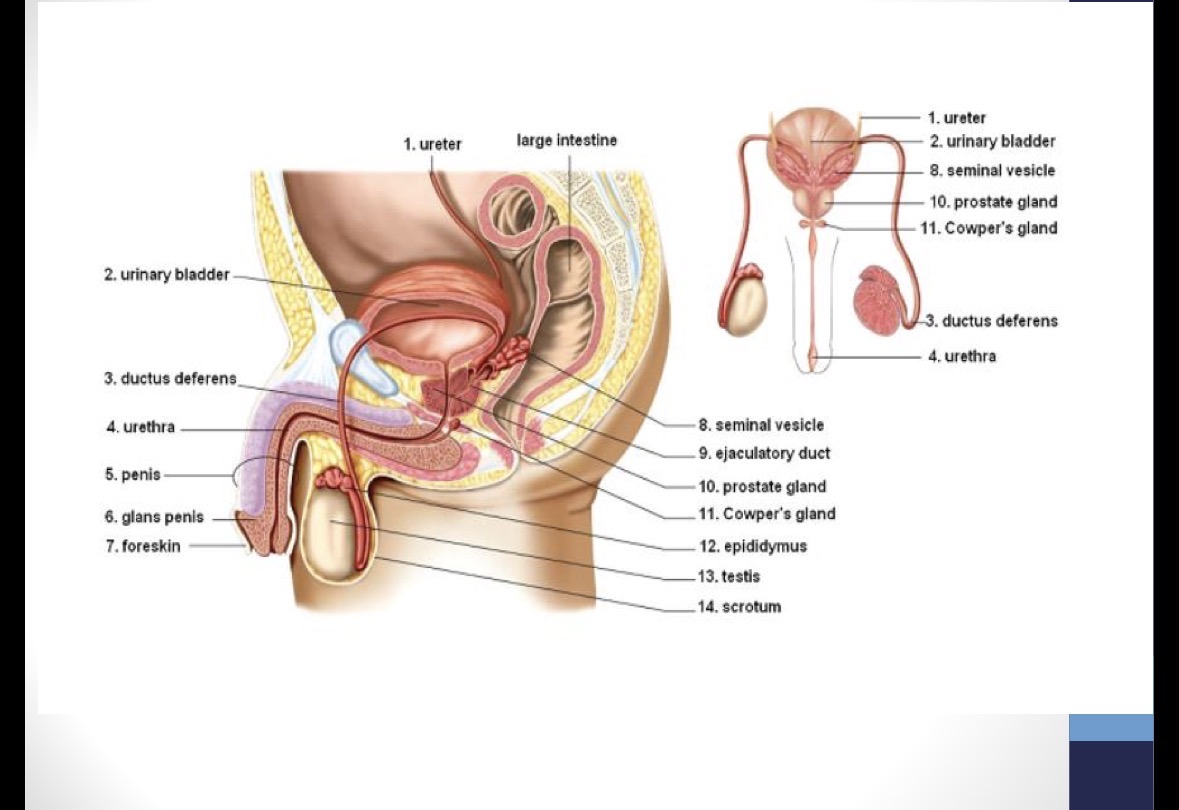
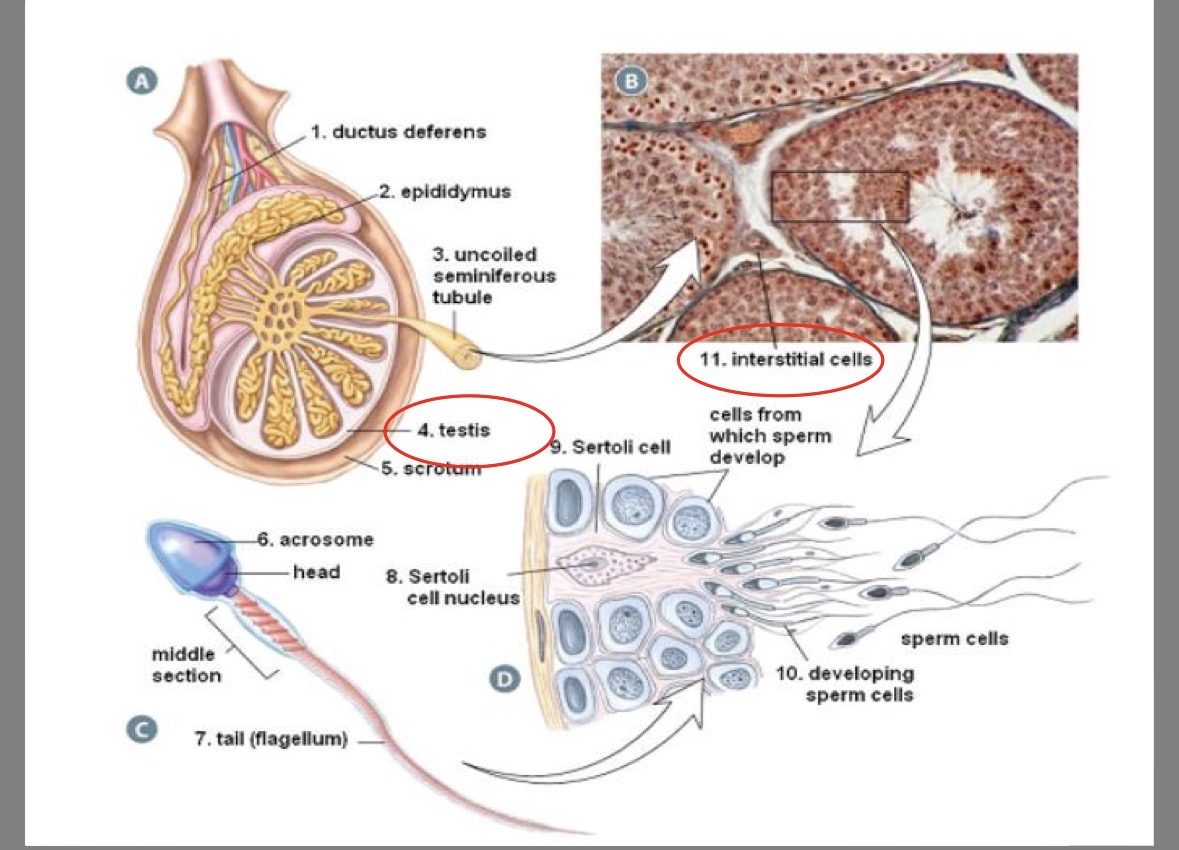
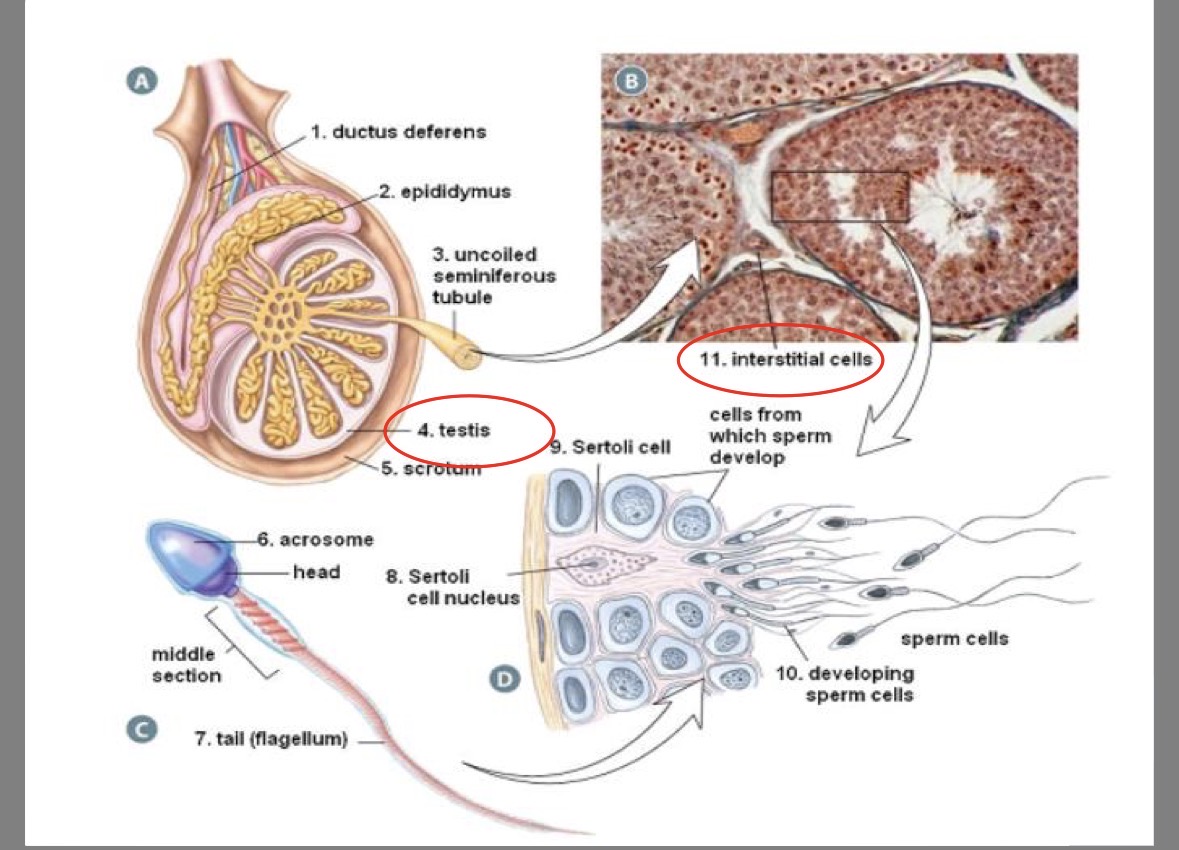
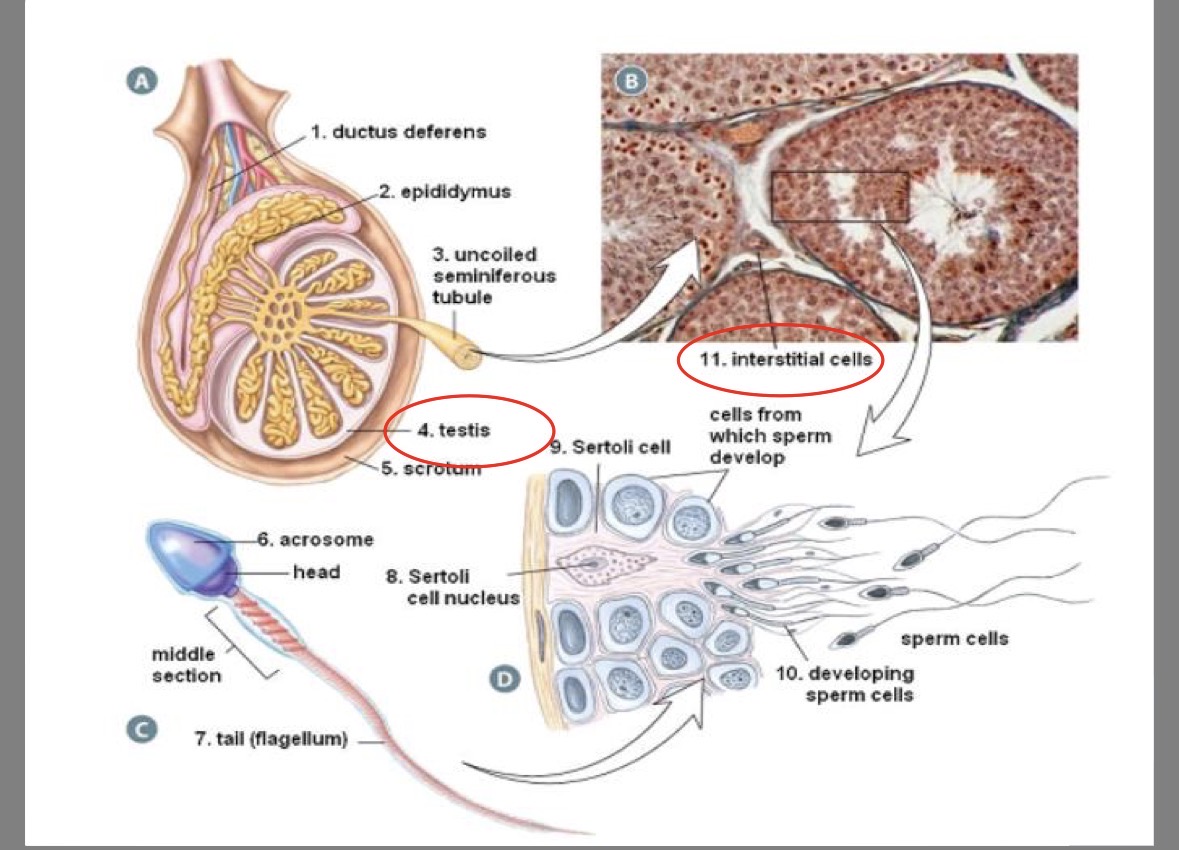
Epididymus
coiled tube attached to outer edge of testis
where sperm completes development/matures
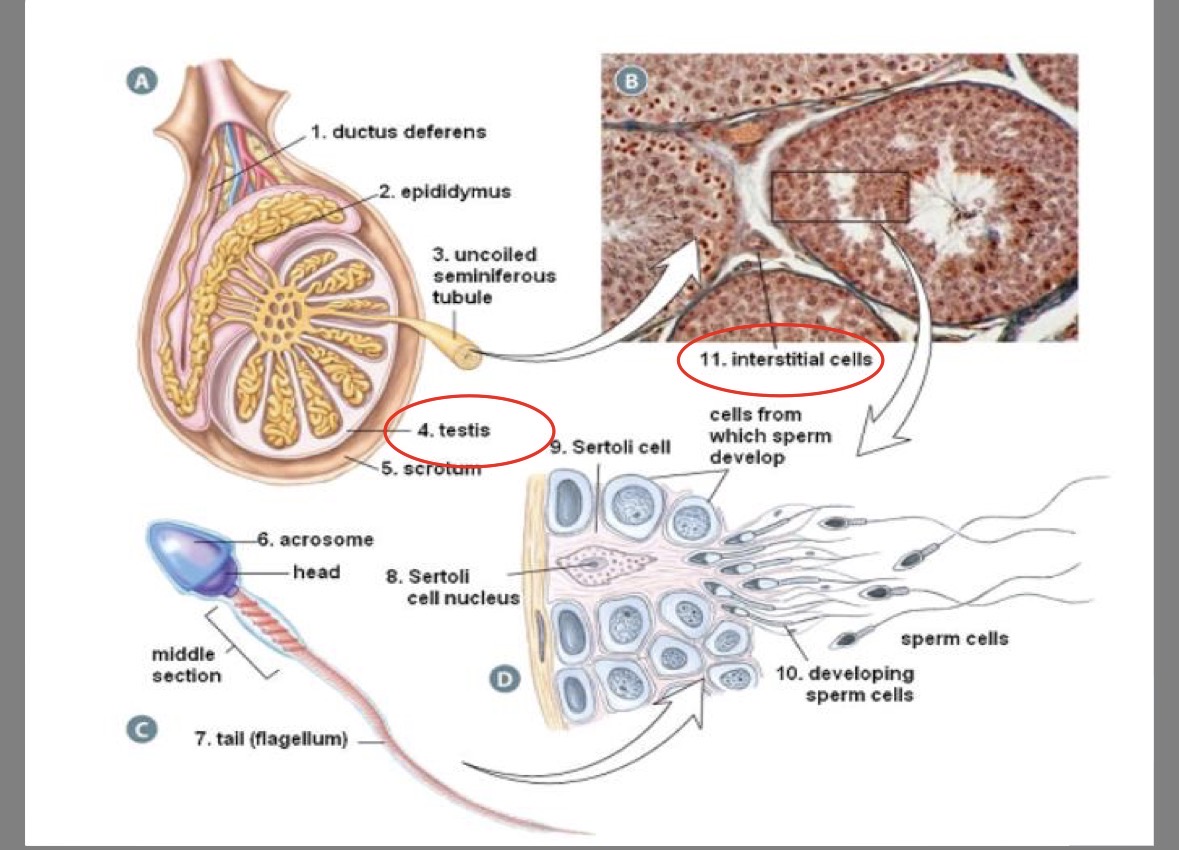
Seminiferous tubules
250m of twisting tubes in testis
site of sperm production
part of testicles
Scrotum
sac that contains testis
made of elastic skin
temperature regulation (sperm develop best at 3 degrees lower than regular body temperature)
part of testicles
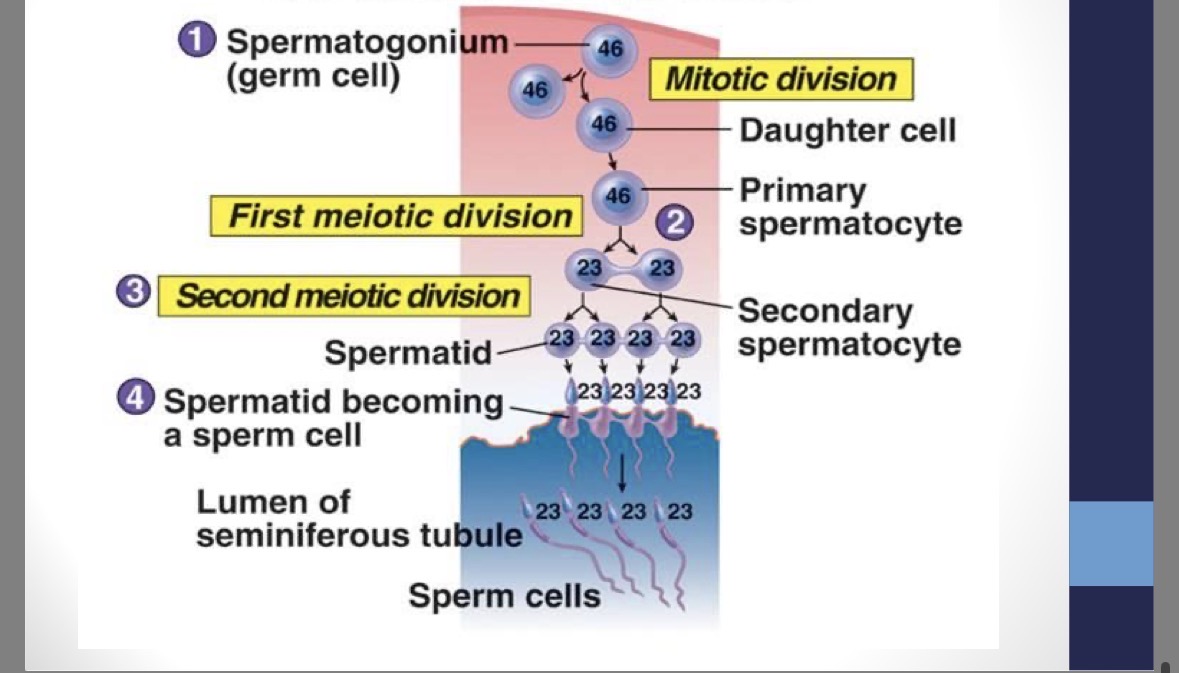
Spermatogenesis
production of sperm begins at puberty and continues until death
1 - spermatogonium (46 chr,) → mitosis → 2 - primary spermatocytes (46 chr.) → meiosis I → 2 - secondary spermatocytes (23 chr.) → meiosis II → 4 spermatids (23 chr.) → 4 mature sperm (23 chr.)
seminiferous tubules: spermatogonium → secondary spermatocytes
epididymus: spermatids → sperm (maturation)
stimulated by FSH and testosterone
Sertoli (nurse) cells
in seminiferous tubules
nourish the sperm as they mature
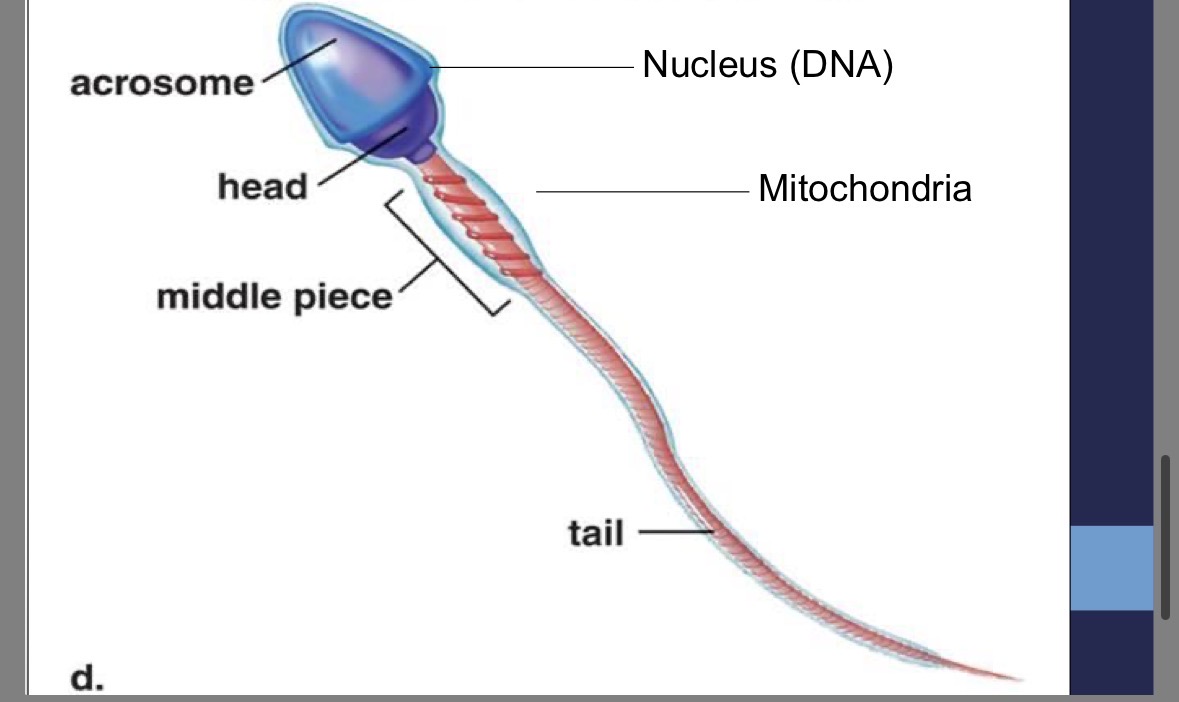
Sperm structure
over 300 000 000 produced daily
designed for travel
nucleus contains DNA
semen includes sperm and secretions from supportive fluids for nourishment and protection against acidic vagina
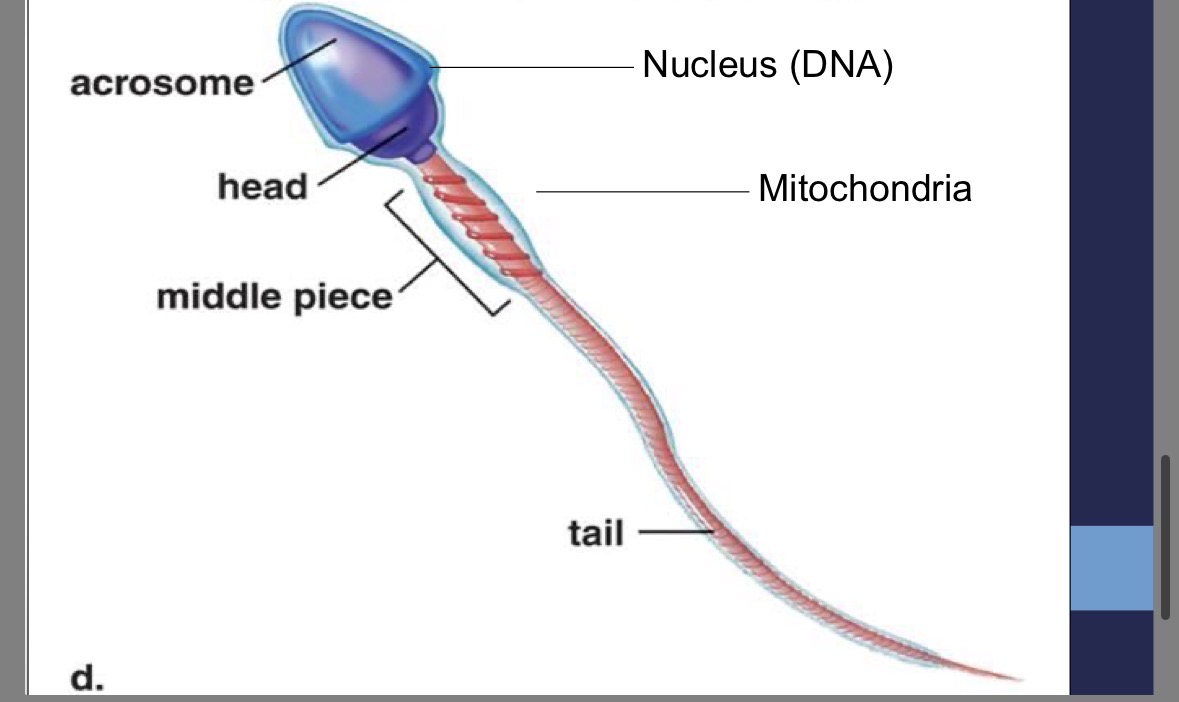
