Pathology practical
1/118
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
119 Terms

Nasal Polyp
Polypoid gelatinous mass with smooth outer surface, filling the left nasal cavity

Nasal Polyp
Polypoid gelatinous mass with smooth outer surface, filling the left nasal cavity
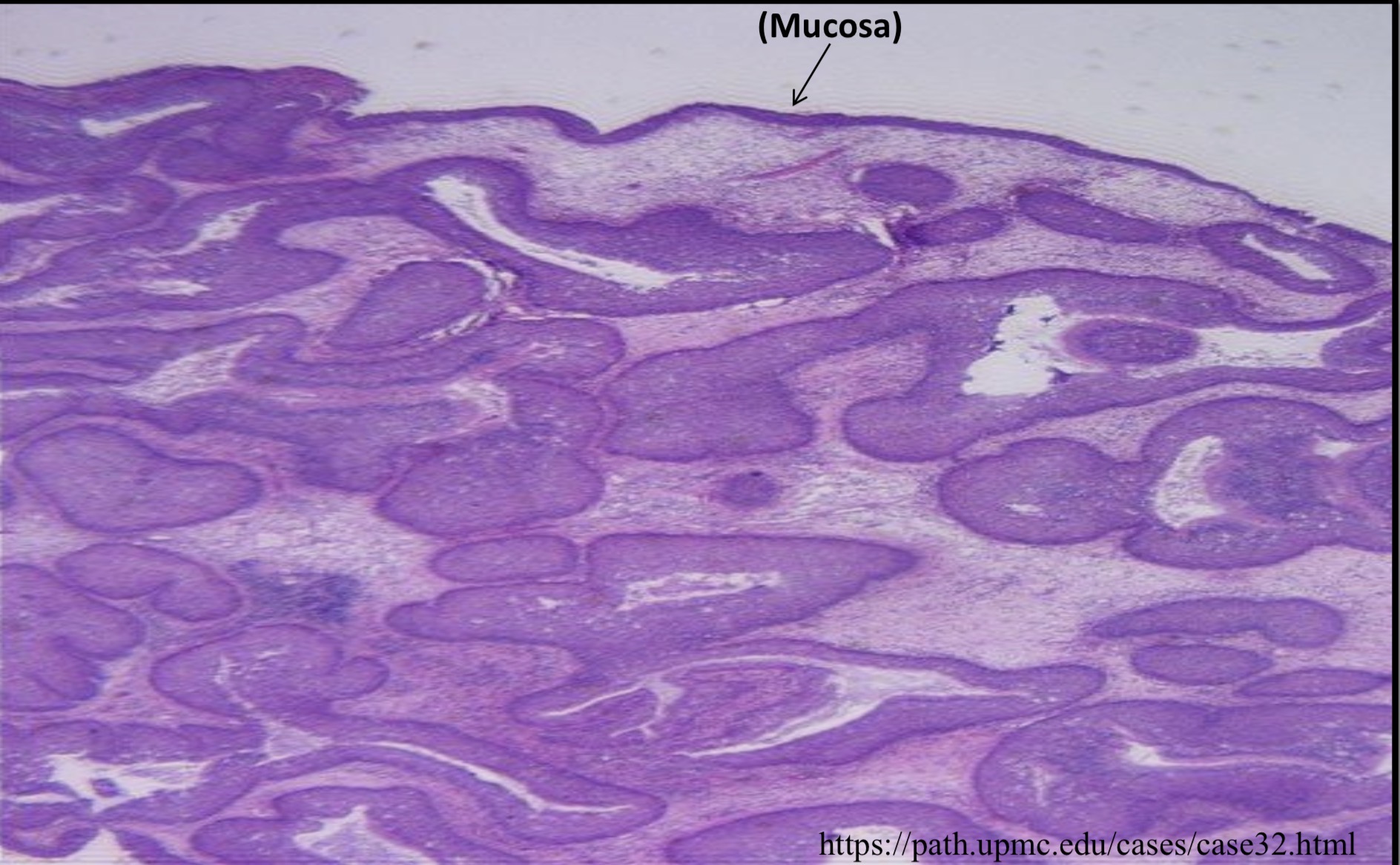
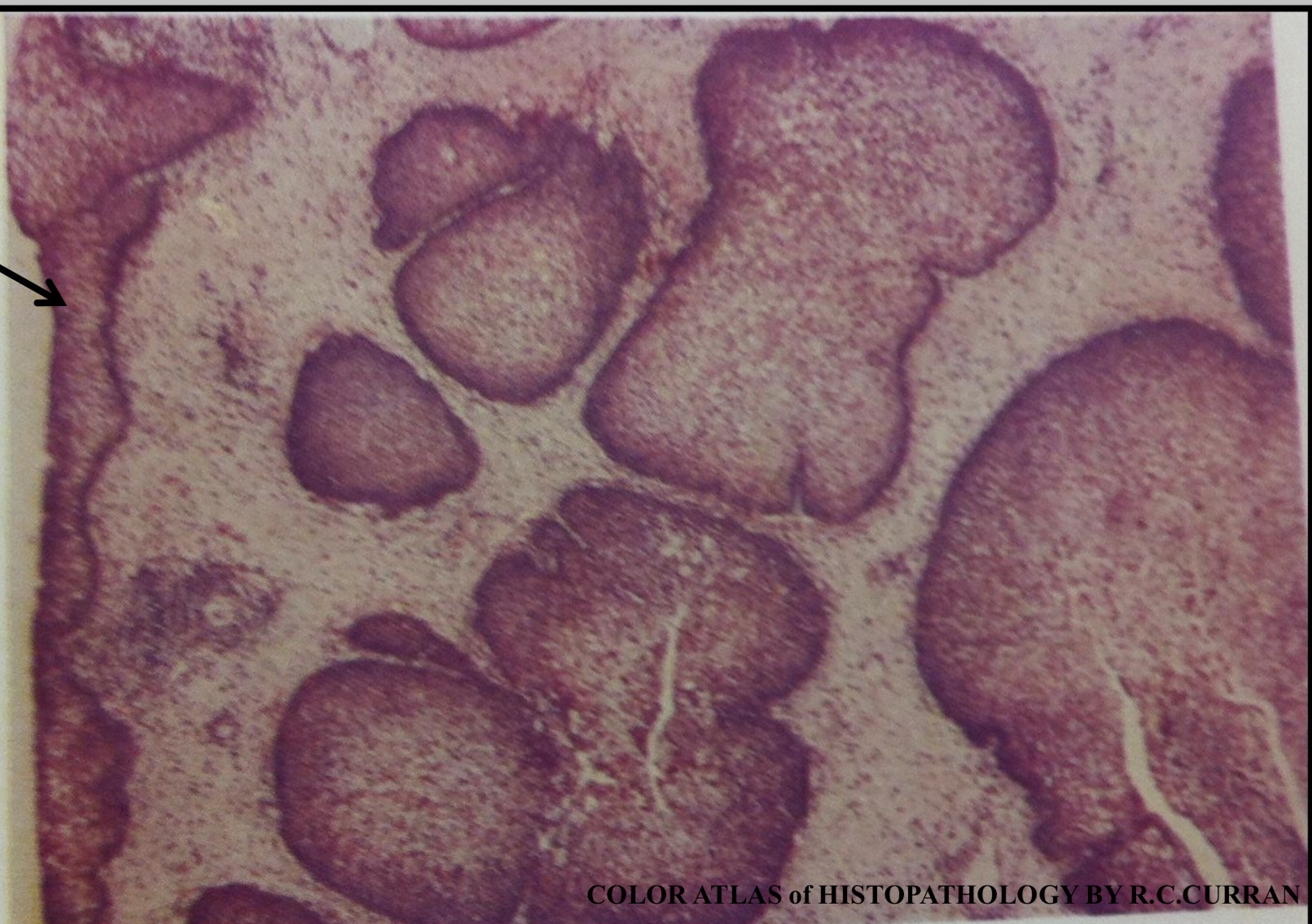
Nasal Papilloma: Exophytic (Fungating) Papilloma
Exophytic papillary growth pattern of benign looking epithelial cells
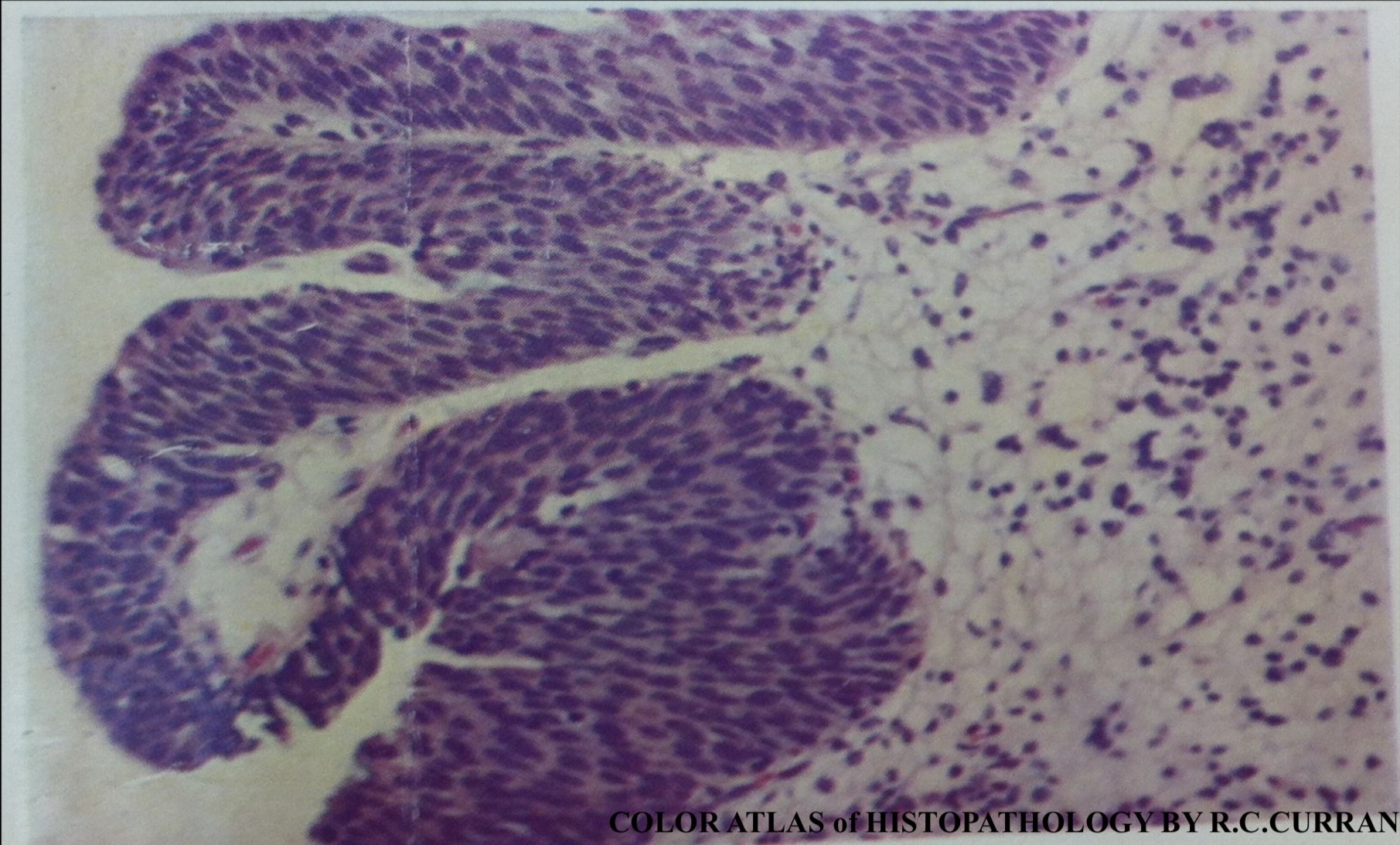
Nasal Papilloma: Inverted Papilloma
Inverted growth pattern of benign looking epithelial cells forming masses of cells in the submucosa
Nasal Papilloma: Inverted Papilloma
Inverted growth pattern of benign looking epithelial cells forming masses of cells in the submucosa

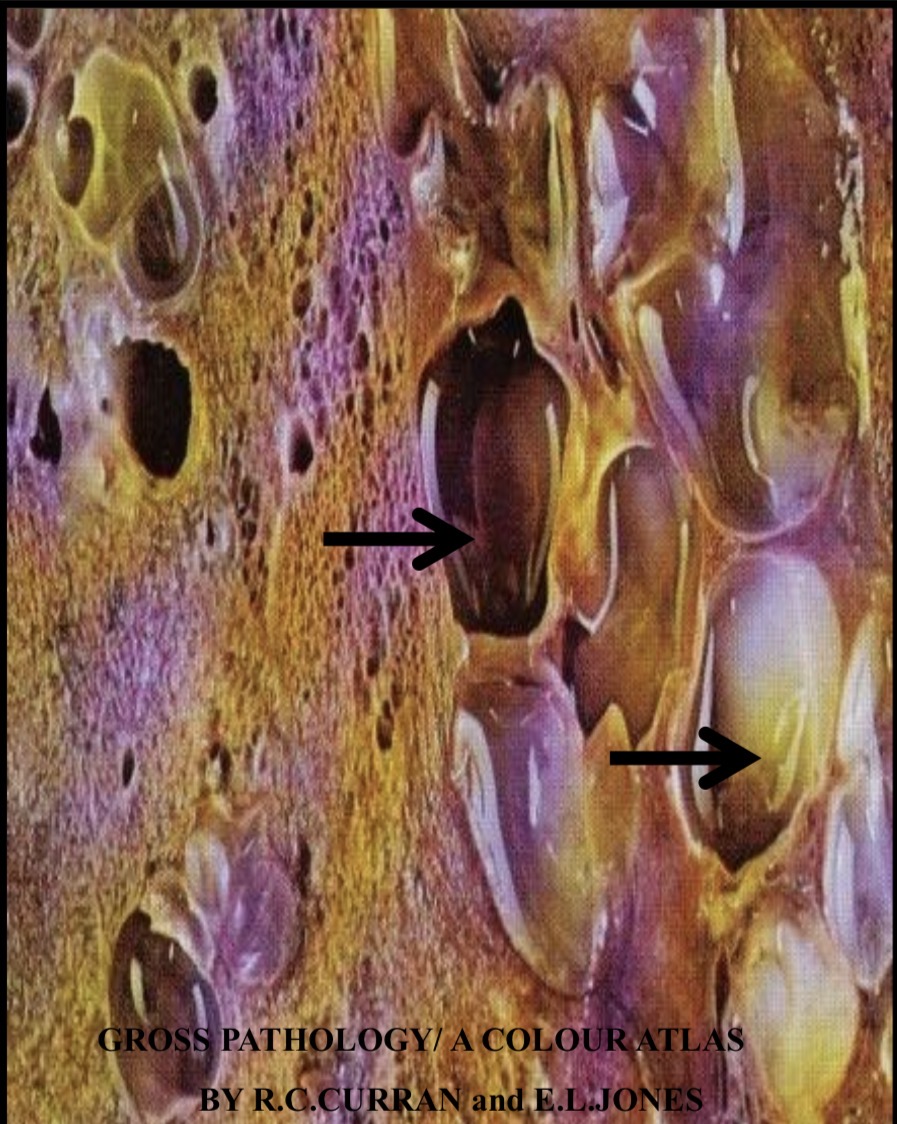
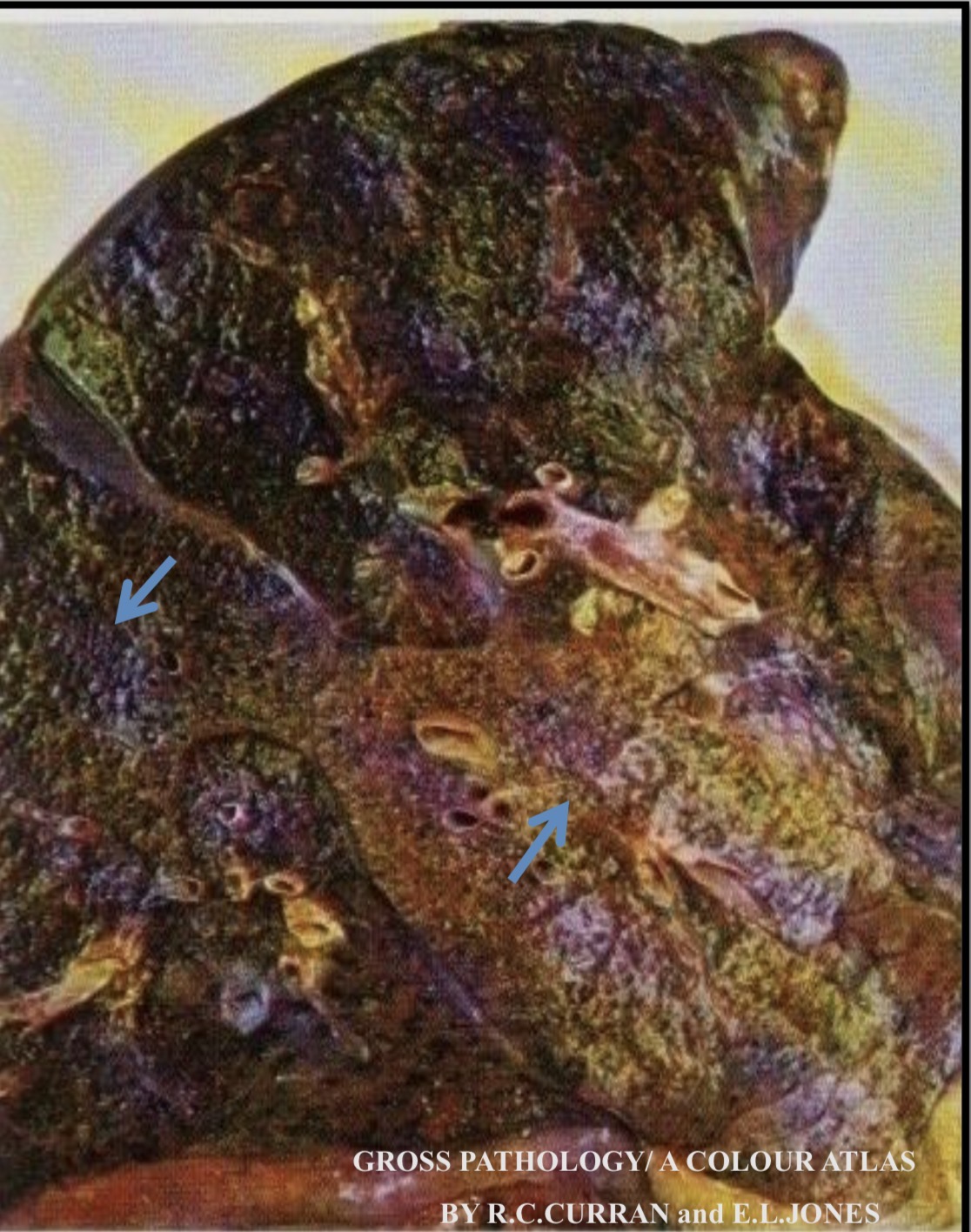
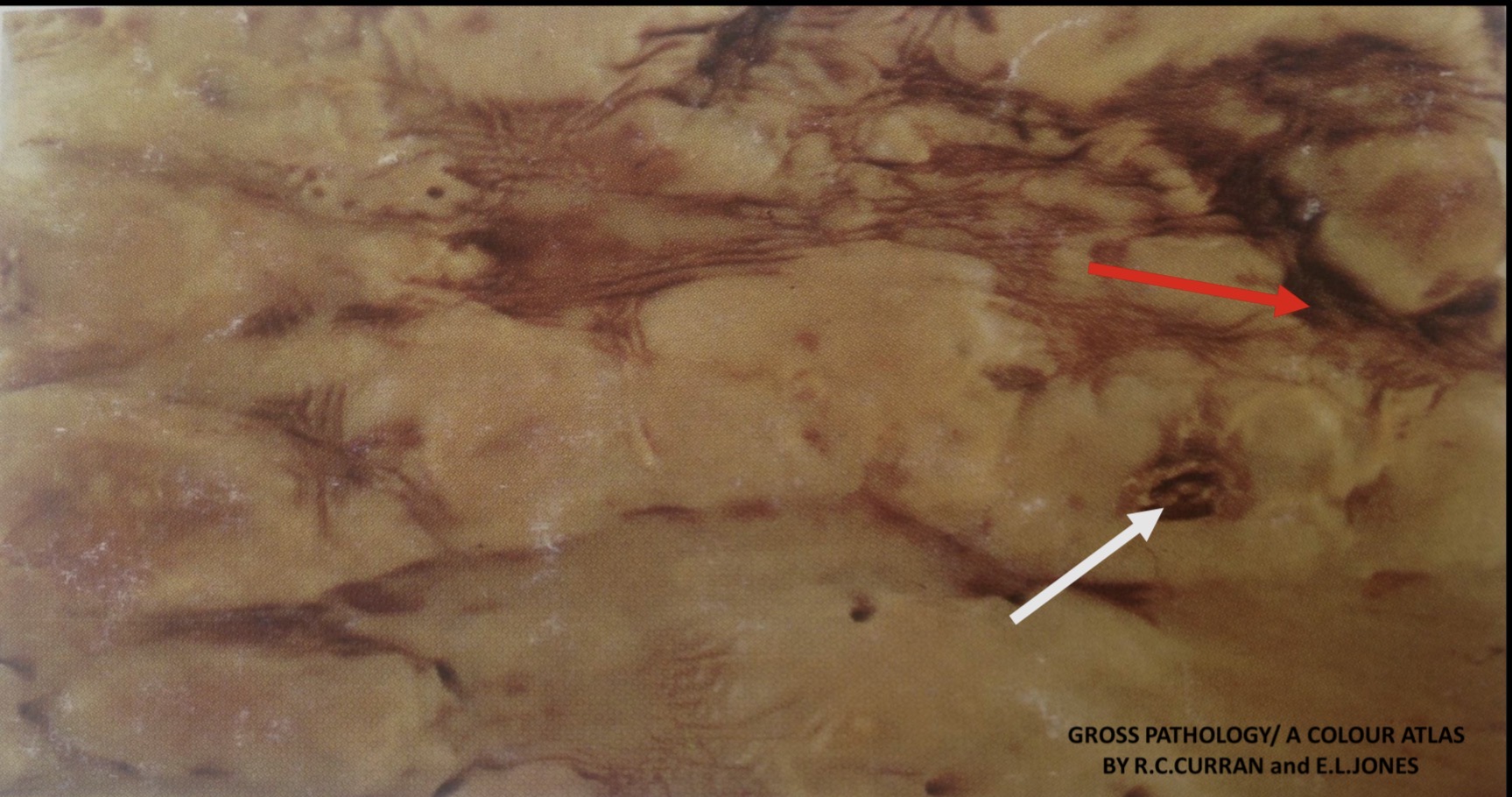
Bronchiectasis
Permanent dilation of bronchi and bronchioles forming prominent cavities (arrows).It is caused by destruction of the muscle and elastic supporting tissue
Bronchiectasis
Bronchiectatic cavities lined by respiratory epithelium and filled with inflammatory exudate
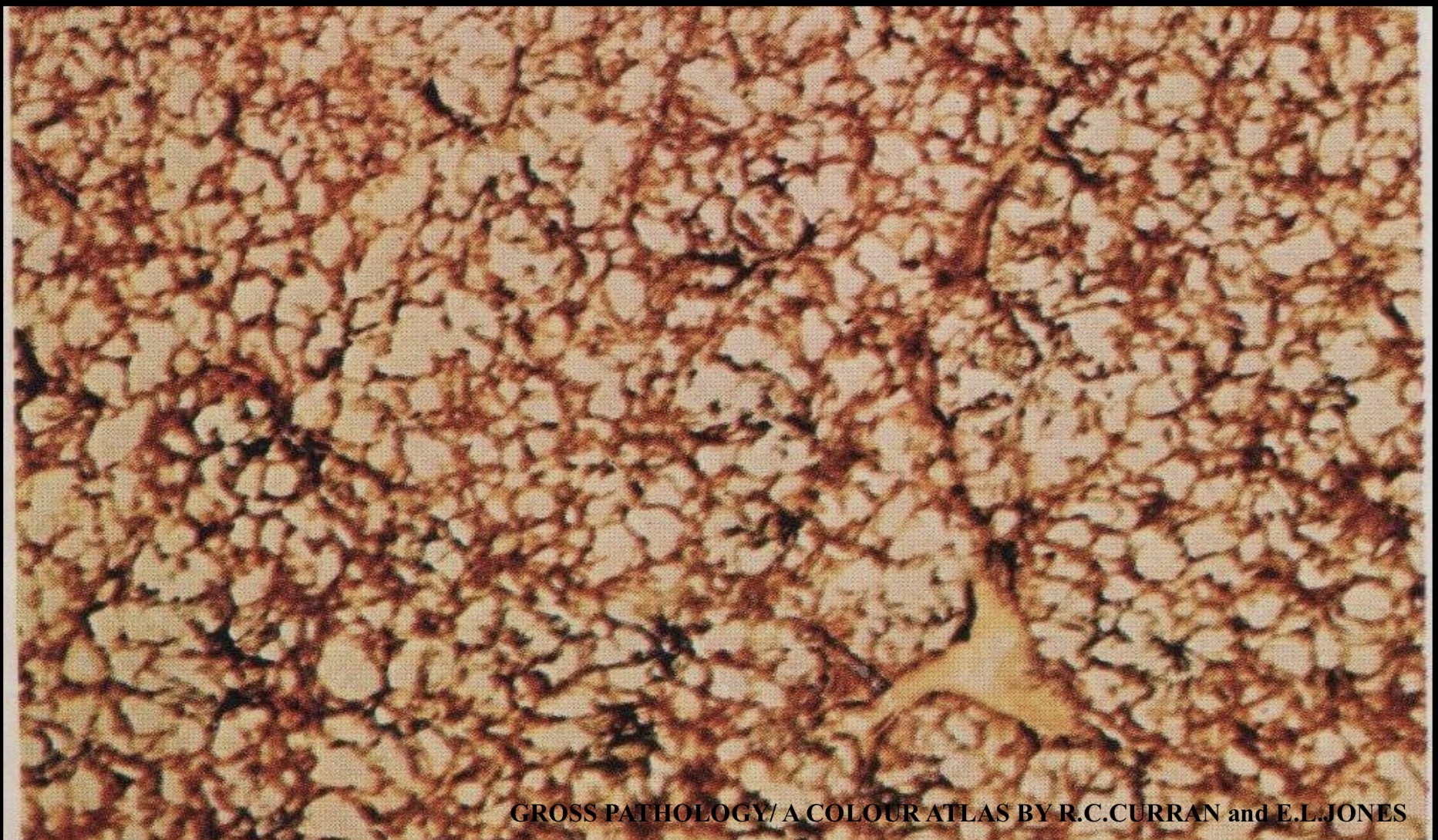
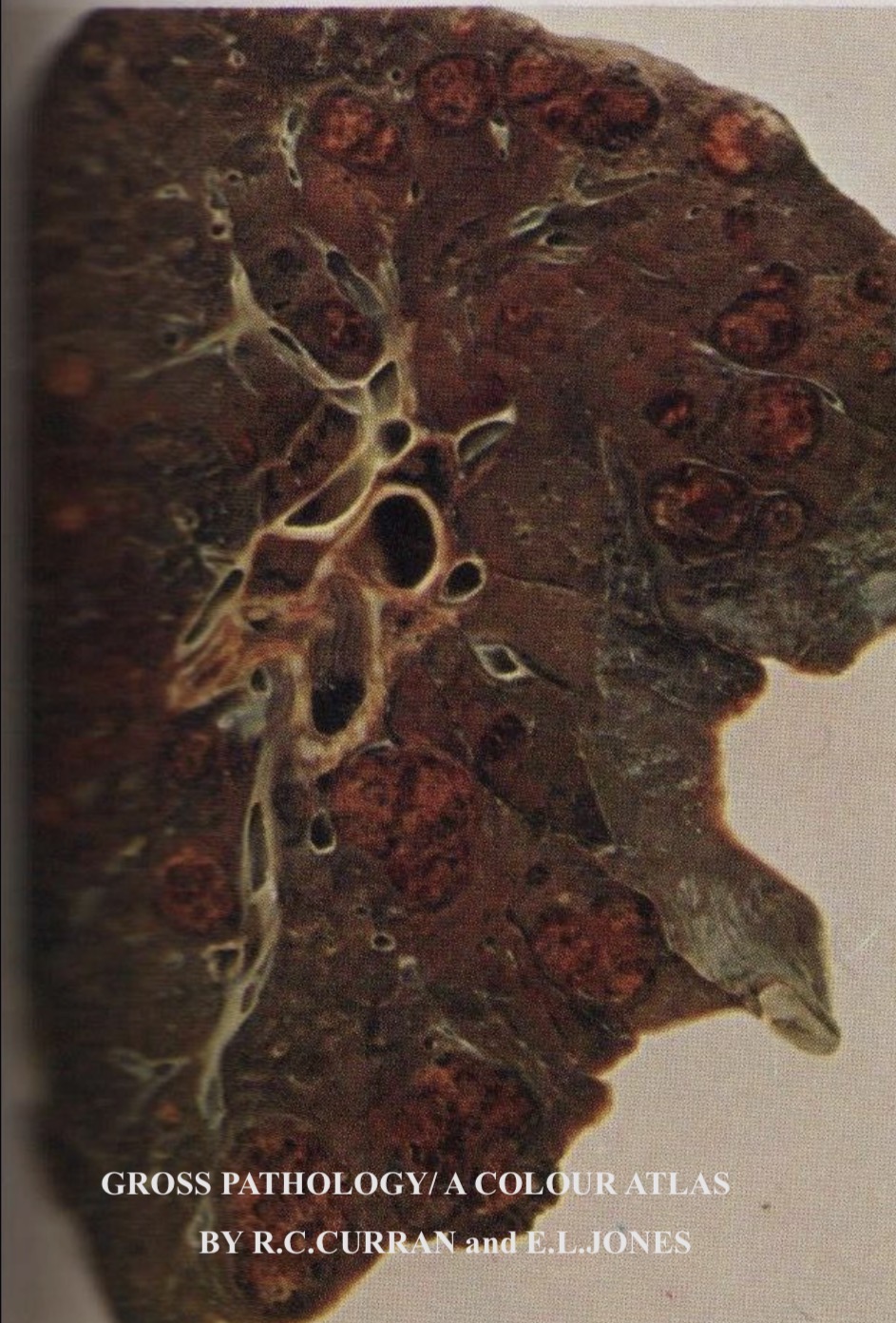
Centrilobular Emphysema
Slice of fixed inflated lung, the dilated air spaces are seen around the center of the lobule(centrilobular) with normal looking lung tissue in- between .
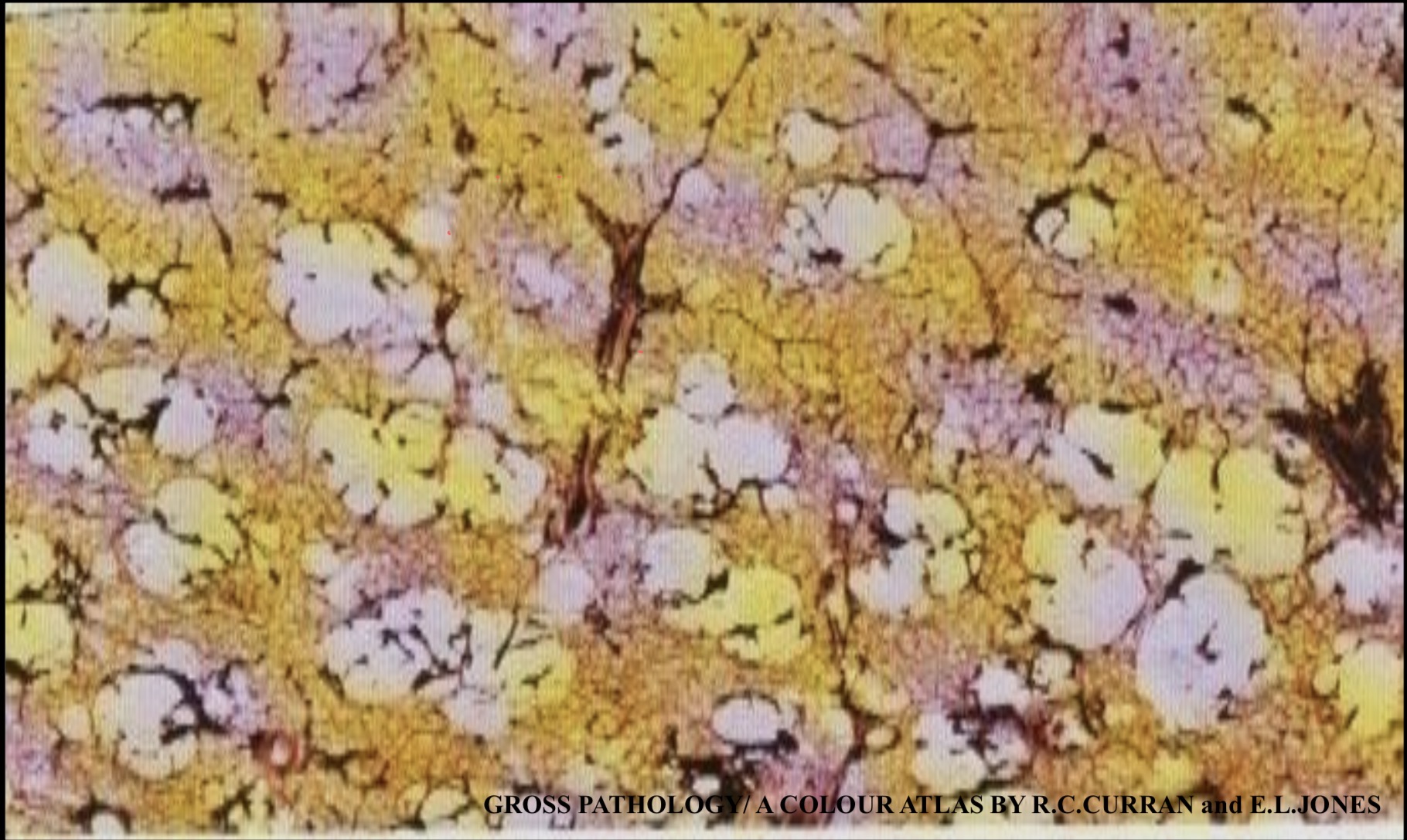
Panacinar Emphysema
Slice of fixed inflated lung, the dilated air spaces are seen to involve the alveolar ducts, alveoli and respiratory bronchioles, thus involving the entire acinus (Panacinar). No normal lung tissue
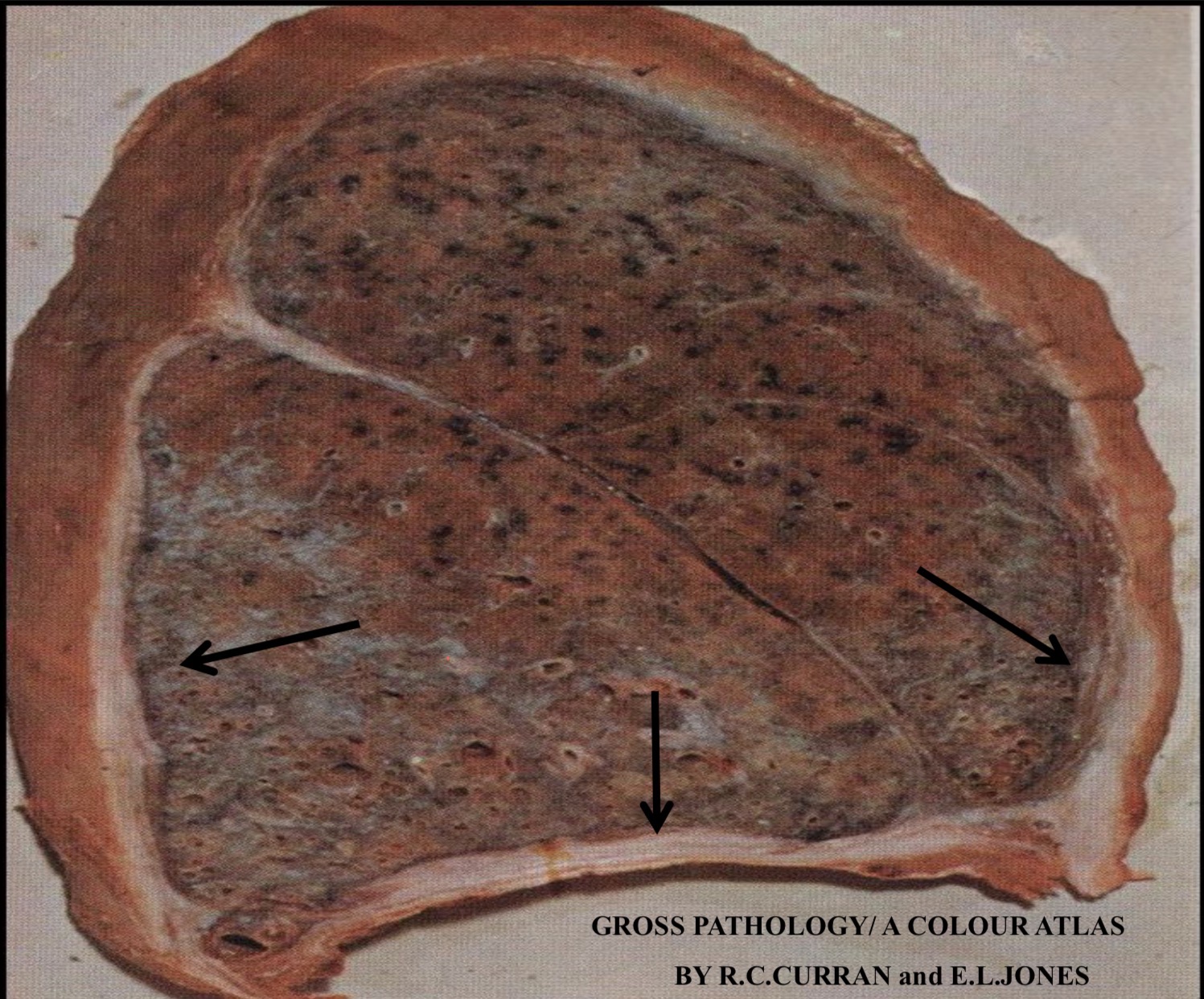
Lobar Pneumonia:
Consolidation that is sharply confined to the middle lobe of the lung (arrows). The affected lobe is Covered by greyish fibrin, it is dry, firm, grey and granular.

