HA- Heeter
1/57
Earn XP
Description and Tags
2 hours
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
58 Terms
Difference between primary and secondary headaches?
primary: not associated with underlying illness
secondary: symptoms of underlying illness
What does the SNOOP acronym stand for in headache red flags?
S- systemic symptoms (fever, weight loss)
N- neurologic symptoms (confusion)
O- onset (sudden, abrupt, etc.)
O- older (new onset or progressive HA)
P- previous history (1st HA or new HA)
Examples of primary headaches?
tension
migraine w or w/out aura
chronic migraine
cluster HA
Which of the following appears to be hereditary (~70%)?
a. tension
b. cluster
c. migraine
c.
Exclusions for Self-Treatment of HA:
idk how imp
Severe head pain, Headaches persisting for 10 days, Last trimester of pregnancy, < 8 years of age, High fever, Liver disease, Secondary headaches, Symptoms consistent with migraine/cluster HA but no formal diagnosis.
Describe the pathophysiology behind migraines:
lowkey I feel like he won’t ask—> more of a Khan type question
combo of neuronal and vascular factors:
activation of trigeminal sensory nerves—> releases neuropeptides (sub P, CGRP, neurokinin A)
results: vasodilation, inflammation, pain
disturbances with serotonin
low levels between attacks
increased levels during attacks/HA
List migraine triggers for each category:
environmental
food
behavioral/physiologic
medications
Environmental:
Changes in barometric pressure
Bright/flickering lights
Loud noise
Odors
Food:
Alcohol, Caffeine, Chocolate, Fermented foods, MSG
Behavioral/Physiologic:
Irregular sleep
Hormonal changes
Skipping meals
Strenuous exercise
Stress
Medications:
nitrates
contraceptives
postmenopausal hormones
reserpine
Migraine premonitory symptoms occur in up to 79% of patients and can be neurologic, psychologic, autonomic, or constitutional.
List the neurologic premonitory symptoms:
allodynia (Nerve pain)
photophobia
phonophobia
hyperosmia (Increased sensitivity to smells)
difficulty concentrating
BASICALLY: sensitivity to all 5 senses 🙃
Is a migraine usually a bilateral or unilateral throbbing or pulsing?
UNILATERAL
What symptoms usually accompany a HA?
GI—> n/v
What are the components of a migraine diagnosis?
Comprehensive HA history (age, frequency, timing, duration, etc.)
rule out secondary HA
MIDAS questionnaire (used to assess impact of migraines on daily life)
What can be used non-pharm for migraines?
(include for prevention and for acute migraine)
prevention:
identify and avoid triggers (keep a diary)
adhere to wellness program (sleep, exercise)
behavioral interventions (therapy)
acute migraine:
apply ice to head
rest/sleep in dark/quiet environment
What do medical devices like Cefaly, Nerivio, Relivion MG, and gammaCore do in migraine?
stimulate nerves to prevent/treat migraine
What is the general treatment approach for mild-moderate headaches? what about severe?
mild/mod: use non-migraine specific agents (NSAIDs, steroids, other analgesics)
severe: migraine specific agents (ergos, triptans, etc.)
What is the most common cause of chronic headaches? how to avoid?
most common—> medication overuse
how to avoid—> limit abortive therapies to max 2-3x a week
WHAT IS FIRST LINE FOR MILD-MODERATE MIGRAINES:
APAP/NSAIDS/SALICYLATES
best evidence for: ASA, diclofenac, IBU, ketorolac, naproxen, APAP/ASA/caffeine combo
What role do opiates play in migraine treatment?
any evidence?
risks?
when is it used?
