Respiratory System- Anatomy and Physiology 2
1/86
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
87 Terms
Purpose for respiratory system
• Cells produce ATP for maintenance, growth, defense, and division
Oxygen (O2 ) is required for aerobic respiration
Produces carbon dioxide (CO2 )
• To obtain oxygen and release CO2
• Exchanged with air via diffusion across the exchange surfaces of the lungs
• Carried to/from cells by the cardiovascular system
Functions of respiratory system
• Provides extensive surface area for gas exchange between air and circulating blood
• Surface area is approximately 750 sqft.
• Moves air to and from exchange surfaces of lungs
• Protects respiratory surfaces
• Facilitates sounds production
• Facilitates olfactory stimulation (smell)
• Acid-Base balance of the blood
• Humidifies the air to protect the airway
Upper respiratory system
Above the larynx
Nose, nasal cavity, paranasal sinuses, pharynx
Function: Filter, warm, and humidify incoming air to protect delicate lower respiratory system & smell
Lower respiratory system
Larynx and below
Larynx, trachea, bronchi, bronchioles, alveoli of lungs
Function: Sound production, conductance of air, gas exchange
Conduction portion of respiratory tract
• From nasal cavity to terminal bronchioles
• Conduct air only
Respiratory portion of respiratory tract
• The respiratory bronchioles and alveoli
• Gas exchange occurs
• Alveoli are air-filled pockets within the lungs where gas exchange takes place
Respiratory mucosa
• Lines the conducting portion of respiratory system
• Consists of:
A superficial epithelial layer
A deep areolar layer called the lamina propria
In the upper respiratory system, trachea, and bronchi it contains mucous glands that secrete onto epithelial surface
In some portions of lower respiratory system, it contains smooth muscle
Nasal cavity and nasopharynx: type of tissue
Pseudostratified ciliated columnar epithelium with numerous mucous/goblet cells
Inferior portions of the pharynx: type of tissue
Stratified squamous epithelium
Superior portion of the lower respiratory system: type of tissue
Pseudostratified ciliated columnar epithelium with goblet cells
Smaller bronchioles: type of tissue
Cuboidal epithelium with scattered cilia
Simple squamous epithelium location
Lines exchange surfaces of alveoli
Cilia production and function
Goblet cells produce mucus to trap and Cilia move to propel unwanted debris, dust, pollen, microbes, and other things up to the oropharynx to be swallowed or discarded.
Respiratory defense system
A series of filtration mechanisms that removes particles and pathogens
Mucocilary Clearance (MCC)
Is the primary innate defense mechanism
Components of MCC
• Filtration by hair in nasal cavity removes large particles
• Mucous / Goblet cells and mucous glands: produce mucus that bathes exposed surfaces making moist and sticky for particulate matter and functions as a mucociliary escalator.
• Cilia: sweep debris trapped in mucus toward the pharynx by coordinated wave movement within the watery periciliary layer.
• Alveolar macrophages engulf small particles that reach lungs
• Surfactant is produced by Pneumocytes (Type II alveolar cells) to decrease the surface tension
Cystic Fibrosis
• Inherited disease that affects the respiratory defense, digestive, reproductive systems, and salt balance (chloride transport)
• Defective Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) gene on Chrom 7
• Respiratory mucosa produces dense, viscous mucus that can’t be transported by the cilia
• Dysfunctional CFTR prevents chloride movement and osmosis, so mucus is thick & sticky
• Mucus blocks small airways making breathing very difficult
• Mucus Plugs block respiratory track, pancreatic ducts, liver & bile duct, vas deference,
• Mucus elevator does not work leading to frequent infections, inflammation, malnutrition, and infertility
• Condition is lethal (predicted survival is 37 years old)
• Research using CRISPR editing for the CFTR gene is underway.
The larynx
Air from pharynx enters the larynx through an opening called the glottis
Larynx is a cartilaginous structure that surrounds the glottis
Main cartilage of the larynx
• Support and protect the glottis / entrance to trachea and vocal cords
• During swallowing:
The larynx is elevated
The epiglottis folds down over the glottis
Prevents entry of food and liquids into respiratory tract
Phonation
• Sound Production via vocal cords
• Vibrate as air passes through
Respiratory control
Regulates airflow
Corniculate and Arytenoid cartilages functions in the larynx
•Opening and closing of glottis
•Production and adjustment of sound
•Displacement or damage leads to hoarseness, difficulty swallowing, and airway issues
The Glottis parts and functions
• Vestibular ligaments (false) and vocal ligaments (true)
• Extend between thyroid cartilage and arytenoid & corniculate cartilages
• Are covered by folds of laryngeal epithelium that project into glottis
• Vestibular folds (false vocal cords) lie on top of vocal folds (true vocal cords)
• Prevent foreign objects from entering glottis
• Protect more delicate vocal folds
How sound is produced
• Air passing through glottis vibrates vocal folds and produces sound waves
• Sound is varied by:
Tension on vocal folds
Voluntary muscles reposition arytenoid cartilages which adjusts vocal folds
Distance increases – folds tense – pitch rises
Distance decreases – folds relax – pitch falls
How speech is produced
• Phonation: Sound production at the larynx
• Articulation: Modification of sound by other structures (tongue, teeth, lips)
Trabeculae
• Fibrous connective tissue partitions of lung
• Branch repeatedly dividing each lobe into increasingly smaller compartments
• The smallest trabecular partitions, interlobular septa, divide lobes into pulmonary lobules
• Branches of conducting airways, blood vessels, and lymphatic vessels follow these partitions
Pulmonary lobules function and physiology
• Each terminal bronchiole delivers air to a single pulmonary lobule
• Each terminal bronchiole branches to form several respiratory bronchioles
• Thinnest and most delicate branches of bronchial tree
• Deliver air to the gas exchange surfaces of the lungs
• Respiratory bronchioles are connected to alveoli along alveolar ducts
• Alveolar ducts end at alveolar sacs
Lung cells
Alveolar Epithelium
• Consists mostly of simple squamous cells
• Thin, delicate epithelium
• Squamous cells are called type I pneumocytes (type I alveolar cells)
• Patrolled by alveolar macrophages
• Contains pneumocytes type II (septal cells) that produce surfactant
Surfactant
Decreases the surface tension in the lungs
• Is an oily secretion containing phospholipids and proteins
• Forms a thin layer on top of the water that coats alveolar surfaces
• Reduces surface tension of the water
• Surface tension collapses air bubbles and would cause the alveoli to collapse
• Surfactant is VERY important in keeping alveoli open!
