USMLE Step 1: Musculoskeletal and Derm
1/160
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
161 Terms
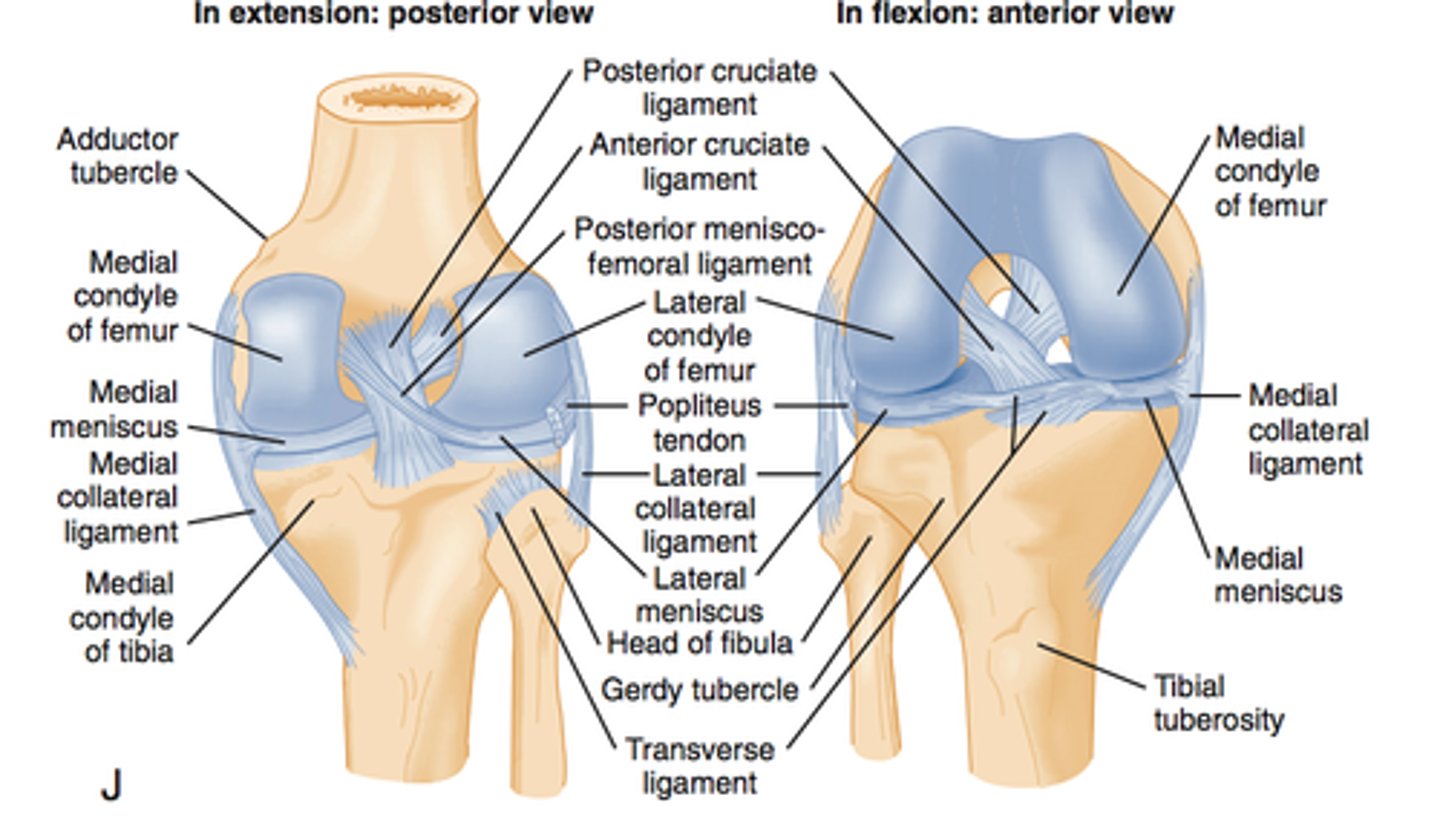
Knee Anatomy:
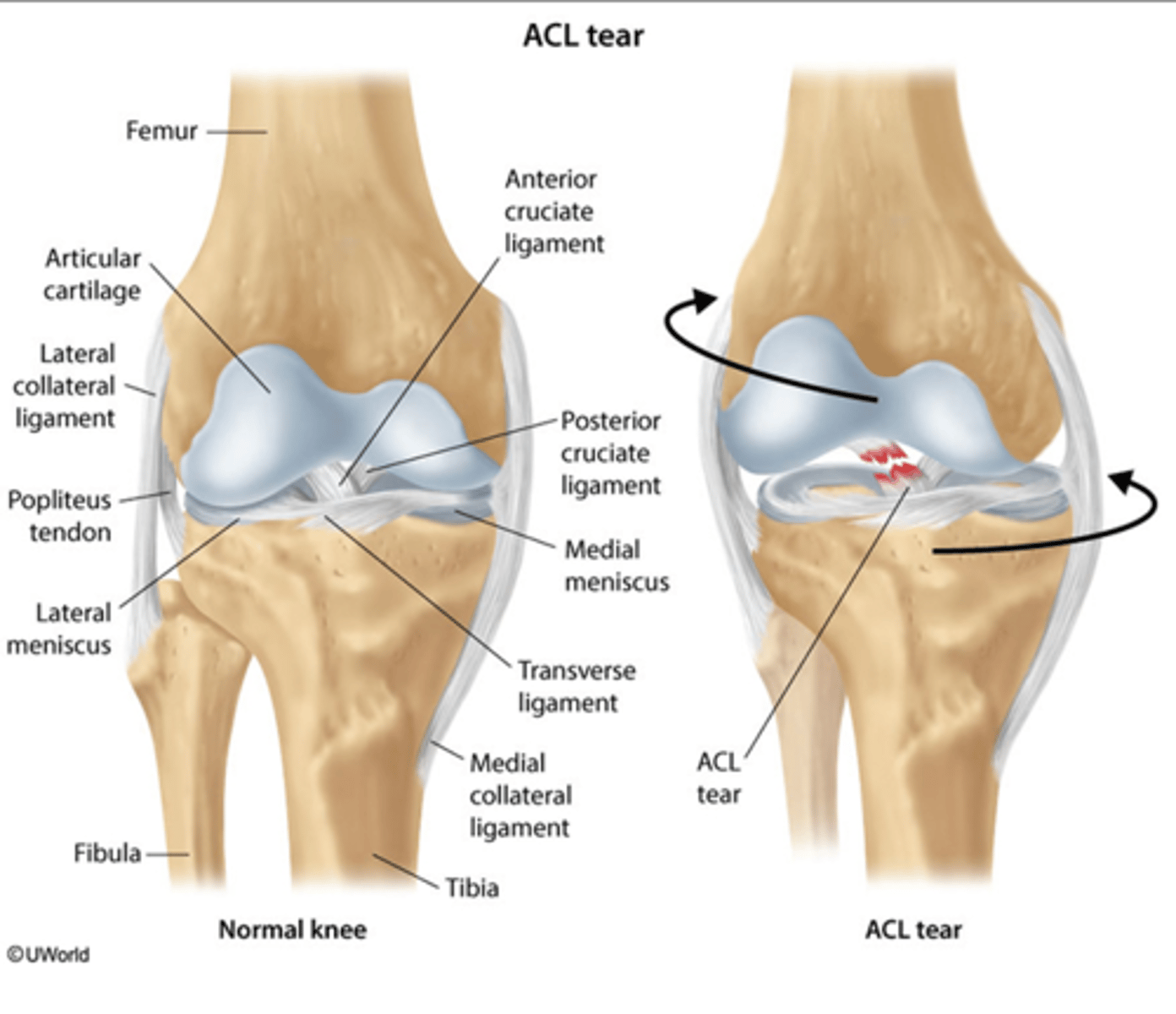
What does the ACL connect?
What does the PCL connect?
What does the ACL connect?
- extends from the lateral femoral condyle to the anterior tibia
- prevents anterior translocation at the knee joint
What does the PCL connect?
- extends from the medial femoral condyle to the posterior tibia
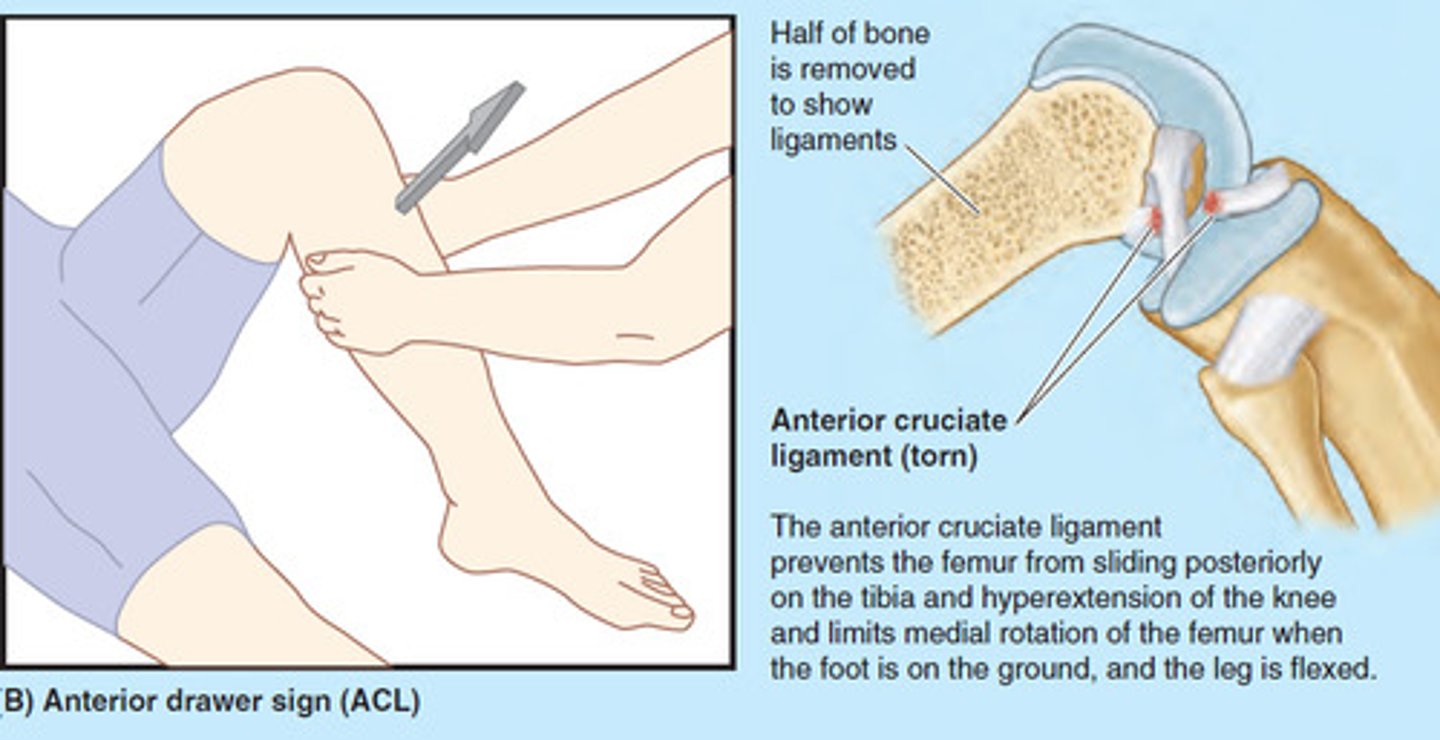
Anterior Drawer Sign
What does it test for?
How do you perform it and when is it positive?
What does it test for?
- tear of the ACL
How do you perform it?
- bending knee at 90 degree, pull knee anteriorly
- increased anterior gliding of the tibia seen in ACL injury
Note:
Lachman test is similar but at 30 degree angle
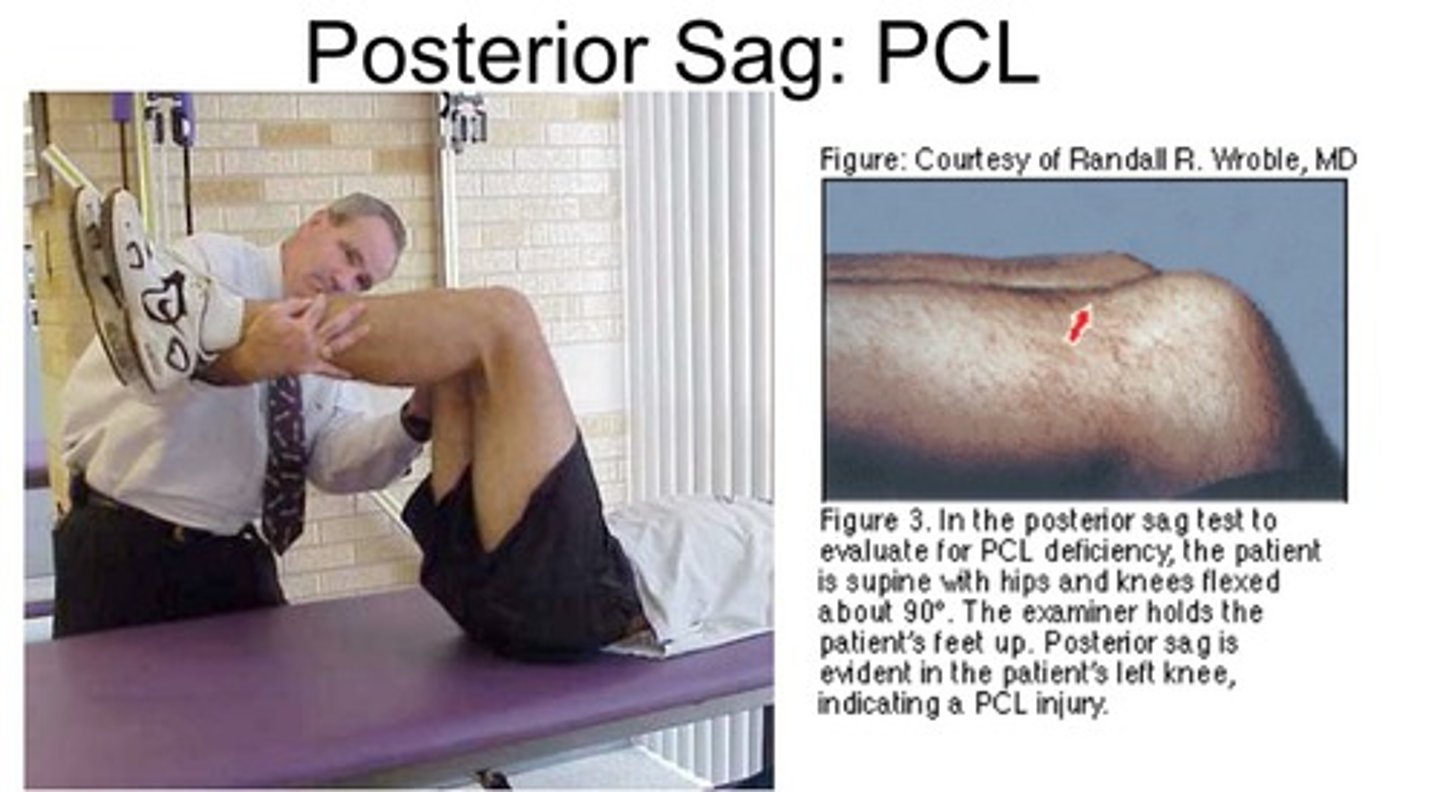
Posterior Drawer Sign
What does it test for?
How do you perform it?
What does it test for?
- torn PCL
How do you perform it?
- bend knee at 90 degree
- increased posterior gliding of tibia = PCL injury
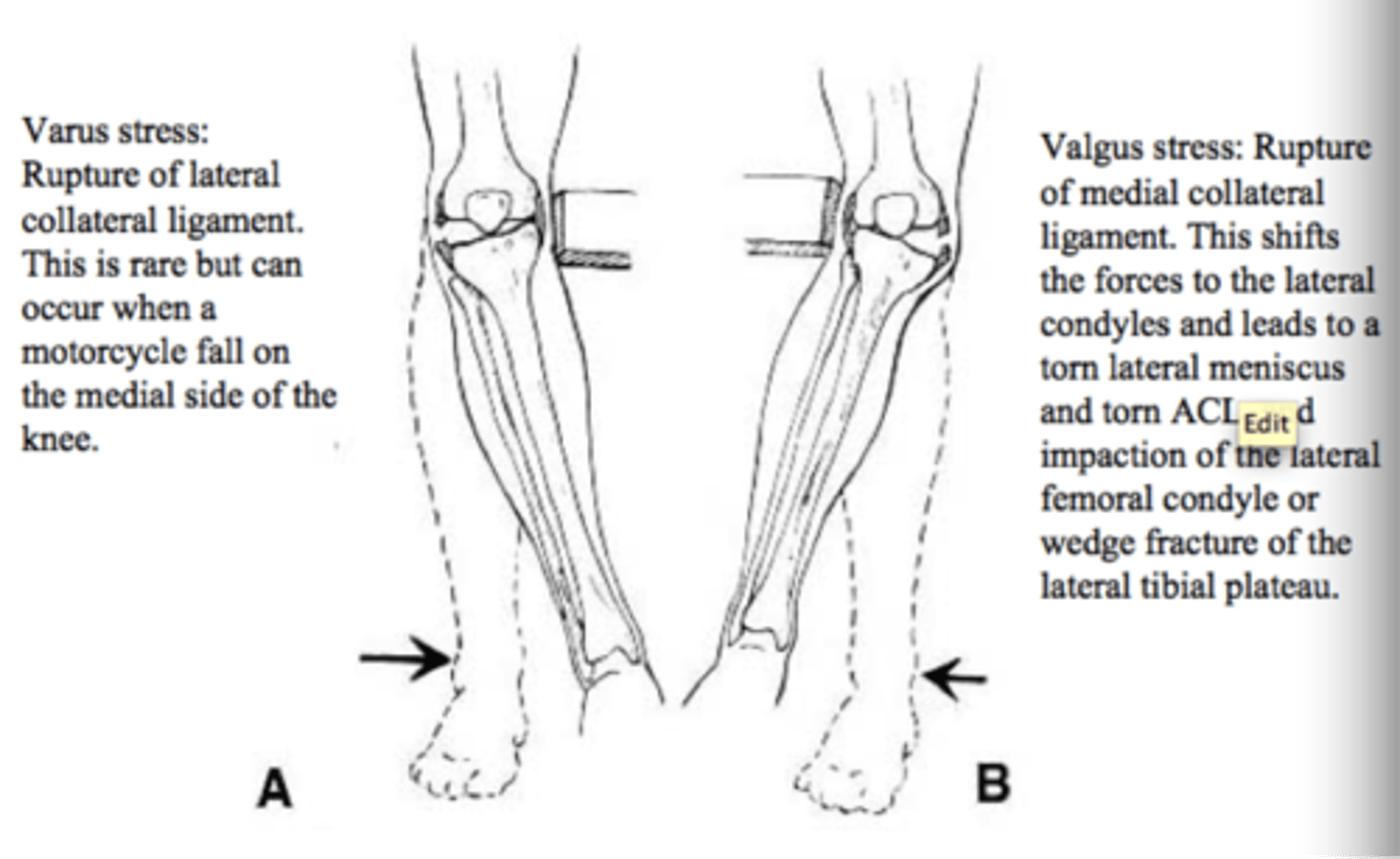
Abnormal Passive Adduction of the knee (VALGUS stress test)
What does it test for?
How do you perform it?
What does it test for?
- tear of the MCL
How do you perform it?
- knee extended or at 30 degree, apply force laterally (VALGUS/external rotation) while stabilizing knee
- if there is medial space widening --> MCL injury
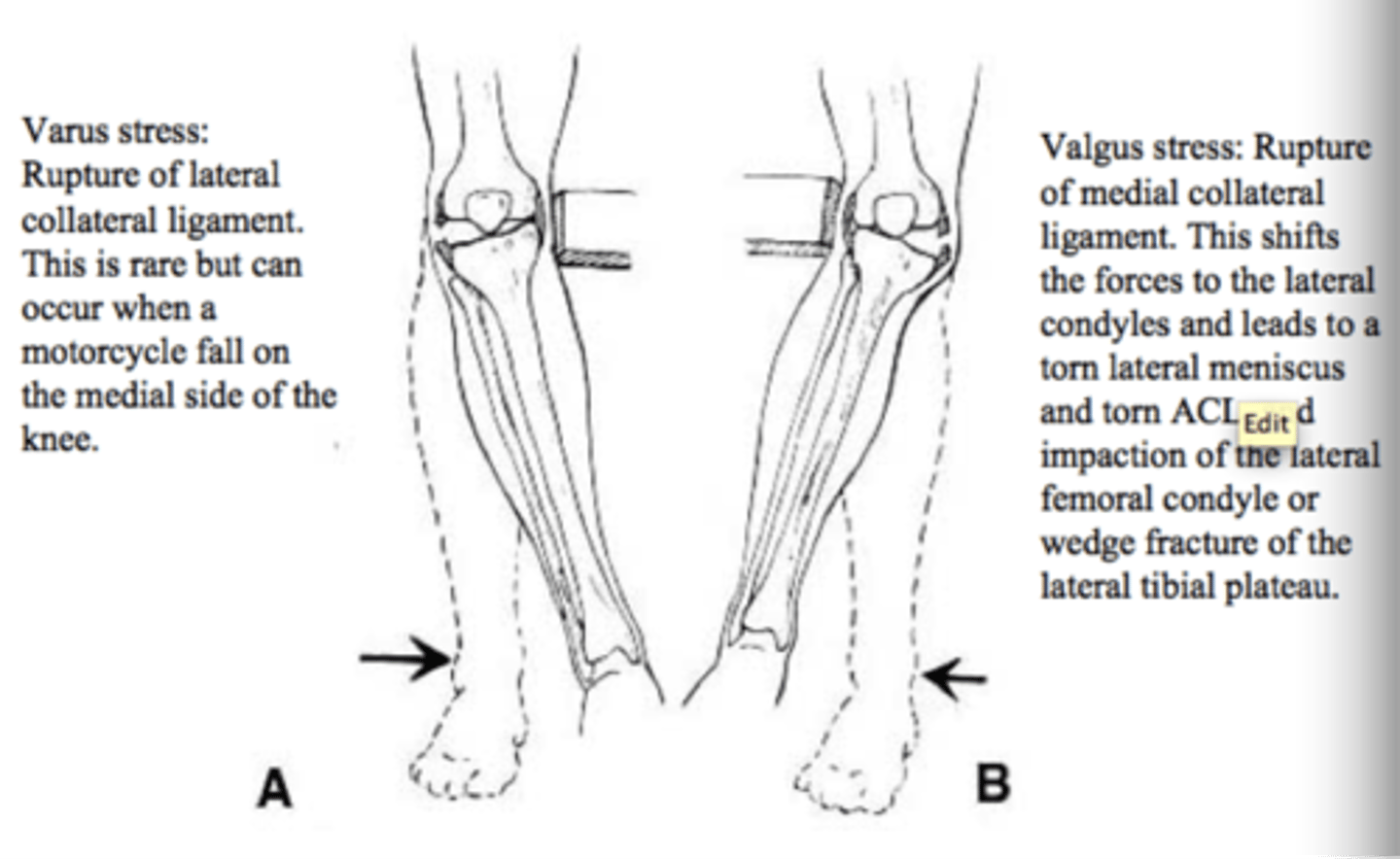
Abnormal Passive Adduction of the knee (VARUS stress test)
What does it test for?
How do you perform it?
What does it test for?
- tear of the LCL
How do you perform it?
- knee extended or at 30 degree, apply force medially (VARUS/internal rotation) while stabilizing knee
- if there is lateral space widening --> LCL injury
McMurray Test
What does it test for?
How do you perform it?
What does it test for?
- meniscal injury/tear
How do you perform it?
- flexion and extension of knee with rotation of the tibia/foot
IF pain, "popping" on external rotation --> medial meniscal tear
IF pain, "popping" on interal rotation --> lateral meniscal tear

Knee Anatomy
What does it test for?
How do you perform it?
What does it test for?
How do you perform it?
What is the "unhappy triad" knee condition caused by?
What is injured?
How does it present?
What is the "unhappy triad" knee condition?
- a common injury in contact sports due to lateral force applied to a planted leg
What is injured?
- classically consists of damage to the ACL, MCL and menial meniscus
- however, damage to the lateral meniscus is more common
How does it present?
- acute knee pain and signs of joint injury and instability
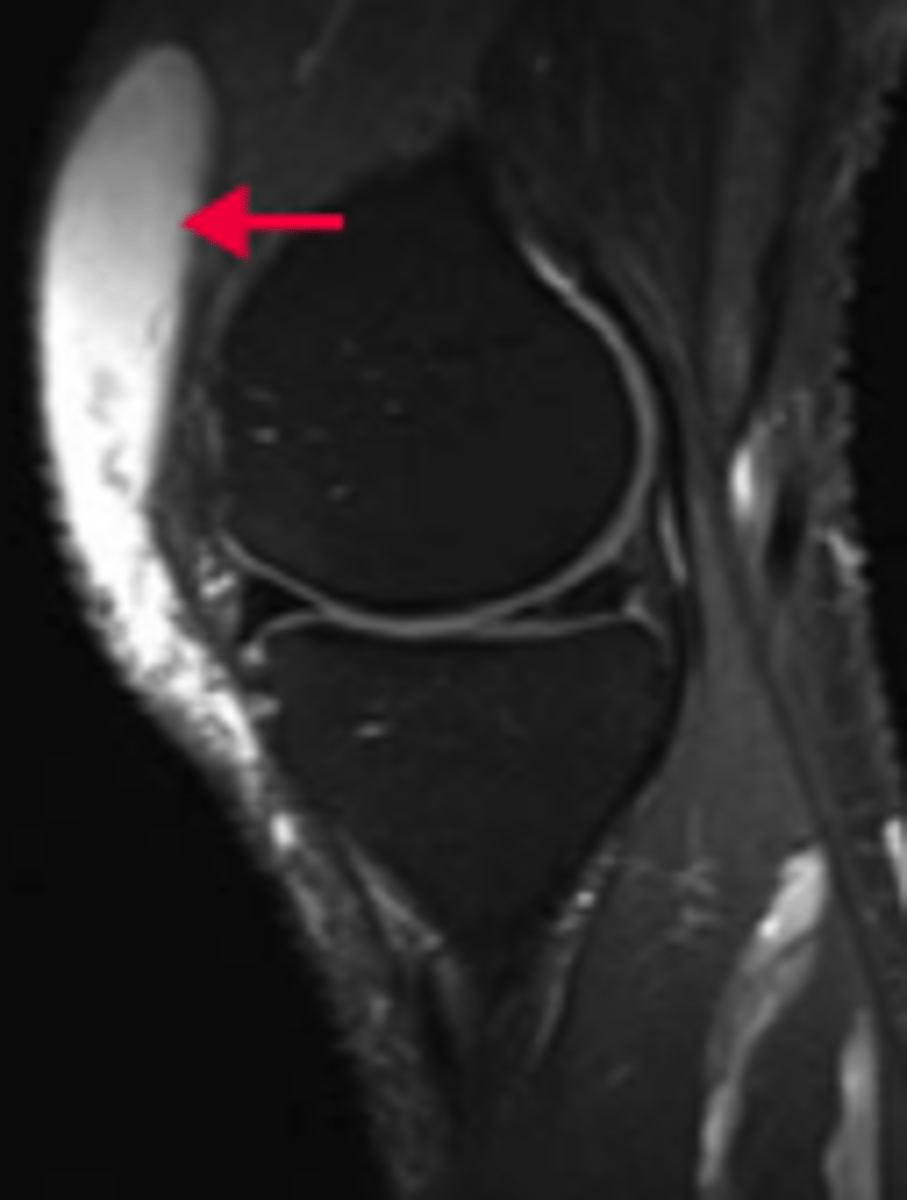
What is prepatellar bursitis?
What causes it?
What is prepatellar bursitis?
- inflammation of the knee's largest sac of synovial fluid
What causes it?
- repeated trauma or pressure from excessive kneeling
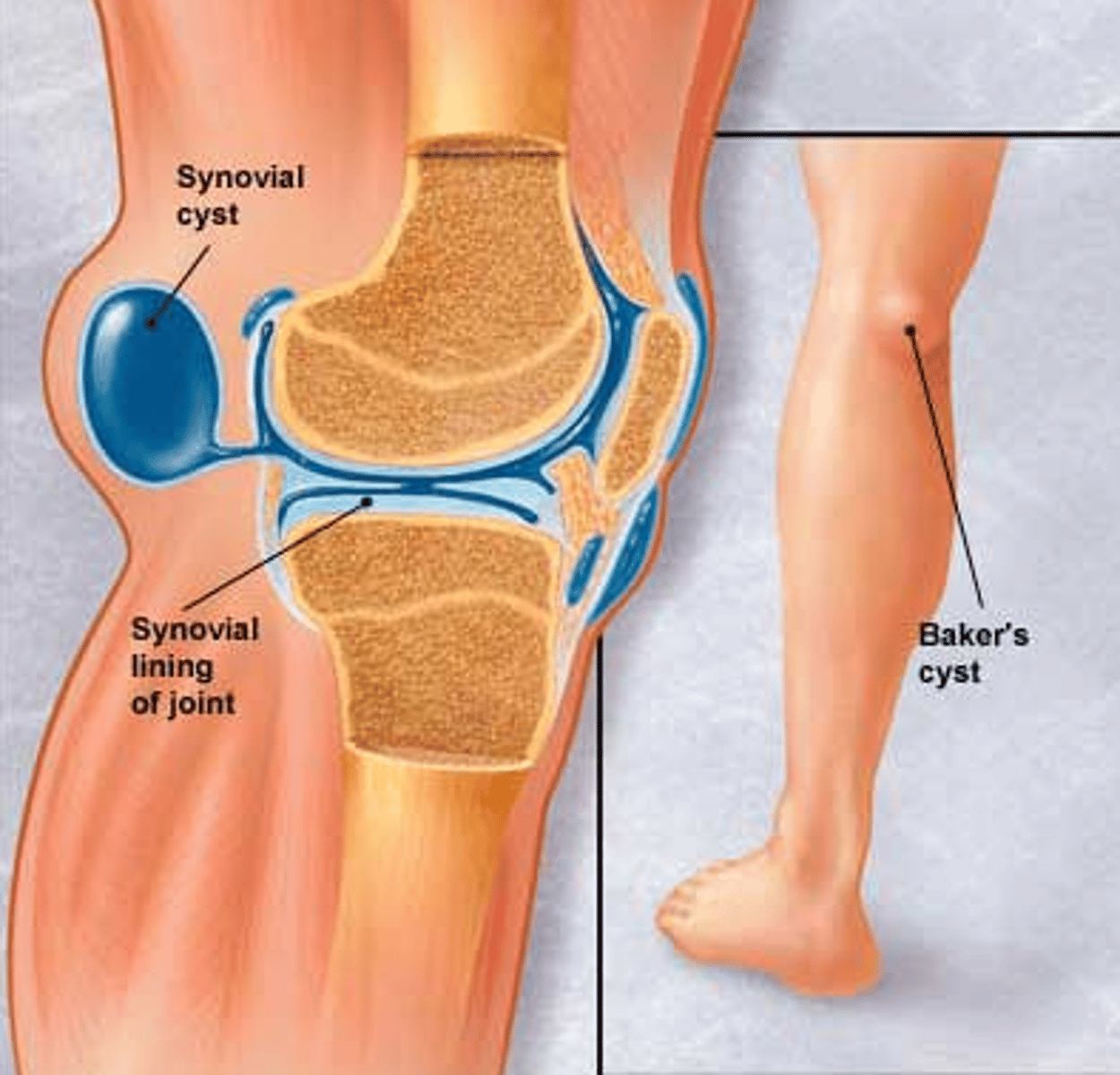
What is a Baker's cyst?
What is a Baker's cyst?