GENERALLY AVOID—> evidence for use is generally negative
risks: medication-overuse HAs, dependence
use only for those who have C/I to other therapies
When to administer antiemetics (ex: metoclopramide, chlorpromazine) for n/v associated with migraines?
admin 15-30 min prior to abortive therapy
Ergot Alkaloids MOA
Nonselective 5HT1 agonists —> vasoconstriction of intracranial blood vessels, inhibition of inflammation
Side effects of ergot alkaloids?
n/v (consider pre-tx)
diarrhea
chest tightness
elevated BP
DO NOT USE ERGOT ALKALOIDS WITHIN 24 HOURS OF _____________.
TRIPTAN
Ergot Alkaloid C/I
renal and hepatic failure
CV—> CAD, PVD, uncontrolled HTN
cerebrovascular disease
sepsis
pregnancy
lactation
WHAT IS THE FIRST LINE TREATMENT FOR MODERATE-SEVERE MIGRAINE AS ABORTIVE THERAPY?
TRIPTANS
Triptans MOA
selective agonists of 5-HT1B and 1D
If I take a triptan and it fails, can I try another triptan or do I switch to another class?
switch to another triptan
TRIPTAN C/I
history of ischemic heart disease (angina, previous MI), uncontrolled HTN, cerebrovascular disease
MAOI within 2 weeks (suma, riza, zolmi)
25% of patients that take triptans may experience what symptom?
tightness, pressure, heaviness, or pain in chest
Which triptans have a slower onset, but longer duration?
These triptans would be best in patients with what kind of migraines?
frovatriptan (t ½ =25hrs), naratriptan (t ½ =5-6hrs), eletriptan (t ½ =4-5hrs)
best for pts. with migraine with slow onset and long duration
What is the only triptan that comes in injection form?
sumatriptan
Lasmiditan (Reyvow) MOA
Selective 5-HT1F agonist—> Minimized vasoconstriction
Do not drive/operate machinery for at least 8 hrs after taking what drug?
Lasmiditan
What are the names of the CGRP Antagonists?
dosage forms of each?
Ubrogepant (Ubrelvy)- tablet
Rimegepant (Nurtec ODT)- orally disintegrating tablet
Zavegepant (Zavzpret)- nasal
What are the C/I of each CGRP antagonist?
Ubrogepant and Rimegepant—> C/I w strong CYP3A4 inhibitors
Zavegepant—> avoid with nasal decongestants (easy to remember bc the dosage form of this one is nasal)
What are the migraine prophylaxis indications?
Recurring migraines with disability (even w/ acute tx)
frequent attacks requiring use of acute tx more than 2x/week
ineffective abortive therapy
patient preference
uncommon migraine types
Trial of ____-____ months required to assess efficacy of prophylaxis tx of migraines.
2-3 months (some say 6)
What are the FDA approved agents for migraine prophylaxis?
(not off-label drugs, only FDA approved)
propranolol
timolol
valproate
topiramate
botulinum toxin A
CGRP agents
What antidepressants have shown the most efficacy and are used off-label for migraine prophylaxis?
amitriptyline and venlafaxine
What beta-blockers are used for Migraine Prophylaxis? (include FDA and off-label)
propranolol, timolol—> FDA approved
nadolol, atenolol, metoprolol—> also effective
What anticonvulsants are used for Migraine Prophylaxis? (include FDA and off-label)
valproate, topiramate—> FDA approved
carbamazepine, gabapentin—> off-label
C/I of valproate?
pregnancy
liver disease
pancreatitis
What is the indication of Botulinium toxin A for migraine prophylaxis?
prophylaxis of headaches in adults with chronic migraines (15+ days/month lasting 4hrs a day or longer)
BBW of Botulinum toxin A?
distant spread of toxin may occur hours-weeks after injection leading to swallowing/breathing problems and potentially death
List the CGRP mabs:
distinguish which target CGRP and which are CGRP receptor antagonists
CGRP mabs targeting CGRP
Fremanezumab
Galcanezumab
Eptinezumab
CGRP mabs targeting CGRP receptor
Erenumab
What are the 3 criteria a pt. must meet in order to taken a CGRP mab?
be at least 18 yrs old
have at least one of the following:
4-7 HA/month with moderate disability
8-14 HA/month
chronic migraines and can’t use botulinum toxin A
failed a 6 week trial of at least 2 other meds for migraine prophylaxis
What CGRP agonists are used for migraine prophylaxis?