Lobar Pneumonia:
Grey Hepatization 4th – 8th day Grossly The affected lobe is covered by greyish fibrin Cut surface of the lobe is dry, firm, grey and granular.
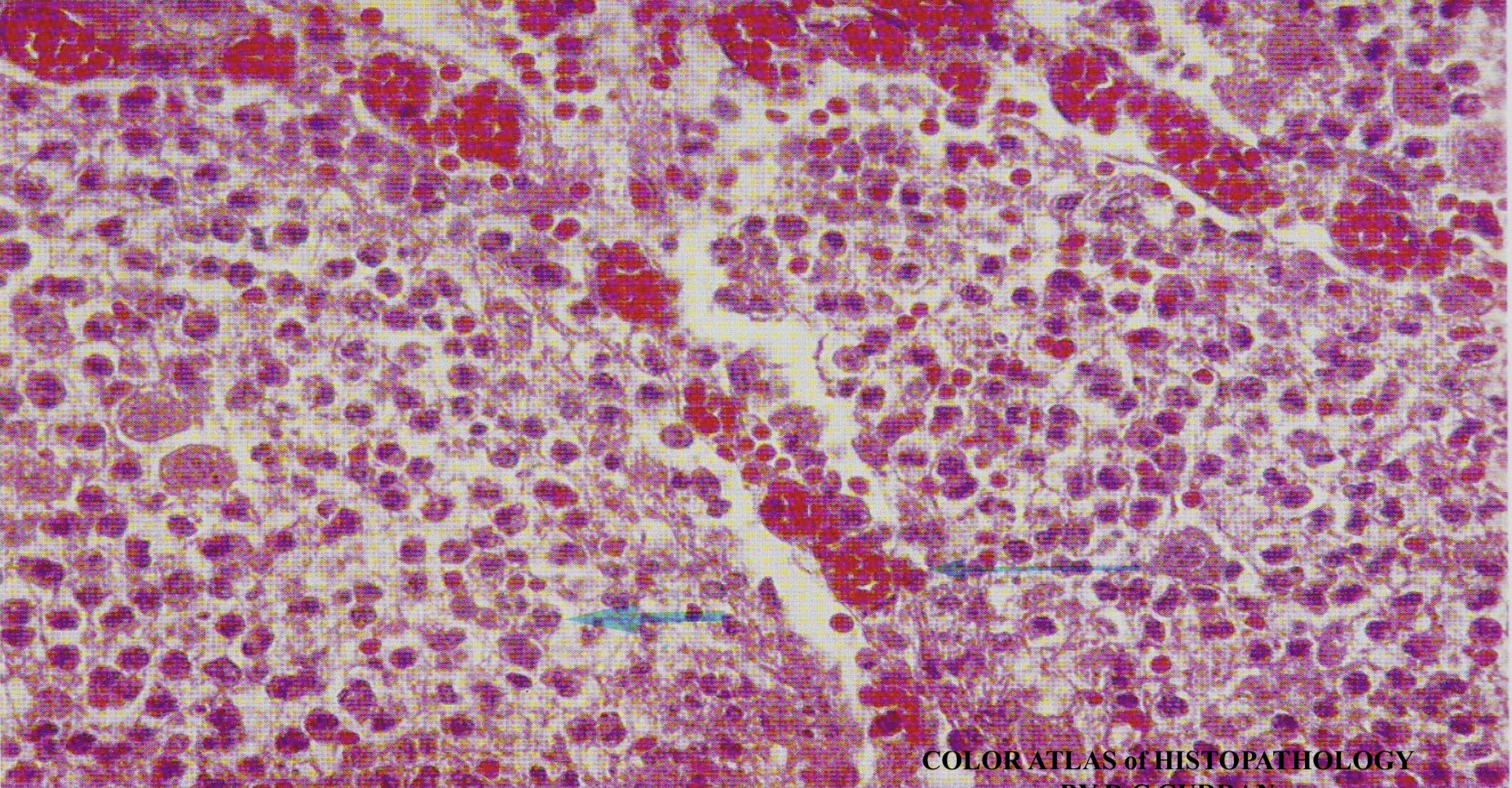
Lobar Pneumonia: Red Hepatization
Congestion of the alveolar capillaries (thin arrow). Alveolar spaces contain fine network of fibrin with large number of neutrophils and RBC (thick arrow)
Lobar Pneumonia: Grey Hepatization
No more congestion of the alveolar capillaries. Alveolar spaces are filled by dense network of fibrin with neutrophils and few RBC

Bronchopneumonia:
Multiple foci of patchy consolidation about 1 cm in diameter which appear to be centered around bronchioles (arrows).
Bronchopneumonia:
Multiple foci of patchy consolidation about 1 cm in diameter which appear to be centered around bronchioles
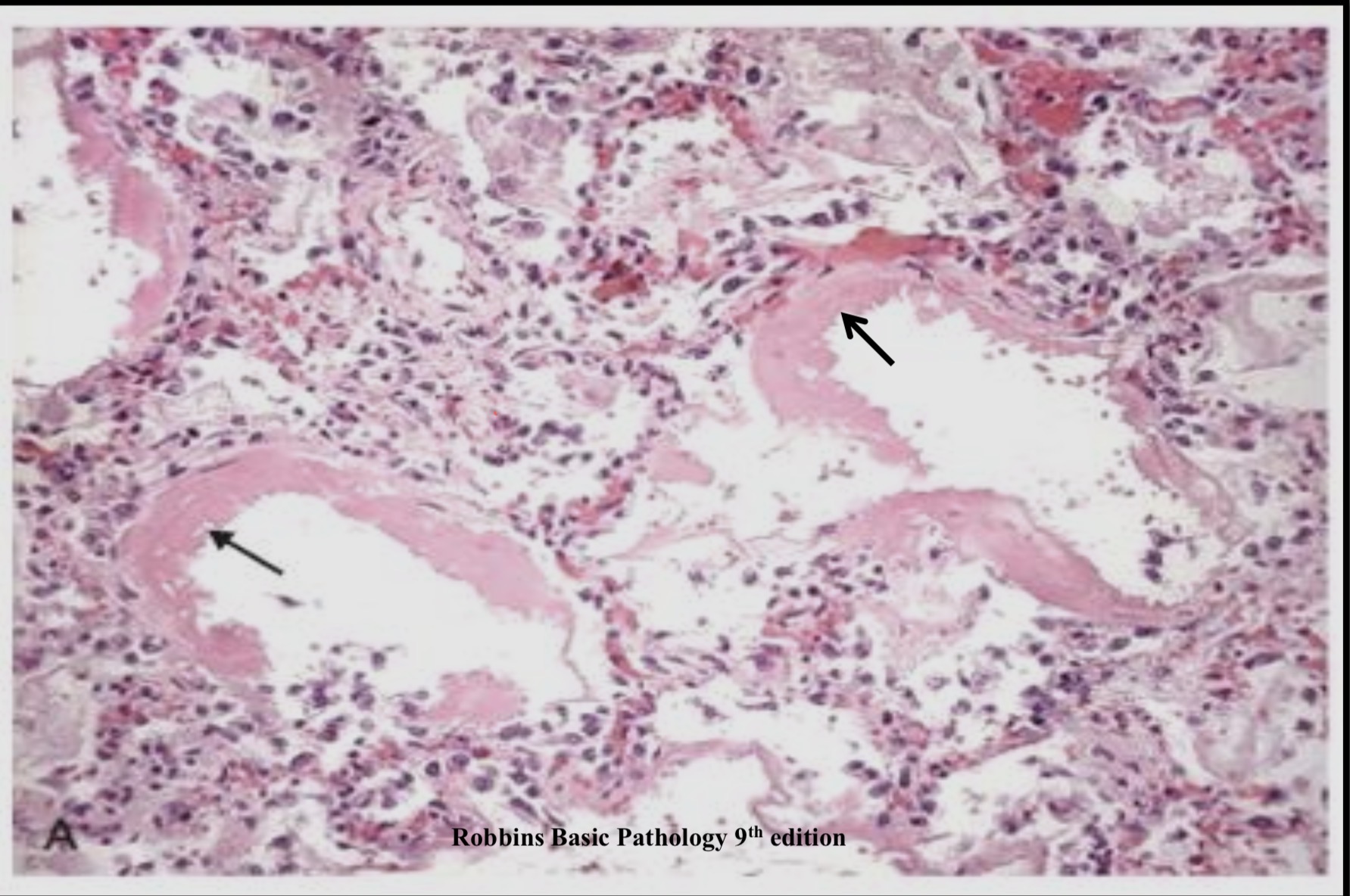
Acute Respiratory Distress Syndrome (ARDS): Lung Intra -alveolar fibrin exudation and Hyaline membrane formation
(eosinophilic material lining the alveoli) (arrows)
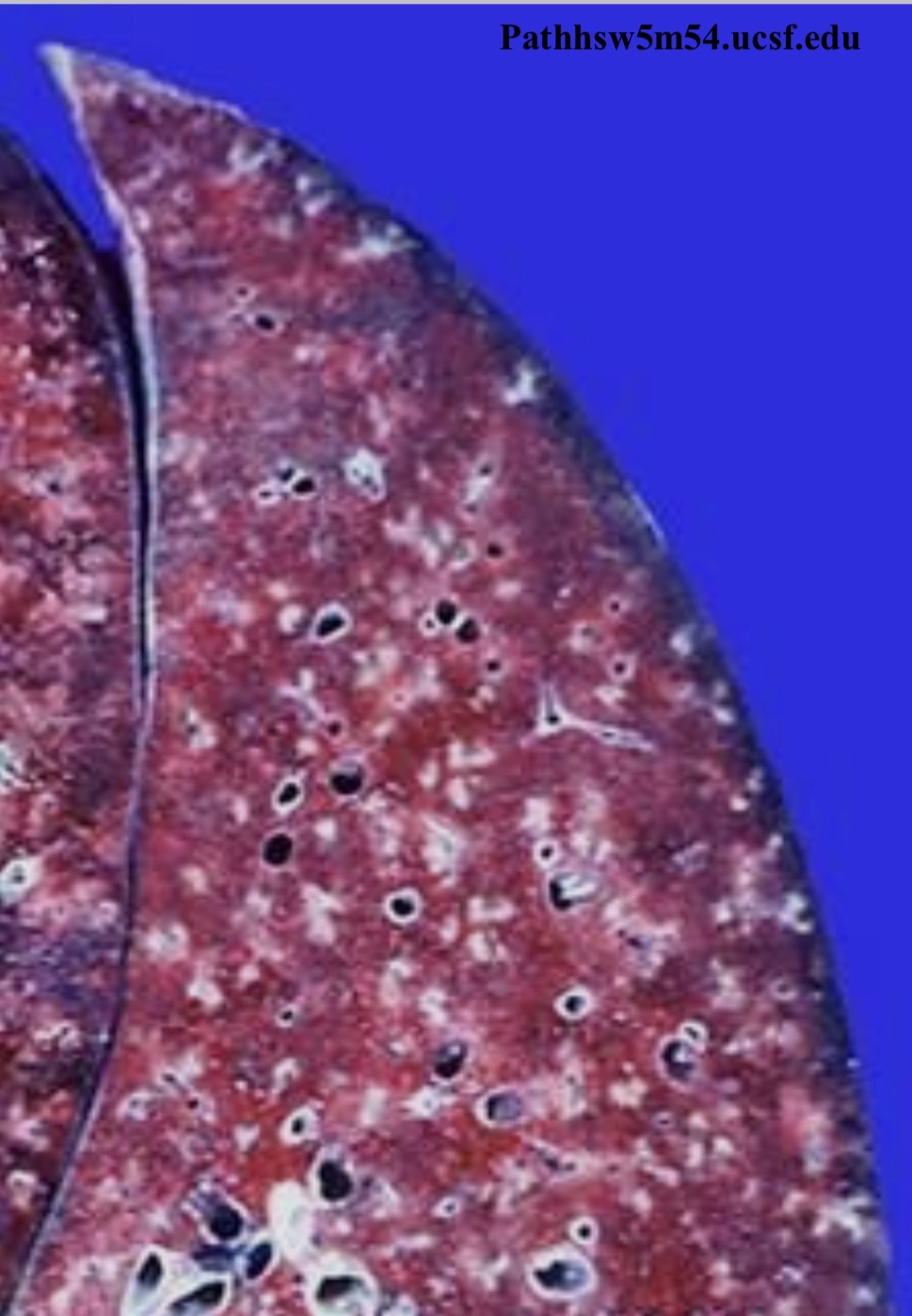
Simple Coal Worker Pneumoconiosis ( Focal Dust Emphysema): Lung
Patchy dilation of air spaces (centrilobular emphysema) with black dust (coal) pigmentation

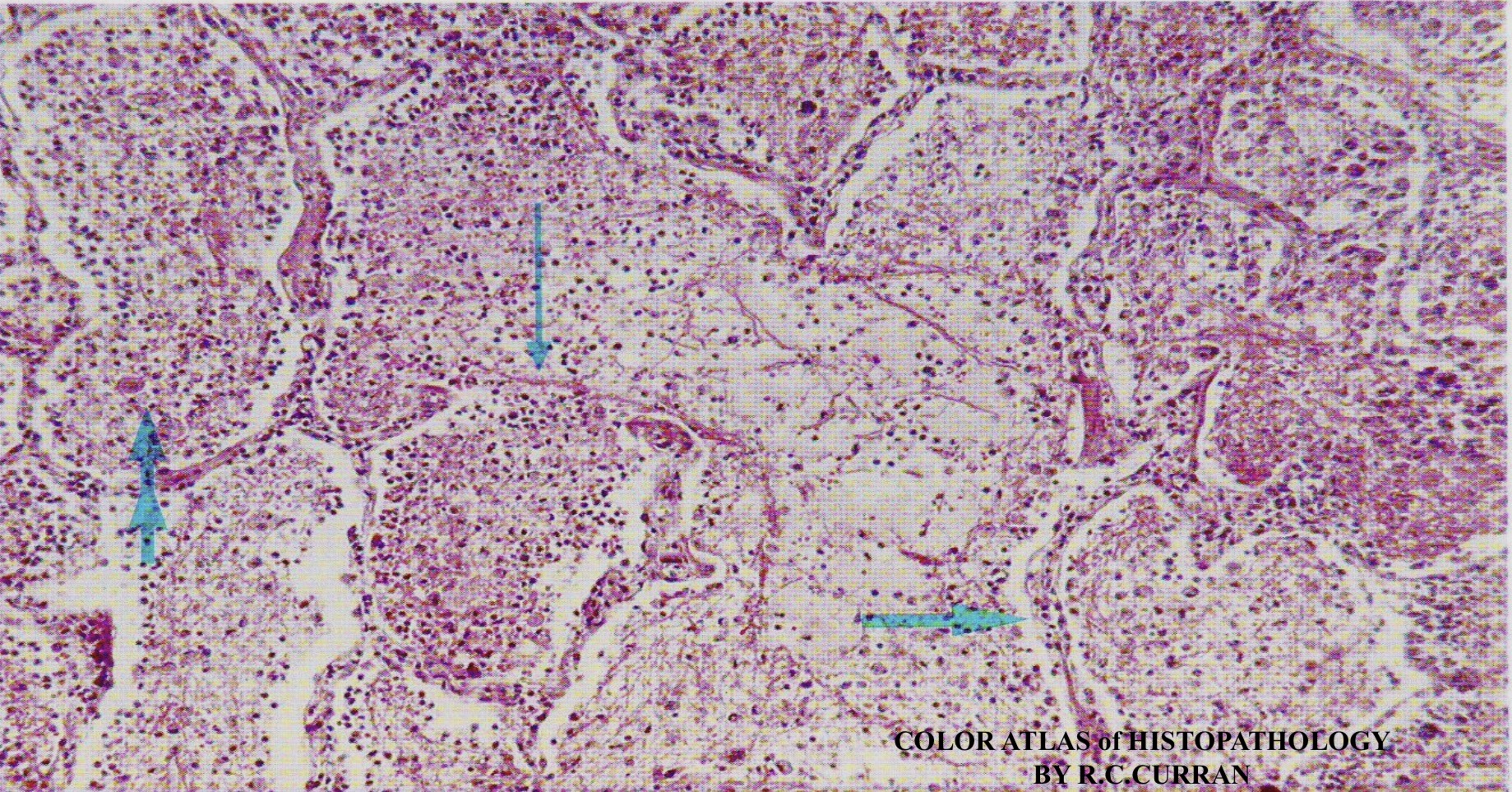
Silicosis: Lung
Multiple fibrous silicotic nodules in the upper zones of the lung (arrows).

