Case 6: Ronnie Olchuk
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
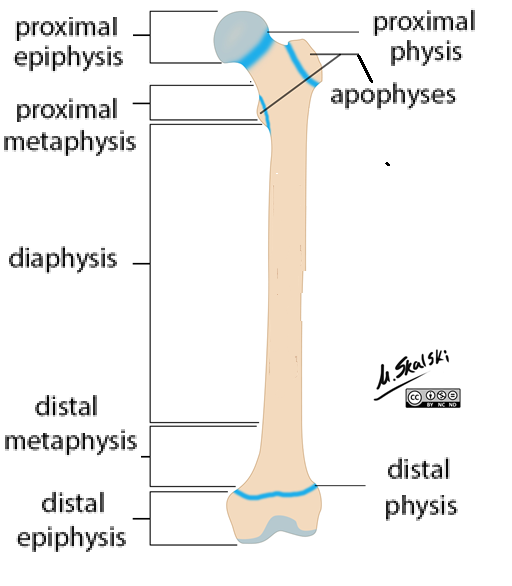
Long Bones: Epiphysis
Proximal + distal ends
Compact bone around trabecular (spongy) bone
Epiphyseal plate (physis)
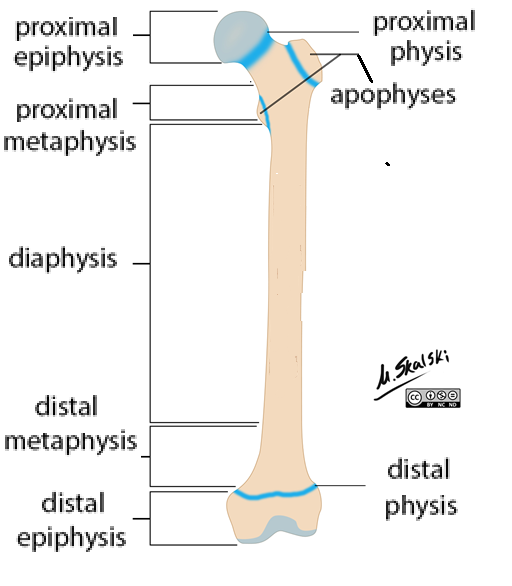
Epiphysis: Physis
Hyaline cartilage between epiphysis + metaphysis
Longitudinal growth location
Closure after puberty = Stop growth
5 layers: Epiphysis → Diaphysis
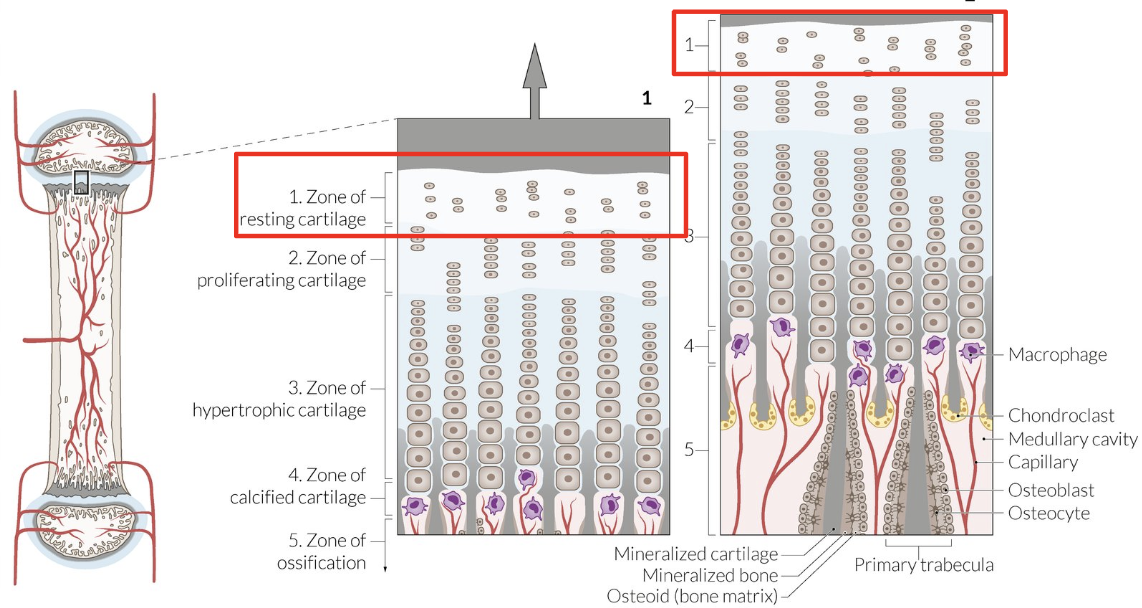
Resting cartilage zone
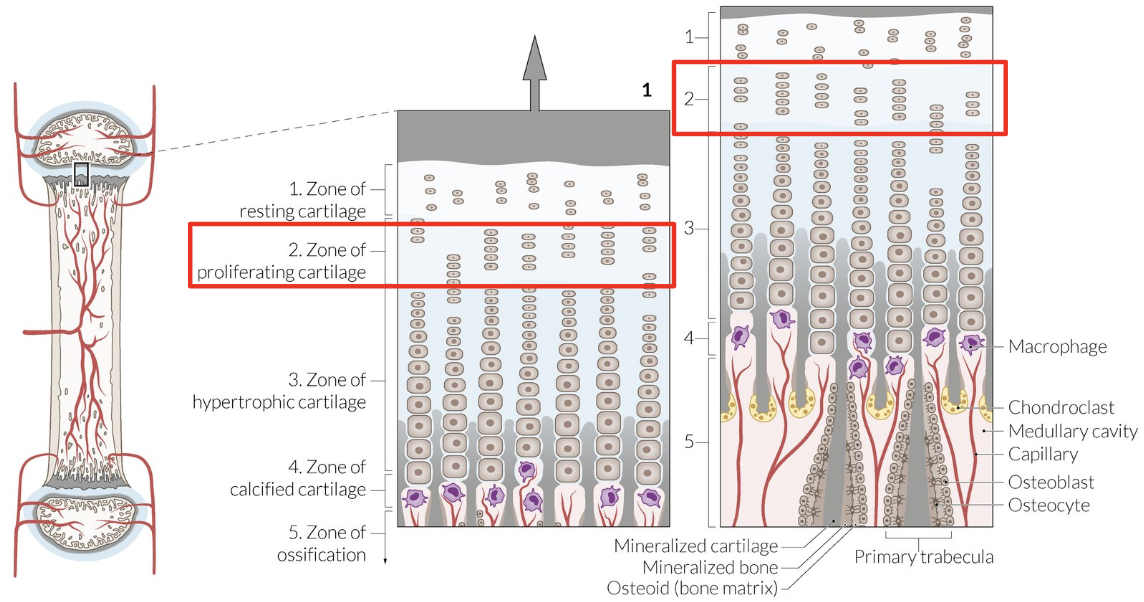
Proliferation zone
Hypertrophy zone
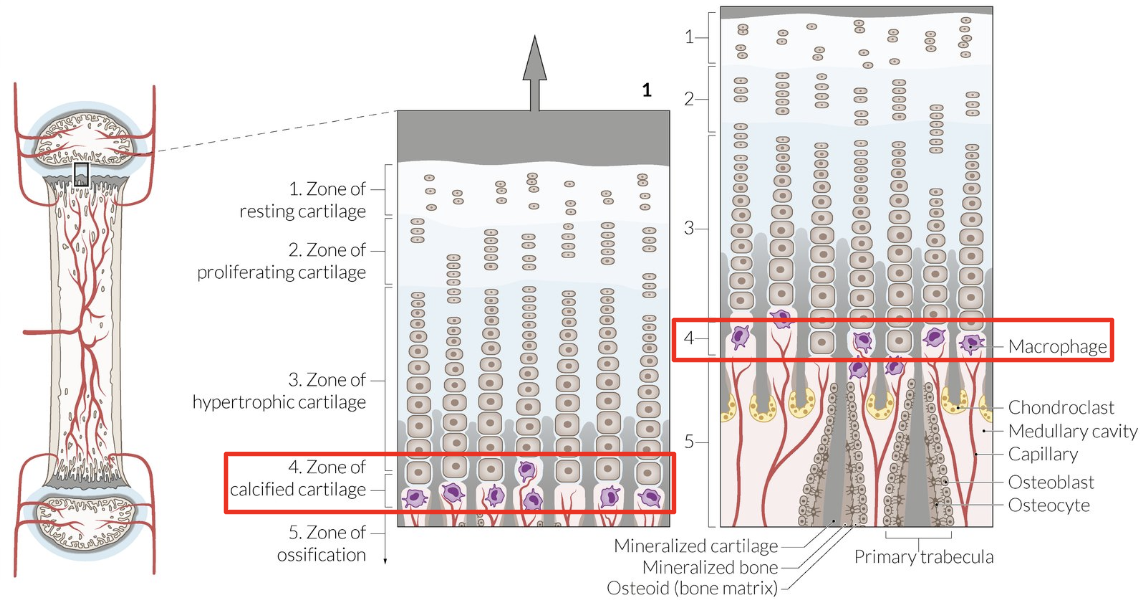
Calcification zone
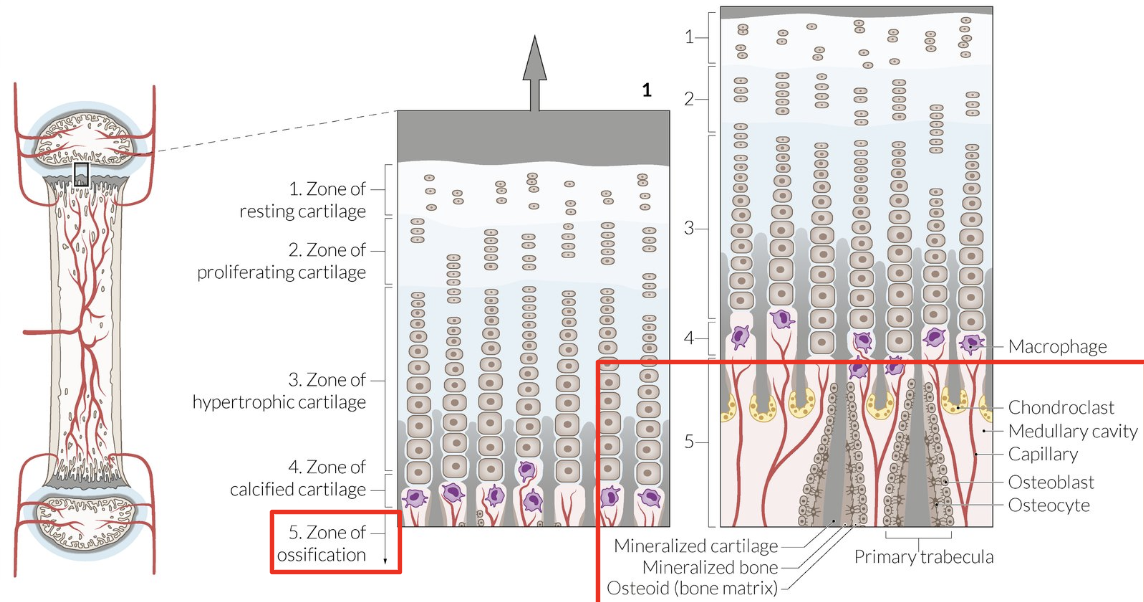
Ossification zone
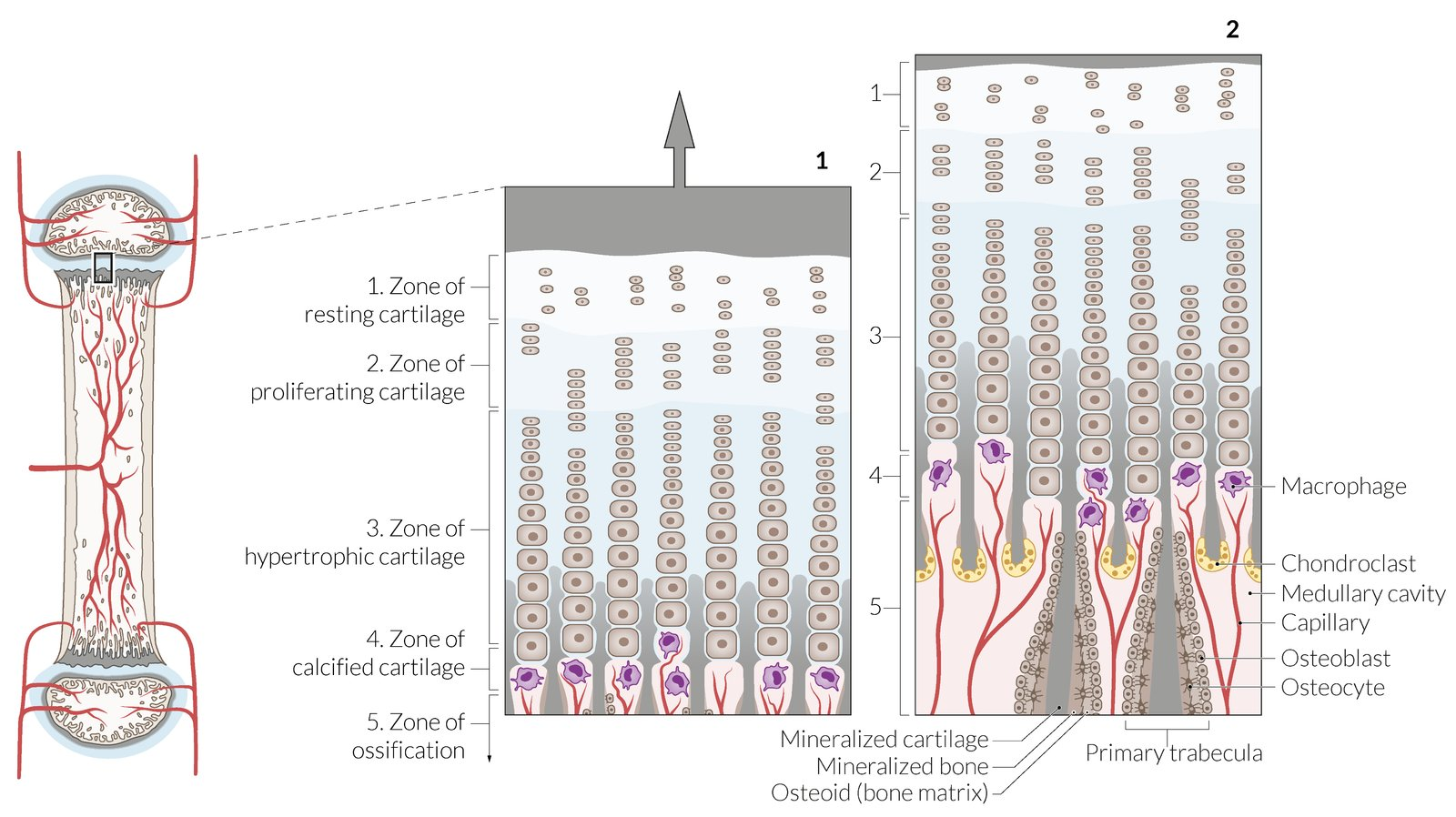
Physis Layer: Resting Cartilage Zone
Undifferentiated precursor chondrocytes
Physis Layer: Proliferation Zone
Chondrocyte mitosis = Cells stack + enlarge = ECM layers
Physis Layer: Hypertrophy Zone
Chondrocyte hypertrophy = Collagen production + longitudinal septa calcification
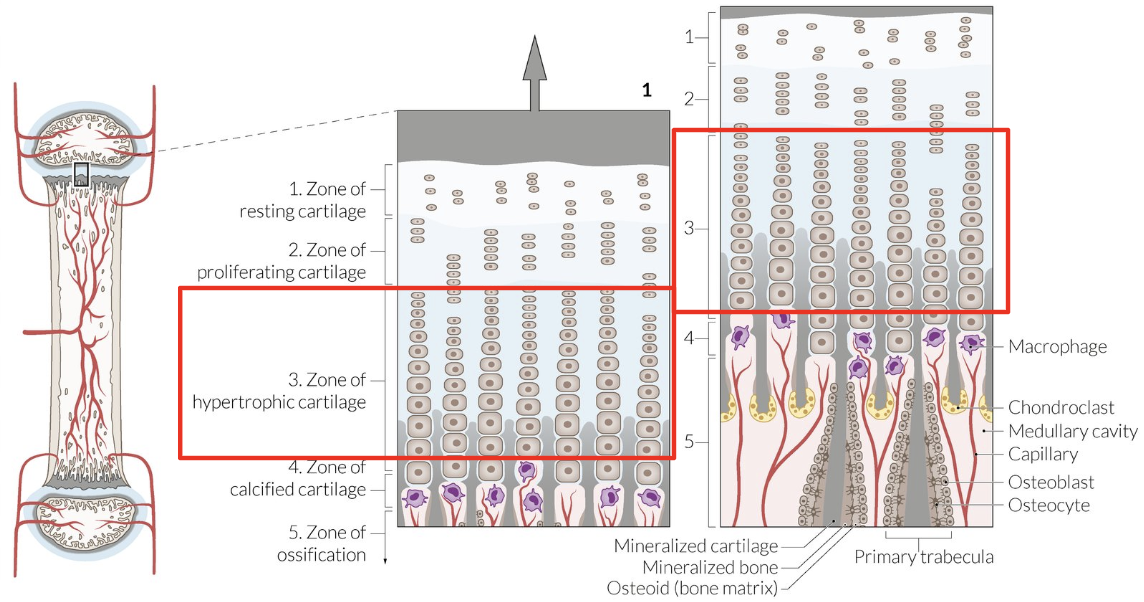
