paeds Periop med - clinical
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
Define and use terms that describe paediatric age and development
Motor = includes fine (picking up obejcts) and gross (walking)
Language = ability to understand precedes speak, even before 18/12 kids can listen and understand story
Cognitive = intellectual maturation of the child, appropriate attachments
Behaviour / emotion = temperament and mood
Outline the implications of the developmental stage of children for their anaesthetic care
Stress of hospital split into 5 fears
Effects post op
In kids, stress of hospitalization has been related to 5 general fears:
Fear of separation from their parents
Fear of the strange hospital environment
Fear of painful procedures
Fear of the operation itself
Fear of anaesthesia
After a stormy siju induction there can be behavioural changes pr regression in developmental milestones
Anxiety
Enuresis
Night crying
Tantrums
Can persist for 1 year post
Greatest in pre-school age
Strategies to deal with kids depend upon age group
Infants
Less than 9 months less likely to have sep anx
1-3 years
SEP ANX
Parent present
Distract
3-6 years
Concerns about bodily MUTILATION
7-12 years
EXPLANATION AND PARTICIPATION
They need control
Adolescence
Increased body awareness, independence and need for privacy
Give them a sense of control as much as possible
Discuss the clinical features and implications for anaesthetic care of the following medical conditions
starting with clinical features
Prematurity
Resp
CVS
CNS
Endo
GIT
delivery of a viable newborn >20 weeks and before full term
Resp
Resp distress syndrome
No T2 pnumocytes - begin after 22/40
No surfactant → atelectasis, decreased compliance
Tachypnoea, nasal flare, grunting, chest wall retraction, access muscle usage, hypoxemia, hypercap, met acidosis
Mx - Steroid prior to delivery
Suppl O2 for PaO2 55-70 and CPAP
Intraop
AVOID hypoxemia
AVOID high FiO2
AVOID high mean airway presures
PEEP 3-5
RR 30-50
APNOEA
Cessation of breathing > 20 seconds or less time if also brady or hypoxemia
V COMMON - resolves usually by 52 weeks post conception
Central - lack of resp effort
Obstructive - OSA from tonsils
CVS
PDA
Common finding in preterm kids with resp disease
In normal newborns closes within first few days of life (due to raised PaO2 and decreased prostaglandins)
LEFT to RIGHT shunt (Ao → PA)
Can be closed by Indomethacin or surgery
Anaemia of prem
due to reduced production of EPO
Tx with EPO or observation
CNS
Intraventricular hamorrhage
spont bleed into and around lat ventricles due to fragile blood vessels → neuro changes; hypotonia, seizures, apnoea, loss of sucking reflex, bulging fontanelle
If severe can lead to cavitary cysts → strong predictor of cerebral palsy in later life
Retinopathy of prem
due to VC of retinal vessels before their full maturation and growth
RFs - LBW, prolonged O2 exposure, mech vent, bacteraemia
Endo
Hypoglycaemia
glycogen is accum in fetal liver in third trimester, therefore prem infants are at risk of hypo
Prolonged hypo → severe nerurodev defecit so tx aggressively with BSL < 5
GIT
Feeding diffculty
Jaundice
Anaesthetic considerations of prem
Airway