Caplan's Syndrome: Lung
Multiple nodules up to 5 cm. in diameter scattered through out the lungs of workers who are exposed to inhaled dusts
Asbestosis: Lung- pleura
Diffuse fibrous thickening of the pleura around the lung (arrows)
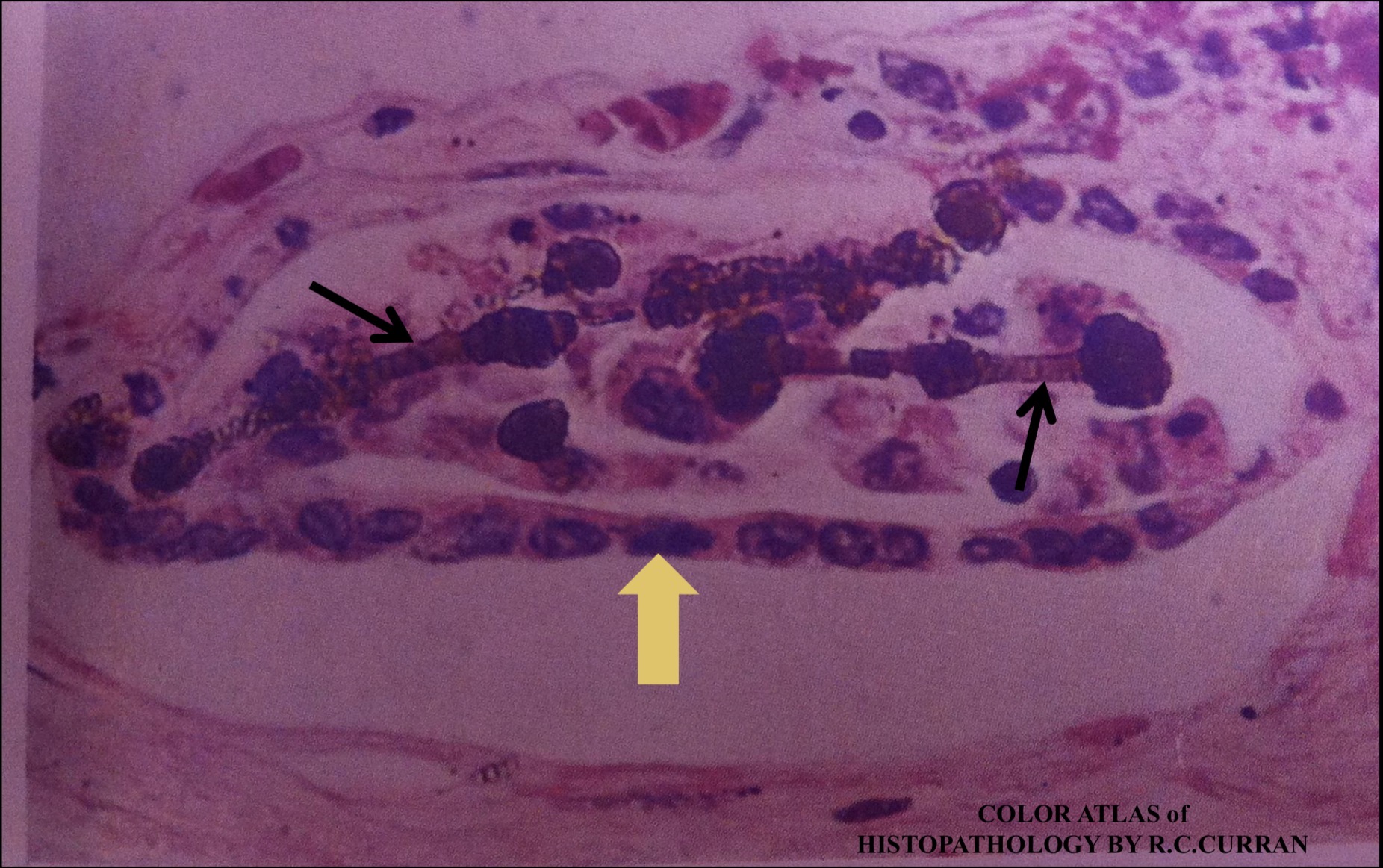
Asbestosis- Asbestos Bodies: Lung
Complete fibers are surrounded by macrophages (yellow arrow) and become coated with iron and protein derived from phagocyte ferritin forming a drumstick shaped body called Asbestos body (black arrows
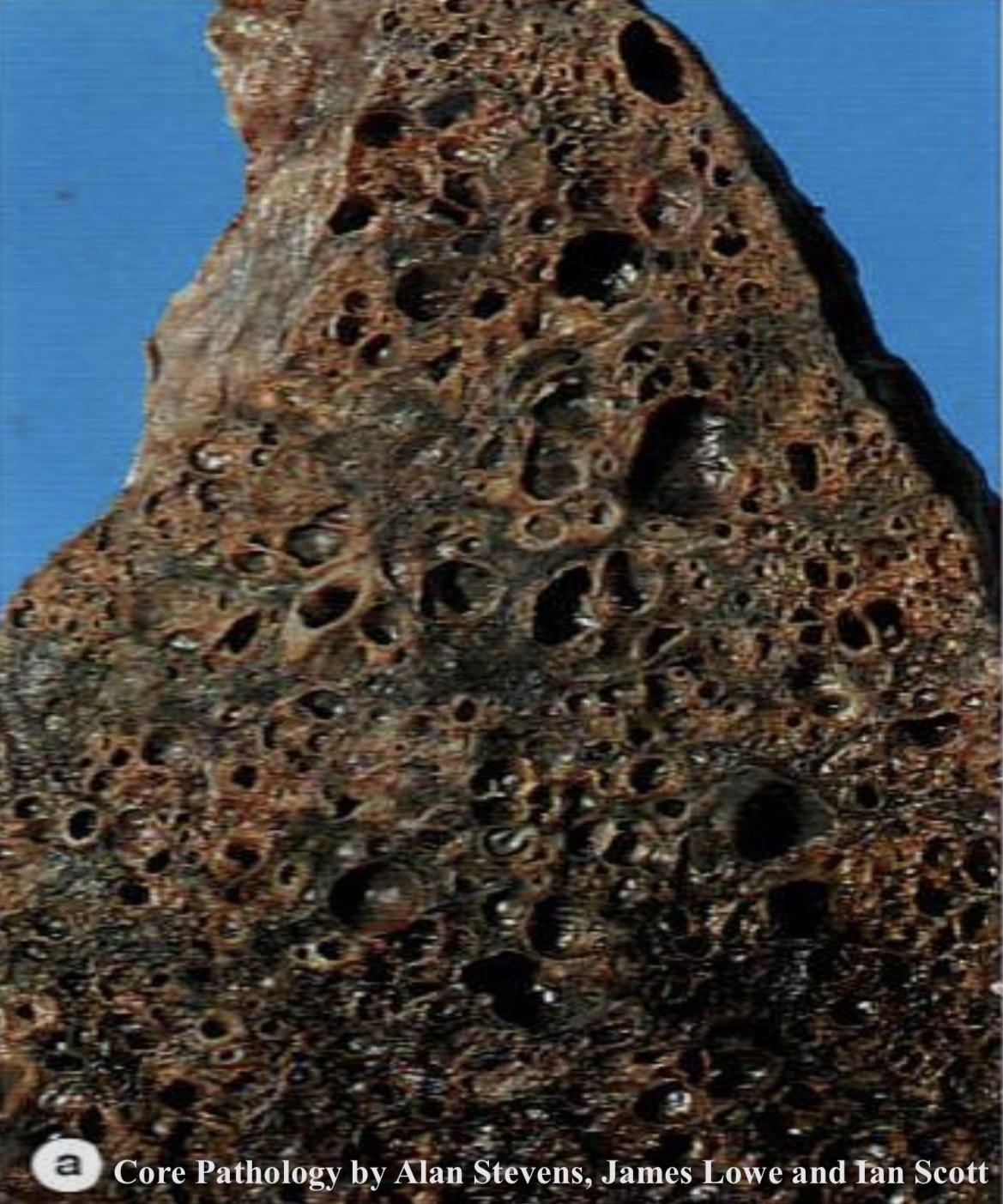
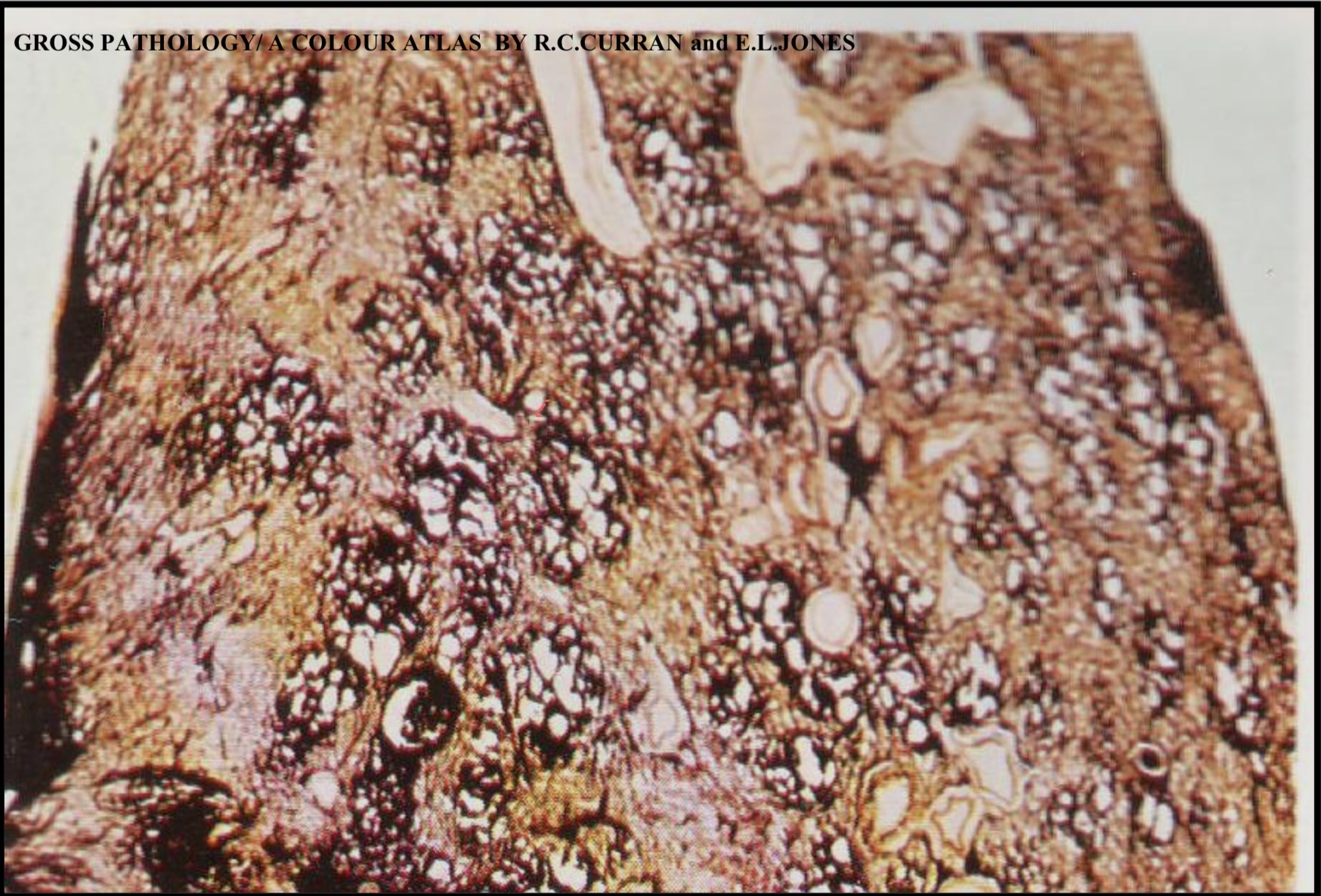
Honeycomb Lung :
Diffuse interstitial pulmonary fibrosis with cystic spaces develop in a fibrotic lung. This is the end stage of most chronic restrictive lung diseases, irrespective of the etiology.
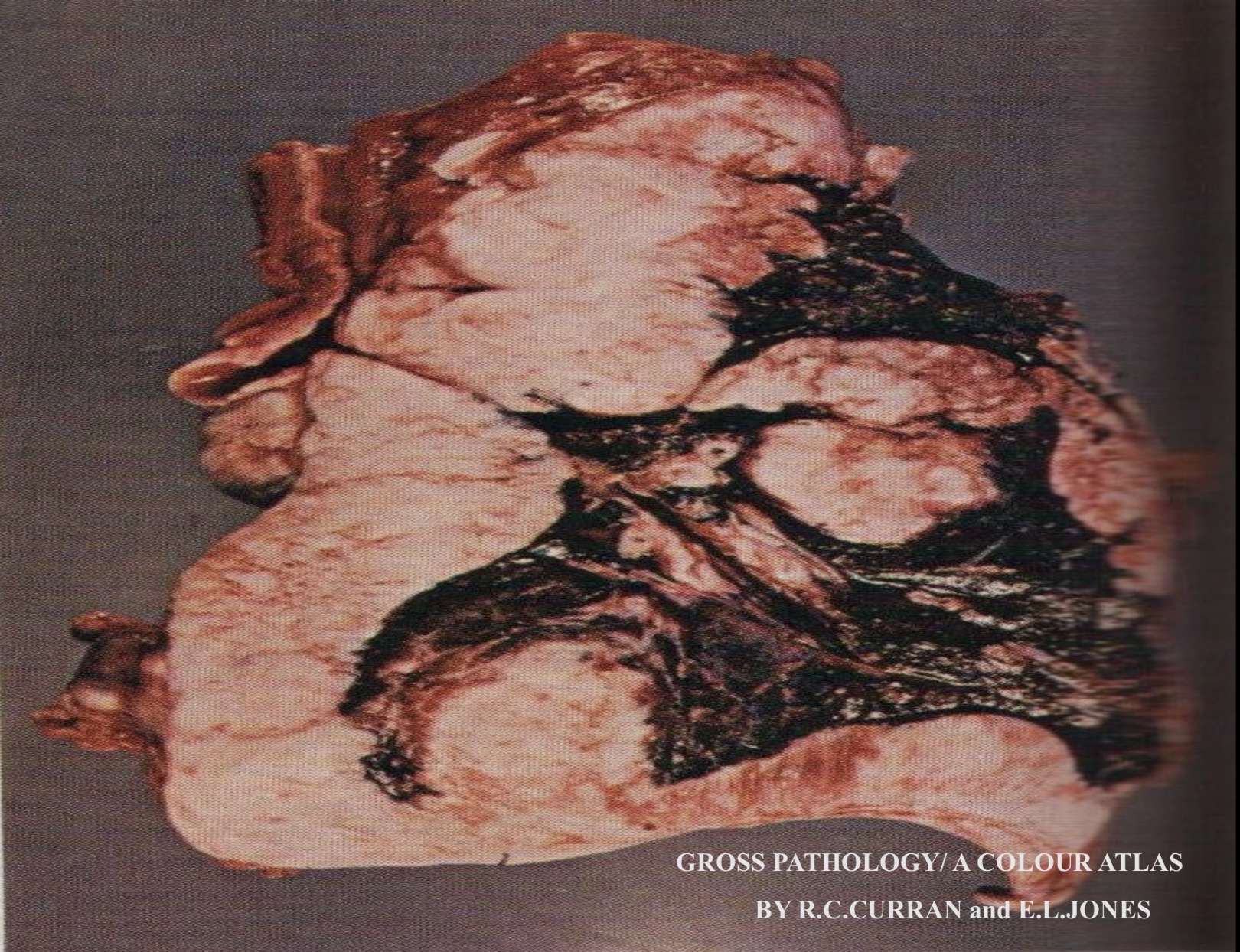
Malignant Mesothelioma
The tumor affects both visceral & parietal pleura forming diffuse thickening of the pleura that ensheathes and invades the lung
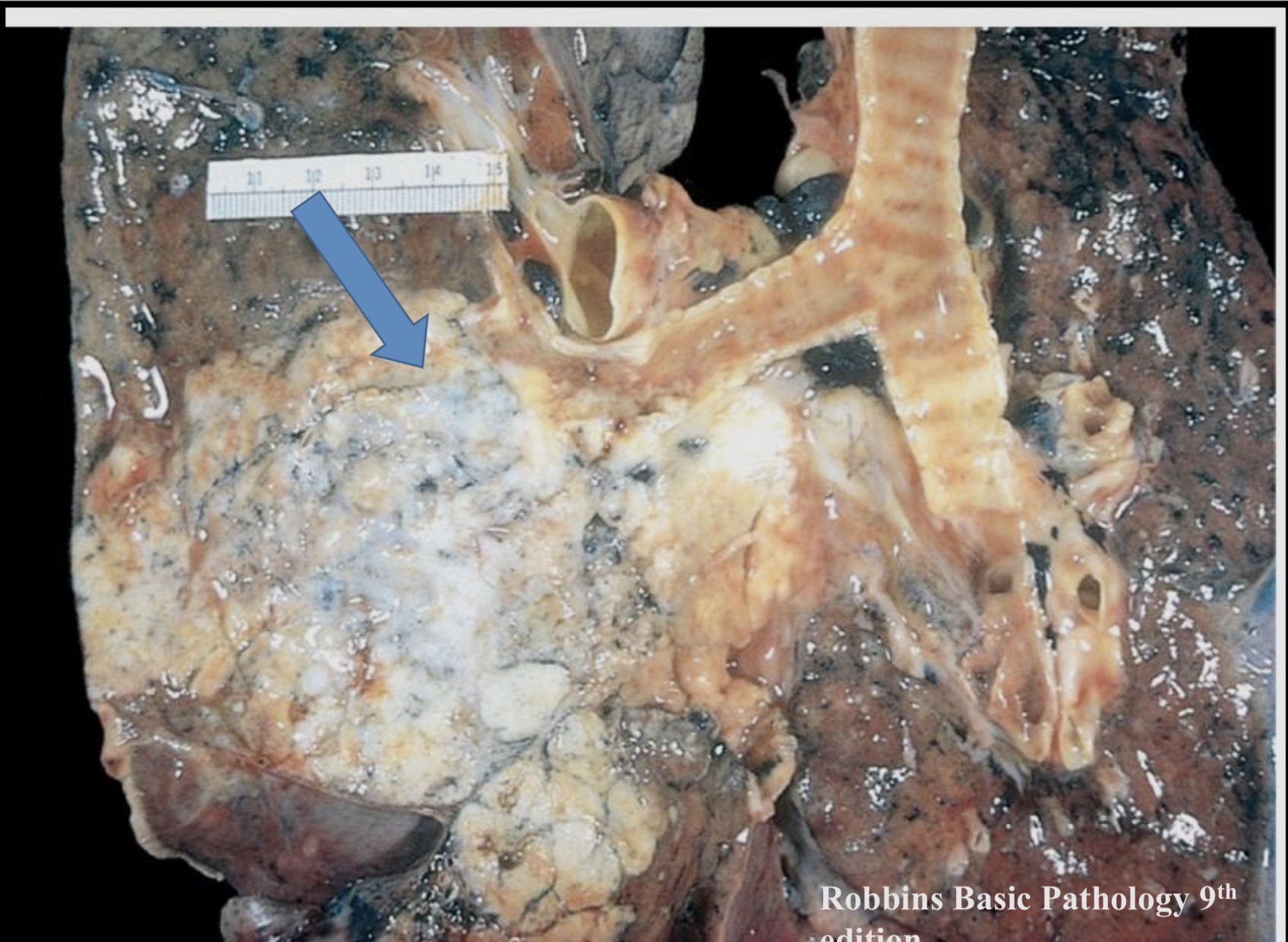
Squamous Cell Carcinoma: Lung
Large tumor arising in the right main bronchus (arrow)
Metastatic carcinoma, lung: multiple tumor masses scattered throughout the lung, cannonball appearance.
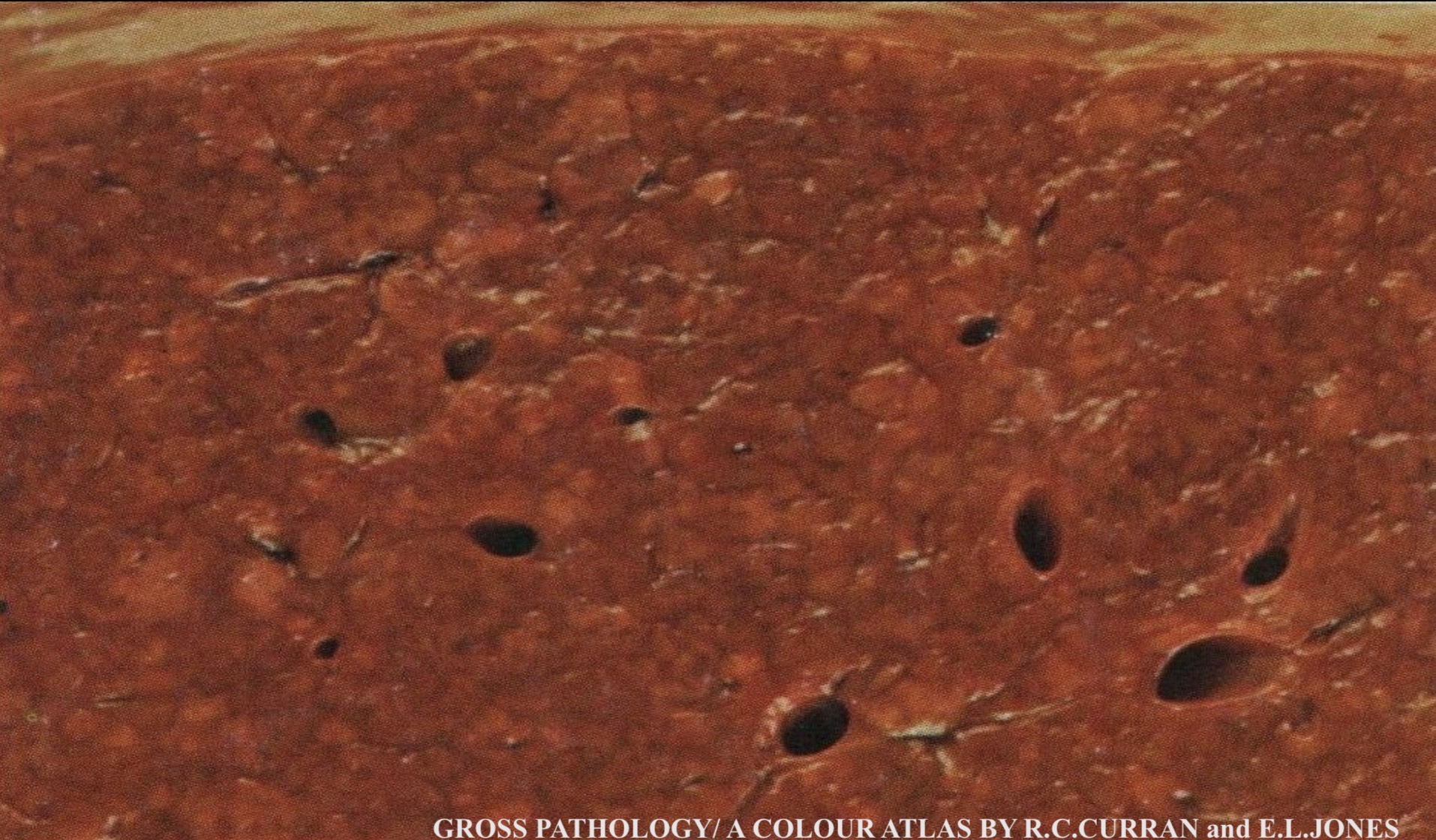
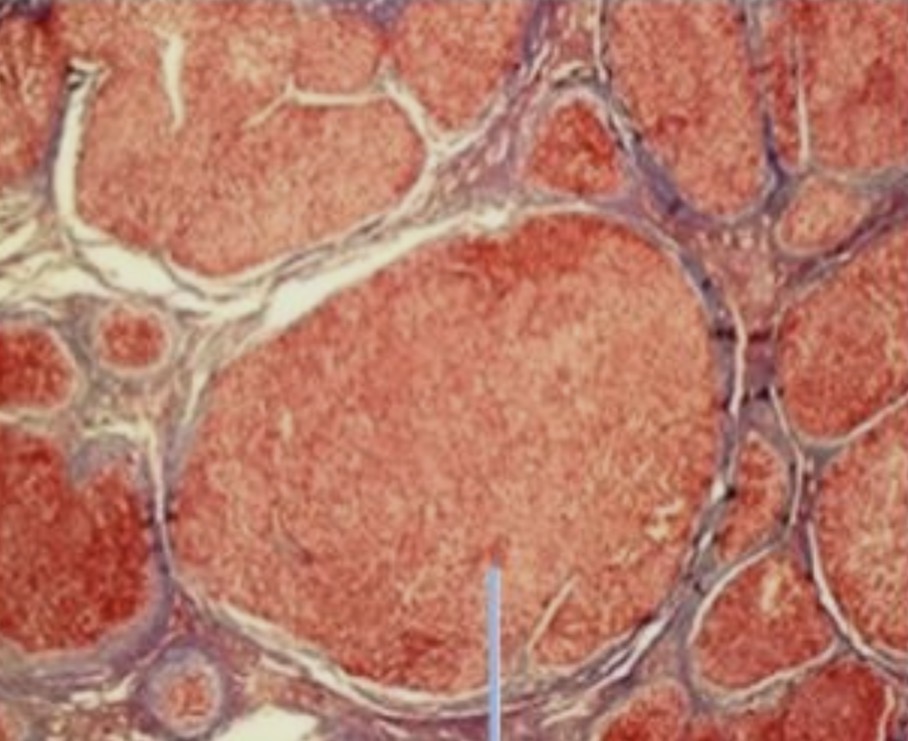
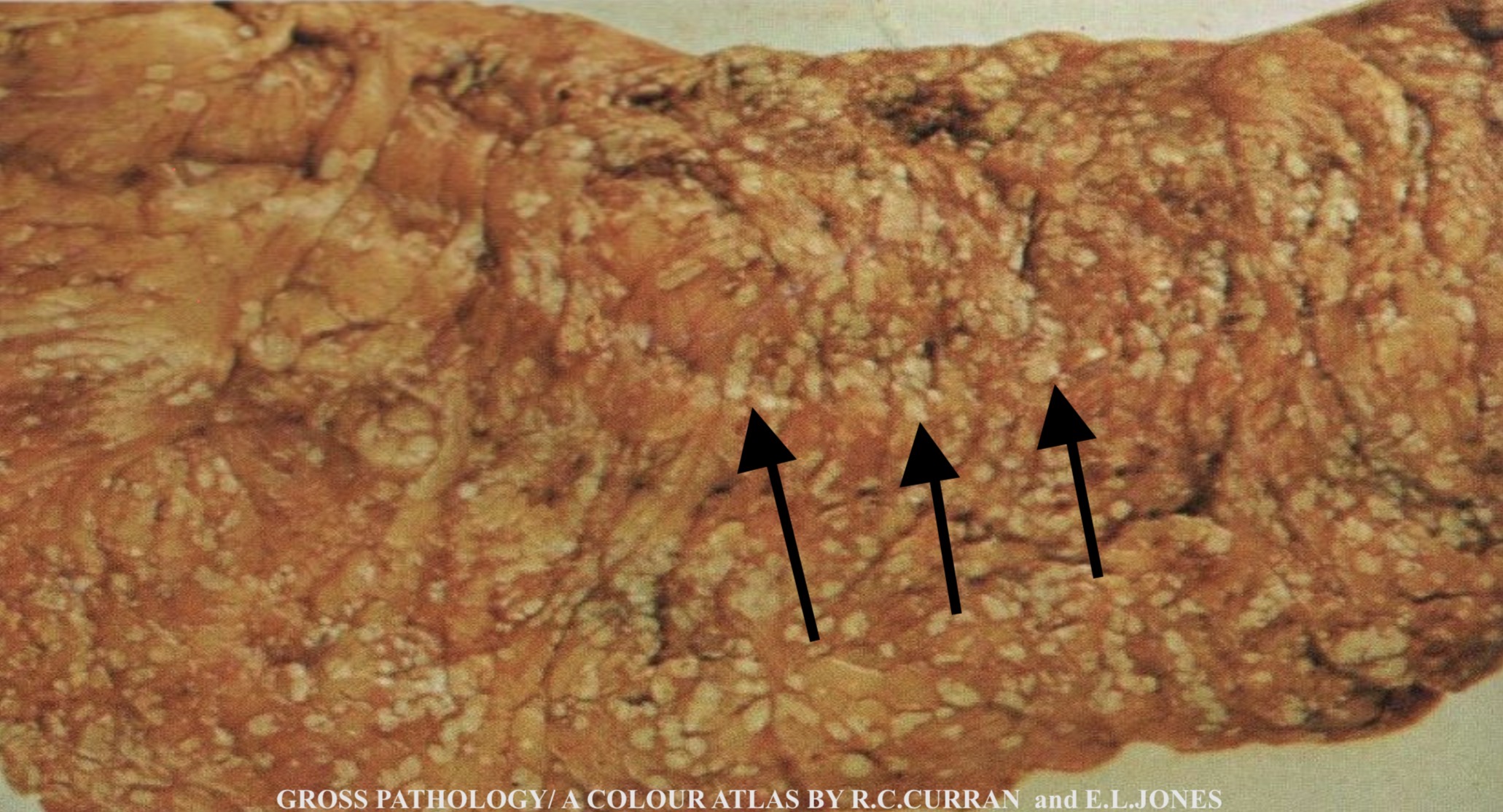
Micronodular Cirrhosis
The cut surface of the liver is diffusely nodular, the size of the nodules of regenerating hepatocytes is less than 3 mm in diameter , therefore called micronodular cirrhosis. The nodules are separated by bands of fibrous tissue
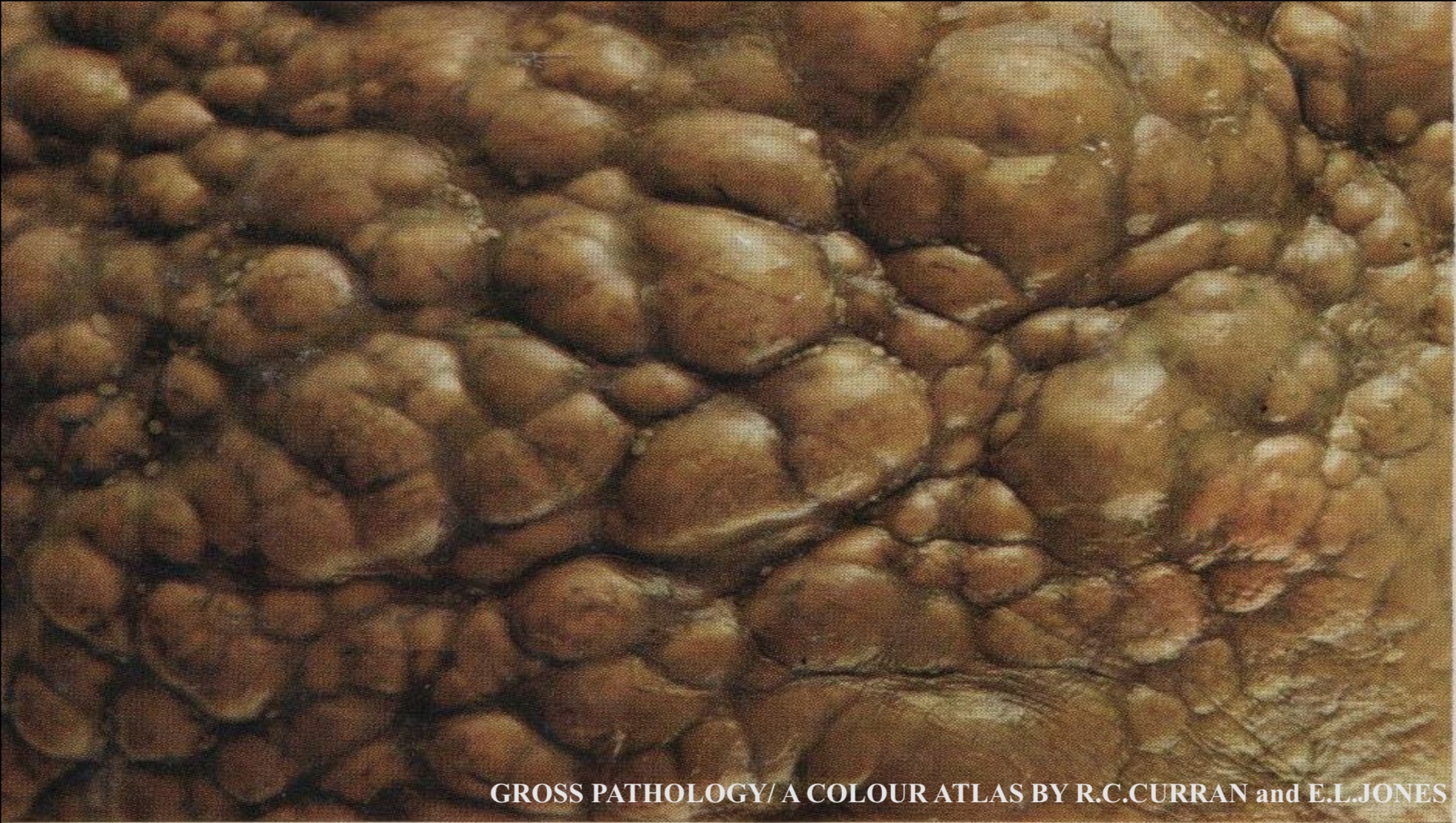
Macronodular Cirrhosis
The external surface of the liver is diffusely nodular , the size of the nodules of regenerating hepatocytes is equal or more than 3 mm in diameter (may reach up to 2 cm), therefore called macronodular cirrhosis. The nodules are separated by bands of fibrous tissue
The cirrhotic liver shows loss of normal liver architecture with fibrous septa dissecting the parenchyma into round nodules of regenerating hepatocytes (blue arrow
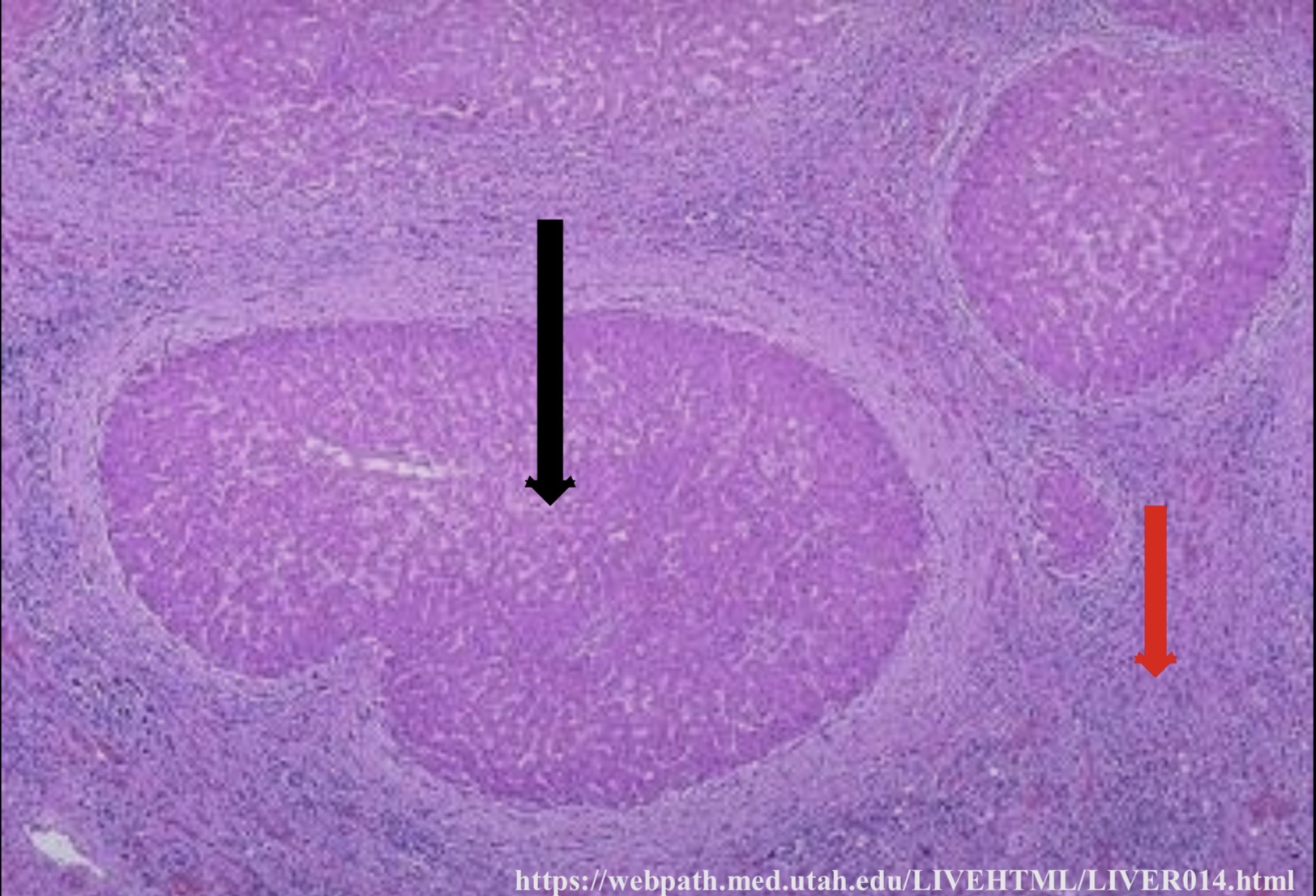
Liver Cirrhosis
The nodules of regenerating hepatocytes ( black arrow ) are surrounded by broad bands of fibrous tissue (red arrow) that connects between portal tracts. Chronic inflammatory cells are seen within the fibrous bands
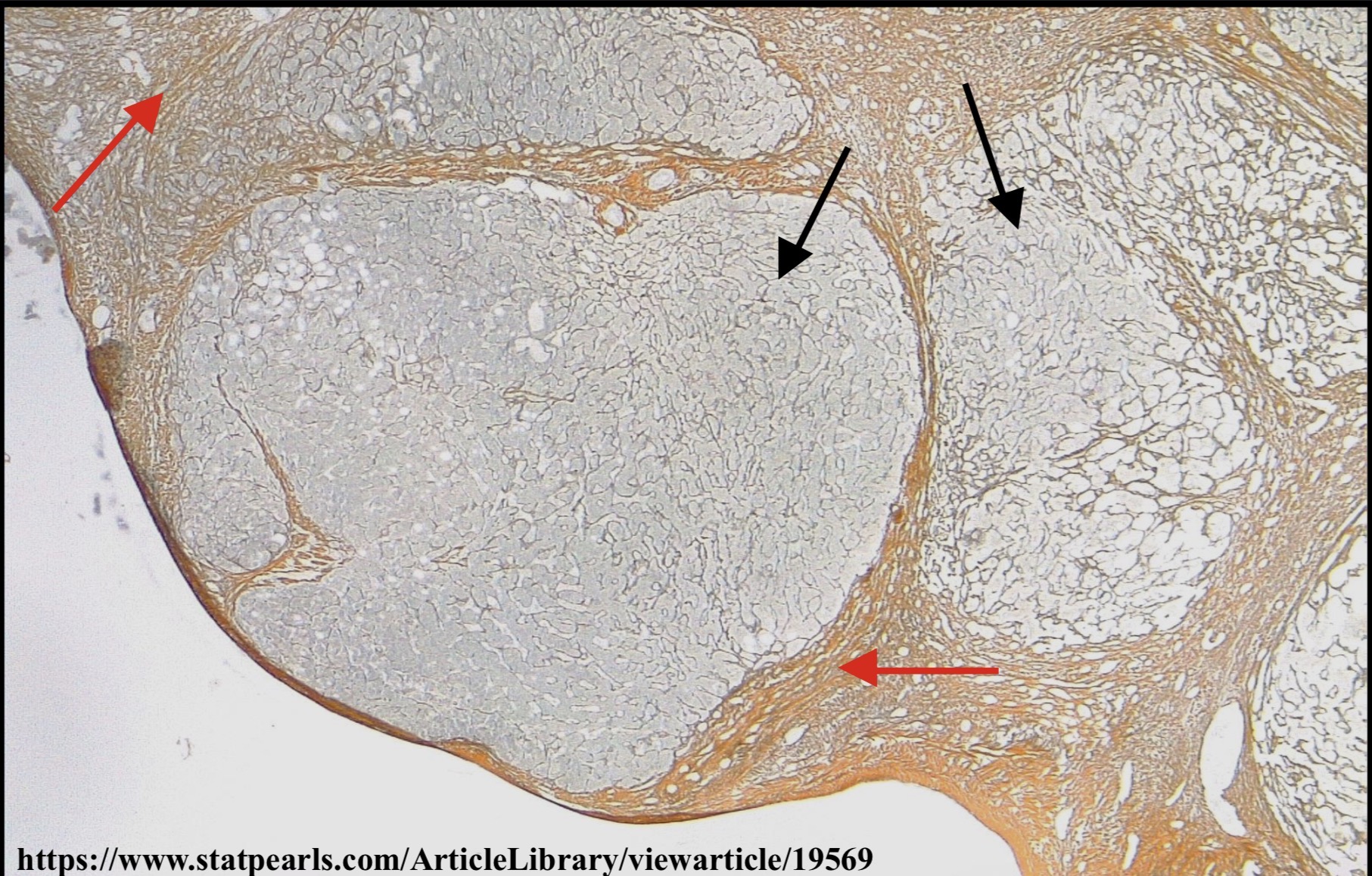
Liver Cirrhosis
This is a section of the liver stained by reticulin stain, showing loss of liver architecture with several pale well demarcated nodules of regenerating hepatocytes (black arrows) separated by wide bands of fibrous tissue ( red arrows)
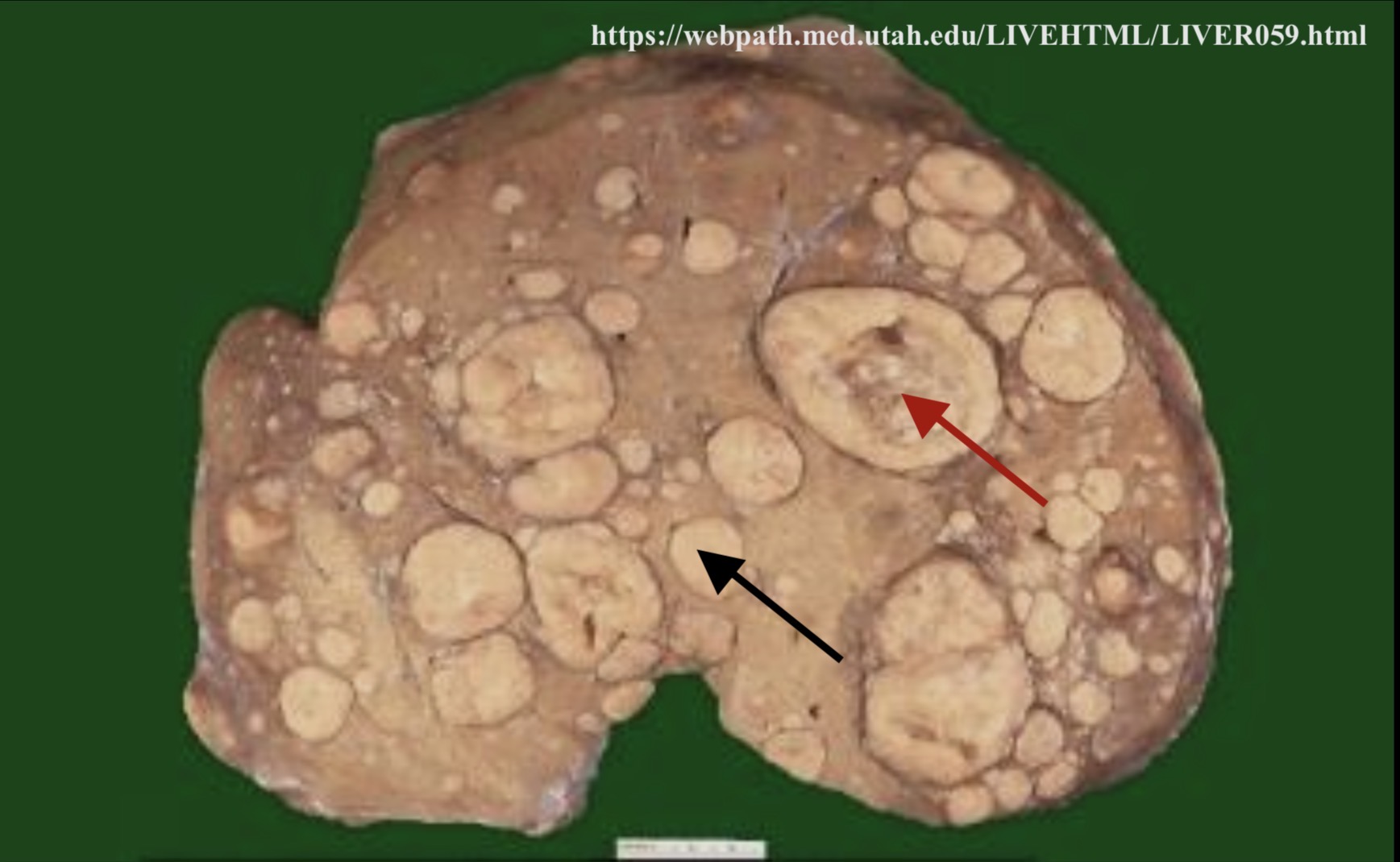
Secondary Carcinoma : Liver
The cut surface of the liver shows several yellowish nodules of variable sizes (black arrow). Some of the larger nodules show a central zone of necrosis (umbilication) ( red arrow). The nodules are metastases ( secondary carcinoma ) to the liver
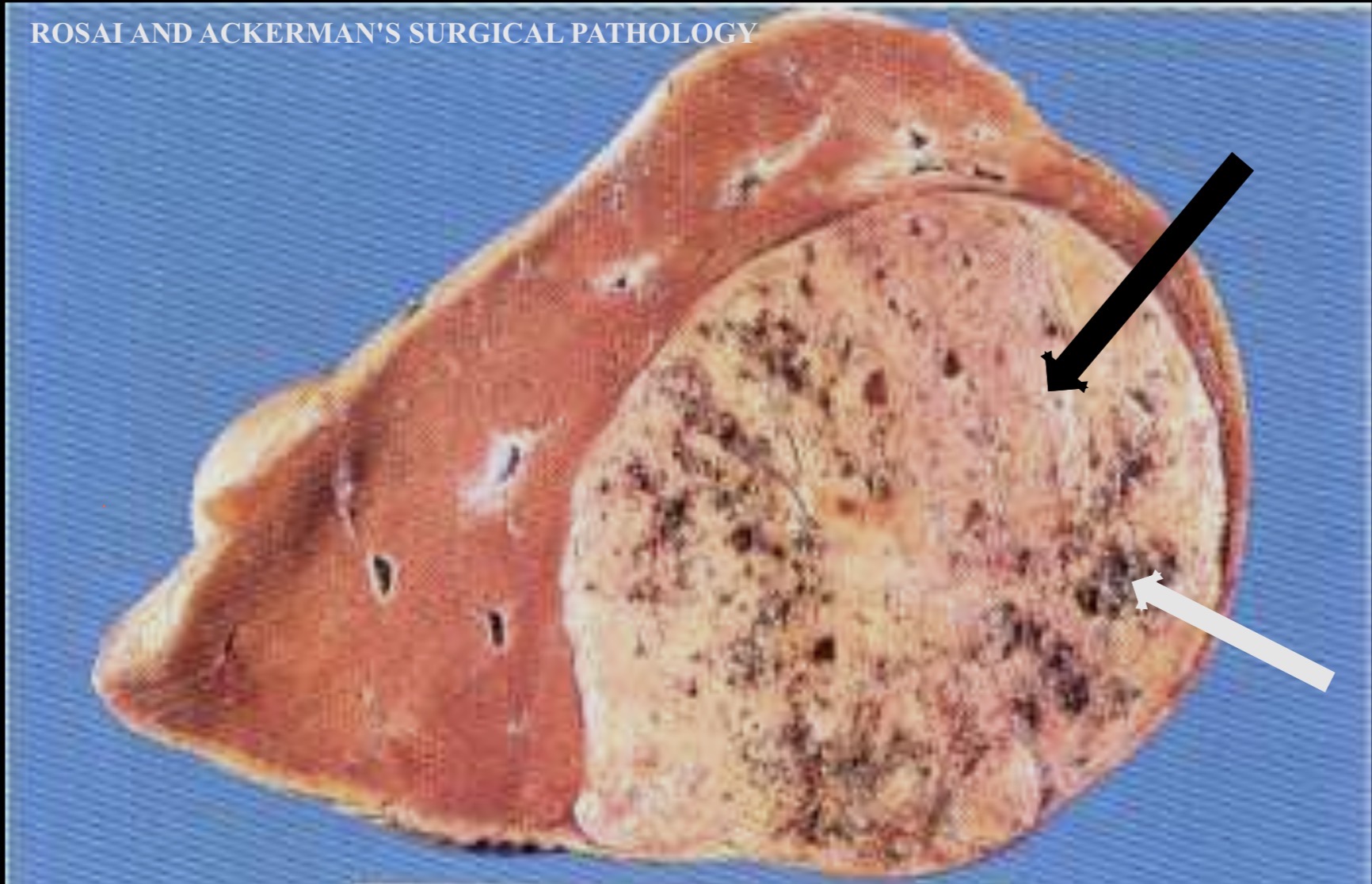
Hepatocellular Carcinoma: Liver
The liver shows a solitary well demarcated grey-whitish mass ( hepatocelluar carcinoma) ( black arrow) with multiple small hemorrhagic areas (white arrow)
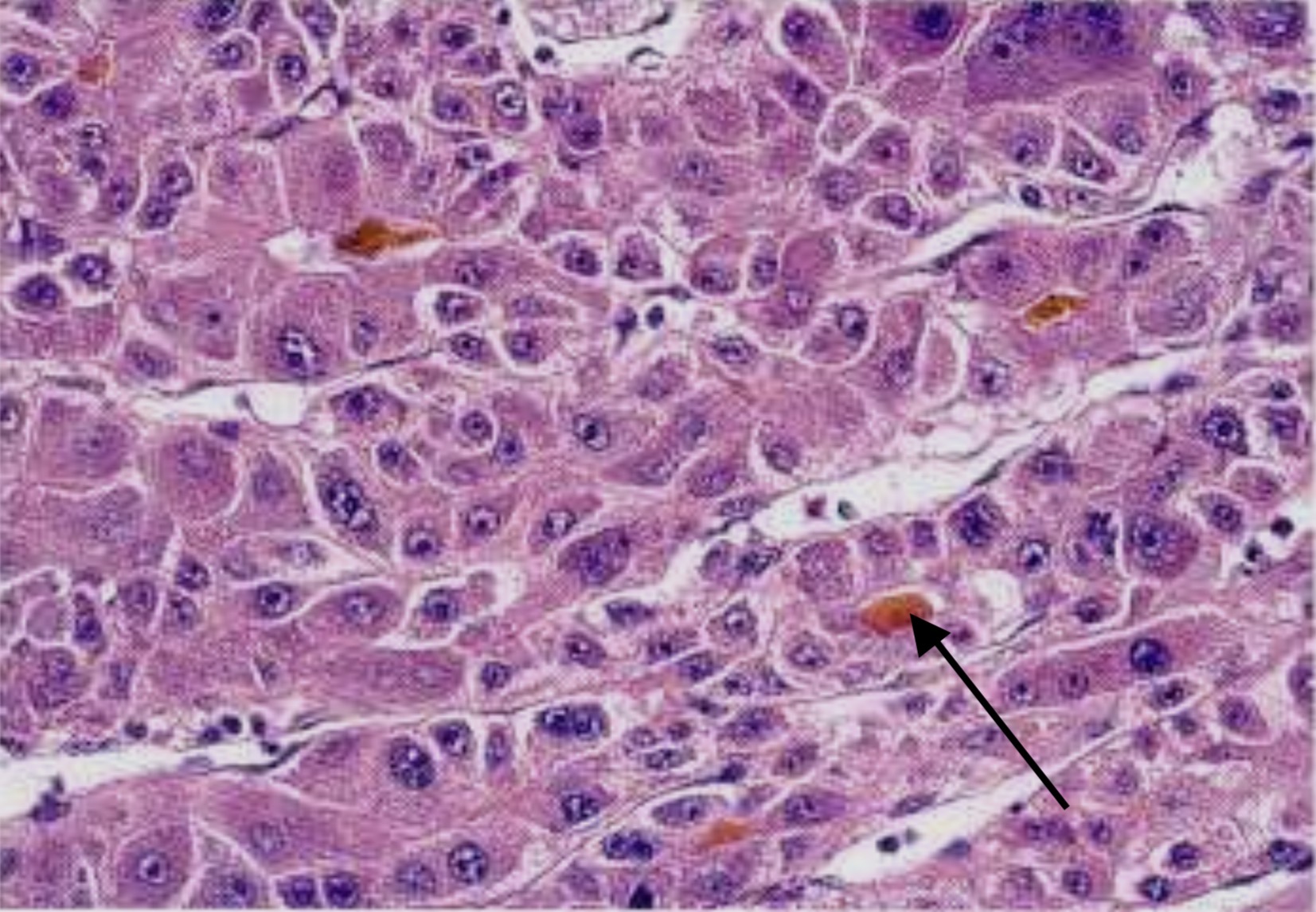
Hepatocellular Carcinoma : Liver
The malignant hepatocytes are arranged in the form of trabeculae, showing features of nuclear atypia and bile production (black arrow).
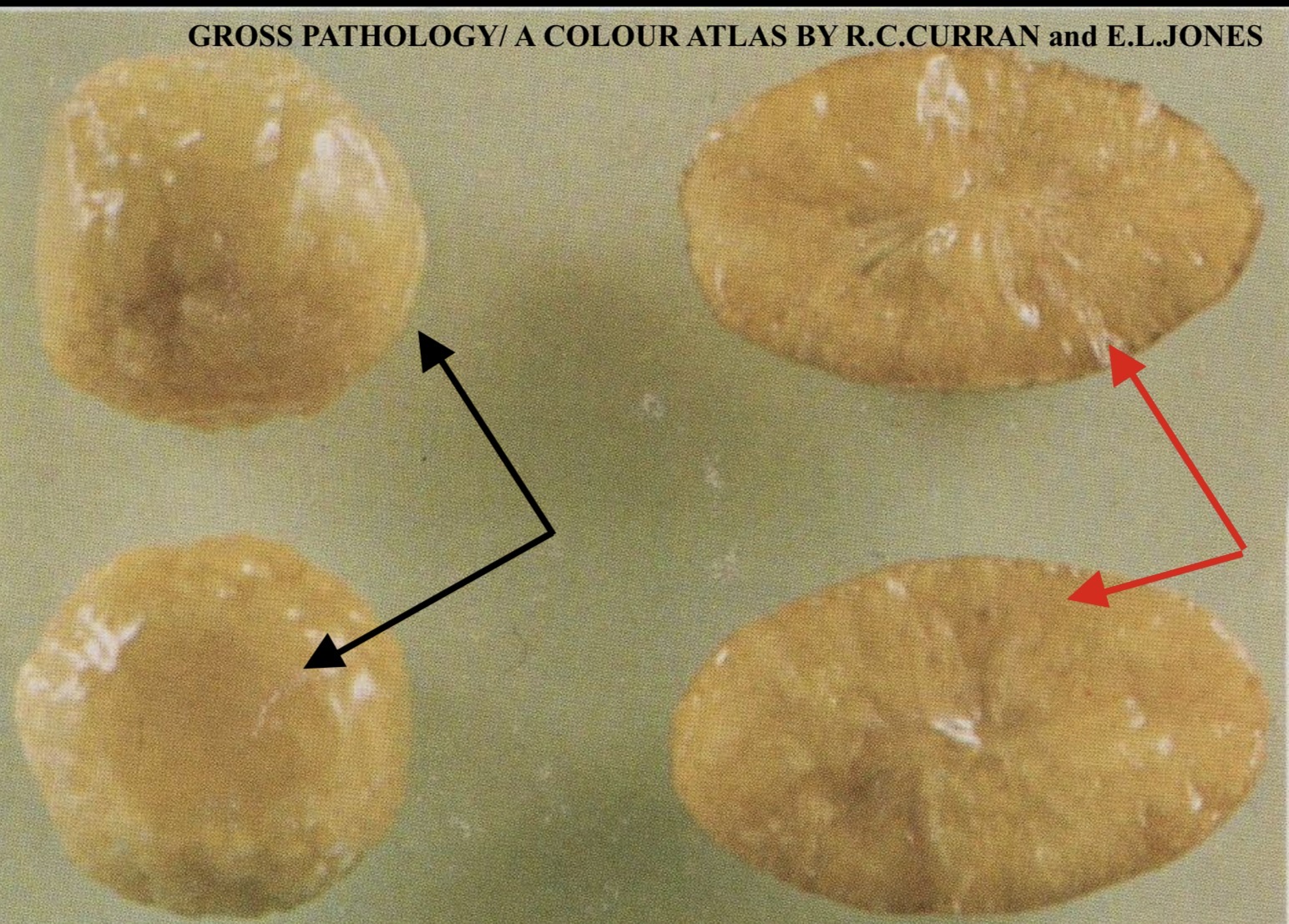
Cholesterol gall stones
These are three pure cholesterol stones: the two spherical stones (black arrows) have a nodular surface and are yellowish in color, while the oval shaped stone (red arrows) has been bisected showing a yellow material (radiating cholesterol crystals ).

