Neuropathology II: Dementia - Alzheimer's Disease and Parkinson's Disease
1/76
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
77 Terms
loss of functionally related neurons
What is neurodegeneration?
the specific neuronal population lost
What do symptoms of neurodegeneration depend on?
dementia
What symptom does neurodegeneration of cortical neurons lead to?
movement disorders
What symptom does neurodegeneration of basal ganglia neurons lead to?
ataxia
What symptom does neurodegeneration of cerebellar neurons lead to?
weakness
What symptom does neurodegeneration of motor neurons lead to?
-neurodegenerative disorders
*Alzheimer's disease
*Dementia with Lewy bodies
*Parkinson's disease
*Frontotemporal lobar degeneration (FTLD)
-vascular disease
*large vessel disease, multiple infarcts
*small vessel disease, Binswanger's disease
*CADASIL
-familial amyloid angiopathies
-inflammatory and immunemediated disorders
-viral infection (e.g. HIV, PML)
-prion disorders (e.g. CJD)
-toxic and metabolic disorders
*alcoholism
*B12 deficiency
-other conditions (e.g. tumors, traumatic injury)
What are 7 potential causes of dementia, and explain?
history of Alzheimer's:
a progressive, degenerative, and "incurable" neurological brain disease that causes deterioration of brain's nerve cells and ultimately death
What is Alzheimer's Disease (AD)?
in their mid-60s
When do most people show symptoms and signs of AD?
> 5 million Americans
What is the number of Americans who may have AD?