- popliteal fluid collection in the gastrocnemius-semimembranous burse
- commonly communicates with the synovial space and is related to chronic joint disease
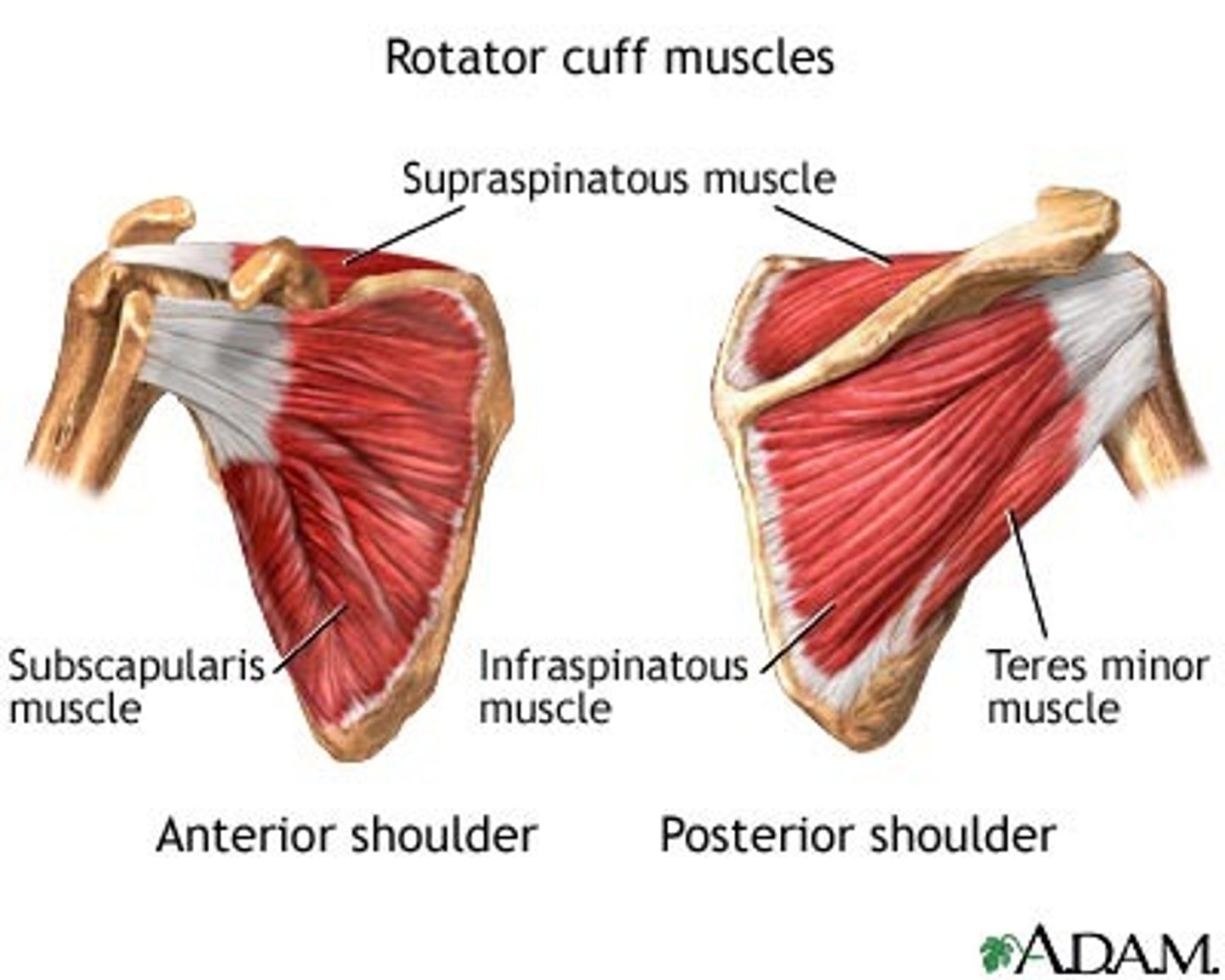
What are the muscles of the rotator cuff?
What are their actions? What are they innervated by?
What spinal nerve roots are primarily responsible for their innervation?
What are the muscles of the rotator cuff?
- SItS (AEEI)
- supraspinatus
- infraspinatus
- teres minor
- subscapularis
What are their actions? What are they innervated by?
Supraspinatus (suprascapular nerve):
- initial ABduction of the shoulder (before deltoid kicks in)
- most common rotatory cuff injury (trauma, degeneration and impingement leading to tendinopathy/tear)
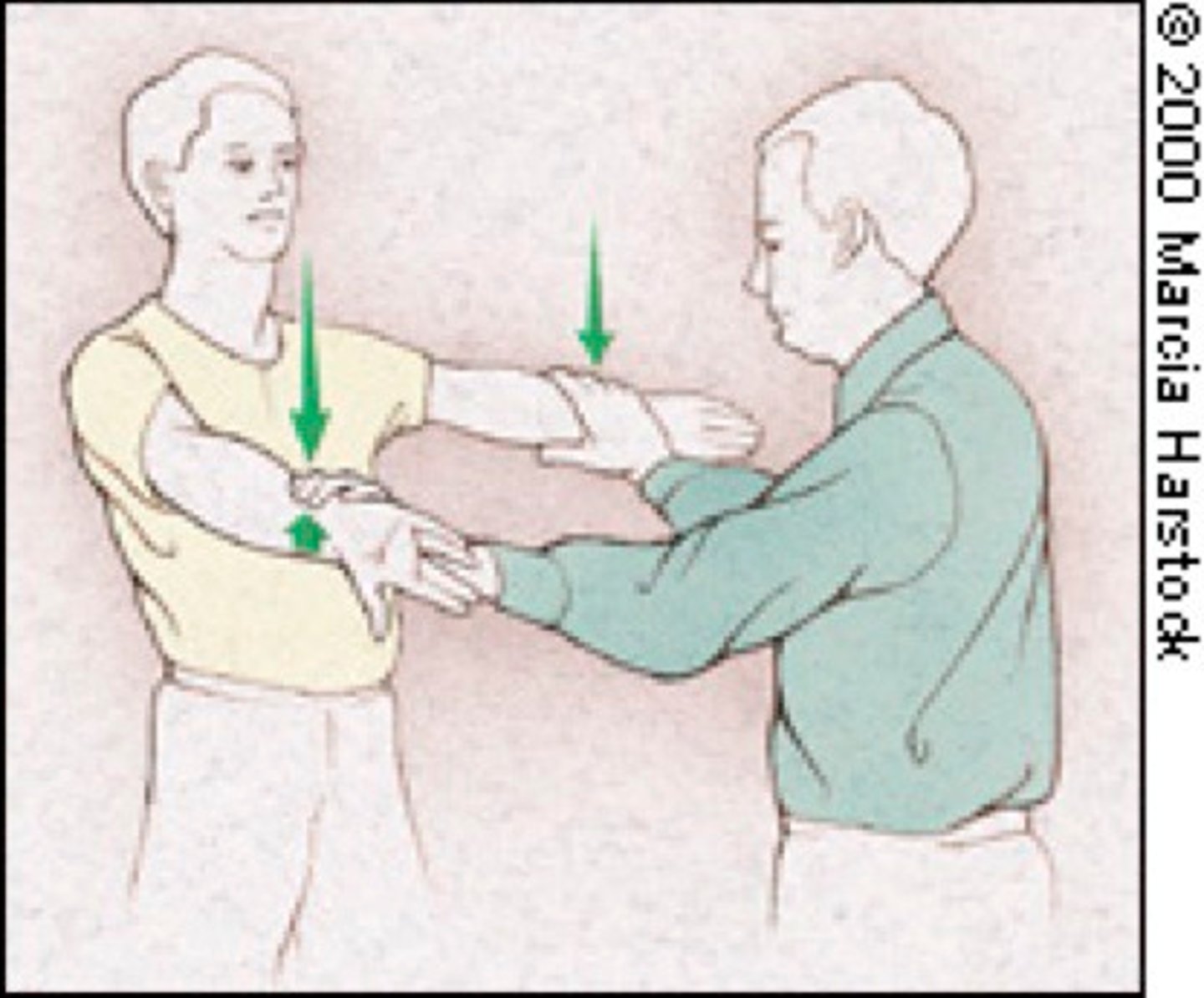
- assessed by the "empty can test"
Infraspinatus (suprascapular nerve)
- external (lateral) rotation
- pitching injury
Teres minor (axillary nerve)
- external (lateral) rotation
Subscapularis (upper and lower subscapular nerves)
- medially rotates and adducts arm
What spinal nerve roots are primarily responsible for their innervation?
- C5-C6
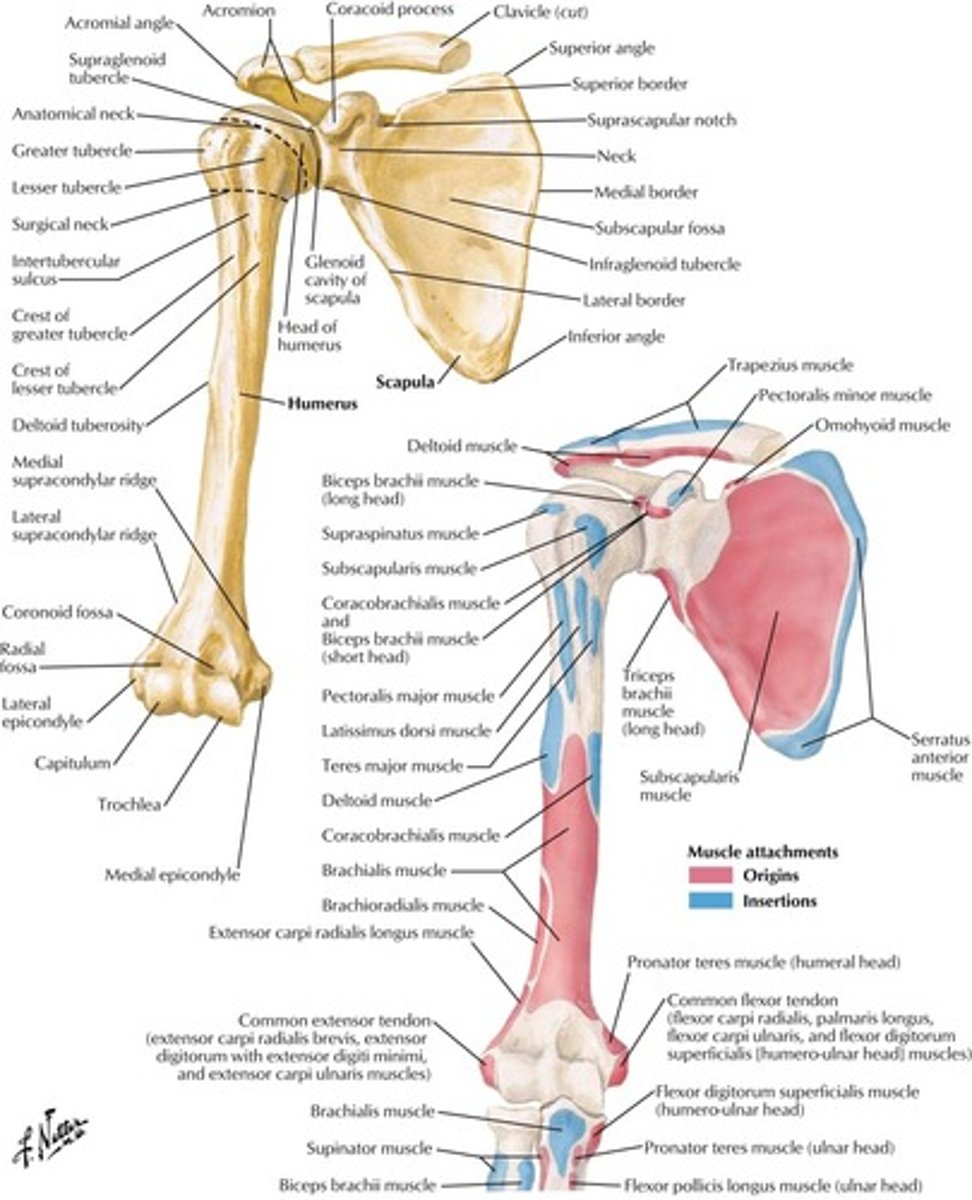
Shoulder Bone Anatomy
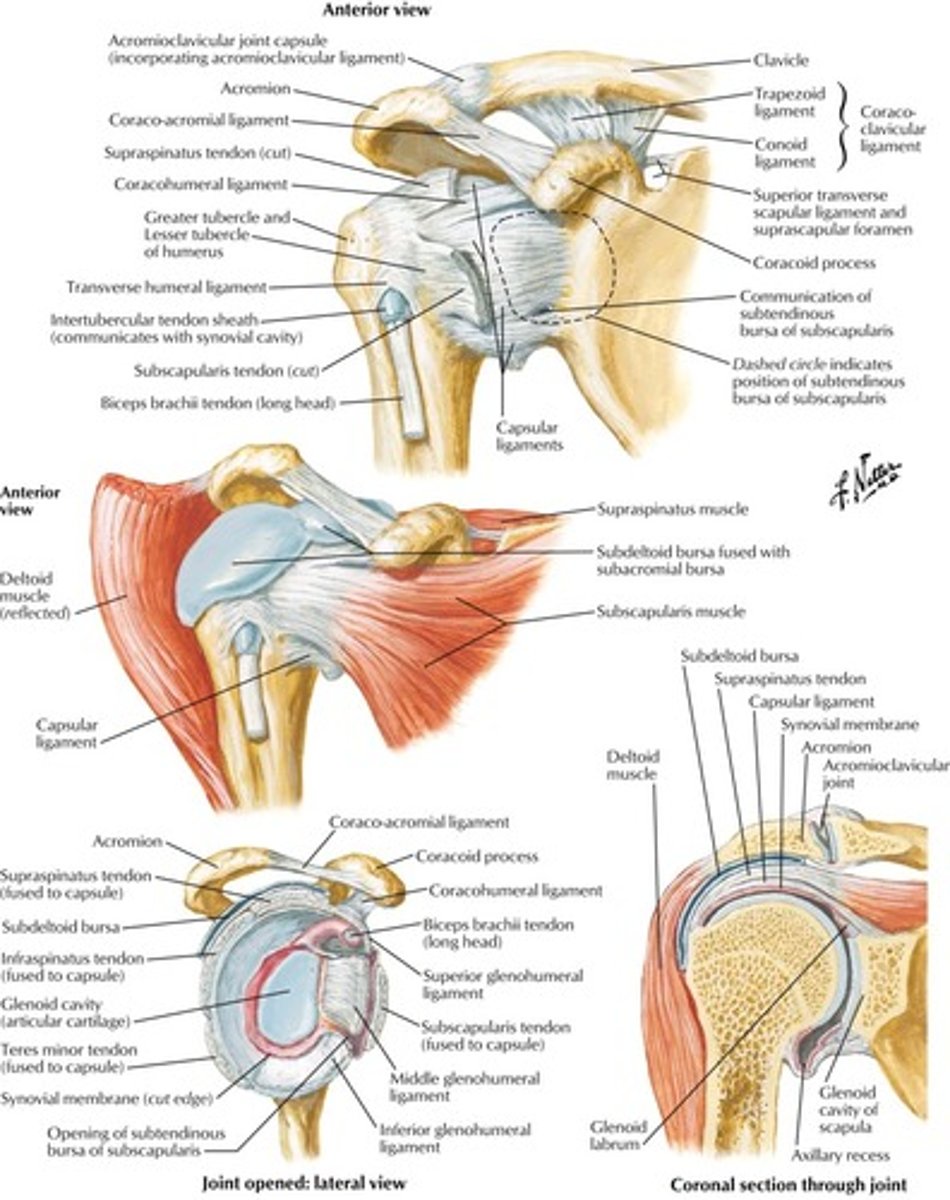
Shoulder Joint Anatomy
What is the most common rotator cuff injury?
How can you test for this injury?
Supraspinatus injury
How can you test for this injury?
- supraspinatus is isolated with the empty can test (see pic) -->
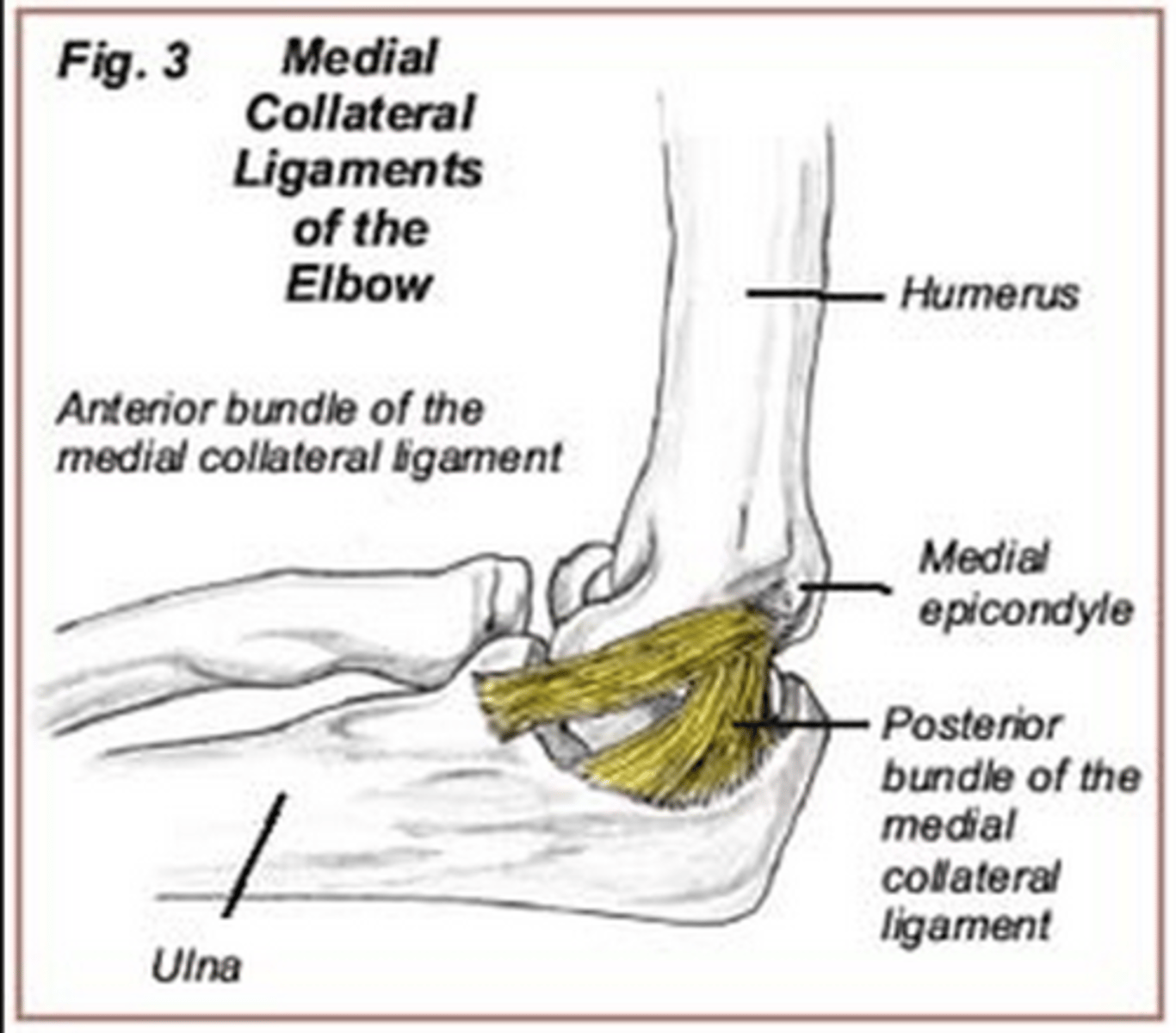
What causes golfer's elbow and where does it hurt?
- overuse injury of the elbow
- due to repetitive flexion (forehand shots) or can be idiopathic
- causes pain at the medial epicondyle
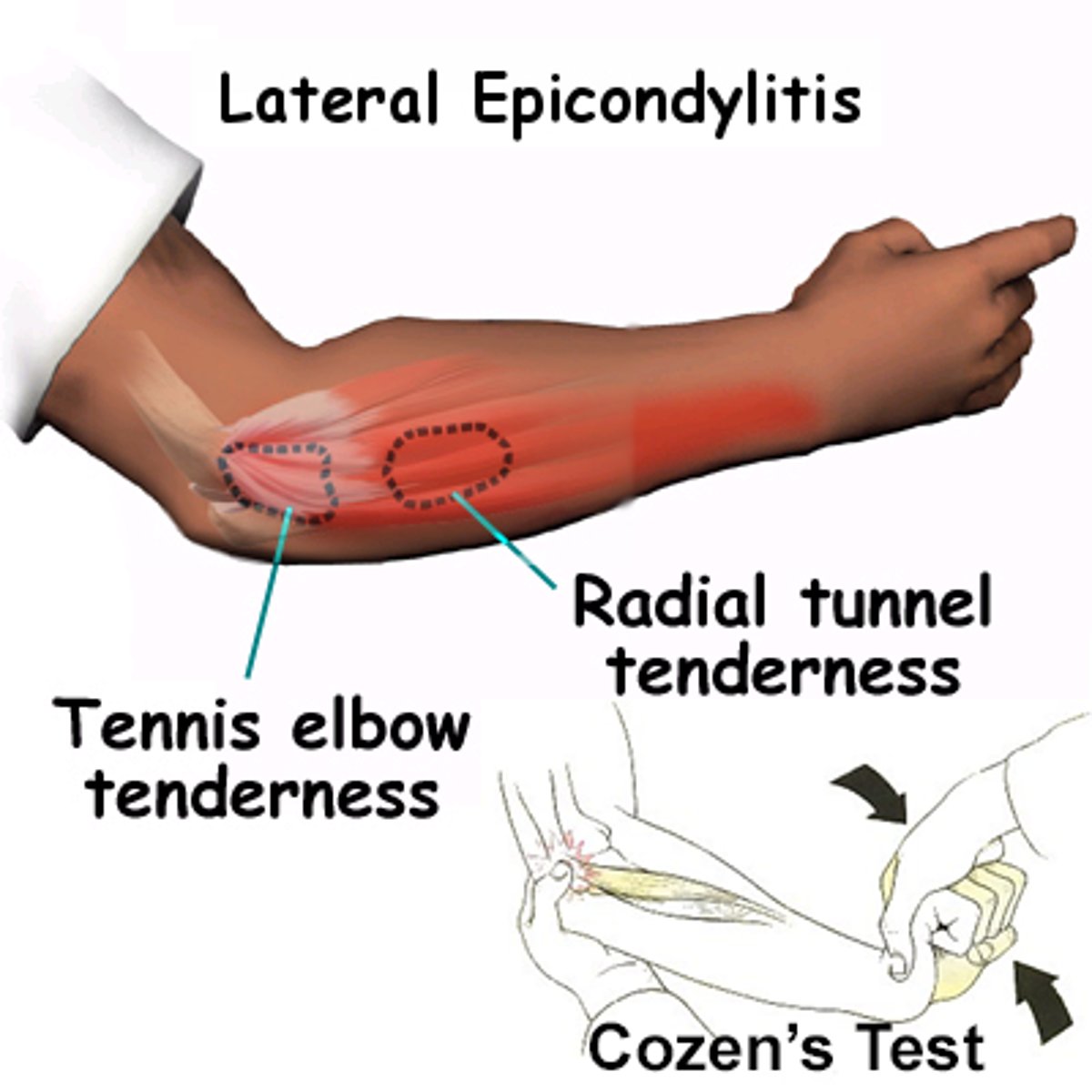
What causes tennis elbow and where does it hurt?
- overuse injury of the elbow
- due to repetitive extension (backhand) or can be idiopathic
- causes pain at the lateral epicondule
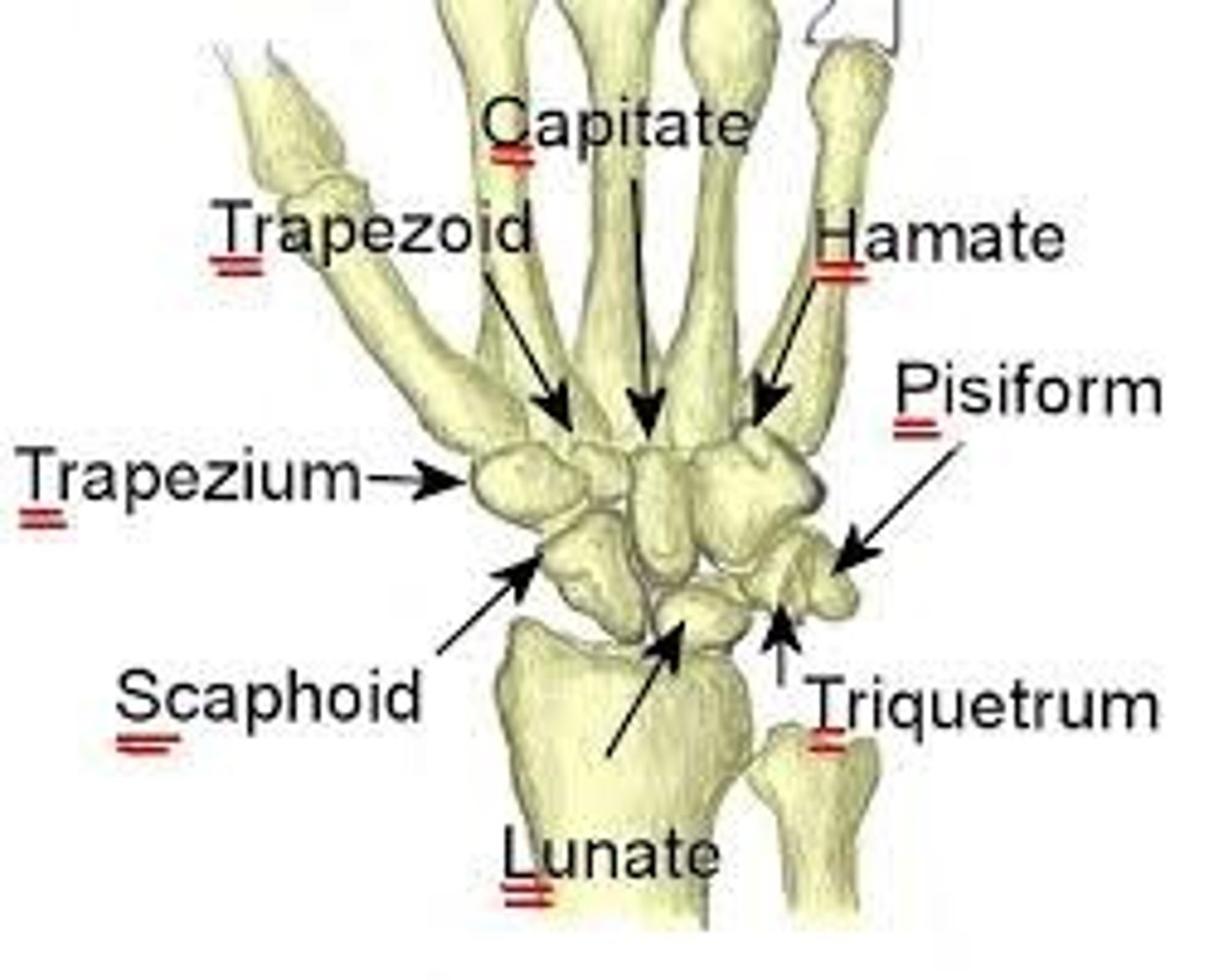
What are the bones of the wrist?
REMEMBER:
So Long To Pinky, Here Comes The Thumb
NOTE: this is looking at the PALMAR surface of the LEFT HAND. Always start at the BASE of the thumb and circle around to the PINKY basally then head back to the thumb!
Identify the wrist bones in the XRAY
A = SCAPHOID
B = LUNATE
C = TRIQUETRUM
D = PISIFORM
H = HAMATE
G = CAPITATE
F = TRAPEZOID
E = TRAPEZIUM
REMEMBER:
So Long To Pinky, Here Comes The Thumb
NOTE: this is looking at the PALMAR surface of the LEFT HAND. Always start at the BASE of the thumb and circle around to the PINKY basally then head back to the thumb!

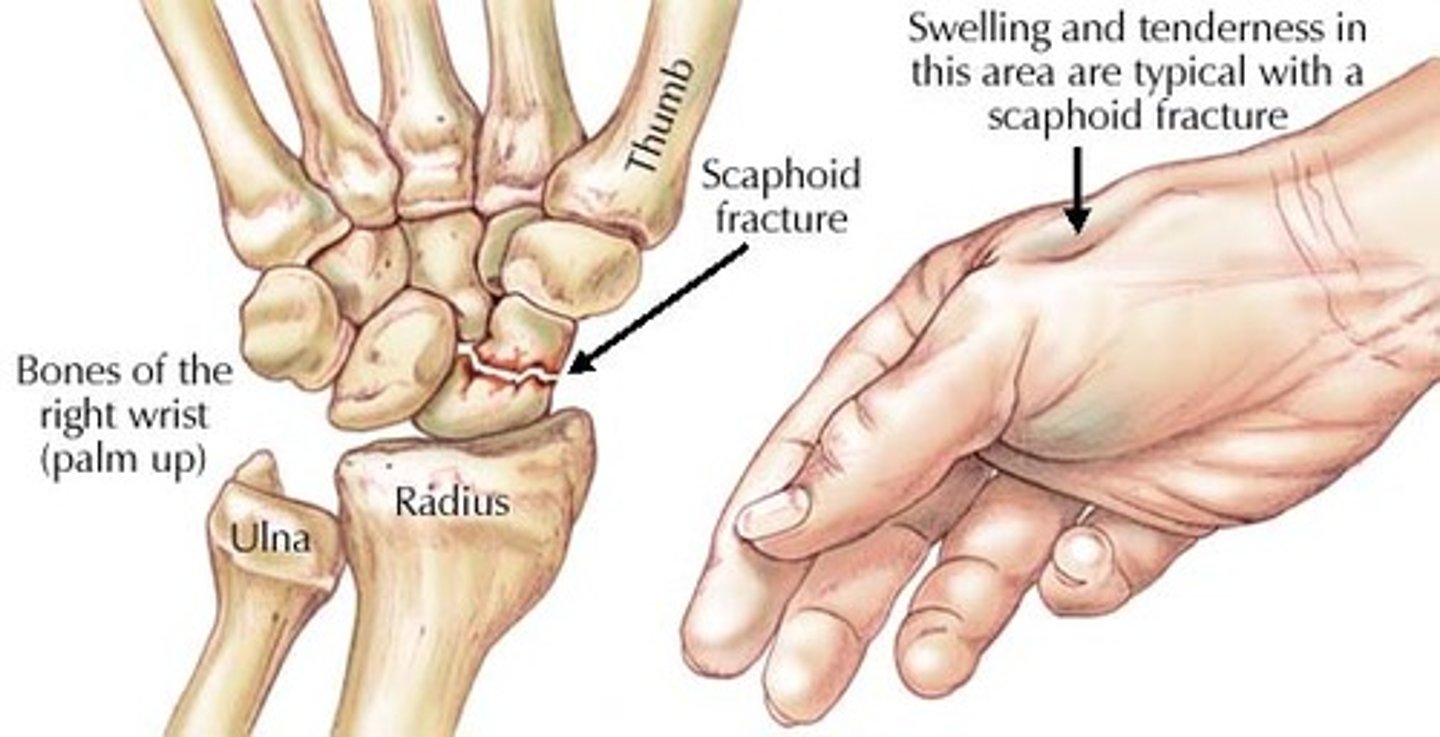
What is the most commonly fractured carpal bone?
Where can this bone be palpated (surface anatomy)?
How does it get injured?
Any other complications of injury?
What is the most commonly fractured carpal bone?
- scaphoid bone
Where can this bone be palpated (surface anatomy)?
- palpated in the anatomic snuff box
How does it get injured?
- typically from a fall on an outstretched hand
Any other complications of injury?
- prone to avascular necrosis due to a retrograde blood supply (the dorsal scaphoid branch of the radial artery supplies the majority of the scaphoid after entering near the bone's distal pole. blood supply to the proximal pole proceeds in a retrograde manner and can be easily interrupted by a fracture)
- nonunion
What demarcates the anatomic snuff box?