Respiratory distress syndrome
• Difficult respiration due to alveolar collapse
• Caused when pneumocytes type II do not produce enough surfactant
Pleural cavities and pleural membranes
• Two pleural cavities (separated by the mediastinum)
• Each pleural cavity:
Encloses and protects a lung
Is lined with a double layer serous membrane (pleura)
Parietal pleura
Visceral pleura
Pleural fluid
Fills the pleural cavities
Lubricates and reduces friction between layers
Holds 2 membranes together because of surface tension fluid
The ABCs & D & E of Respiration- Life or DEATH
Normal Continuous Breathing is VITAL for LIFE
◦ 12 – 20 breaths per minute (Adult)
◦ Hold your breath
◦ 30 – 90 sec capacity
◦ Oxygen Reserve capacity
◦ Result in CO2 Build-up
Key Objectives
◦ O2 & CO2 Partial Pressure
◦ Surface Areas for Gas Exchange
◦ Oxygen Carrying Capacity
◦ Dynamic Oxygen Affinity
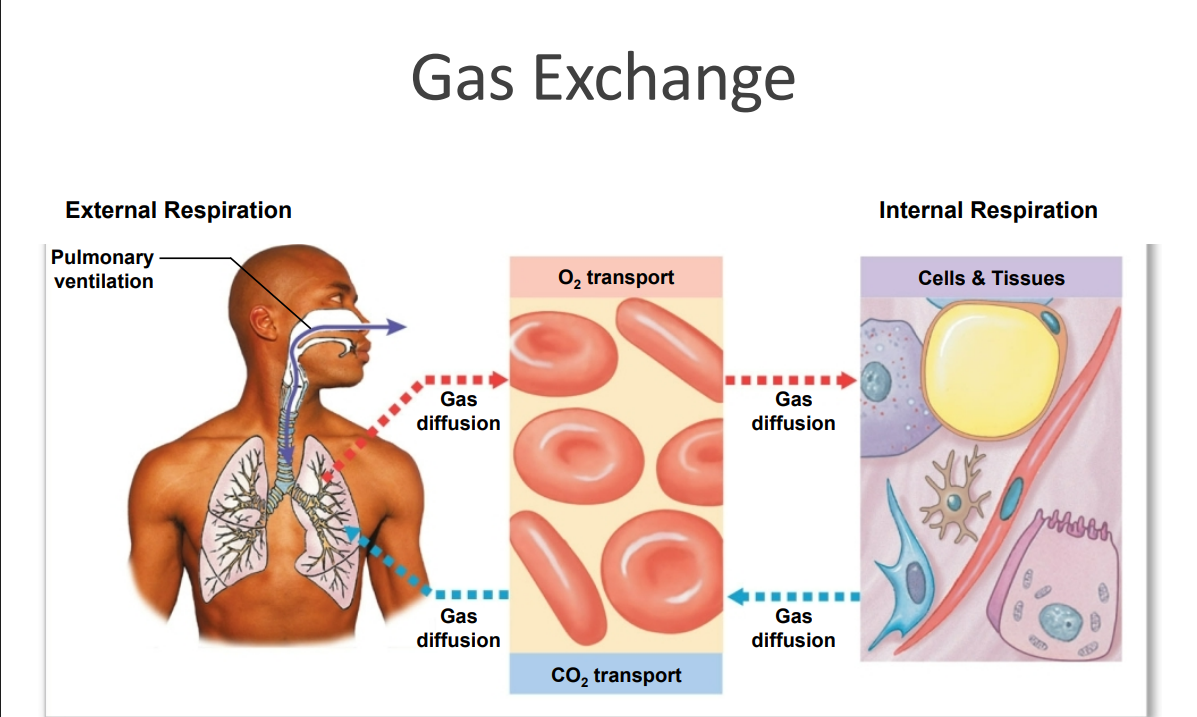
External respiration (pulmonary respiration)
Includes all processes involved in exchanging O2 and CO2 with the environment
Internal respiration (tissue respiration)
• Result of cellular respiration
• Involves the uptake of O2 and production of CO2 within cells / tissues
Three processes of external respiration
1. Pulmonary ventilation (breathing)
2. Gas diffusion
3.Transport of O2 and CO2
Between alveolar capillaries and capillary beds in other tissues
Circulatory system for gas transporter and Acid-Base Buffer
Asthma vs COPD
Abdormal external respiration is dangerous
Hypoxia
Low tissue oxygen levels
Anoxia
Complete lack of oxygen
Hypercapnia
• Buildup of CO2
• Results in acidosis (pH < 7.35)
CO2 + H2O -> H2CO3 -> HCO3 - + H+
Hypocapnia
• Too low CO2
• Results in alkalosis (pH > 7.45)
Where CO2 originates from