Cholesterol gall stones: Gall bladder
The wall of the gall bladder is thick and fibrotic due to chronic cholecystitis. The lumen contains multiple yellowish brown stones with faceted surfaces

Pigment gall Stones: Gall Bladder
The gall bladder is distended and contains several faceted black pigmented gall stones.
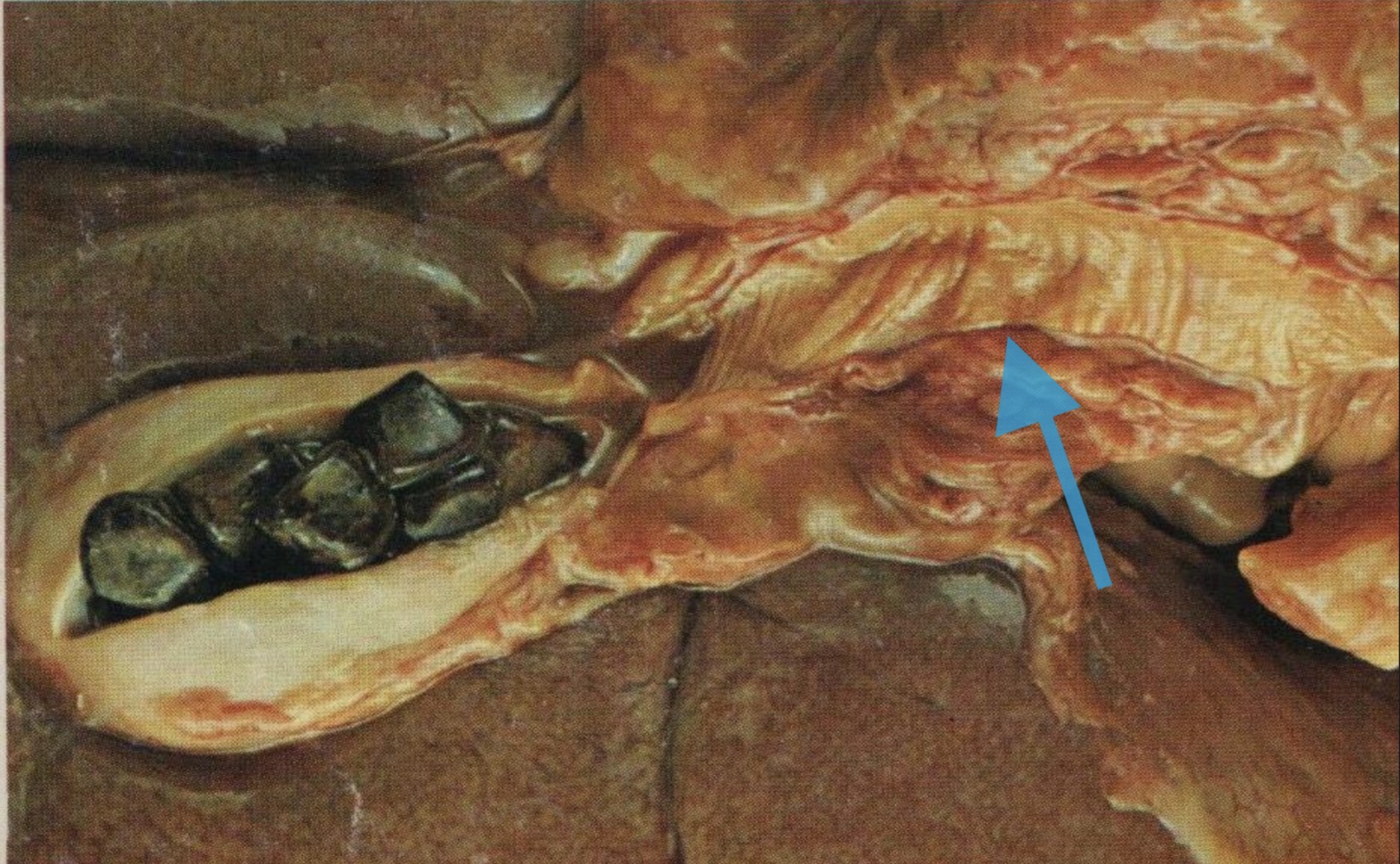
Chronic Cholecystitis and Cholelithiasis
The figure shows the inferior surface of the liver, gall bladder and common bile duct . The gall bladder is contracted with a thickened , fibrosed wall, the lumen is full with several facetted gall stones . The common bile duct is dilated (blue arrow
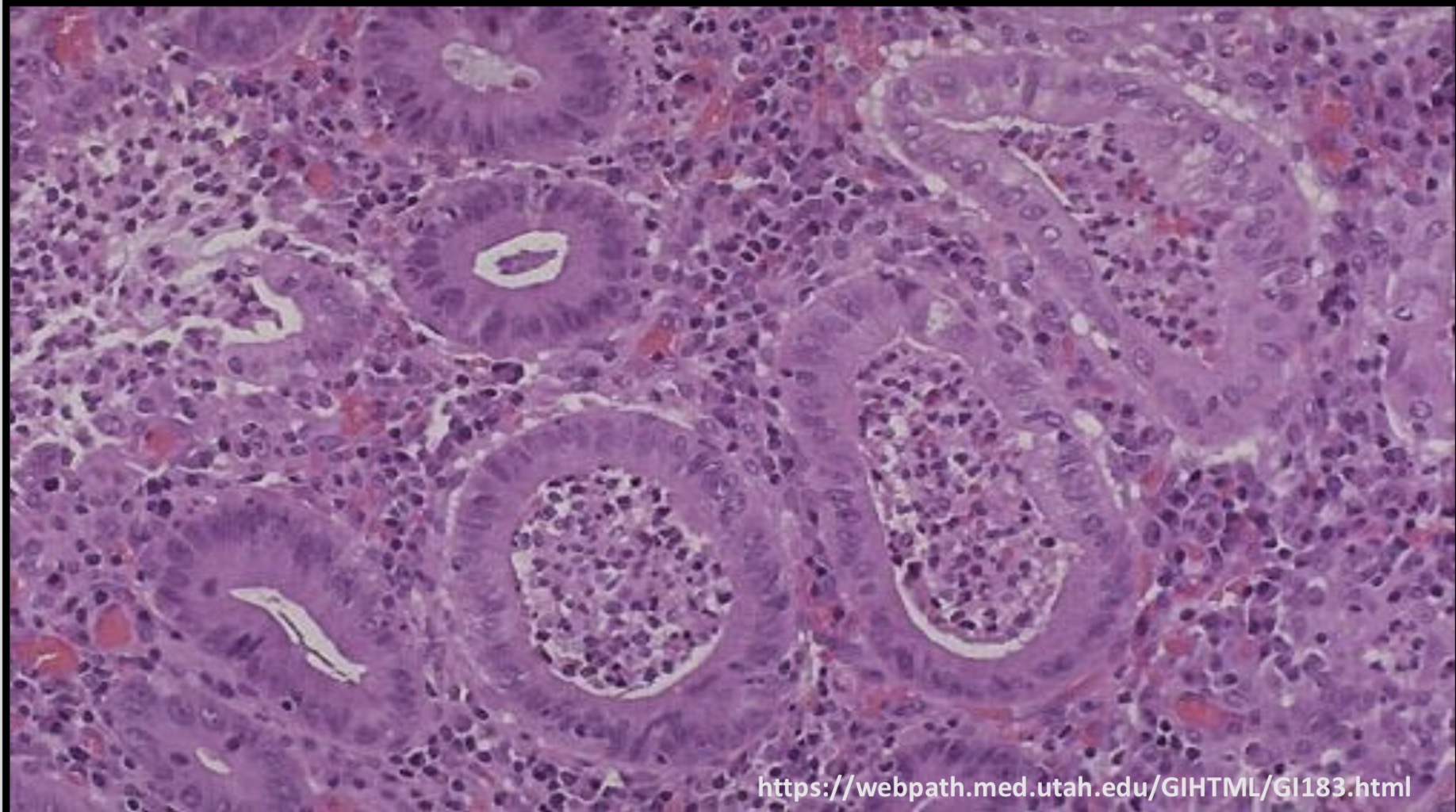
Chronic Cholecystitis: Gall Bladder
The mucosa is chronically inflamed with dense chronic inflammatory cells infiltration through the wall (red arrow) . The elongated glands are lined by a single layer of columnar cells ( black arrow), and the muscle coat is hypertrophied and thick (blue arrow). There is slight increase in the amount of fibrous tissue.