- the anatomic snuff box is a shallow depression at the dorsoradial wrist bound medially by the tend of the extensor pollicis longus and laterally by the tendons of the abductor pollicis longus and extensor pollicis brevis
- the scaphoid and trapezium bones form the floor of the snuffbox
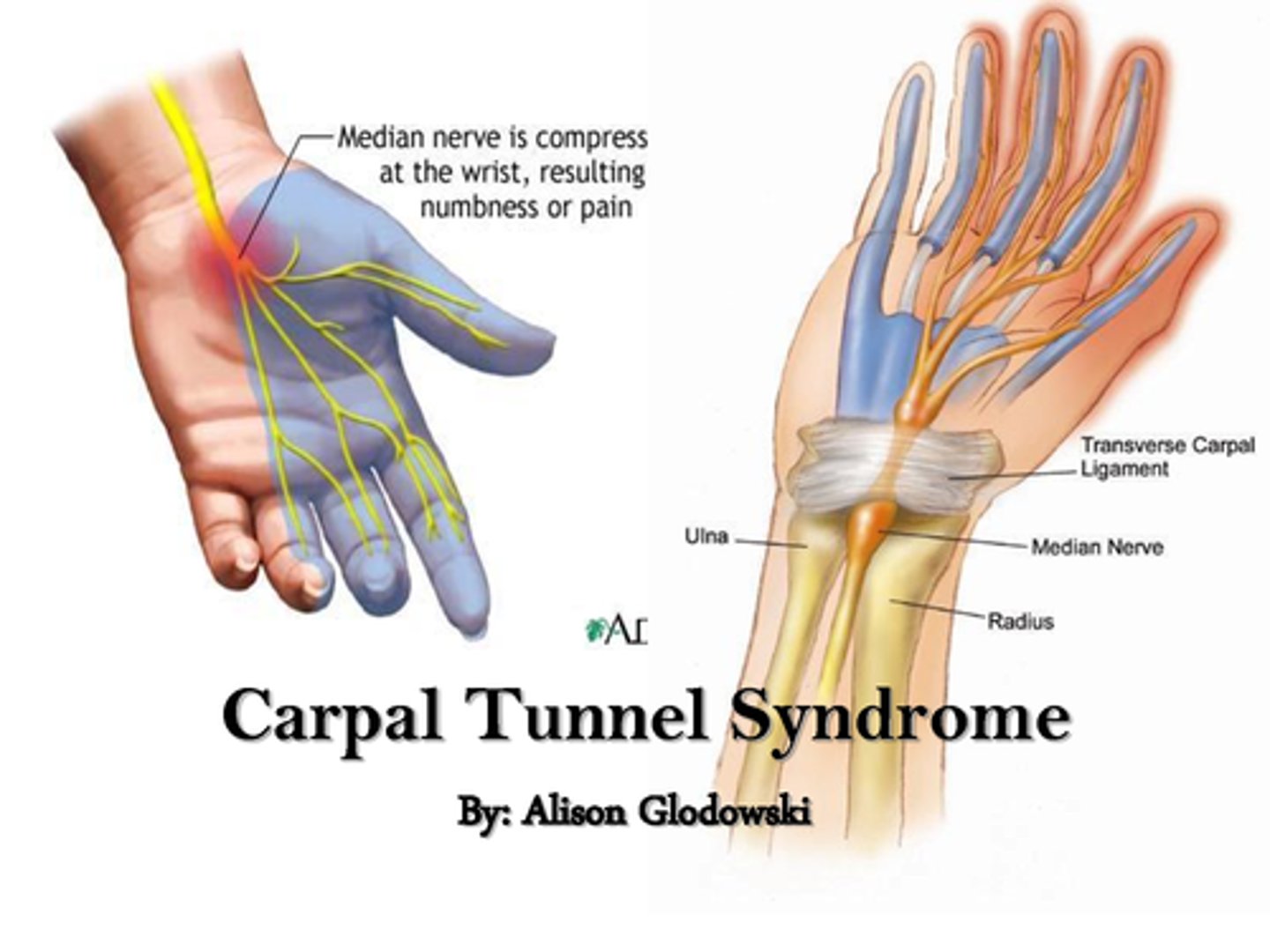
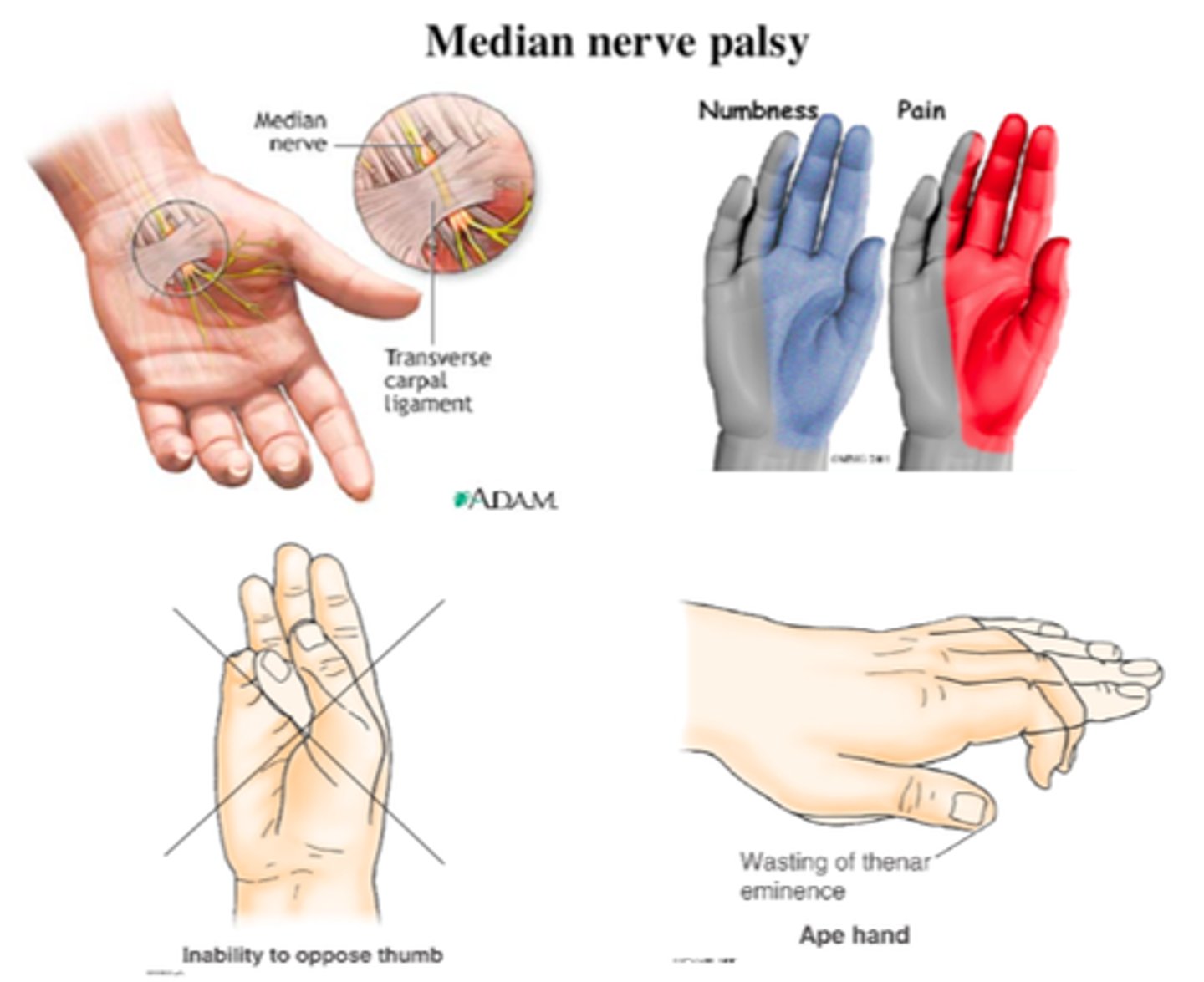
What is carpal tunnel syndrome?
Symptoms?
What diseases is it associated with?
What is carpal tunnel syndrome?
- entrapment of the median nerve in the carpal tunnel
- this leads to nerve compression
Symptoms?
- paresthesias, pain, and numbness in the distribution of the median nerve
- note that the thenar eminence atrophies but sensation is spared, because the palmar cutaneous branch enters the hand external to the carpal tunnel
What diseases is it associated with?
- pregnancy
- RA
- hypothyroidism
- diabetes
- dialysis related amyloidosis
- also, repetitive use
What is Guyon canal syndrome?
What kind of people typically get these injuries?
What is Guyon canal syndrome?
- compression of the ulnar nerve at the wrist or hand
What kind of people typically get these injuries?
- classically seen in cyclists due to pressure from the handle bars
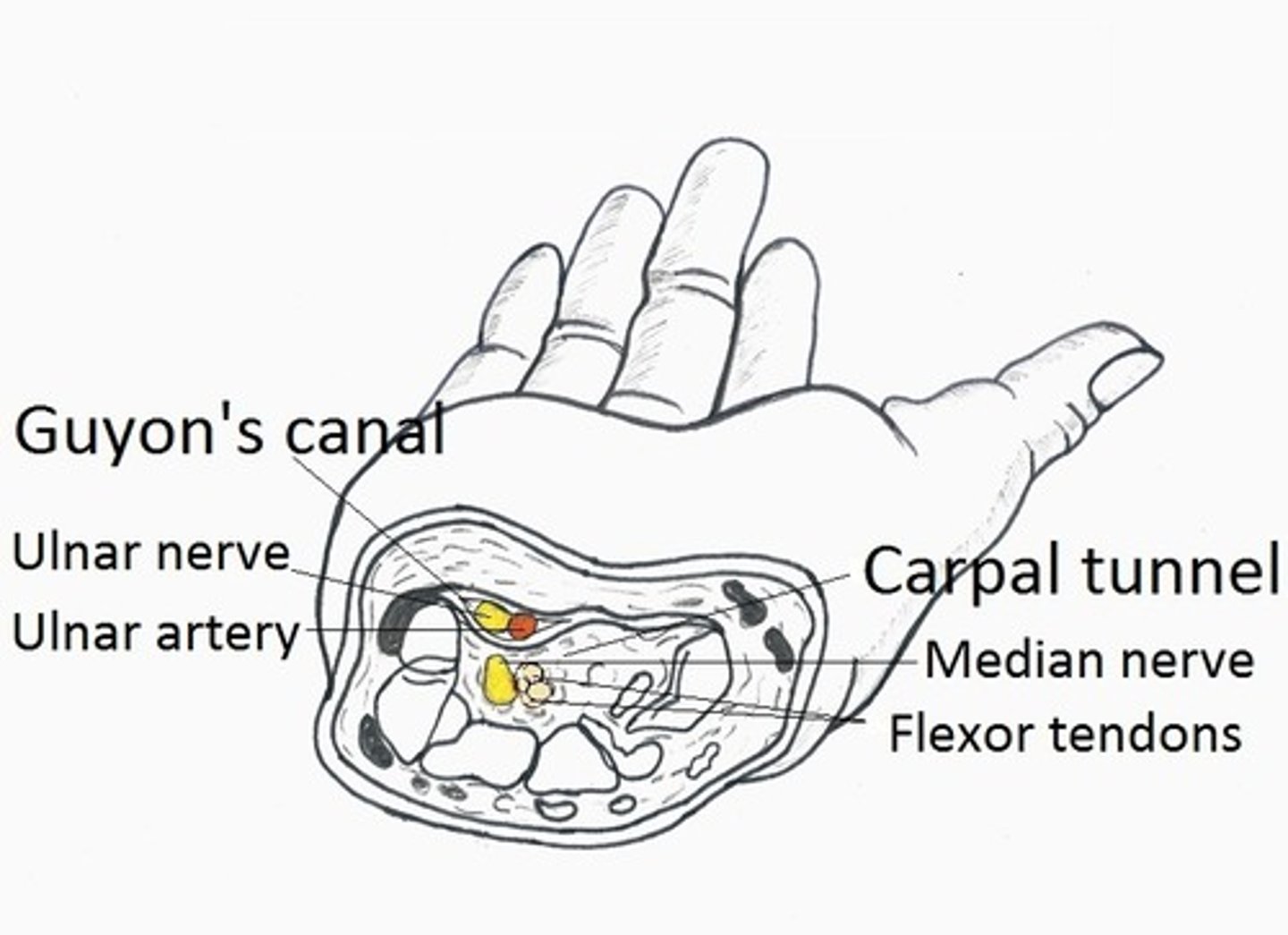
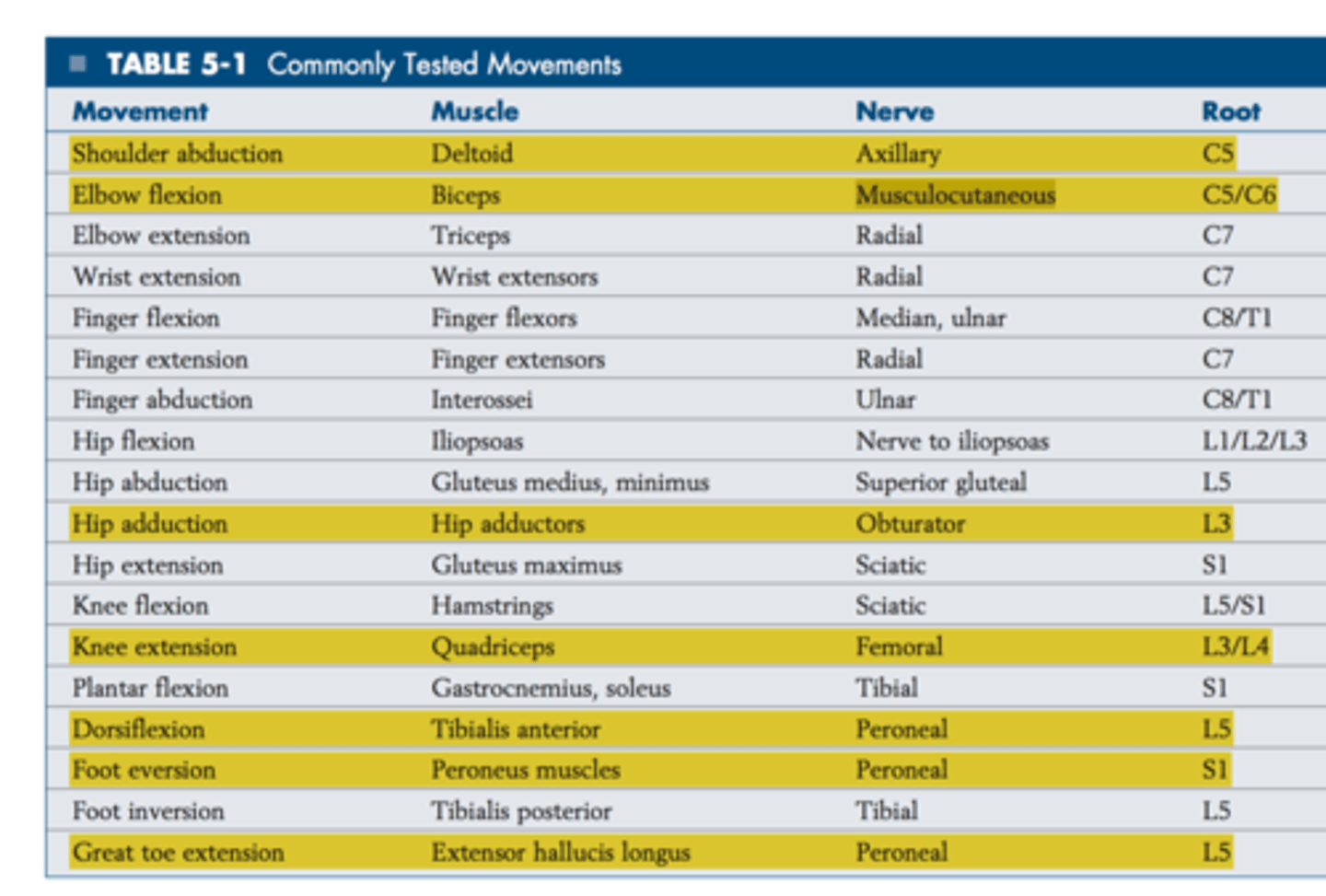
TABLE of MOVEMENTS, MUSCLES, NERVES AND ROOTS
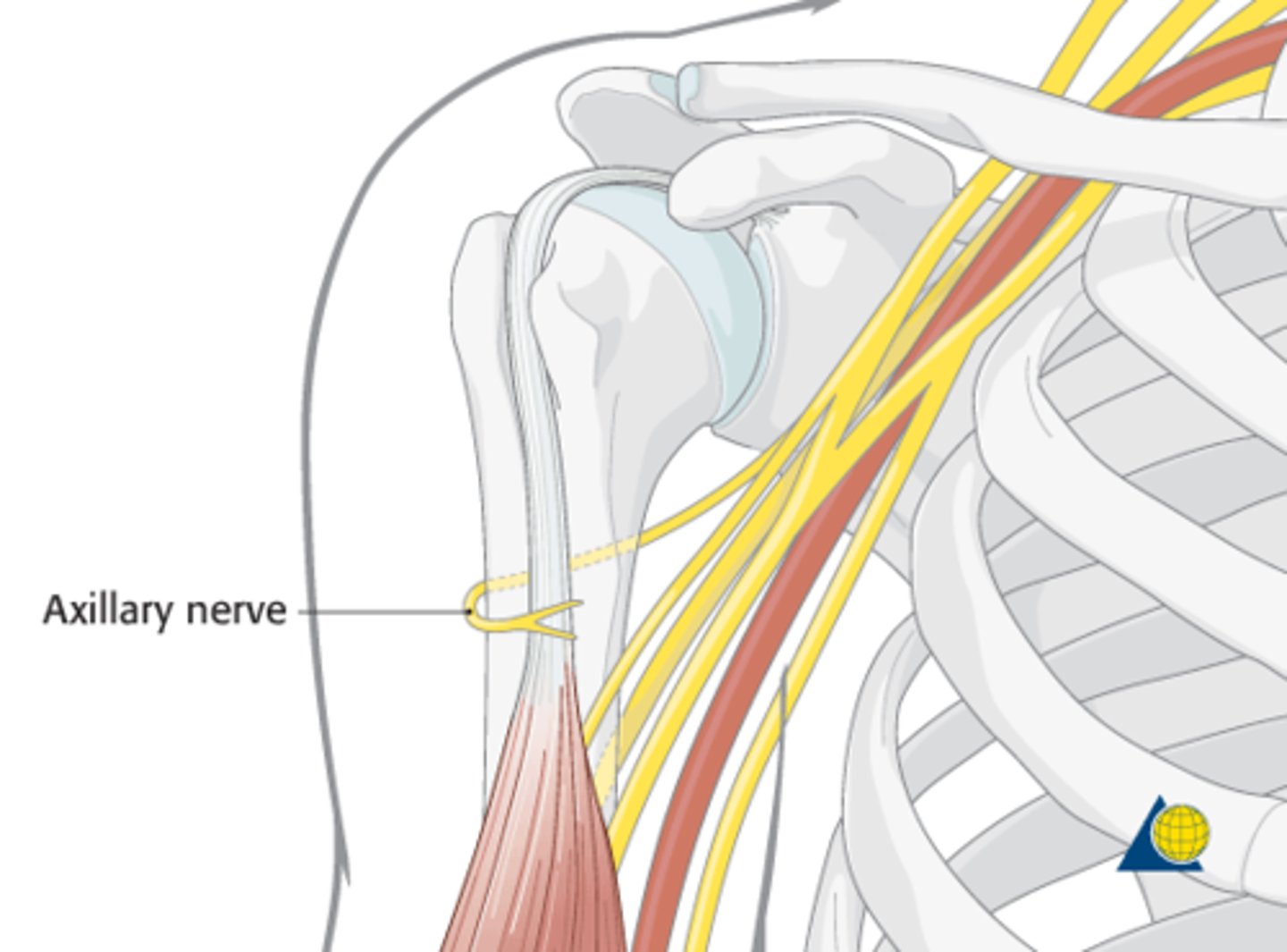
Axillary Nerve
Spinal Roots:
Cause of Injury:
Presentation:
Spinal Roots: C5 - C6
Cause of Injury:
- fractured surgical neck of the humerus
- anterior dislocation of the humerus
Presentation:
- flattened deltoid
- inability to ABduct at the shoulder (can't go > 15 degrees; first 15 by supraspinatus)
- loss of sensation over deltoid muscle and lateral arm
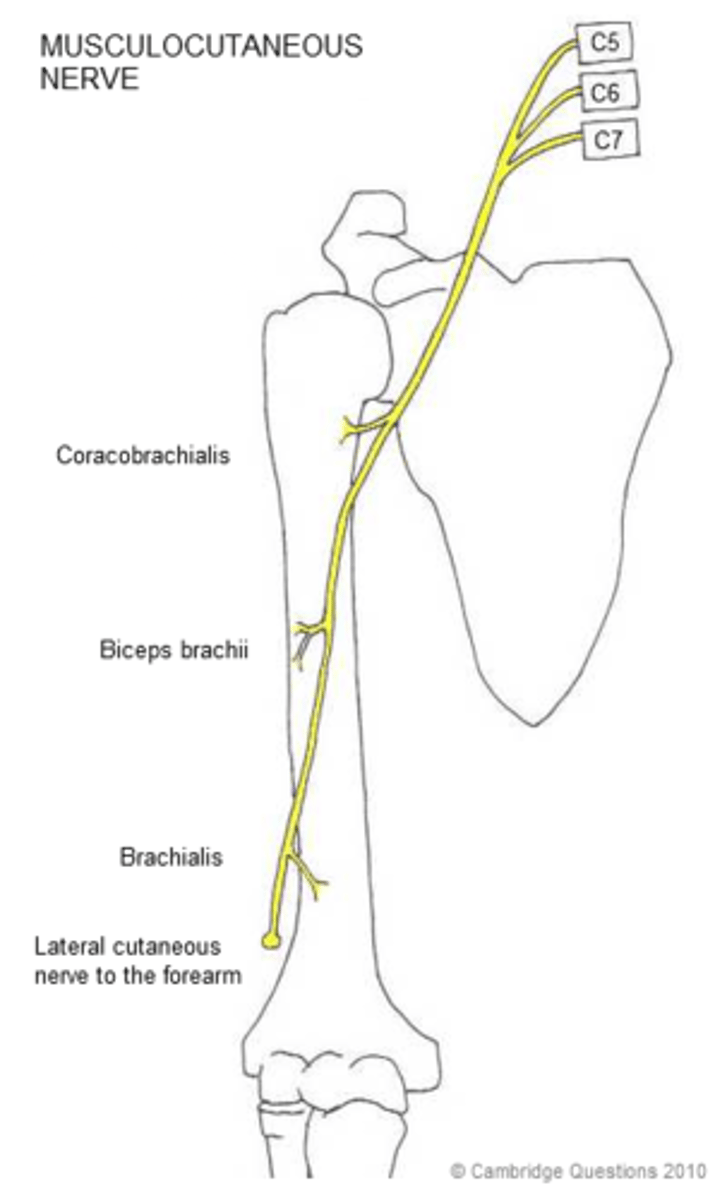
Musculocutaneous nerve
Spinal Roots:
Cause of Injury:
Presentation:
Spinal Roots: C5-C7
Cause of Injury:
- upper trunk compression
Presentation:
- loss of forearm flexion and supination (biceps)
- loss of sensation over lateral forearm
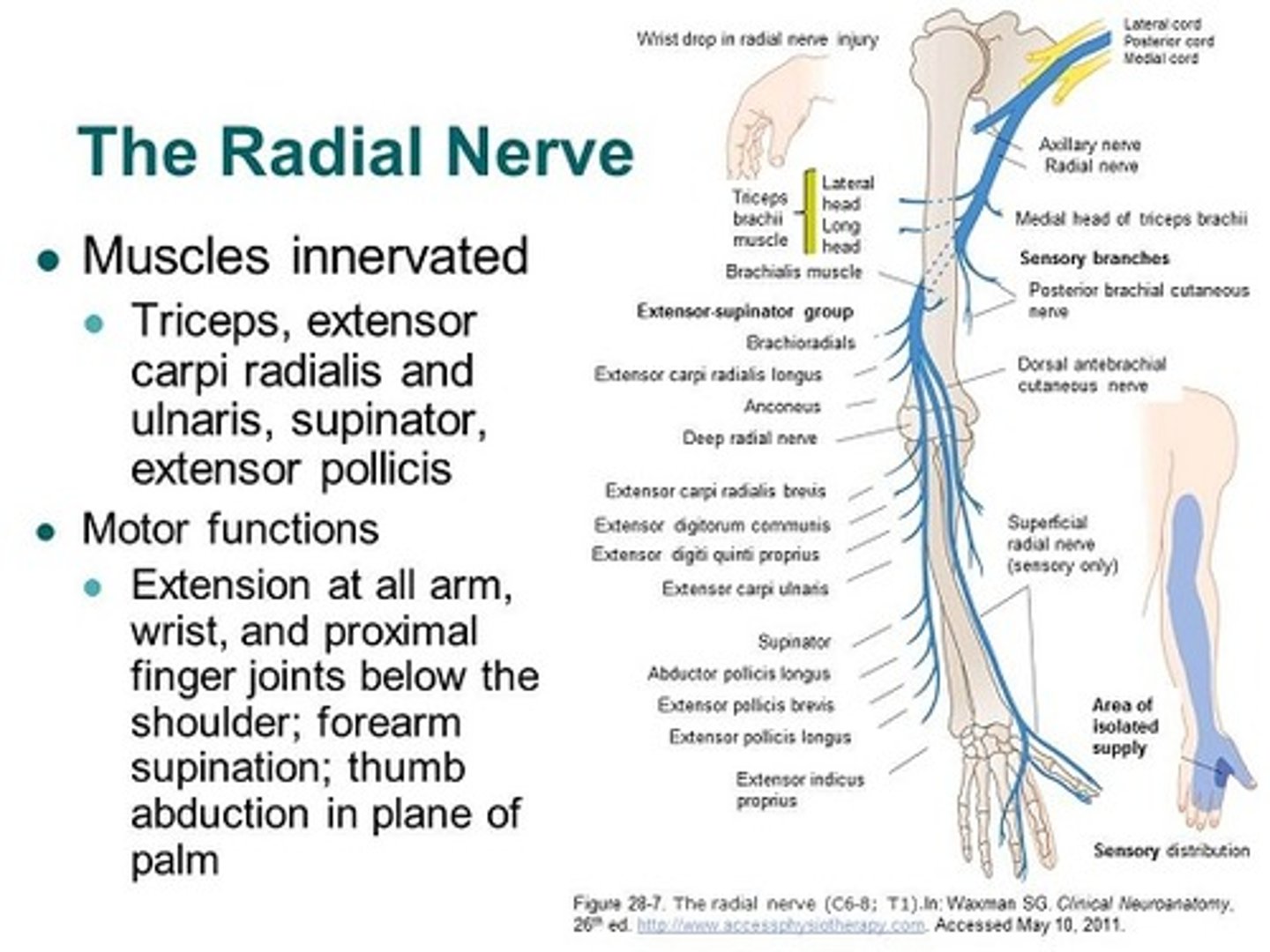
Radial Nerve
Spinal Roots:
Cause of Injury:
Presentation:
Spinal Roots: C5-T1
Cause of Injury:
- midshaft fracture of the humerus
- compression of the axilla (ie: crutches, sleeping with arm over chair "saturday night palsy")
Presentation:
- WRIST DROP: loss of elbow, wrist and finger extension (because radial does ALL the extensors)
- decreased grip strength (wrist extension necessary for maximal action of flexors)
- loss of sensation over posterior arm/forearm and dorsal hand
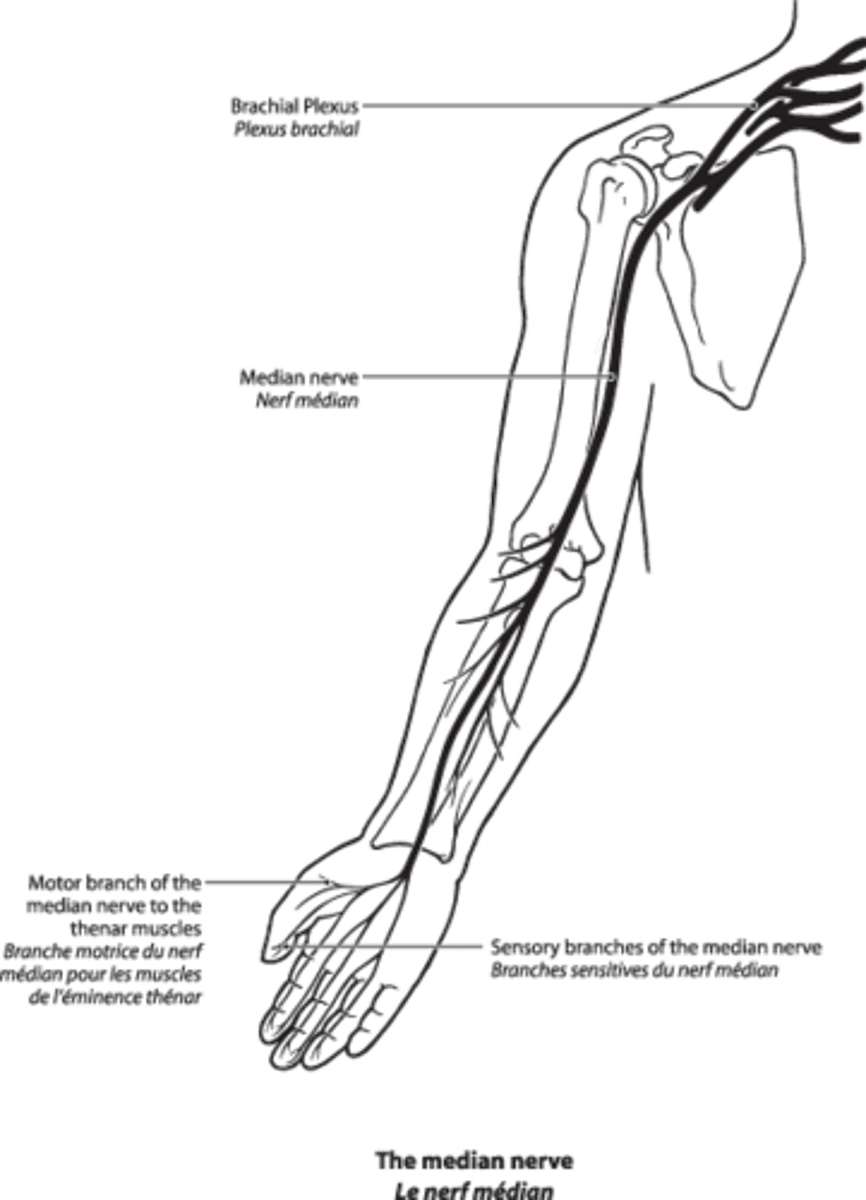
Median Nerve
Spinal Roots:
Cause of Injury:
Presentation:
Spinal Roots: C5-T1
Cause of Injury:
- proximal lesion = supracondylar fracture of the humerus - distal lesion = carpal tunnel syndrome and wrist laceration
Presentation:
- APE hand and Popes Blessing
- loss of wrist flexion, flexion of lateral fingers, thumb opposition, lumbricals of 2nd and 3rd digits
- loss of sensation over thernar eminence and dorsal and palmar aspects of lateral 3.5 fingers with proximal lesion
- Tinnel sign (tinling on percussion) and Phalen sign (compression) in carpal tunnel syndrome