Physis Layer: Calcification Zone
Chondrocyte secrete VEGF + metalloproteinases = Blood vessels + macrophages migrate = Transverse septa erode
Physis Layer: Ossification Zone
Osteoblasts colonize longitudinal septa = Osteoid formation = Mineralization
Long Bones: Metaphysis
Between epiphysis + diaphysis
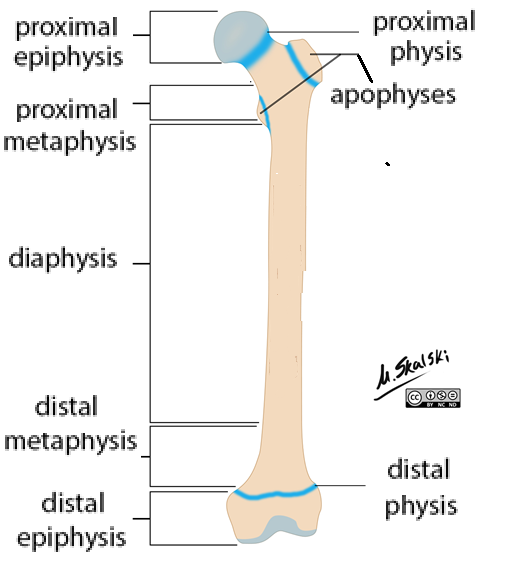
Long Bones: Diaphysis
Shaft
Compact bone around medullary cavity (bone marrow)
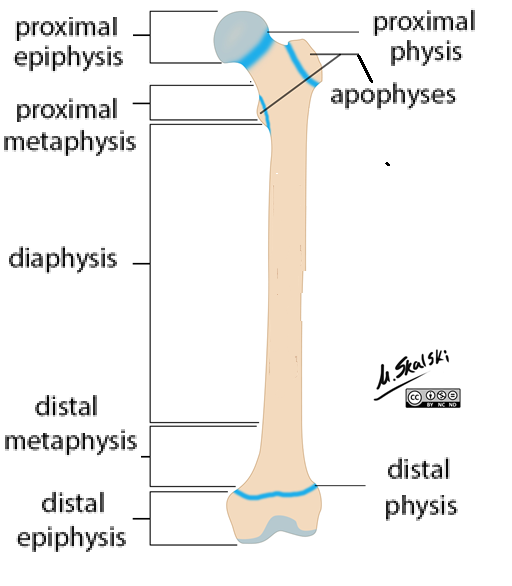
Long Bones: Apophysis
Bony projections
Attach ligaments + tendons
Fractures Classification: Anatomy
Location
Position (dia, meta, epiphysis)
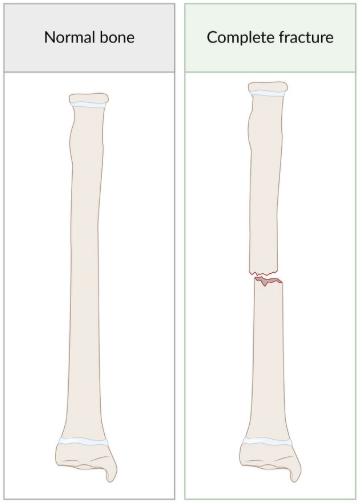
Fractures Classification: Extent
Complete: Fracture line through entire bone
Incomplete: Fracture line not through entire bone
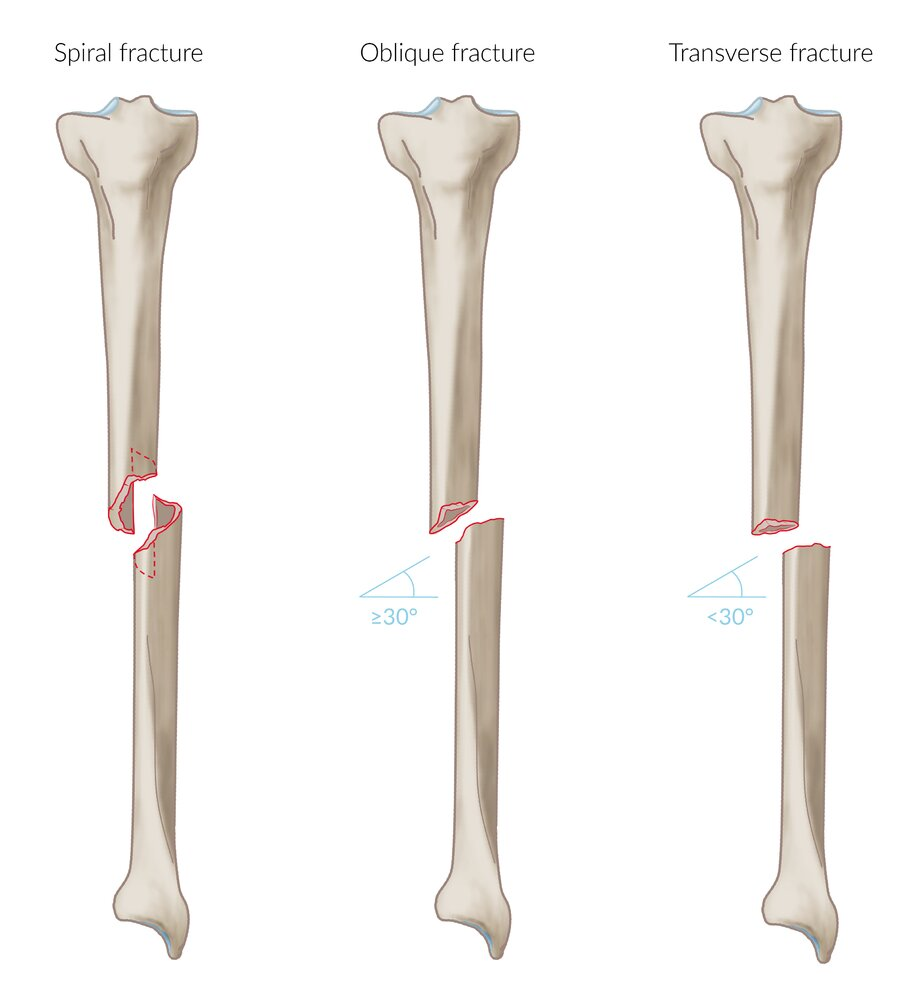
Fractures Classification: Orientation
Transverse: Perpendicular (horizontal) fracture line
Oblique: Diagonal fracture line
Spiral: Twisted fracture line (corkscrew shape)
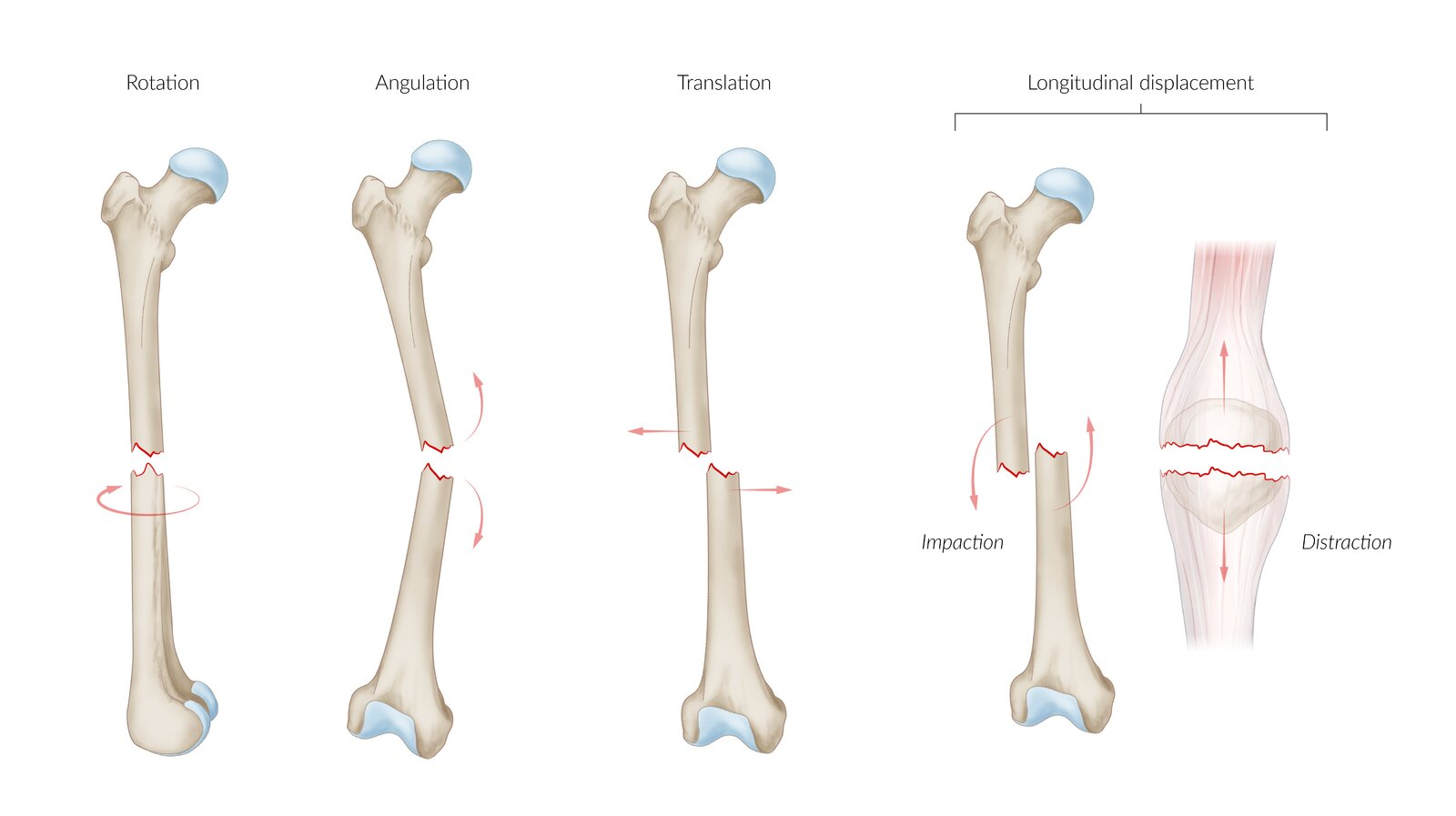
Fractures Classification: Displacement