Acrosome
head of the sperm
contains enzymes to penetrate the egg
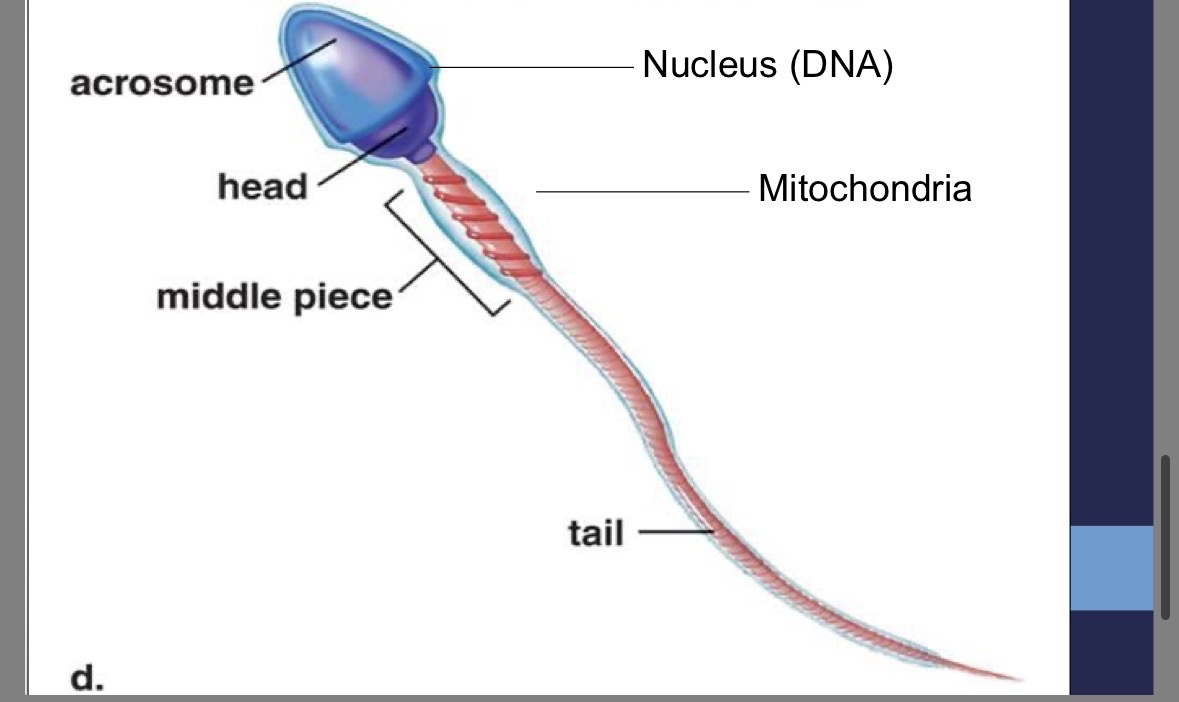
Sperm tail
contains centriole for structure of flagellum
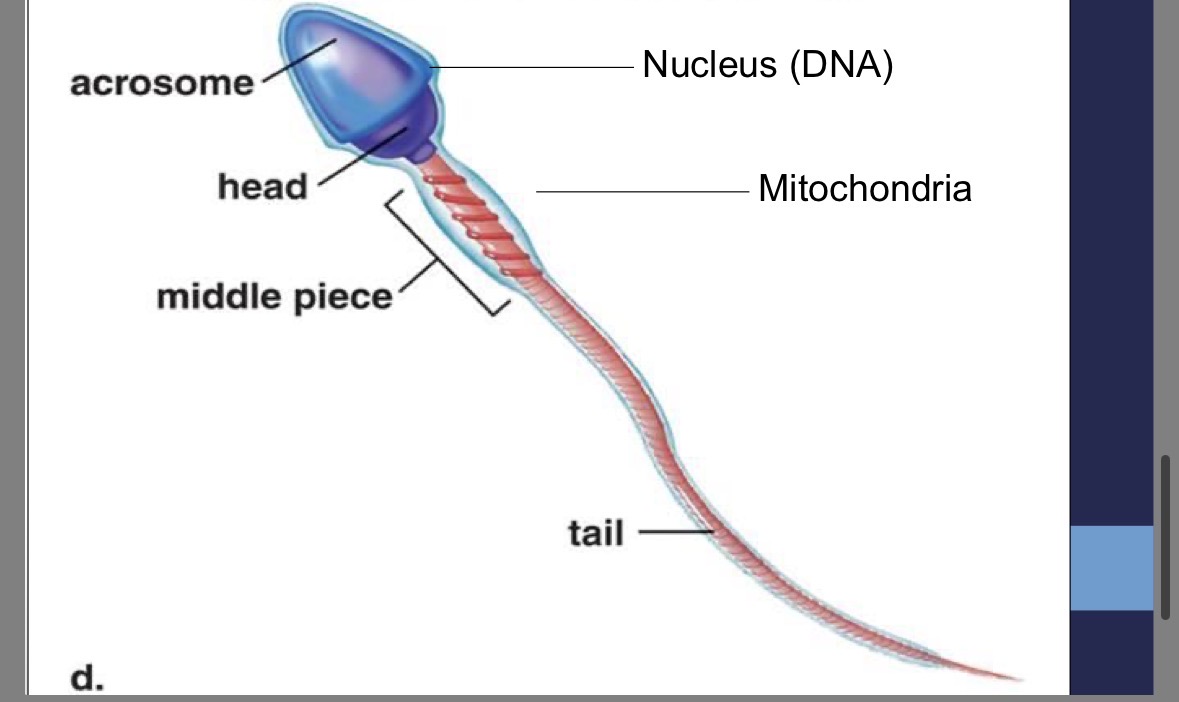
Sperm mid-piece
contains mitochondria to provide the energy for whipping motion
Vasectomy
snipping of vas deferens thus preventing sperm from entering ejaculate
What happens if testicles don’t descend?
viable sperm will not develop
Hernia
rupture occurs in thin membrane separating testes and small intestine → small intestine slips through → impairs blood supply for either testis or small intestine
Testicular cancer
found primarily in young males
Prostate problems
found in older males
enlargement leads to urinary problems
prostate cancer → treated with excision
Path of sperm development to the outside world
seminiferous tubules (site of spermatogenesis)
collecting duct
epididymus (“mature”)
vas deferens
seminal vesicles: add sugar solution to the semen and prostaglandin to increase sperm movement (triggers contractions)
prostate gland: secretes an alkaline buffer to combat the acidic vagina
Cowper’s gland: produce a mucous-rich alkaline secretion
urethra
semen
Female reproductive system flow chart
primary reproductive organs (gonads) → ovaries → produce ova (eggs)
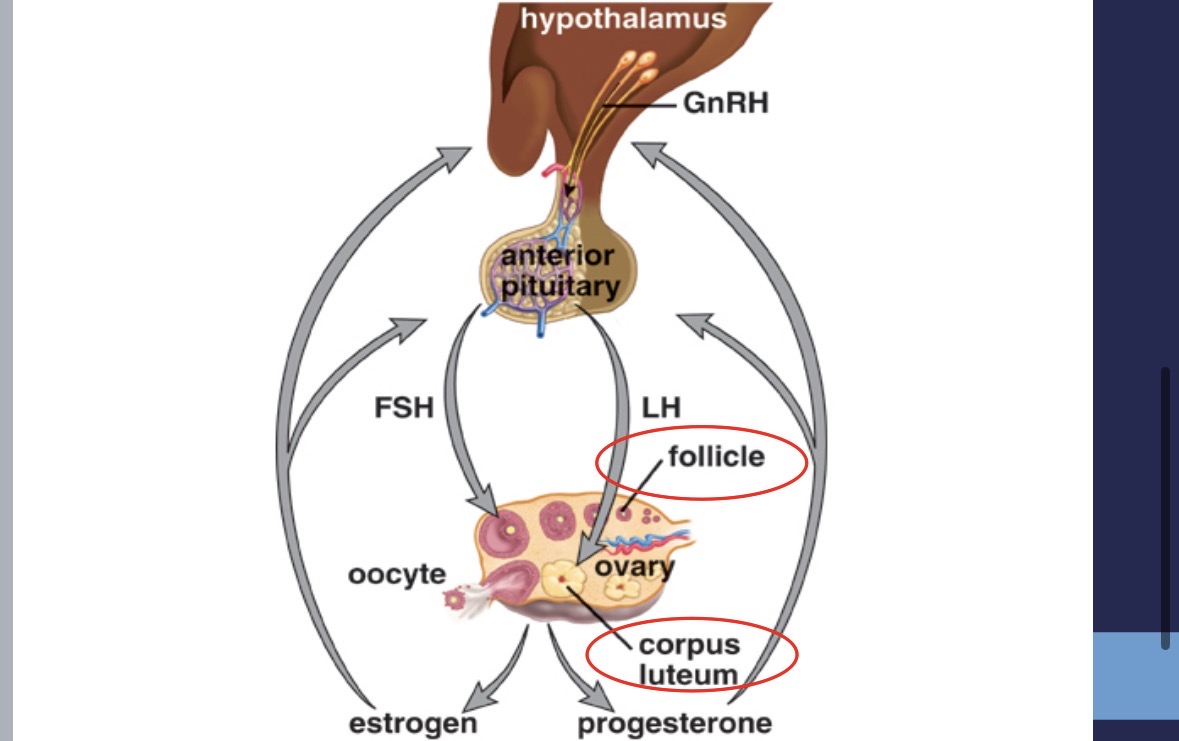
Female gonads function