Median Nerve injury
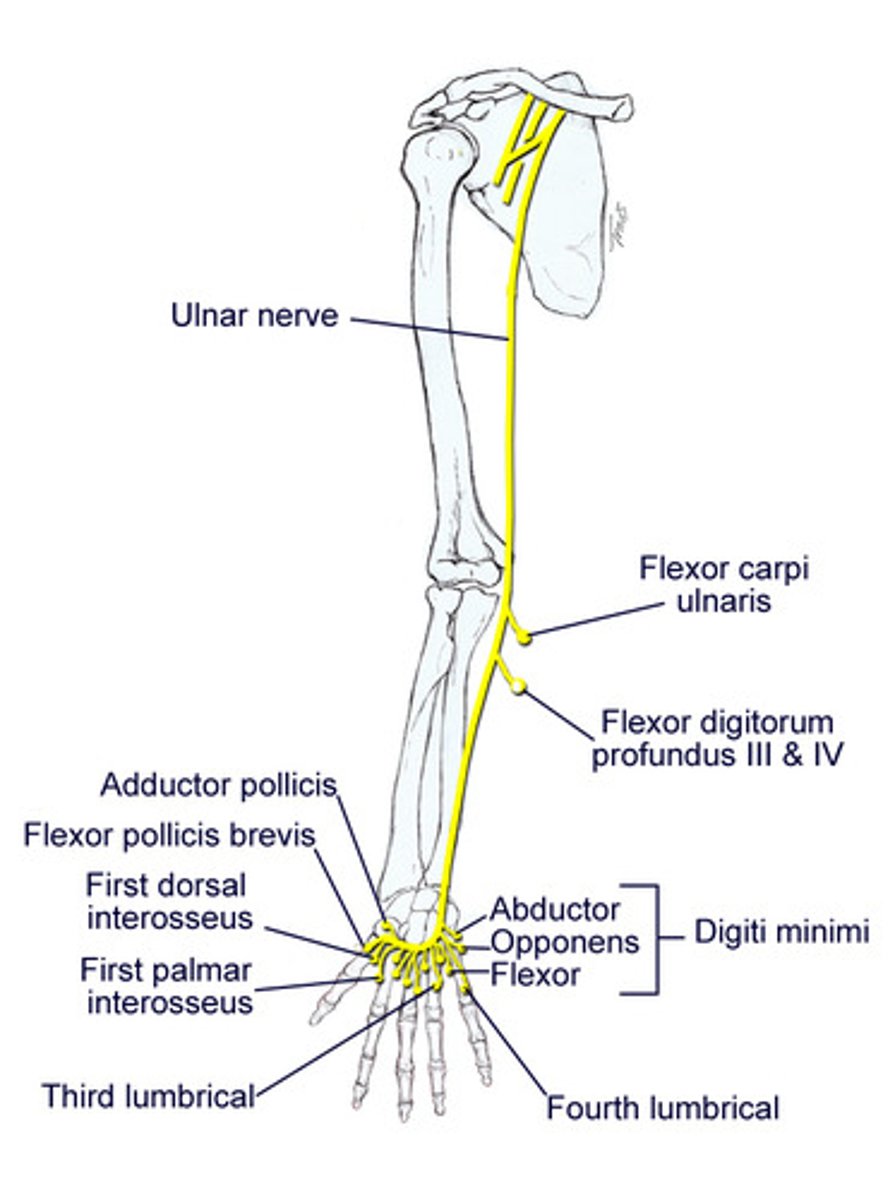
Ulnar Nerve
Spinal Roots:
Cause of Injury:
Presentation:
Spinal Roots: C8-T1
Cause of Injury:
- proximal lesion = fracture of medial epicondyle of humerus (funny bone)
- distal lesion = fractured hook of hamate
Presentation:
- ulnar CLAW on digit extension (finger flexors and abductors)
- radial deviation upon flexion (proximal lesion)
- loss of wrist flexion, flexion of medial fingers, abduction and adduction of fingers (interossei) , actions of medial 2 lumbrical muscles
- loss of sensation over medial 1.4 fingers including HYPOTHENAR eminence
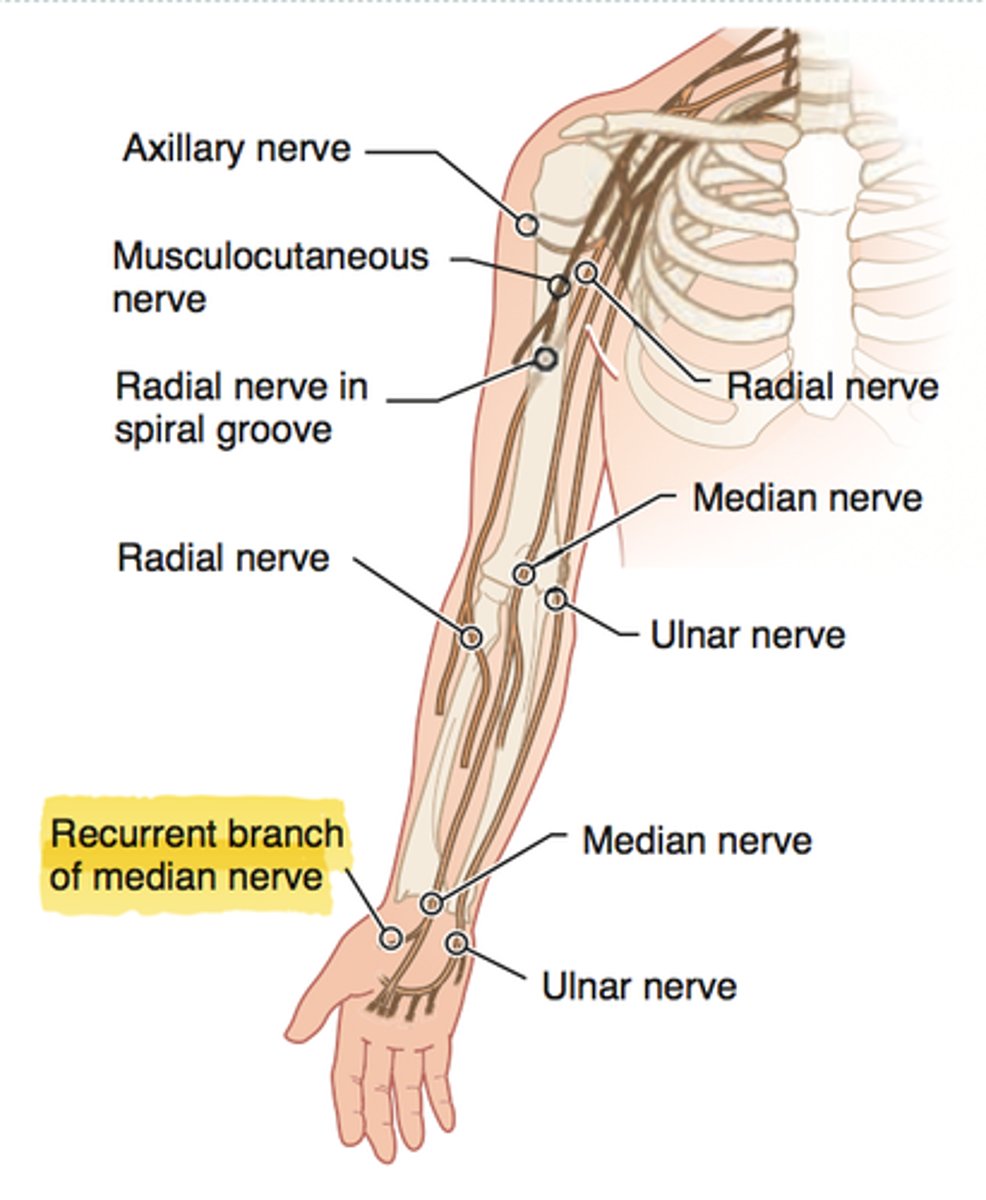
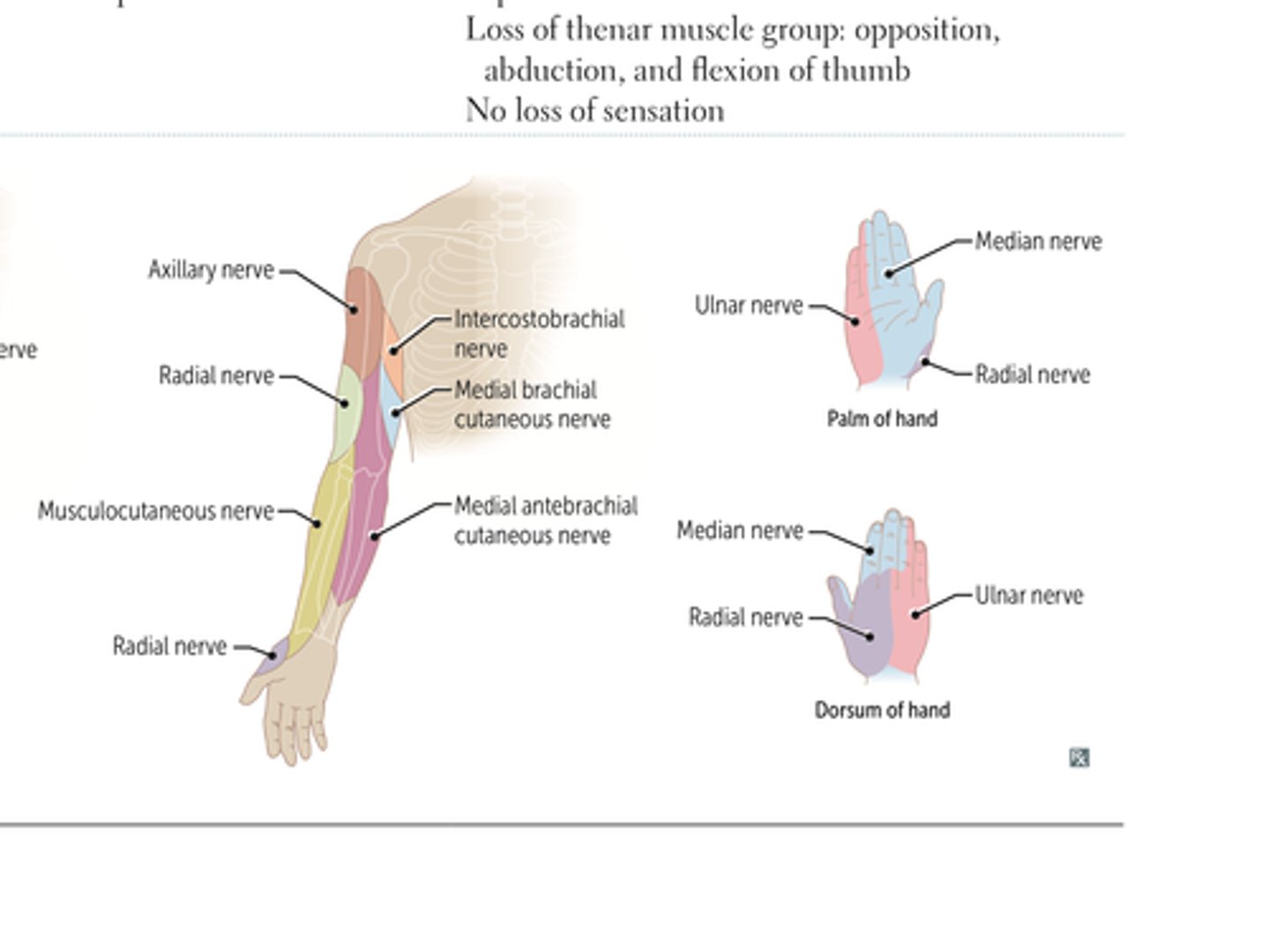
Recurrent Branch of median nerve
Spinal Roots:
Cause of Injury:
Presentation:
Spinal Roots: C5-T1
Cause of Injury:
- superficial laceration of the palm
Presentation:
- "Ape Hand"
- loss of thenar muscle group; opposition, abduction, and flexion of the thumb
- no loss of sensation
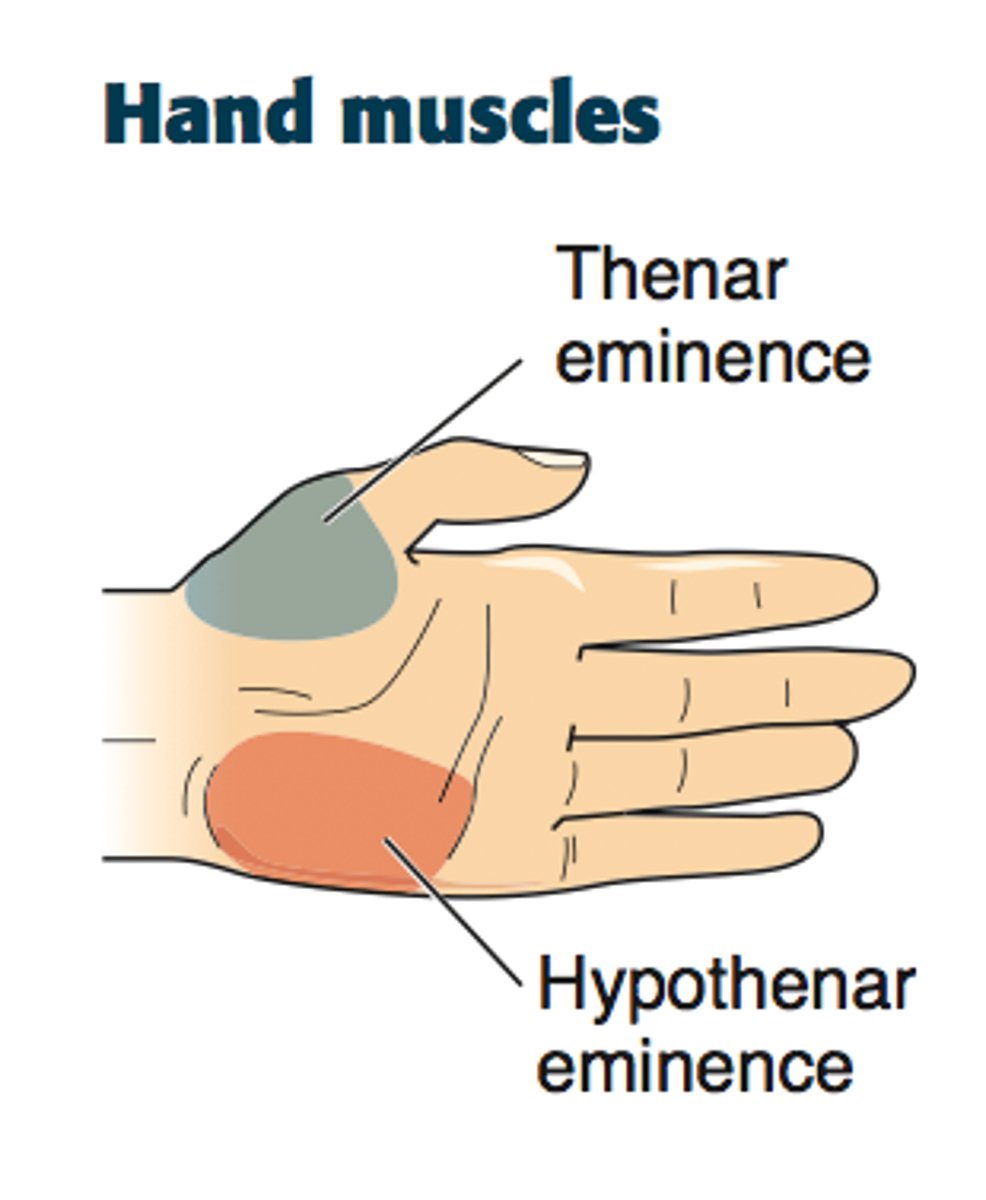
HYPOTHENAR eminence
UPPER EXTREMITY NERVES AND DERMATOMES
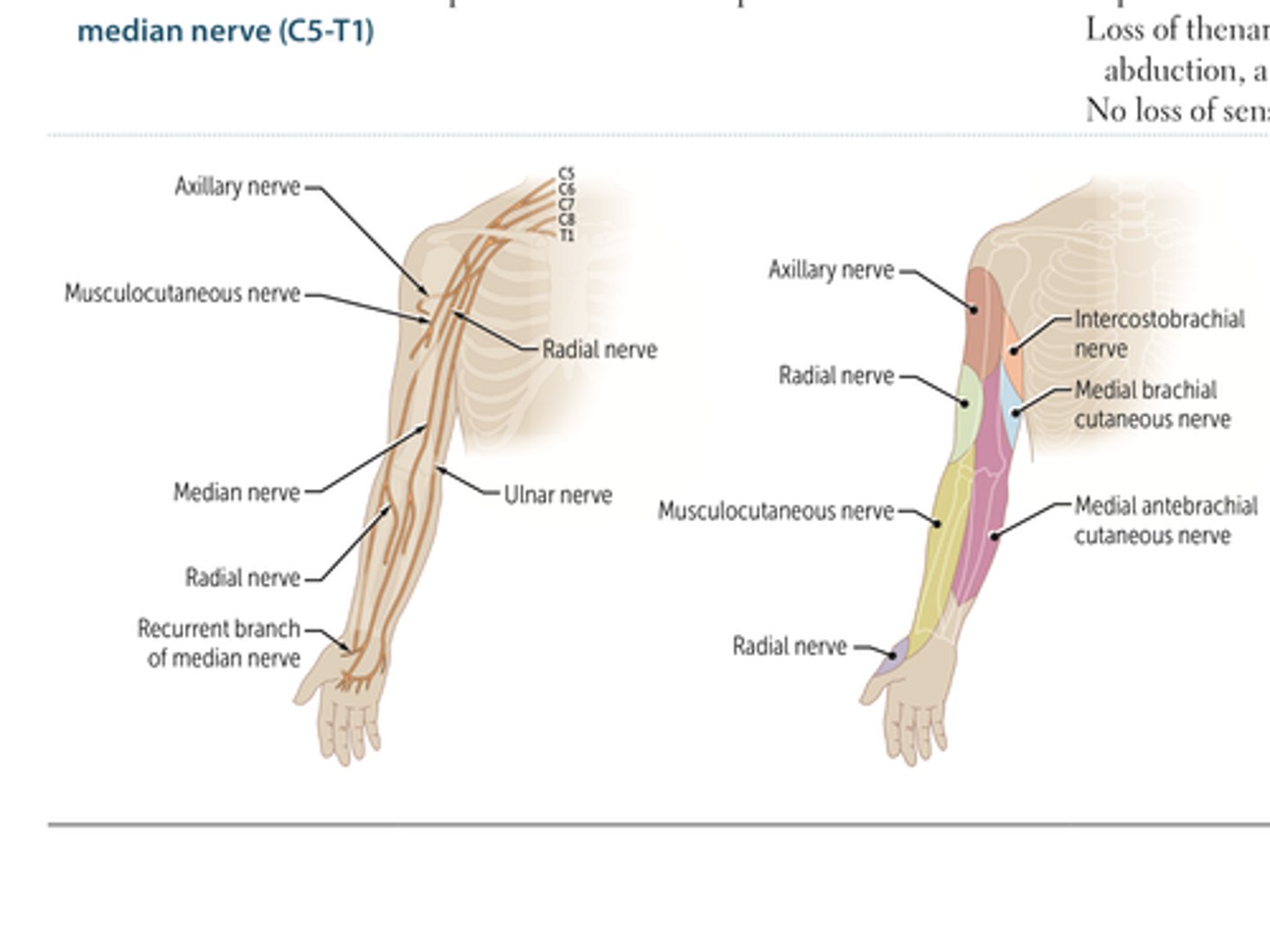
UPPER EXTREMITY DERMATOMES
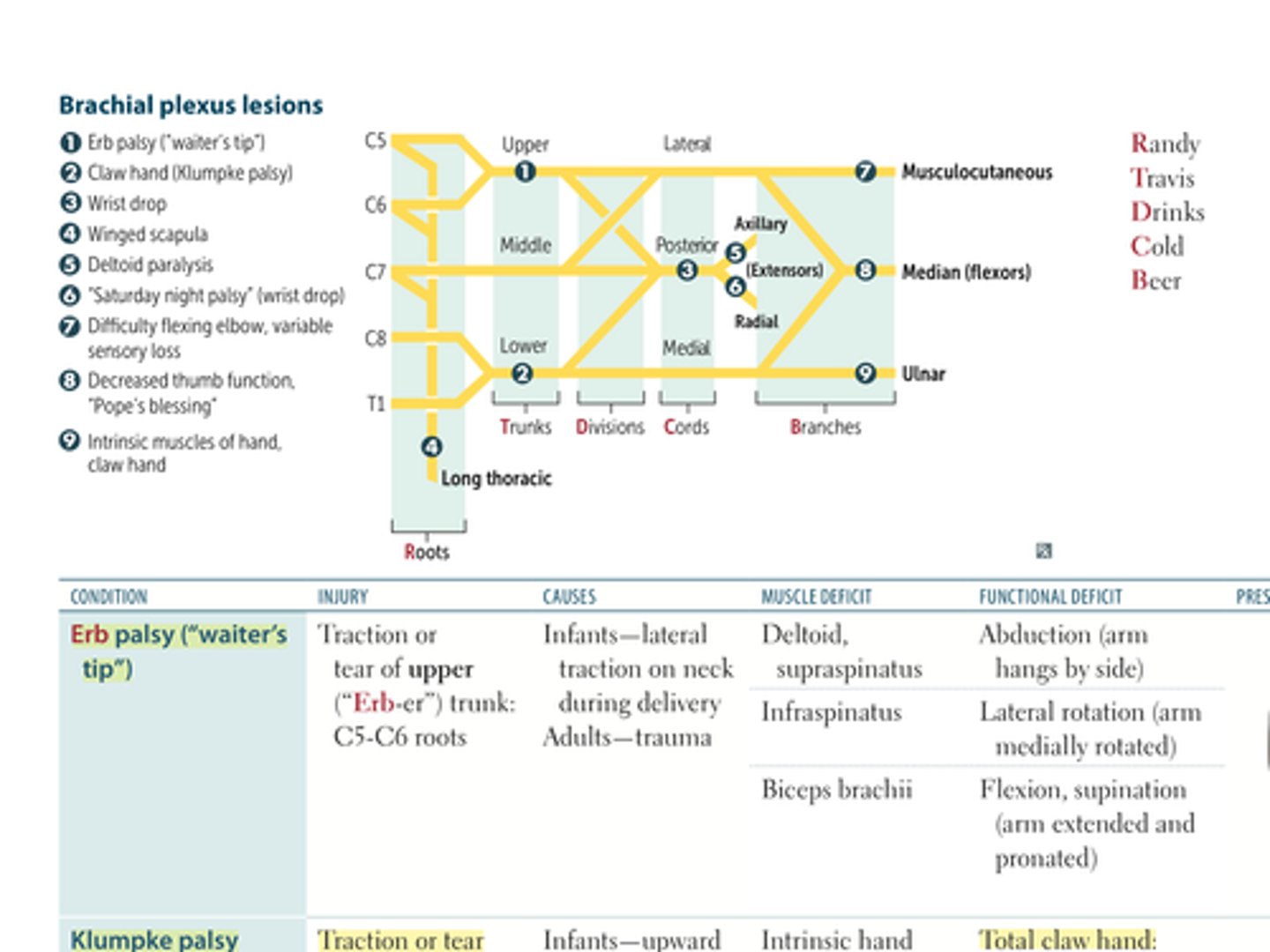
BRACHIAL PLEXUS AND INJURIES
BRACHIAL PLEXUS INJURY TABLE
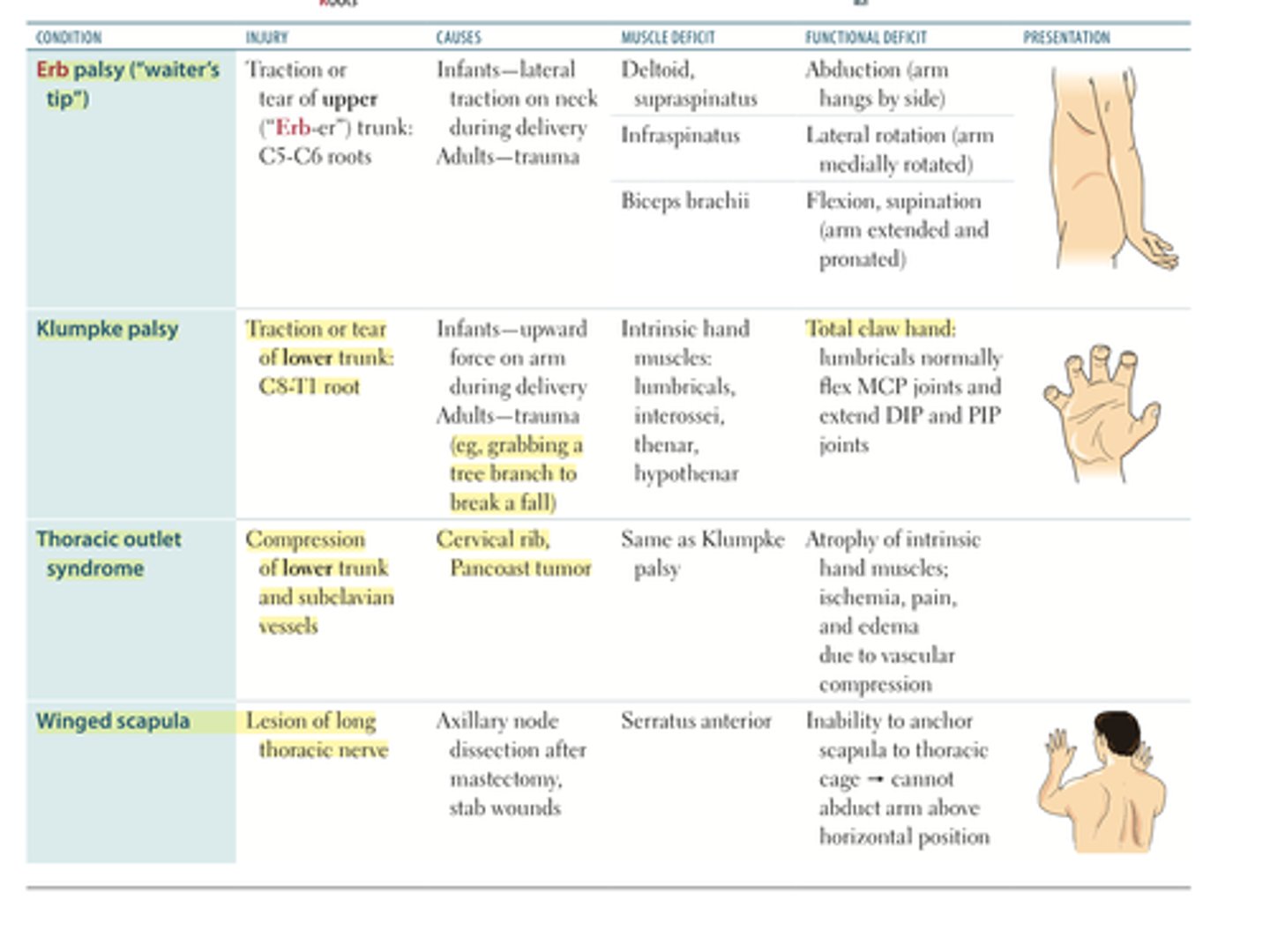
Erb Palsy
Injury:
Causes:
Muscle Deficit:
Functional Deficit:
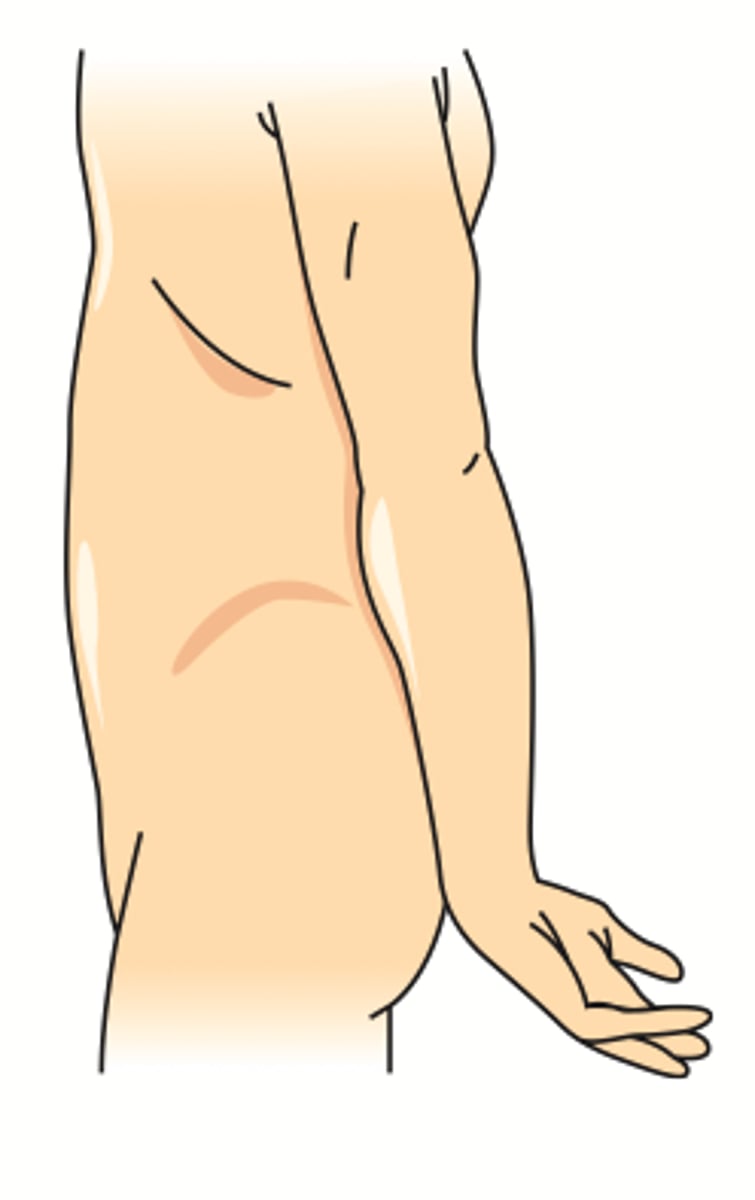
Presentation:
Aka WAITER'S TIP
Injury: upper trunk, roots C5-C6
Causes:
infants - lateral traction on neck during delivery
adults - trauma
Muscle Deficit/Functional Deficit:
1. deltoid, supraspinatus --> abduction (arm hangs at side)
2. infraspinatus --> lateral rotation (arm medially rotated)
3. biceps brachii --> flexion, supination (arm extended and pronated)
Presentation:
see picture
Klumpke palsy
Injury:
Causes:
Muscle Deficit/Functional Deficit:
Presentation:
Injury: traction or tear of lower trunk: C8-T1
Causes:
infants - upward force on arm during delivery
adults - trauma (ie: grabbing a tree branch to break a fall)
Muscle Deficit/Functional Deficit:
1. intrinsic hand muscles (lumbricals, interossei, thenar, hypothenar) --> total claw hand (lumbricals normally flex the MCP joints and extend DIP and PIP joints)
Presentation:
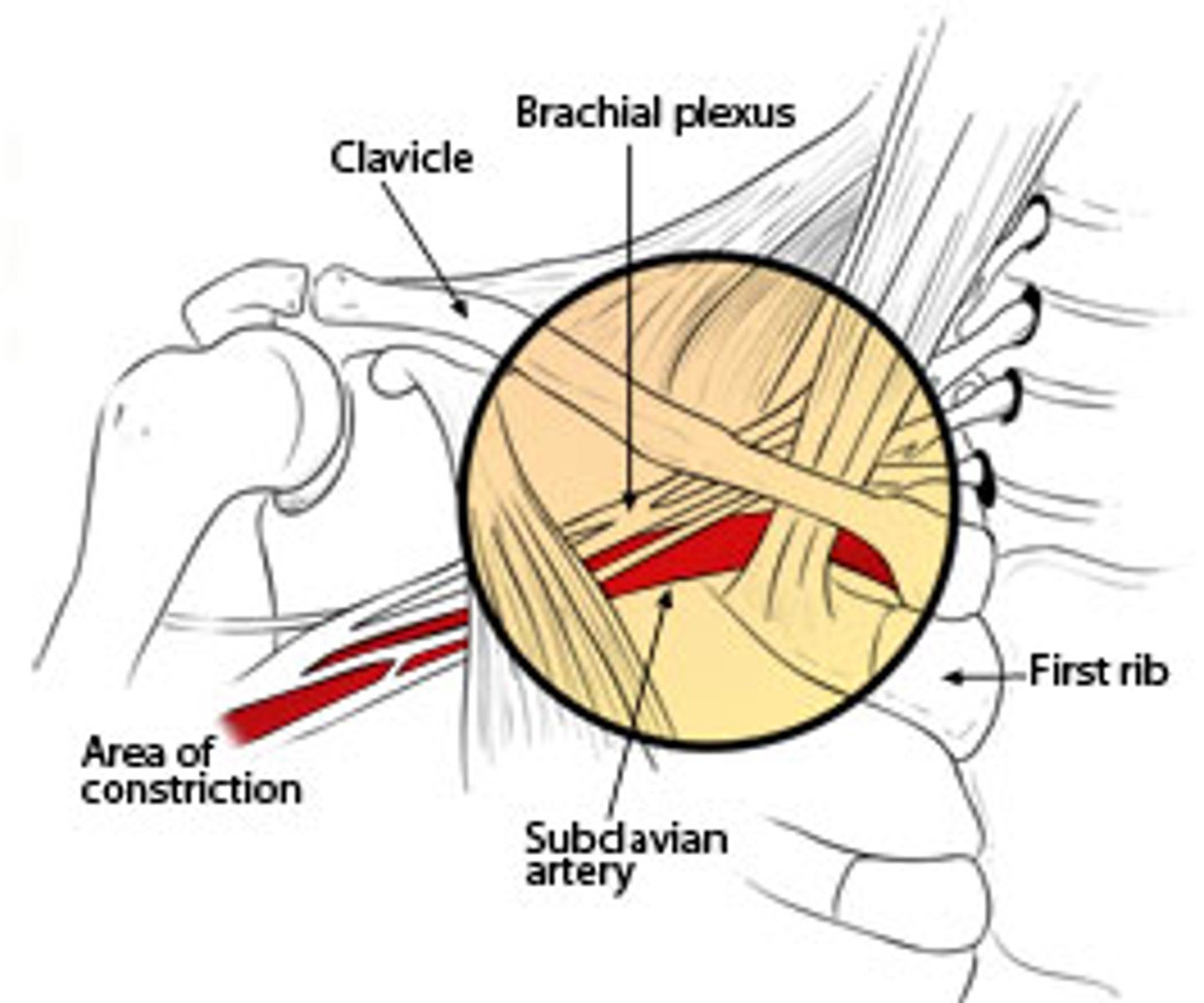
Thoracic Outlet Syndrome
Injury:
Causes:
Muscle Deficit/Functional Deficit:
Presentation:
Injury: compression of the lower trunk and subclavian vessels
Causes:
- cervical rib
- pancoast tumor
Muscle Deficit/Functional Deficit:
- same as klumpke palsy
Presentation:
- atrophy of intrinsic hand muscles
- ischemia, pain, and edema due to vascular compression
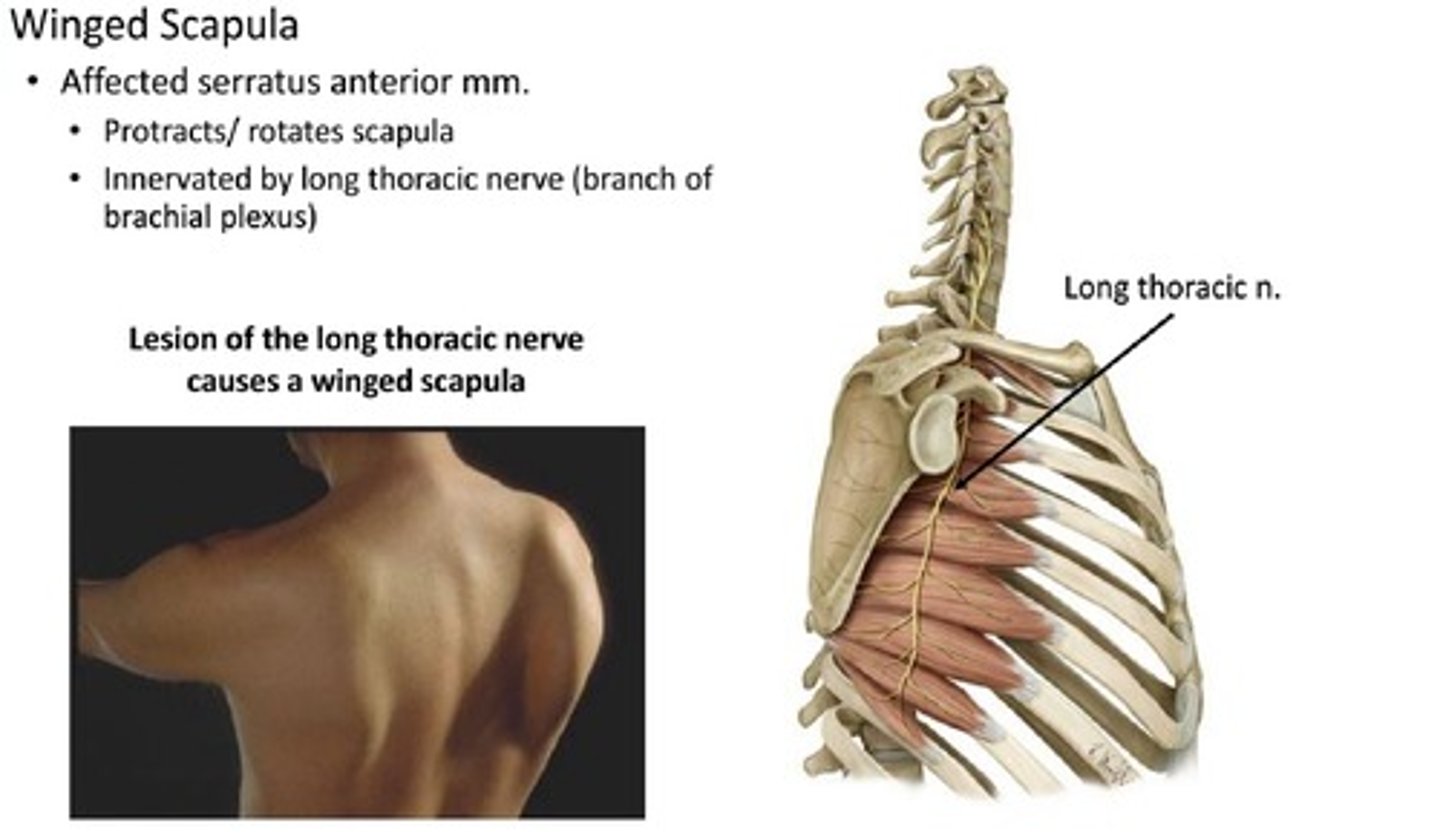
Winged Scapula
Injury:
Causes:
Muscle Deficit/Functional Deficit:
Presentation:
Injury: lesion of the long thoracic nerve
Causes:
- axillary node dissection after mastectomy
- stab wounds
Muscle Deficit/Functional Deficit:
- serratus anterior
Presentation:
- inability to anchor scapula to the thoracic cage --> cannot abduct arm above horizontal position
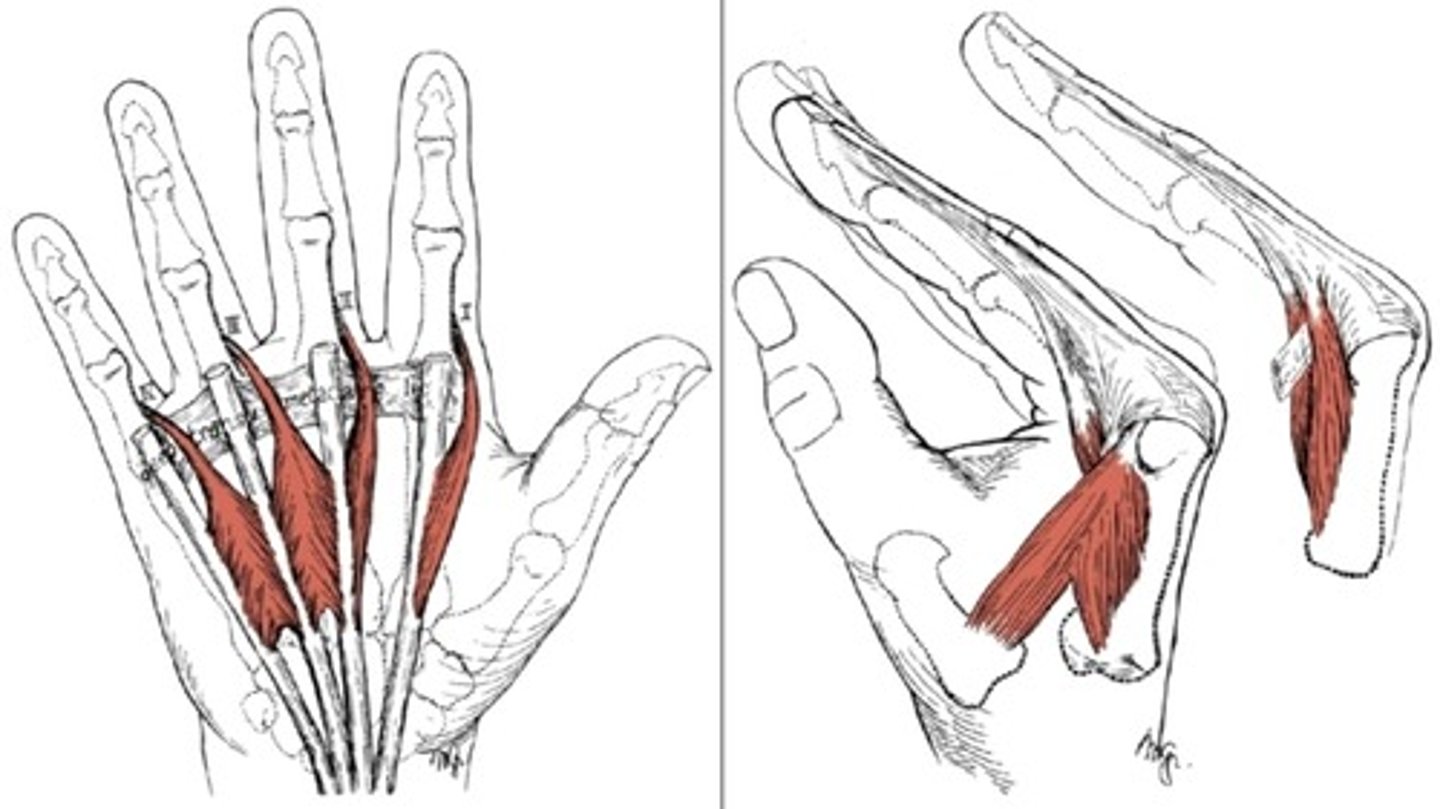
What is the action of the lumbrical muscles of the hand?