Angulation: Angled axis
Translation: Lateral bone fragment displacement
Rotation: Around longitudinal axis
Longitudinal bone fragment displacement
Distraction: Elongated
Impaction: Shortened
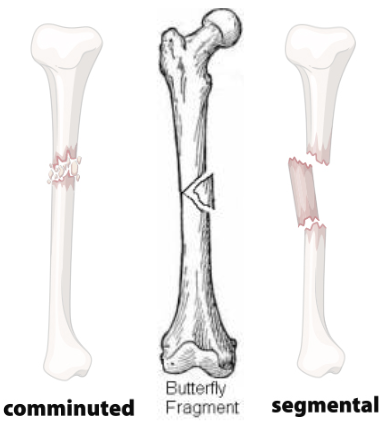
Fracture Classification: Fragmentation
Comminuted: 2+ fracture lines = Multiple bone fragments
Butterfly Fragment: Triangle-shaped fragment
Segmental: 2 fracture lines + bone fragment between proximal + distal bone portions
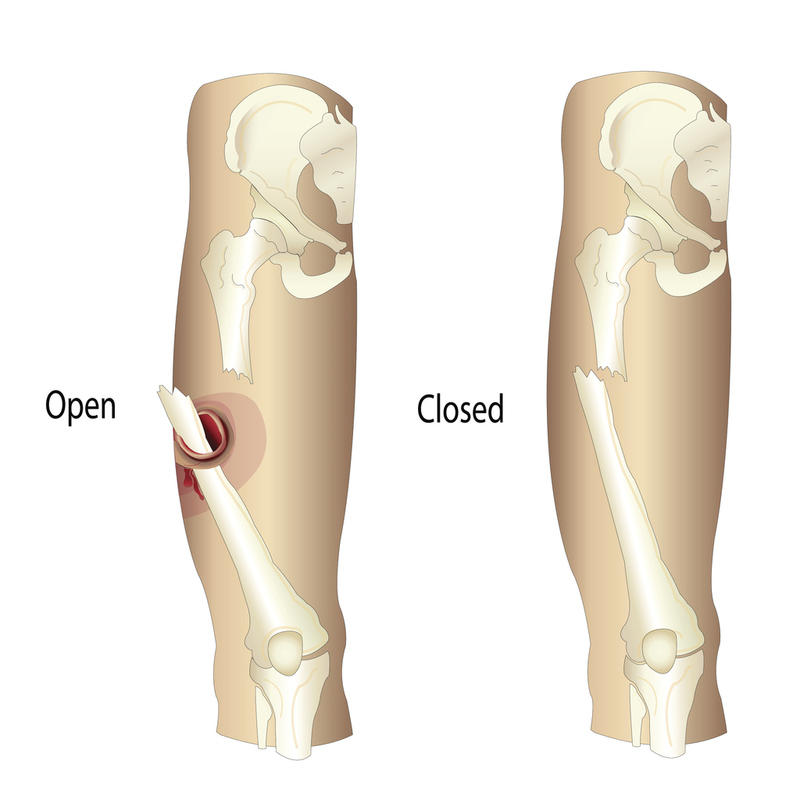
Fracture Classification: Soft Tissue Involvement
Closed/Simple: No contact with outside environment
Compound/Open: Bone/soft tissue contact with outside environment
Fracture Classification: Stability
Stable: Bone fragments in alignment (no significant displacement)
Low dislocation + open fracture risk
Unstable: Bone fragments not in alignment (displaced, misaligned, shifted)
High displacement + healing complication risk
Fracture Acceptable Alignment
Location
Low Tolerance:
Intraarticular
Close to joint
Forearm
High Tolerance:
Diaphyseal
Humerus