Small airway, small equipment
Generally intubated and ventilated for procedures to reduce WOB
Breathing
Apnoeas especially in prematurity (see card)
Biphasic response to hypoxia with hyperventilation and then apnoea
Quick desaturation (increased O2 consumption, CC > FRC)
Possible lung disease (increased risk with prematurity)
Neonatal respiratory distress syndrome (especially if < 32 weeks)
Deficient surfactant, exudate forms hyaline membrane
Begins within 4 hours of birth
Decreased compliance, atelectasis, V/Q mismatch
Ground glass appearance on CXR and air bronchograms
Treatment with O2 (minimize), surfactant, CPAP
Bronchopulmonary dysplasia – see card
O2 toxicity → Retinopathy of prematurity
Most common <32 weeks or low birth weight <1.5kg
Fatigueable diaphragm
Circulation
HR dependent CO (200mL/kg versus 70mL/kg in adult)
Due to noncompliant ventricle and 2x basal metabolic rate
Difficulty increasing CO much further in illness
Reversion to fetal circulation
May be caused by ↑ PVR (e.g. hypoxia) and/or ↓ SVR (e.g. sepsis).
Increased incidence of PDA
Contractility dependent on extracellular Ca concentration
Poorly developed SNS
Unable to increase SVR due to poorly developed SNS
Prone to bradycardia due to PNS predominance
Bradycardia in response to hypoxia
Persistent pulmonary hypertension of prematurity
PDA - care with bubbles and monitor pre and post ductal sats
Thermoregulation
Hypothermia (see card for prevention)
Immature thermoreg, prone to loss, difficulty generating heat
Strict environmental temperature control, warm blanket and warm fluids & HME
Thermoneutral environment ~34°C
Metabolic
Hypoglycaemia
Limited glycogen stores
Minimise fasting time, unable to suck feed <34 weeks (need NGT)
Glucose requirement = 6-8mg/kg/min
Na requirement = 3 mmol/kg/day
10% glucose is common maintenance
Generally continue what NICU is doing
Haematological
Lower Hb compared to term
High HbF concentration
Aim Hct 40-45%
Coagulation and immunity immature
Renal
Decreased GFR and poor concentrating ability
↓ tubular capacity to reabsorb HCO3- → “Normal” newborn acidosis
Ability to retain Na+ not effective till 32 weeks → Hyponatremia
TBW = 90% of body weight (c.f. 80% at term, 60% at 1 yr)
Gastrointestinal
Decreased hepatic function
NEC
GORD
CNS
Prone to intraventricular haemorrhage (care with surges in BP)
Retinopathy (oxygen)
Lower MAC values than term neonates
ASTHMA
BG
Preop
Intraop
Postop
BG
10% of kids
Most common childhood illness
Triad
Bronchial hyperactivity
Inflamm
Mucous secretion
P/w - dry cough, SOBOE, wheezing
Pre-op
assess severity
control with Rx (number of ED presentations, hospitalization and ICU)
current status
physical exam (looking for use of accessory muscles and prolonged expiratory time)
Sp02 (<96% on room air is bad)
Intra-op
aim to prevent and avoid bronchospasm (usually from ETT)
if can use face mask or LMA do so
if need ETT make sure sufficiently deep
use volatile for bronchodilatation
consider ketamine and consider Mg
Avoid opioids or neuromuscular blockers that cause histamine release
consider deep extubation
Post-op
continue regular asthma treatments
physio
PRN relievers
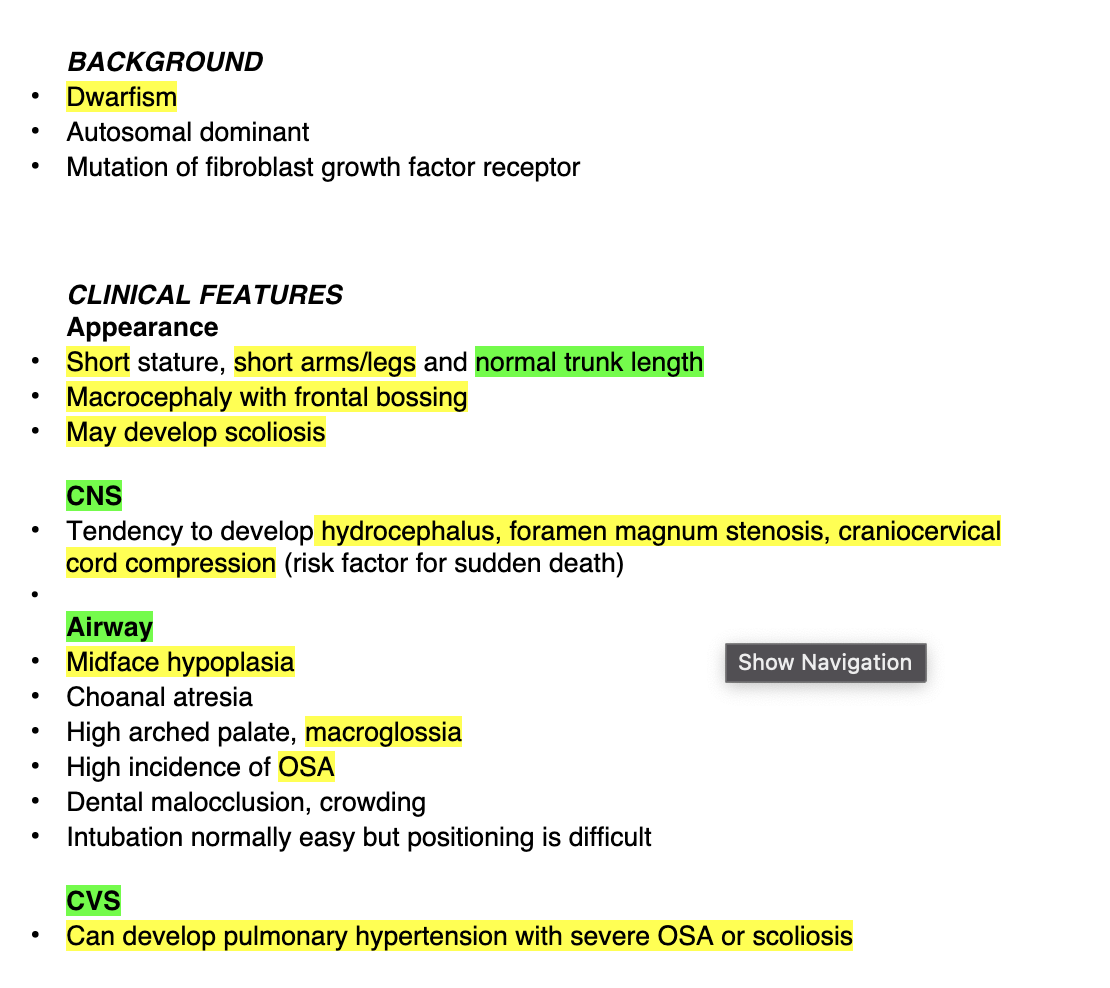
OSA
BG