Dose Dependent Feedback Relationship with O2 & CO2 Regulation
◦ Waste Product of Cellular Respiration & decreases pH
◦ Central (Medulla) & Peripheral Chemoreceptors (Carotid a. & Aortic Arch)
◦ Sense & Respond to Increased CO2, Bi-Carb, Lactic Acid, H+ Levels or Decreased O2
◦ Normal Blood pH: 7.35 – 7.45
◦ Higher PP of CO2 or O2 , Increases Rate of Diffusion & Elimination
◦ Inverse: States of Meditation & Hibernation
◦ Emotions, pain, temperature, sympathetic vs parasympathetic
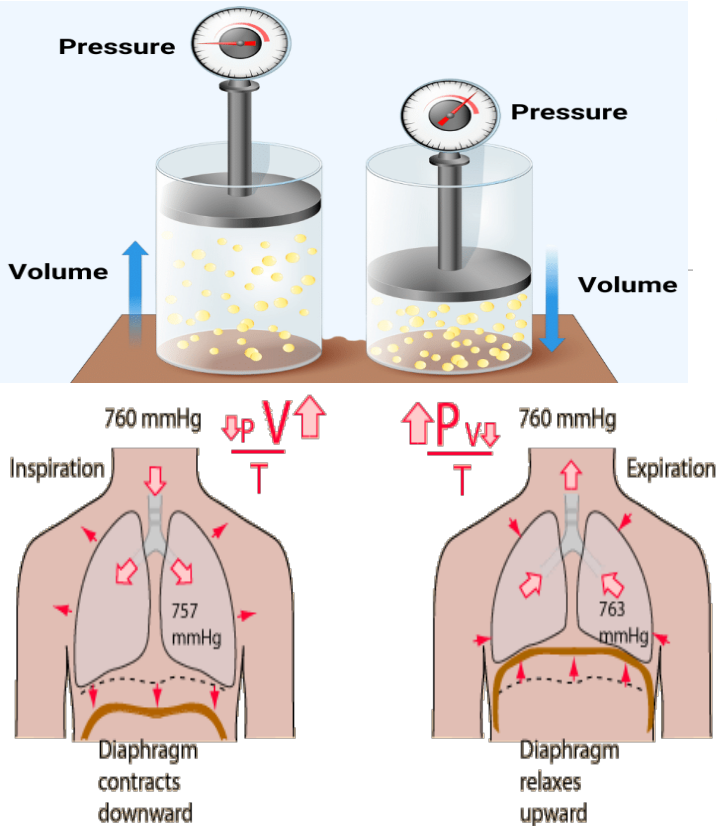
Pulmonary Ventilation- Mechanism of Breathing
• Is the physical movement of air in and out of respiratory tract
• Driven by pressure differences between the atmosphere and alveoli along with the contraction of the diaphragm.
• Diaphragm contracts (moves down) and external intercostal muscles lift the ribs, thereby increase thoracic cavity volume and decreasing thoracic cavity pressure and allowing air to move inside.
Atmospheric pressure
Is a key contributer to the movement of air
Pressure of the air around us
760 mmHg = 1 atm
Boyles’s Law
Boyle’s Law P1V1 = P2V2
• Defines the relationship between gas pressure and volume
• P = 1/V
• The pressure of a gas varies inversely with its volume
Phrenic nerve
Pressure and Airflow to the Lungs
• Pulmonary Ventilation causes volume changes that create changes in pressure
• Air flows from area of higher pressure to area of lower pressure
• Volume of thoracic cavity changes
• During inhalation and exhalation
• With expansion or contraction of diaphragm or rib cage
• Phrenic nerve from cervical vertebral nerves 3, 4, 5 descend to innervate the diaphragm
Rib Cage Movement
As the rib cage is elevated or the diaphragm is depressed, the volume of the thoracic cavity increases.