Femur
Age: Younger = Increased remodelling capacity
Tolerate higher degree angulation, malrotation, displacement
Fracture Management: Stable Fractures
Closed reduction
Realign displaced fracture/dislocation
Immobilization (cast-splint)
Lower limbs: VTE prophylaxis
Elevation above heart
Ice
Analgesics
Fracture Management: Analgesics
Non-opioid
Acetaminiophen
NSAIDs
Gabapentin (Inhibit Ca2+ channels = Reduce neuropathic pain)
Opioids: Severe pain
Tramadol
Hydrocodone
Fracture Management: Unstable Fractures
Open/closed reduction
Immobilization
External Fixation: Pins/screws outside skin
Internal: Implants (plates, screws, wires)
Fracture Management: Compound Fractures
STAND
S: Stabilize + immobilize
T: Tetanus shot
A: Antibiotic prophylaxis (Ancef)
N: Neurovascular exam
D: Dressing
Acute wound management
Remove foreign bodies + debris
Irrigate wound
Cover with dressing
Operative irrigation + debridement (remove dead tissue)
≤ 24h
Pediatric Fractures: Description
Fractures in children
Pediatric vs Adult Fractures
Pediatric: Softer bones = Different fracture patterns
Physeal: Involving growth plate (Salter-Harris fractures)
Non-Physeal: Not involving growth plate
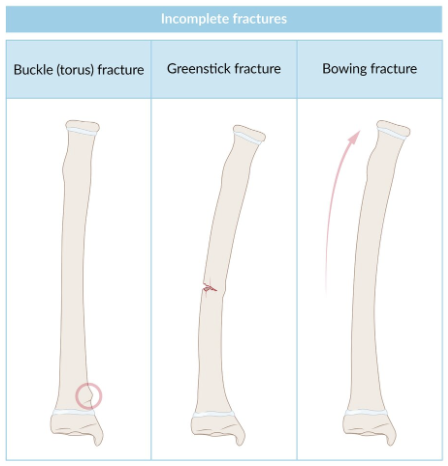
Bowing
Buckle/torus
Greenstick
Adults:
Intraarticular fractures (crossing joints)
Comminuted fractures
Pediatric Fractures: Epidemiology
Physeal: Beginning of puberty
Pediatric Fractures: Etiology
Non-Physeal: Indirect axial force (FOOSH)
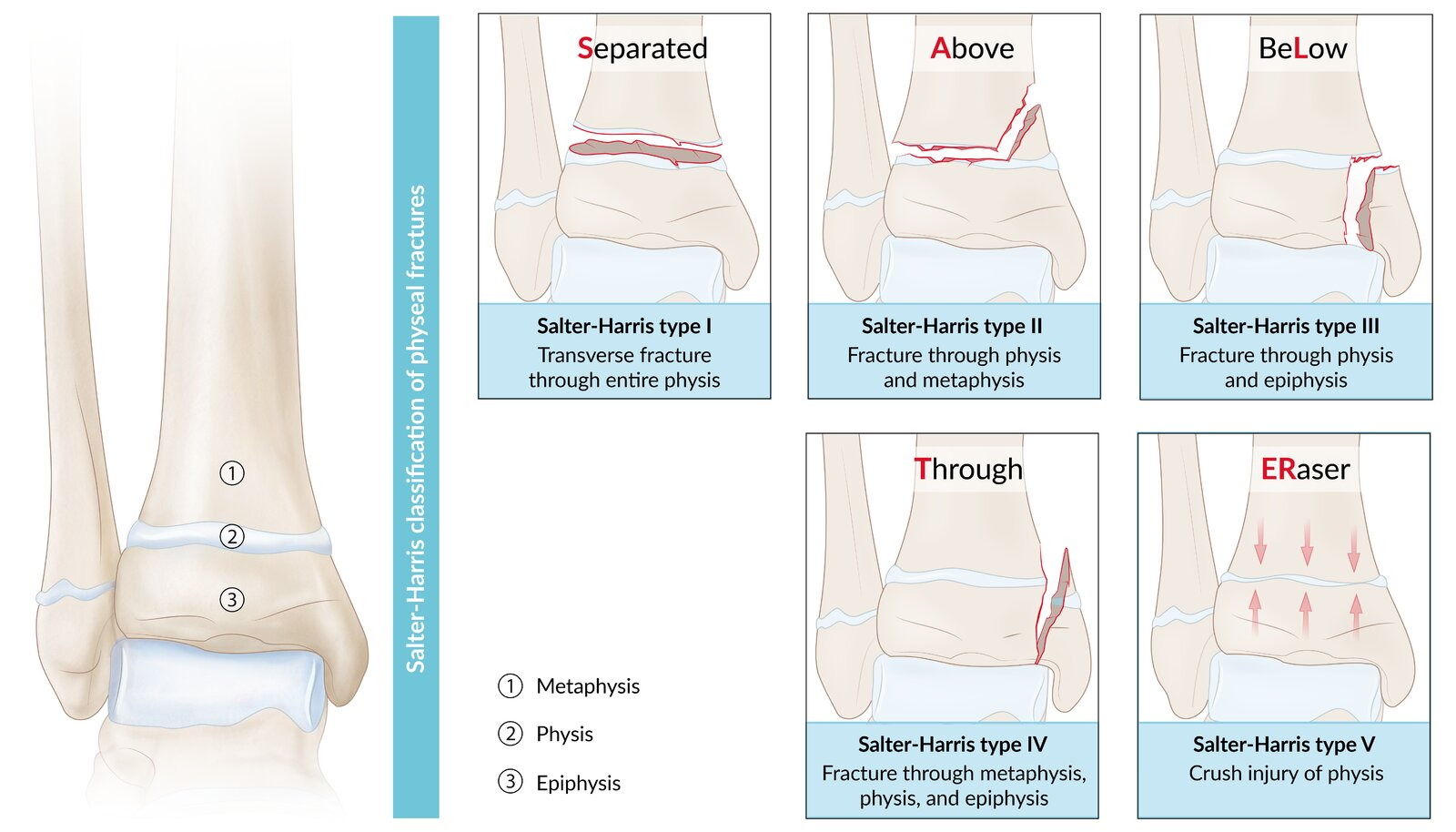
Pediatric Physeal Fractures: Pathophysiology
Salter-harris fractures: SALTER
Type 1: Straight across joint
Transverse fracture through physis
Separate epiphysis from metaphysis
Type 2: Above joint
Transverse fracture through physis + metaphysis
Most common
Type 3: Lower
Transverse fracture through physis + epiphysis
Type 4: Through everything
Fracture through physis + epiphysis + metaphysis
Intraarticular fracture
Type 5: Ruined/rammed
Crush injury from compression
Pediatric Non-Physeal Fracture: Pathophysiology
Bowing: Bone bending + no break
Buckle/Torus: Bone compressing + no break
Compressed side = Buckling deformity