Pathophys
Clinical features
BG
Cessation of nasal/oral airflow during sleep with preserved resp effort
Prevalance 1 – 3%
Usually results from adenotonsillar hypertrophy
PATH
Enlarged soft tissues
Adenotonsillar hypertrophy (most common in child), macroglossia, obesity
Small bony upper airway
Craniofacial syndromes, Pierre Robin, Down syndrome, achondroplasia
Hypotonia of upper airway
Cerebral palsy, neuromuscular disorders
Clinical features
Failure to thrive, behavioural problems, poor school performance, snoring, restless sleep
Daytime somnolence & obesity uncommon
Snoring is sensitive (91% for OSA) but not specific (75%)
Polycythaemia (chronic hypoxaemia)
Right heart failure and pulmonary hypertension
ECG evidence of Right heart strain: Tall R in V1, Deep S in V6, tall P in II and V1
ECHO
CXR: cardiomegaly
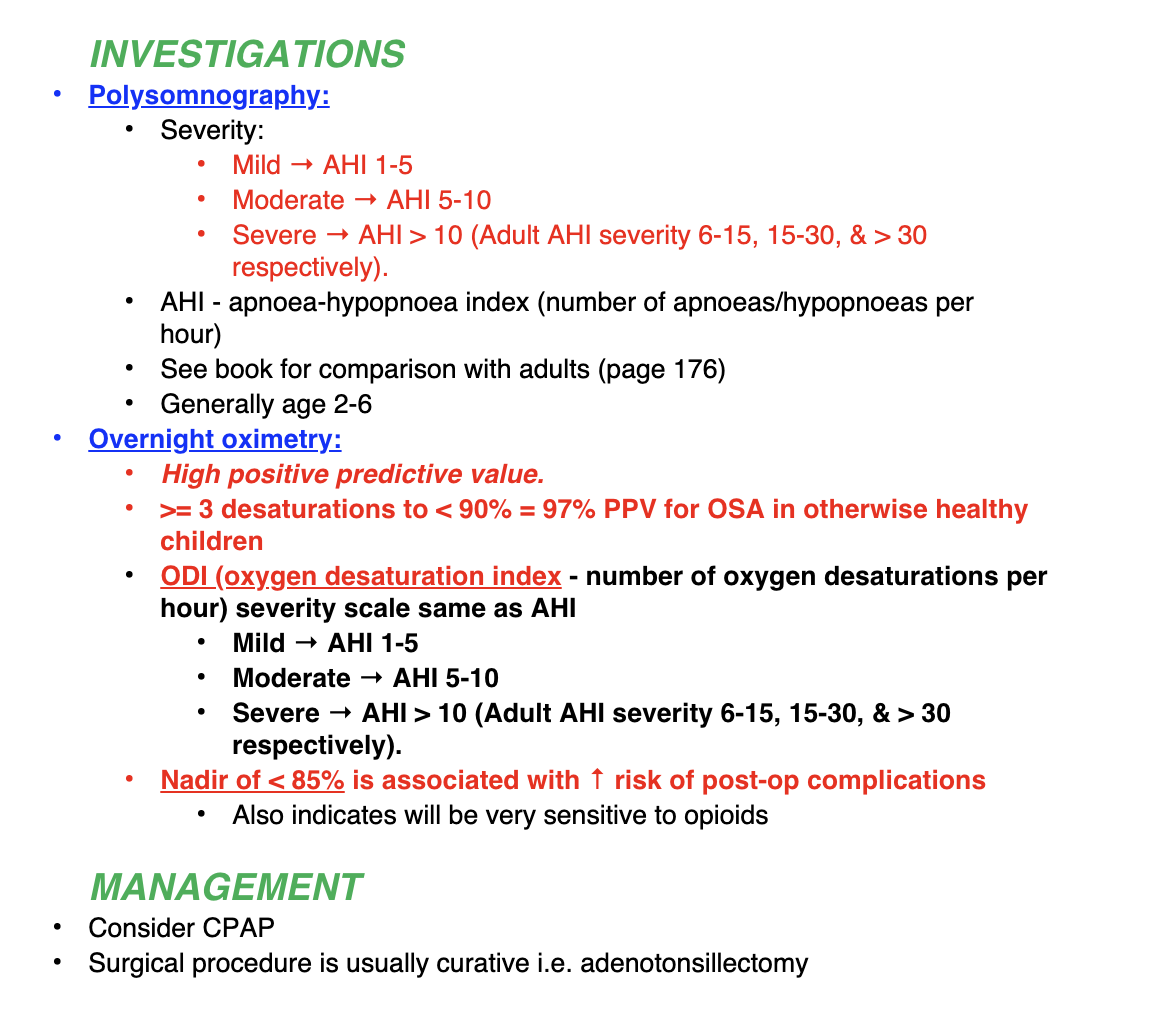
OSA Ix and Mx
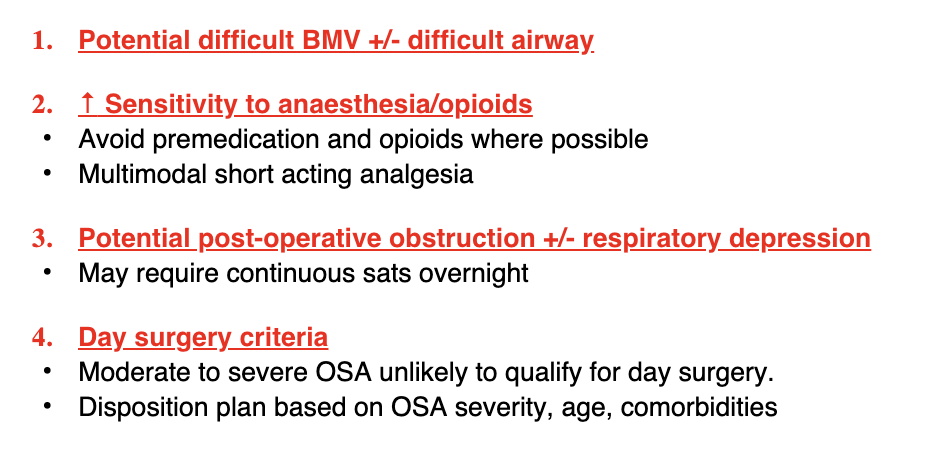
KEY OSA ANAES SAFETY CONCERNS
OSA anaes Mx
Preop
Intraop
Postop
o Pre-op – assess child for severity of OSA and apnoeas at home, assess airway for potential difficulties (obesity or syndromes) and consent parents for likely admission post-op and monitoring if severe OSA
o Intra-op – communicate with surgeon, usually gas induction ETT and throat pack and gag. Kids with OSA will exhibit partial or complete upper airway obstruction on induction – use guedel. Try to minimize sedatives used (avoid pre-med) and minimize long-acting opioids due to risk of post-op apneas (<0.1mg/kg morphine equivalent)
o Post-op – suction oropharynx, remove throat pack, extubate awake in lateral position, oral short acting opioids and anti-emetics PRN only. If severe OSA they should be hospitalized overnight due tendency toward upper airway obstruction during sleep and sedation/GA will worsen this
CYSTIC FIBROSIS
BG
CLINICAL PRES
COMMON PRESENTING SURGERIES
Medical mx
BG
1:3000 live births
Median life expectancy 40 years
Progressive and worsens with age
Most common fetal AR disease of caucasians
Mutation of CFTR on Ch 7 → abnormal Cl transport → VISCID secretions in lung, pancreas, liver, intestine and reproductive tract
CLINICAL PRES
RESP
Copious secretions and mucous plugging
Repeated infections and bronchiectasis, colonisation
Progressive mixed obstructive/restrictive pattern
Severe V/Q inequality even in seemingly well patients
Hypoxaemia leading to PHTN and right heart failure
Nasal polyps and sinusits common
GIT
Pancreatic insufficiency (malabsorption, diabetes, failure to thrive)
Biliary cirrhosis
Hepatic fatty infiltration, cirrhosis, portal hypertension, GORD
Neonates often present with meconium ileus
OTHER
Sweat glands: sweat deficiency, may become hyperthermic
Infertiliy often in males
Osteoporosis and osteoarthritis
COMMON PRESENTING SURGERIES
Bronchoscopy
Venous lines
Nasal polypectomy
Recurrent pneumothorax
Lung transplant
Medical mx
Chest pT
Exercise
Bronchodilation
Aggressive Abx therapy
Neb pulmozyme
Pancreatic enzyme replacement
Fat soluble vitamins
High cal and High protein
CF Anaesthetic implications
Pre
Intra
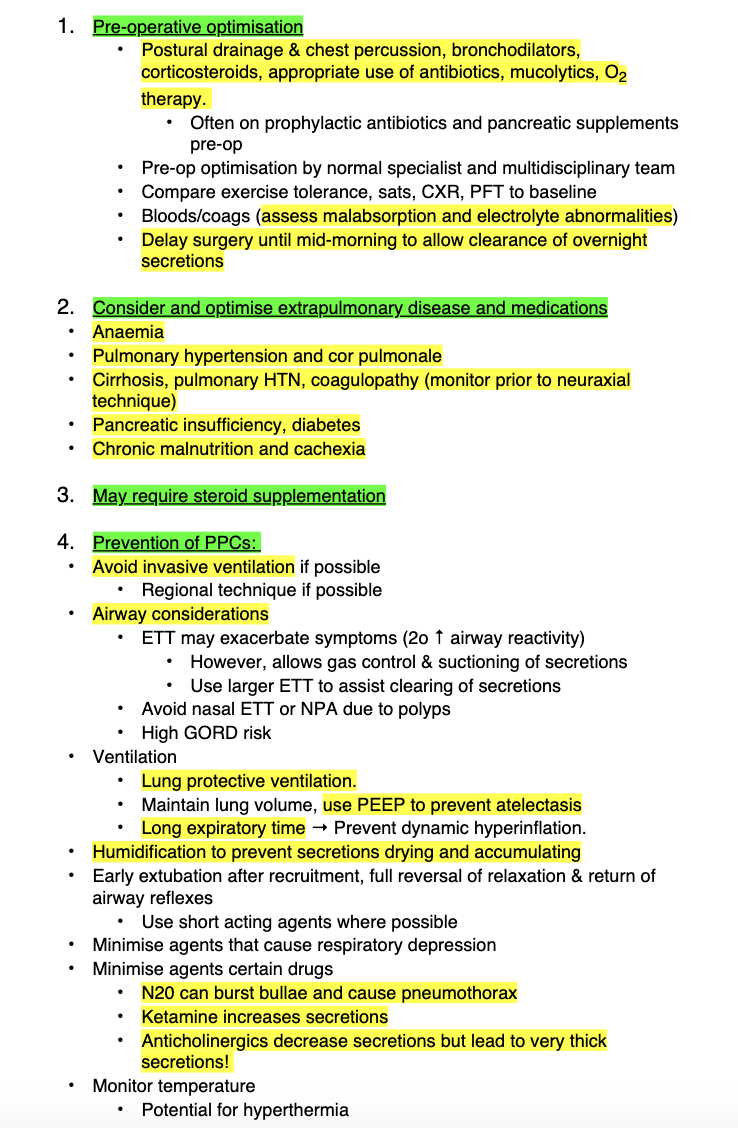
CF
Postop
Physiotherapy +/- NIV
Humidified gases
Excellent pain control to facilitate breathing.