- flexion of the MCP
- extension of the DIP and PIP
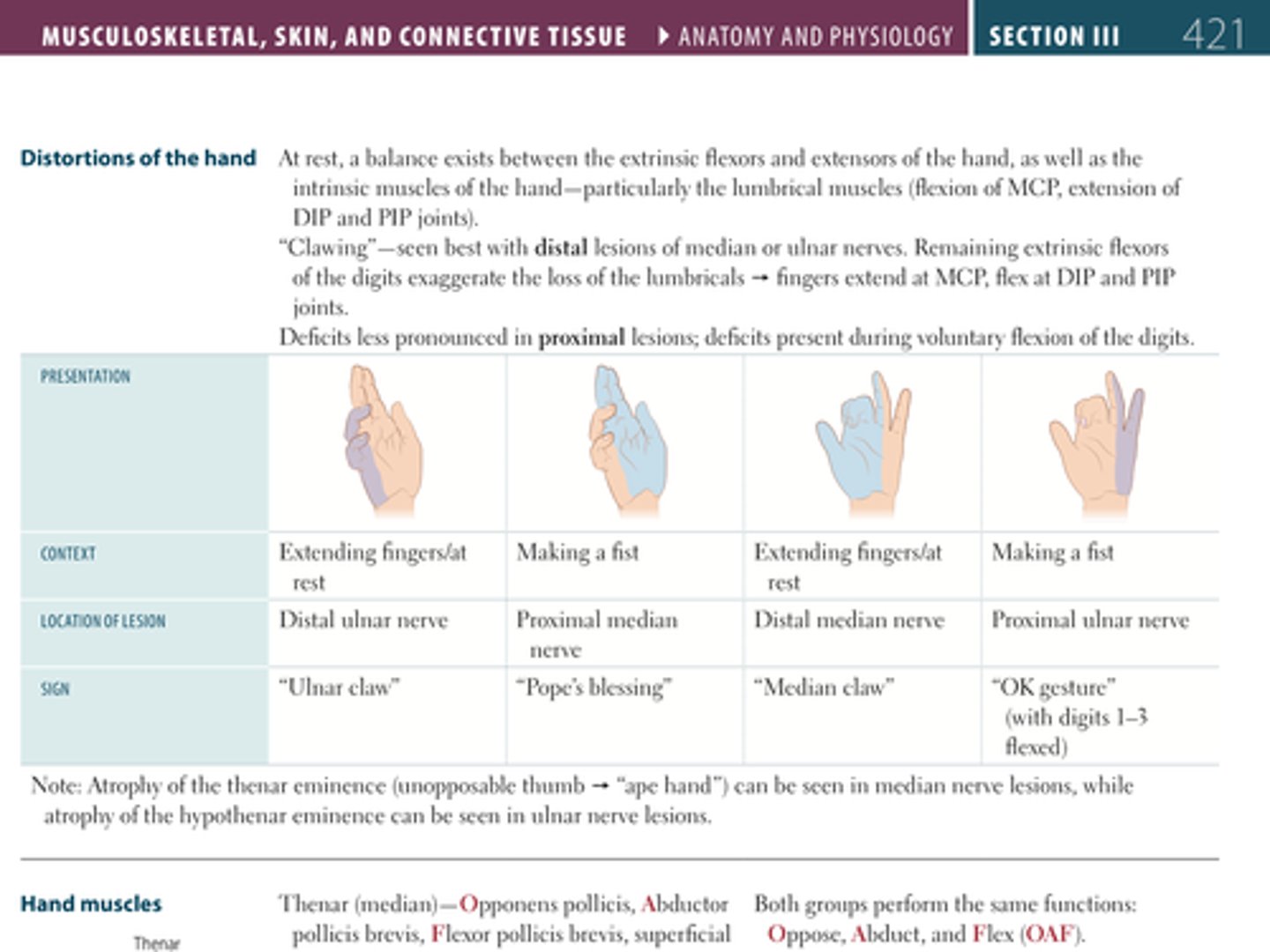
Compare and contrast the hand distortions seen in:
Distal ulnar nerve injury
Proximal median nerve injury
Distal median nerve injury
Proximal ulnar nerve
Give the CONTEXT in which the deficit will become apparent, the appearance of the sign and the name of the sign.
Lesions of what nerve = thenar eminence atrophy?
Lesions of what nerve = hypothenar eminence atrophy?
Lesions of what nerve = thenar eminence atrophy?
- MEDIAN NERVE
Lesions of what nerve = hypothenar eminence atrophy?
- ULNAR NERVE
For the following intrinsic hand muscles, give their actions:
Thenar muscles (median nerve)
Hypothenar muscles (ulnar nerve)
Dorsal interossei
Palmar interossei
Lumbricals
Thenar muscles (median nerve):
- opponens pollicis
- abductor pollicis brevis
- flexor pollicis bracis
- superficial head
= OAF = oppose, abduct, flex
Hypothenar muscles (ulnar nerve):
- opponens digiti minimi
- abductor digiti minimi
- flexor digit minimi
= OAF = oppose, abduct, flex
Dorsal interossei = abduct the fingers (DAB, Dorsal ABduct)
Palmar interossei = adduct the fingers (PAD, Palmar ADucts)
Lumbricals = flex at the MCP, extend at DCP and PIP
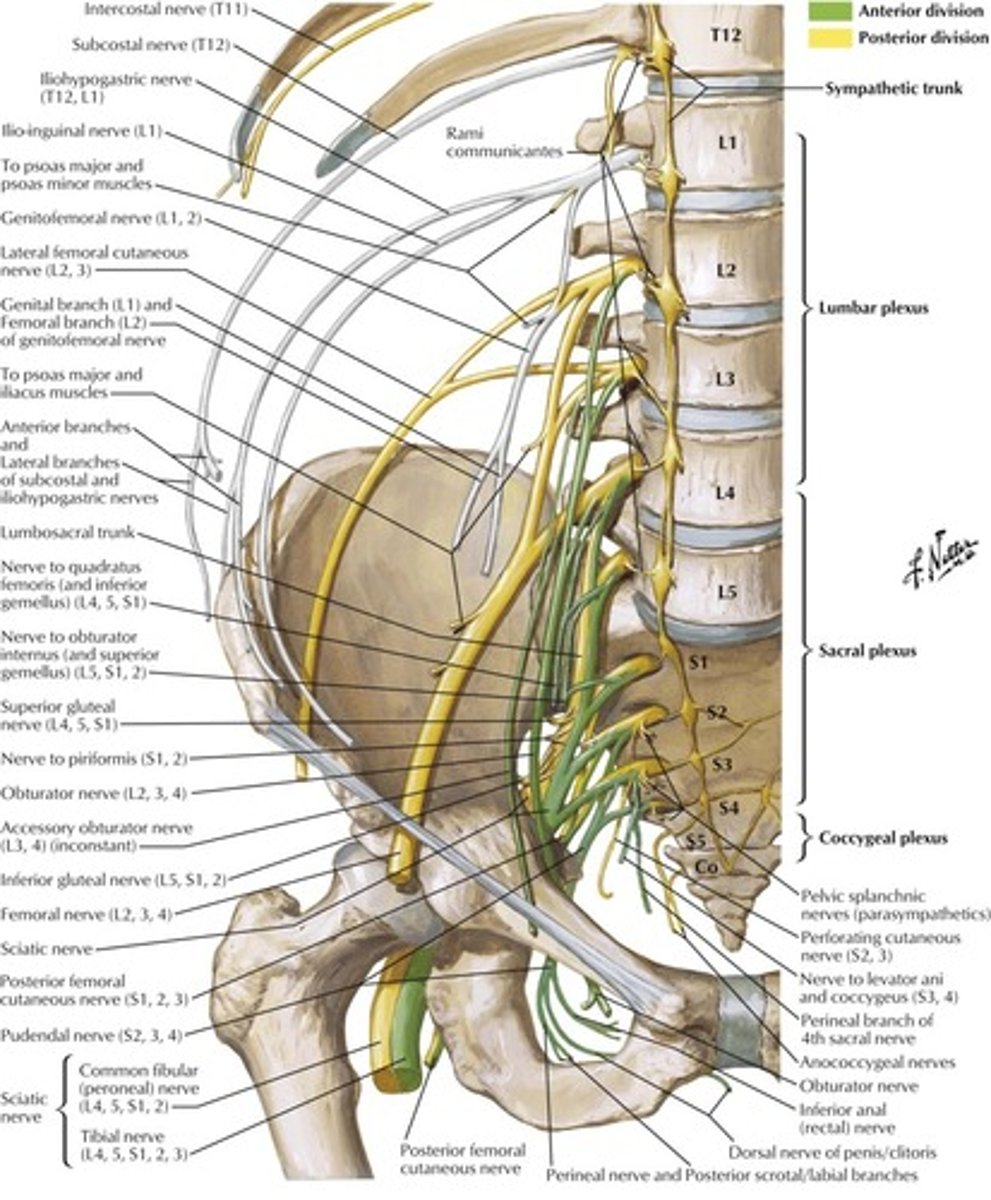
Obturator Nerve
Root:
Cause of injury:
Presentation:
Root: L2-L4
Cause of injury:
- pelvic surgery
Presentation:
- decreased medial thigh sensation
- decreased hip adduction
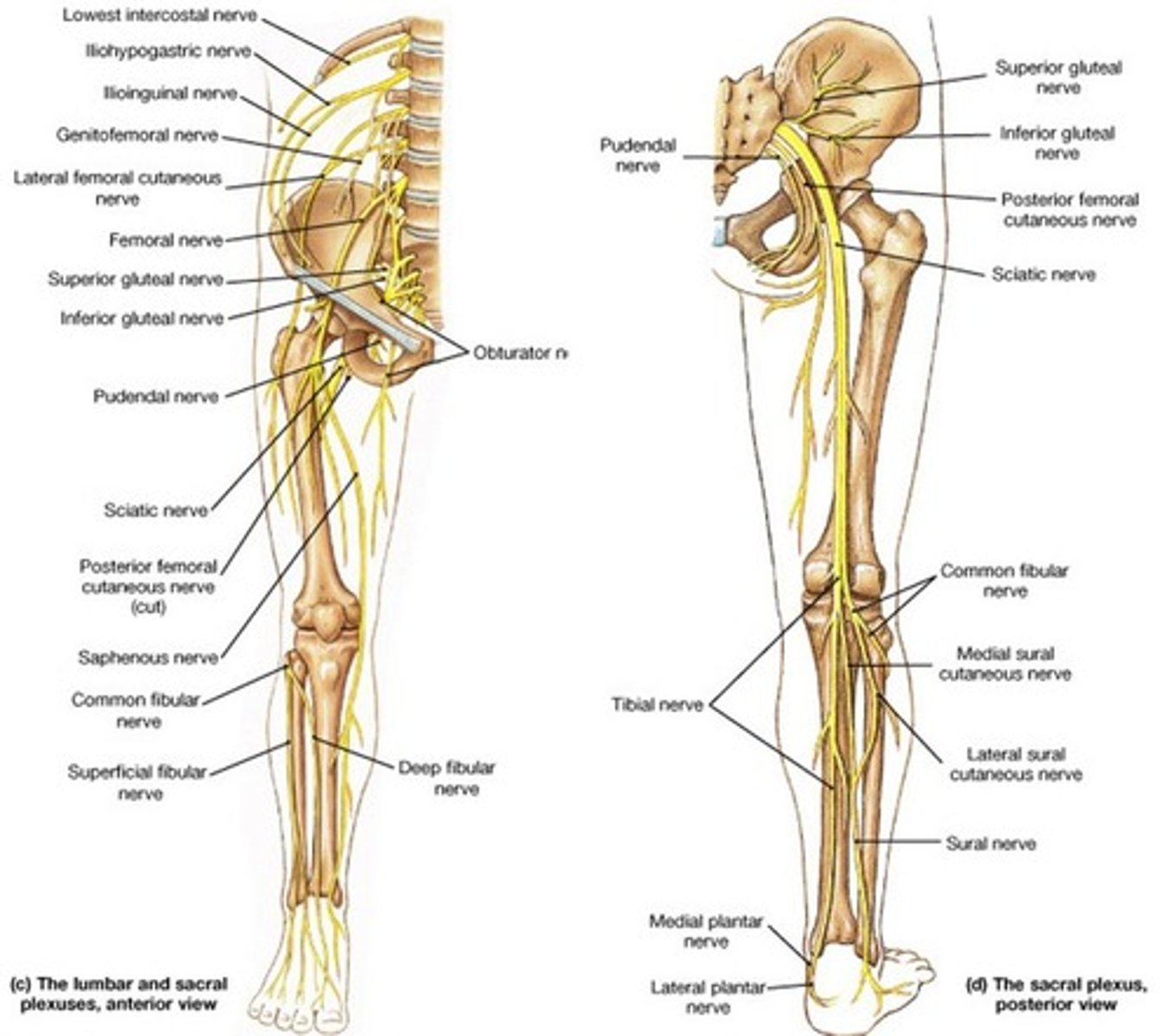
Femoral
Root:
Cause of injury:
Presentation:
Root: L2-L4
Cause of injury:
- pelvic fracture
Presentation:
- decreased thigh flexion and leg extension (quads)
(remember femoral does anterior thigh only; sciatic does posterior thigh and lower leg)
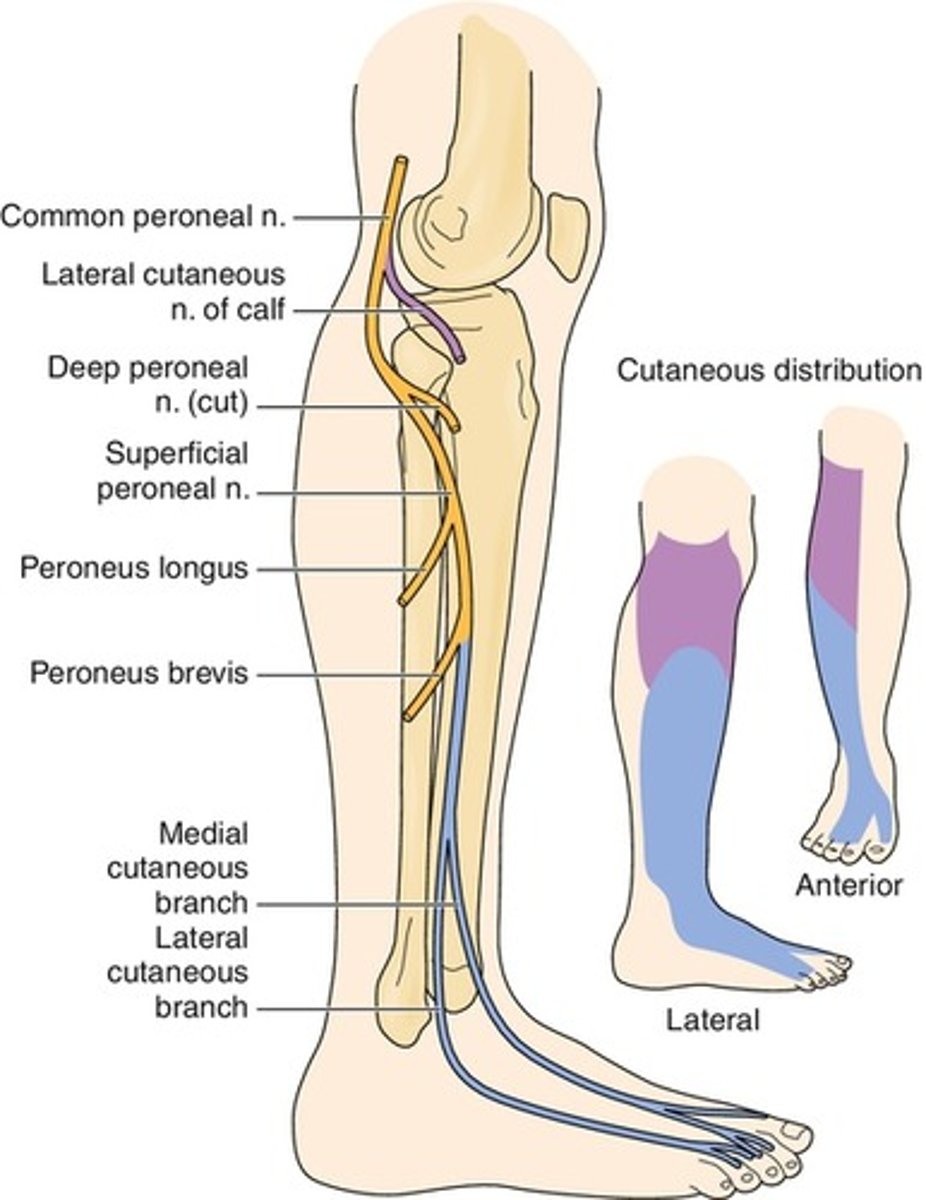
Common Peroneal
Root:
Cause of injury:
Presentation:
Root: L4-S2
Cause of injury:
- trauma or compression of the lateral aspect of the leg, fibular neck fracture
Presentation:
- foot drop --> innverted and plantar flexed at rest due to loss of eversion and dosiflexion
- "steppage" gait
- loss of sensation on the dorsum of the foot
Remember:
- the sciatic nerve innervates the posterior thigh
- from the sciatic arises both the tibial and the common fibular (peroneal) nerve, which both innervate the lower leg
- the common peroneal emerges from the posterior thigh, wraps around the neck of the fibula at the lateral head then innervates the anterior surface of the lower leg
- the tibial nerve innervates the posterior lower leg
NOTE:
- the superficial peroneal gives off branches that provide sensory innervation to the dorsum of the foot and lateral shin
- deep peroneal provides sensory innervation only to the region between the first and second digits of the toe
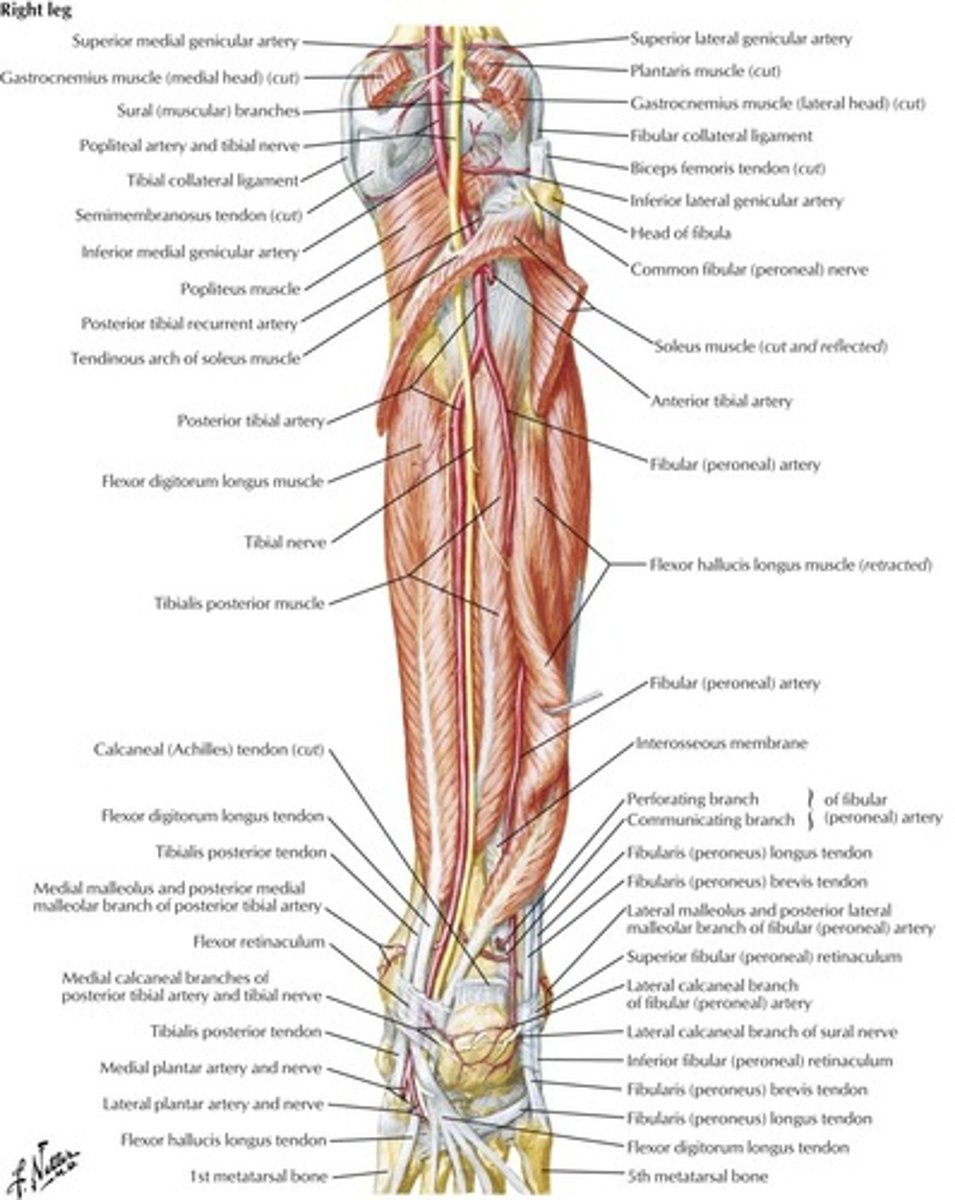
Tibial Nerve
Root:
Cause of injury:
Presentation:
Root: L4-S3
Cause of injury:
- knee trauma
- baker's cyst (proximal lesion)
- tarsal tunnel syndrome (distal lesion)
Presentation:
- inability to curl toes and loss of sensation on SOLE of foot
- in proximal lesions, foot is everted at rest with a loss of inversion and plantarflexion
Remember:
- the sciatic nerve innervates the posterior thigh
- from the sciatic arises both the tibial and the common fibular (peroneal) nerve, which both innervate the lower leg
- the peroneal emerges from the posterior thigh, wraps around the head of the femur at the lateral head then innervates the anterior surface of the lower leg
- the tibial nerve innervates the posterior lower leg
Superior Gluteal Nerve
Root:
Cause of injury:
Presentation:
Root: L4-S1
Cause of injury:
- iatrogenic injury during intramuscular injection to upper medial gluteal region
Presentation:
- Tendelenburg sign/gait --> pelvis tilts because weight bearing leg cannot maintain alignment of pelvis through hip adduction
- lesion is CONTRALATERAL to the side of the hip that drops, ipsilateral to the extremity on which the patient stands
Note:
- the superior gluteal nerve innervates gluteus medius, minimus and tensor fascia latae
- the inferior gluteal nerve innervates gluteus maximus

Superior Gluteal Nerve
Inferior Gluteal Nerve
Root:
Cause of injury:
Presentation:
Root: L5- S2
Cause of injury:
- posterior hip dislocation
Presentation:
- difficulty climbing stairs, rising from seated position
- loss of hip extension
Note:
- the superior gluteal nerve innervates gluteus medius, minimus and tensor fascia latae
- the inferior gluteal nerve innervates gluteus maximus
What muscles does the superior gluteal nerve innervate?
What muscles do the inferior gluteal nerve innervate?
What are the actions of the peroneal nerve?
What are the actions of the tibial nerve?
What muscles does the superior gluteal nerve innervate?
- gluteus medius
- gluteus minimus
- tensor fascia latae
What muscles do the inferior gluteal nerve innervate?
- gluteus maximus
What are the actions of the peroneal nerve?
- eversion and dosiflexion of foot
What are the actions of the tibial nerve?
- inversion and plantar flexion of foot
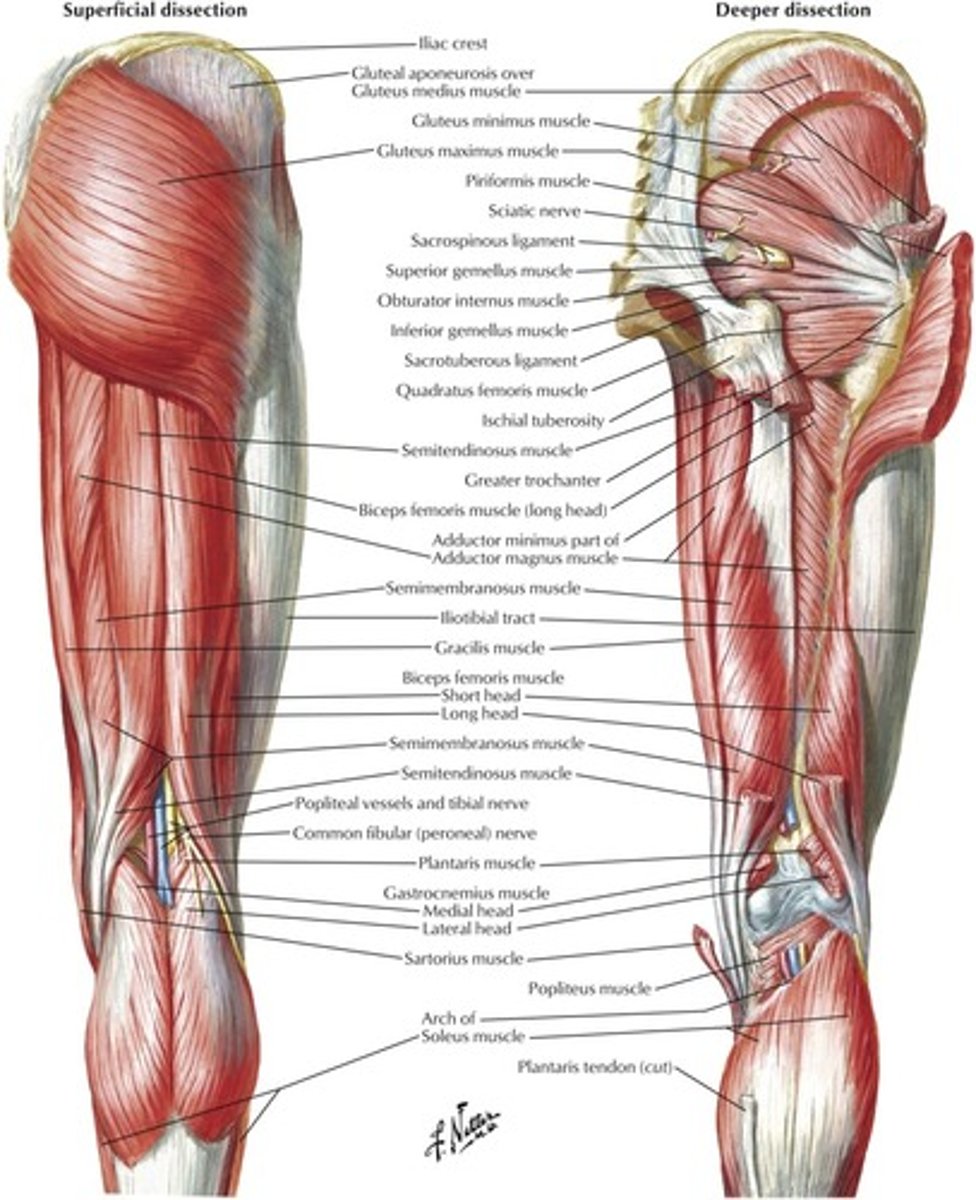
What is the course of the sciatic nerve?
Arises from L4-S3
Innervates the posterior thigh
Splits into the tibial and common peroneal (which innervate the lower leg)
What does the pudendeal nerve innervate?
Arises from S2-S4
Innervates the perineum
Can be blocked with local anesthetic during childbirth using the ischial spine as a landmark for injection
What gluteal quadrant should be chosen for IM injection to avoid nerve injury?