Rimegepant
Atogepant
Answer the following about prophylaxis medications:
what NSAID has the most data for use? when are they most useful?
what CCB can be used as 2nd or 3rd line when other meds have failed?
what is the only situation where triptans are used for prophylaxis?
naproxen—> most useful for predictable HA
verapamil
only useful for prevention of menstrual migraines (start 1-2 before period)
What is a tension HA?
Is it acute or chronic?
What is the pathophys behind them?
tension HA—> in response to stress, anxiety, depression
can be acute or chronic
pathophys:
activation of pain perception structures in brainstem
chronic HA evloves from acute, episodic HA
What symptoms are ABSENT in tension headaches?
What are the symptoms of tension HAs?
premonitory and aura symptoms are ABSENT
symptoms: mild-mod pain, BILATERAL most common
generally no associated symptoms
Nonpharm for tension HA?
behavior tx (therapy)
NO CONSISTENT BENEFIT seen with heat, cold, massage, exercise, etc.
What pharm tx is used for tension headaches?
APAP
ASA
APAP/ASA/Caffeine combo
NSAIDs (IBU, naproxen, indomethacin, ketoprofen, ketorolac)
APAP and ASA are available in combo with bulalbital and caffeine but is generally avoided why?
due to dependency/overuse risk
What are the symptoms of a SINUS HEADACHE?
dull, pressure-like pain in forehead area
usually pt. will have other sinus symptoms (nasal discharge, congestion)
Tx of sinus headaches?
treated like TENSION headaches (APAP, ASA, NSAIDS)
may be combined with decongestants to help with nasal symptoms
Cluster HAs are rare, but considered the most severe.
What are the symptoms?
most are episodic in nature—> attacks, then remission
SEVERE pain, described as sharp, penetrating
usually UNILATERAL
often accompanied by cranial autonomic symptoms (face sweating, lacrimation, nasal stuffiness)
NO AURA
What is the preferred 1st line tx for prevention of cluster HA?
Verapamil
Tx for cluster HA?
what dosage forms are preferred for abortive therapy?
abortive therapy
oxygen
triptans- SC or intranasal formulations (especially sumatriptan SC)
ergotamine derivatives- IV dihydroergotamine
galcanezumab- 3 injections at onset of HA, then monthly till end of cluster period
prophylaxis
verapamil
lithium
steroids
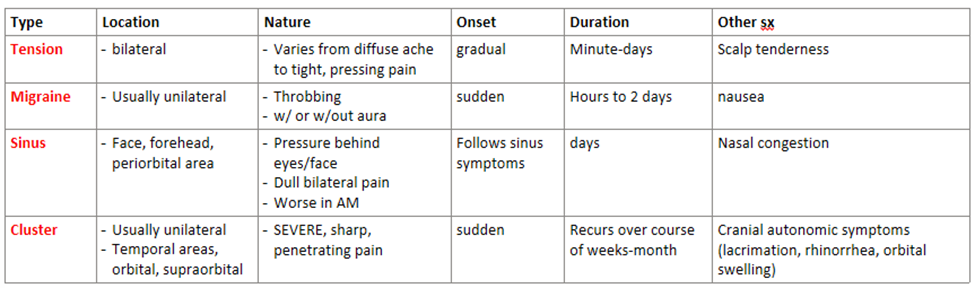
REVIEW:
Compare the location, nature, onset, duration, and identify other symptoms associated with each kind of HA:
HA type | Location | Nature | Onset | Duration | Other sx |
Migraine | |||||
Tension | |||||
Sinus | |||||
Cluster |
PRACTICE:
What is the ONLY type of headache where pts. pay experience aura?
a. tension
b. migraine
c. sinus
d. cluster
b.