Nutritional status and glucose management
Consider HDU/ICU
Achrondoplasia
BG
CF
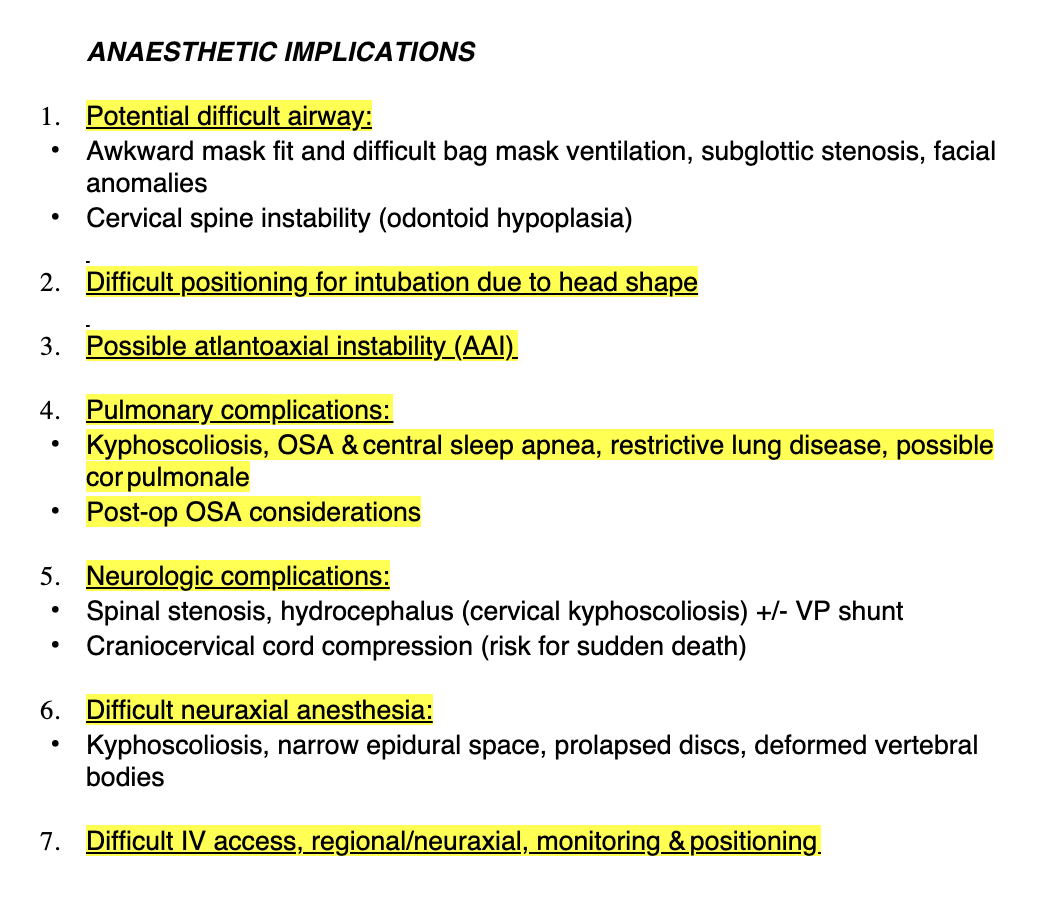
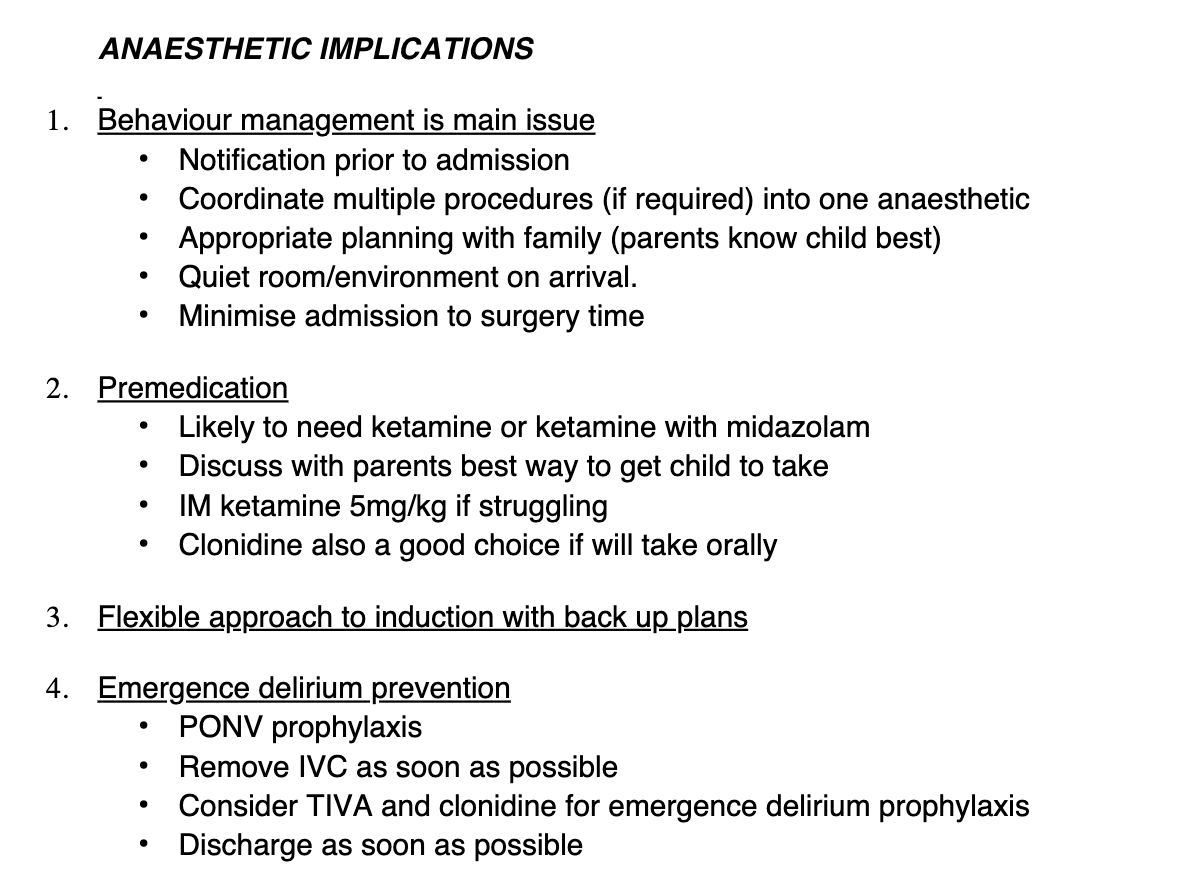
Achrondoplasia anaes implications
AUTISM
BG
Features
BG
ASD = lifelong developmental disability
Males = 4x more common than females
Affects how a person communicates with and relates to other people and the world around them.
Features
Triad of impairments:
Difficulty with social communication
Difficulty with social interaction
Difficulty with social imagination
They may have lower than average IQ or may have normal or high intelligence
They have difficulty seeing another’s perspective
They have a lack of understanding that people’s minds do not hold the same information – explains why they become confused with repeated questioning or a lack of appreciation of their wants or needs
Kids with ASD view the world in a very literal way, they cannot generalize information and have very little imagination or understanding of fantasy or fiction.
Kids with ASD are very reluctant to be touched or examined and may display repetitive patterns of behaviour and become distressed if they can’t do those behaviours. They may have a limited range of preferred food and drinks and be reluctant to make eye contact and be non-verbal or conversely demand repeated complex factual explanations of every stage of the procedure
