5- traumatic luxations
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
16 Terms
Injury to a permanent tooth is dictated by…
Concern for vitality of PDL and pulp
Endo may be indicated if spontaneous pain, abnormal response to pulp sensitivity tests, lack of root formation, apexogenesis
May need to stabilise tooth with splint
What are 7 characteristics of an ideal splint?
Easily fabricated in the mouth without additional trauma
Passive unless orthodontic forces are intended
Allows physiologic mobility
Non-irritating
Doesn’t interfere with occlusion
Allows endodontic access and vitality testing
Easily cleansed and removed
Concussion- what, treatment, radiographic
Tooth tender to touch but not displaced- normal mobility, no sulcular bleeding
None- observe, careful when eating, prevent plaque- clean area with soft brush/cotton swab with alcohol free mouth rinse, apply chx gluconate topically 2x daily for 1 week
Only do if pathology present
Subluxation- what, radiographic recommendations and findings, treatment
Tender to touch AND increased mobility BUT not displaced, maybe bleeding in gingival crevice
Periapical (size 0) or occlusal (size 2) initially- normal to slightly widened pdl space
None- same as concussion
A passive/flexible splint used to stabilise tooth for up to 2 weeks- ONLY if excessive mobility or tenderness when biting
Extrusive luxation- what, radiographic, treatment depends on and is?
Partial displacement out of socket, tooth appears elongated and very mobile, possible occlusal interference
Periapical (size 0) or occlusal (size 2) initially, slight increase to very wide pdl space
Depends on degree of displacement, mobility, interference with occlusion, root formation and child’s compliance
If not interfering with occlusion- let it spontaneously reposition
If very mobile or extruded over 3mm- extract with LA
What is lateral luxation- what, radiographic, treatment if- minimal occ interference, severe displacement, unstable in new position, necrotic?
Tooth displaced, usually palatal/labial direction- immobile, possible occlusal interference
Periapical (size 0) or occlusal (size 2) initially, increase pdl space apically- better seen on occlusal esp if tooth displaced labially
Minimal/no occlusal interference- spontaneously reposition- occurs within 6 months
If severe displacement- under LA- extract if risk of ingesting tooth or gently reposition
If unstable in new position- flexible splint attached to adjacent uninjured tooth for 4 weeks
If pulp becomes necrotic- endo
Intrusive luxation- what, radiographic findings, treatment
Displaced through labial bone plate or can impinge on permanent tooth bud- almost/completely disappeared into socket, can be palpated labially
Periapical or occlusal initially-
When apex displaced toward or through labial plate- can see apical tip and tooth will appear shorter
Apex displaced toward permanent tooth germ- can’t see apical tip and tooth looks longer
Spontaneous reposition
Avulsion- what, radiographic findings, DONT, treatment depends on…
Tooth completely out socket, explore location of missing tooth, risk of embedded in lip, cheek or tongue, if tooth not found- refer to hospital
If tooth lost, xray ensures it not intruded
DONT REPLANT
Treatment depends on maturity of root and condition of PDL cells which depend on time out of mouth and medium in which it’s stored
After an extra alveolar dry time of 30 mins, most PDL cells are non viable
How can you classify an avulsed tooth in 3 groups before treatment?
PDL cells…
Most likely viable- planted immediately or within 15 mins at accident site
Viable but compromised- tooth kept in storage medium (milk, HBSS, saliva, saline) for under 60 mins
Non viable- extra oral dry time over 60 mins
What are the treatment guidelines for a avulsed permanent tooth with CLOSED APEX?- tooth replanted before clinic
Clean injured area with water, saline or chx
Verify correct position clinically and with x ray
Admin LA (no VC)
If tooth replanted in wrong socket or rotated- reposition within 48hrs
Suture gingival lacerations if present
Initiate RCT within 2 weeks
Admin systemic ATB
Check tetanus status
What are the treatment guidelines for an avulsed permanent tooth with CLOSED APEX?- tooth replanted in storage medium for less than 60 mins
Check avulsed tooth for surface debris- remove by gently agitating it in storage and rinse
Give LA without VC
Irrigate socket with sterile saline
Examine alveolar socket, if socket wall is fractured- reposition fractured fragment into og position
Remove coagulum with saline and replant tooth slowly with slight pressure
Stabilise tooth for 2 weeks with passive splint the RCT treatment
Why do avulsed tooth extraoral have poor long term diagnosis?
PDL becomes necrotic, can’t regenerate
May result in ankylosis related (replacement) root resorption
We can replant to temporarily restore aesthetics and function
What are the treatment guidelines for an avulsed permanent tooth with OPEN APEX?
Potential for spontaneous healing in forms of new ct with vascular supply- allow continued root dev
Only do endo if definite signs of pulp necrosis and infection
What appliances (other than education) can be used to prevent dental injuries?
Face guards- prefabricated cage attached to helmet
Mouth guards- absorb/deflect blows, shields from laceration, prevents opposing teeth violently contacting, support for mandible
3 types of mouth guards?
Stock prefabricated
Mouth formed
Custom made
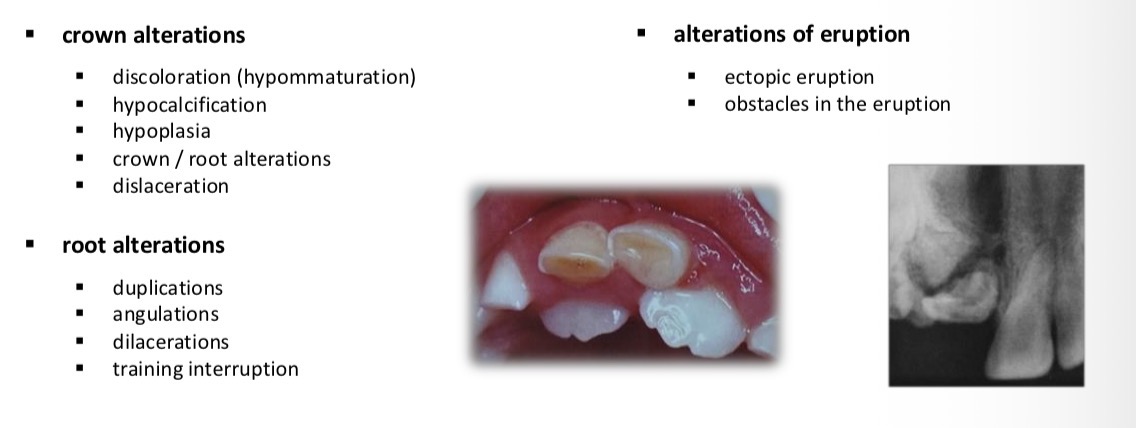
Effects on permanent teeth any trauma in primary teeth