Choose the superolateral gluteal quadrant as the IM injection site to avoid nerve injurt
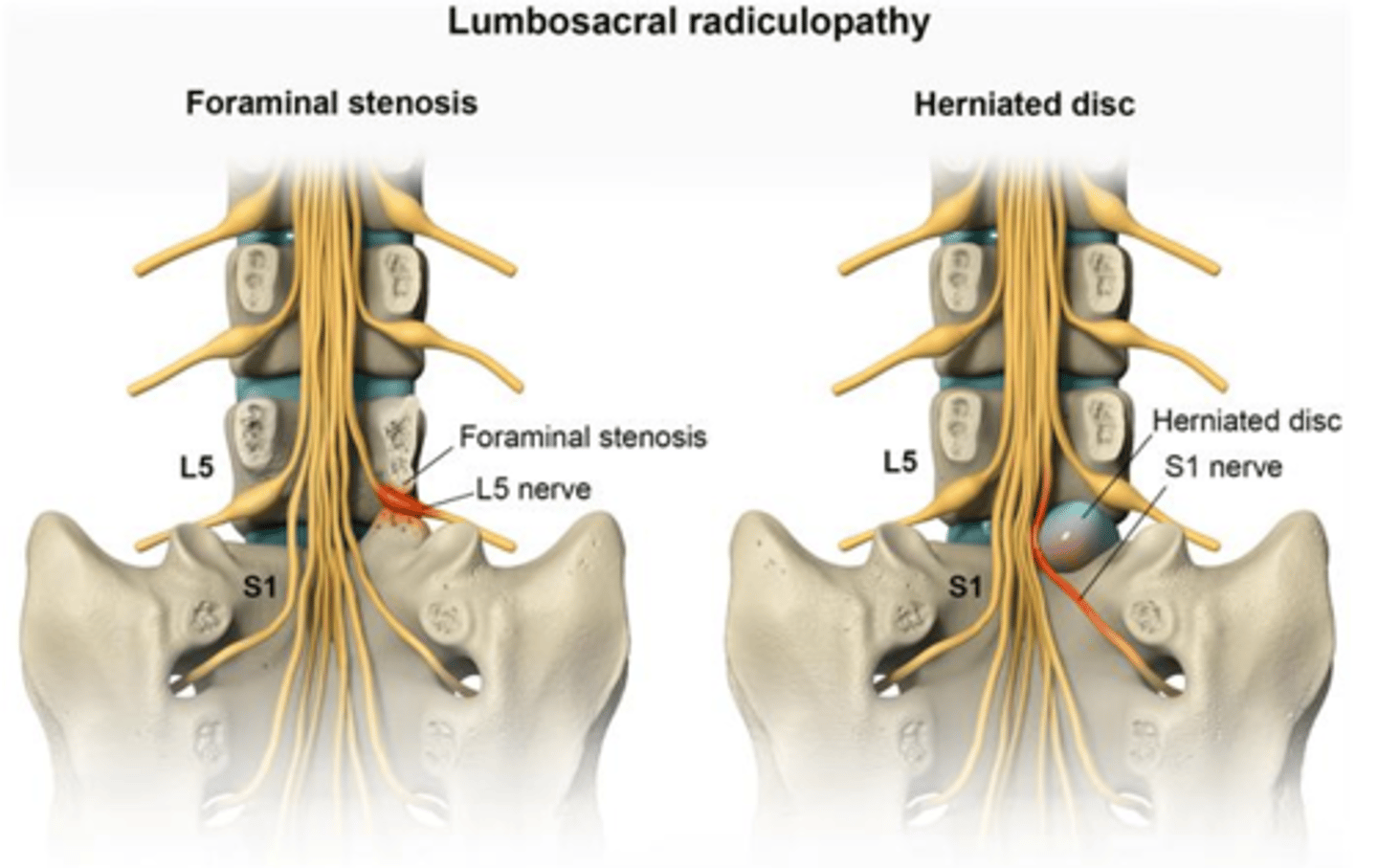
What are the signs of a lumbrosacral radiculopathy?
What is the pathophysiology of a slipped disc (ie: lumbrosacral radiculopathy)? What nerve level tends to be pinched?
Which direction do the intervertebral discs tend to herniate?
What are the signs of a lumbrosacral radiculopathy?
- numbness, paresthesias, weakness in the distribution of a specific lumbar or sacral spinal nerves
What is the pathophysiology of a slipped disc (ie: lumbrosacral radiculopathy)? What nerve level tends to be pinched?
- often due to invertebral disc herniation in which the nerve associated with the inferior vertebral body is impinged
- ie: herniation of the L3/L4 disc affects the L4 spinal nerve
Which direction do the intervertebral discs tend to herniate?
- generally herniate posteriolaterally
- this is because of the thing posterior longitudinal ligament and THICK anterior longitudinal ligament along the midline of the vertebral bodies
Herniation/radiculopathy at the following disc levels result in what physical exam findings?
L3-L4
L4-L5
L5-S1
L3-L4: weakness of knee extension, decreased patellar reflex
L4-L5: weakness of dorsiflexion, difficulty in heel walking
L5-S1: weakness of plantarflexion, difficulty in toe-walking. Diminished Achilles reflex
For the following anatomic locations, name the associated NERVE and ARTERY:
Axilla/lateral thorax
Surgical neck of the humerus
Midshaft of the humerus
Distal humerus/cubital fossa
Popliteal fossa
Posterior to medial malleous
Axilla/lateral thorax:
nerve: long thoracic
artery: lateral thoracic
Surgical neck of the humerus
nerve: axillary
artery: posterior circumflex
Midshaft of the humerus
nerve: radial
artery: deep brachial
Distal humerus/cubital fossa
nerve: median
artery: brachial
Popliteal fossa
nerve: tibial
artery: popliteal
Posterior to medial malleous
nerve: tibial
artery: posterior tibial
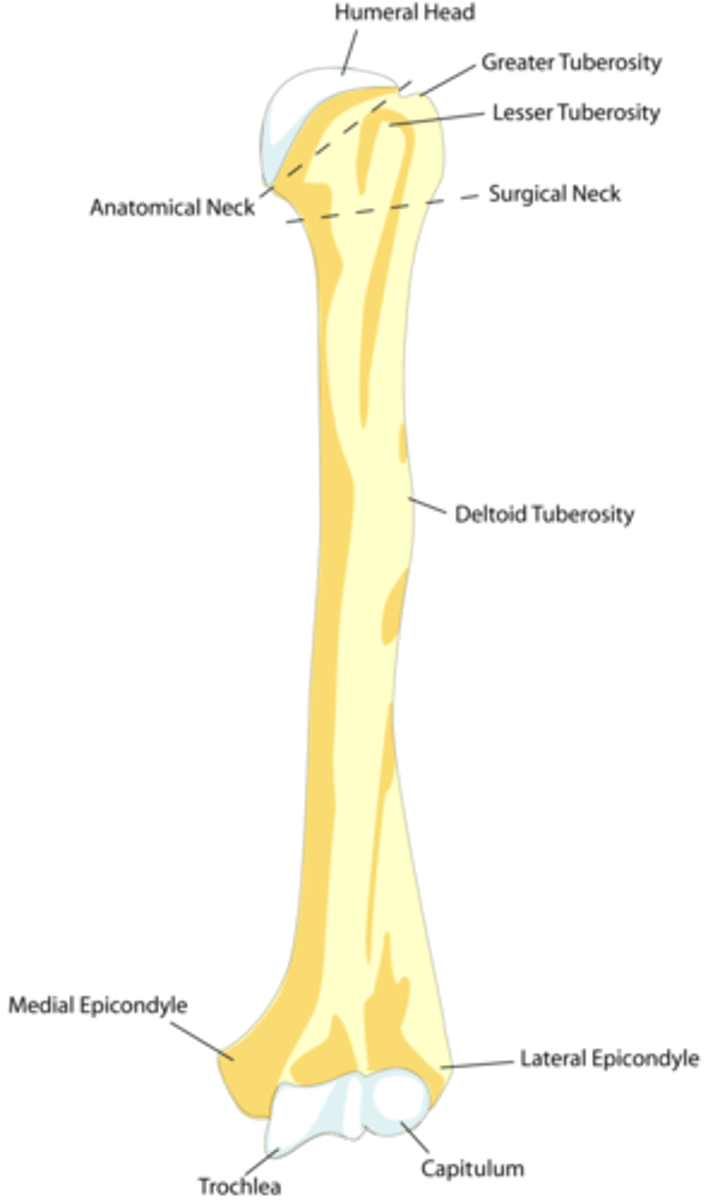
Humeral anatomy
Where is the surgical neck of the humerus?
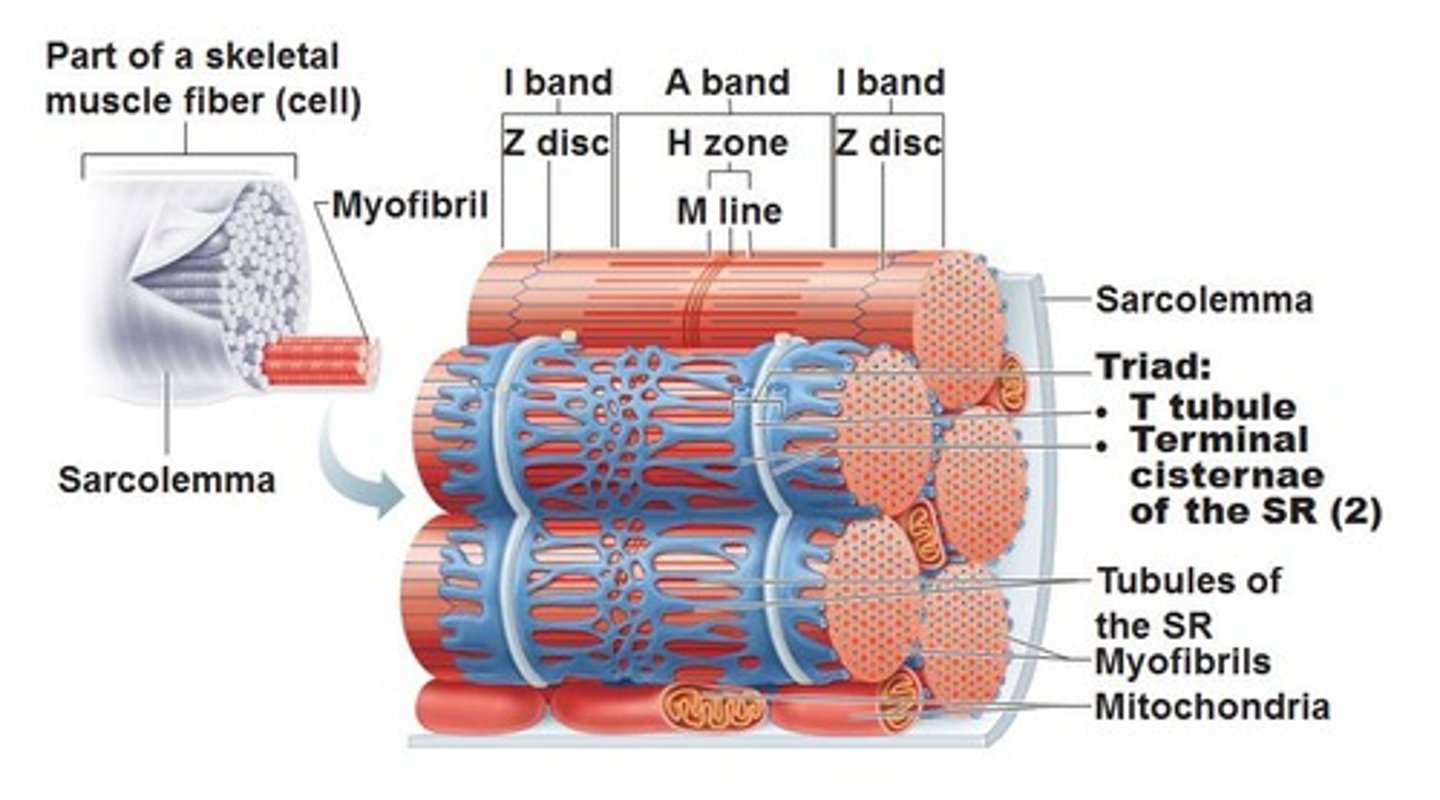
How is muscle conduction translated into muscle contraction?
What are T-tubules?
What is a triad?
What is a dyad?
What are T-tubules?
- extensions of plasma membrane juxtaposed with terminal cisternae of the sarcoplasmic reticulum (terminal cisternae are enlarged areas of the sarcoplasmic reticulum surrounding the transverse tubules.)
What is a triad?
- in skeletal muscle
- 1 T-tubule + 2 terminal cisternae
What is a dyad?
- in cardiac muscle
- 1 T-tubule + 1 terminal cisternae
Describe the physiology of skeletal muscle contraction
1. AP depolarization opens presynaptic voltage-gated Ca2+ channels, including neurotransmitter release
2. Postsynaptic ligand binding leads to muscle cell depolarization in the motor end plate
3. Depolarization travels along the muscle cell and down the T-tubule
4. Depolarization of the voltage-sensitive dihydropyridine receptor, mechanically coupled to the ryanodine repcetor on the SR, induces a conformational change in both receptors, causing Ca2+ release from the sarcoplasmic reticulum.
5. Released Ca2+ binds to troponin C, causing a conformational change that moves tropomyosin out of the myosin-binding groove onto actin filaments
6. Myosin releases bound ADP and Pi --> displacement of myosin on the actin filament (power stroke). Contraction results in shortening of the H and I bands between Z lines (HIZ shrinkage) BUT the A band always remains the same length)
7. Binding of a new ATP molecule causes detachment of myosin head from actin filament. Hydrolysis of bound ATP ---> ADP, myo head adopts high-energy postion ("cocked") for the next contration cycle
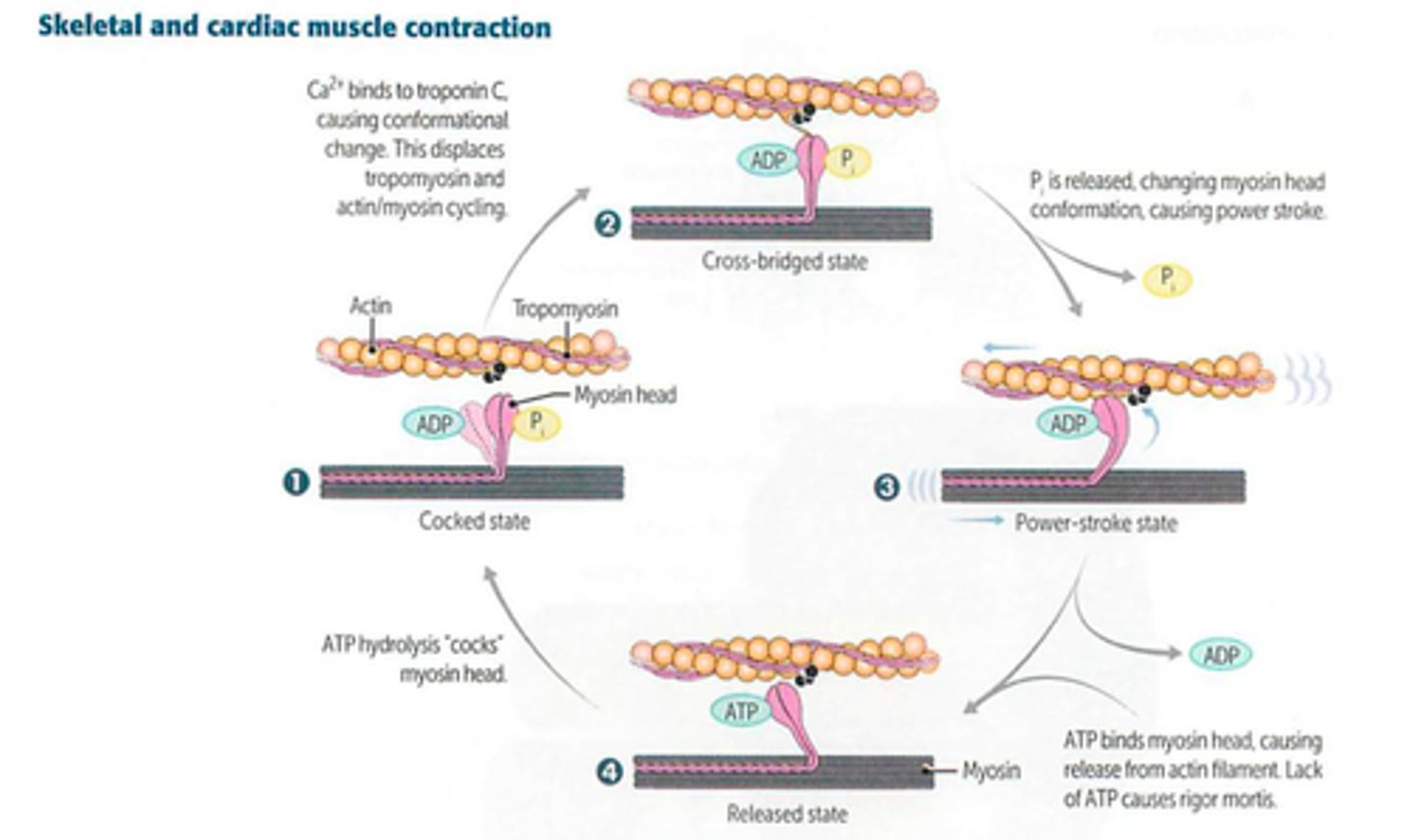
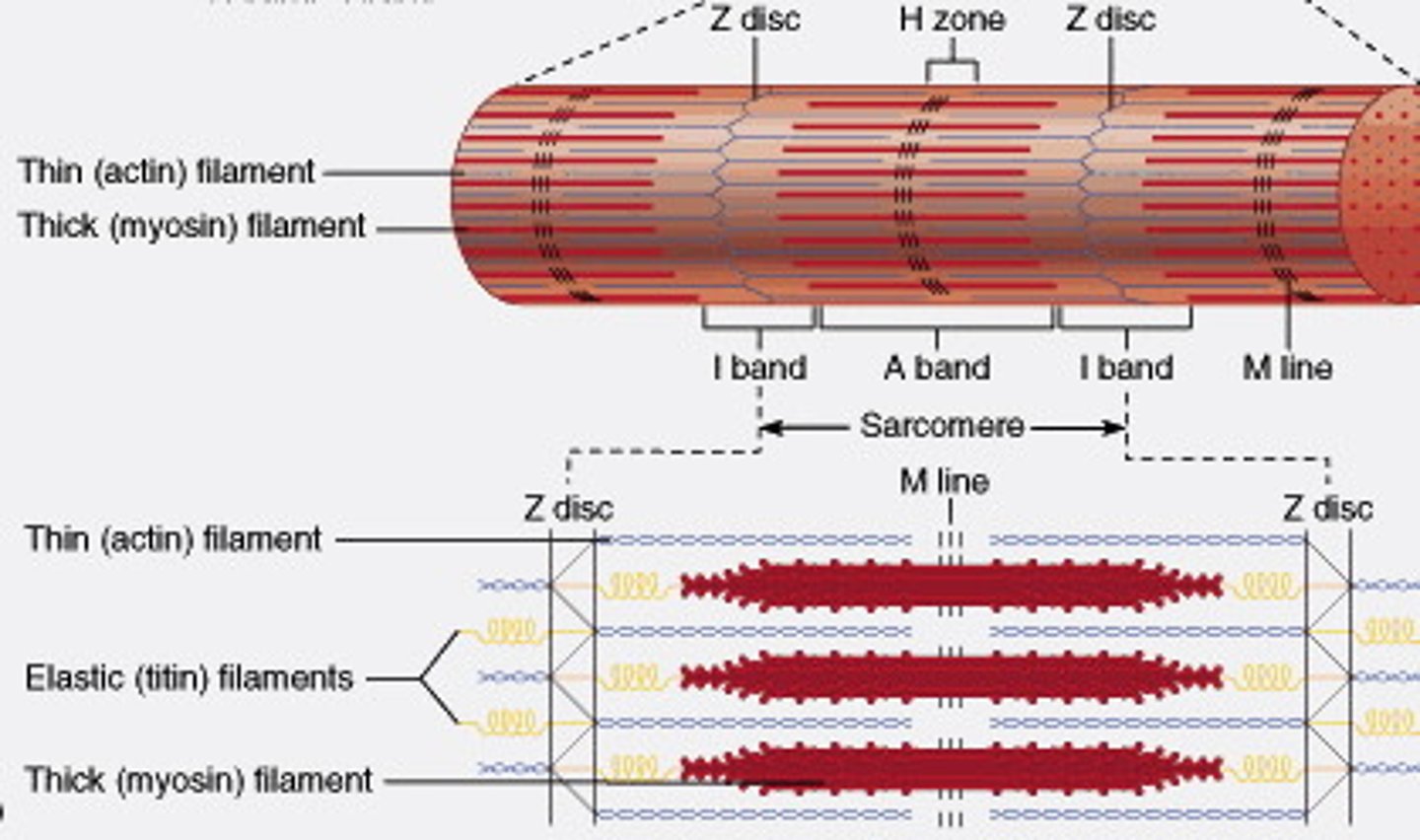
Provide the anatomy of a sarcomere --> what is each bit made of?
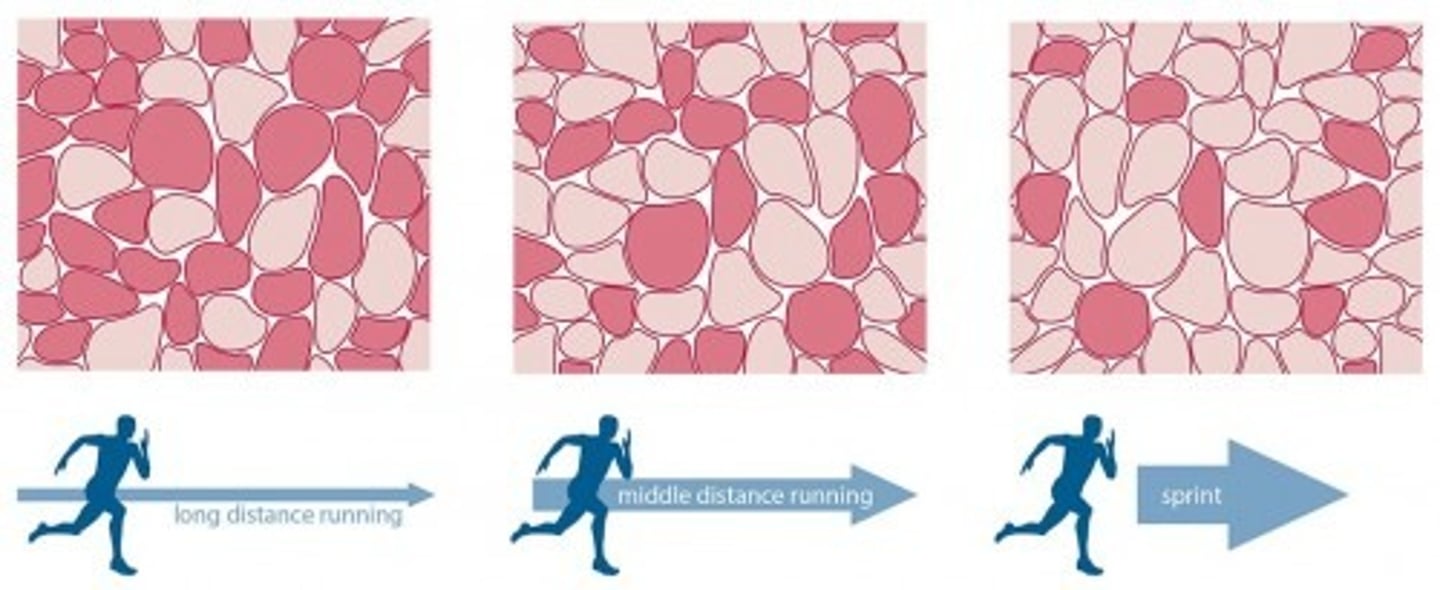
What is the difference between Type 1 and Type 2 muscle fibers?
Type 1 muscle:
- SLOW twitch
- RED fibers due to increased mitochondria and myoglobin concentration (increased oxidative phosphorylation) --> allows for sustained contraction
- proportionally increased after endurance training
Type 2 muscle:
- FAST twitch
- WHITE fibers resulting from decreased mitochondria and myoglobin concentration (increased anaerobic glycolysis)
- proportionally increased after weight/resistance training
What makes NO?
What is the precursor AA from which NO is made?
What is the process by which NO induces smooth muscle relaxation?
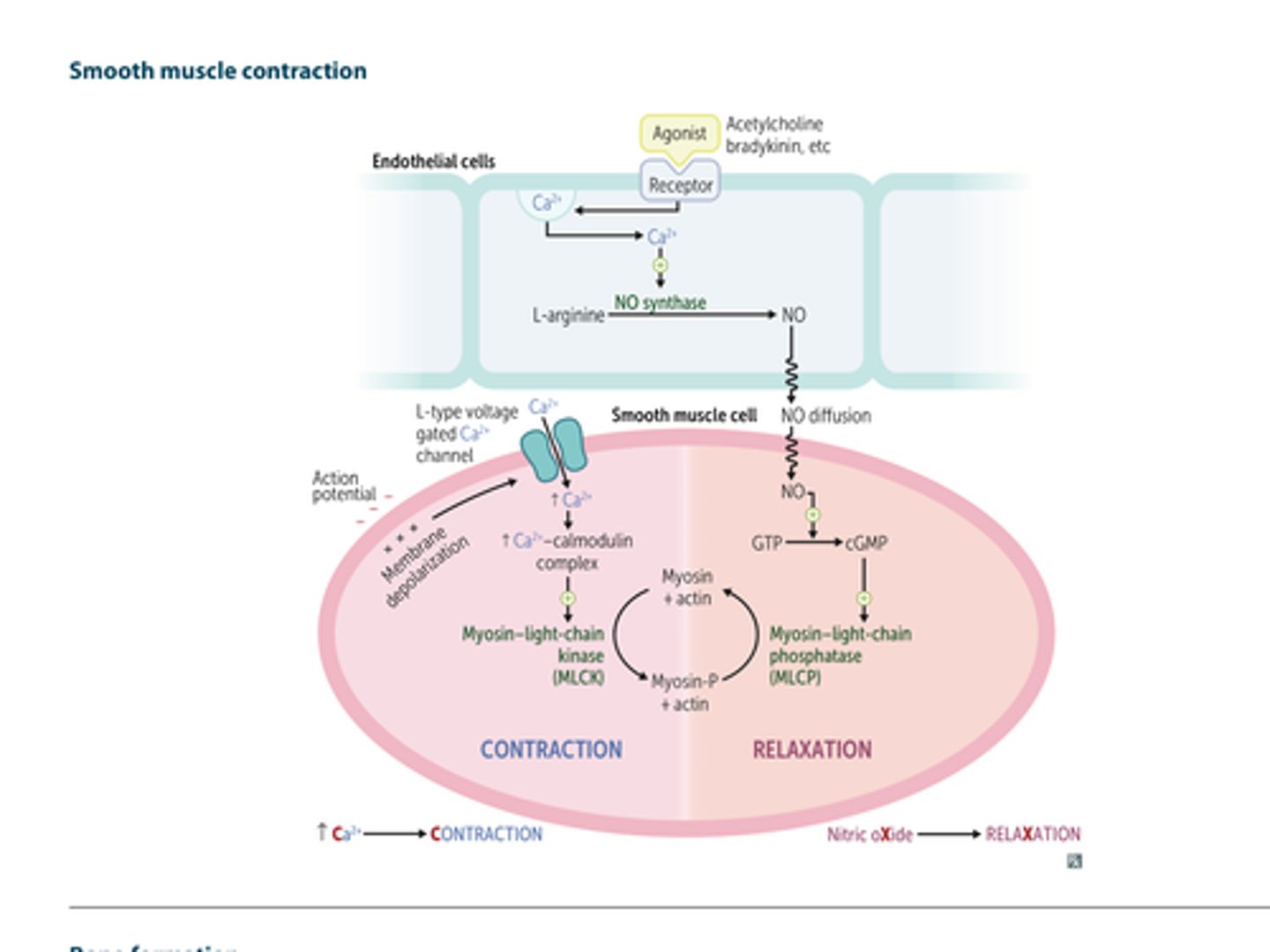
What is the process by which smooth muscle contracts?
What is endochondrial ossification?
When does it occur outside of the bone growth phase of childhood/adolescence?
What bones are synthesized via endochondrial ossification?
What is endochondrial ossification?
- occurs when a cartilaginous model of bone is first made by chrondrocytes
- osteoclasts and osteoblasts later replace the cartilaginous model with woven bone and then remodel that to lamellar bone
When does it occur outside of the bone growth phase of childhood/adolescence?
- in adults, woven bone occurs after fractures and in Paget disease
What bones are synthesized via endochondrial ossification?
- axial skeletal bones
- appendicular skeleton
- base of skull
What is membranous ossification?
What bones are synthesized via membranous ossification?
What is membranous ossification?
- woven bone is formed directly without cartilage and then later remodeled to lamellar bone
What bones are synthesized via membranous ossification?
- bones of the calvarium (skull) and facial bones!
With regard to the cell biology of the bone:
What is the function of osteoblasts? What do they differentiate from?
What is the function of osteoclasts? What do they differentiate from?
What is the effect of PTH on bone?
What is the effect of estrogen on bone?
What is the function of osteoblasts? What do they differentiate from?
- BUILDS BONE by secreting collagen and catalyzing mineralization in alkaline environments via alkaline phosphatase
- differentiate from mesenchymal stem cells in the periosteum
What is the function of osteoclasts?
- dissolves bone by secreting H+ and collagenases
- differentiates from a fusion of monocyte/macrophage lineage precursors
What is the effect of PTH on bone?
- at low, intermittent levels --> exerts anabolic (building) effects on osteoblasts (stim) and osteoclasts (block)
- chronically increased PTH levels (like in primary hyperparathyroidism) cause catabolic effects (osteitis fibrosa cystica)
- XS --> BREAKS DOWN BONE
What is the effect of estrogen on bone?
- inhibits apoptosis in bone-forming osteoblasts and induces apoptosis in bone-resorbing osteoclasts
- thus OVERALL --> BUILDS BONE
- an estrogen deficiency (surgical or postmenopausal), excess cycles of remodeling and bone resorption leads to osteoporosis
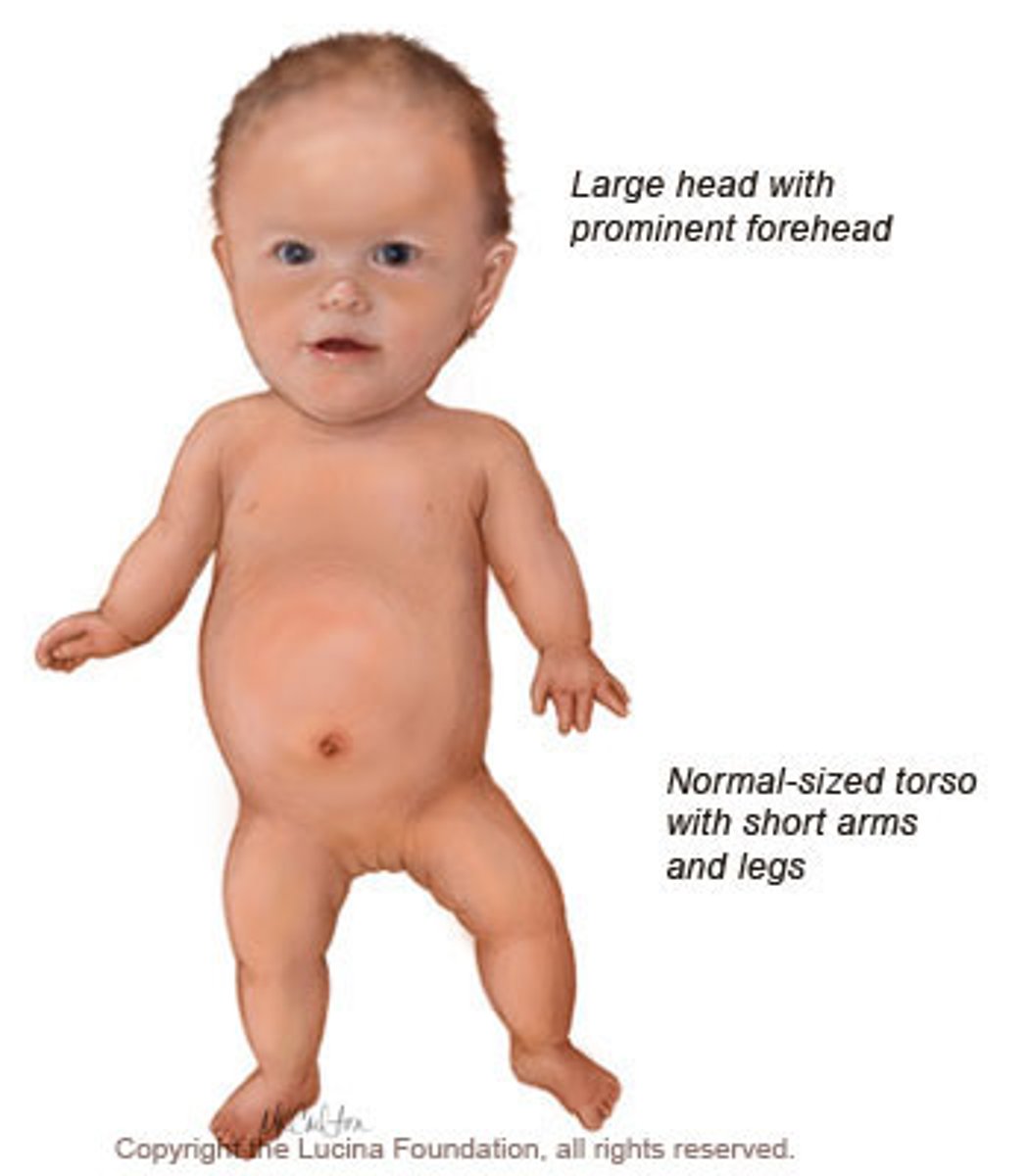
What is Achondroplasia?
What is the pathophys and findings?
What is the mutation and inheritance patter?
Most common cause of dwarfism!
What is the pathophys?
Due to a failure of longitudinal bone growth (endochondrial ossification) that results in SHORT LIMBS! Note that membranous ossification is not affected thus, the head is relatively large compared to the limbs.
What is the mutation?
- due to constitutive activation of fibroblast growth factor (FGFR3) which actually INHIBITS chrondrocyte proliferation
- greater than 85% of mutations occur sporadically
- autosomal dominant with full penetrance (homozygous is lethal)
Osteoporosis
What is it?