secretion of sex hormone from gonads → estrogen & progesterone
puberty (point where reproduction is possible) → females must be able to ovulate (release eggs)
controlled by specific hormones
Anterior pituitary secretions (female)
FSH (follicle stimulating hormone) → stimulates follicle in ovary
LH (luteinizing hormone) → stimulates follicle release and formation of corpus lutetium
Female secondary sex characteristics
development of pubic hair
maturation of internal and external genitalia
increase in hip width
voice changes
skin → sebaceous gland secretion thickens and increases (acne)
distribution of fat in breasts and buttocks
Labia
protective flaps of skin on either side of vaginal opening
majora: homologous to male scrotum
minora: homologous to male urethra and penile tissue
vulva
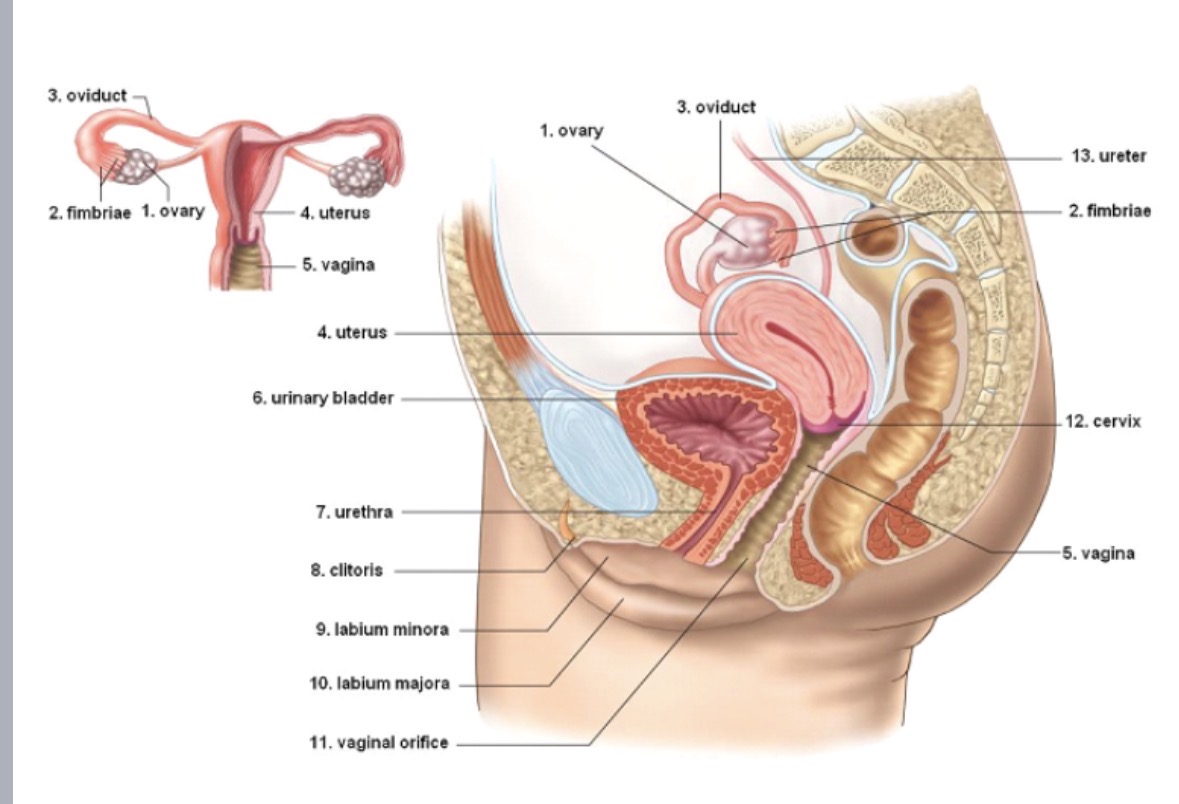
Clitoris
packed with sensory nerves
homologous to male penis
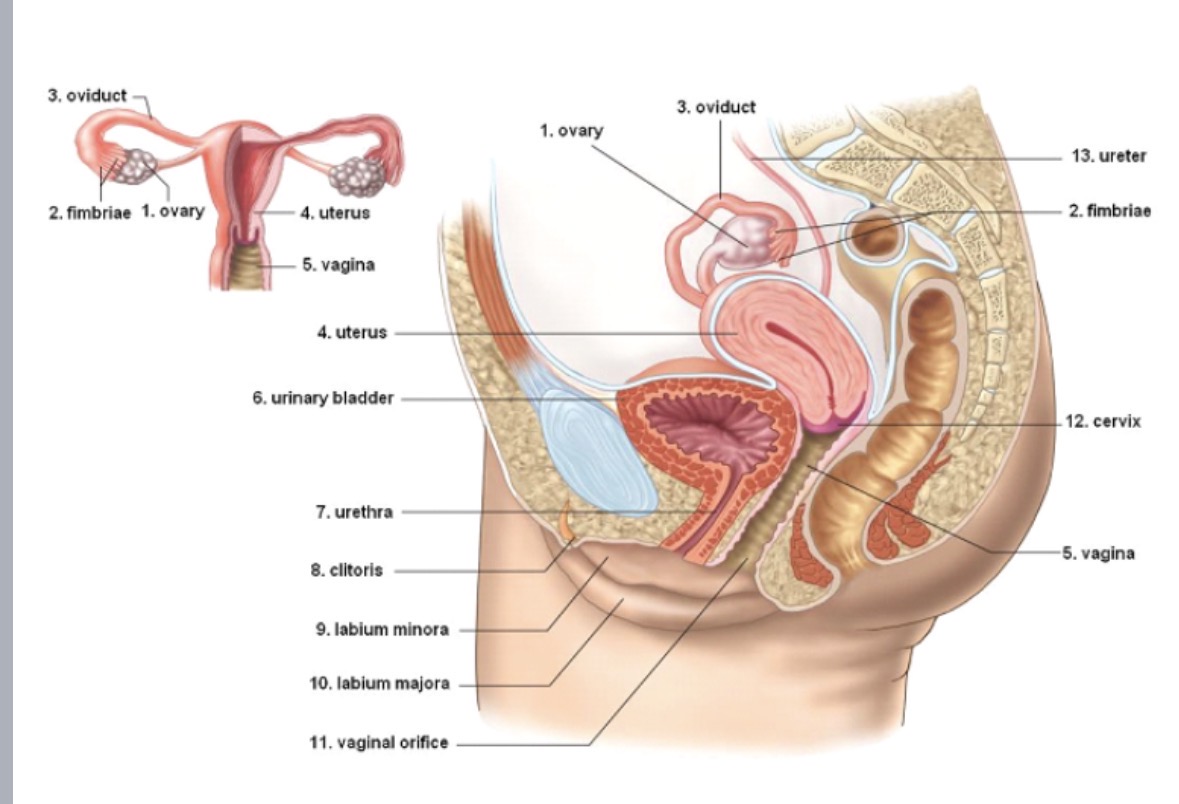
Vagina
connects the uterus with outside world
site of sperm deposition, birth canal, protection from bacterial invasion (highly acidic)
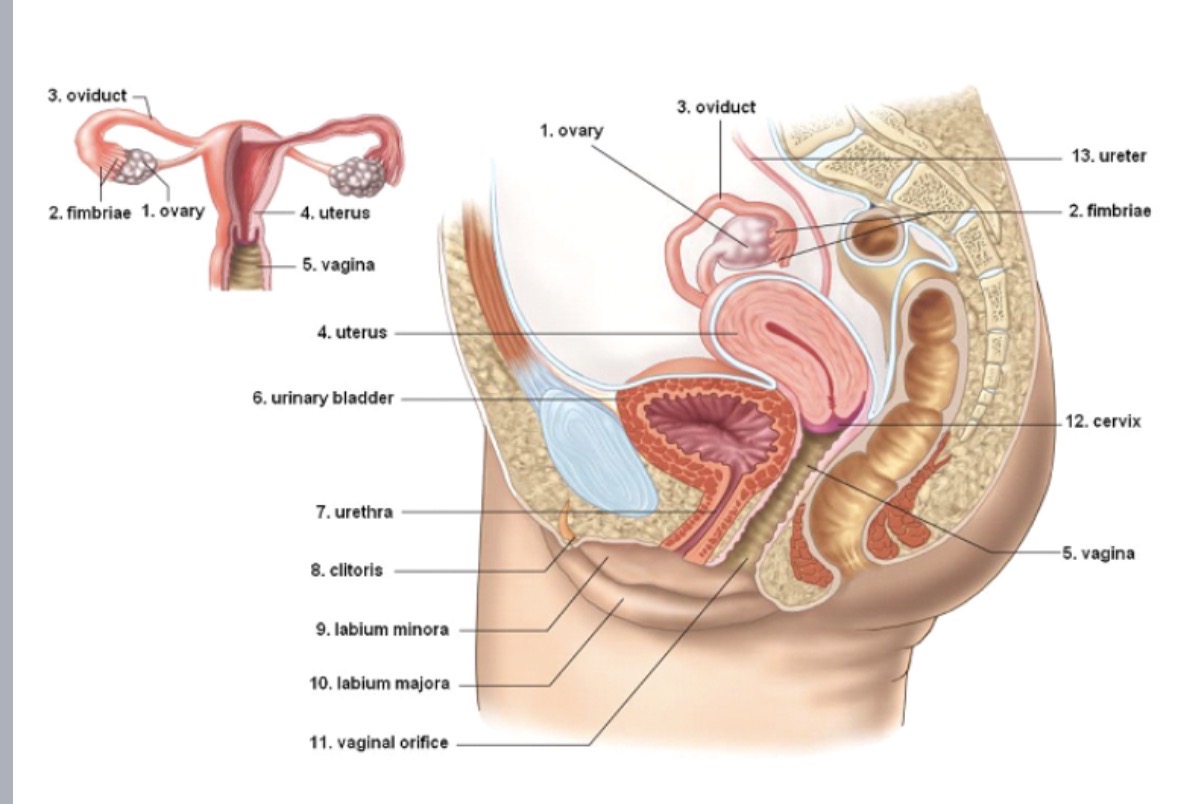
Cervix
cervical canal
muscular band that prevents fetus from delivering prematurely
dilates during birth
Uterus
womb
pear shaped
fertilized ovum embeds in endometrium (uterine lining)
Ovary
store and produce ova
generally one mature ovum produced monthly (alternating ovaries)