Anaesthesia and sedation do not present a problem for most kids with ASD, but unpredictable regression in skills and behaviour is noted in a small number of patients after GA
Overall anaesthetic implications ASD
ASD
Preop
Intraop
Postop
PREOP
Limit fasting times
Maintain hydration
Limit crowded areas
Open and clear comms
Premedication - PO clonidine as tasteless
Warn re: emergence delirium
INTRAOP
Gas induction with parent present
Physical restraint last resort in urgent surg
IV access
hydrate, BSL and antiemetic
Deep extubation and propofol at extubation
Liberal use of paracet, NSAID, opioids
POSTOP
Pain assessment may be hard
FLACC score
Parent knowledge of pain behaviour
May not engage with PT
Ideally day case and home asap
CEREBRAL PALSY
BG
BG
Cerebral Palsy is a term covering a group of non-progressive, but often changing, motor impairment syndromes secondary to anomalies in the brain sustained in early development
May be associated with mental impairment and/or epilepsy
Characterized by varying degrees of motor, sensory, & intellectual impairment
Incidence ~1 in 500
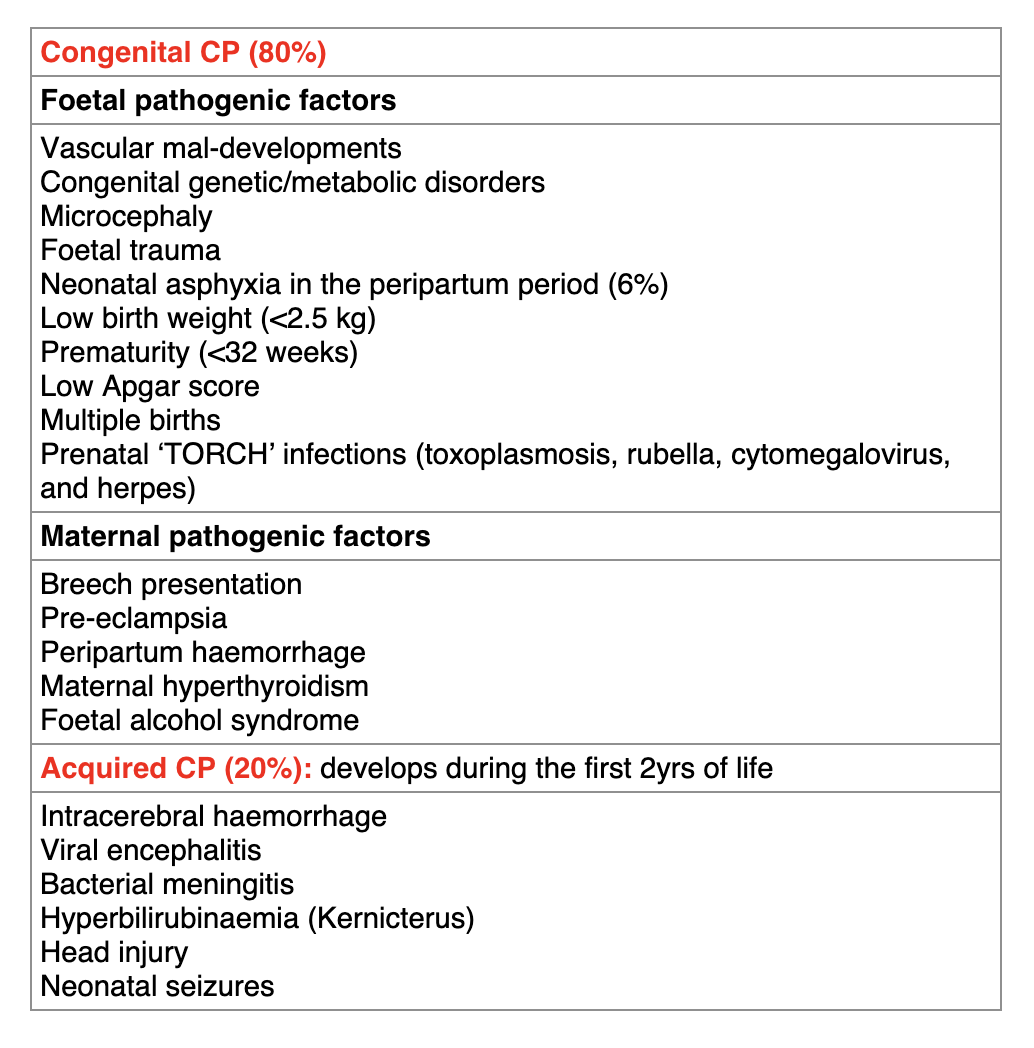
Causes
Caused by pathological insult to developing brain in utero or postnatally
80% occur antenatally
See table
Just briefly
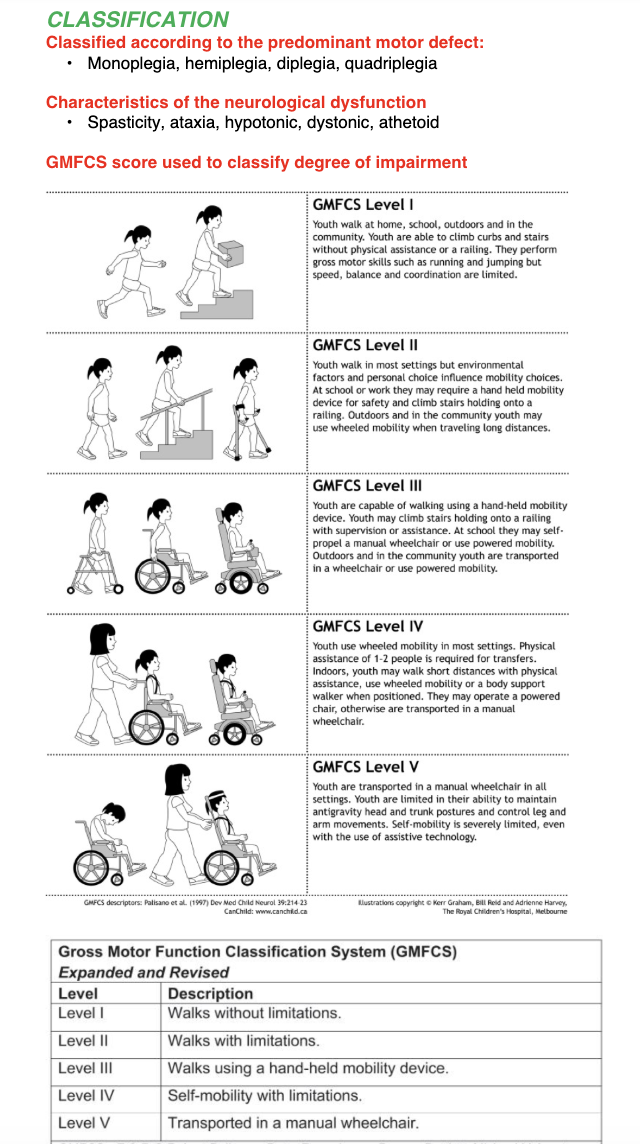
Classified according to