is the 6th leading cause of overall death in the US; the 3rd leading cause of death for older people (just behind heart disease and cancer)
How does AD contribute to death in the US, and explain?
complex interactions among multiple genetic, epigenetic, and environmental factors -> multifactorial!
What is the etiology of AD like?
-gene mutations
-Down syndrome
-Apolipoprotein E4
-aging
-epigenetic mechanisms
-potential environmental risk factors
What are the 6 main risk factors for AD?
*amyloid precursor protein (APP)
*presenilin-1 (PS-1)
*presenilin-2 (PS-2)
What are the 3 main gene mutations that function as risk factors for AD?
-autosomal dominant AD
-early onset (<65 years)
-<1% of AD cases
How do gene mutations, amyloid precursor protein (APP), presenilin-1 (PS-1), and presenilin-2 (PS-2), play a role in AD?
the APP gene is on chromosome 21, thus the additional copy of this chromosome increases the chance of AD
How does Down syndrome play a role in AD?
two copies of the apo34 gene (2% of the population) -> late onset (>65 years), familial or sporadic AD
How does Apolipoprotein E4 play a role in AD?
is the most important known non-genetic risk factor for late onset of AD
How does aging play a role in AD?
-abnormal DNA methylation
-histone modification
-> not known if it is a cause or consequence
What are 2 epigenetic mechanisms that play a role in AD, and explain?
-head injury
-diabetes
-obesity
-hyperlipidemia
-HTN
-low education levels
What are 6 potential environmental risk factors of AD?
-clinically
-brain autopsy