Chronic Cholecystitis : Gall Bladder
The mucosa shows irregular mucosal folds with chronic inflammatory cells infiltration through the wall, muscle coat hypertrophy and fibrosis (black arrows). Rokitansky-Aschoff sinuses ( herniations of the mucosal epithelium through the wall) are present (blue arrow)
Acute Hemorrhagic Pancreatitis: Omentum
The greater omentum is covered with small yellow-white foci of fat necrosis (arrows)
Squamous Cell Carcinoma: Uterine Cervix
Irregular ulcerative papillary growth within the uterine cervix
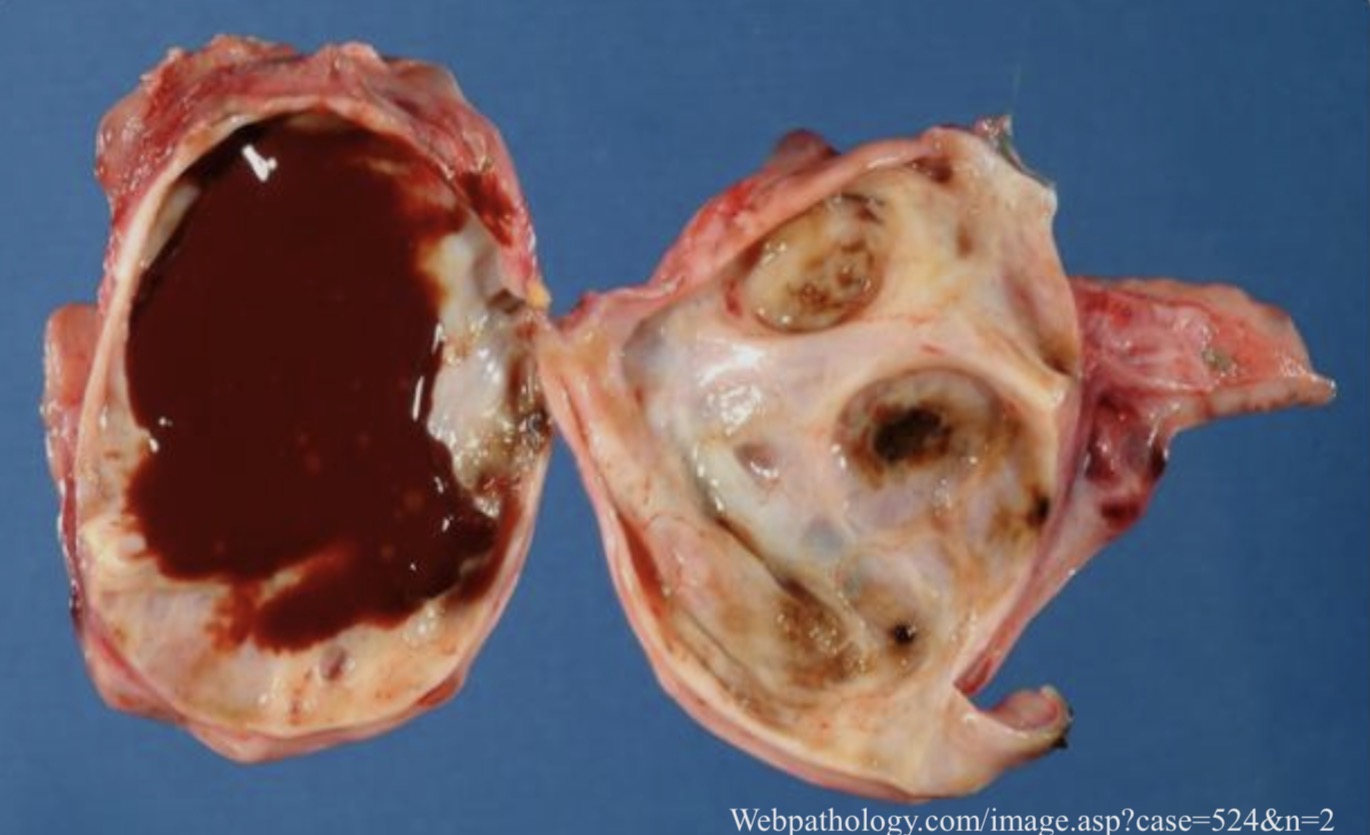
Endometriosis : Ovary (Chocolate Cyst)
Thin-walled cyst filled with altered blood
Endometriosis : Ovary
Part of the cystic wall within the ovary lined by endometrial epithelium with endometrial gland (thick arrow) surrounded by fresh bright red hemorrhage and cellular stroma (thin arrow). Brown debris of old hemorrhage is present within the lumen of the cyst (double arrow)
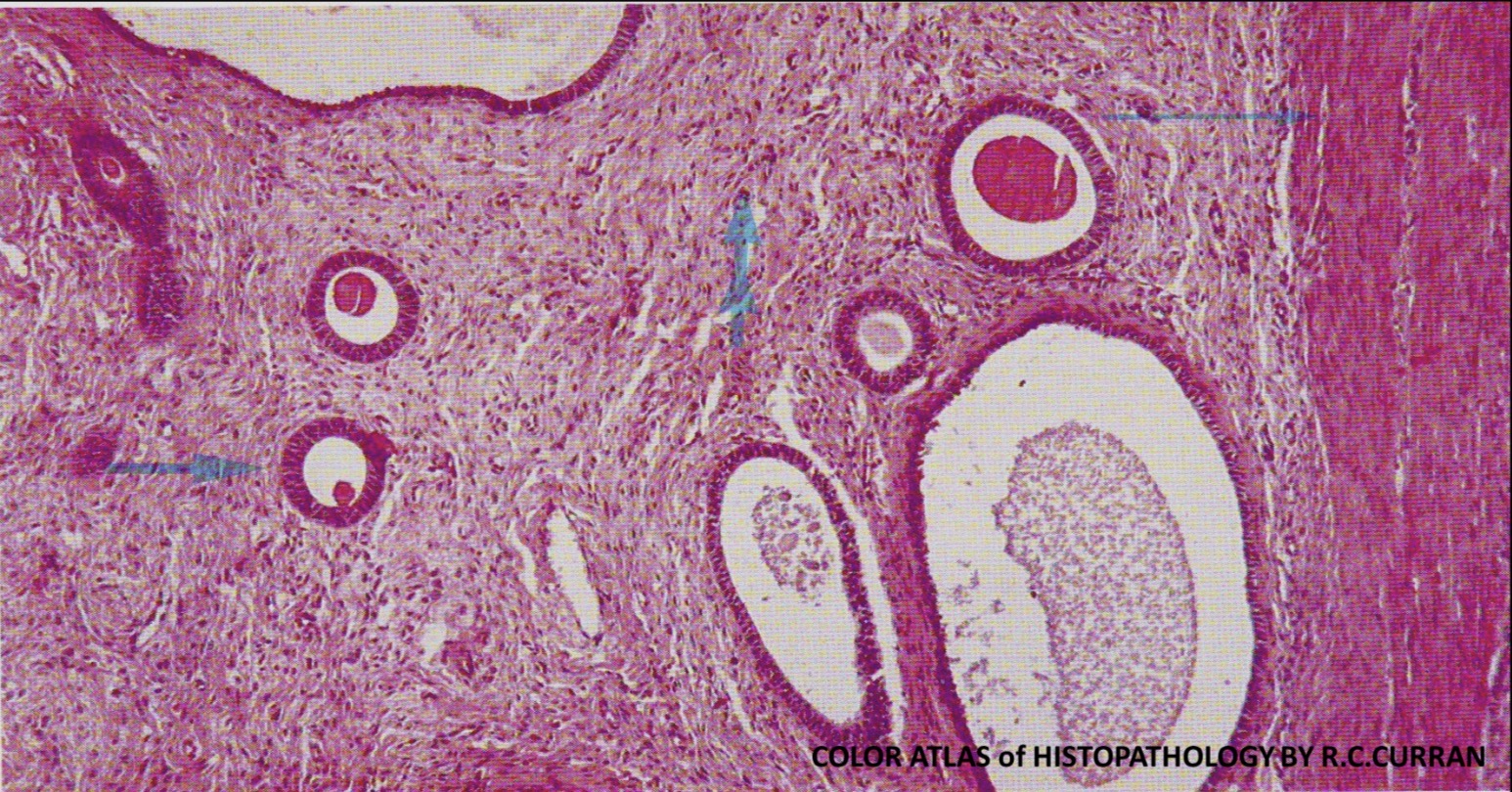
Adenomyosis : Uterus
Thick muscular coat of the myometrium is seen on the right (thin arrow), there is endometrial tissue which consists of cellular fibrillary stroma (double arrow) and endometrial glands (thick arrow)
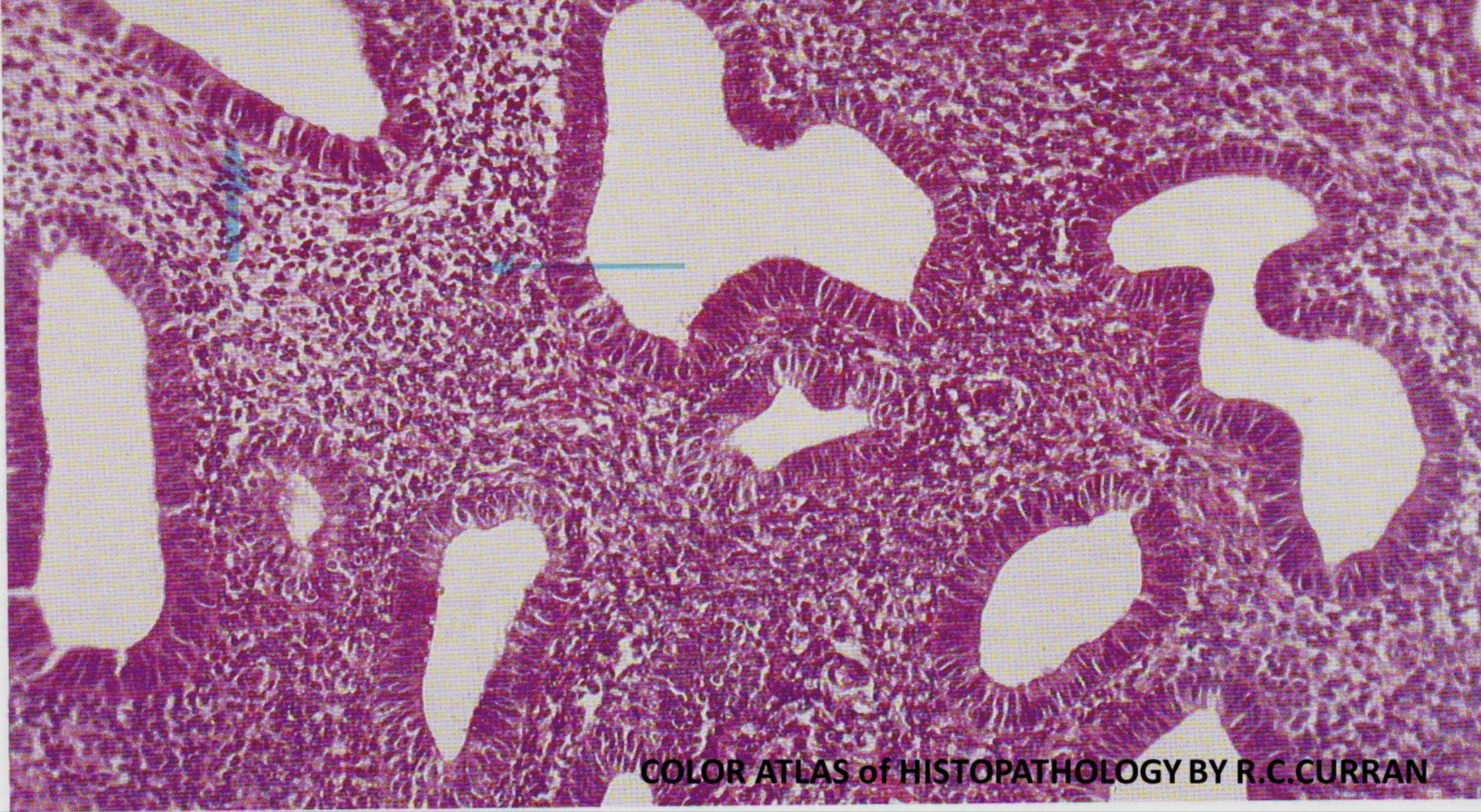
Endometrial hyperplasia without atypia: Uterus
The endometrial glands are cystically dilated lined by single layer of pseudosratified columnar epithelium (thick arrow). The stroma is highly cellular (thin arrow). No evidence of cellular atypia

Endometrial Carcinoma: Uterus
Exophytic, friable gray nodular mass projecting from the endometrium within the fundus of the uterus
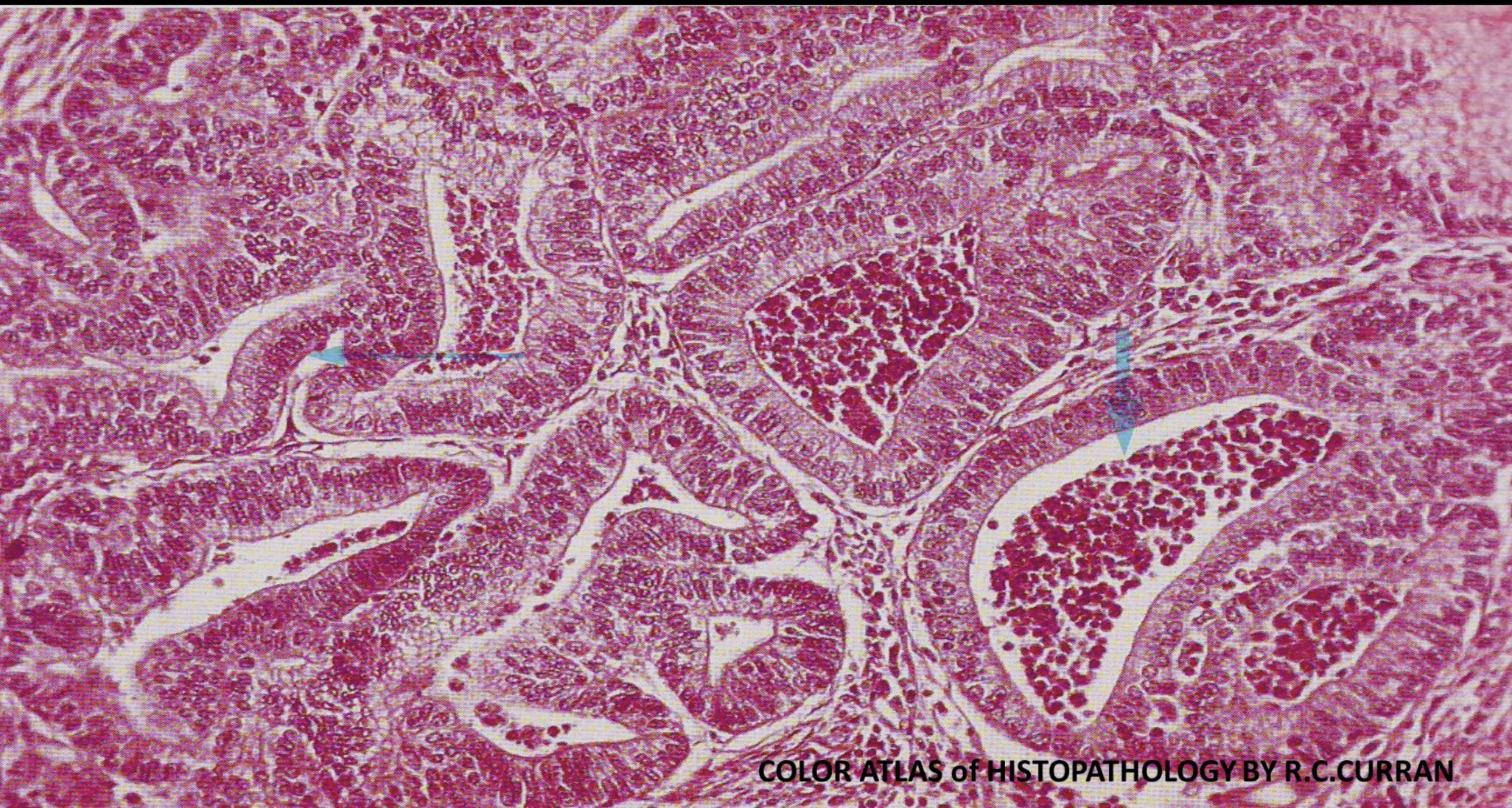
Primary Adenocarcinoma: Endometrium
Abnormal glands arranged back to back, lined by malignant columnar epithelium (thin arrow). The glands contain necrotic debris (thick arrow) Scanty stroma is present in between the glands

Serous Cystadenoma : Ovary
Solitary thin walled cyst, smooth surface, filled with clear serous flui
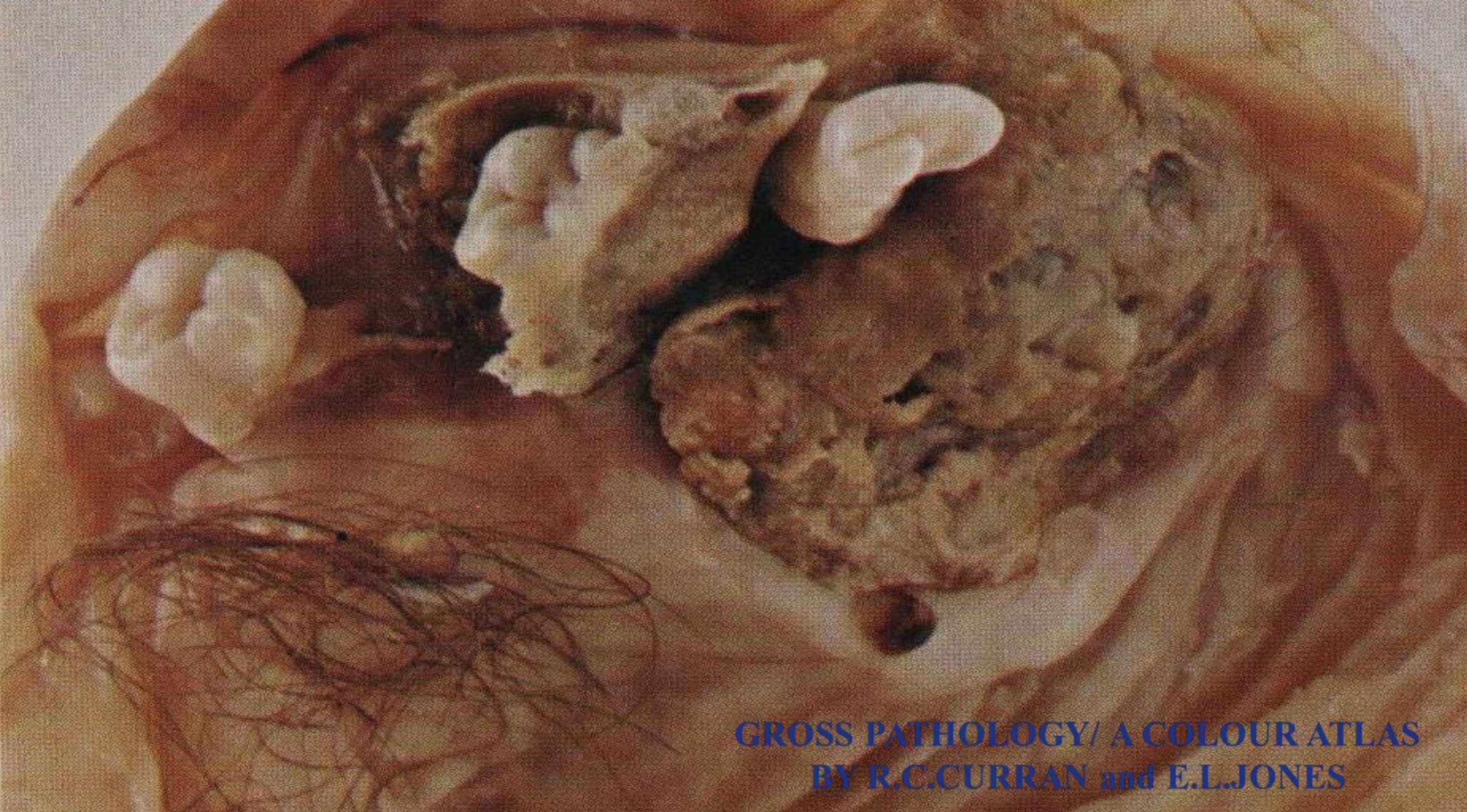
Benign Mature Cystic Teratoma (Dermoid Cyst): Ovary
Unilocular cyst containing hair and yellowish-brown sebaceous material with three teeth
Benign Mature Cystic Teratoma (Dermoid Cyst): Ovary
Unilocular cyst containing hair and yellowish-brown sebaceous material with three teeth