Pleural cavity at rest
Pressure outside = Pressure inside
Pressure outside and inside are equal, so no air movement occurs
Pleural cavity during inhalation
Pressure outside > Pressure inside
Pressure falls inside, so air flows in
Elevation of the rib cage and contraction of the diaphragm increase the size of the thoracic cavity
Pressure within the cavity decreases
Air flows into the lungs
Pleural cavity during exhalation
Pressure outside < Pressure inside
Pressure inside rises, so air flows out
The rib cage returns to its original position and the diaphragm relaxes
The volume of the thoracic cavity decreases and the pressure increases
Air moves out of the lungs
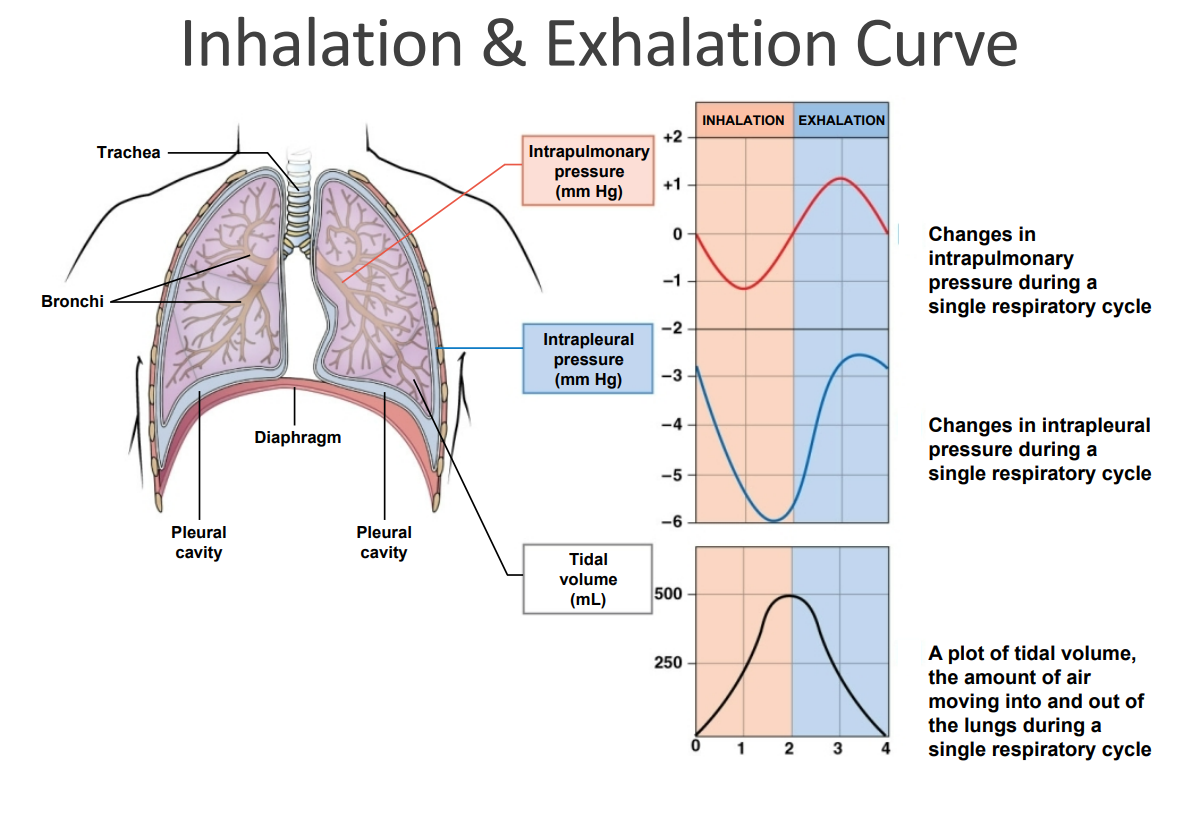
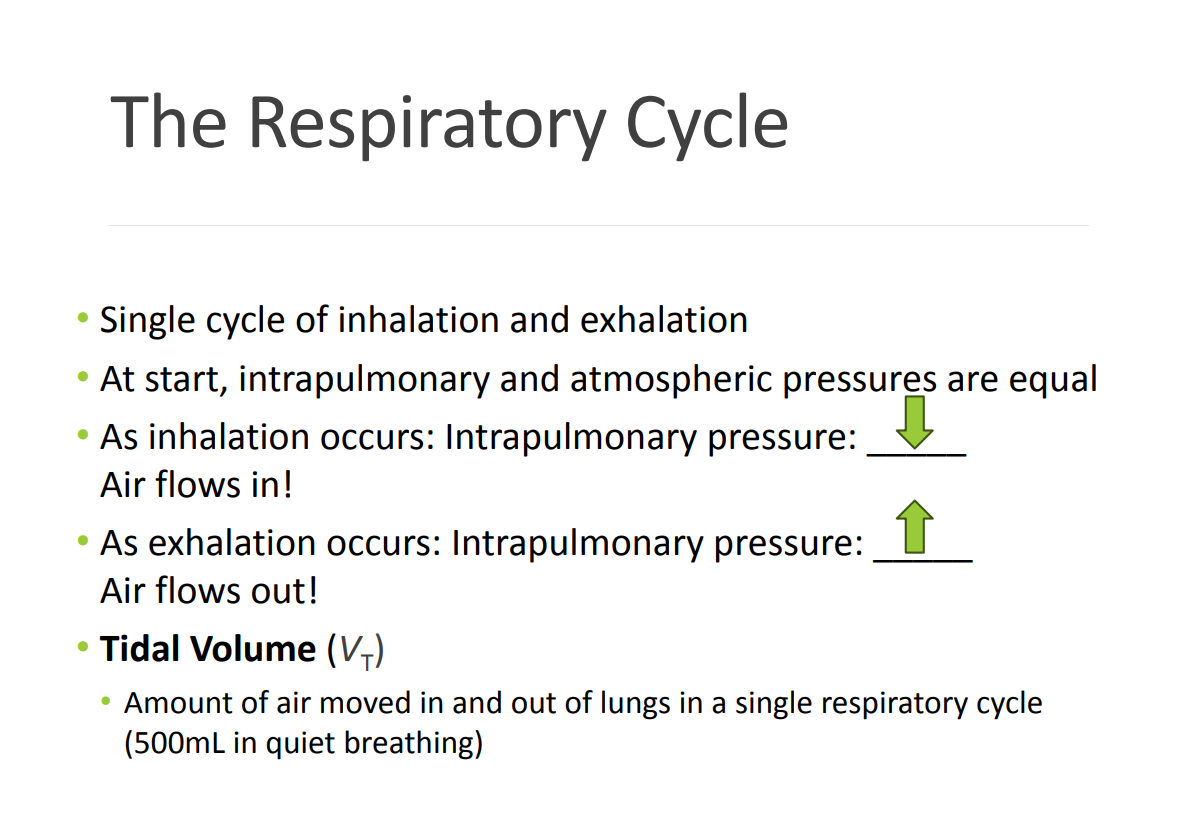
Intrapulmonary Pressure or “Intra-alveolar Pressure”
• Is relative to atmospheric pressure (760 mmHg)
• In relaxed breathing, the difference between atmospheric pressure and intrapulmonary pressure is small (-1 cm H2O on inhalation or +1 cm H2O on exhalation)
• Normal 500mL Tidal Volume
Intrapulmonary Pressure
Maintained at 0 (+/- 1) at rest or 0 (+/- 2) with deep breathing.
Intrapleural Pressure
Maintained at -4 (+/- 2)
• -4 mmHg