Characteristics of neuro dysfunction
What score is used to classify impairment
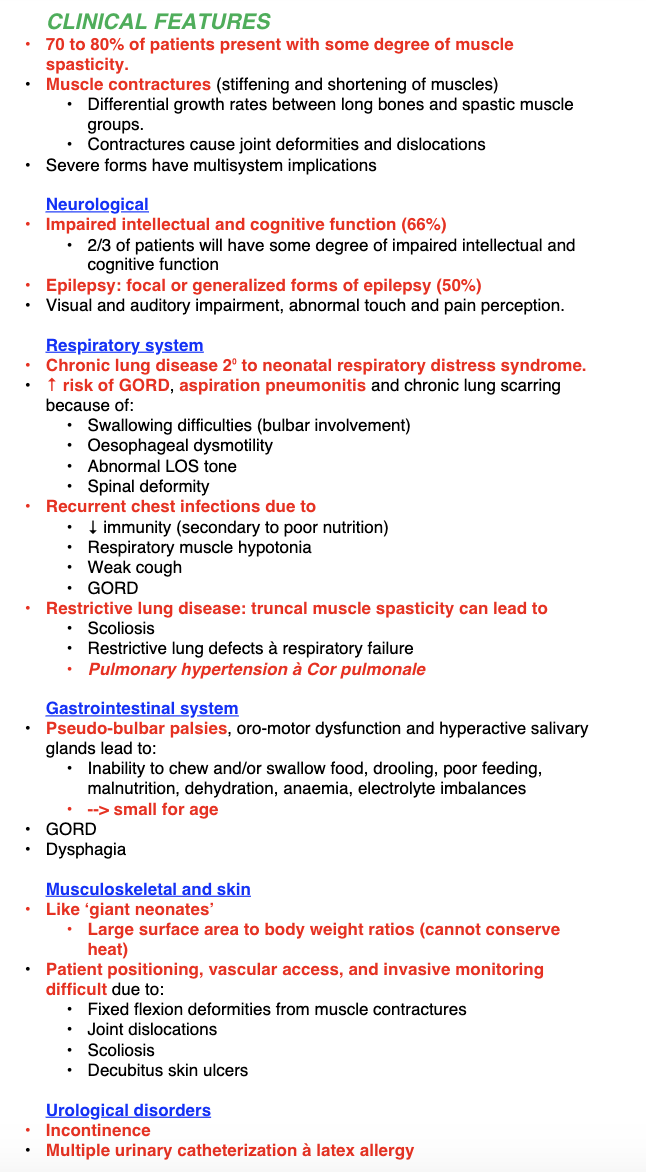
CP Clinical features
Neuro
Resp
GI
MSK
Urol
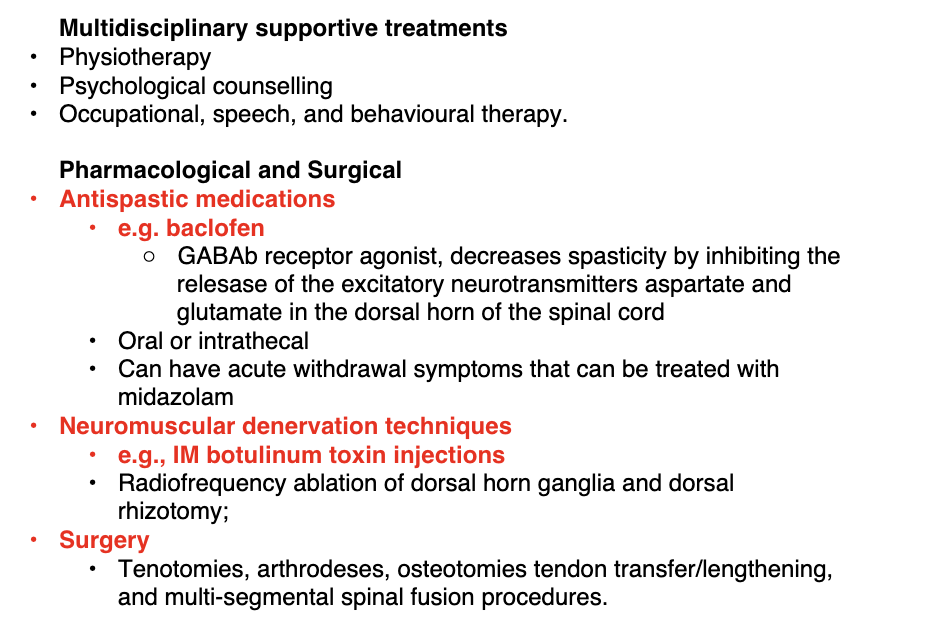
Mx
Aims
Aims
Improve mobility and posture
Min contractures, spasticity anf spasms
Control sx of accomp disorders
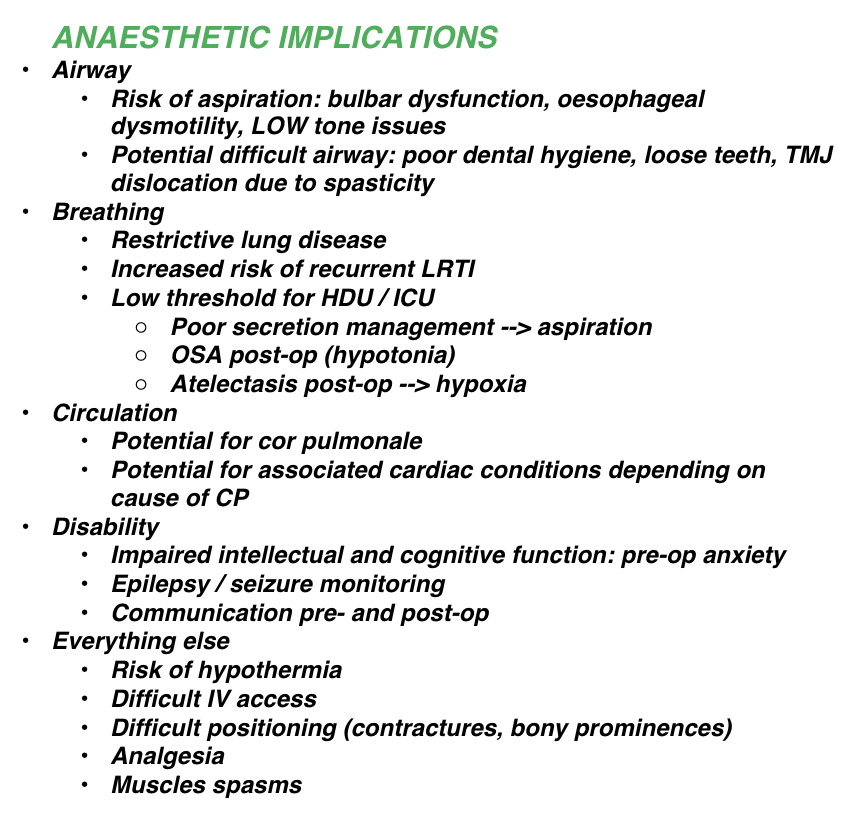
CP Anaesthetic implications
Down Syndrome
MAJOR CONCERNS
BG
CLINICAL Features
Gen
A
B
C
D
Endo
GI
Haem
Immune
OSA
Cardiac defects
Atlantoaxial instability
BG
trisomy 21
1/800
Exponential increase with icreasing maternal age
Antenatal screen with nuchal fold and amniocentesis
CLINICAL FEATURES
General
Small head
Brachycephaly
Upward sloping palpebral fissures
Flat nasal bridge
Short thick neck, macroglossia
Single transverse palmar crease (simian) in both hands 50%
LBW, obesity in childhood
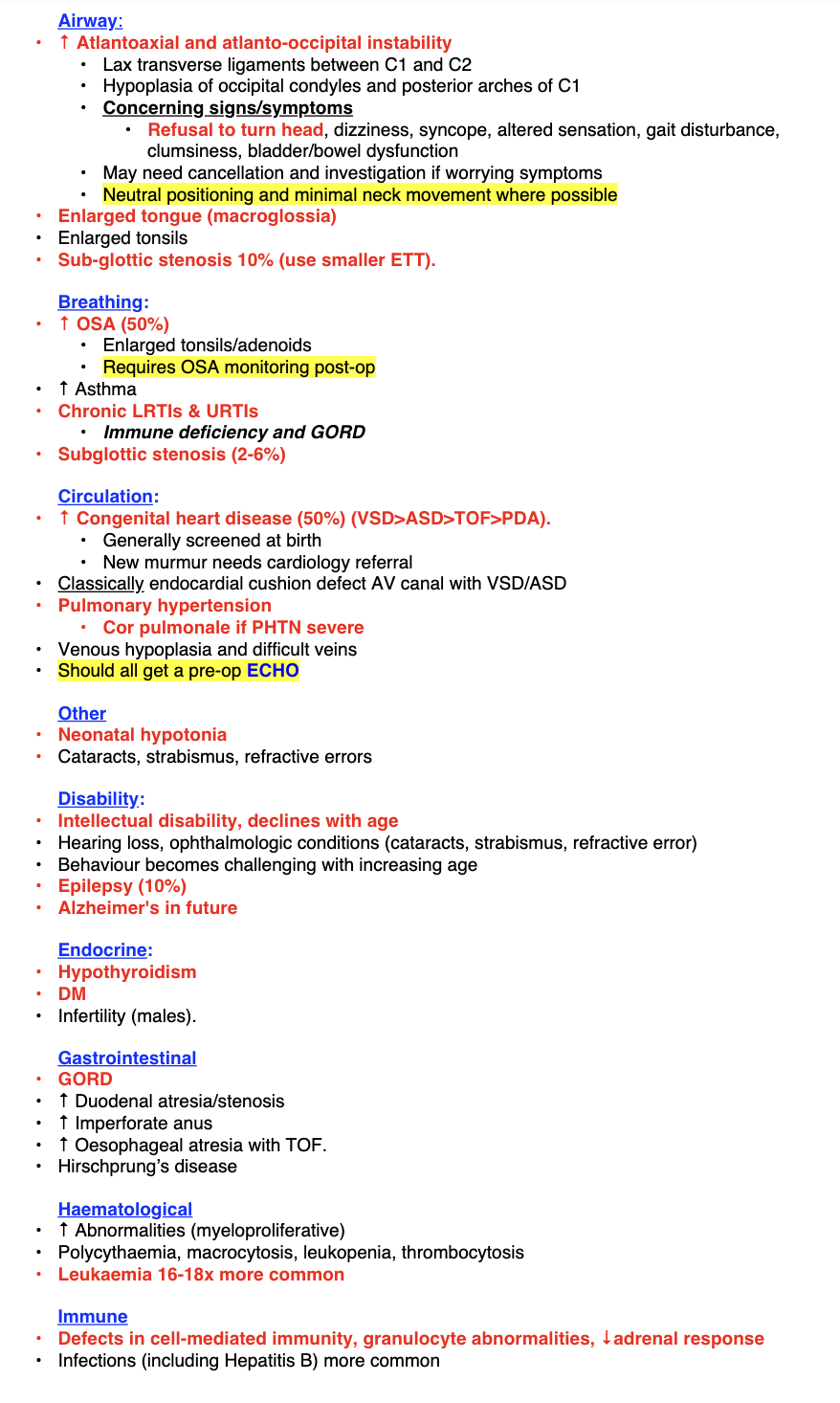
ANAES CONSIDERATIONS IN RESPONSE TO FEATURES
A and B
C
D (CNS)
Other
A and B
OSA
Intubation
Keeping neck neutral
Risk of post op RTI
GORD
C
Cardiac defects
Prone to brady
D
C spine
Neck neutral
E
Immune def - strict asepsis
Other
Difficult IV access
Often anxious
Often emergence delirium
Childhood Obesity
Increased risk of what comorbs
Anaesthetic Implications
Increased risk of
HTN
T2DM
Asthma
OSA
ANAES IMPS
Preop identification
Identify and optimize comorbs
HTN