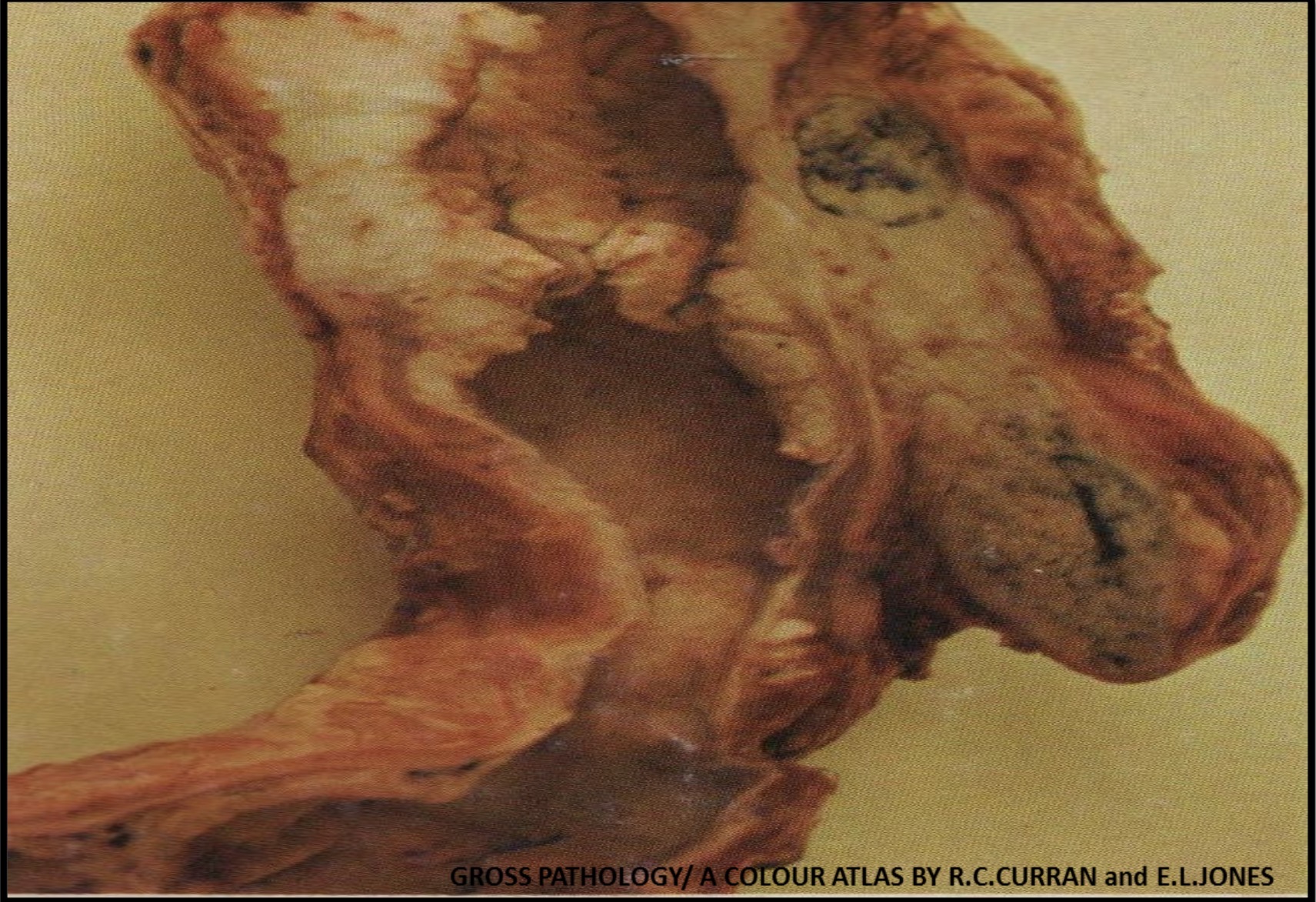
Hydatidiform Mole: Placenta
Abnormal friable mass consists of translucent cystic vesicles containing clear watery fluid (hydrobic villi) which appear as grape-like structure
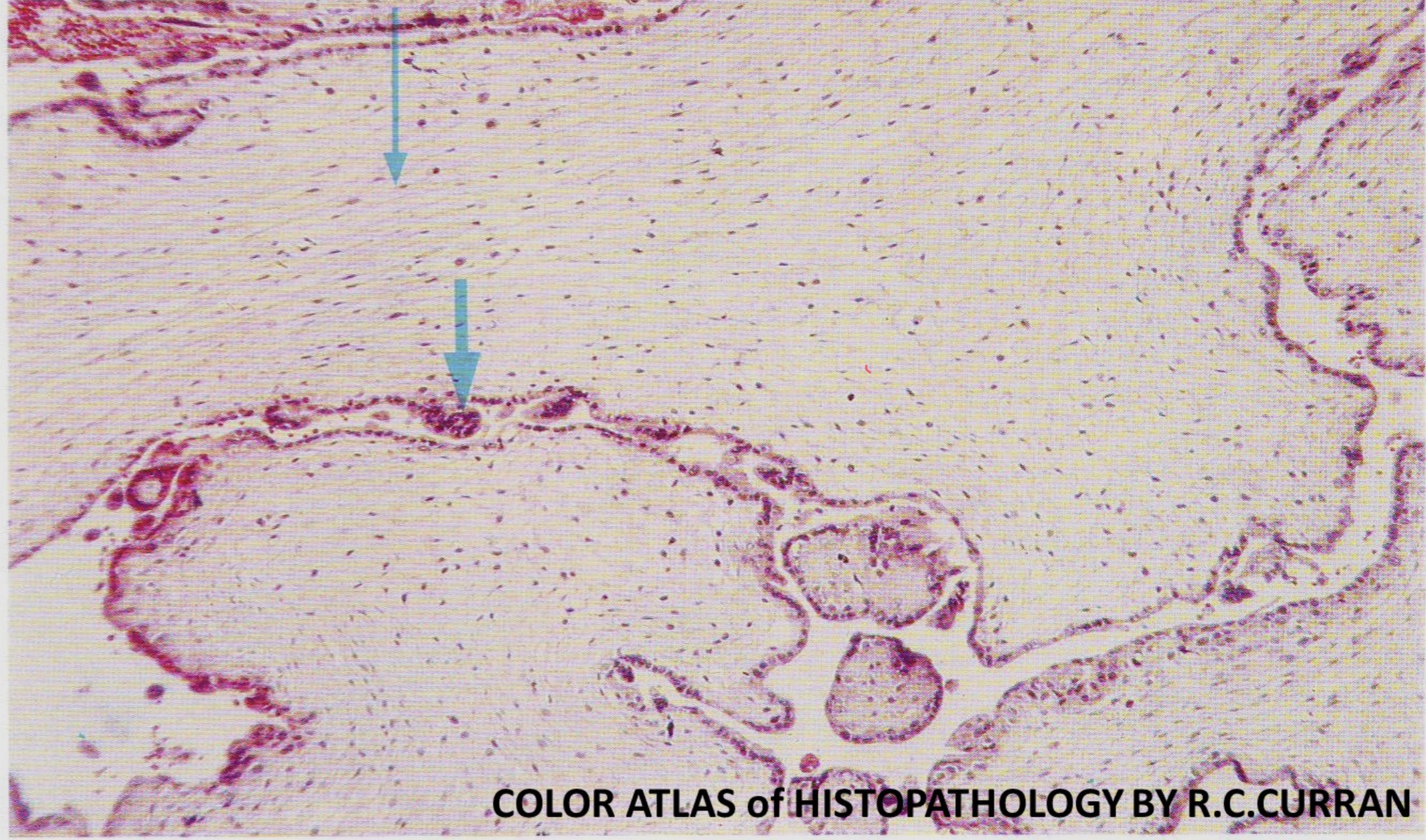
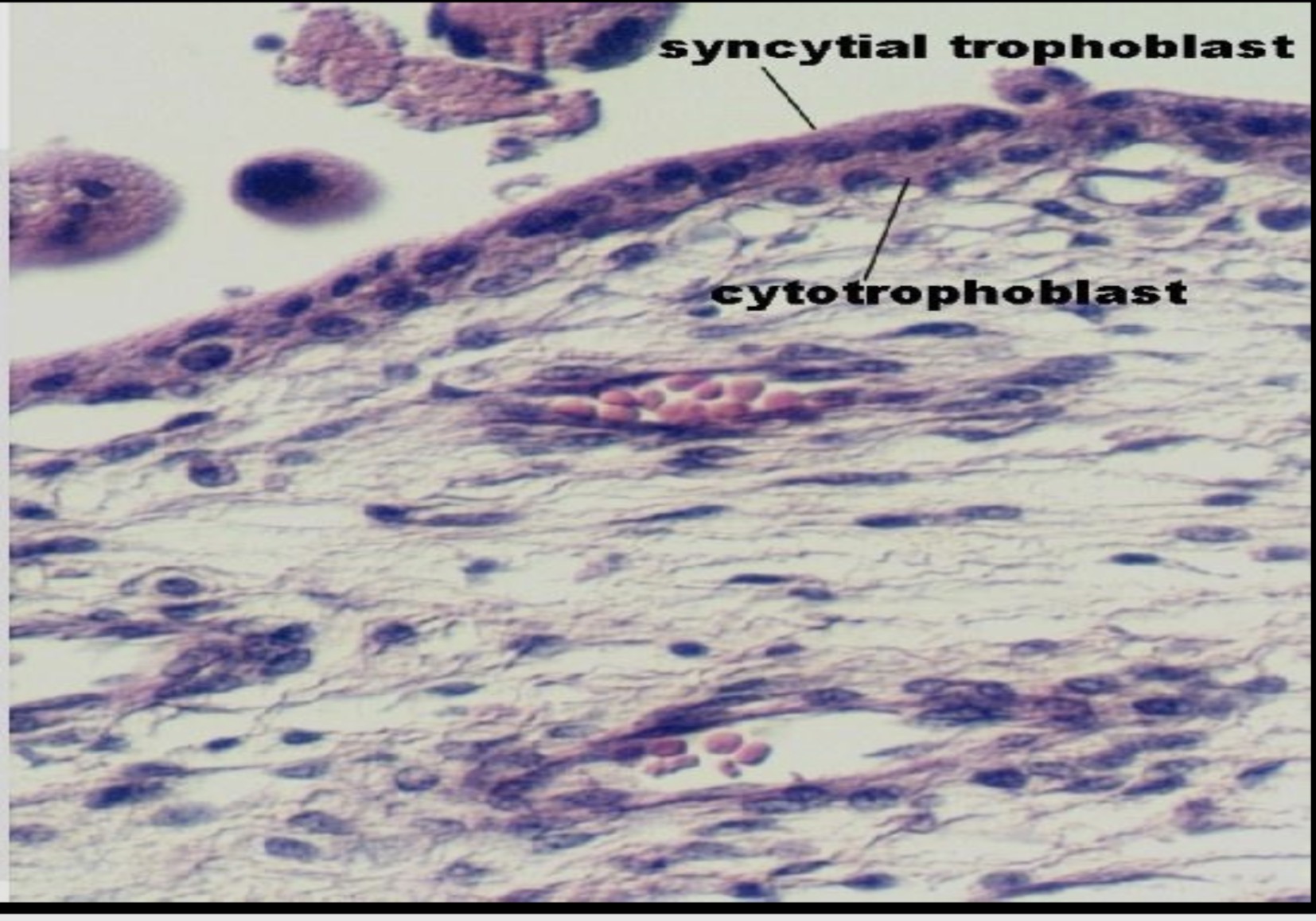
Hydatidiform Mole: Placenta
Cystically dilated chorionic villi with loose edematous connective tissue core ( thin arrow) with no fetal blood vessels. There is proliferation of both cyto- and syncytiotrophoblasts (thick arrow)
Squamous Cell Carcinoma: Esophagus
The middle and lower third of the esophagus are encircled by an annular constricting growth, with extension through the wall, and infiltration of the serosa. Two adjacent lymph nodes on the right are enlarged due to the metastatic carcinoma
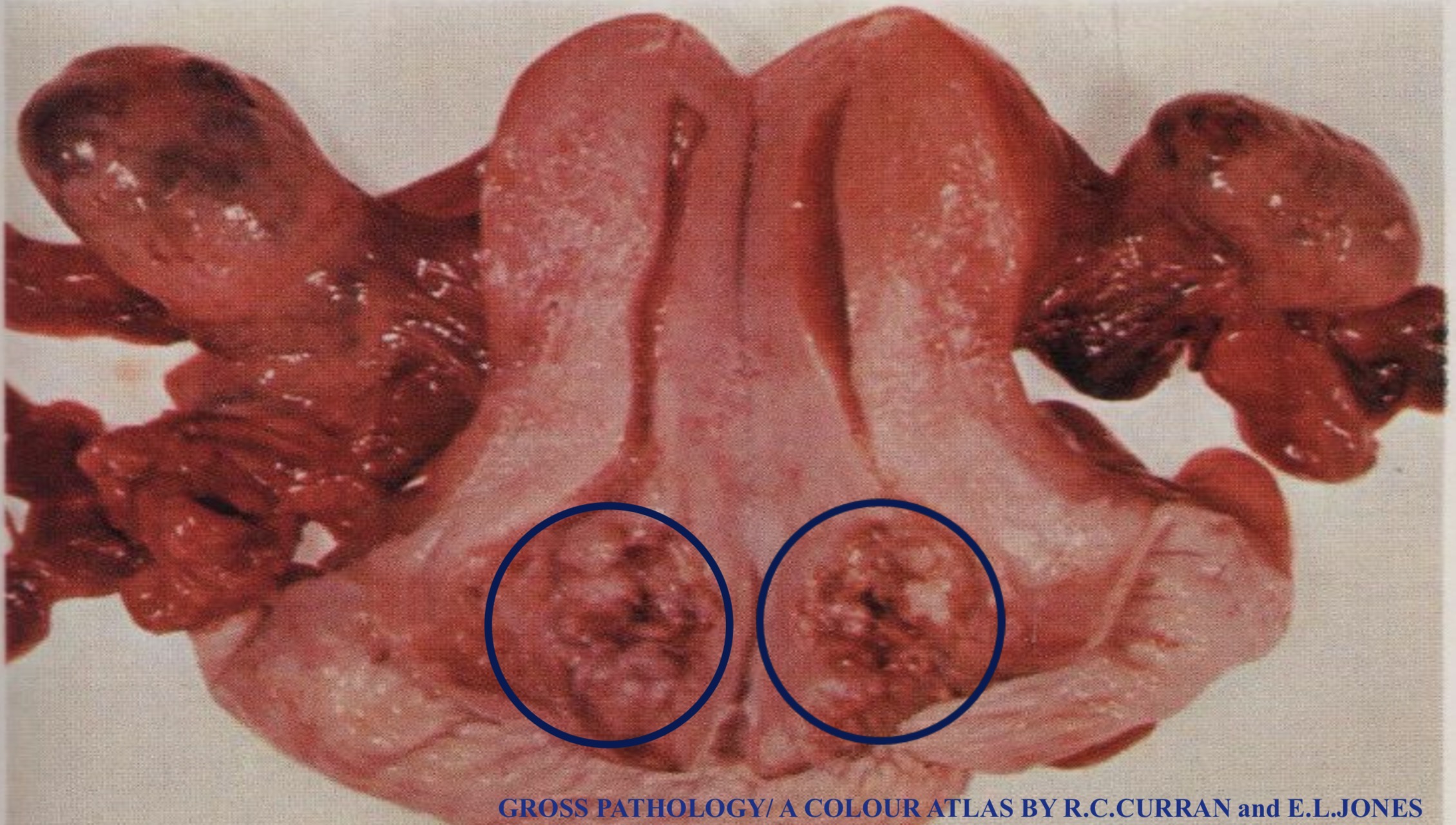
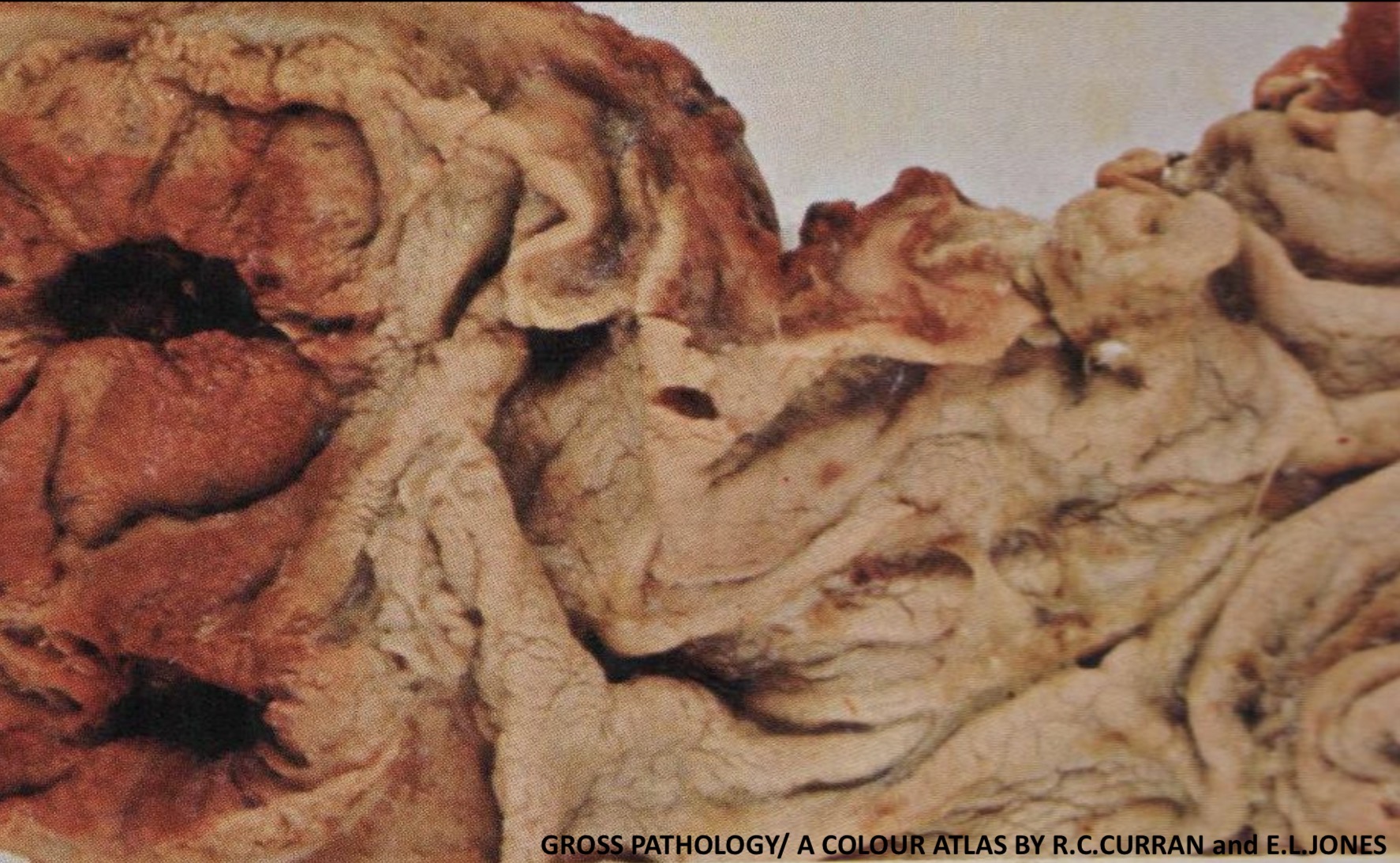
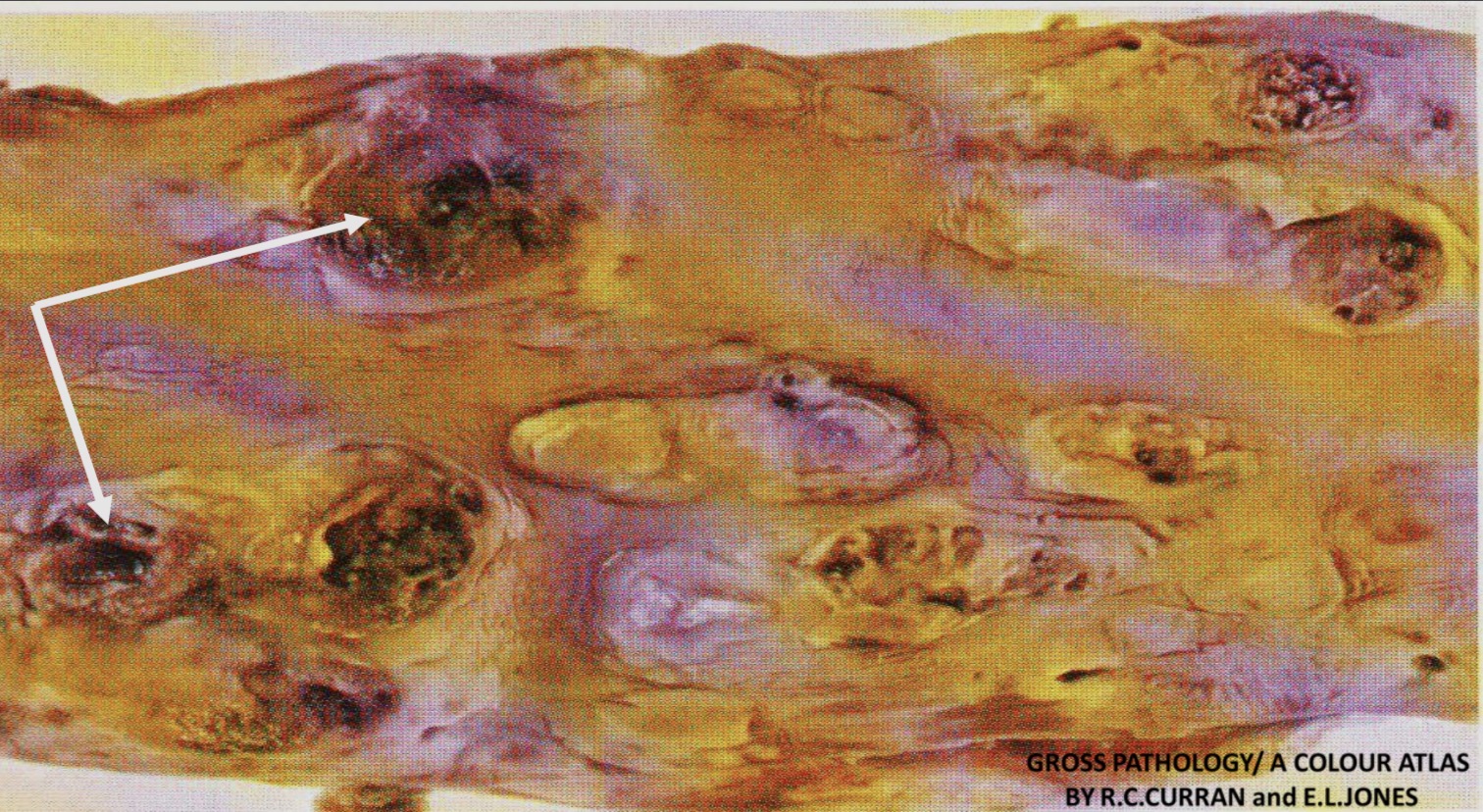
Acute ( Stress ) Ulcers: Stomach
Two acute stress ulcers, small, superficial, multiple, which are situated in the fundus of the stomach (cushing ulcers)
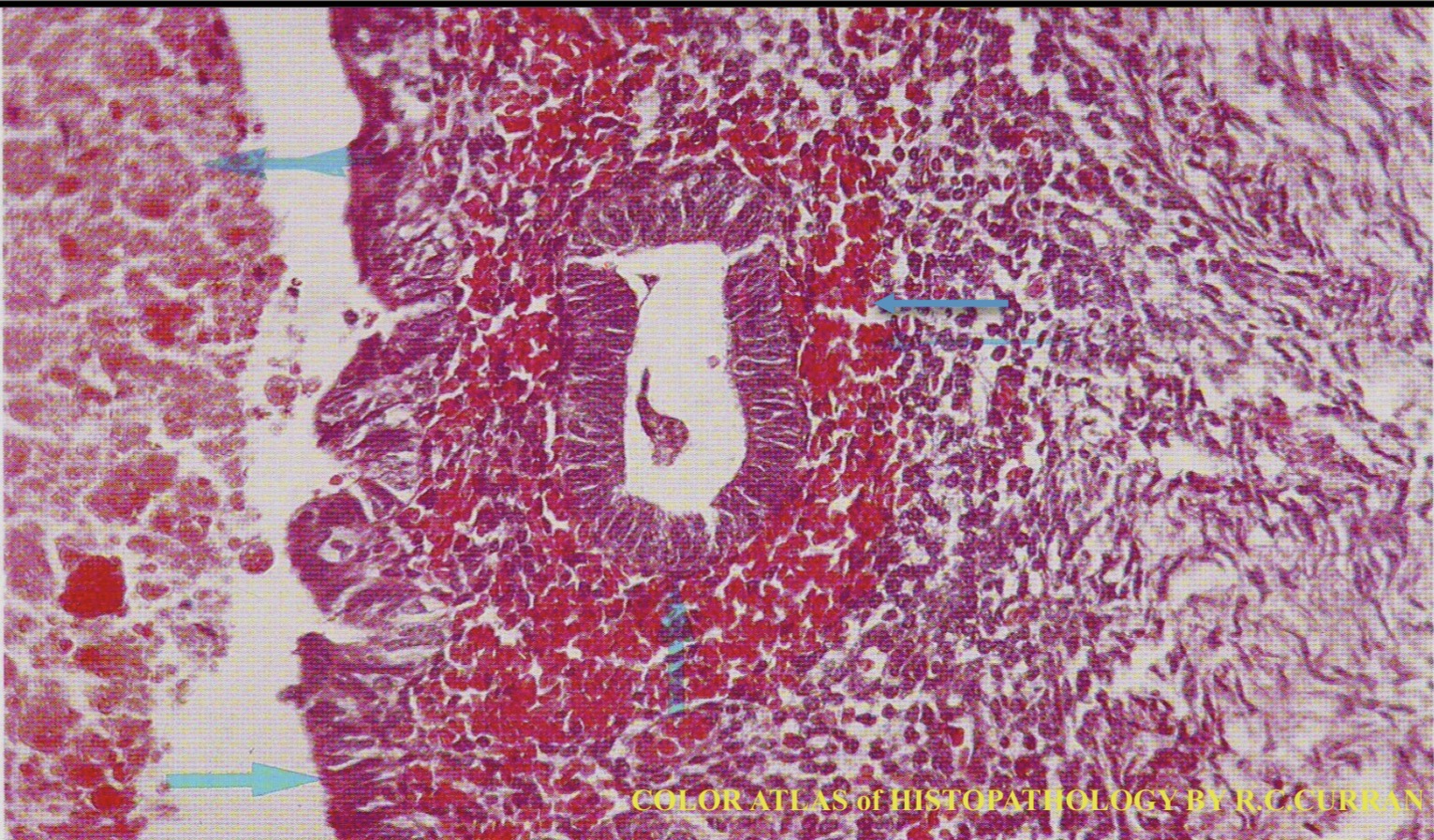
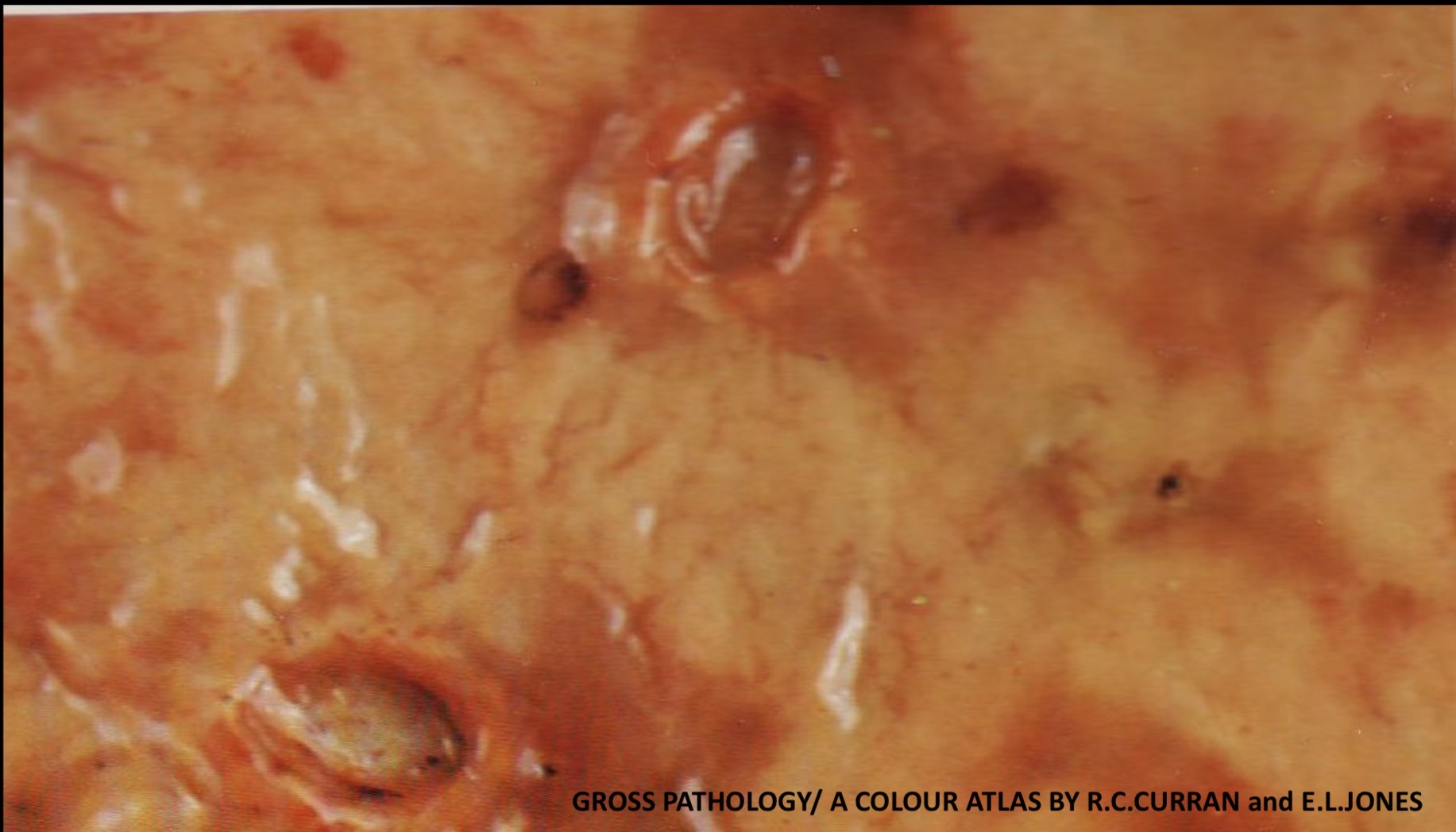
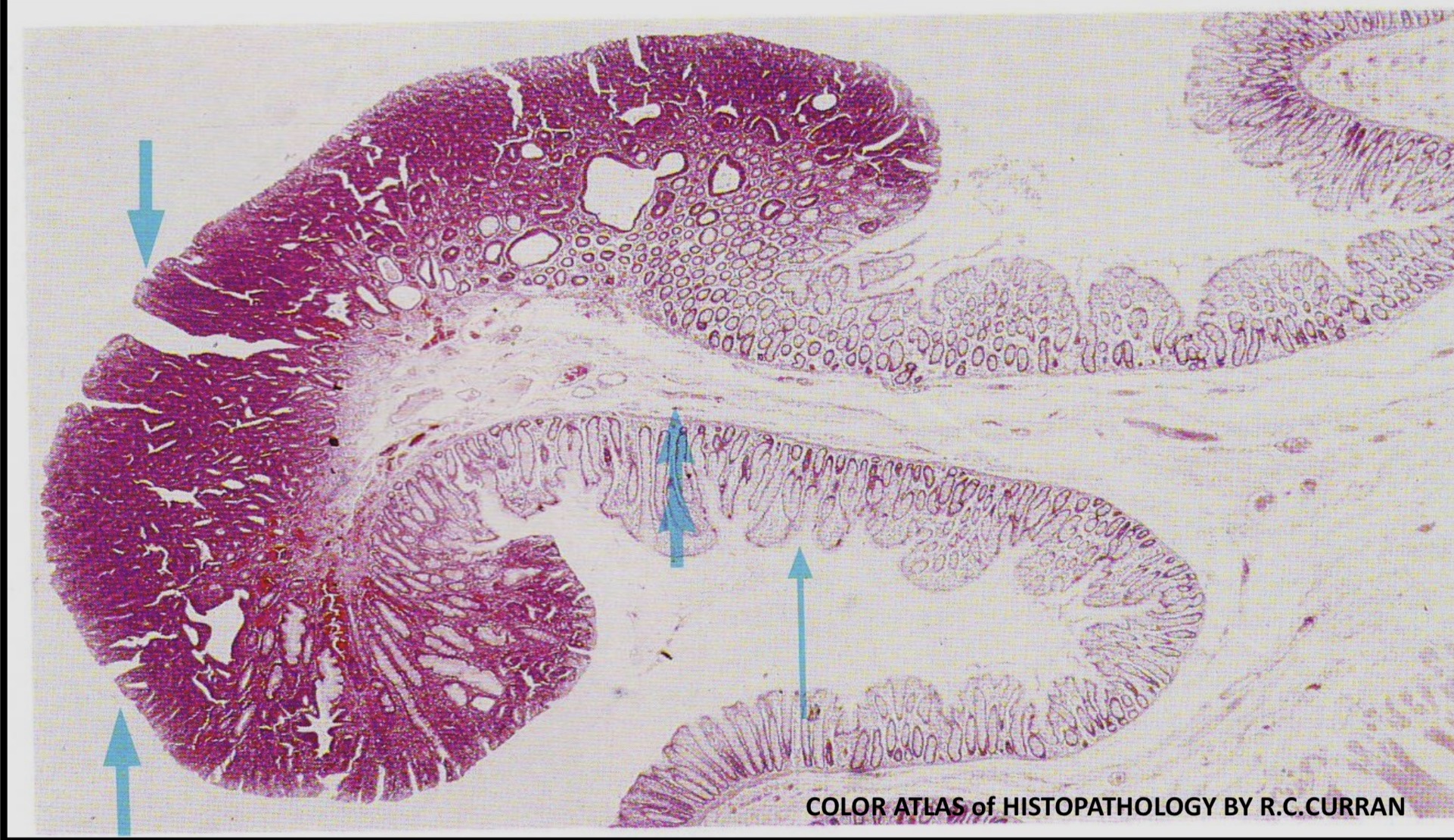
Chronic Peptic Ulcer: Stomach
A chronic peptic ulcer is present on the lesser curvature of the stomach ,the ulcer crater is oval and the base is covered with a greenish-yellow slough consisting of necrotic granulation tissue, the folds of mucosa are radiating from the ulcer. Later on healing is by fibrosis
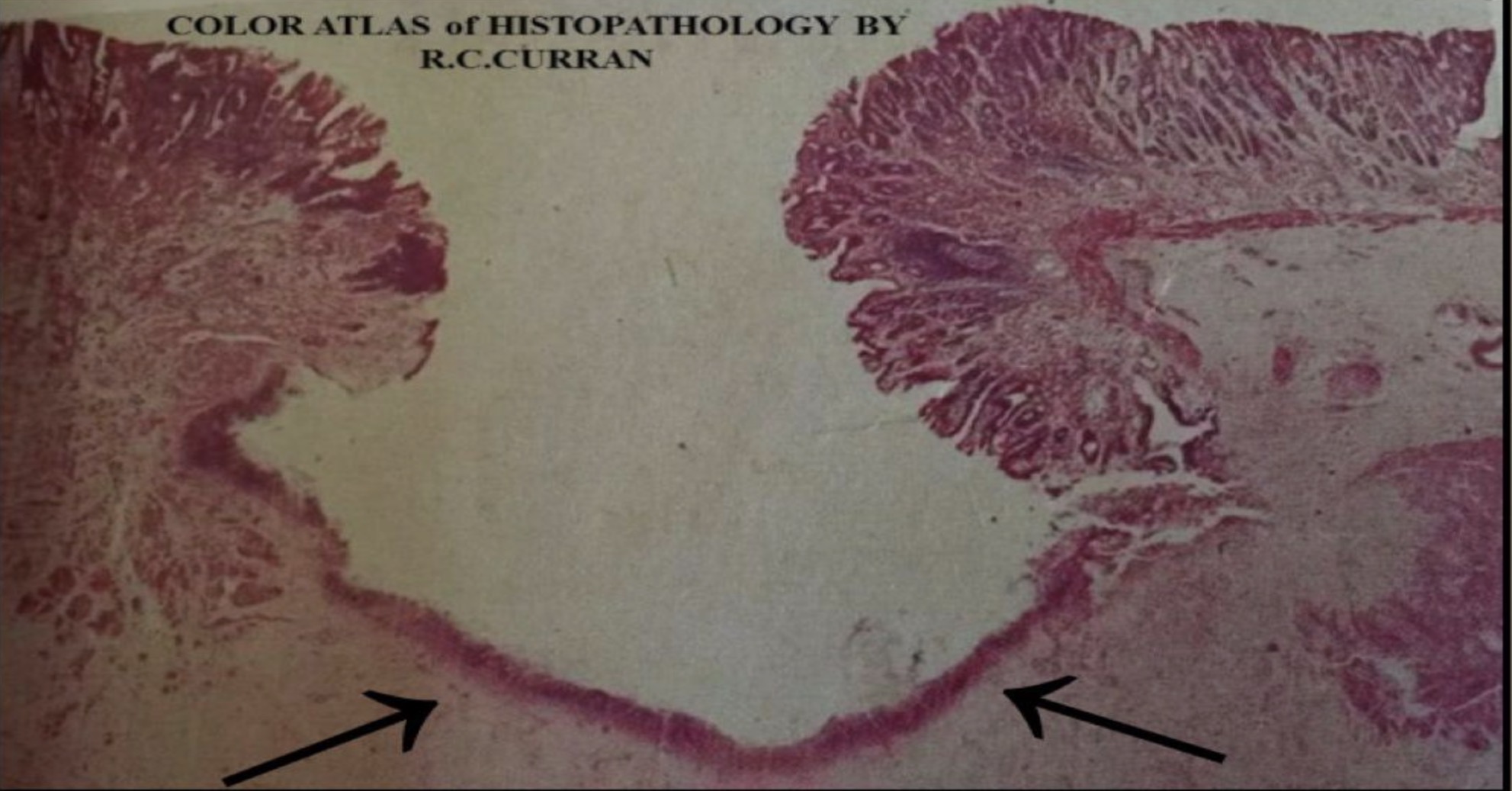
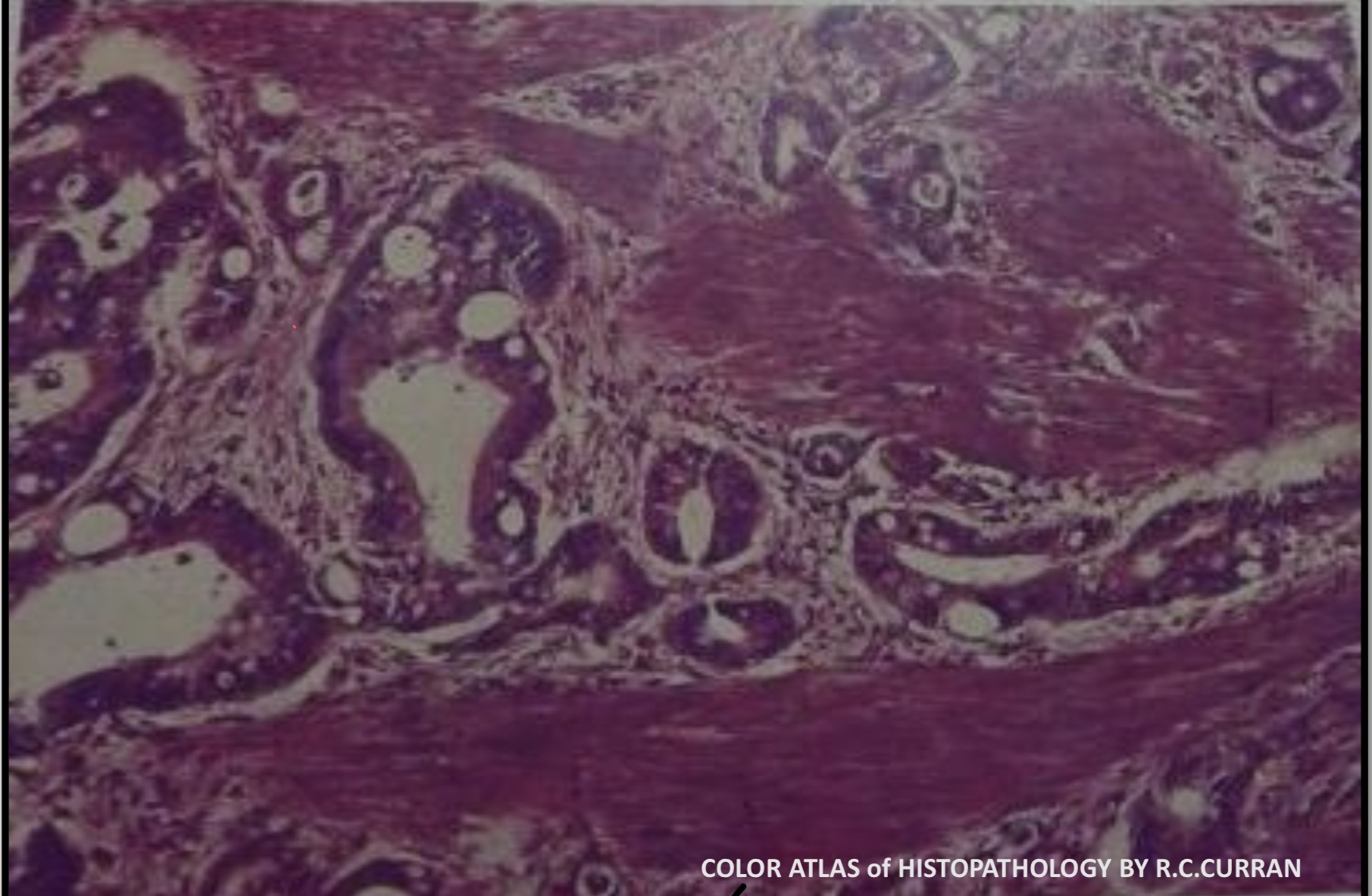
Chronic Peptic Ulcer : Stomach
A large mucosal defect forming chronic gastric ulcer with hyperplastic gastric epithelium on both sides of the ulcer. The floor of the ulcer consists of necrotic debris and dense fibrous tissue ( black arrows)
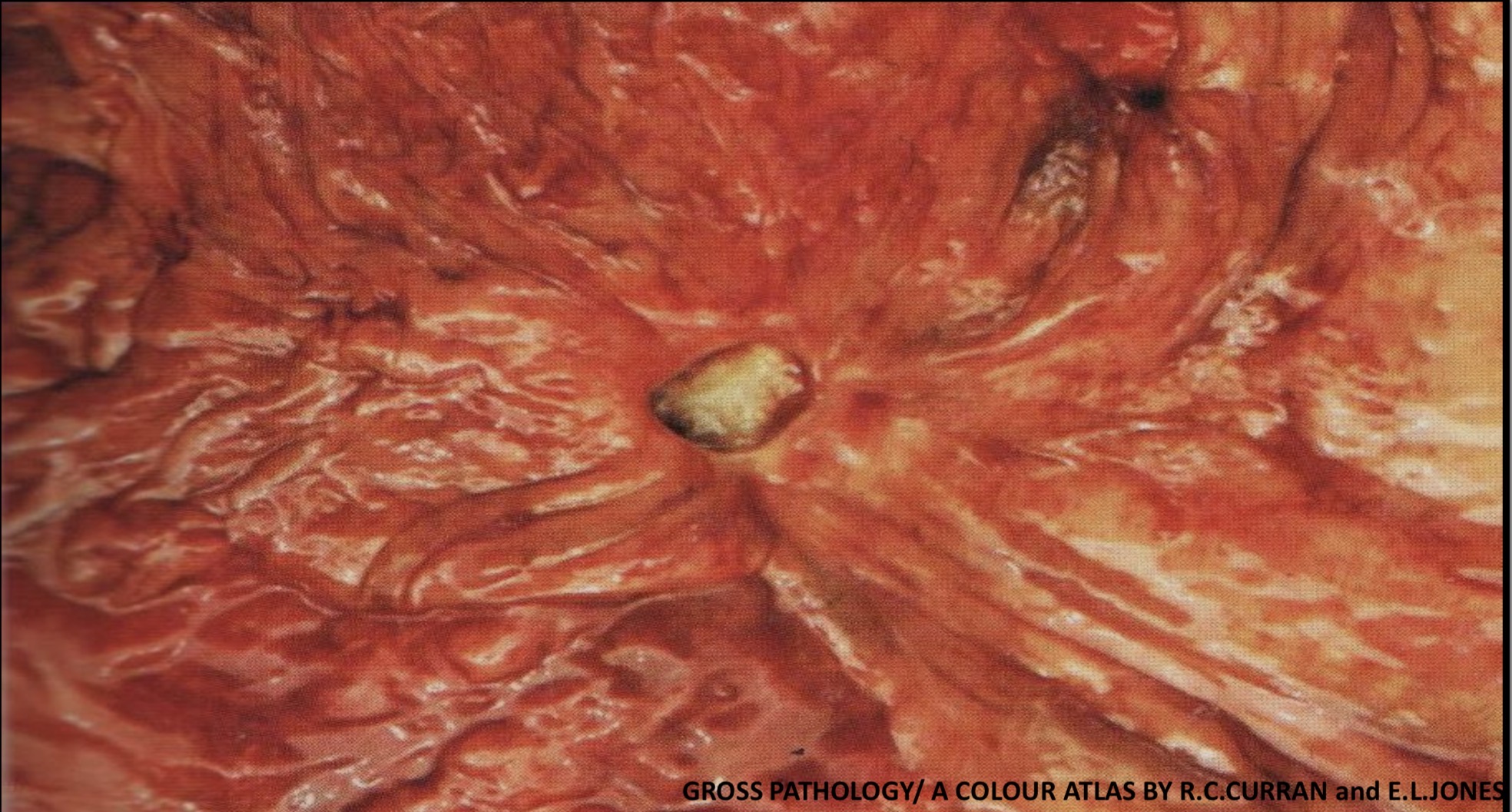
Chronic Peptic Ulcer: Duodenum
Immediately distal to the pylorus are two chronic deeply penetrating duodenal ulcers