What are the 2 ways in which AD can be diagnosed?
-possible AD
OR
-probable AD
(NOT definitive)
What are the diagnostic results like in a clinical diagnosis of AD?
*slow-onset memory loss (begins with short-term memory loss, progress to long-term memory loss), eventually disorientation
*changes in behavior and personality
*loss of learned motor skills and language
*mute and bedridden -> infection is a common cause of death
What are the clinical features of AD seen in a clinical diagnosis of AD?
definitive diagnosis
What are the diagnostic results like in a brain autopsy diagnosis of AD?
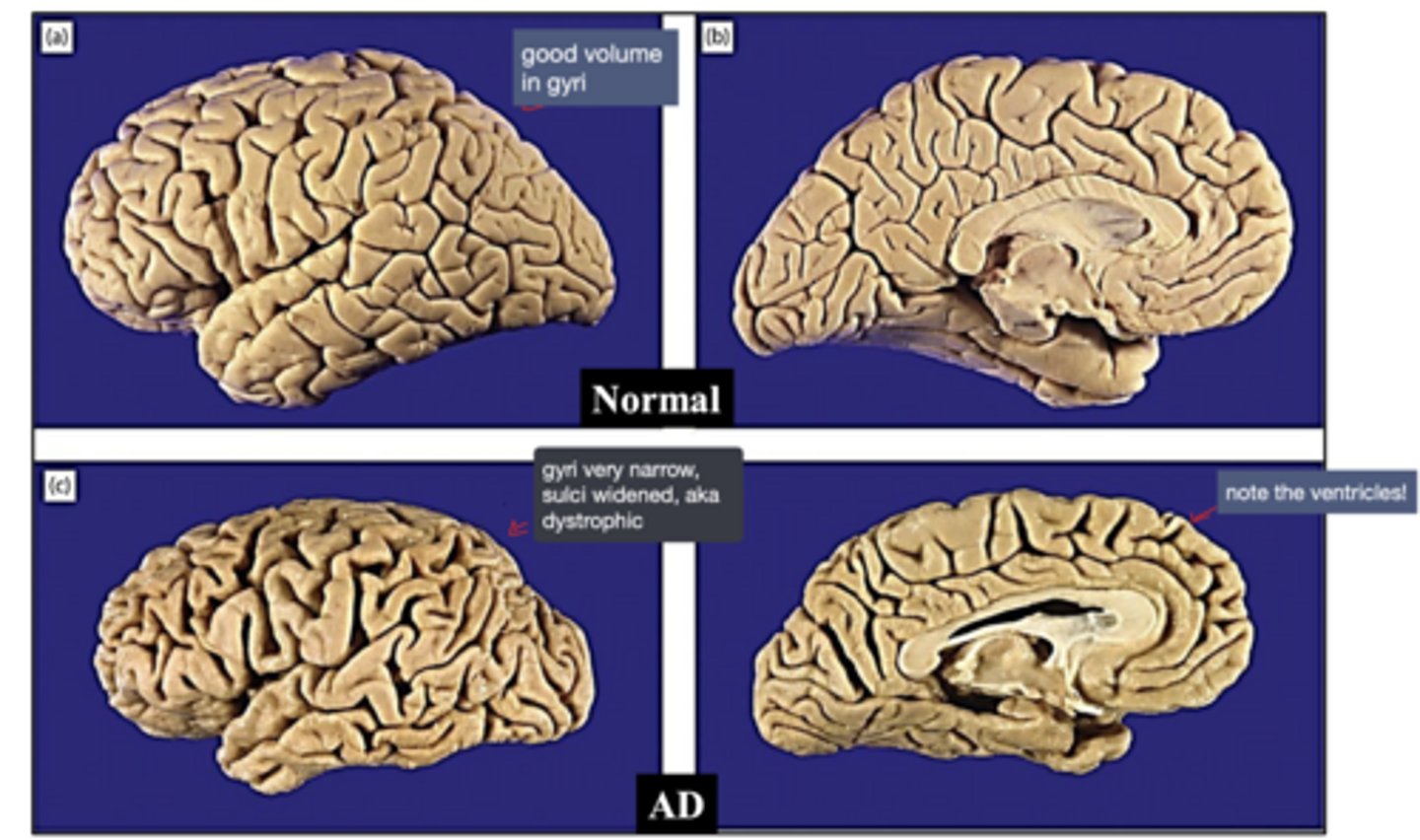
neuropathological changes in AD:
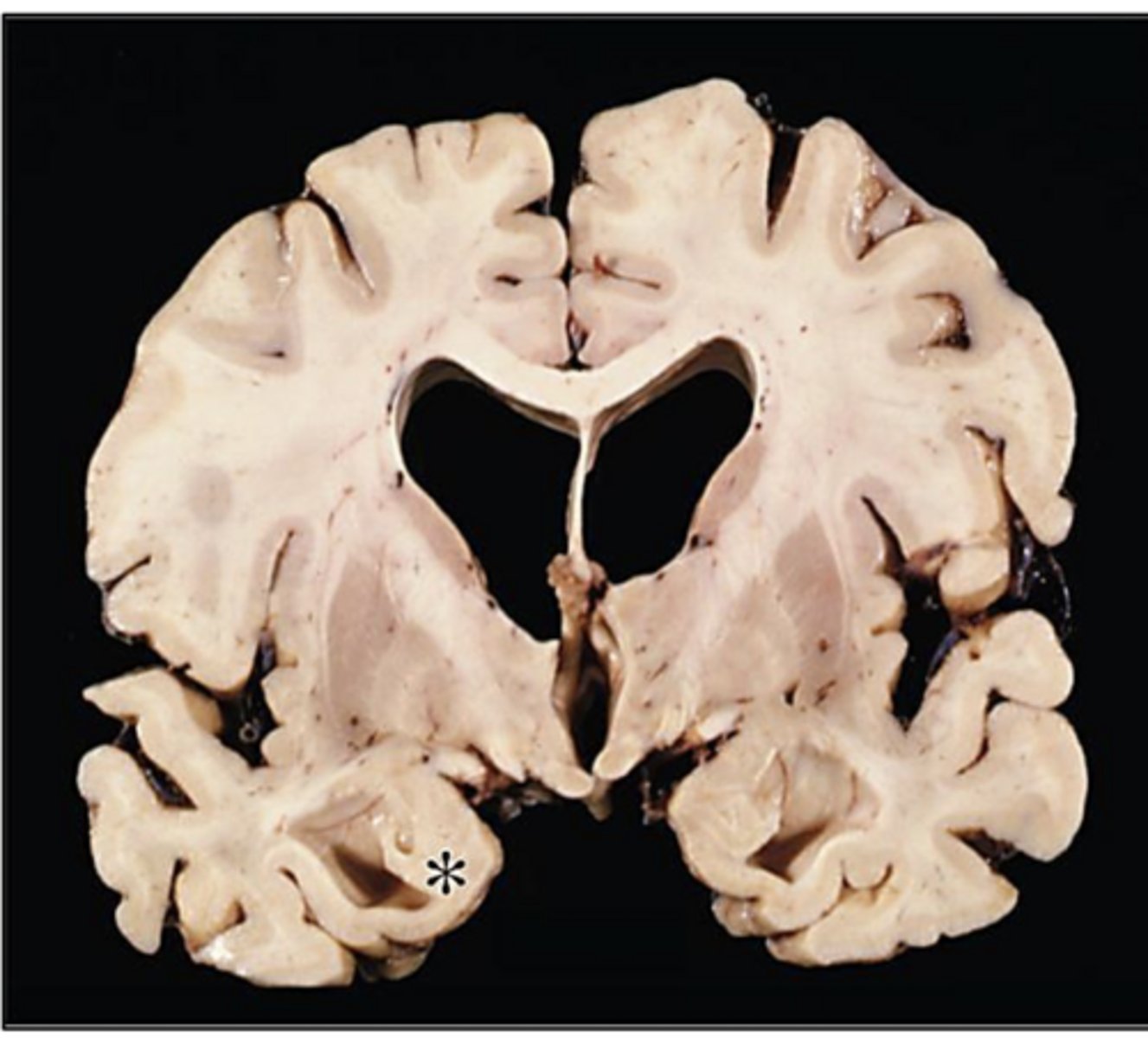
AD -> characteristic atrophy of the entorhinal cortex is seen, with resultant dilation of the temporal horn of the lateral ventricles
* = amygdala
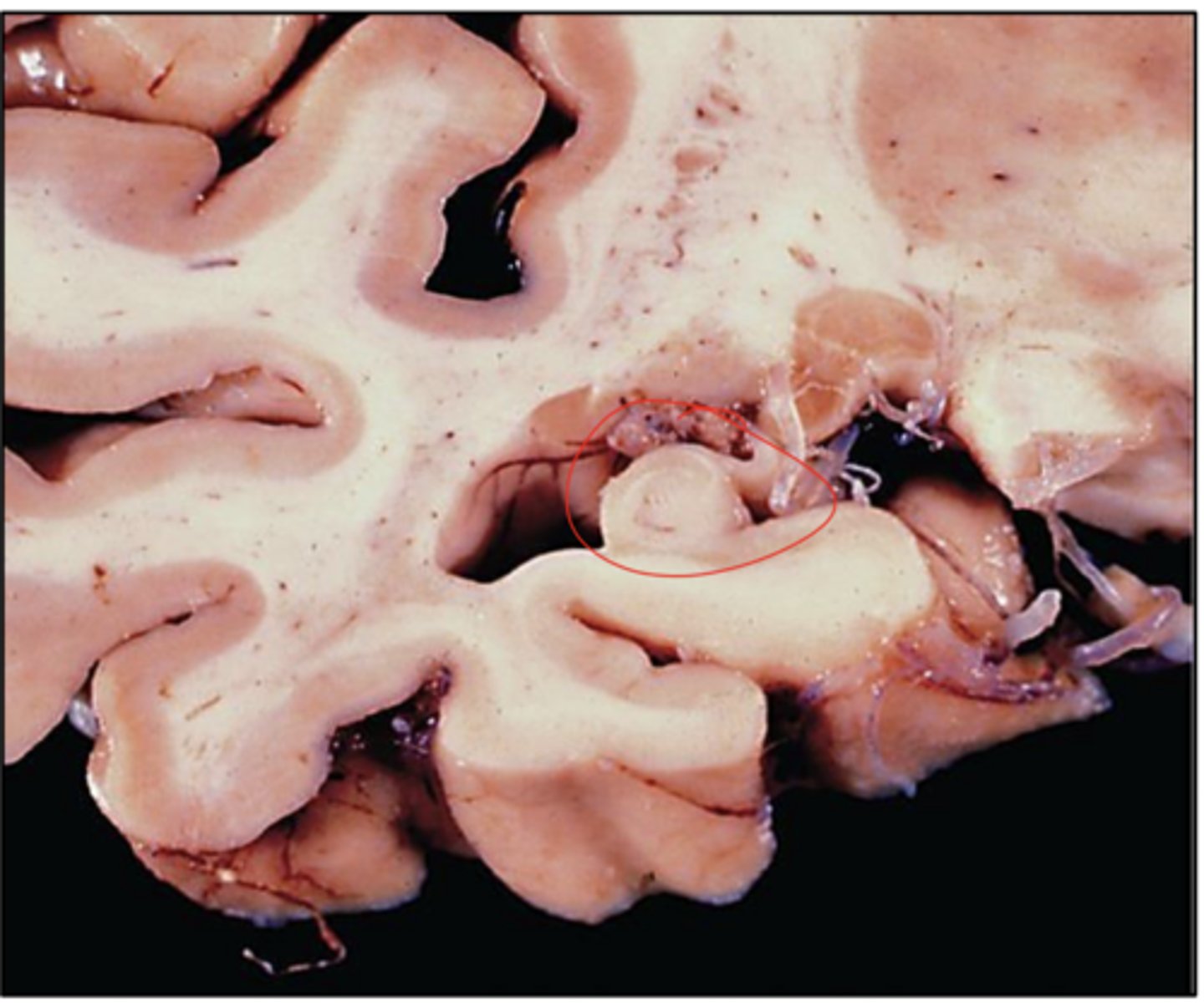
small hippocampus in case of AD -> associated with memory loss
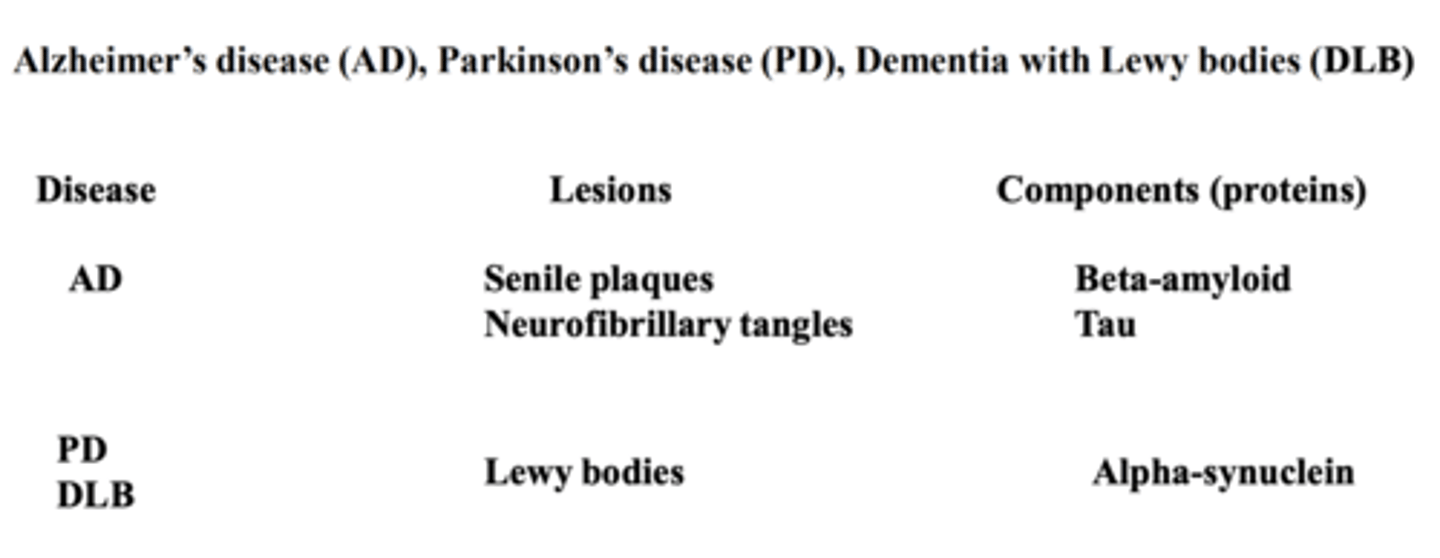
-amyloid plaques
-neurofibrillary tangles (NFTs)
What are the 2 main neuropathological hallmarks of AD?
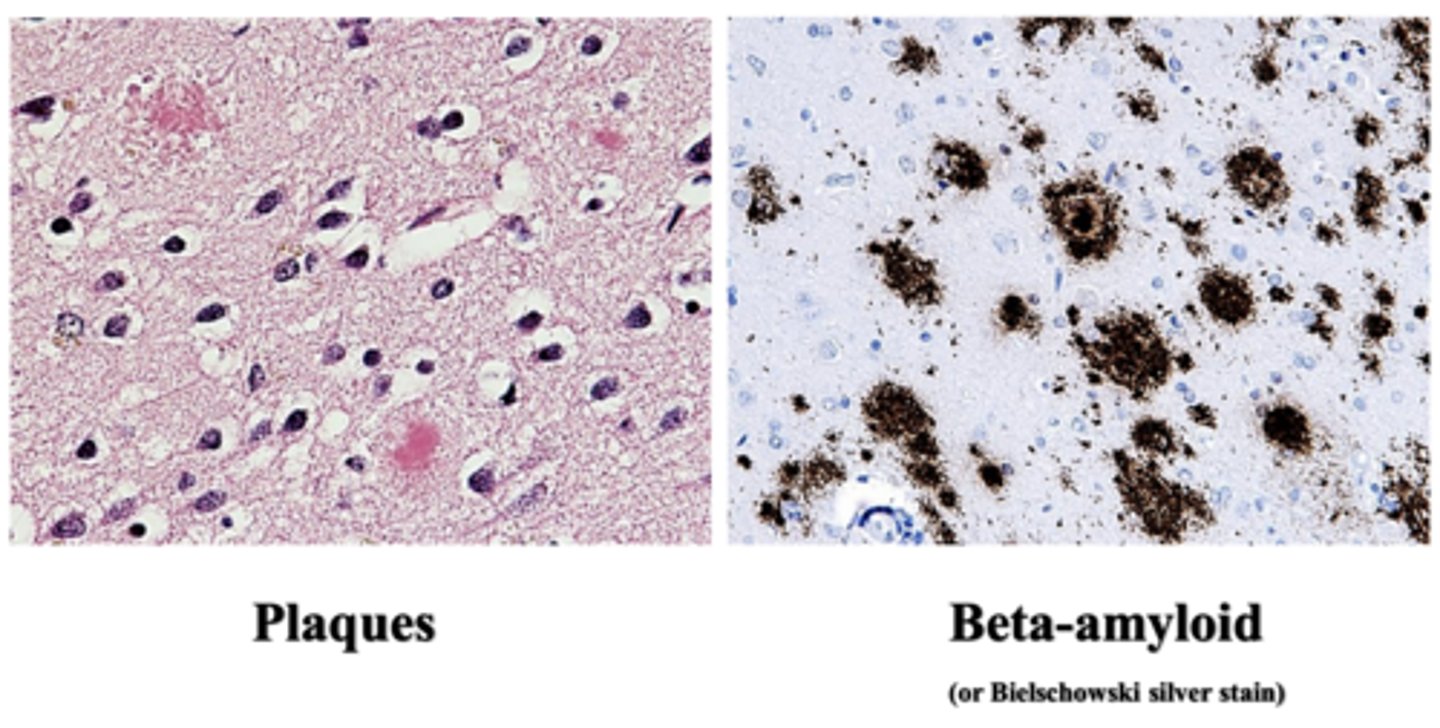
extracellular deposition of small spherical structures in brain parenchyma (amyloid-β peptide fragments)
What are amyloid plaques?
senile plaques
What are amyloid plaques also known as?
beta amyloid
What is the core of senile plaques/amyloid plaques comprised of?
transmembrane amyloid precursor protein (APP)
Where is beta amyloid derived from?
locus on chromosome 21
Where is the APP gene encoded?
