Depth of wounds and types of wounds
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
19 Terms
Superficial
does not break the skin (epidermis only)
very painful
red burns that blanch with pressure

Superficial partial thickness
involves the epidermis and the superficial dermis
blistering wounds that blanch with pressure
typically moist and weeping

Deep partial thickness
involved the epidermis and the deep dermis
waxy appearance, does not blanch with pressure
dry and pale
typically painless

Full thickness
involves the epidermis, dermis, and hypodermis
colorless (waxy white, or leathery gray)
typically painless

full thickness with muscle and bone involvement
involves the epidermis, dermis, hypodermis, and bone/muscle

Arterial/ ischemic ulcers
causes: poor O2/CO2 diffusion, inadequate blood flow
signs and symptoms: intermittent claudication, dependent rubor, white skin, tissue death, mild to moderate edema, weak pulse (1+)
clinical presentation: round, regular border, punched out, pink wound bed, dry necrotic tissue, usually distal, minimal drainage, pain in elevated position
treatment: dressing to provide moisture and prevent infection, restore BF

venous ulcers
causes: arteries become more elastic> blood pooling in LEs
Clinical presentations: edema, strong pulse (3+), hemosiderin deposition, spider veins, dull acheiness when on feets, irregular borders
treatment: compression, elevation, exercise in elevated position, dressing to absorb fluid

Diabetic/ neuropathic ulcers
causes: hyperglycemia, decreased sensation, increased plantar foot pressure
clinical presentation: usually along pressure points, punched out appearance, deep w/ calloused edges, not painful, minimal drainage, dry cracked skin, callous
treatment: offload, glucose control, non-occlusive dressing
Use Wegener scale to grade

Pressure ulcers
pressure to bony prominence
different stages
Treatment: offload, dressing to absorb drainage, nutrition consult and supplementation (albumin and prealbumin)
Stage 1 pressure ulcer
change in skin color/ temp
persistent red discoloration
skin is intact
non blanchable erythema

Stage 2 pressure ulcer
partial thickness
skin loss of dermis and epidermis
red, pink, moist blistered

Stage 3 pressure ulcer
full thickness
skin loss fo dermis and/or epidermis
adipose visible
slough/ eschar may be present
no tendon, muscle, or bone

Stage 4 pressure ulcer
full thickness skin less to muscle, bone, and/or supporting structures
tendon, bone, muscle exposed
Deep tissue injury pressure ulcer
deep red/purple discoloration that is not blanchable, includes blood filled blisters

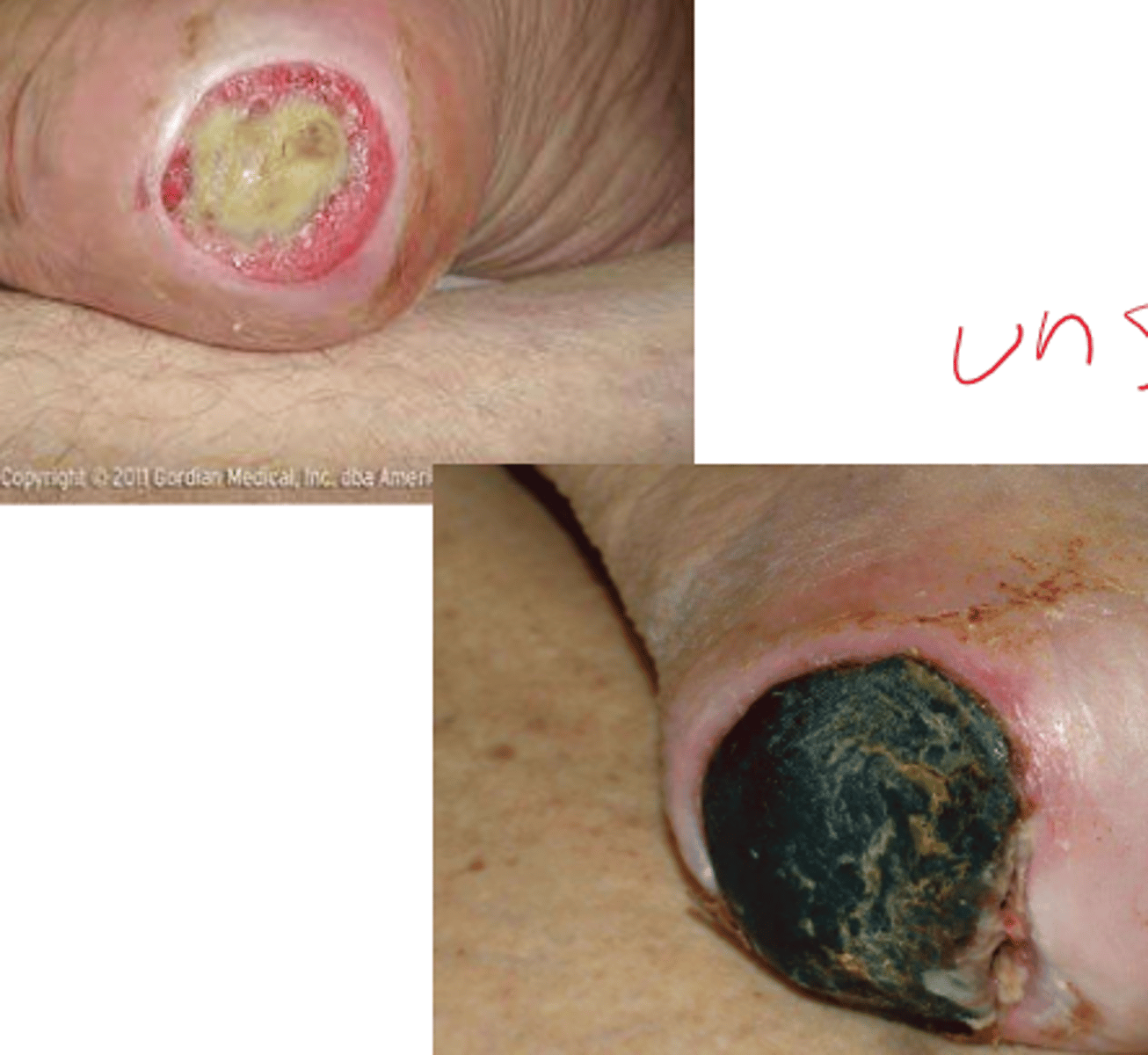
Unstageable pressure ulcer
necrosis present such that base cannot be visualized
cannot be staged
Surgical wounds
treatment: wound vac
dressing to prevent
compression
nutrition
acute surgical wound/ primary intention
surgically closed
Secondary intention wound healing
not surgically closed
Inflammatory reaction is more intense, much larger amounts of granulation tissue are formed
Tertiary wound healing
delayed primary closure
days. This occurs when the process of secondary intention is intentionally interrupted and the wound is mechanically closed. This happens after granulation tissue has formed, sutures are used and opens back up.