Oviduct
fallopian tube
tube carrying mature ova to uterus
site of fertilization
ova swept in by fimbria at open ends
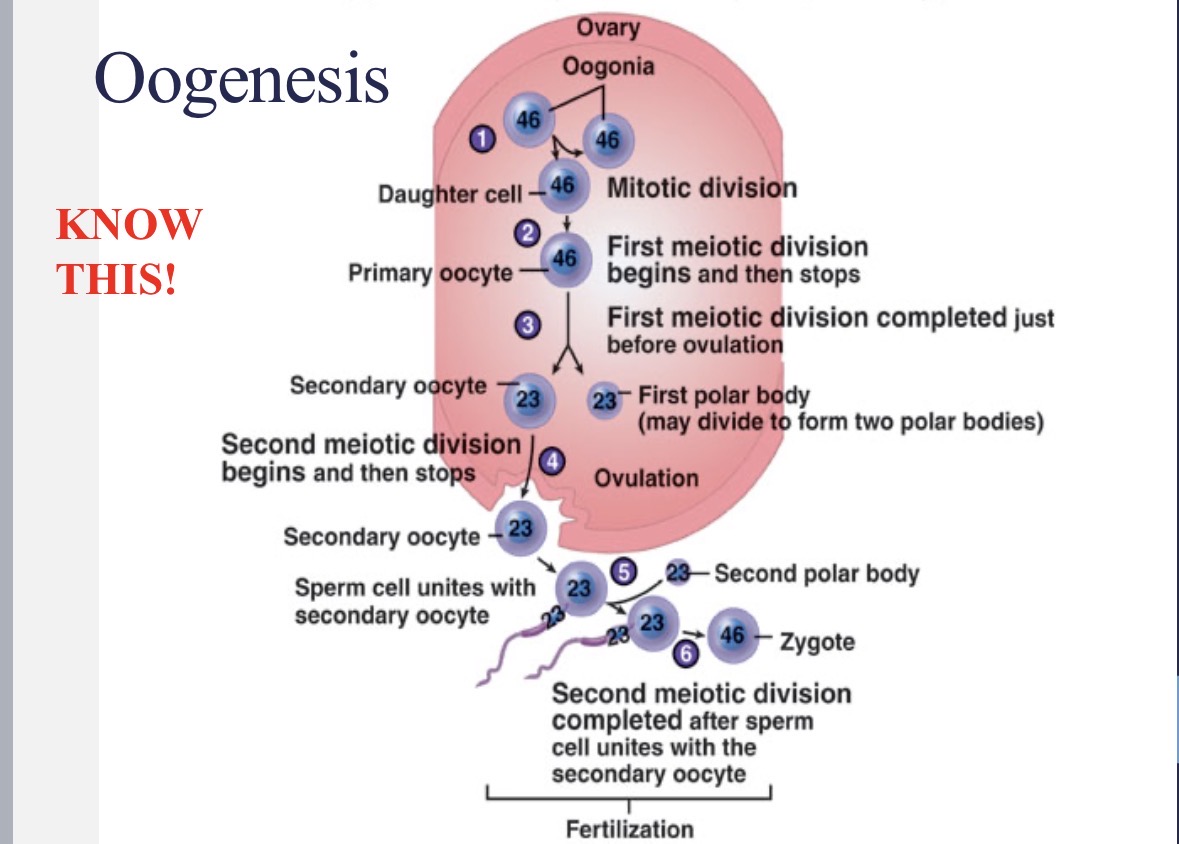
Oogenesis
girls are born with all of their primary ooctyes in Prophase I of meiosis
every month after puberty until menopause, a primary oocyte continues with meiosis I and meiosis II to develop into a secondary ooctye
ovulation occurs at Metaphase II
meiosis II proceeds through Anaphase II and Telophase II if the egg is fertilized
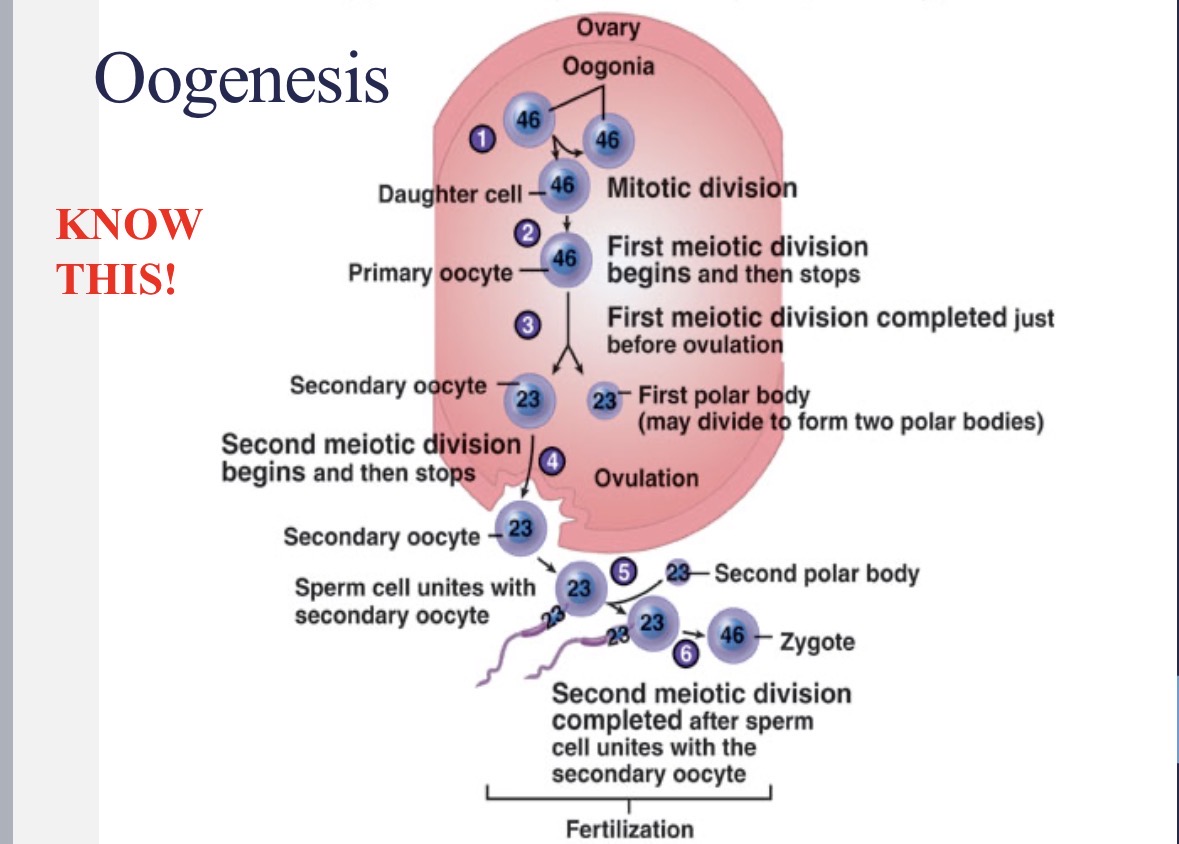
Oogenesis flow chart
1 - oogonium (46 chr.) → 1 - primary oocyte (46 chr.) → 1 - secondary oocyte (23 chr. + 1 polar body) → 1 - mature ovum (23 chr. + 3 polar bodies)
before birth in ovary: oogonium → secondary oocyte
monthly in oviduct: mature ovum
Male hormonal regulation
Sertoli cell inhibin (hormone) negatively feeds back to hypothalamus and anterior pituitary in males to inhibit sperm production
Menstruation
periodic discharge of blood and fluid from uterus
caused by low levels of estrogen and progesterone at end of monthly cycle (hormone withdrawal)
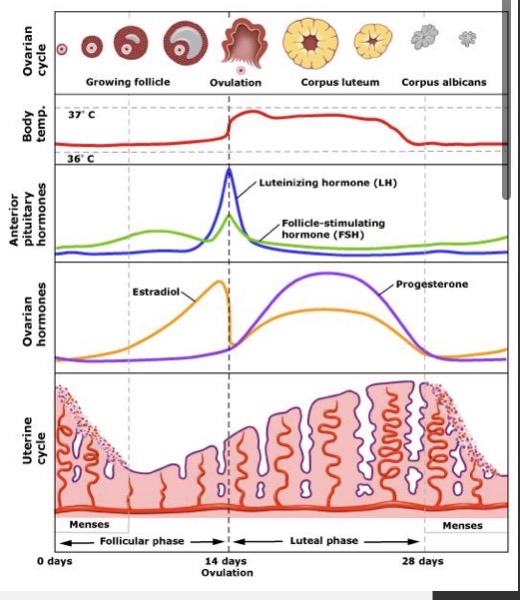
Menstrual cycle
repetitive sequence of shedding the uterine lining (menstruation), development and release of egg (ovulation), and replacement of the endometrium
continues from puberty to menopause
What are uterine contractions triggered by?