Carcinoma: Stomach
There is a large polypoid (fungating) mass arising from the body of the stomach

Carcinoma: Stomach
There is a large polypoid (fungating) mass arising from the body of the stomach
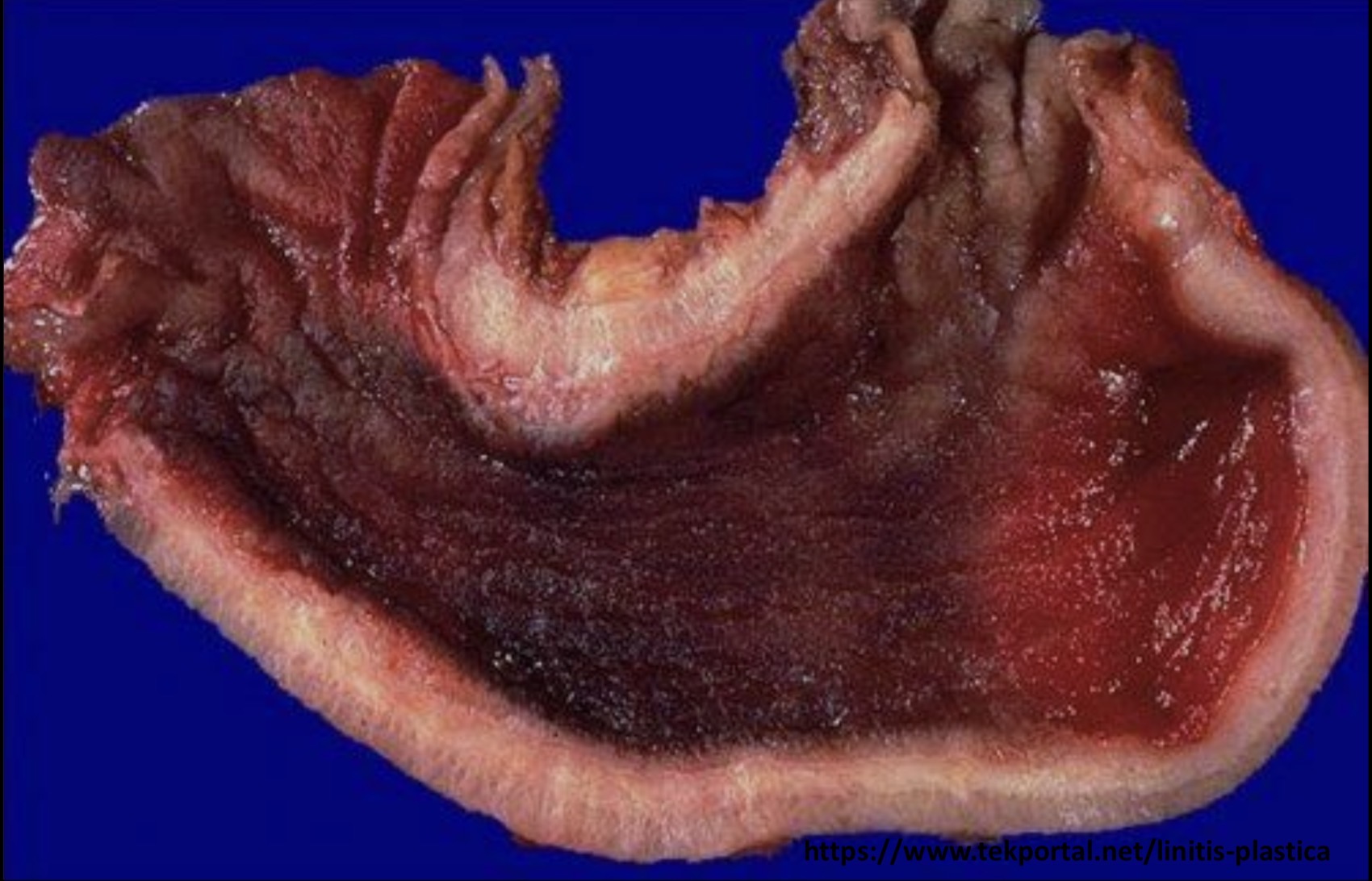
Carcinoma: Stomach
The stomach shows diffuse infiltrative type of tumor in which the gastric wall is markedly thickened (linitis plastica)
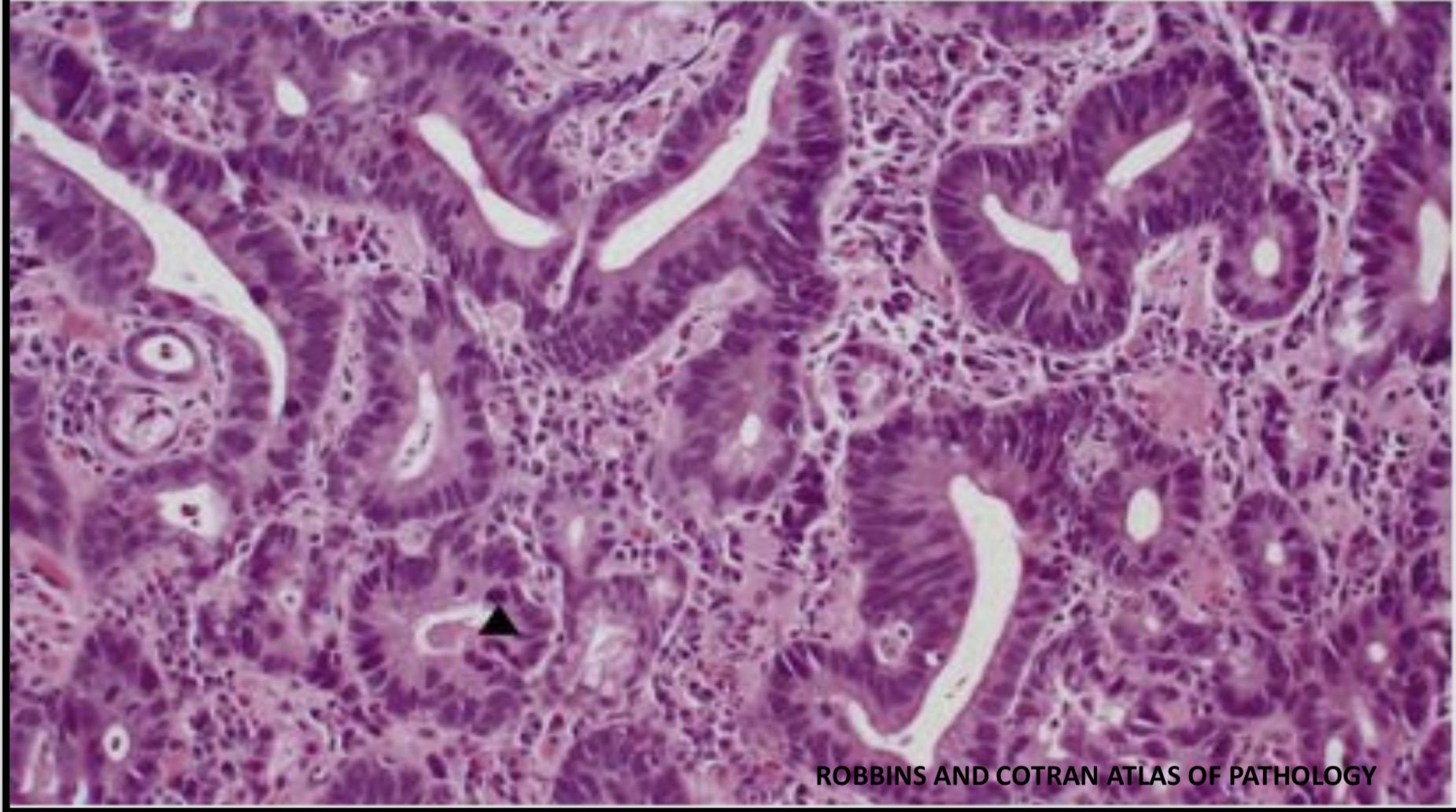
Primary Adenocarcinoma: Stomach
Irregular shapes and sizes of neoplastic glands infiltrating into the submucosa. Some of the cells show mitoses (black head arrow), pleomorphism and Hyperchromatism
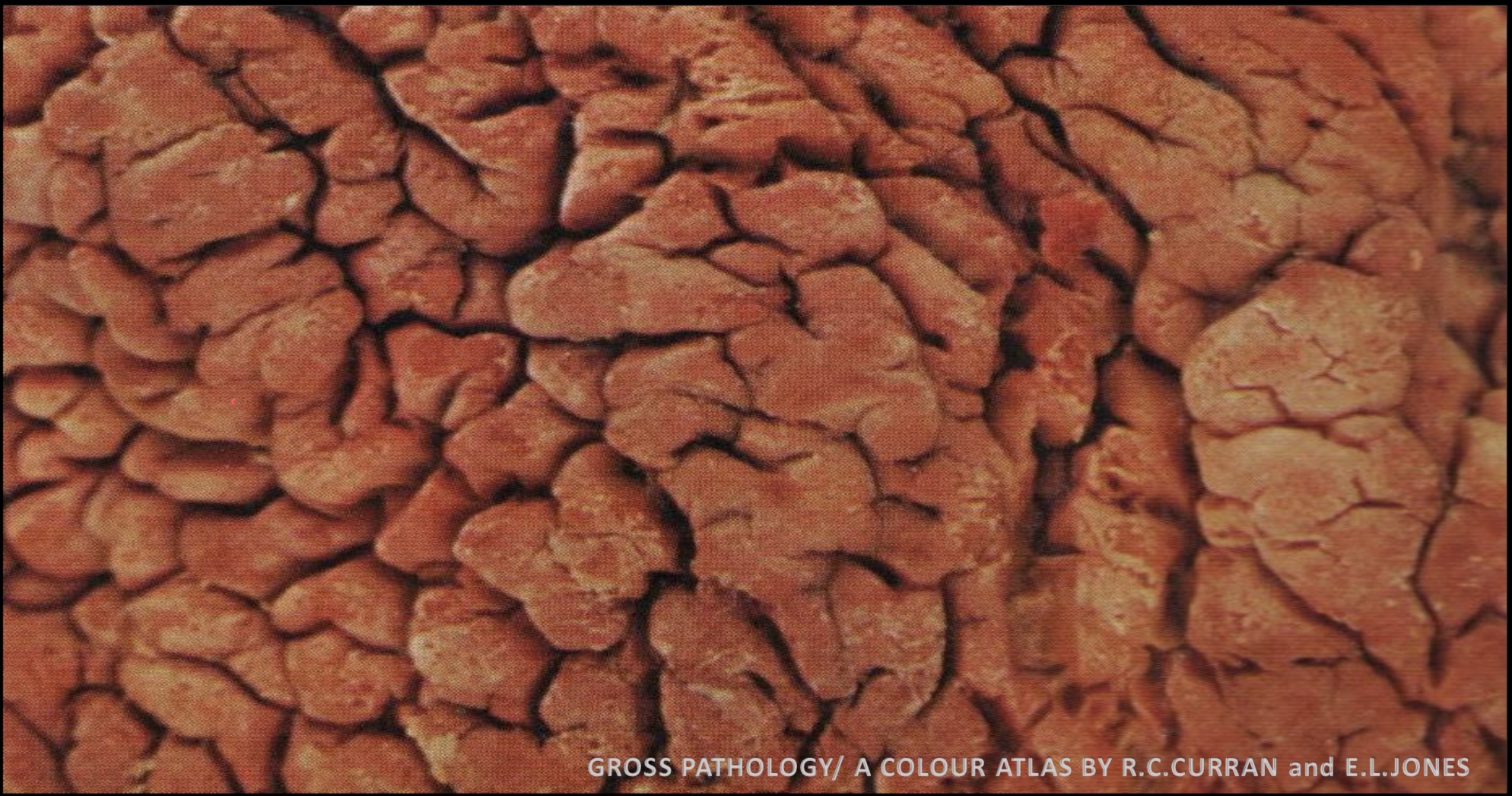
Crohn Disease : Cecum
The classic cobblestone appearance which is linear mucosal ulcers (fissures ) and thickened intestinal wall
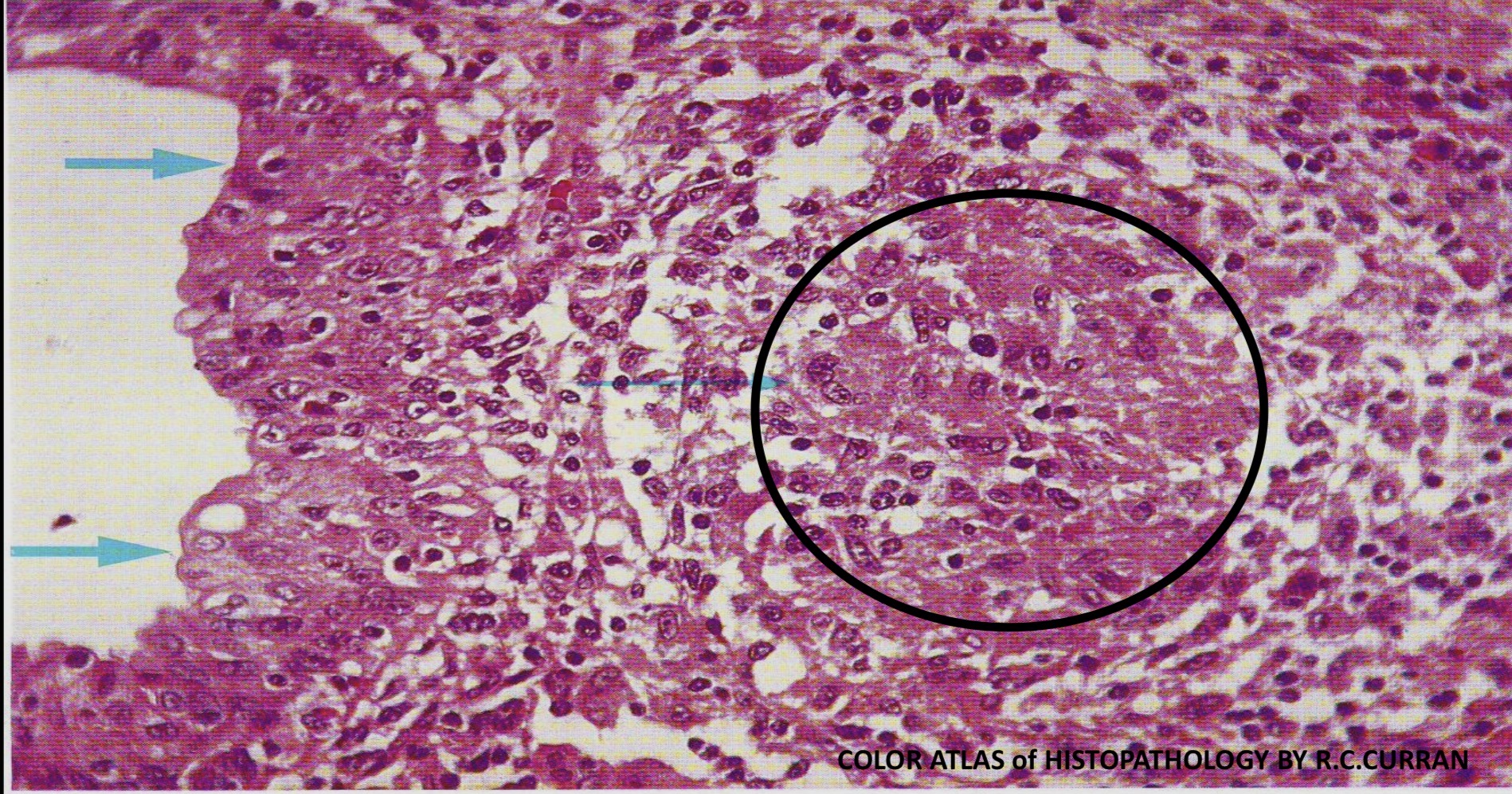
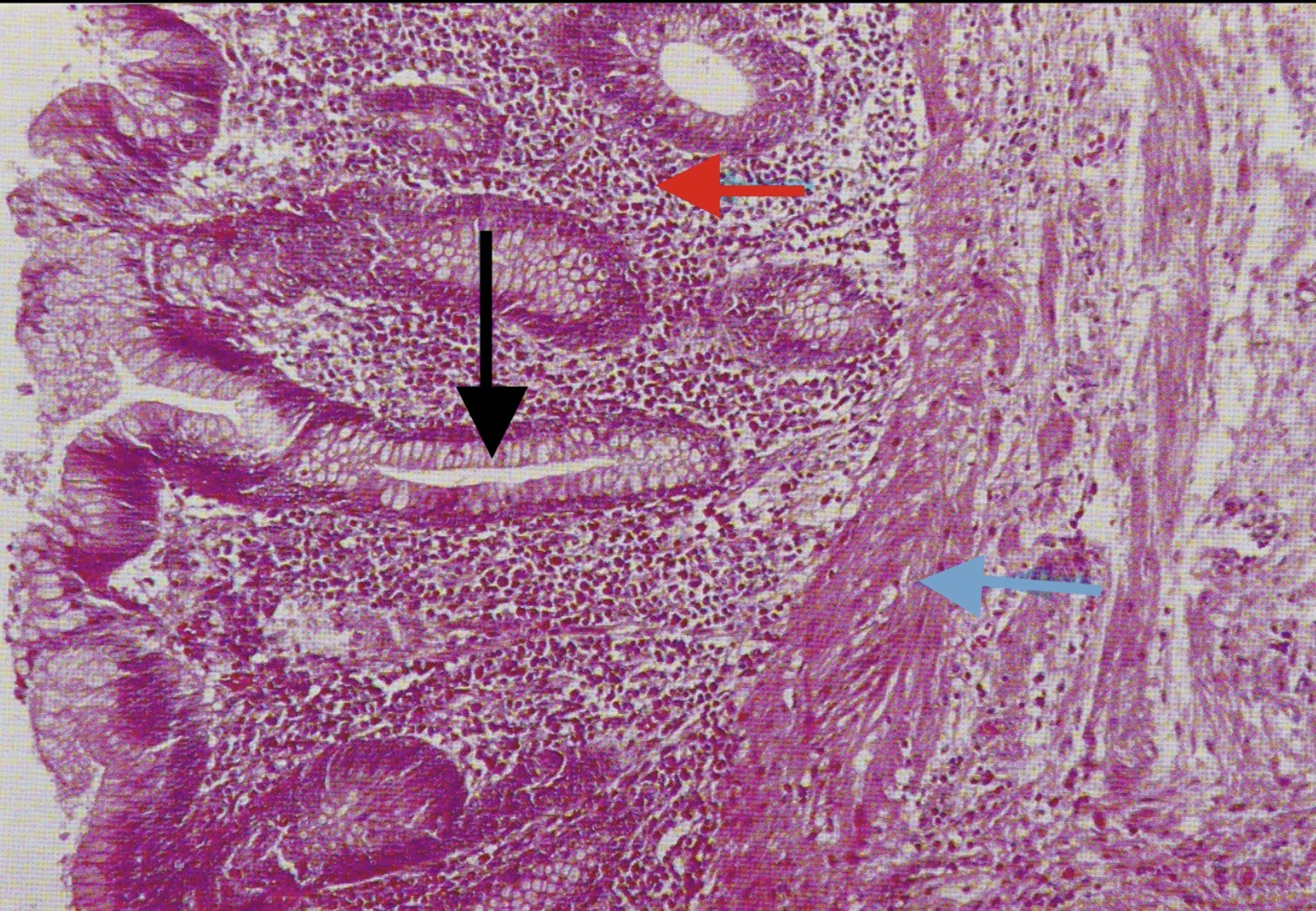
Crohn Disease : Anal Canal
The stratified squamous epithelium lining the canal (left ) is infiltrated with polymorph leukocytes and in the submucosa, there is a non- caseating epitheliod granuloma