T2DM
Asthma
OSA
ASPIRATION
DIFF AIRWAY - usually BVM
DIFF IV ACCESS
CROUP
What
Path
Indications for Intubation
What to remember for intubations
WHAT
acute laryngotracheobronchitis
viral infection (parainfluenza, RSV)
occurs in autumn & spring between 6/12 – 2years
characterized by barking cough/hoarseness with profuse secretions and dysphagia
PATH
Larynx, trachea and bronchi are all involved and become oedematous -> stridor, worse with anxiety (trachea can collapse on inspiration)
INDICATIONS FOR INTUBATION
CLINICAL SIGNS
EFFORT - of breathing
EFFICACY - cyanosis is late, desat is pre-terminal
EFFECTS - on other organs - eg. drowsy
PREP FOR TF
NATURAL HX AND ?BACTERIAL OR VIRAL
Most are viral but if bacterial then higher chance needing ETT
RESPONSE TO MEDICATIONS
> 1hr of neb adrenaline
0.5 ml/kg of 1/1000 up to MAX 6 ml
FOR ETT
Remember that sub glottic airway is surprisingly narrow
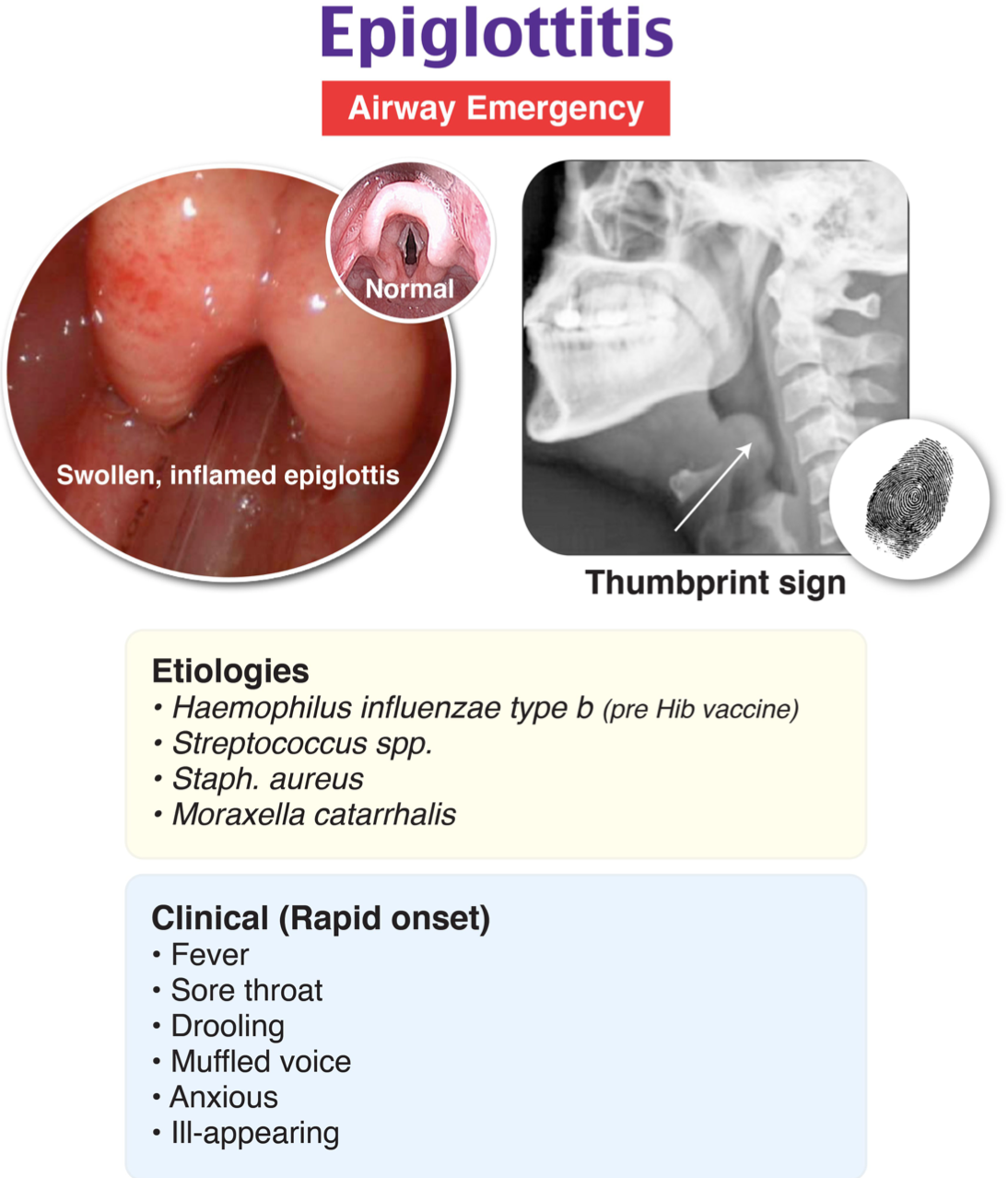
EPIGLOTTITIS
BG
FEATURES
HOW OFTEN INTUBATION
MX
BG
Acute life-threatening infection caused by
Haemophilus influenza type B (Hib)
staph
strep
Most commonly age 2-3
DDx would be croup
FEATURES
Rapid onset of oedema of the epiglottis and aryepiglottic folds,
high fever (usually >39.5),
present sitting or leaning forwards,
drooling saliva,
unable to swallow with
tongue pushed forwards,
adopting a ‘tripod’ position.