• Can fluctuate, but remains below atmospheric pressure throughout respiratory cycle
• MUST maintain a negative baseline (-4 mmHg) at rest
• Elasticity of the chest wall naturally pulls outward (suction)
• Keeps the lungs expanded by increasing the volume ( Pressure - 6)
• If Intrapleural Pressure equals atmospheric pressure (+4 mmHg), then the lungs collapse (Pneumothorax)
Transpulmonary Pressure
Difference between Intrapleural and Intrapulmonary pressure
The Respiratory Cycle
Muscles and Nerves MOST importantly involved in Inspiration are:
Diaphragm innervated by phrenic nerve
External Intercostals innervated by intercostal nerve
Accessory respiratory muscle
Are activated when respiration increases significantly
• Sternocleidomastoid & Scalene muscles & Pectoralis minor and major
• Exercise, Stress, Sympathetic Response, Coughing, Respiratory distress
Normal exhalation
Is a passive process that utilizes elastic rebound
Foreful exhalation activates accessory muscles
Rectus abdominis, obliques, transversus abdominis, internal intercostals
Quiet breathing (Eupnea)
Involves active inhalation and passive exhalation
Diaphragmatic breathing or deep breathing
Is dominated by intense diaphragm contraction
Costal breathing or shallow breathing
Is dominated by rib cage movements
Labored Breathing
Normal during exercise
Abdormal breathing at rest is a sign of:
Respiratory distress
Hyperpnea
Forced breathing (Hyperpnea)
• Involves active inhalation and active exhalation
• Assisted by accessory muscles
• Maximum levels occur in exhaustion
• During intense exercise, labored singing, or associated w/ immediate sympathetic response
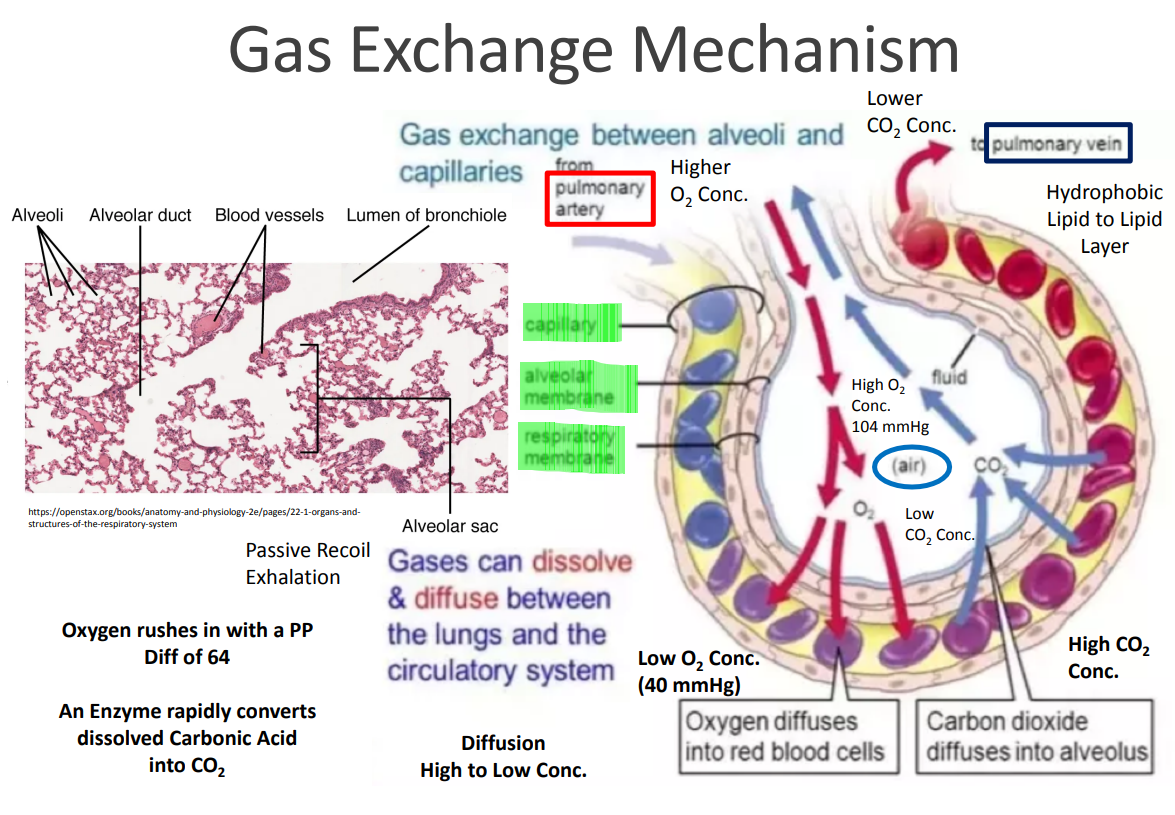
Gas exchange location
• Occurs between blood and alveolar air
• Across the respiratory membrane
• Squamous cells lining the alveoli
• Endothelial cells lining adjacent capillary
• Fused basement membranes between the alveolar and endothelial cells.
Depends on:
Partial pressures of the gases
Diffusion of molecules between gas and liquid
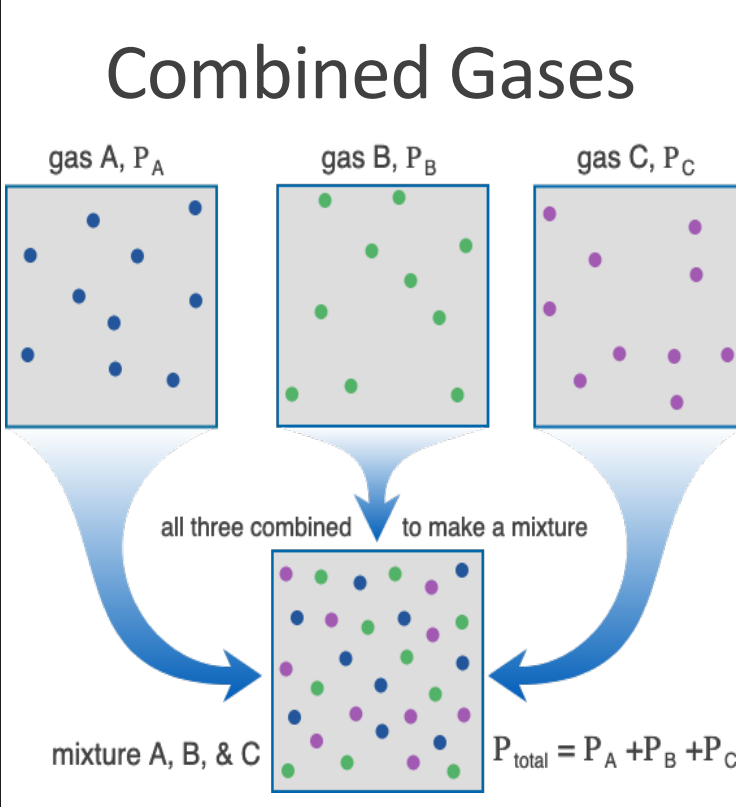
Dalton’s Law
• Each gas in a mixture contributes to the total pressure in proportion to its relative abundance
• The more of a particular gas, the more it contributes to the overall pressure
• At sea level, respiration is optimized for O2 saturation
• At higher (airplane) or lower (deep sea diving) heights/depths, partial pressure of O2 changes.