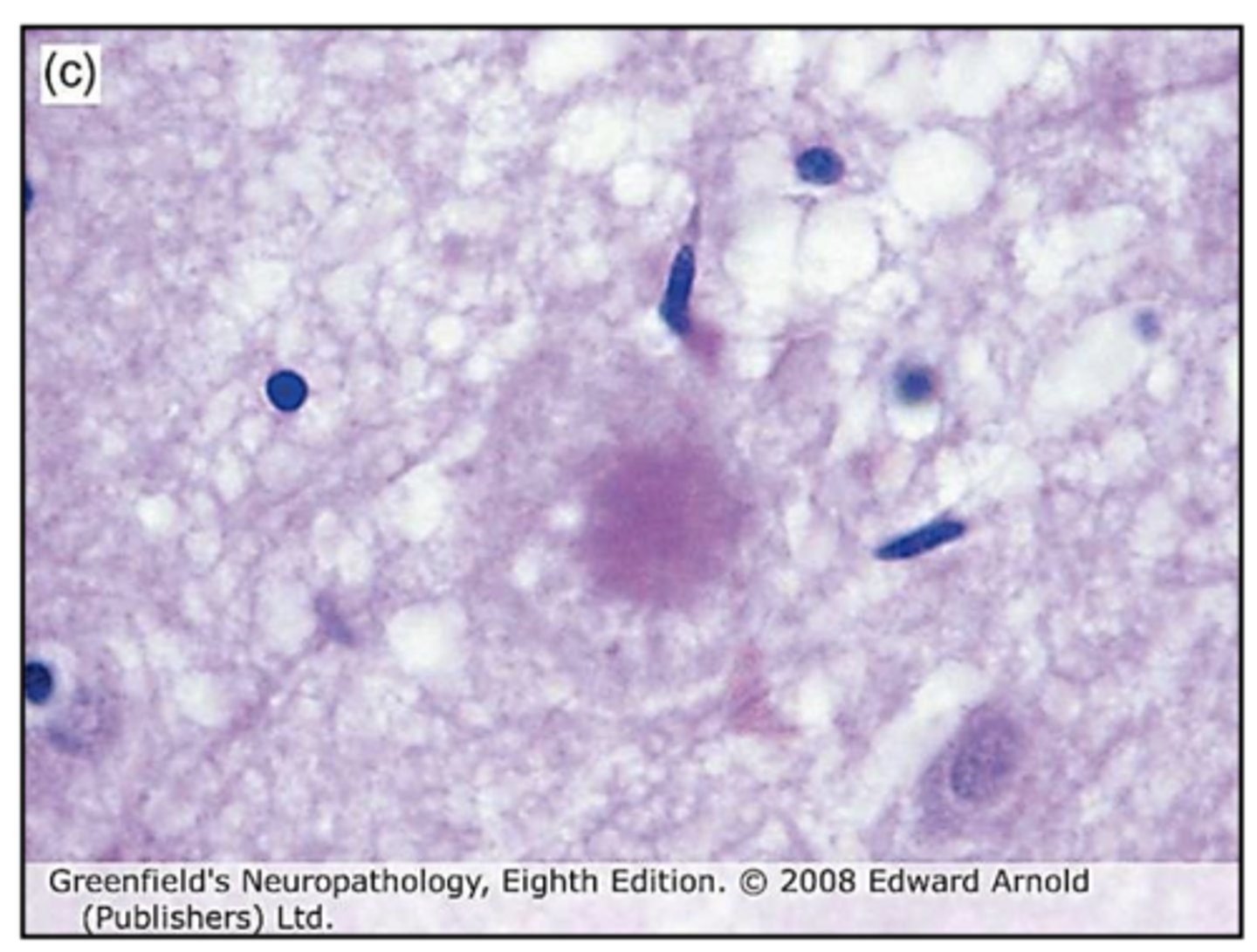
senile plaques
plaques
*well-formed tangles
*"ghost tangles"
*"pre-tangles"
What are the 3 different types of neurofibrillary tangles (NFTs) that act as neuropathological hallmarks of AD?
intracytoplasmic flame-shaped fiber-like bundles
What are well-formed tangles?
when neurons are lost
What are "ghost tangles"?
perinuclear, non-fibrillary Tau-positive structures
What are "pre-tangles"?
Tau protein
What are neurofibrillary tangles (NFTs) formed by?
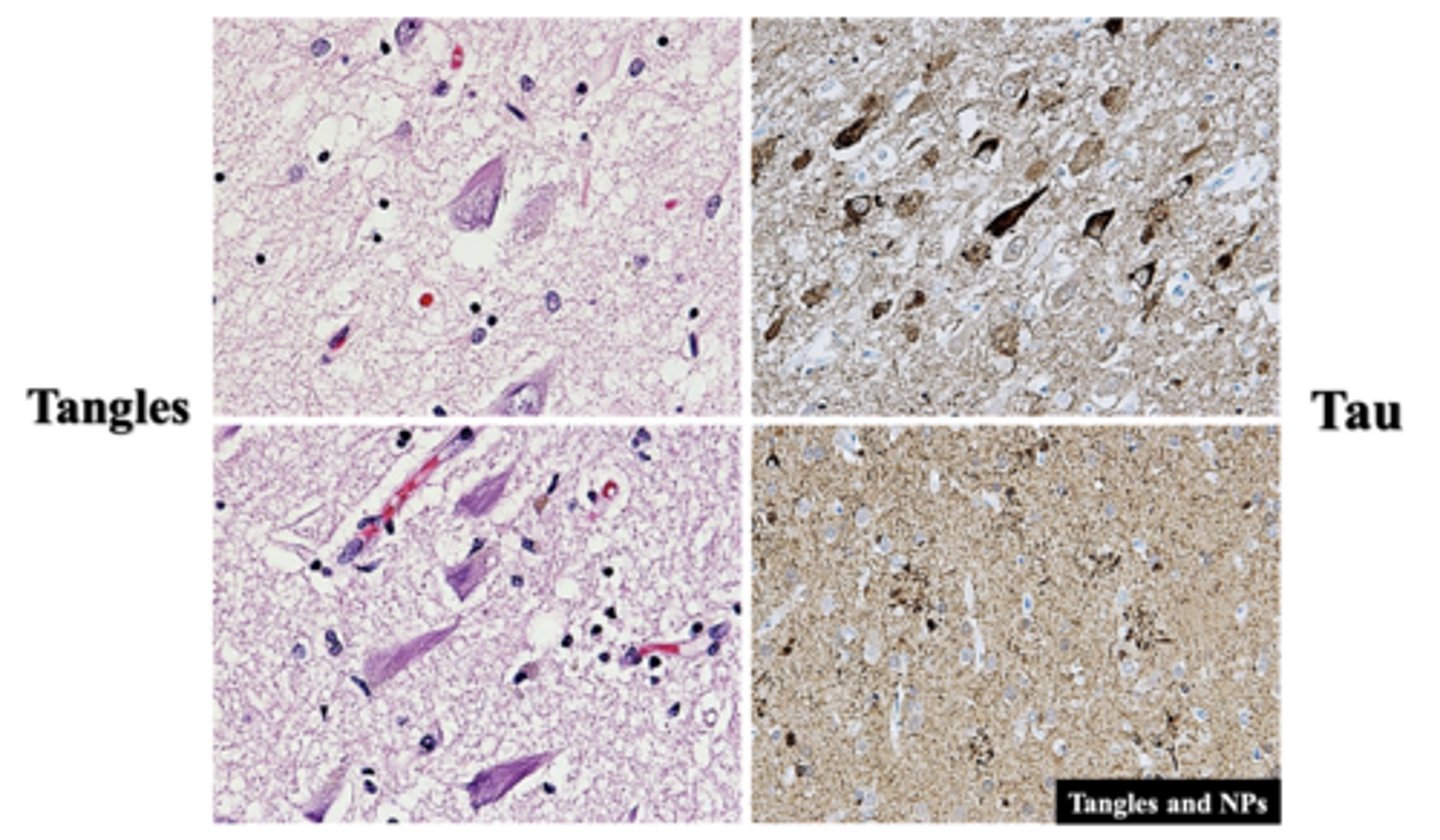
tangles
a vascular disease involving amyloid protein buildup in brain blood vessels; commonly co-exists with AD
What is cerebral amyloid angiopathy (CAA), and how is it relevant to AD?