Tension side = Intact
Greenstick: Bone bend (1 side) + bone break (1 side)
Compressed side = Intact
Tension side = Break
Pediatric Fractures: Clinical Presentation
Localized pain, edema, erythema
Limb/bone deviation from normal axis
Gap on bone surface
Crepitus
Pediatric Fractures: Investigations
XR
MRI: Salter-Harris fractures
Confirm XR findings
Pediatric Fractures: Treatment
Thicker periosteum (outer bone connective tissue layer) = Metabolically active = Faster healing
Non-Physeal:
Buckle: Splint
Greenstick + Bowing
Acceptable angulation: Splint/cast
Unacceptable angulation: Reduction
Physeal/Salter-Harris:
Type 1 + 2: Closed reduction + splint/cast
Type 3 + 4 + 5: Surgery = Open reduction + internal fixation + cast
Analgesics
Ice
Elevation
Pediatric Fractures: Complications
Growth arrest: Bone bridge across physis = Connect metaphysis + epiphysis = Cover growth plate…
Completely: Limb-length discrepancies
Partially: Angular deformity
Abnormal bone angulation
Acute Compartment Syndrome (ACS): Description
Tissue ischemia from increased pressure in fascial compartment
ACS: Epidemiology
Common in limbs (Usually lower leg)
ACS: Etiology
Trauma
Burn (scar tissue, edema)
Fractures
Reperfusion injury (returning blood supply after ischemia = Increase vessel permeability = Tissue swelling)
Non-Traume
Poor limb position (immobile)
Shock (increase capillary permeability)
ACS: Pathophysiology
Pressure from fascial compartment > Pressure from arteries = Block blood flow = Ischemia → Necrosis
ACS: Clinical Presentation
Rapid progression
Early:
Extreme pain
Worse with muscle movement
Tenderness
Tight muscles
Later: Impaired perfusion (6 Ps)
Pain
Pallor/cyanosis
Pulselessness
Paresthesia
Paralysis/muscle weakness
Pokilothermia
Inability to regulate body temp
Cold extremities
ACS: Investigations
Clinical diagnosis
Etiology/risk factors + ≥ 1/6 Ps
Peripheral nerve exam
Invasive compartment pressure measurement
Blood test
Imaging
ACS Investigations: Peripheral Nerve Exam
Sensory: Decreased sensation
Motor: Decreased movement
Gait
Balance: Impaired proprioception
ACS Investigations: Invasive Compartment Pressure Measurement
If unclear clinical findings
Method:
Insert device into compartment + inject saline
Measure pressure + determine ΔP = DBP - intracompartmental pressure
Normal: ΔP ≤ 30 mmHg
Increased compartment pressure
ACS Investigations: Blood Tes
Rhabdomyolysis + Crush Syndrome: Increased creatine kinase + myoglobin
Skeletal muscle breakdown = Release cell components → Blood = Cause AKI
ACS Investigations: Imaging
XR: Fractures
US: DVT + evaluate arterial bloodflow
ACS: Treatment
Surgery: Fasciotomy
Incision in skin + fascia = Relieve compartment pressure + restore perfusion
Leave wound open
Supportive care
Analgesia
O2
ACS: Complications
Necrosis
Rhabdomyolysis + Crush syndrome
Volkmann ischemic contracture
ACS Complications: Volkmann Ischemic Contracture
Description: Permanent forearm muscle shortening = Claw-like fingers, hand, wrist
Pathophysiology: Supracondylar humeral fracture → Compartment syndrome = Flexor muscle atrophy
Treatment:
Physical therapy
Elbow splint
Surgery: Tendon transfer, nerve decompression