Cardio Exam 1: Yang
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
_______ (CHDs) arise from the abnormal formation of the heart or major blood vessels. (most popular with pediatric patients)
At least 21 specific anatomic or hemodynamic lesions have been identified.
Many infants have _______.
~25% require invasive treatment during the _______
Associated with significant morbidities (e.g arrhythmias, infective endocarditis, thrombotic disorder, congestive HF).
Infants _______
Account for almost 50% of the deaths associated with CHD
Congenital heart diseases, more than 1 lesion, 1st year of life, <1 y/o
Acyanotic (PINK → adequate oxygen supply (_______%, not all blood goes to systemic), but not optimal) KNOW!!
_______ (_______)
_______ (_______)
_______ (_______)
_______ (_______)
Cyanotic (BLUE → not enough sufficient oxygen supply (<_______%))
Transposition of Great Arteries (TGA)
Hypoplastic Left Heart Syndrome (HLHS)
Tetralogy of Fallot (ToF or Tet)
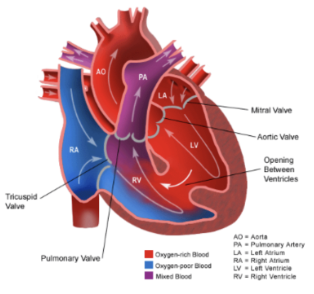
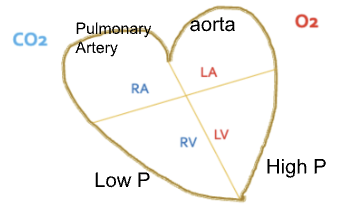
LV → _______ pressure (than RV) → aorta
High pressure (_______) → Low pressure (_______)
85-90, Atrial Septal Defect, ASD, Ventricular Septal Defect, VSD, Coarctation of Aorta, CoA, Patent Ductus Arteriosus, PDA, 60, higher, LV, RV
Which is this?
Acyanotic CHD: Ventricular Septal Defect (VSD)
Which is this?
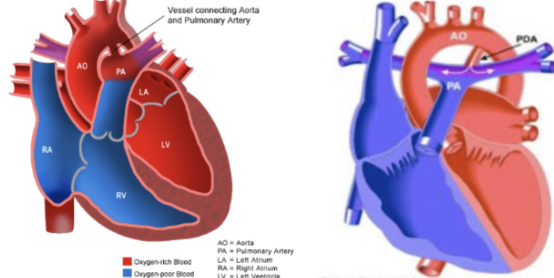
Acyanotic CHD: Patent Ductus Arteriosus (PDA)
Patent Ductus Arteriosis (PDA)
PDA in term infants is reported to be _______ live births and around 5%-10% of all CHDs.
Female:male = _______
Much _______ rate in pre-term neonates (_______)
Ductus Arteriosus
Fetus: allows blood _______
Oxygen exchange through _______ (_______)
After birth (KNOW):
In response to _______ and _______, the newborn ductus will functionally close during the first few days after delivery.
Closed about _______ after birth with permanent destruction at about _______
PVR drops
1 in 2000, 2:1, higher, 37 weeks, bypass lungs, placenta, mother, increased O2, removal of placental prostaglandins, 96 hours, 2 weeks
Patent Ductus Arteriosis (PDA)
What if DA is not closed?
PDA
_______
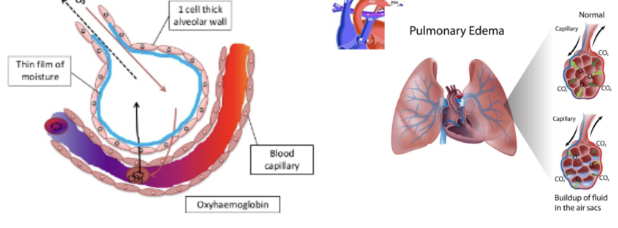
Aorta PA and lungs pulmonary over-circulation pulmonary edema reduced gas exchange reduced oxygenation
_______
Pulmonary _______ and _______
Acyanotic Left-to-Right Shunt, Increasing pulmonary blood flow, HTN/edema, CHF
Patent Ductus Arteriosis (PDA)
Why is PDA not closed?
_______ infants
Ductal tissue _______ respond to high levels of circulating _______ like term _______ does.
Genomic/family history??
Family history is a predictor of _______
Spontaneous preterm birth in the current pregnancy was significantly associated with a maternal family history of preterm birth among female relatives within 3 generations and notably sisters.
Am J Obstet Gynecol MFM, 2021
No consistent conclusions
_______
Being born at a high altitude.