in the parieto-occipital region
Where is cerebral amyloid angiopathy (CAA) more prominent?
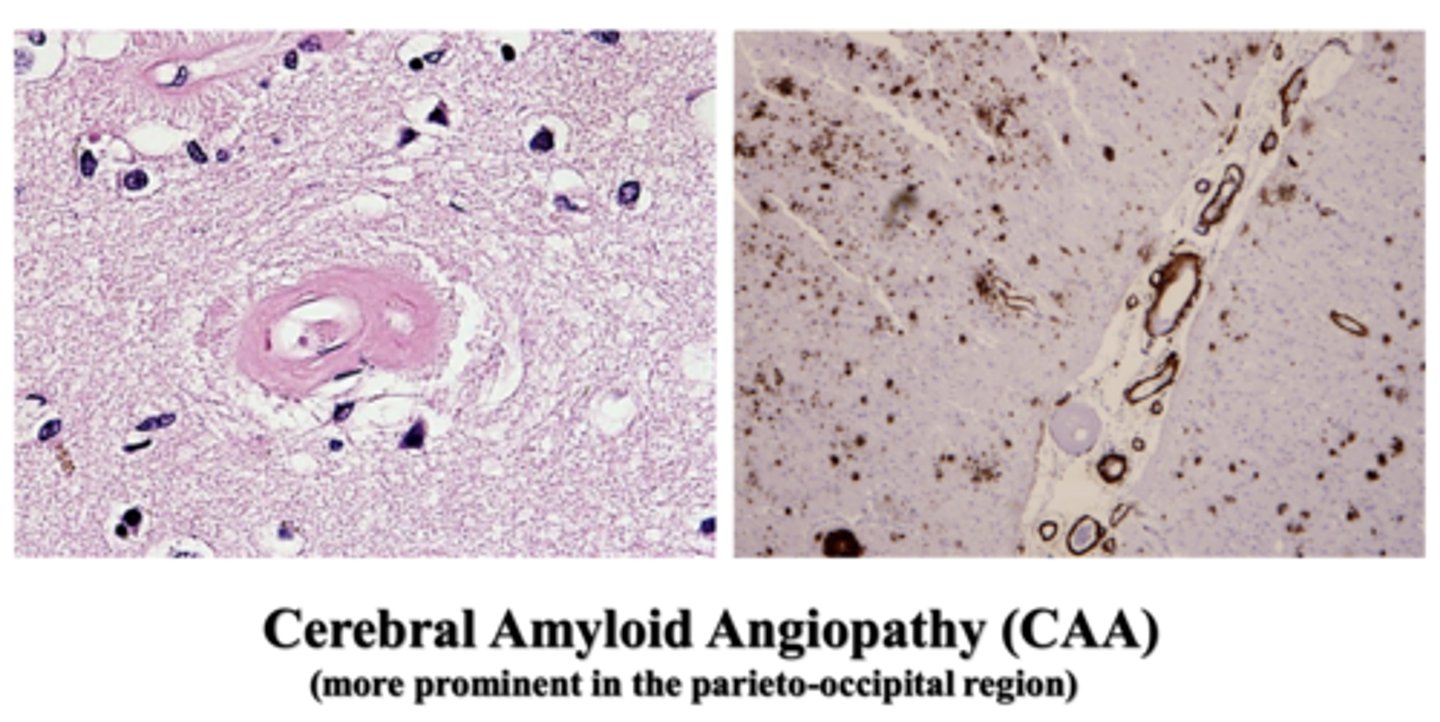
note the hyalinized, thickened vessel wall on the left
using "ABC score"
How is the severity of AD assessed?
the distribution and density of plaque and NFTs
What does the "ABC score" analyze?