by prostaglandins
cause much of the pain felt during menstrual cramps
contractions inhibit blood flow to the lining of the uterus (endometrium)
Flow phase
day 1-5
marked by the shedding of endometrial lining
triggered by a decrease in ovarian hormones (esp. progesterone) → stimulates FSH & LH from pituitary
corpus luteum degenerates forming corpus albicans
low hormone levels → headaches, cramps, nausea, mood changes
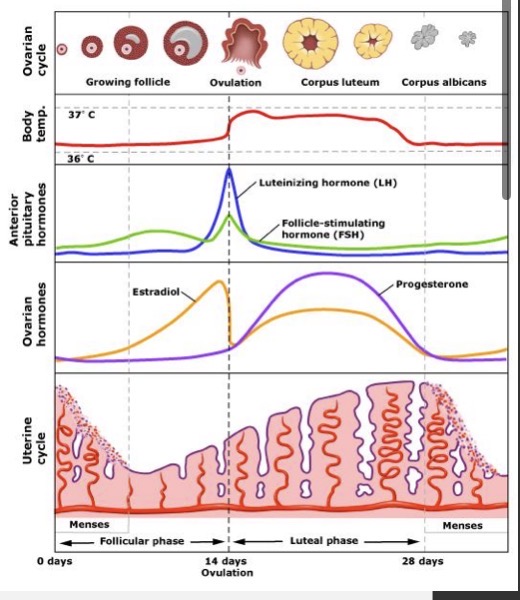
Follicular phase
day 6-13
until ovulation
governed by estrogen released by developing follicle (which is stimulated by FSH)
endometrial lining thickens (estrogen)
FSH decreases (negative feedback from estrogen)
LH production increases (positive feedback by estrogen)
follicle matures
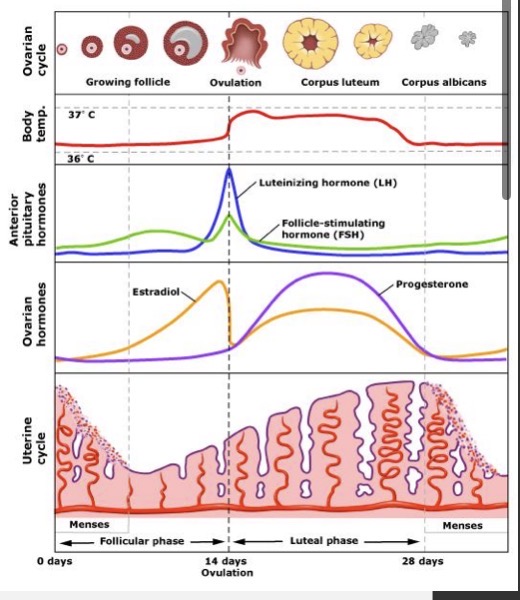
Ovulation
day 14
estrogen peaks just before
LH & FSH peaks at ovulation
follicle erupts
ovum is released into the fallopian tube
female’s temperature peaks (contraceptive method or to help in impregnation)
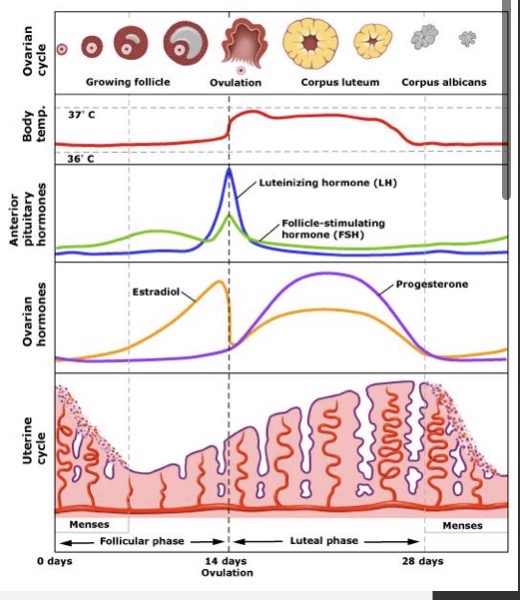
Luteal phase
day 15-28
corpus luteum develops
until menstruation
governed by progesterone released by the corpus luteum (stimulated by LH)
further ovulation and uterine contractions are inhibited (progesterone)
endometrial lining continues to thicken (preparing for pregnancy) → progesterone and estrogen from corpus luteum
progesterone and estrogen inhibit LH release (negative feedback) → corpus luteum starts to degenerate = breakdown of endometrium = flow phase
3 things to remember about female hormones
drop in progesterone = menstruation OR miscarriage
peak/spike/increase in LH = positive ovulation test (for trying to get pregnant)
peak/spike/increase in HCG = positive pregnancy test as it is ONLY made by cells in the placenta
detected via urine/blood test
Tubal ligation
tying or cutting of the tubes
method of “permanent” birth control
How is cervical cancer tested for?
PAP smear
sampling cells
looking for signs of irregular cells
Endometriosis
sometimes debilitating disease caused by endometrial lining forming inside the abdominal cavity (and is still shed monthly)
How do birth control pills work?
prevent ovulation through increased progesterone levels which inhibits the hormonal release of GnRH, FSH, and LH
What determines the degree of secondary sex characteristics?
the relative quantities of androgens and estrogens present in BOTH males and females
Ectopic pregnancies
result from implantation in the fallopian tube instead of the uterus
pregnancy will rupture the fallopian tube if allowed to continue
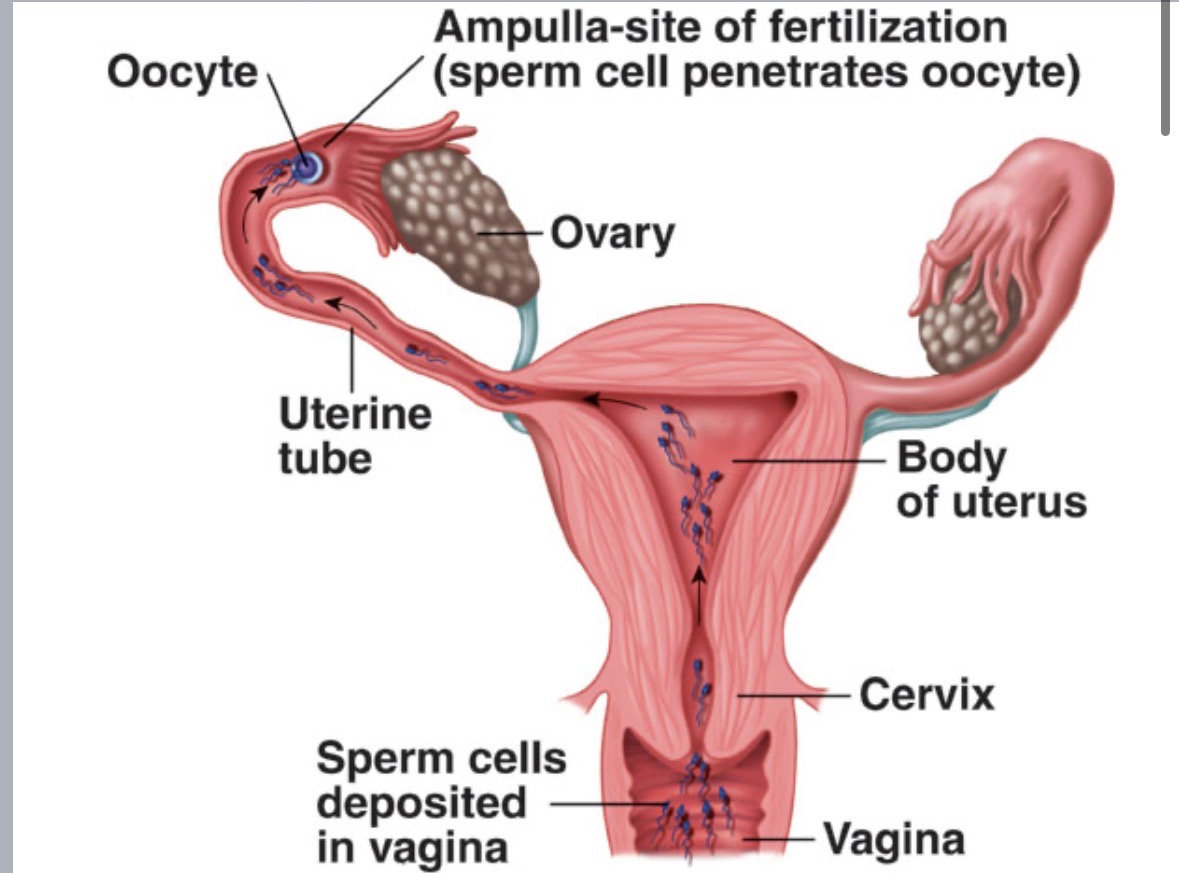
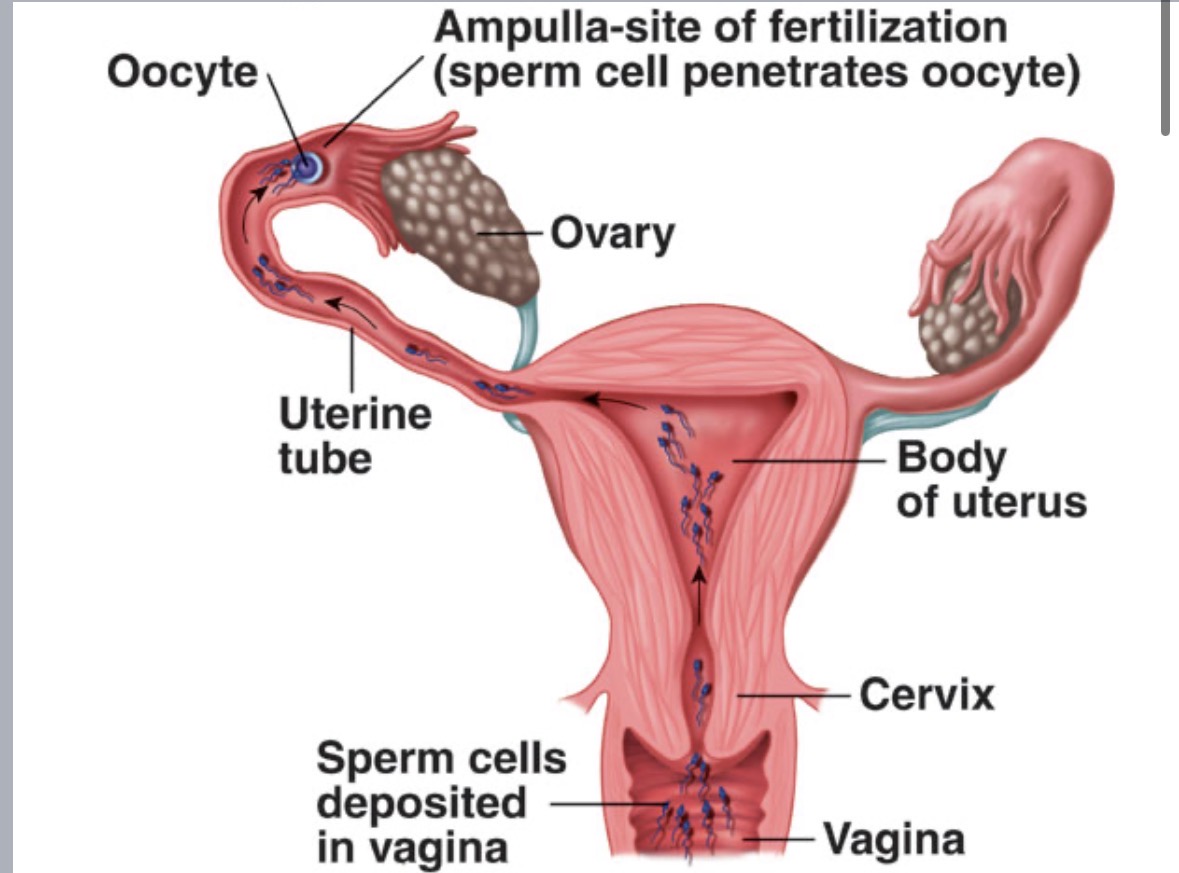
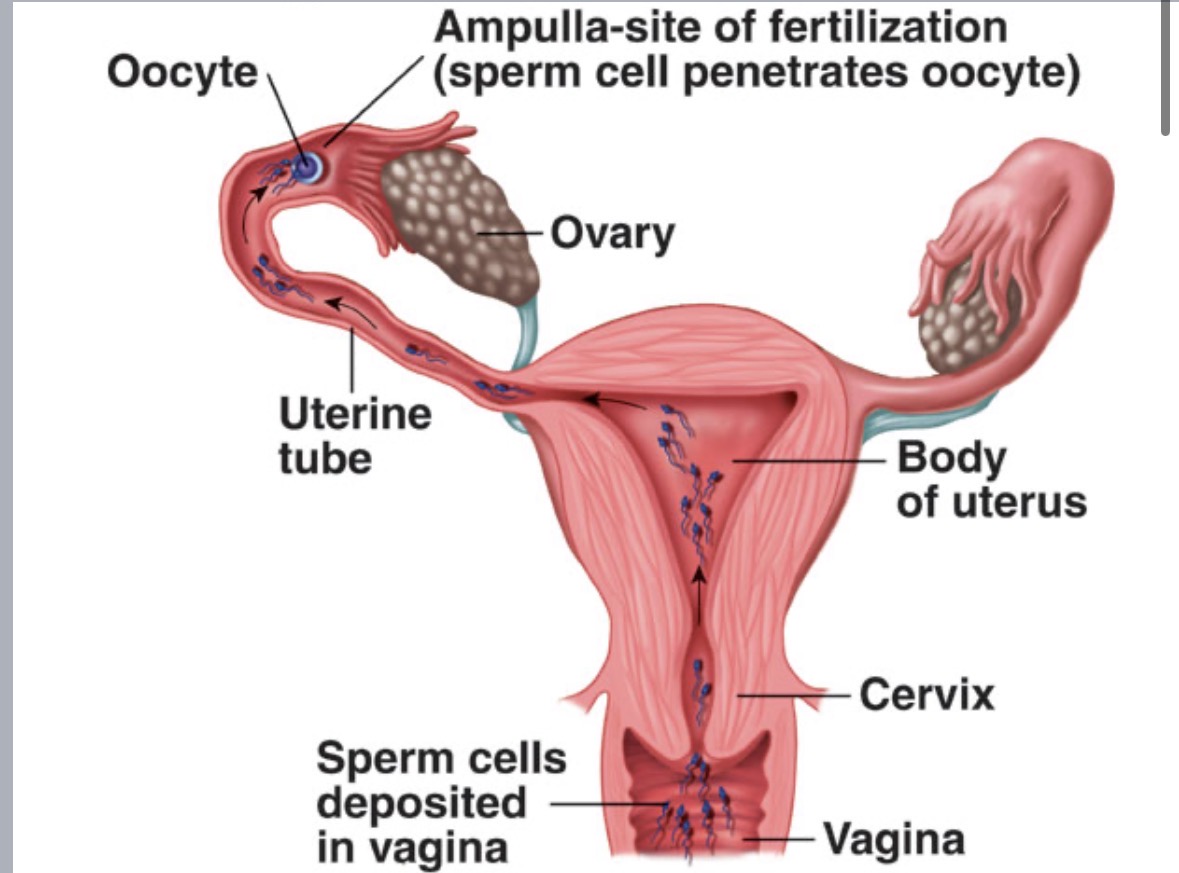
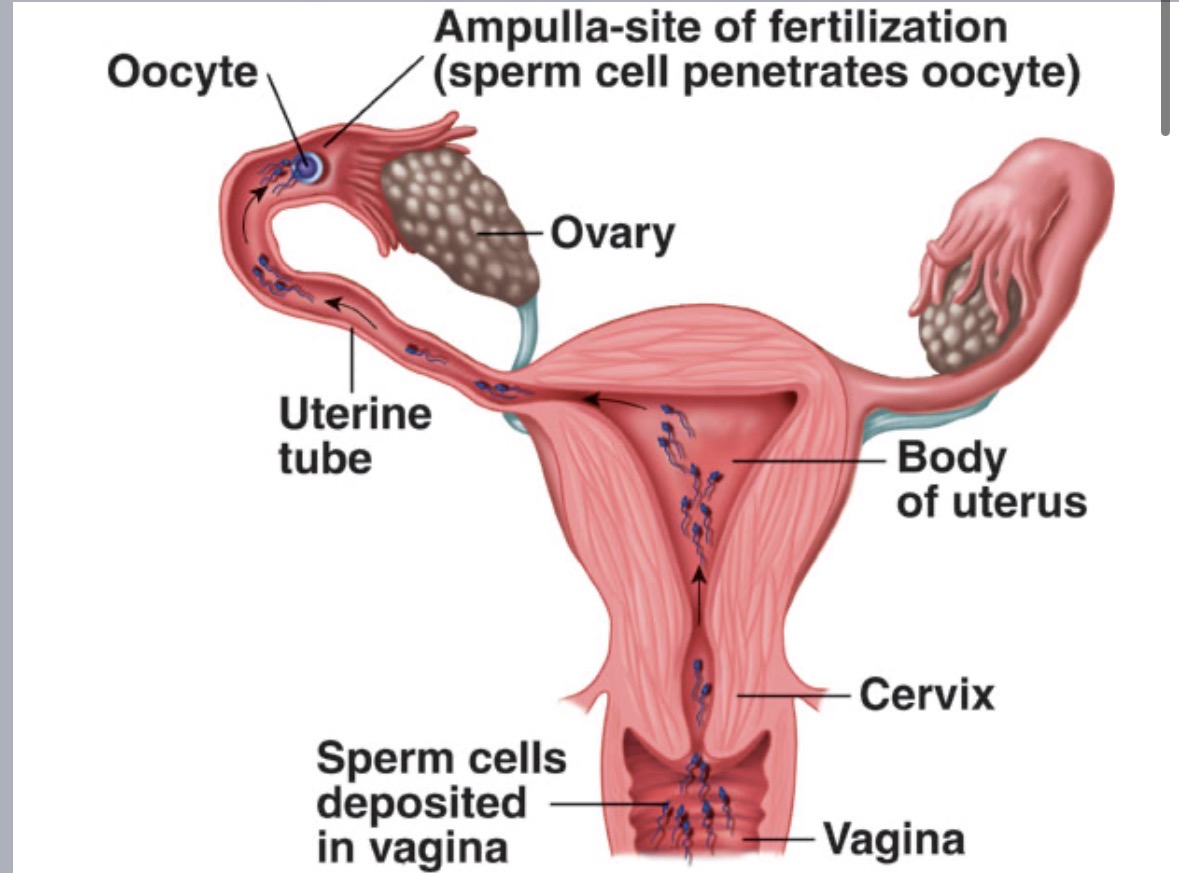
Male perspective of fertilization
several hundred million sperm released into vagina per ejaculation
many sperm destroyed by vaginal acidity
sperm then travel up vagina (cervix → uterus → oviduct (fallopian tube))
Fertilization
only a few dozen to a few hundred sperm survive to reach egg
usually occurs in a single oviduct (fallopian tube)