The Bends
• Decompression Sickness
• Inc. nitrogen dissolution
• N2 Gas bubbles up in tissue, joint pain, stroke
Air Gas components
• The air we breath is a mixture of gasses
• Composition of Air
• Nitrogen (N2 ) is about 78.6%
• Oxygen (O2 ) is about 20.9%
• Water vapor (H2O) is about 0.5%
• Carbon dioxide (CO2 ) is about 0.04%
• Atmospheric pressure (760 mmHg) is a result of the combined effects of each type of molecule in air (Dalton’s Law)
• 78.6% of pressure is the result of nitrogen (597mmHg)
• 20.9% of pressure is the result of oxygen (159mmHg)
Gas in Fresh Air
• Partial Pressure
• The pressure contributed by each gas in the mixture
• All partial pressures together add up to the total pressure of that gas mixture
• Partial pressures for the gases in the atmosphere must = 760 mmHg
• Nitrogen: 597
• Oxygen: 159
• Water Vapor: 3.7
• Carbon dioxide: 0.3
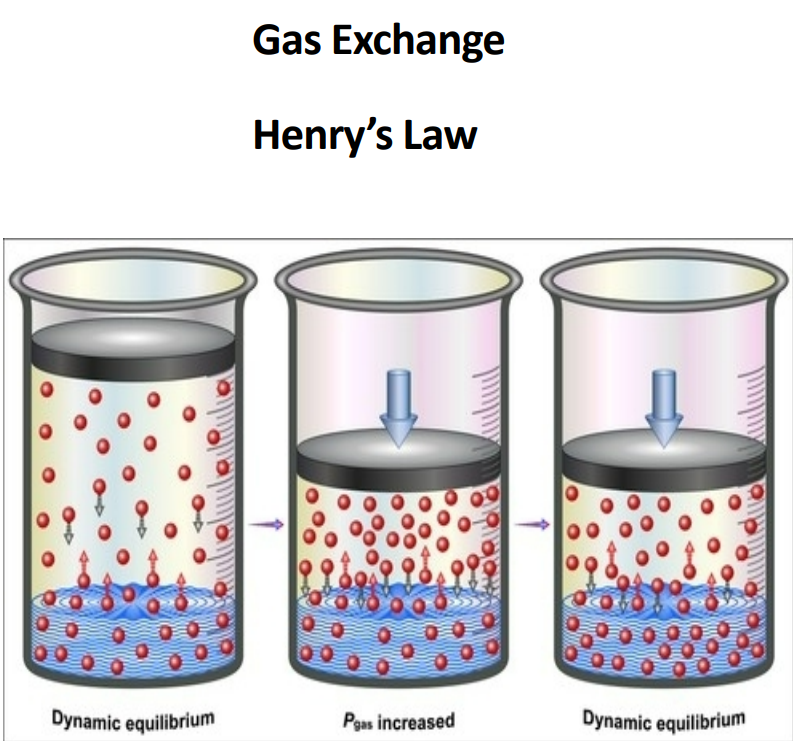
Diffusion between liquids and gases
• When gas under pressure comes in contact with liquid:
• Gas dissolves in liquid
• Gas molecules enter solution until an equilibrium is reached
• Increase pressure, increase amount of gas in solution
• Decrease pressure, decrease amount of gas in solution
Henry’s Law
At a given temperature, the amount of a gas in solution is proportional to partial pressure of that gas
Five reasons for effieciency of gas exchange
1. Substantial differences in partial pressure across the respiratory membrane
2. Distances involved in gas exchange are short
3. O2 and CO2 are lipid soluble (Hydrophobic)
4. Total surface area is large (7000 sf of alveolar space)
5. Blood flow and airflow are coordinated (Ventilation – Perfusion Match)
Pulmonary gas exchange: Oxygen Diffusion
• PO2 in alveolar air: 104 mmHg
• PO2 in blood of pulmonary capillaries: 40 mmHg
• O2 diffuses from alveolar air to blood
Pulmonary gas exchange: Carbon Dioxide Diffusion
• PCO2 in alveolar air: 40 mmHg
• PCO2 in pulmonary capillaries: 46 mmHg
• CO2 diffuses from blood to pulmonary air
Hemoglobin in erythrocytes
• Positive Hemoglobin Cooperativity of binding sites
• Structural confirmation change that increases affinity
• Hemoglobin Saturation 95% - 99%
• Pulse Oximetry (Sat. of Peripheral O2 )
• Arterial Blood Gas at Radial a. (ABG)
Tissue Capillary Gas Exchange: Internal Respiration; Oxygen Diffusion
• PO2 in blood of systemic capillaries: 95 mmHg
• PO2 in interstitial fluid: 40 mmHg
• O2 diffuses from blood to interstitial fluid / tissues
Tissue Capillary Gas Exchange: Internal Respiration; Carbon Dioxide Diffusion
• PCO2 in blood of systemic capillaries: 40 mmHg
• PCO2 in interstitial fluid: 45 mmHg
• CO2 diffuses from interstitial fluid / tissues to blood