just for reference
*DON'T memorize, understand -> based on this table and known distribution and density of amyloid plaques and NFTs, one can obtain an A, B, and C score
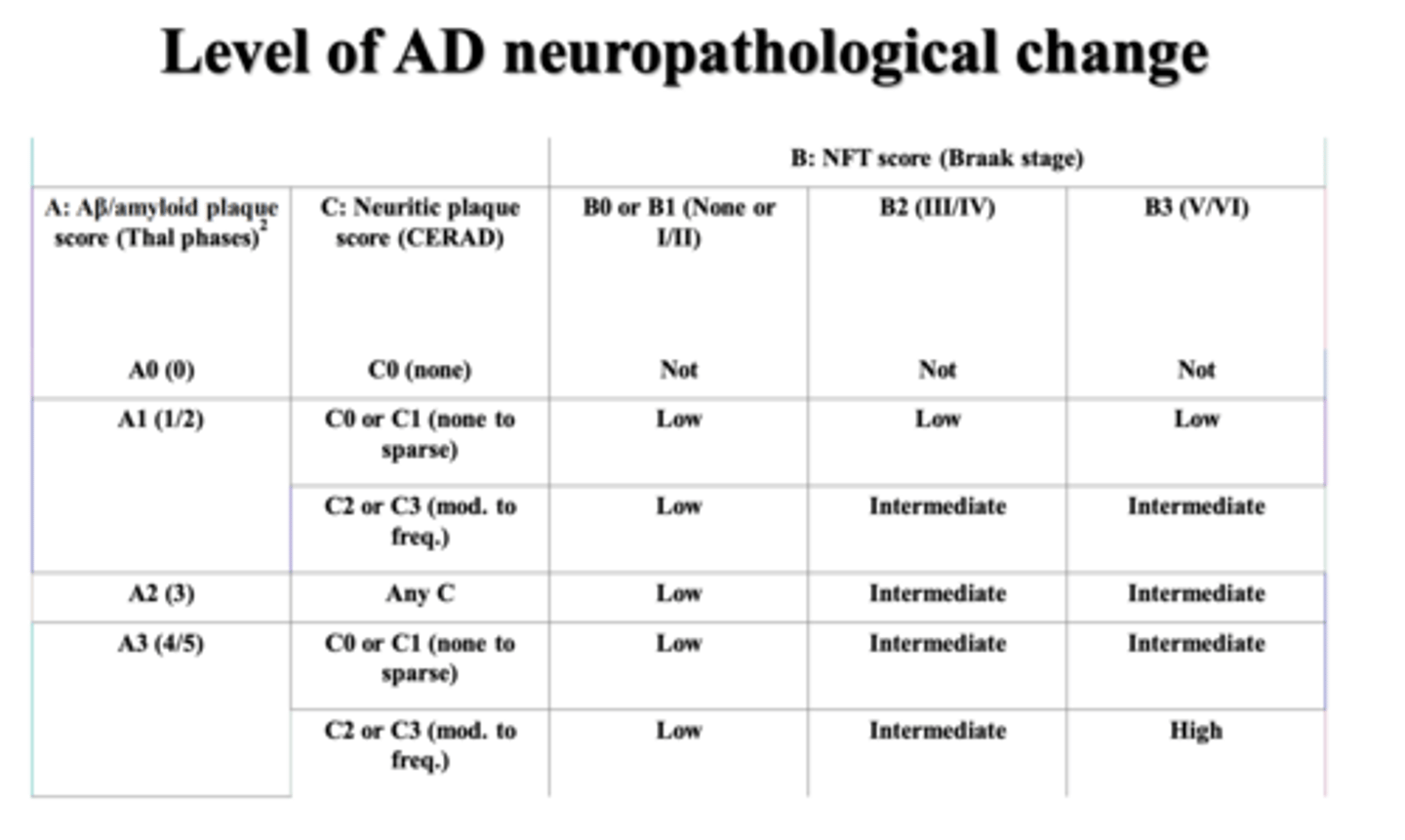
brain, autopsy
-> Alzheimer's disease neuropathological changes: A3B3C3 or A1B1C1
Regardless of clinical history, what format should reports follow, and explain?
intermediate or high level
For individuals with known cognitive impairment/dementia at the time tissue was obtained, what is considered adequate explanation of cognitive impairment/dementia?
a group of neurological disorders that cause movement problems similar to those seen in Parkinson's disease; such as tremors, slow movement, and stiffness
What is Parkinsonism, and explain?
-history
-clinical examination
What 2 things does the diagnosis of most movement disorders rest on?
definitive dx does not require pathology, as does AD
How does the diagnosis of most movement disorders differ from AD?
accurate recognition of the entire clinical phenotype
What is the key step towards a diagnosis of a movement disorder?
-Parkinson's disease
-Atypical Parkinson's disorders (Parkinson's plus )
-secondary or symptomatic Parkinsonism
-common mimics of Parkinsonism
What 4 conditions fall under the category of Parkinsonism?
-classical clinical syndrome
-loss of dopaminergic neurons in SN
-brainstem with Lewy bodies
What are 3 differential features of Parkinson's disease?
a neurodegenerative disease marked by a prominent hypokinetic movement disorder that is caused by loss of dopaminergic neurons from the SN
What is Parkinson's disease (PD)?
-age
-hereditary/genetic factor
-sex
-exposure to toxins
What are 4 main risk factors for PD?
>/= 60; ~5-15% onset before 50
How is age a risk factor for PD?