head of one sperm cell penetrates egg plasma membrane → triggers completion of meiosis II in egg → sperm nucleus (n=23) & egg nucleus (n=23) → formation of zygote (2n=46)
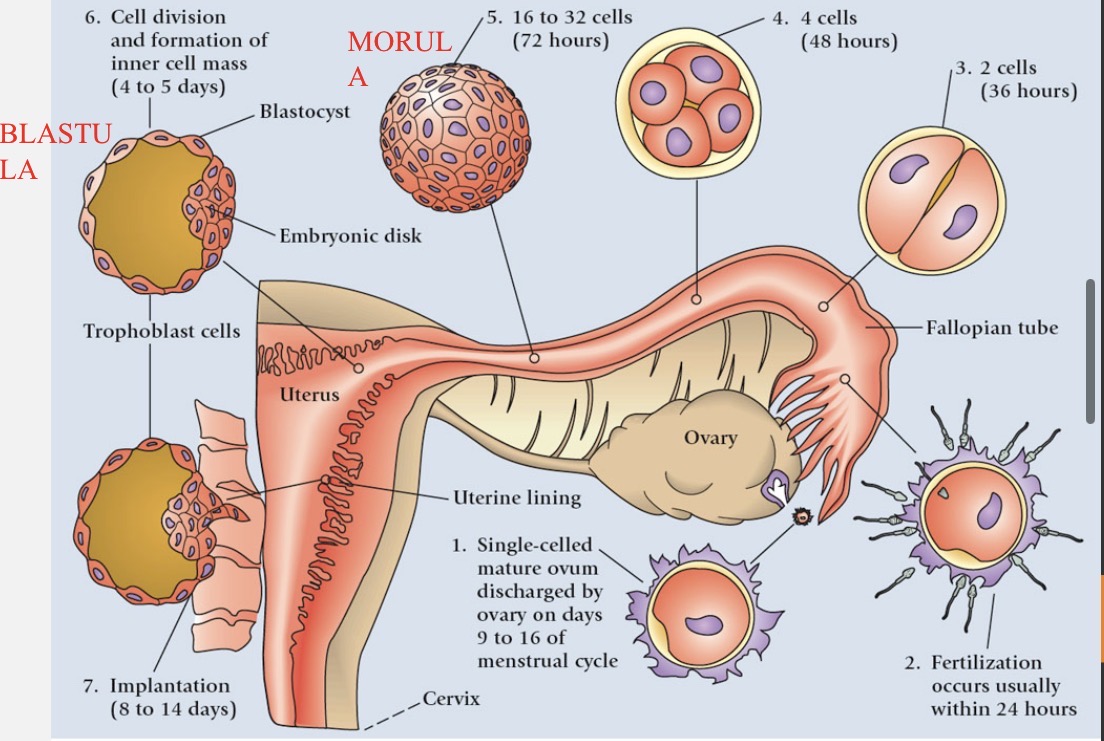
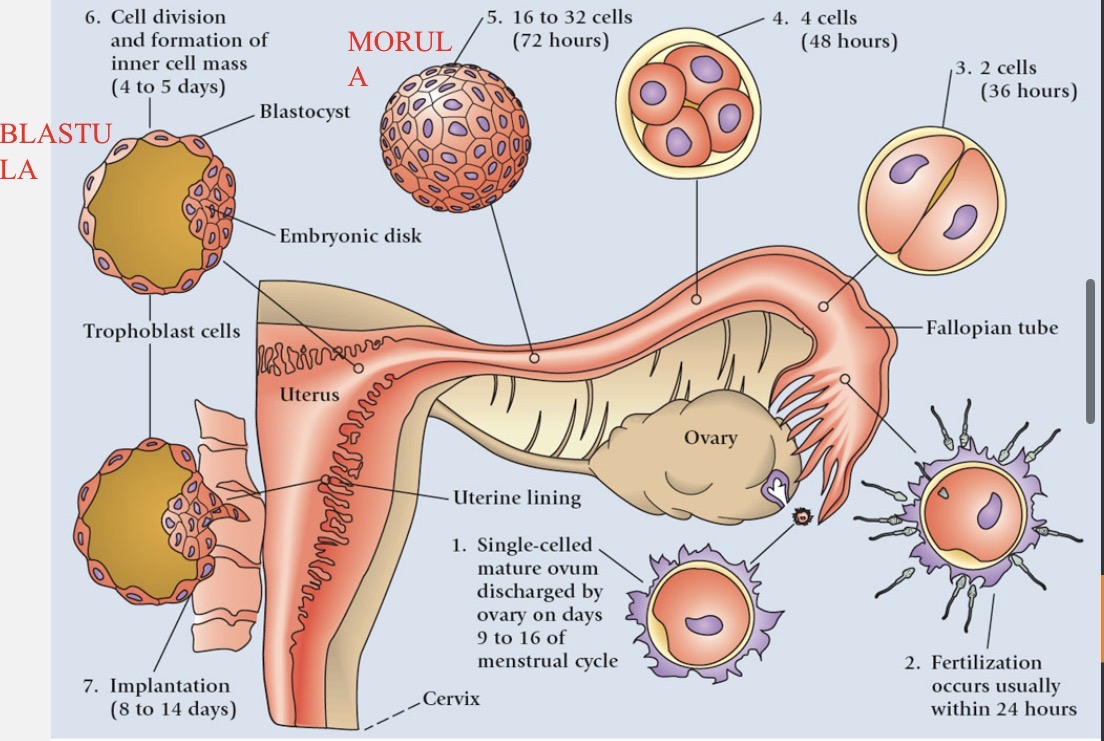
Cleavage process
zygote (~0.1 mm) undergoes first mitotic division within 30 hours of fertilization as it travels down oviduct
2 cells → 4 cells → 8 cells (stays the same size)
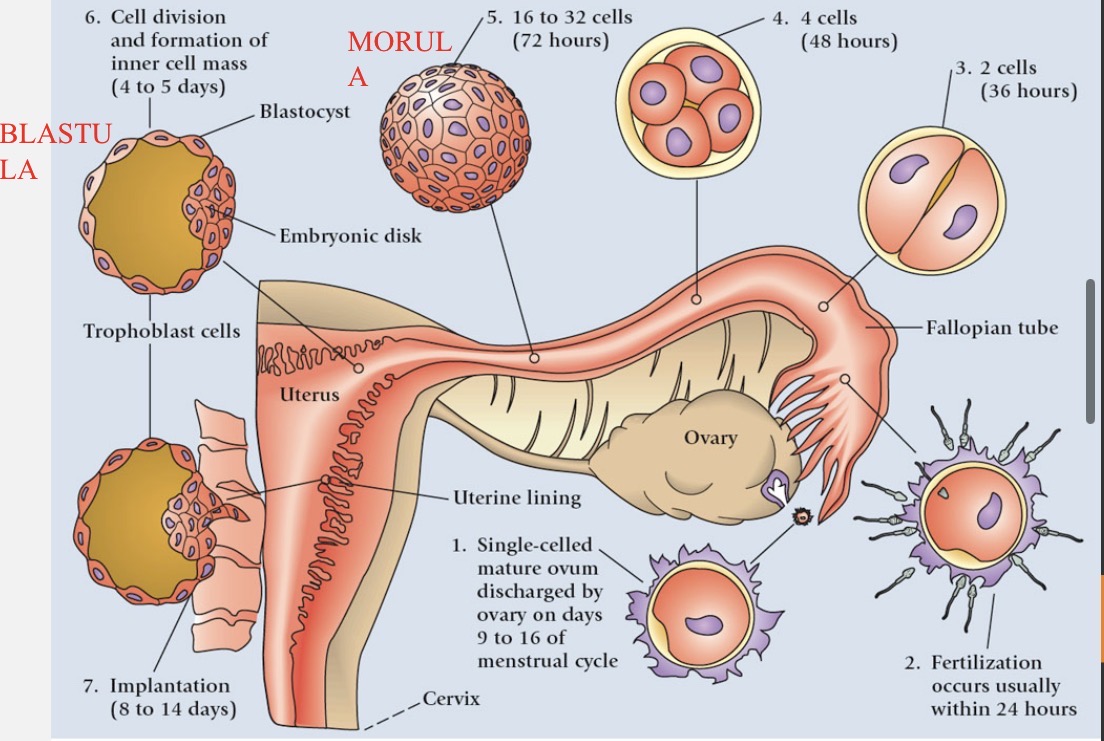
Blastocyst formation
morula (16 cells) reaches uterus 3-5 days after fertilization
fills with uterine fluid and two different groups of cells form a sphere called a blastocyst (blastula)
inner blastocyst → becomes embryo
outer cells (trophoblast) → become chorion → eventually forms placenta
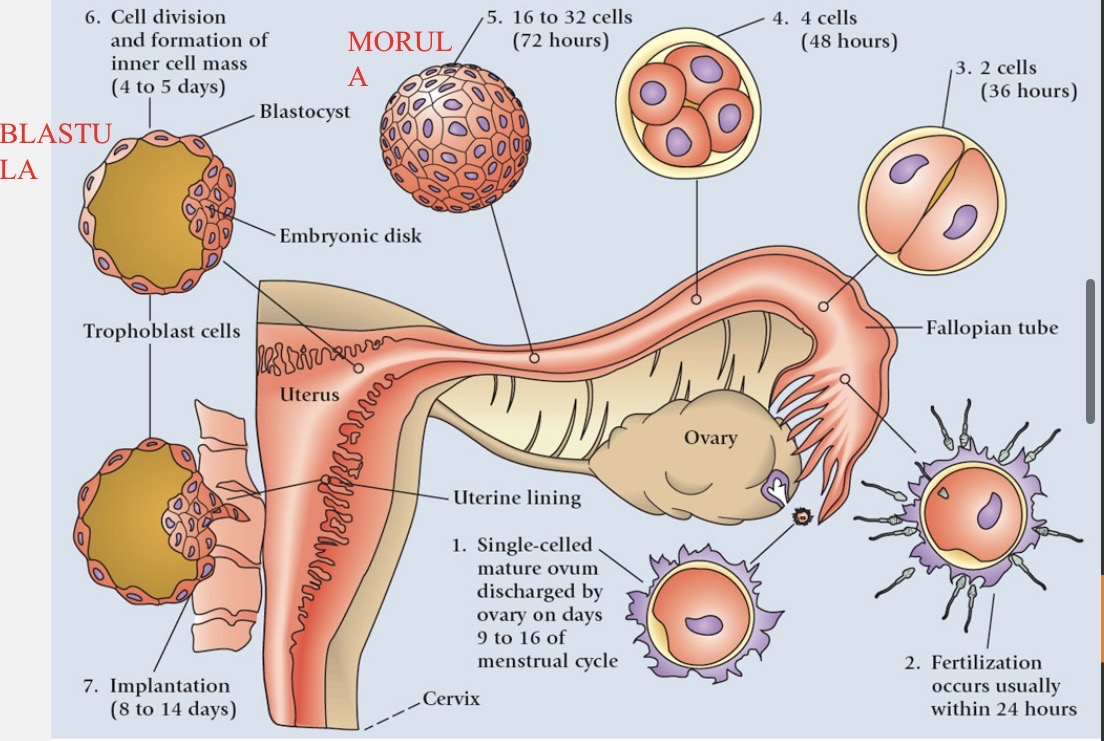
What does implantation result in/mean?
pregnancy
hCG
human chorionic gonadotropic hormone secreted by outer cells (chorion) of blastocyst to maintain corpus luteum
maintains levels of progesterone and estrogen
maintain endometrium
used in pregnancy tests
Gastrulation
formation of 3 primary germ layers of blastocyst in 2nd week
meso-, ecto-, & endoderm
developing embryo → gastrula
start of morphogenesis → differentiation = cell specialization
considered an embryo after implantation is complete (2 weeks after fertilization)
Neuralation
folding process where neural plate becomes neural tube which eventually develops into the brain and spinal cord
Organ formation
weeks 3-8
organs form from primary germ layers (not fully functional)
ecto/meso/endoderms
Ectoderm
nervous system
epidermis (closest to amniotic cavity)
Mesoderm
skeleton
muscles
reproductive structures
middle layer
Endoderm
lining of digestive & respiratory systems
endocrine glands
inner layer
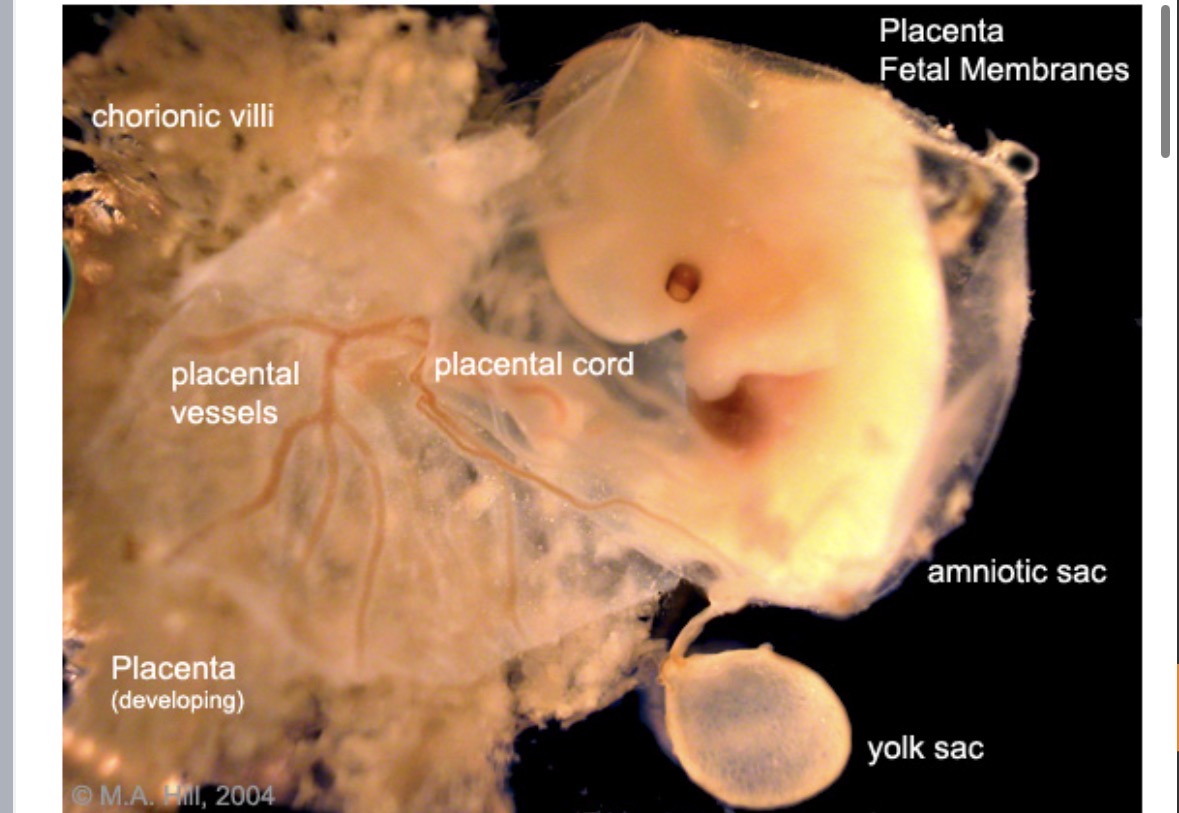
Amnion
forms fluid filled sac (amniotic cavity) → insulation and protection against dehydration, impact, infection, temp. changes, etc.
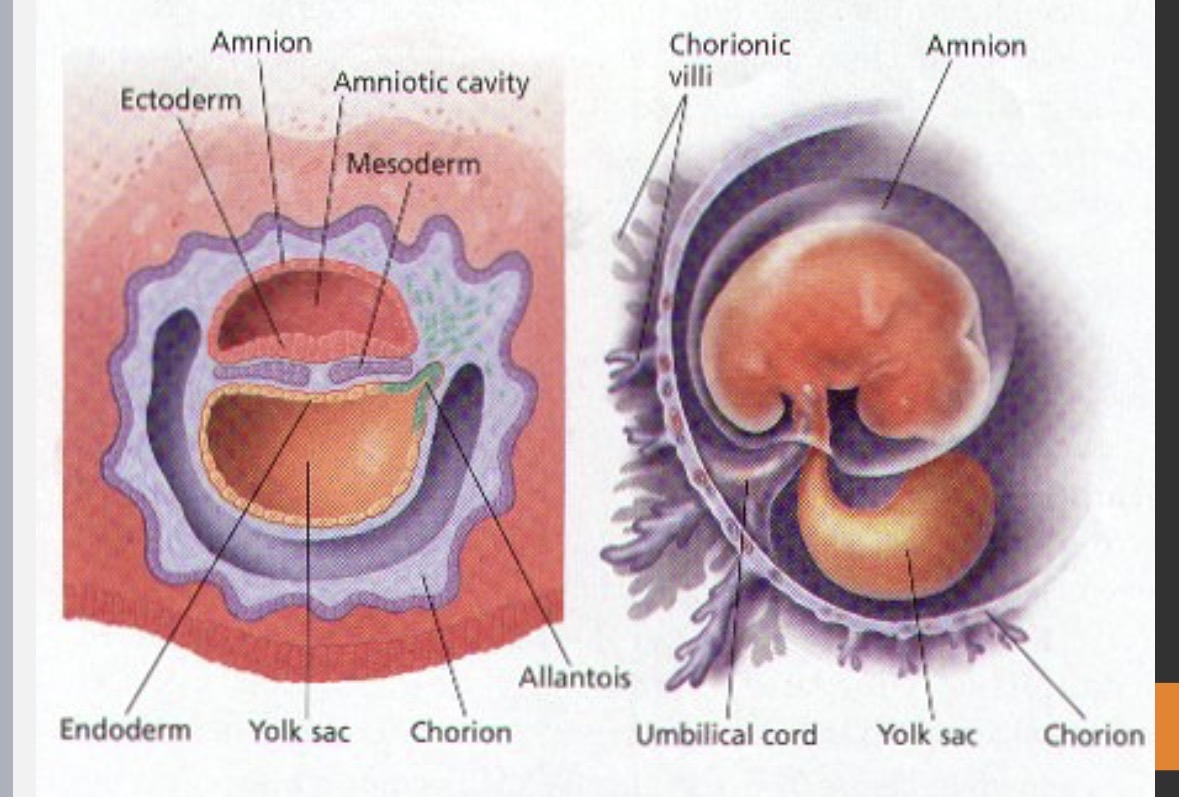
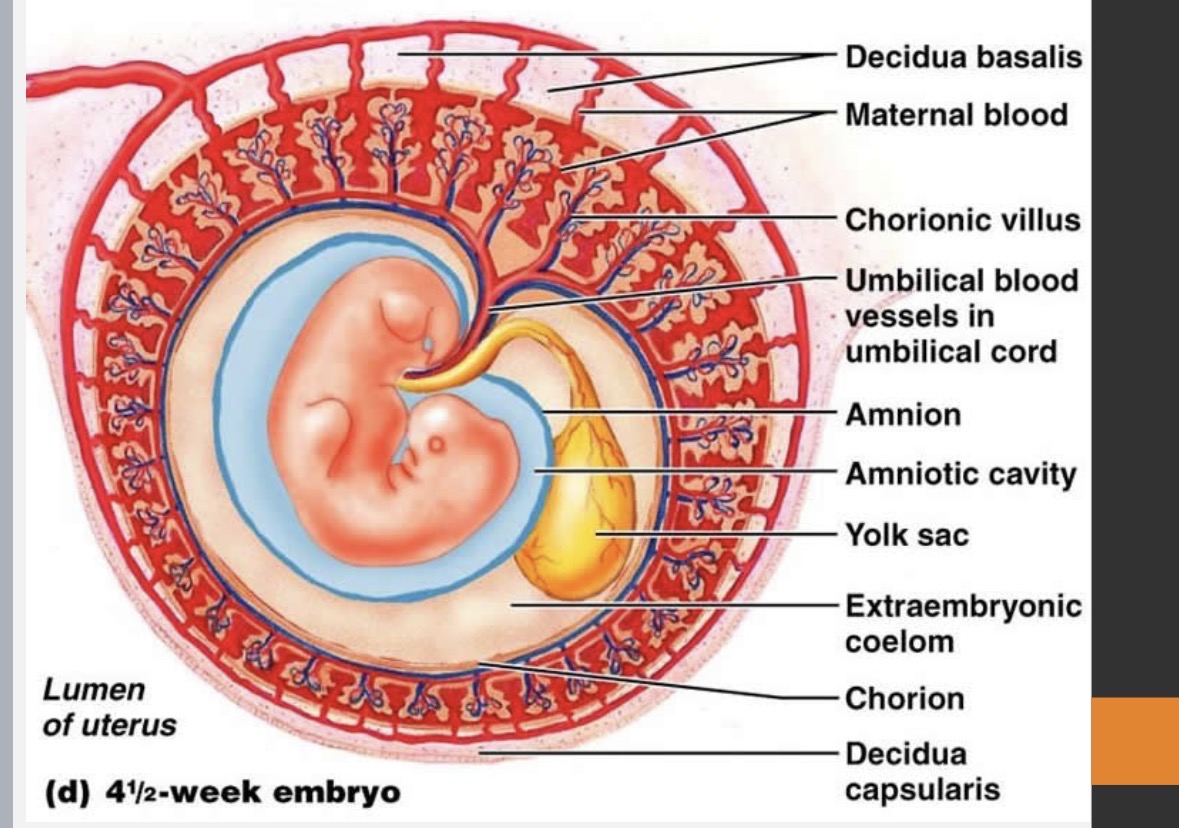
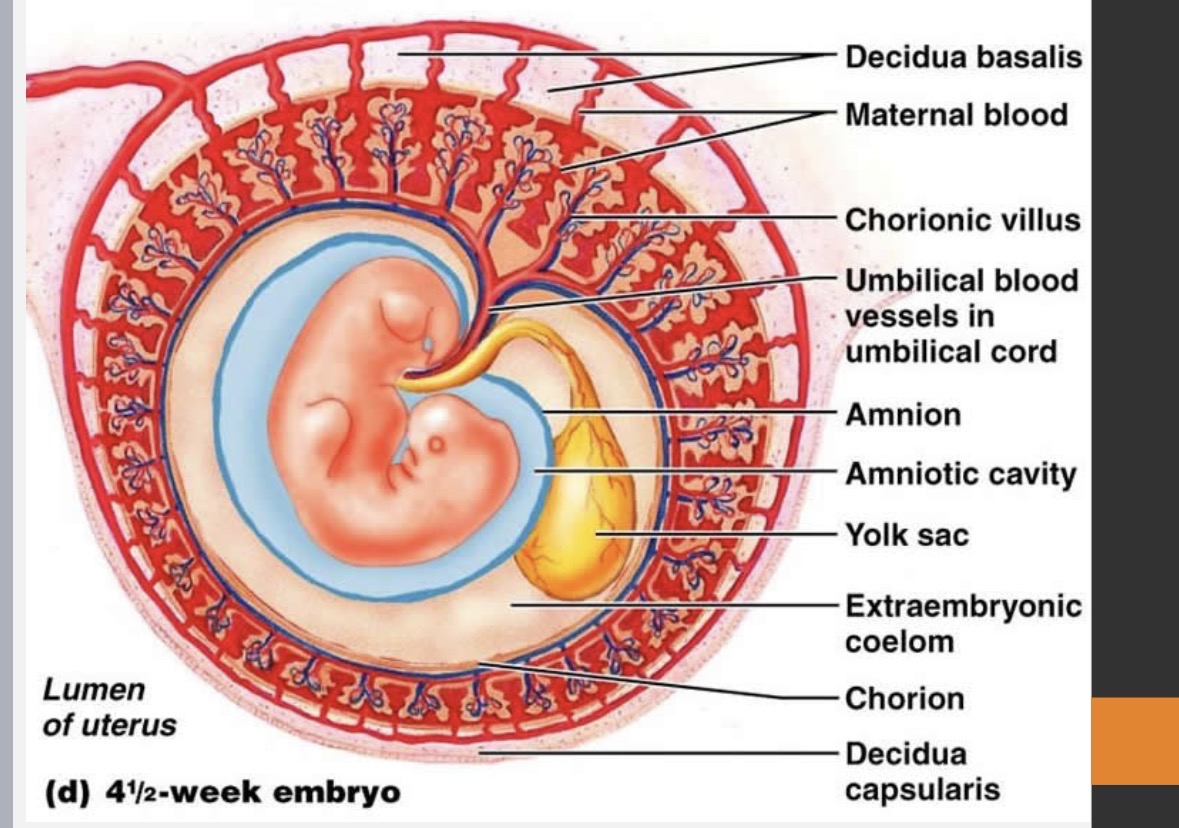
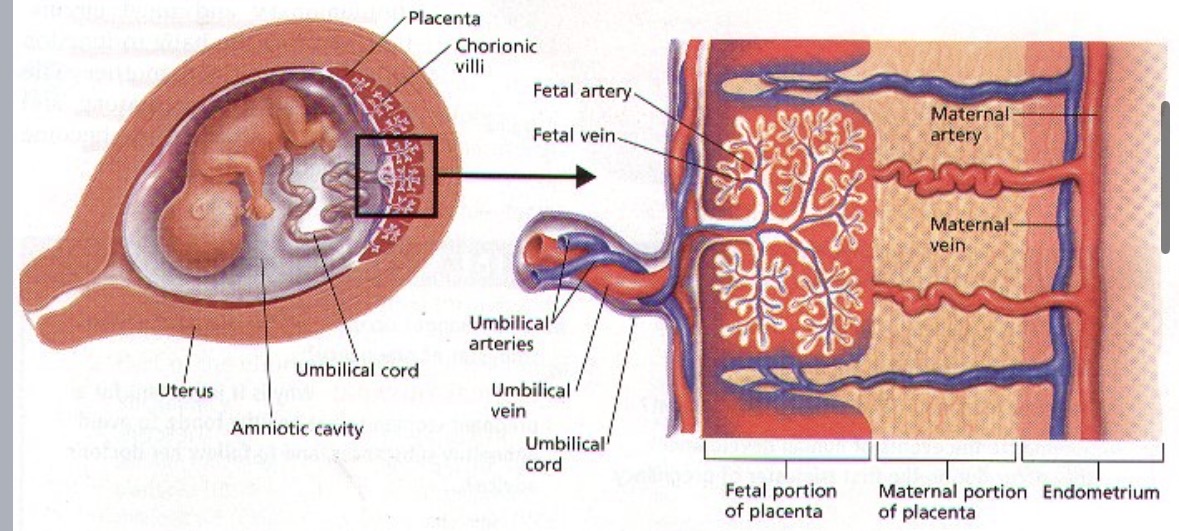
Chorion
chorionic villi invade endometrium → allows for transfer of nutrients/waste between maternal blood and fetal blood
becomes placenta
Allantois
initial source of nutrients in first 5 weeks
forms umbilical cord
1st trimester
weeks 1-13
fertilization to the end of 3rd month
2nd week → germ layers form
1 month → 7 mm
8th week → considered fetus
9th week → movement occurs & heart/brain formed
10th week → heart beat, limb buds w/ fingers/toes present, placenta & umbilical cord develop, and sucking reflex
Placenta
temporary organ
connects developing fetus to uterine wall
responsible for nutrient uptake, waste elimination, and gas exchange via mother’s blood supply
connects to fetus via umbilical cord
Umbilical cord
contains 1 vein and 2 arteries
vein → carries nutrients and oxygen-rich blood TO fetus
arteries → return blood containing waste FROM fetus back to placenta → to mom
2nd trimester
weeks 14-27