What is it commonly caused by?
How is it diagnosed?
Ppx?
Treatment?
What kinds of fractures can osteoporosis present with?
What is it?
- when there is loss of trabecular (spongy) and cortical bone mass as well as loss of interconnections despite normal bone mineralization and lab values (serum Ca2+ and PO4^3-)
What is it commonly caused by?
- increased bone reabsorption related to decreased estrogen levels and old age
- can also be secondary to drugs (ie: steroids, alcohol, anticonvulsants, anticoagulants, thyroid replacement therapy) or other medical conditions (ie: hyperparathyroidism, hyperthyroidism, MM, malabsorption syndromes)
How is it diagnosed?
- DEXA scan with T-score of < -2.5 or by a fragility fracture of the hip or vertebra
Ppx?
- regular weight bearing exercise and adequate Ca2+ and vitamin D intake throughout childhood
Treatment?
- bisphosphonates
- teriparatide
- SERMs
- rarely calcitonin
- denosumab (monoclonal antibody against RANKL)
What kinds of fractures can osteoporosis present with?
- vertebral compression fractures (acute back pain, loss of height, kyphosis)
- can also present with fractures of the femoral neck, distal radius (Colles fracture) --> note that femoral neck fractures lead to increased risk of osteonecrosis of the femoral head. the blood supply to the femoral head is mainly from the branches of the medial circumflex artery --> these vessels are especially vulnerable to damag from fractures of the head

What is osteopetrosis (aka Marble Bone Disease)?
What mutations can cause it?
Xray findings?
Complications?
What is osteopetrosis?
- failure of normal bone resorption due to defective osteoclasts --> thickened, dense bone that are prone to fracture
- bone fills the marrow space resulting in pancytopenia and extramedullary hematopoiesis
What mutations can cause it?
- mutations (carbonic anhydrase II) impair the ability of the osteoclast to generate an acidic environment necessary for bone reabsorption
Xray findings?
- bone-in-bone (stone bone) appearance
Complications?
- cranial nerve impingement
- palsies due to narrowed foramina
- bone marrow transplant is potentially curative as osteoclasts are derived from monocytes

Osteomalacia/Rickets
What is it?
Pathogenesis?
X ray findings?
What is it?
- defective mineralization of osteoid (osteomalacia) or cartilaginous growth plates (rickets, only in children)
- most commonly due to vitamin D deficiency
Pathogenesis?
- decreased vitamin D --> decreased serum Ca2+ --> increased PTH secretion --> decreased serum phosphate
X ray findings?
- osteopenia and "Looser zones" (pseudofracture) in osteomalacia
- epiphyseal widening and metaphyseal cupping/fraying in rickets
- children with rickets have bow legs, bead-like costochondral junctions (rachitic rosary), craniotabes (soft skull)

Paget Disease of Bone
(osteitis deformans)
What is it?
What are the lab findings?
What does the bone look like?
Complications?
What are some exam findings?
What are the stages of disease?
What is it?
- common, localized disorder of bone remodeling caused by increased osteoclastic activity following by increased osteoblastic activity that forms poor-quality bone
What are the lab findings?
- serum Ca2+, phosphorous and PTH levels are normal
- INCREASED ALP
What does the bone look like?
- mosaic pattern of woven and lamellar bone (osteocytes with lacunae in chaotic juxtaposition)
- long-bone chalk stick fractures
Complications?
- increased blood flow from increased AV shunts may cause high output cardiac failure
- increased risk of osteogenic sarcoma
What are some exam findings?
- hat size increased due to skull thickening
- hearing loss if common due to auditory foramen narrowing
What are the stages of disease?
Lytic --> osteoclasts
Mixed --> osteoclasts + osteoblasts
Sclerotic --> osteoblasts
Quiescent --> minimal osteoclast/osteoblast activity
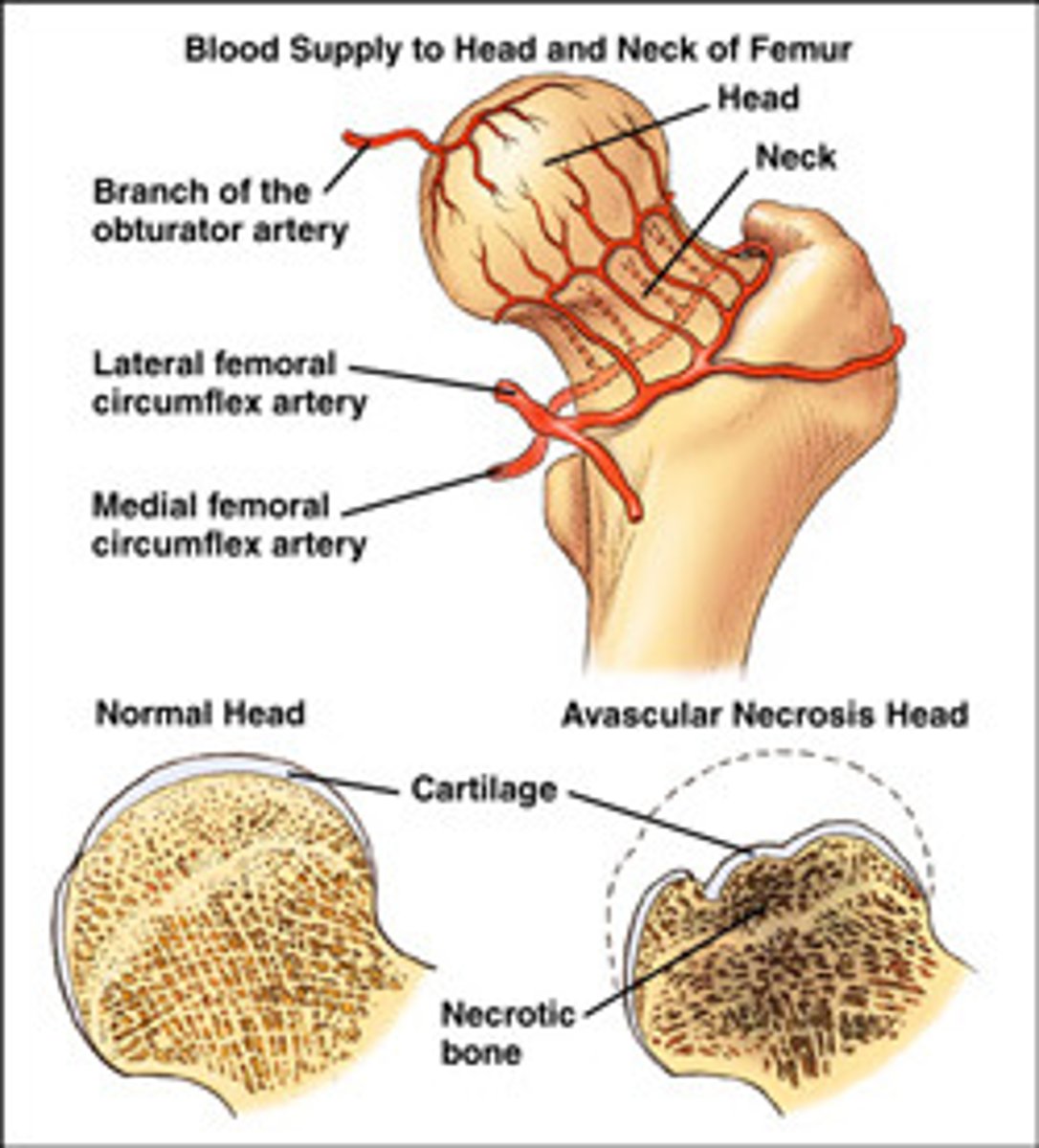
Osteonecrosis (avascular necrosis)
What is it?
Where is the most common site of occurrence?
What are the causes?
What is it?
- infarction of bone and marrow
- usually very PAINFUL
Where is the most common site of occurrence?
- most common site is the FEMORAL HEAD (watershed zone between the branch of the obturator and the medial femoral circumflex artery)
- fractures of the femoral head (common in the elderly with osteoporosis who have sustained a fall) lead to increased osteonecrosis risk due to shearing of the branches of the medial circumflex artery!
What are the causes?
- CAST Bent LEGS
C: corticosteroids
A: alcoholism
S: sickle cell disease
T: trauma
B: the Bends (caisson/decompression disease)
LE: LEgg-Calve-Perthes disease (idiopathic)
G: gaucher disease
S: slipped capital femoral epiphysis
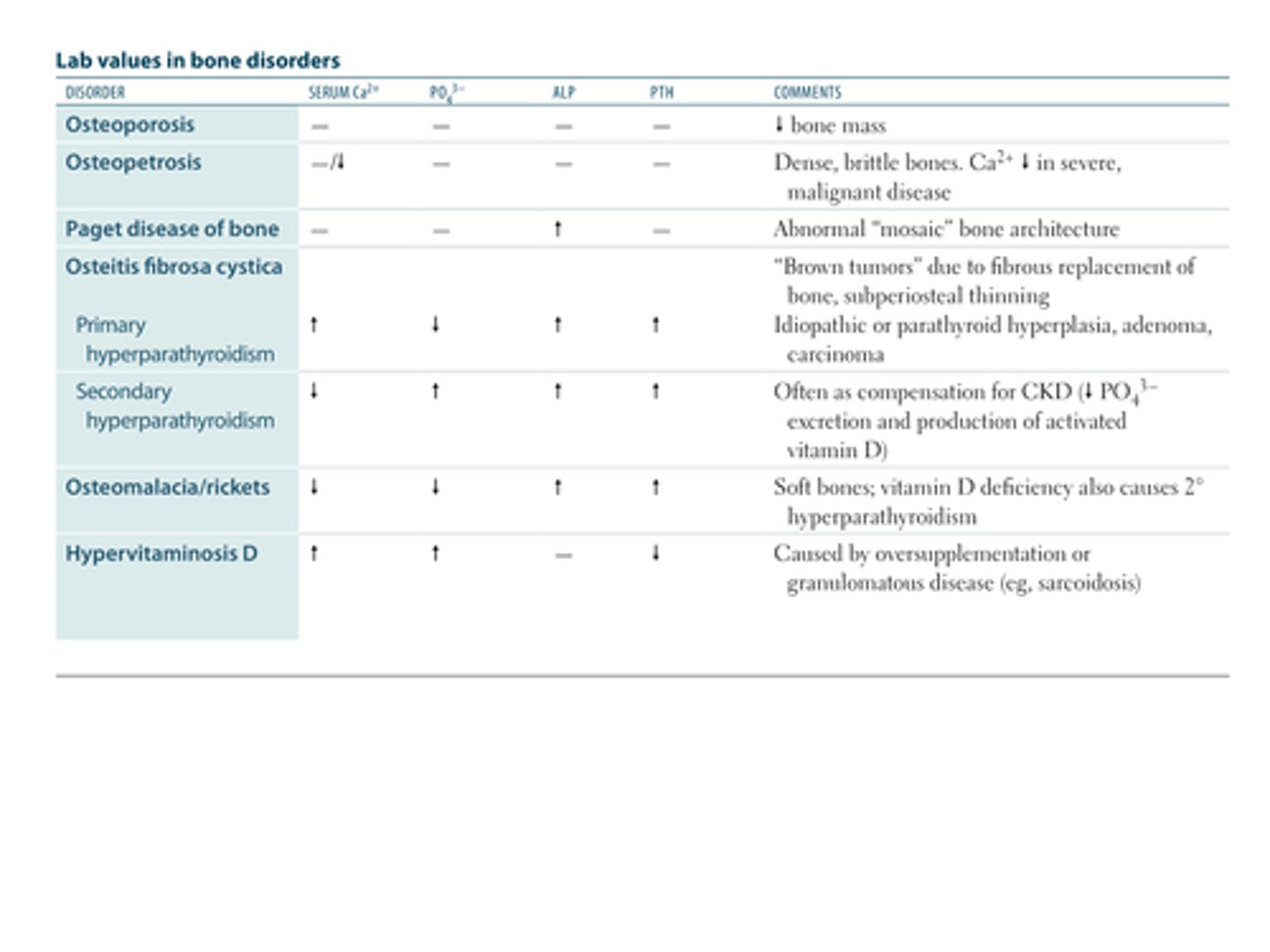
For the following bone disorders, please provide the observed change/alteration in:
Serum Ca2+
PO4^3-
ALP
PTH
Plus any additional pertinent findings
OSTEOPOROSIS
OSTEOPETROSIS
PAGET DISEASE OF BONE
OSTEITIS FIBROSA CYTISCA (finding in what disease?)
OSTEOMALACIA/RICKETS
HYPERVITAMINOSIS D
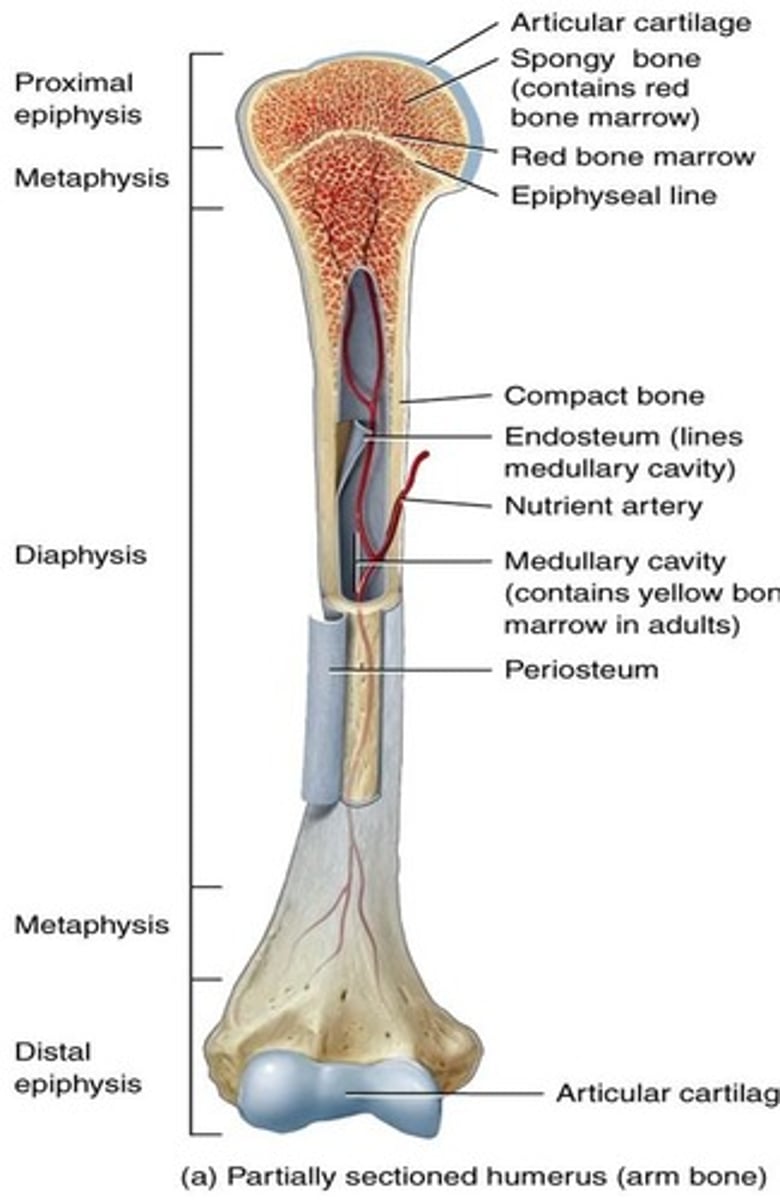
Long bone anatomy
Osteochondroma
tumor type:
epidemiology/location:
characteristics:
tumor type: benign primary bone tumor
epidemiology/location:
- most common benign bone tumor
- males < 25 years old
characteristics:
- bony exostosis with cartilaginous (chondroid) cap (A)
- rarely transforms to chondrosarcoma
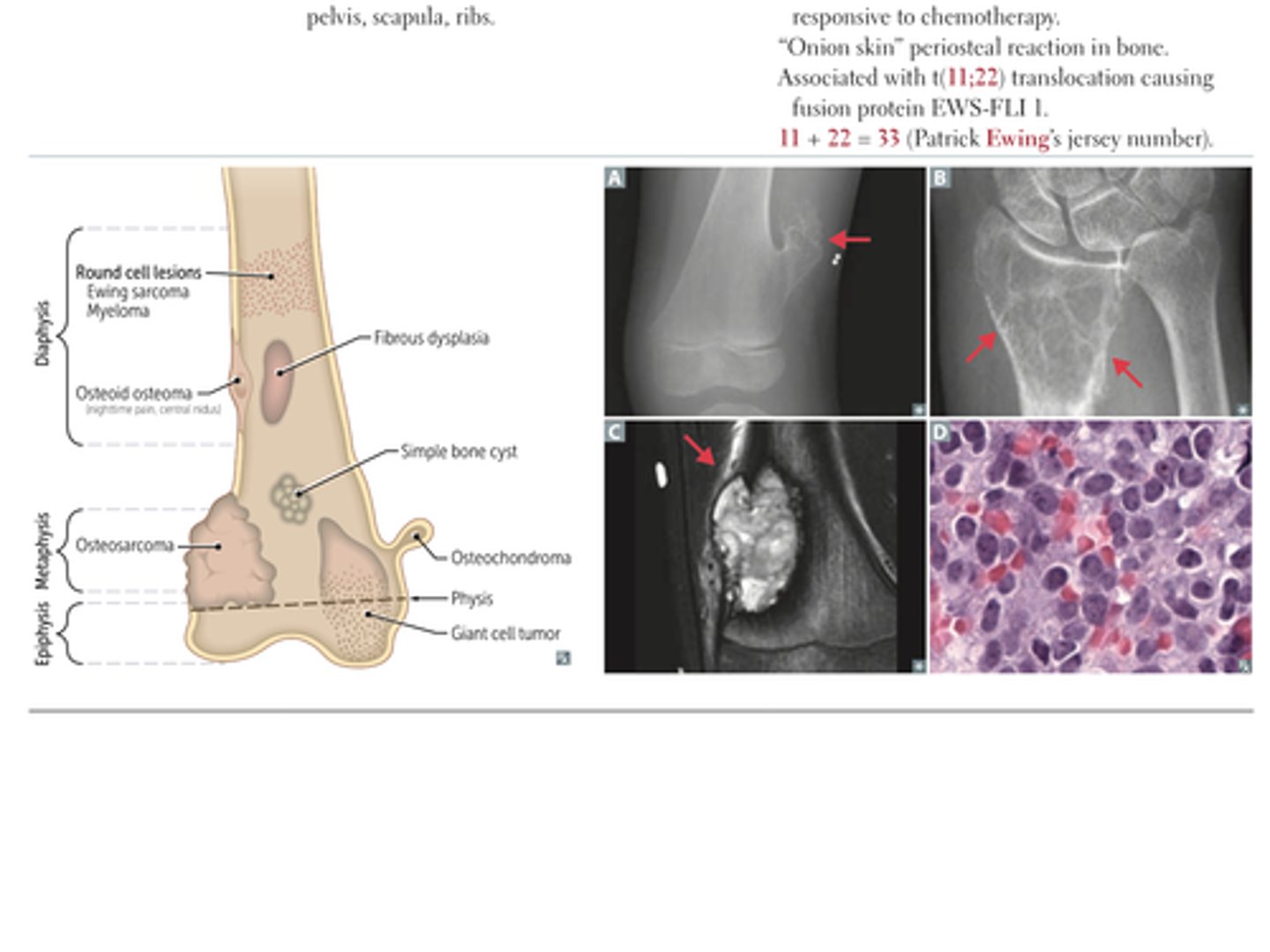
Giant Cell Tumor
tumor type:
epidemiology/location:
characteristics:
tumor type: benign primary bone tumor
epidemiology/location:
- 20 to 40 yro
- at epiphyseal end of long bones, often around knee
- "Osteoclastoma"
characteristics:
- locally aggressive benign tumor
- "soap bubble" appearance on xray
- multinucleated giant cellls

Osteosarcoma (osteogenic sarcoma)
tumor type:
epidemiology/location:
predisposing factors:
characteristics:
tumor type: malignant bone tumor (primary)
epidemiology/location:
- 2nd most common primary malignant bone tumor (after multiple myeloma)
- bimodal distribution: 10-20 yo, > 65
- location --> metaphysis of long bone often around knee
predisposing factors:
- paget disease of bone
- bone infarcts
- radiation
- familial retinoblastoma
- li-fraumeni syndrome (germiline p53 mutation)
characteristics:
- Codman triangle (from elevation of periosteum) or sunburst pattern on x-ray
- aggressive, treat with surgical en bloc resection (with limb salvage) and chemotherapy

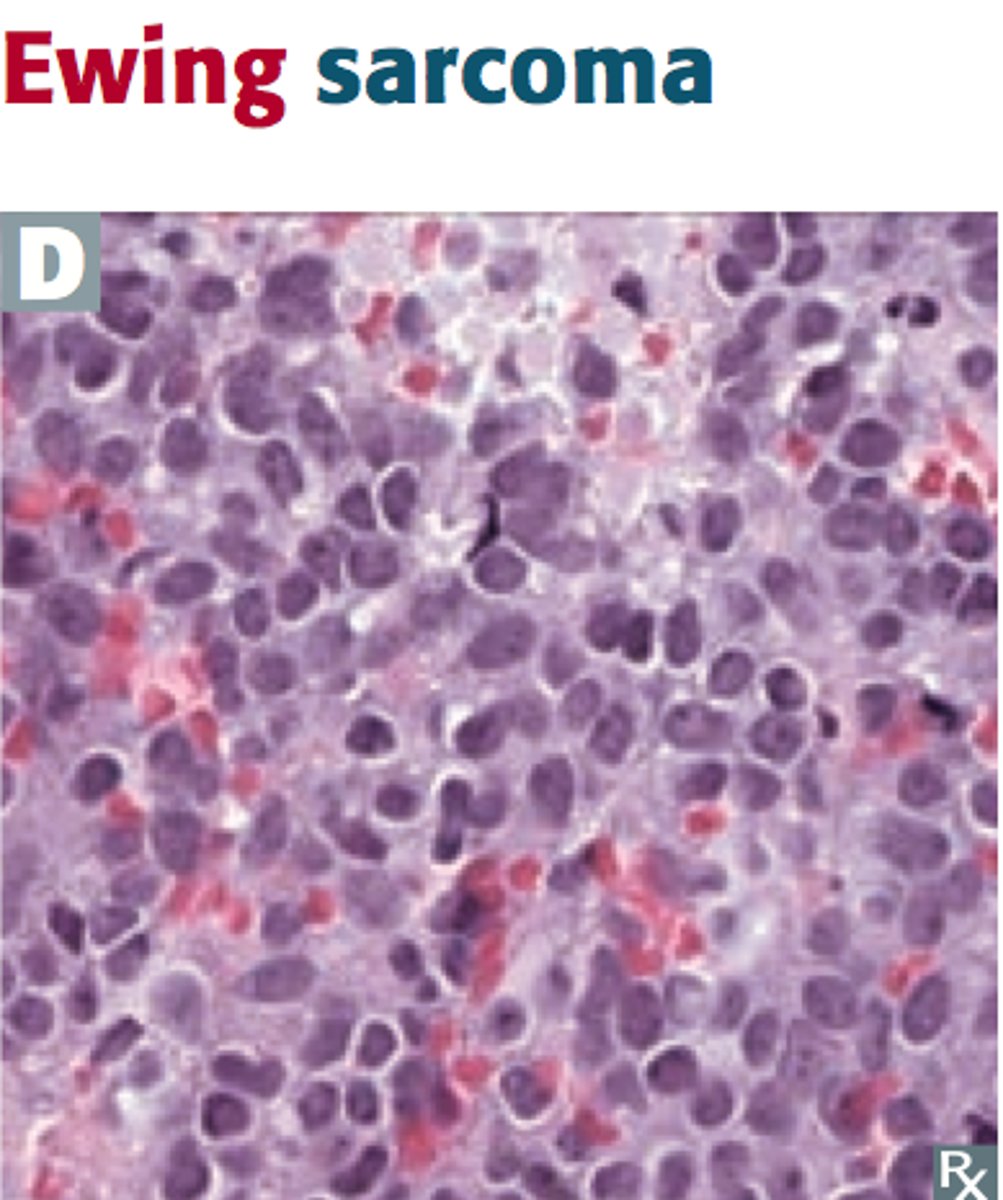
Ewing Sarcoma
tumor type:
epidemiology/location:
characteristics:
tumor type: malignant bone tumor (primary)
epidemiology/location:
- boys < 15 yo
- commonly appears in diaphysis of long bones, pelvis, scapula and ribs
characteristics:
- anaplastic small blue cell malignant tumor
-extremely aggressive with early mets, but responsive to chemotherapy
- "onion skin" periosteal reaction in bone
- associated with t(11;22) translocation causing fusion protein (EWS-FLI 1)
-11 + 22 = 33 (Patrick EWING's jersey number)
Locations of the various benign and malignant bone tumors
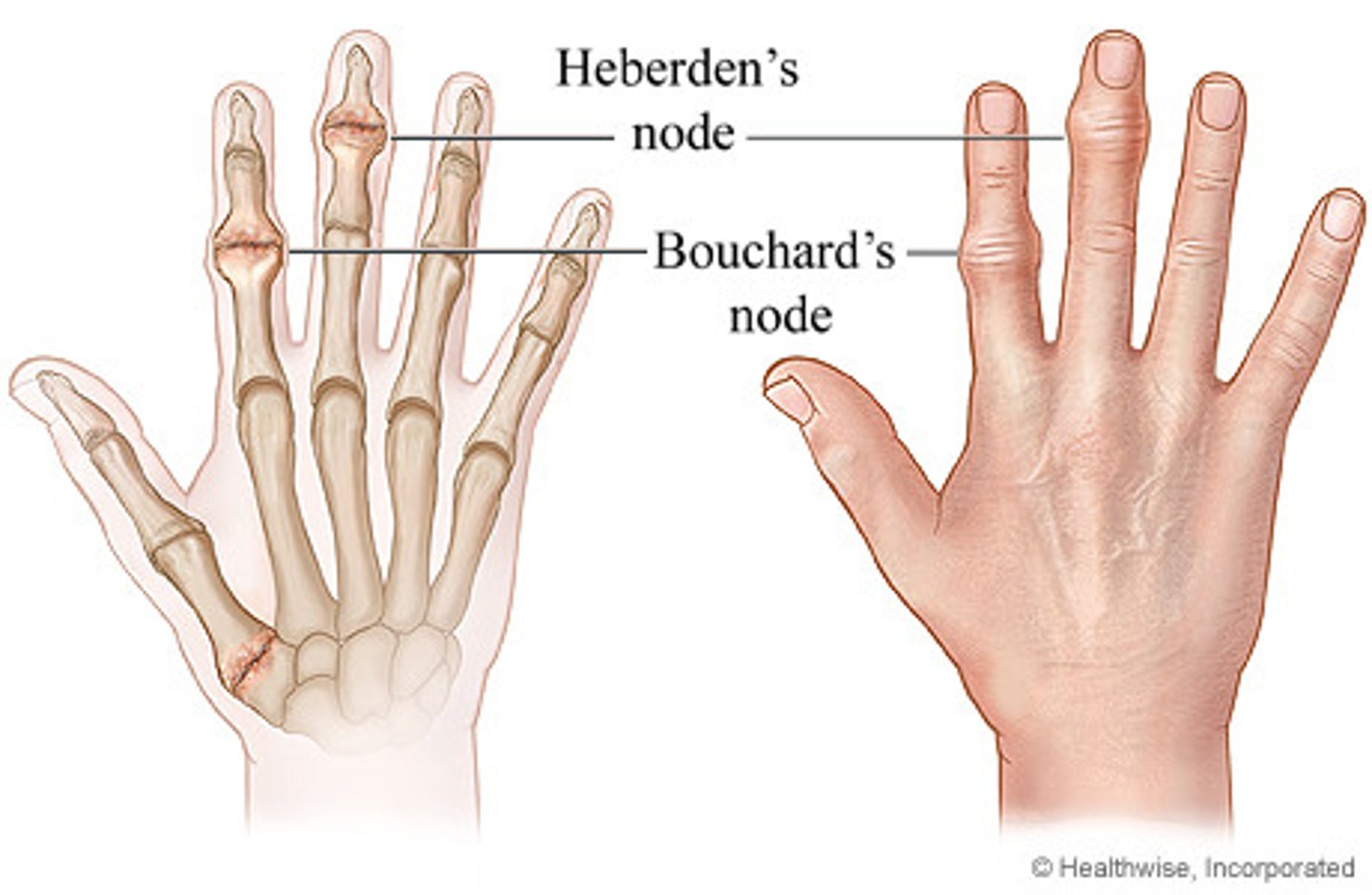
Osteoarthritis
Pathogenesis:
Predisposing factors:
Presentation:
Joint findings:
Treatment:
Pathogenesis:
- mechanical --> due to wear and tear that destroys the articular cartilage (degenerative joint disease)
- chondrocytes mediate degradation and inadequate repair
Predisposing factors:
- age, female, obesity, joint trauma
Presentation:
- pain in weight bearing joints after use (at end of day)
- improvement with rest
- asymmetric joint involvement
- knee cartilage loss begins medially (bowlegged)
- NO systemic symptoms
Joint findings:
- osteophytes (bone spurs)
- joint space narrowing
- subchondral sclerosis and cysts
- synovial fluid reveals non-inflammatory nature (WBC < 2000)
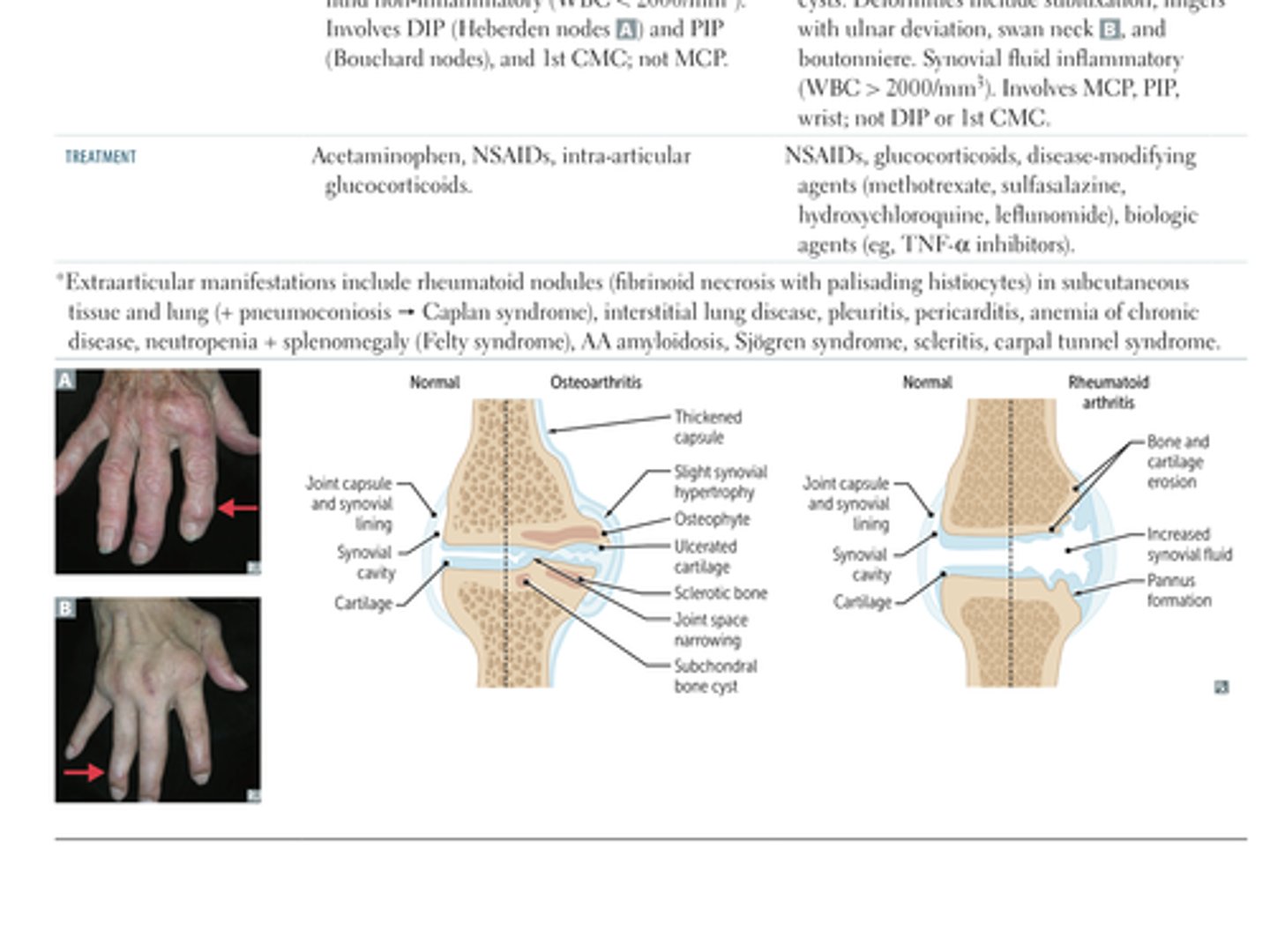
- involves DIP (Heberden) and PIP (Bouchard) and 1st CMC; NOT MCP
Treatment:
- acetaminophen
- NSAIDS
- intra-articular glucocorticoids
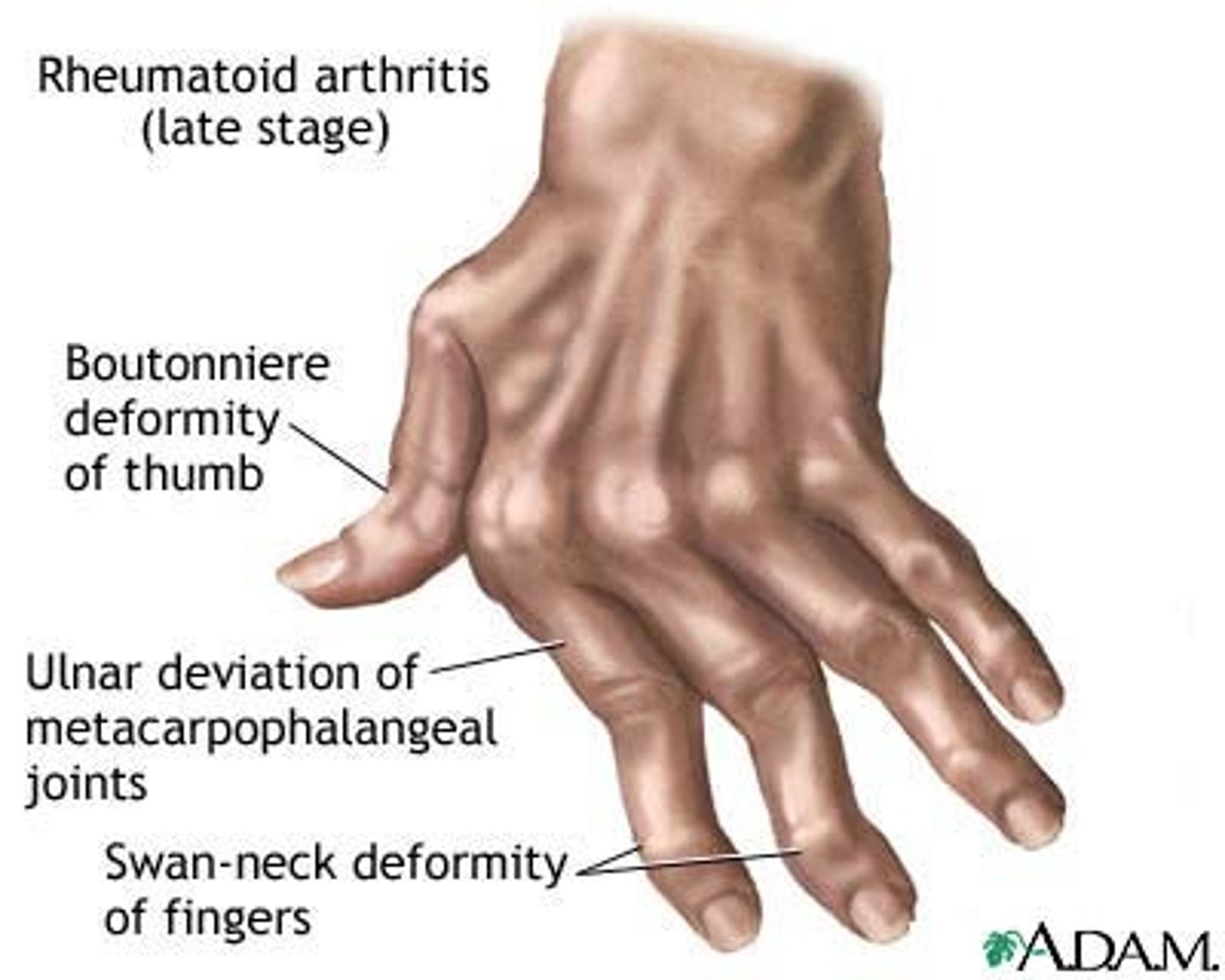
Rheumatoid Arthritis
Pathogenesis:
Predisposing factors:
Presentation:
Joint findings:
Treatment:
Pathogenesis:
- autoimmune --> inflammatory cytokines and cells induce pannus (proliferative granulation tissue) formation, which erodes the articular cartilage and bone
Predisposing factors:
- female
- HLA-DR4
- smoking
- silica exposure
*- + rheumatoid factor (anti-IgG antibody, seen in 80%)
- anti-citrullinated peptide antibody (anti-CCP; highly specific; measured by ELISA)* [tissue inflammation causes arginine residues in proteins like vimentin to be enzymatically converted into cirtulline through a process called citrullination. this can significantly affect the shape of these proteins, which can then serve as antigens and generate an immune response. in RA, the immune response is exaggerated resulting in high titers of anti-CCP not seen in other inflammatory conditions. )
Presentation:
- pain, swelling and morning stiffness > 1 hr
- improves with use
- symmetric joint involvement
- systemic symptoms (fever, fatigue, weight loss)
- extra-articular manifestations are common
Joint findings:
- erosions, juxtaarticular osteopenia
- joint space narrowing
- soft tissue swelling
- subchondral cysts
- deformities include: sublaxation, fingers with ulnar deviation, swan neck, and boutonnniere
- synovial fluid is inflammatory (WBC > 2000)
- involves MCP, PIP, wrist; NOT DIP or first CMC
Treatment:
- NSAIDS
- glucocorticoids
- disease-modifying agents --> methotrexate, sulfasalazine, hydrochloroquine, leflunodmide
- biologic agents --> TNF-alpha inibitors
OA vs RA
Gout
Findings:
Crystal appearance:
Symptoms:
Treatment:
Findings:
- acute inflammatory monoarthritis caused by precipitation of monosodium urate cyrstals in the joints
- more common in males
- associated with hyperuricemia
- hyperuricemia can be due to
1. under excretion of uric acid (90% patients) - this is largely idiopathic but can be exacerbated by certain medications
2. over production of uric acid (10%) - seen with Lesch-Nyhan syndrome, PRPP excess, increased cell turnover (ie: tumor lysis syndrome), von Gierke disease
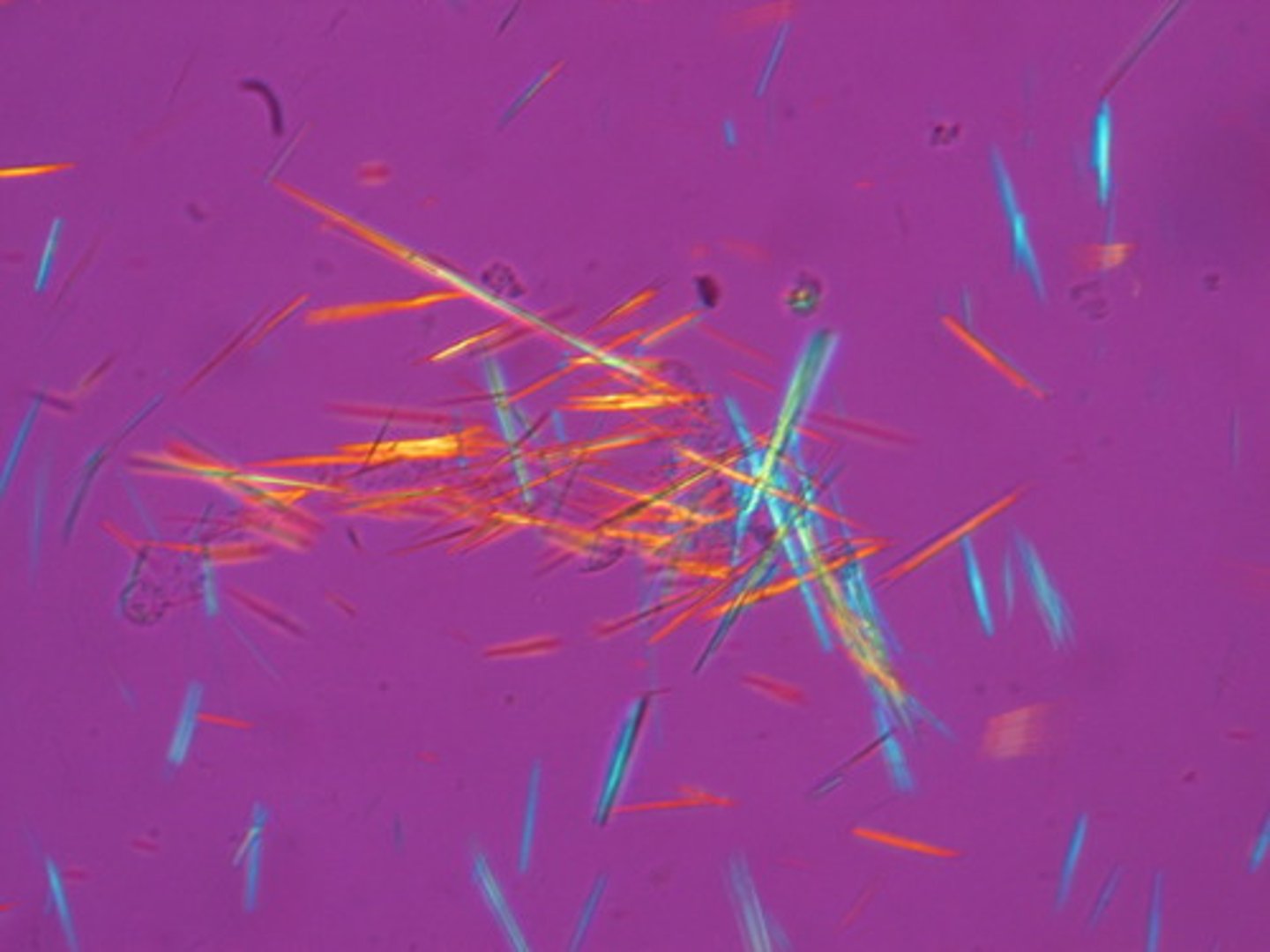
Crystal appearance:
- needle shaped
- negative birefringent under polarized light (yeLLow under paraLLel light; blue under perpendicular light)
Symptoms:
- asymmetric joint distribution
- swollen, red, painful joint
- classically MTP joint of the big toe (podagra)
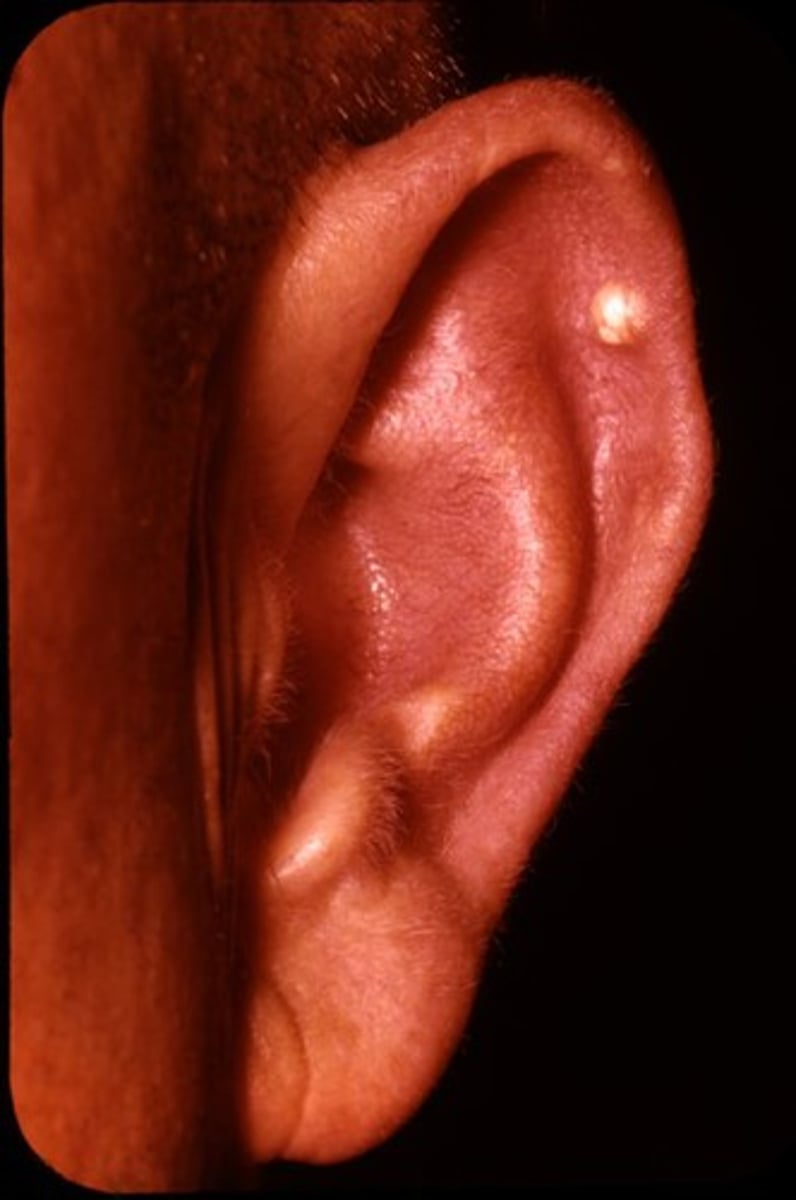
- tophus (a deposit of crystalline uric acid and other substances at the surface of joints or in skin or cartilage, typically as a feature of gout) formation often on external ear, olecranon bursa or achilles tendon
- acute attack tends to occur after a large meal or alcohol consumption
Treatment:
- acute: NSAIDS (indomethacin), glucocorticoids, colchicine
- chronic (preventative): xanthine oxidase inhibitors (ie: allopurinol, febuxostat)
Tophus
a deposit of crystalline uric acid and other substances at the surface of joints or in skin or cartilage, typically as a feature of gout) formation often on external ear, olecranon bursa or achilles tendon
Why do acute gout attack tend to occur after alcohol consumption?
Why do acute gout attack tend to occur after alcohol consumption?
- alcohol metabolites complete for the same excretion site in the kidneys as uric acid --> this decreased the amount of uric acid being secreted, leading to build up in blood
Calcium Pyrophosphate Deposition Disease
What is it?
Findings:
Crystal appearance:
Treatment/PPX:
What is it?
- deposition of calcium pyrophosphate crystals within the joint space
- occurs in patients > 50 years old, both sexes affected equally
- usually idiopathic, sometimes associated with hemochromatosis, hyperparathyroidism, joint trauma
Findings:
- pain and swelling with acute inflammation (pseudogout) and/or chronic degeneration (pseudoarthritis)
- knee is the most commonly affected joint
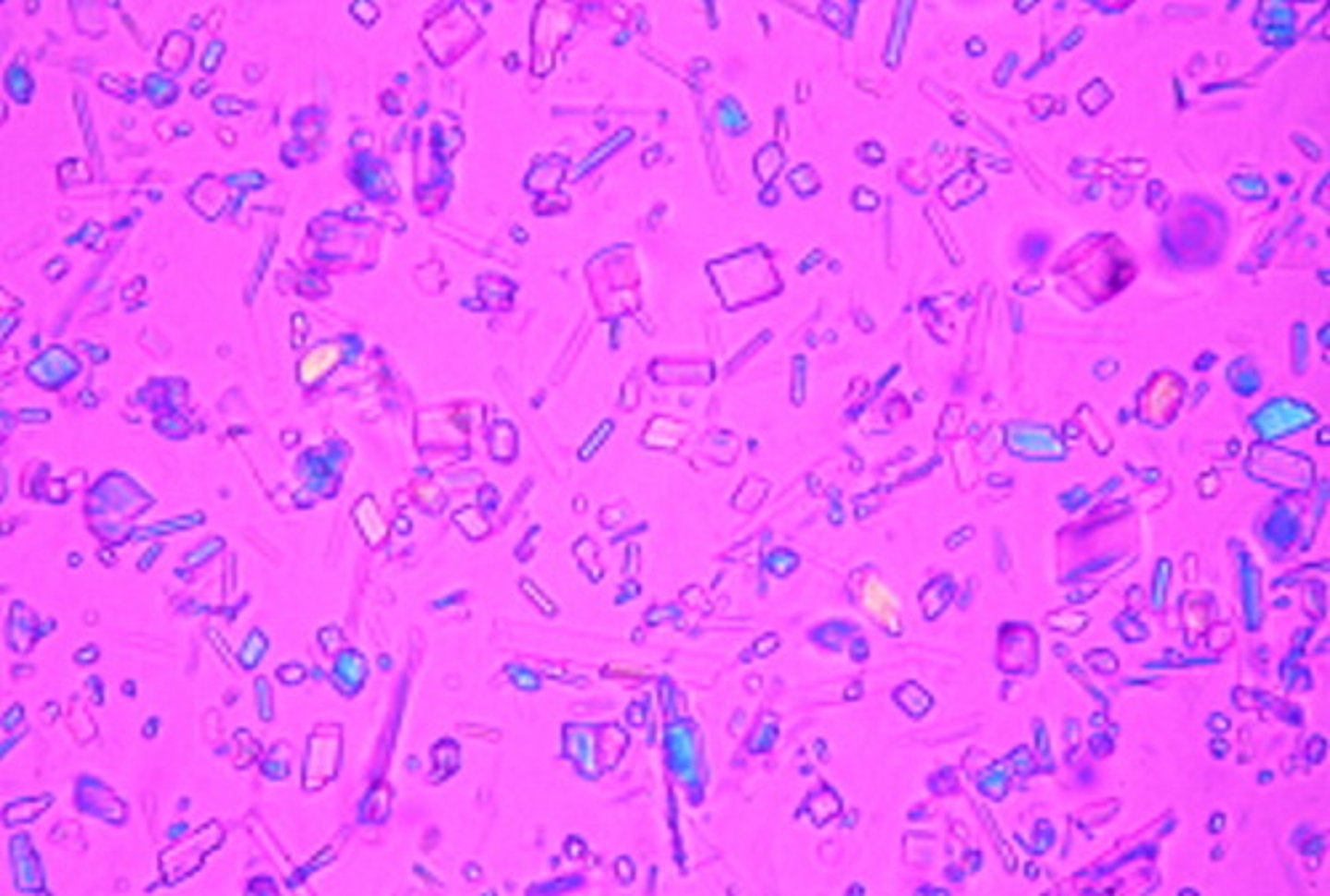
Crystal appearance:
- crystals are RHOMBOID and weakly positively birefringent under polarized light (blue when parallel to light)
Treatment/PPX:
acute rx: NSAIDS, colchicine, glucocorticoids
ppx: colchicine
Sjogren Syndrome
What is it?
Epi?
Findings?
Associated Antibodies?
Complications?
What is it?
- autoimmune disease characterized by destruction of exocrine glands (especially lacrimal and salivary) by lymphocytic infiltrates
- can be primary or secondary with other autoimmune diseases
Epi?
- predominantly affects females 40-60 years old
Findings?
- inflammatory joint pain
- keratoconjunctivitis sicca (decreased tear production and subsequent corneal damage)
- xerostomia (decreased saliva production)
- bilateral parotid enlargment
Associated Antibodies?
- anti-nuclear antibodies --> SS-A (anti-RO) and SS-B (anti-LA)
Complications?
- dental caries
- mucosa associated lymphoid tissue lymphoma (may present as parotid enlargement)
Septic Arthritis
Common causative organisms?
Findings and synovial fluid?
What is the presentation of gonococcal arthritis?
Common causative organisms?
- s aureus
- streptococcus
- n gonorrhea
Findings and synovial fluid?
- affected joint is swollen, red and painful
- synovial fluid purulent (WBC > 50K)
What is the presentation of gonococcal arthritis?
- STI that presents as either purulent arthritis (ie: knee) or triad of polyarthalgias, tenosynovitis (ie: hand), dermatitis (pustules)
What is the definition of the seronegative spondyloarthropathies?
What is the serotype associated with them?
What are the subtypes and what are their common findings?
What is the definition of the seronegative spondyloarthropathies?
- arthritis without rheumatoid factor (no anti-IgG antibody)
What is the serotype associated with them?
- strong association with HLA-B27 (MHC class I serotype)
What are the subtypes?
- remember PAIR
Psoriatic arthritis, Ankylosing Spondylitis, Inflammatory bowel disease, Reactive Arthritis
What are their common findings?
- variable occurrence of inflammatory back pain (morning stiffness, improves with exercise)
- peripheral arthritis
- enthesisits (inflammation insertion sites of tendons, ie: Achilles)
- dactylitis (sausage fingers)
- uveitis
Psoriatic arthritis
What is it?
Findings?
What is it?
- one of the seronegative spondyloarthropathies (PAIN)
- associated with HLA B27
- seen in less than 1/3 psoriasis patients
Findings?
- skin psoriasis and nail lesions
- asymmetric and patchy involvement
- dactylitis and "pencil in cup" deformity of DIP on xray
Ankylosing spondylitis
What is it?
Findings?
What is it?
- one of the seronegative spondyloarthropathies (PAIN)
- associated with HLA B27
- more common in males (young, 20s)
Findings?
- symmetric involvement of spine and sacroiliac joints --> ankylosis (joint fusion), uveitis, aortic regurgitation
- bamboo spine (vertebral fusion)
IBD
What is it?
Findings?
What is it?
- one of the seronegative spondyloarthropathies (PAIN)
- associated with HLA B27
- more common in males (young, 20s)
Findings?
- Crohns or UC
Reactive Arthritis
What is it?
Findings? (classic triad)
Follows what kind of infections?
What is it?
- one of the seronegative spondyloarthropathies (PAIN)
- associated with HLA B27
- formerly known as Reiter syndrome
Findings?
- classic triad of --> conjunctivitis, urethritis, arthritis
- "Can't See, Can't Pee, Can't Bend my knee"
Follows what kind of infections?
- Post-GI (Shigella, Salmonella, Yersinia, Campylobacter) or Chlamydia infections
Systemic Lupus Erythematosus
Presentation:
Epi:
Findings (antibodies)
Treatment:
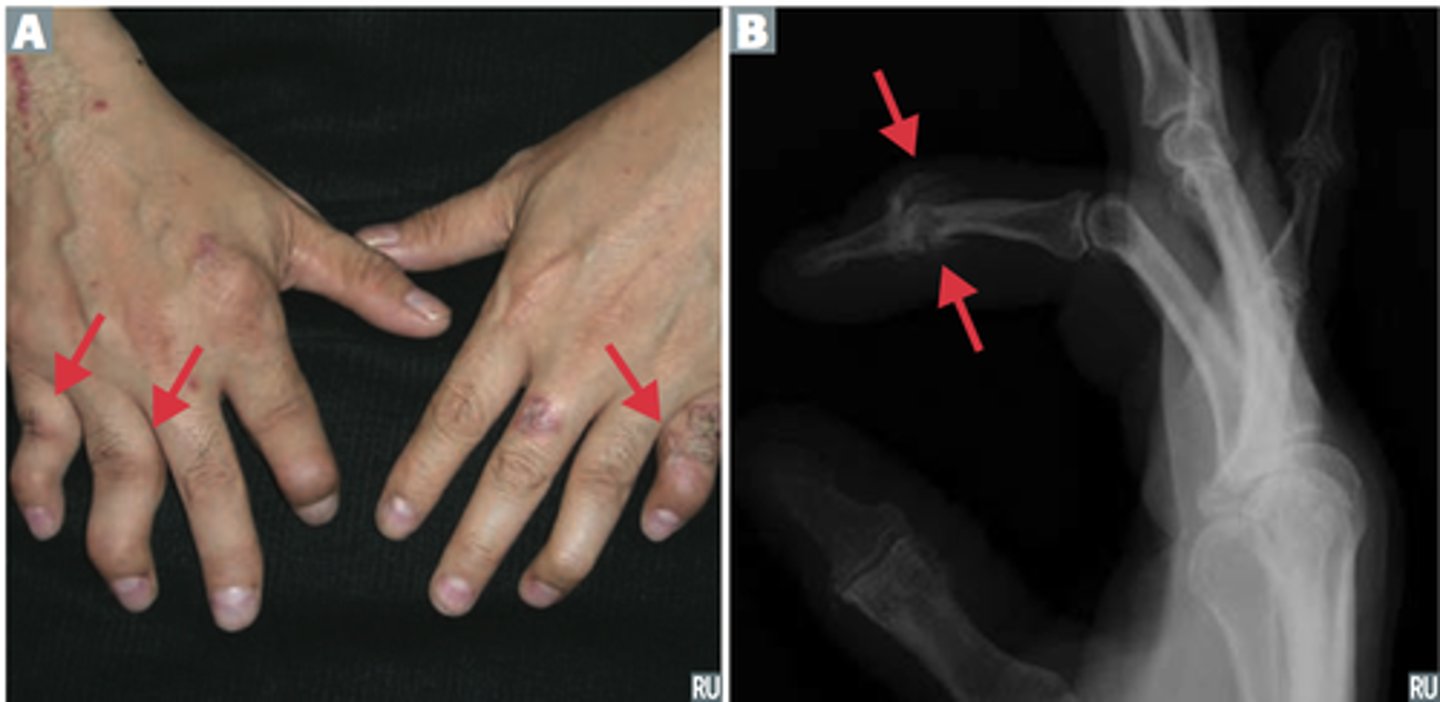
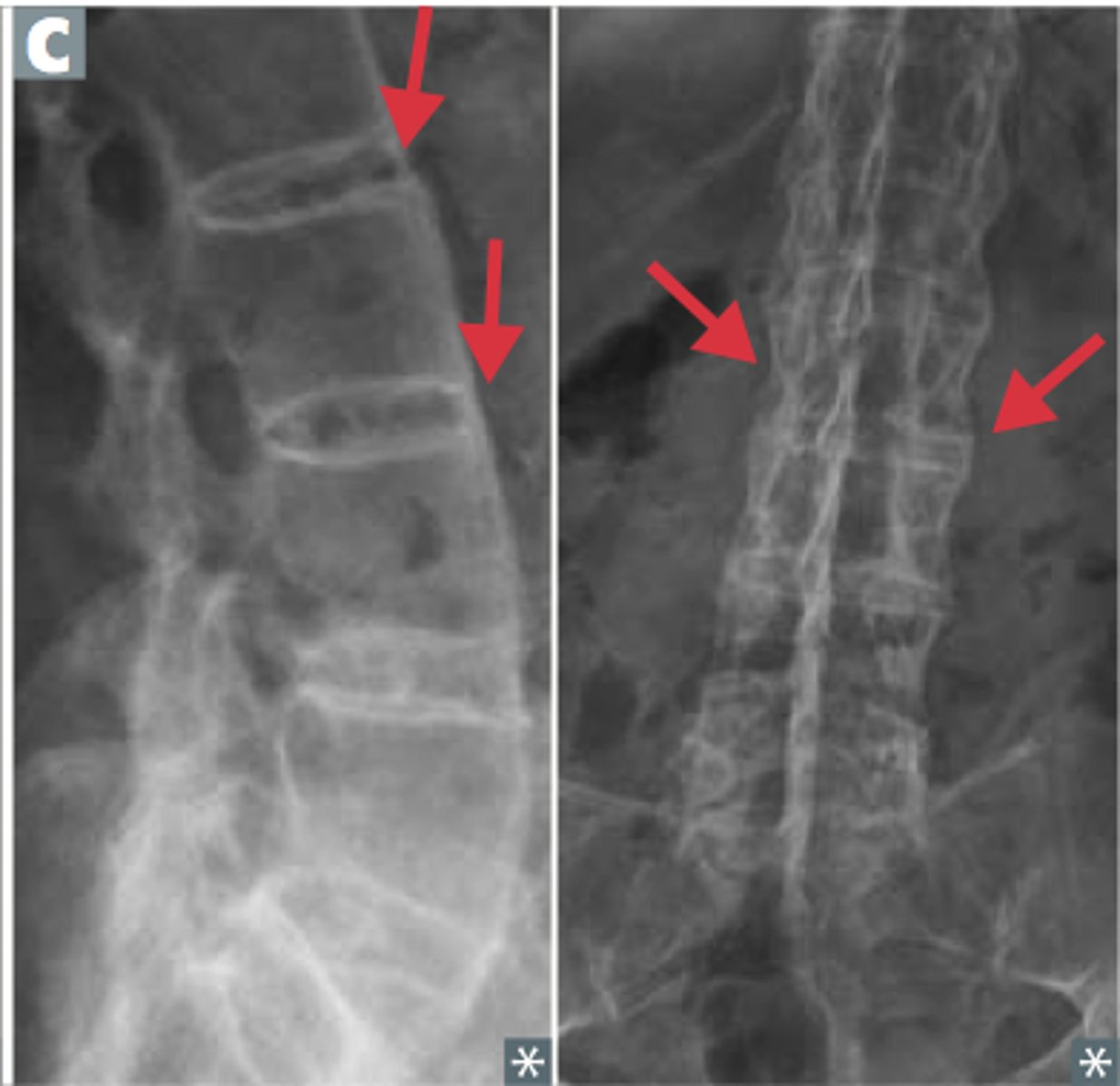
Presentation: remember RASH OR PAIN
Rash (malar or discoid)
Arthritis (non-erosive)
Serositis
Hematologic disorders (cytopenias)
Oral/nasopharyngeal ulcers
Renal disease
Photosensitivity
Anti-nuclear antibodies
Immunologic disease (Anti-ds DNA, anti-Smith, antiphospholipid)
Neurologic disorders (seizures, psychosis)
Treatment:
- NSAIDS, steroids, immunosuppressants, hydrochloroquine
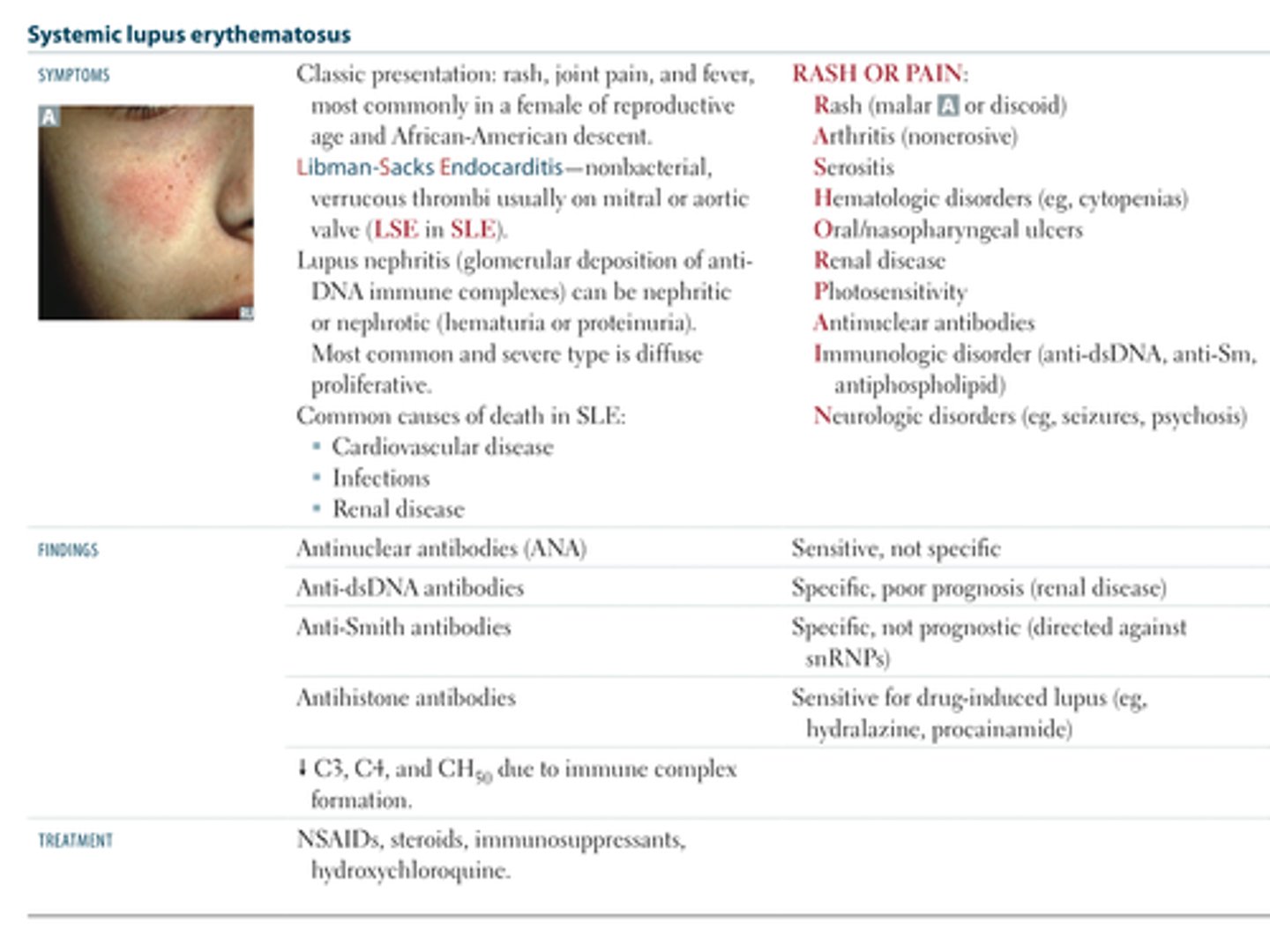
Most common causes of death in SLE?
Cardiovascular disease
Infection
Renal disease
What is Libman-Sacks Endocarditis?
What is Libman-Sacks Endocarditis?
- non-bacterial, verrucous thrombi usually on the mitral or aortic valve (LSE in SLE)
- see in SLE!
What is serositis?
Serositis refers to inflammation of the serous tissues of the body, the tissues lining the lungs (pleura), heart (pericardium), and the inner lining of the abdomen (peritoneum) and organs within. It is commonly found with fat wrapping or creeping fat