-juvenile Parkinsonism (onset <21)
-young onset Parkinsonism (onset between 21-40)
What are 2 examples of heredity/genetics as a risk factor for PD?
male > female; neuroprotective effect by estrogen
How is sex a risk factor for PD, and explain?
exposure to herbicides, pesticides leads to slightly increased risk of PD
How is exposure to toxins a risk factor for PD?
-loss or degeneration of the dopaminergic neurons in the SN
-development of Lewy Bodies (the pathologic hallmark) in dopaminergic neurons
-significant neuronal loss of locus coeruleus with Lewy bodies formation
What are the 3 main pathophysiologic characteristics associated with PD?
-protein accumulation and aggregation (alpha synuclein)
-mitochondrial abnormalities
-neuronal loss in the substantia nigra and elsewhere in the brain
(he said not so important)
What 3 molecular genetics/pathogenesis characteristics is PD associated with?
“TRAP”
-Tremor -> pill rolling tremor at rest, disappears with movement
-Rigidity -> cogwheel rigidity in the extremities
-Akinesia/bradykinesia -> slowing of voluntary movement; expressionless face
-Postural instability and shuffling gait
What are the 4 main components of the clinical presentation of PD?
-cognitive changes (e.g. dementia)
-depression (up to 45-50%)
-diminished sense of smell
-sleep disturbances
-90% of PD patients experience non-motor symptoms during the course of the disease
-the greatest challenges to quality of life and appropriate management in PD, since they usually do not respond to dopamine therapy
What are the 6 main non-motor symptoms associated with PD?
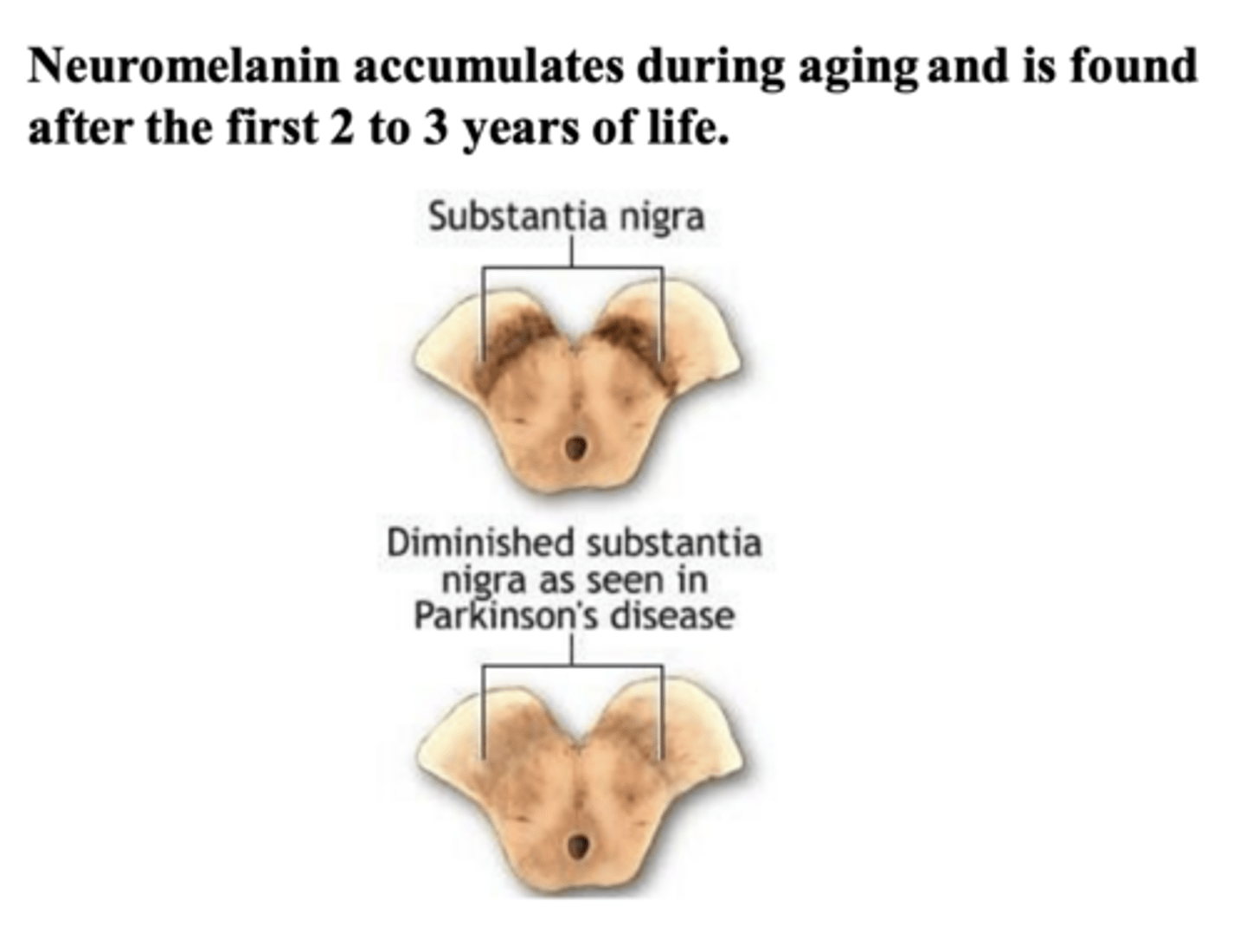
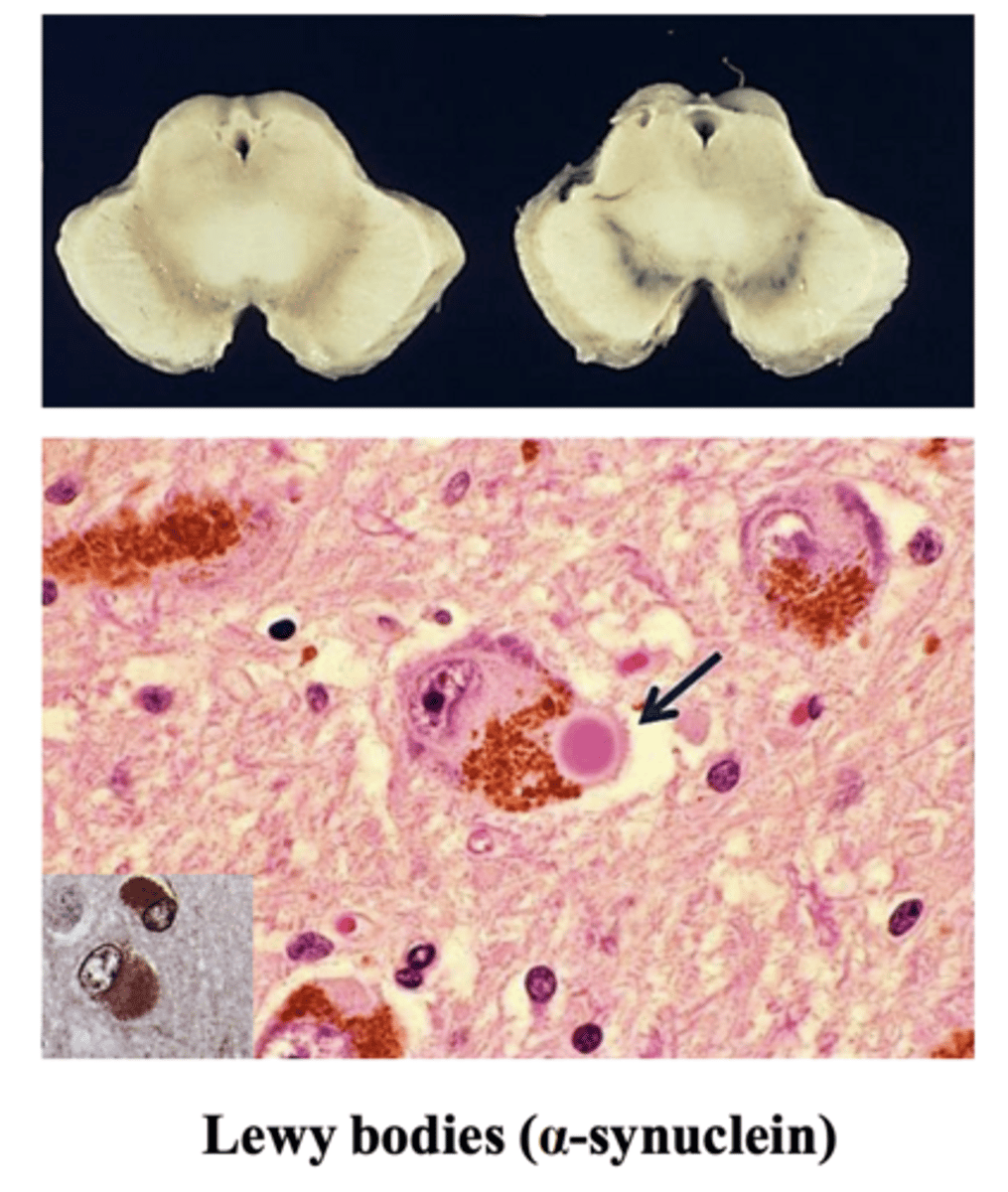
diminished substantia nigra pigmentation (hypopigmentation)
What is the neuroanatomy change that occurs in a PD patient?