17 weeks: sucking and swallowing reflexes, sex identifiable, skin = bright pink and transparent, and soft, downy hair
21 weeks: fetal movement, internal organs maturing, and eyebrows/lids/lashes appear
25 weeks: eyes open occasionally for short periods, skin = protective coating of vernix, and able to hiccup
3rd trimester
weeks 28-40
rapid growth → 350 mm - 530 mm long, mass from 0.68kg to 3.4 kg, and organs mature
7th month: born before 37 weeks = premature, taste buds developed, fat layers forming, and skin = wrinkled and red
8th month: tremendous brain growth, most body organs fully developed (EXCEPT LUNGS), strong movements, kidneys mature, skin is less wrinkled, and fingernails extend beyond fingertips
9th month: respiratory system LAST to develop, digestive system 2nd last to develop, baby fully developed and can survive outside of mother’s body, skin = smooth and pink, and baby in lower abdomen to prepare for birth (less active)
Parturition
birth
uterine contractions signal beginning of labour
cervix thins and dilates (max. 10 cm)
labour starts when contractions are 10-15 mins. apart
amniotic membrane forced into birth canal → often bursts during or before delivery (lubrication and water breaks)
contractions start moving baby through birth canal
Relaxin
produced by placenta
loosens ligaments in pelvis
dilates cervix
Oxytocin
hormone from posterior pituitary
positive feedback loop enhance strength of contractions
synthetic oxytocin → induced labour
stimulates milk release (milk let-down)
shrinks uterus back down after labour
Prolactin
stimulates milk production
Female infertility
failure to ovulate
blockage of reproductive tract
repeated miscarriages
absence/malformation of part of reproductive tract
hormone imbalance
Male infertility
low sperm count
low testosterone/FSH levels
poor sperm motility
absence/malformation of reproductive structure
Effect of STIs
sexually transmitted infections
untreated → scar tissue that cause blockage in males or females
may be asymptomatic
viral and/or bacterial
HPV
human papillomavirus
world’s most common STI overall and most common viral STI
2-3 month incubation period for warts
most are asymptomatic
low-risk strain: genital warts
high-risk strain: pre-cancerous lesions which may lead to cancer (cervical, penile, anal, etc.)
test: pap smear for women
cure: none
prevention: only NEW cases = Gardasil vaccine
Genital herpes (HSV)
herpes simplex virus
2-12 days incubation period
most are asymptomatic
sores on the penis, vagina, anus, butt, thighs, mouth, or finger
test: no good screening
cure: none
treatment: viral medication can EASE symptoms (still able to spread)
may be passed to babies during childbirth
Hepatitis B
contracted through sexual contact or through other contact with bodily fluids or blood
1.5-6 months incubation period
initially flu-like (fever, headache, nausea, etc.)
skin = jaundiced
progress to cirrhosis of liver, liver failure, liver cancer, and death
can cross placenta to infect unborn child
test: blood sample
cure: none
prevention: vaccines for A and B are available
HIV