Inspiratory and expiratory stridor is a rapidly progressive AND LATE
INTUBATION
Indicated in 60% of cases
MX
IV Steroids
IV Abx (Cefotaxime 50 mg/kg IV BD)
Procedure
In OT
INTUBATION CAN BE EXCEEDINGLY DIFFICULT
May have a small mucus bubble
Consider intubation via stylet
May need smaller ETT
Personnel
Anaesthetist for induction
ENT scubbed with trache kit open
Equipment
IV access - CI as can precipitate laryngospasm but ok if EMLA
QUINSY
BG
BG
Often due to dental abscess
FEATURES
Stridor
Upper airway obstruction
Trismus
ANAES ISSUES
Issue not usually larynx
Mainly that laryngoscopy may be hard due to poor MO
Gas induction
Spont breathing
Topicalise
VL
ENT back up
Muscular Dystrophies
4 x criteria
Duchenne muscular dystrophy
Brief what
Anaes implications
4 CRITERIA
Primary myopathies
Genetic basis
Progressive
Degeneration and death of muscle fibres occur at some stage of the disease
Duchenne
X linked recessive
Early childhood as weakness and motor delay
Pseudohypertrophy of calves
Elevated CK
Mild cognitive imp
Usually wheelchair bound by 20s
Death by early adult
Anaesthetic Implications
AVOID VOLATILES - increased risk of rhabdo, short period ok
AVOID AVOID SUX - LIFE THREATENING HYPERKAL
CAUTION NMBDs - delayed onset and delayed recovery
CONGENITAL ABNORMALITIES
What is a shunt
How can paed congenital heart lesions be classified with examples
Shunt
A shunt is an abnormal flow between the cardiac chambers that results in mixing of blood
Classified
ACYANOTIC
L → R shunt
ASD, VSD, PDA
Large defects assoc with CCF in infancy
If unrepaired can → Pul HTN and Eisenmengers (R to L shunt)
Obstructive lesions
AS, coarctation, pul stenosis
severity determines age of pres
CYANOTIC
R → L shunt eg. TOF - may present with sevee cyanosis
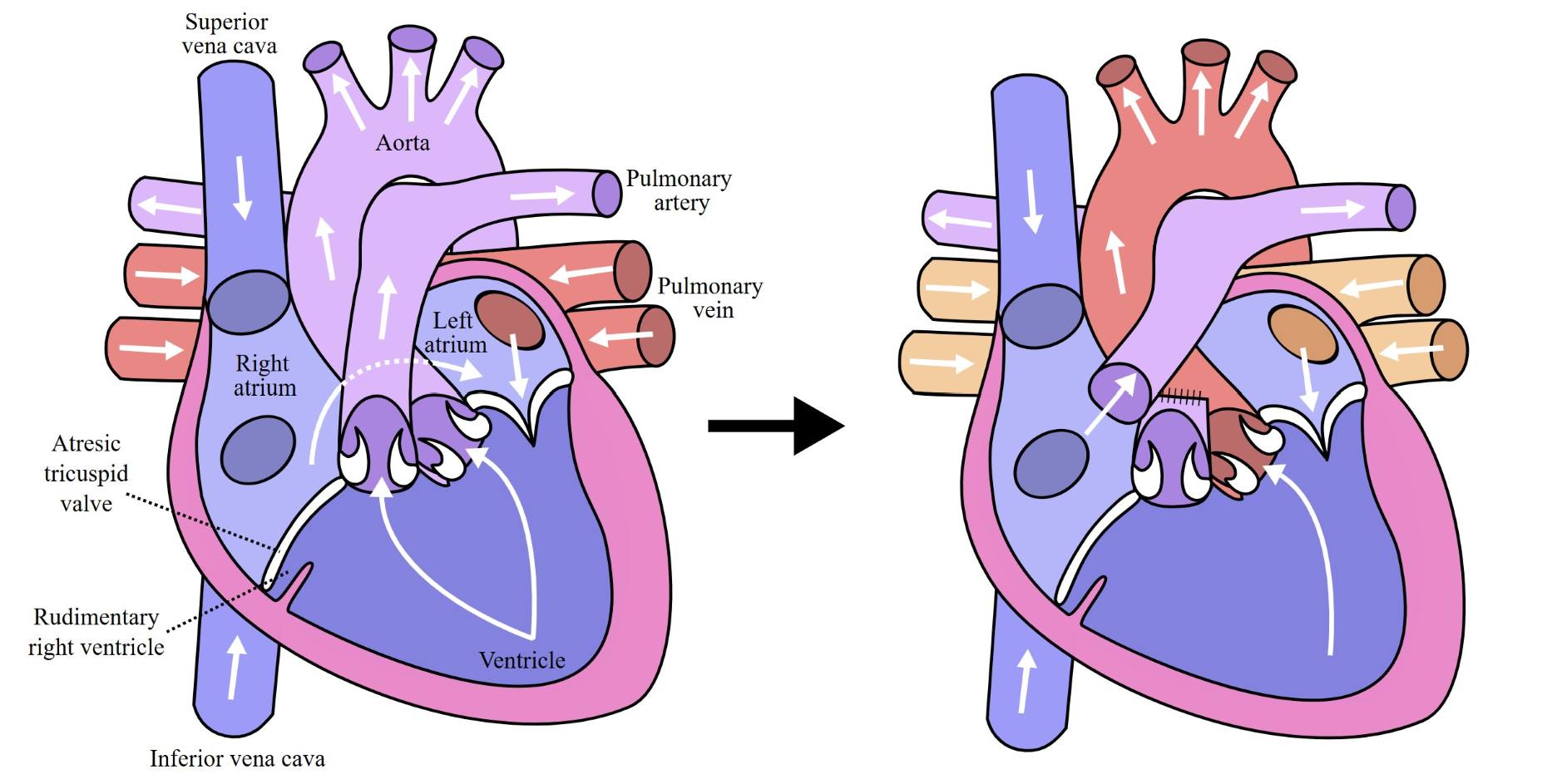
What is FONTAN Circulation
Implications
The fontan circulation consists of a hypoplastic right heart or tricuspid atresia where there is a single ventricle
As a result these children have a palliative procedure performed whereby their single ventricle pumps blood to the systemic circulation but the pulmonary circulation is driven by purely passive flow of blood returning via SVC/IVC into the right heart and flowing into the pulmonary artery (without any pressure established from an RV)
The implications of this are that:
They are very preload dependent and loss of preload results in loss of pulmonary circulation and CO
They respond poorly to changes in Pa02 / PaC02 upon their pulmonary circulation
PEEP and IPPV are tolerated relatively poorly on the pulmonary circulation
They are at risk of VTE and are generally anti-coagulated
How do you anaesthetise a 30 year old man with a Fontan Circulation for Appendicectomy?
See Matts notes
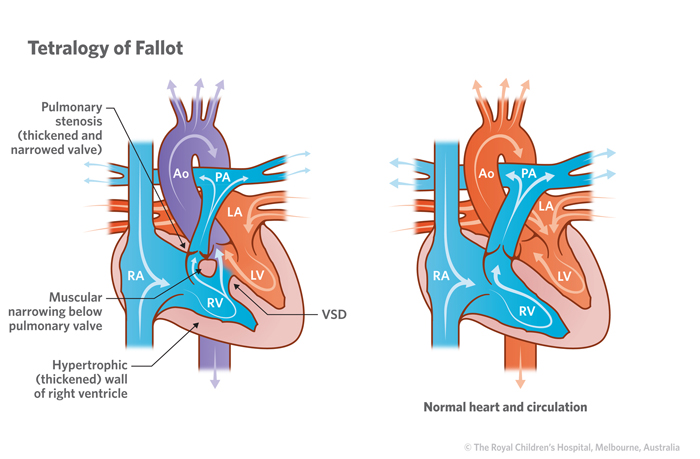
Tetralogy of Fallot
BG
Principles
BG
TOF often corrected by the time of presentation for other surgical procedures
Occasionally they are treated with an initial surgical shunt (Modified BT shunt) between right subcalvian artery and pulmonary artery to provide pulmonary blood flow and allow the lungs to grow before progressing to full repair.
It is very very very unlikely they will ask you about partially treated TOF. For the purposes of FANZCA, in the unlikely event of a non-corrected, non operated TOF
PRINCIPLES
VSD
RVOT Obstruction (various levels – dynamic and static obstruction, pulmonary valve or subpulmonary level; severe TOF may have pulmonary atresia)
RV Hypertrophy
Aorta overriding VSD
Treat them like a right sided HOCM.
Sympathetic stimulation (increased contractility and tachycardia) is bad.
Increased contractility worsens the RVOTO, as does dehydration.
Therefore, they need to be well hydrated (1st on list, 2 hours after a drink of clear fluids) and calm (maybe with premed).
Reduced systemic vascular resistance is also bad, so alpha agonists useful
Implications
SIGNIF impaired pul blood flow due to RVOT obstruction and pul hypoplasia
They require ductus arteriosus to remain patent to allow adequate CO to PUL circ
SIGNIF mixing of blood across VSD
Reduce FiO2, target normal MAP, Nnormal temp and normal PaCO2
Anticipate lower PaO2 and SpO2
Maintain preload