Premature, does not, oxygen postpartum, newborn, current preterm birth, female sex
Closure of PDA → _______ (_______) + _______ (_______)
_______: push or pull (a train or part of a train) from the main line to a siding or from one track to another.
increases O2, Ventilator, decreases prostaglandins, NSAID, Shunt
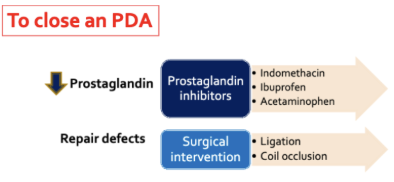
KNOW IMAGE
Indomethicin
MOA: Decrease prostaglandins through _______ of _______
Dose: Based on _______ age at time of _______ and _______ after _______
Indication
Landmark Clinical Study in Premature Infants:
__% of patients achieved ductal closure.
Patients receiving indomethacin experienced significantly _______ episodes and _______
Given _______ (_______)
reversible inhibition, COX-1 and COX-2, postnatal, 1st dose, urine output, 1st dose, 79, more bleeding, increasing SCr, IV, 3-dose series
Ibuprofen
MOA: Decrease prostaglandins through _______ of _______
DOC
Based on birth weight
_______ age ≤ _______ (_______ at birth)
___ mg/kg/dose IV, followed by ___ mg/kg/dose IV _______ and _______ (_______→ if closure didn’t work, then _______ → if not, then _______)
Oral solution: ___ mg/ml; _______ solution: ___ mg/ml or _______
Indication
_______
As effective as indomethacin
Reduced risk of necrotizing enterocolitis and transient renal insufficiency
Contraindication
Do NOT initiate ibuprofen for ductal closure with _______
If DA does not close or reopen after the initial course, a second course may be considered versus indomethacin or surgical closure.
_______ ibuprofen: at least as effective as _______ administration
Reversible inhibition, COX-1 and COX-2, Gestational, 32 weeks, 500-1500 g, 10, 5, 24 hours, 48 hours after 1st dose, 3-dose course, do another 3-dose course, surgical closure, 20, IV, 10, PO, drug of choice for the closure of PDA, renal impairment, Enteral, IV
Acetaminophen
MOA: Decrease prostaglandins through _______ of _______
Indication
FDA approves _______ of acetaminophen in 2010
_______ risk
Ok for _______ patients
_______
Ofirmev
Suggest that acetaminophen is an _______ to ibuprofen or indomethacin
reversible inhibition, COX-1 and COX-2, IV formulation, reduced GI bleeding, renal insufficient, expensive, alternative
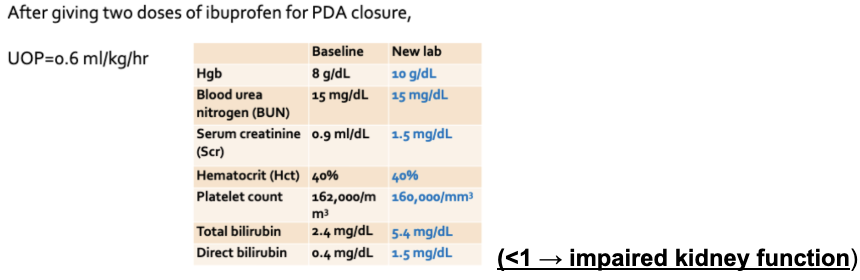
What’s the C/I of Ibuprofen for PDA treatment?
Severe _______ impairment
What’s the C/I of Acetaminophen for PDA treatment
Severe _______ impairment
renal, hepatic
Patient Case:
C.P. is a 25-weeks post-conceptional age baby boy (current body weight=680 g) who remains ventilator-dependent. He was born at 24 weeks gestational age with a birth weight of 650 g.
He has a continuous murmur and bounding peripheral pulse, and his chest radiography shows evidence of pulmonary over-circulation with mild cardiomegaly consistent with patent ductus arteriosus (PDA).
He has no evidence of intra-ventricular hemorrhage on cranial ultrasonography
For patient CP, what would you recommend for his PDA management?
Requires _______ (requires _______)
Urine output during the past 24 hours was 4 ML/kg/hr. As a clinical pharmacist, which is the best treatment option for CP at this time?
Give _______ 6.5 mg followed by 3.3 mg at _______ after the 1st dose (USE: _______)
Before starting PDA treatment, you noticed the patient’s urine output during the past 24 hours was reduced from 1.4 mL/kg/hr. As a clinical pharmacist, which is the best treatment option for CP at this time? (urine output >1 mL)
Give _______ 6.5 mg _______ depending on the _______ after the 1st dose
pharmacological closure, ventilator, IV ibuprofen, 24 and 48 hours, 10 mg/kg, IV ibuprofen, 1st with holding the 2nd and 3rd doses, urine output
As a clinical pharmacist, which is the best treatment option for CP at this time?
_______ + _______
Need further workup + assess the patients _______ before making a recommendation
hold ibuprofen, start IV APAP, liver function
_______ is the DOC (Drug of Choice); less _______ toxicity compared to indomethacin
Indomethacin + Ibuprofen (_______)
If anuria or marked oliguria (urinary output < ___ ml/kg/hr) is evident at the scheduled time of the _______ dose, _______ until renal function returns to normal.
C/I in _______ with significant _______.
Ibuprofen, renal, kidney impairment, 0.6, 2nd or 3rd, hold dose, preterm infants, renal impairment
T/F: Closing PDA is always beneficial for patients with CHD
False
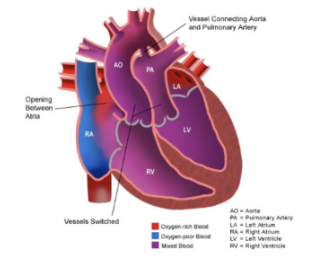
What is this?
Cyanotic CHD: Transposition of Great Arteries (TGA)