Oxyhemoglobin Dissociation curve
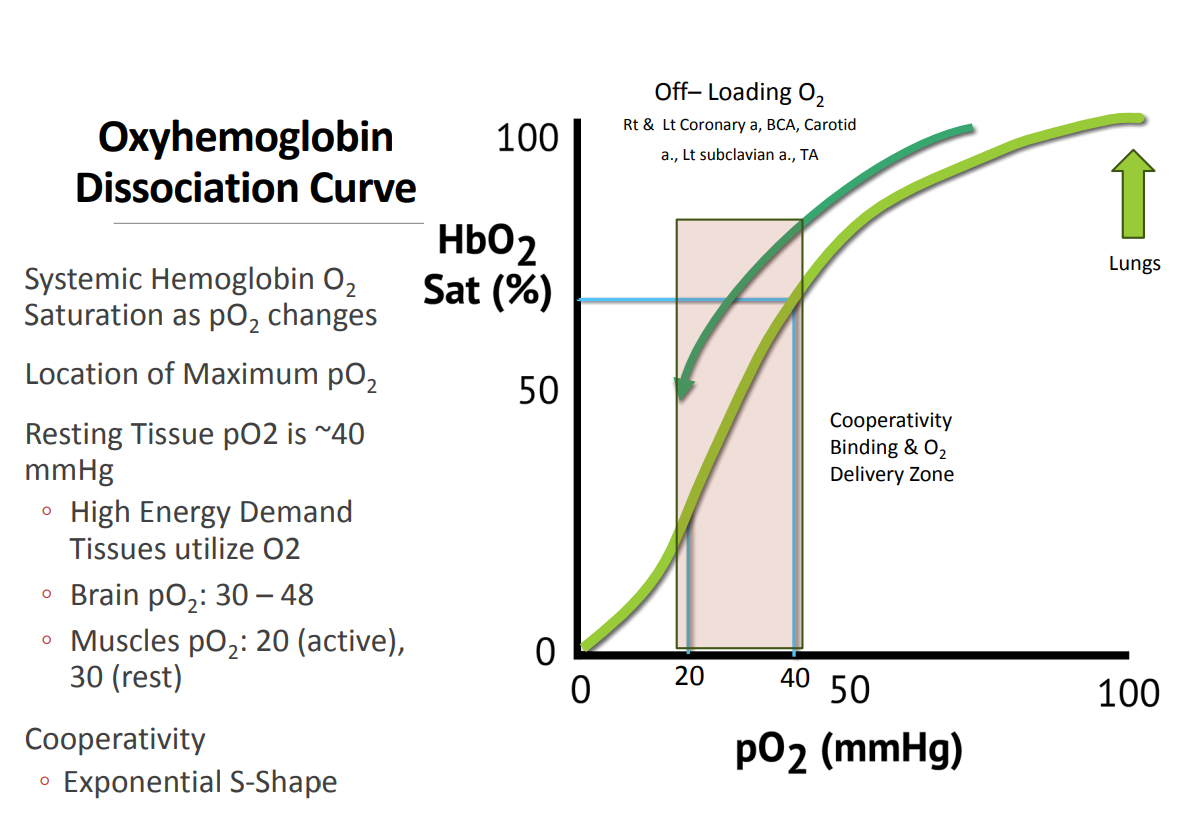
Factors affecting the OxyHemoglobin
Dissociation/Saturation
• Rt = Greater Release of O2
• Lt = Decreased Release of O2
• Dynamic Metabolic Reactions
• Exercise = Inc. O2 Utilization
• Temperature
• Bohr Effect Acid on Hb
• 2,3-Bisphophoglycerate
Confirmational Change to Hb
Inc. Anerobic Respiration
Sympathetic NS
Epi/NorEpi, Androgens, T3 /T4 , GH
Control of Respiration V/Q Coupling
V = Ventilation & Q = Perfusion
Local regulation of gas transport and alveolar blood flow
• Smooth muscle in alveolar capillaries is sensitive to P O2
•When P O2 is low, alveolar capillaries constrict
•Diverts blood flow to areas with high O2
• Smooth muscle in bronchioles is sensitive to P CO2
•When P CO2 declines, bronchioles constrict
•When P CO2 rises, bronchioles dilate
•Directs airflow to alveoli with high carbon dioxide
• Overall, local regulation improve efficiency of gas exchange / transport
Control of Respiration
The Respiratory Centers of the Brain
◦ Include the Pneumotaxic Center (pontine respiratory group) (Pons) and the Respiratory Rhythmicity Centers (Medulla Oblongata) (DRG, VRG)
◦ Monitor the composition of blood and CSF and adjust respiration to maintain homeostasis
◦ pH (7.35-7.45)
◦ Partial pressure of CO2
◦ Partial pressure of O2
◦ Hypercapnia triggers a respiratory reflexes
Ventral Respiratory Group (VRG)
• Controls motor neurons of the diaphragm and external intercostals
• Functions during every respiratory cycle
• Determines base respiratory rate
Dorsal Respiratory Group (DRG)
• Controls motor neurons of the accessory inspiratory and accessory expiratory muscles
• Functions only when ventilation demands increase and accessory muscles are utilized for deep breathing
Pneumotaxic Center (Pontine Respiratory Group)
Adjusts output from VRG to adjust respiratory rate
Respiratory Reflexes: Chemoreceptors
Are sensitive to PCO2 , PO2 , or pH of blood or cerebrospinal fluid
Respiratory Reflexes: Stretch Receptors (propiroceptors)
Respond to changes in airway & lung volume
Irritating physical or chemical stimuli in nasal cavity, larynx, or bronchial tree
Other sensations including pain, changes in body temperature, emotional stress, exercise
Carbon Monoxide Poisoning
• Usually from incomplete burning of fuels in poorly ventilated areas.
• Car in the Garage
• Furnace, Stove, Water Heater
• House Fire - Furniture
• CO Detector • Clinical Presentation
Sudden Onset
HA, Confusion, Dizziness, Chest Pain, Weakness
Etiology
• HbCO Affinity is >240X HbO2
• Depletes Available Hb
• Insufficient O2 Delivery, CO2 Toxicity, Hypoxia, H2CO3 & LA
• Rx: 100% O2 , Hyperbaric Tx, TCM Blood transfusion