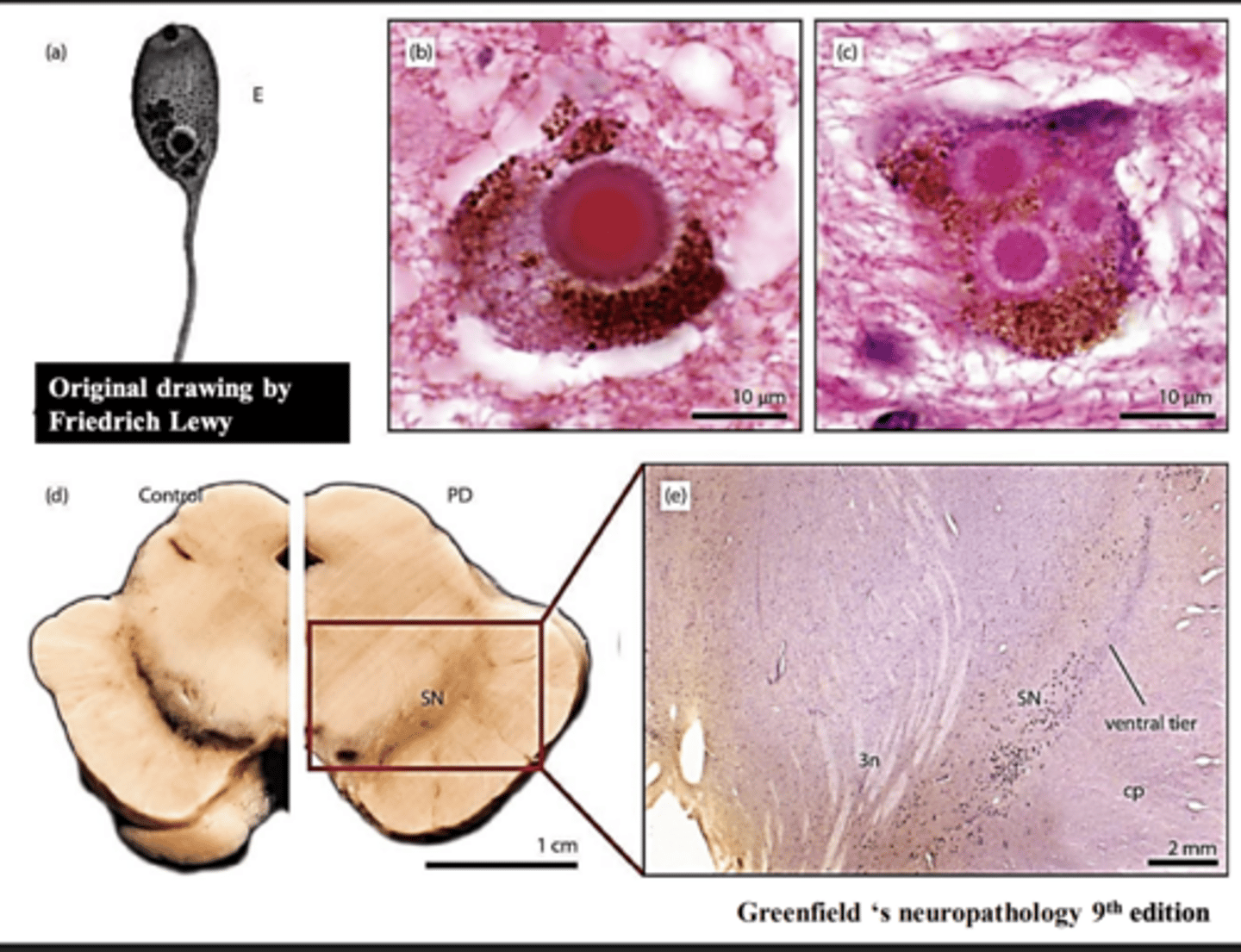
Lewy body -> homogenous spheroid structure
α-synuclein
What protein is responsible for the formation of Lewy bodies?
-dementia with Lewy bodies (DLB)
-multiple system atrophy (MSA)
-progressive supranuclear palsy (PSP)
-corticobasal degeneration (CBD)
What are 4 examples of atypical Parkinsonism disorders?
-more rapid disease progression
-a poor response to dopamine replacement therapy
-more widespread brain pathology
(clinical presentation of DLB is what makes it differ from classic PD)
What are the 3 main ways in which atypical Parkinsonism disorders differ from classic PD?
-numerous LBs in cerebral cortex
-hallucinations
-fluctuation in the level of consciousness
-if the onset of dementia is within 12 months of Parkinsonism’s onset, likely to be DLB
-by contrast, if the onset of Parkinsonism is more than 12 months earlier than dementia, likely to be PDD
What are 5 symptoms associated with dementia with Lewy bodies (DLB)?
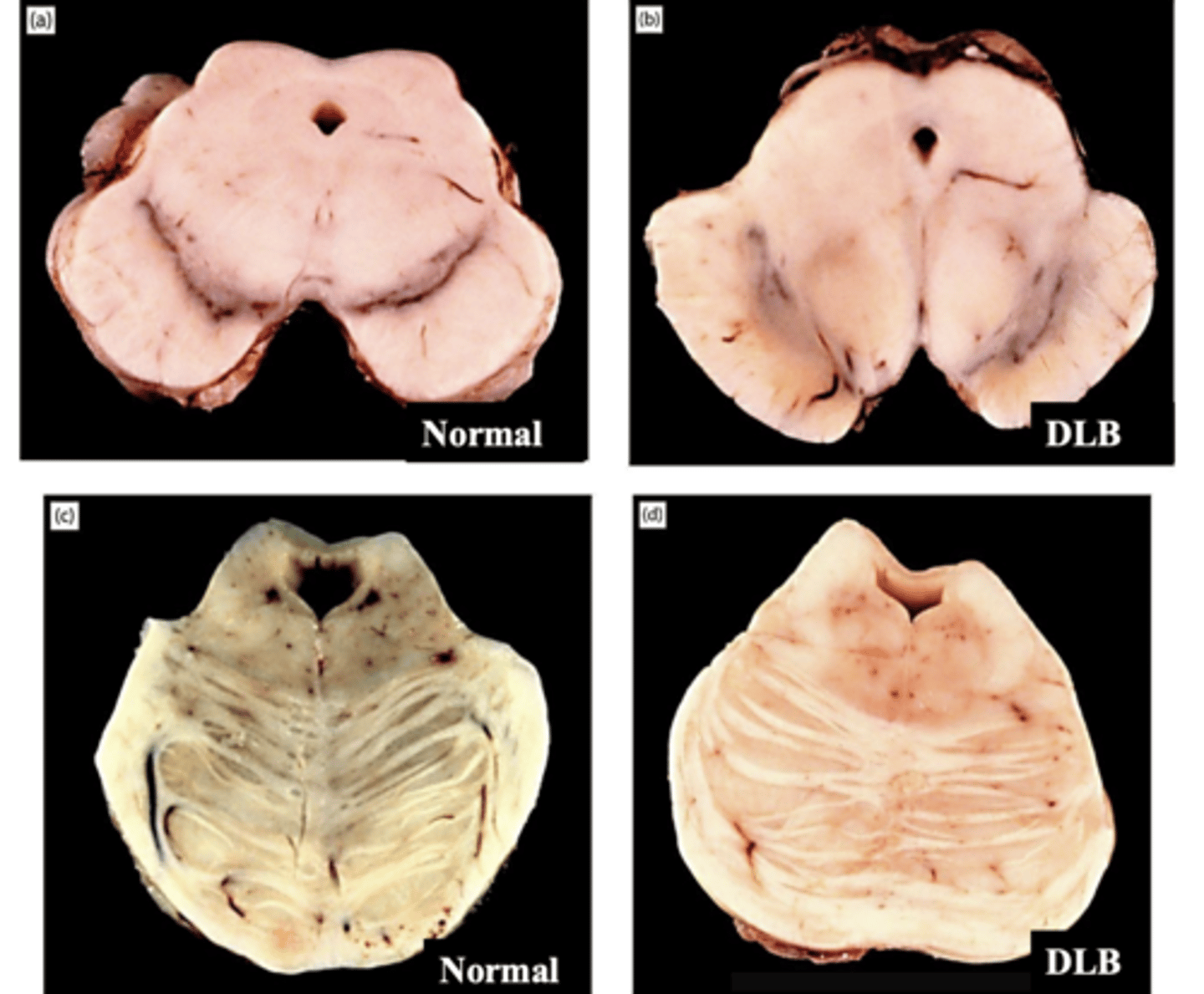
hypopigmentation of substantia nigra (top) and hypopigmentation of locus coeruleus (bottom)
KNOW THIS