human immunodeficiency virus
10 year average incubation period (HIV infection → AIDS (Acquired Immune Deficiency Syndrome)
attacks Helper T cells → level decreases → immune system severely damaged → infected person susceptible to opportunistic infections/diseases
progress to AIDS
test: HIV blood test
cure: none (2 children cured)
prevention: working on a vaccine
Chlamydia
most commonly reported bacterial STI in Canada
2-3 weeks incubation period
usually asymptomatic
abnormal discharge from vagina or penis
pain during sex (females) OR burning during urination (males)
untreated → infertility
pelvic inflammatory disease or ectopic pregnancies (females) OR swollen and tender testes/epididymitis (males)
test: urine or swab
cure: antibiotics (damage prior cannot be repaired)
may be passed to babies during childbirth
Antibiotic eye drops
prevent bacterial eye infections that may cause blindness
often due to the same bacteria that cause chlamydia or gonorrhoea or even HSV in women
Gonorrhea
2nd most commonly reported bacterial STI in Canada
1-14 days incubation period
usually asymptomatic
abnormal discharge/bleeding from vagina or penis
pain during sex/urination (females) OR burning during urination (males)
untreated → infertility, disseminated gonococcal infection (DGI)
pelvic inflammatory disease (PID) or ectopic pregnancies (females) OR swollen and tender testes /epididymitis (males)
test: urine or swab
cure: antibiotics (damage prior cannot be repaired)
may be passed to babies during childbirth
Syphilis
least common STI in Canada
10-90 days incubation period (~21 days average)
test: urine or swab
cure: antibiotics (damage prior cannot be repaired)
may be passed to babies during childbirth
Symptoms of syphilis in all stages
primary: chancre (painless sores) may be located on the genitals, lips, anus, etc.
secondary: skin rashes lasting 2-6 weeks
late: mainly neurological
Artificial insemination
man donates sperm → sperm concentrated
two methods:
Intrauterine insemination (IUI): catheter deposits sperm into uterus
Intravaginal insemination (IVI): syringe with sperm inserted into women’s vagina
In-Vitro Fertilization (IVF)
hormone therapy and superovulation → stimulates ovaries to produce numerous mature follicles
eggs extracted surgically or via transvaginal ultrasound
sperm donated
egg and sperm in petri dish → stimulated to fertilize
zygote forms → cleavage → blastocyst inserted via catheter
Surrogacy
mother and father each donate egg and sperm
IVF performed
embryo transfer to surrogate mother
used when female has fertility problems (e.g. no eggs, removal of part/whole uterus, etc.)
How can fetus disorders be determined/tested for?
chorionic villi sampling - can happen early
amniocentesis: remove small sample of amniotic fluid for analysis → 2nd trimester
spina bifida detection
karyotyping to detect a trisomy or monosomy
Who has fetal diagnostics done?
pregnant mothers with high probability of chromosomal abnormalities
higher incidence of non-disjunction during meiosis
people with a family history of genetic disorders/diseases