Ulcerative Colitis: Colorectum
Diffuse erythema, edema , and many inflammatory polyps (pseudopolyps ) are distributed in the rectum, left colon, transverse colon, hepatic flexure, and the right colon while the terminal ileum is normal
Ulcerative Colitis: Crypt Abscess
Crypt abscesses are a histologic finding more typical with ulcerative colitis, the lumen of the glands are filled with pus - like material which consists of polymorph leukocytes

Familial Adenomatous Polyposis : Colon
The mucosa of this part of an affected colon is covered with polypoid adenomas of various sizes, the large pedunculated polyp (top center ) has undergone carcinomatous change
Adenomatous Polyp: Colon
Pedunculated adenoma showing a fibro-vascular stalk covered by normal colonic mucosa and a head that contains abundant neoplastic epithelial glands

Carcinoma: Colon
A large fungating polypoidal type of colonic carcinoma
Primary Adenocarcinoma : Colon
An invasive adenocarcinoma of the colon, showing malignant glands infiltrating the smooth muscle layers of the colon
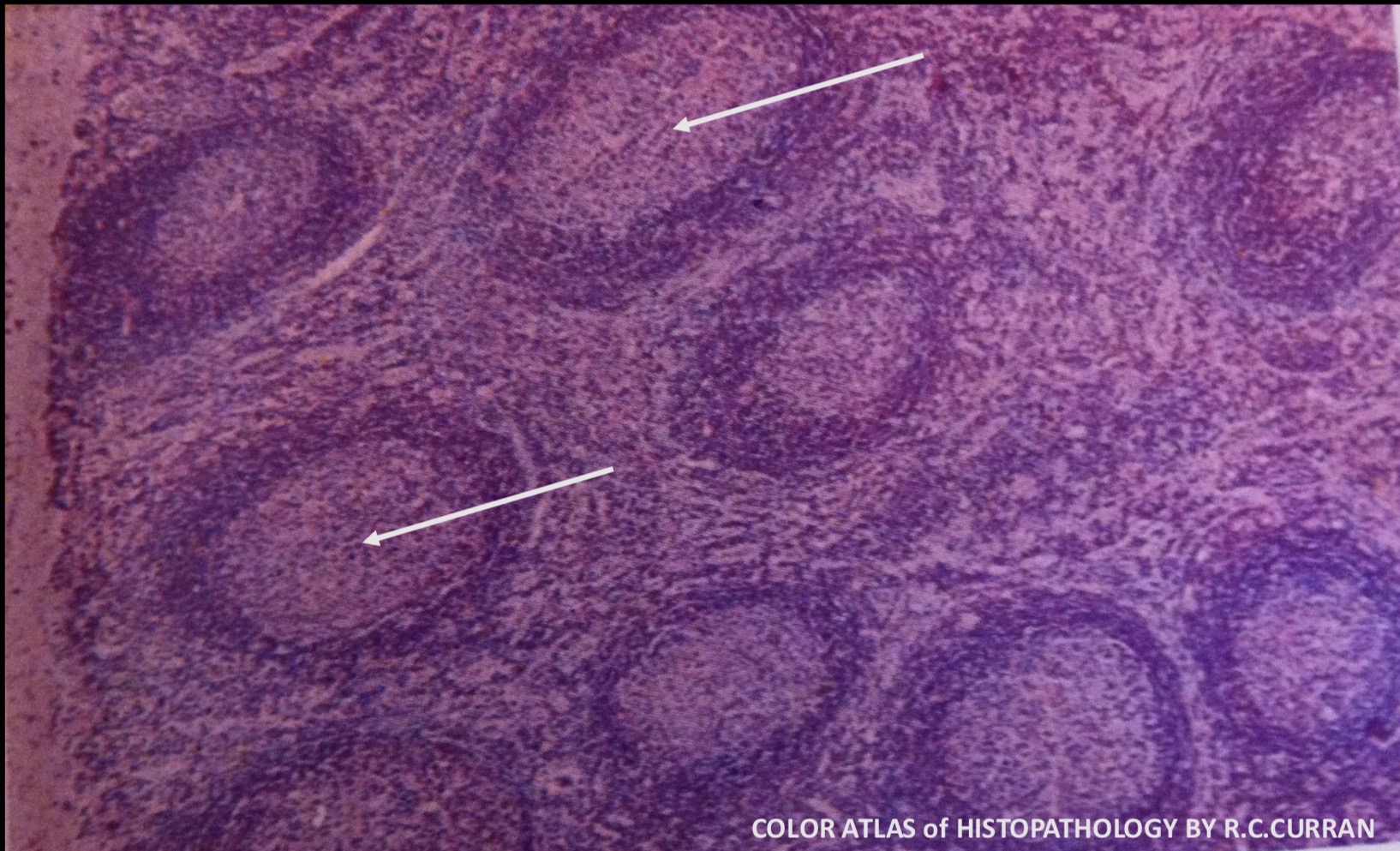
Chronic Lymphadenitis : Follicular Hyperplasia ( Lymph Node )
There is an increase in the number of lymphoid follicles which are variably sized and have enlarged prominent germinal centers. Germinal centers appear as pale areas within the lymphoid follicles (arrow)
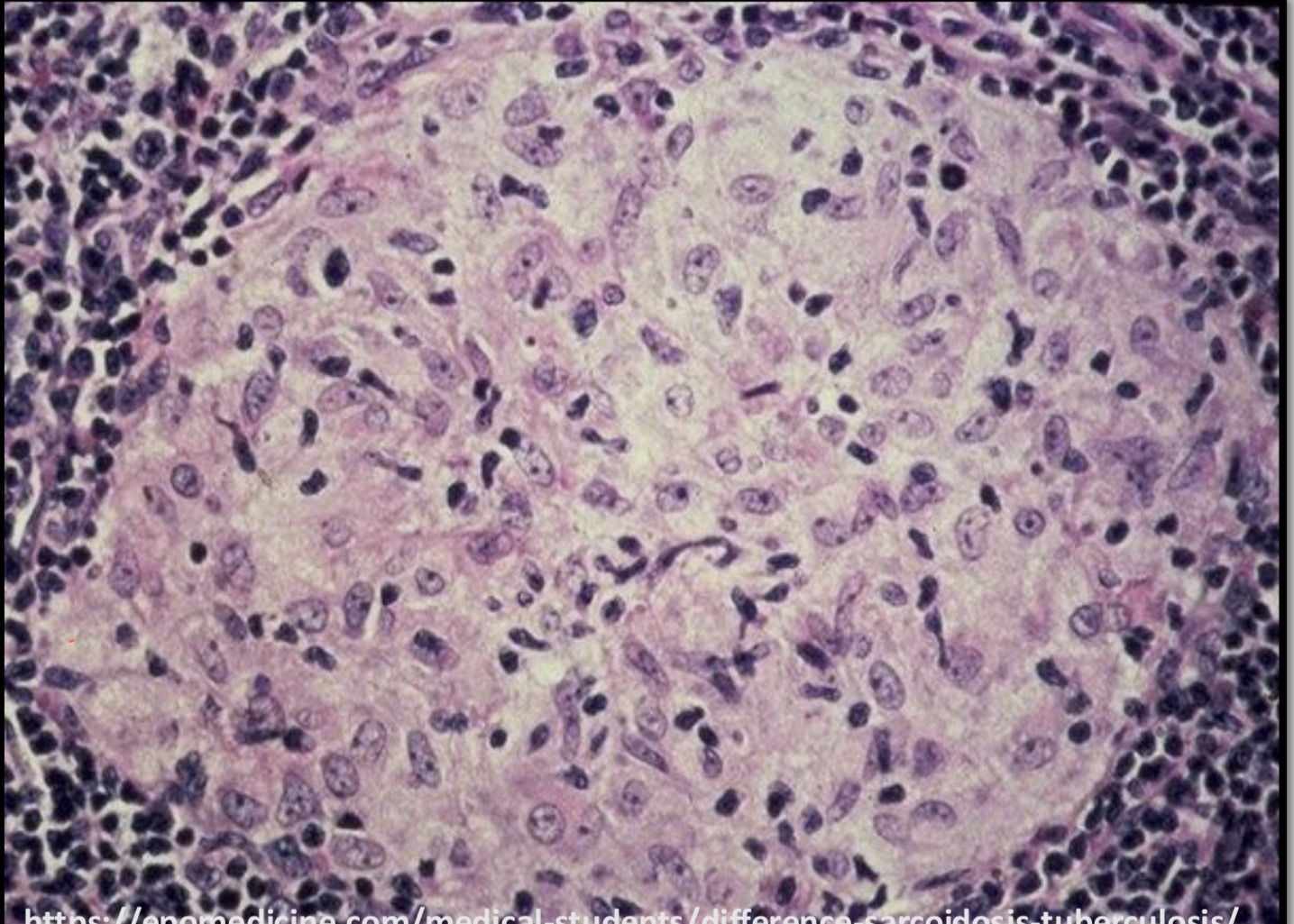
Sarcoidosis :Lymph Node
Compact non-caseating granuloma is composed of epithelioid cells (modified macrophages). Unlike tuberculous granuloma, there is no central caseous necrosis

Secondary Carcinoma : Lymph Node
Multiple enlarged lymph nodes are replaced by grayish-white deposits of secondary ( metastatic) carcinoma
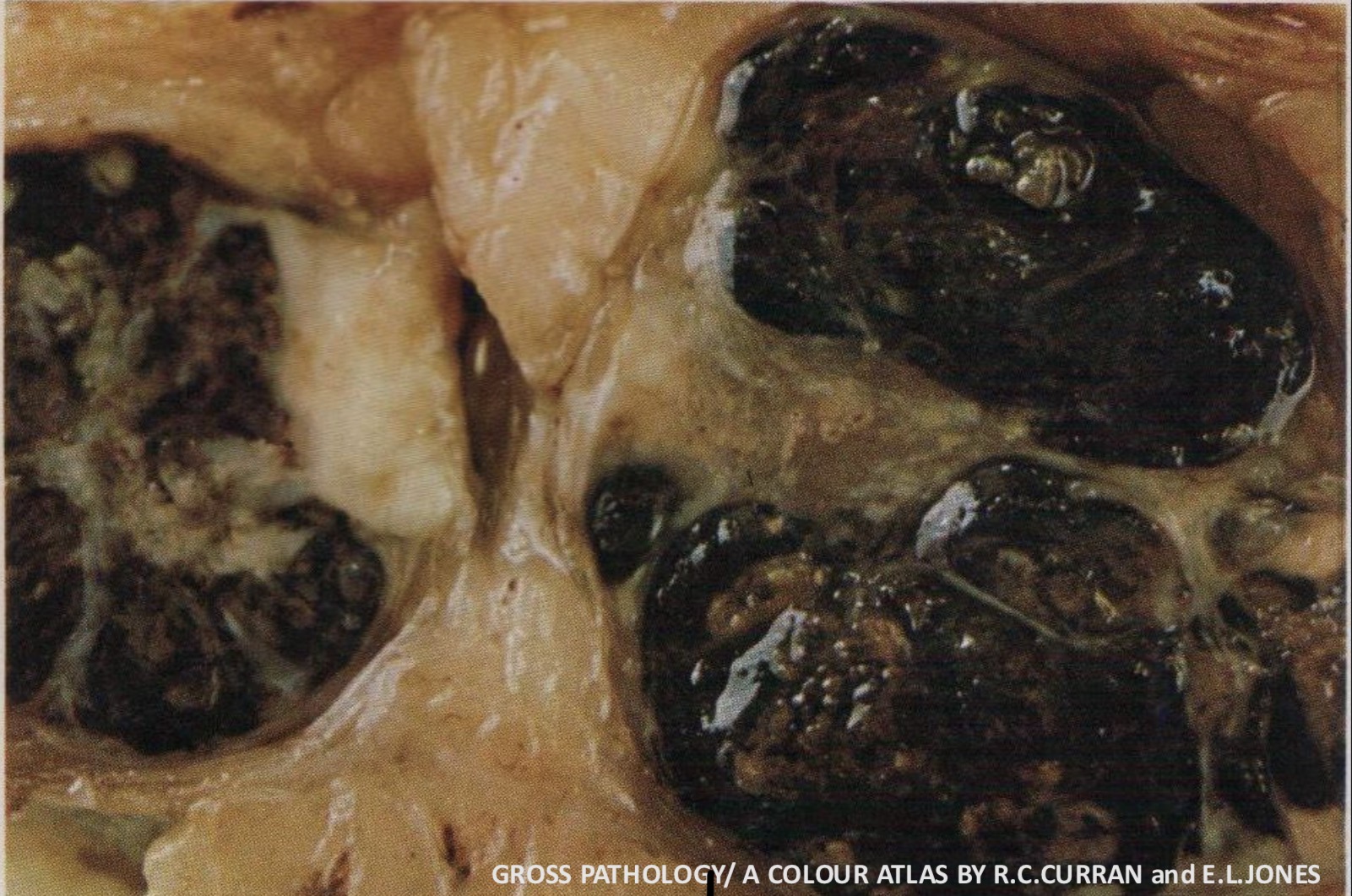
Secondary ( metastatic) malignant melanoma : Lymph Node
Three enlarged lymph nodes are extensively replaced by metastatic or secondary deposits of malignant melanoma. They appear dark- brownish or black in color due to melanin pigment produced by the tumor cells.
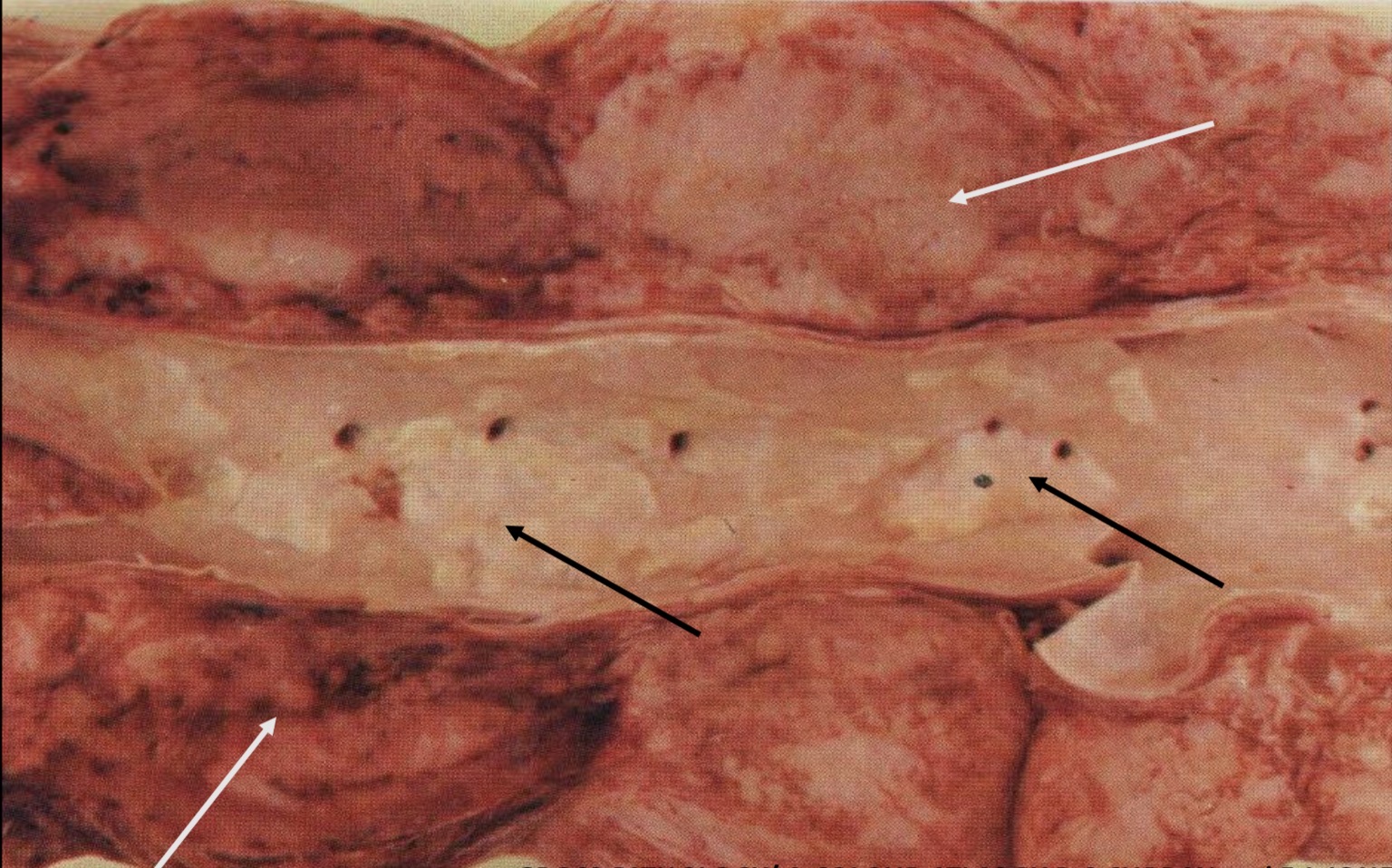
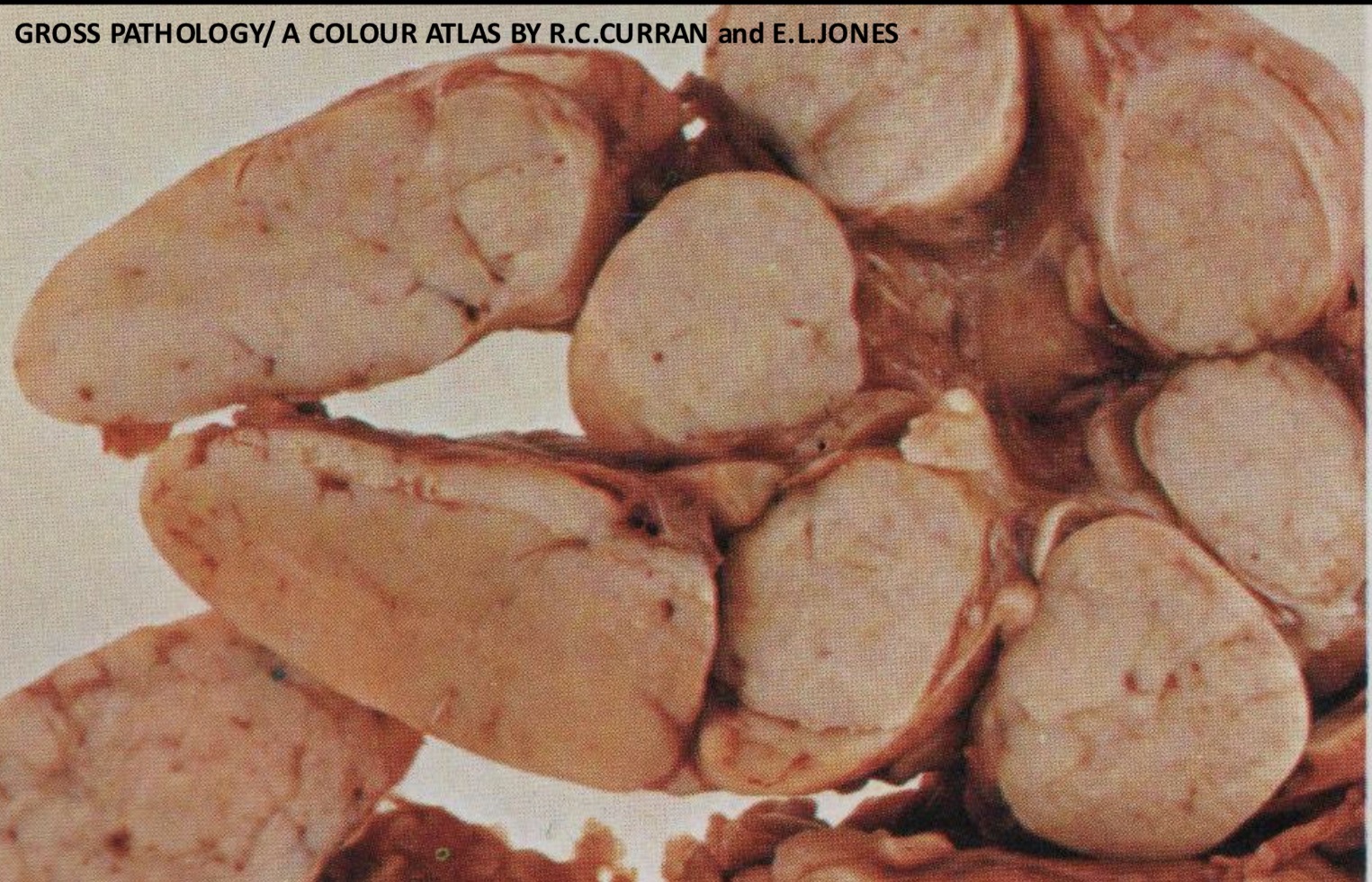
Non Hodgkin Lymphoma : Para aortic Lymph Nodes
The para-aortic lymph nodes (white arrows) are enlarged and matted together due to pericapsular infiltration. They are replaced by pinkish-gray tissue of lymphoma. The abdominal aorta also has atherosclerosis (black arrows) mainly around the openings of its branches
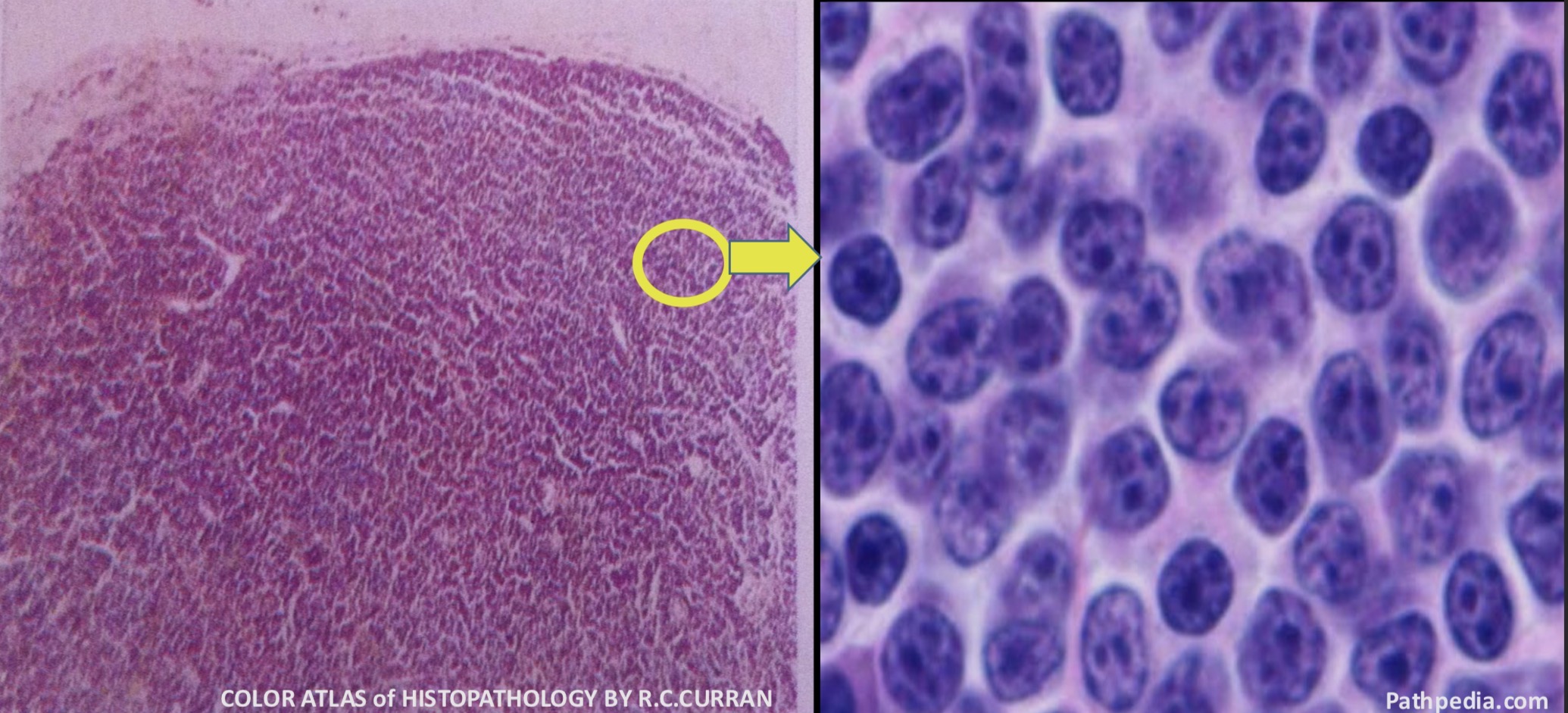
Small Lymphocytic Lymphoma (NHL) : Lymph Node
The normal architecture of the lymph node is lost and replaced by diffuse proliferation of uniform small well differentiated lymphocytes having prominent nucleoli
Follicular Lymphoma (NHL): Lymph Nodes
Multiple enlarged lymph nodes which are replaced by creamy-white tissue of lymphoma on cut surface
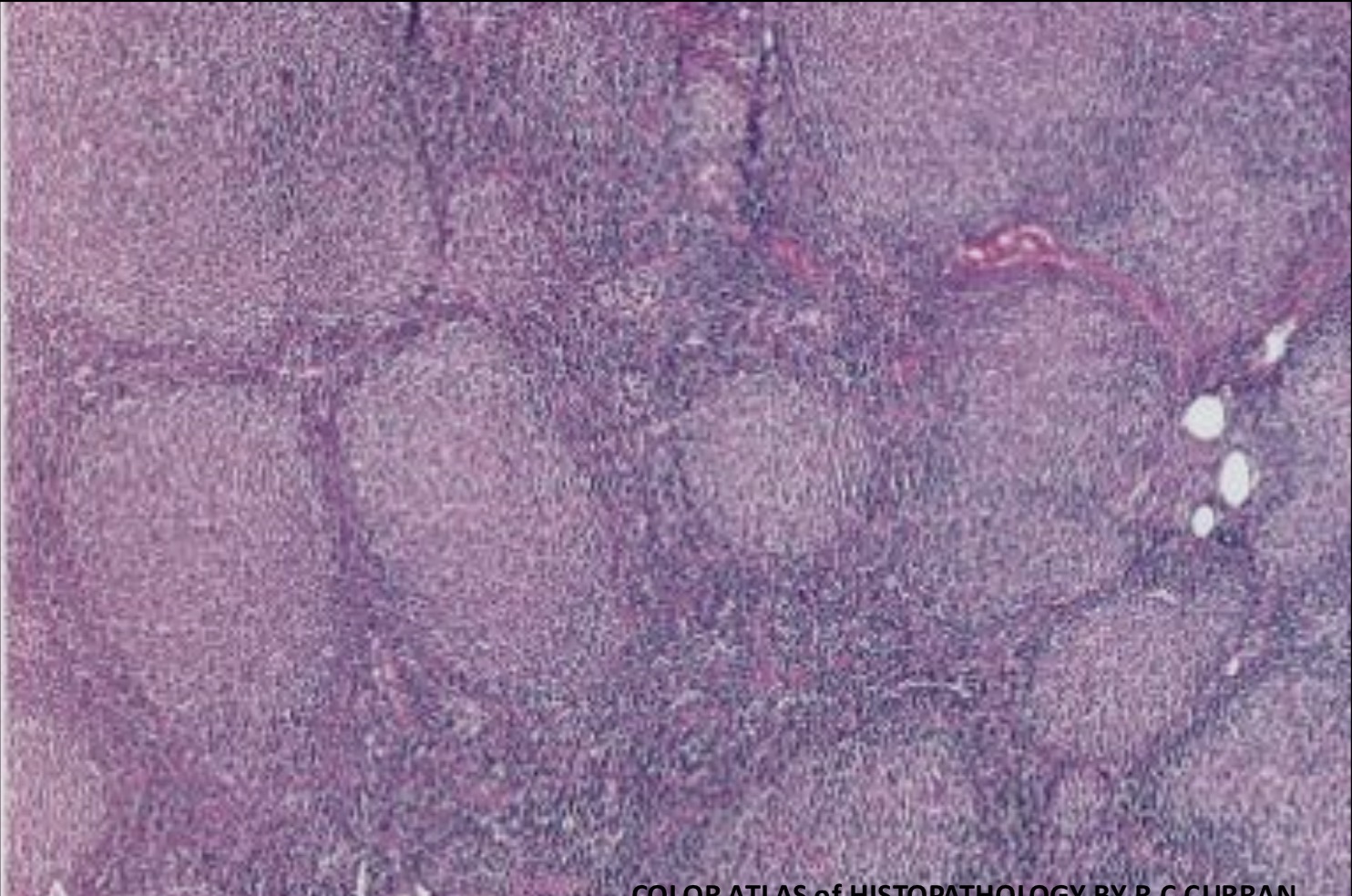
Follicular Lymphoma (NHL): Lymph Node
This lymphoma has a nodular or follicular growth pattern. Unlike follicular hyperplasia, neoplastic lymphoid follicles are ill-defined or less well-defined and without prominent germinal centers
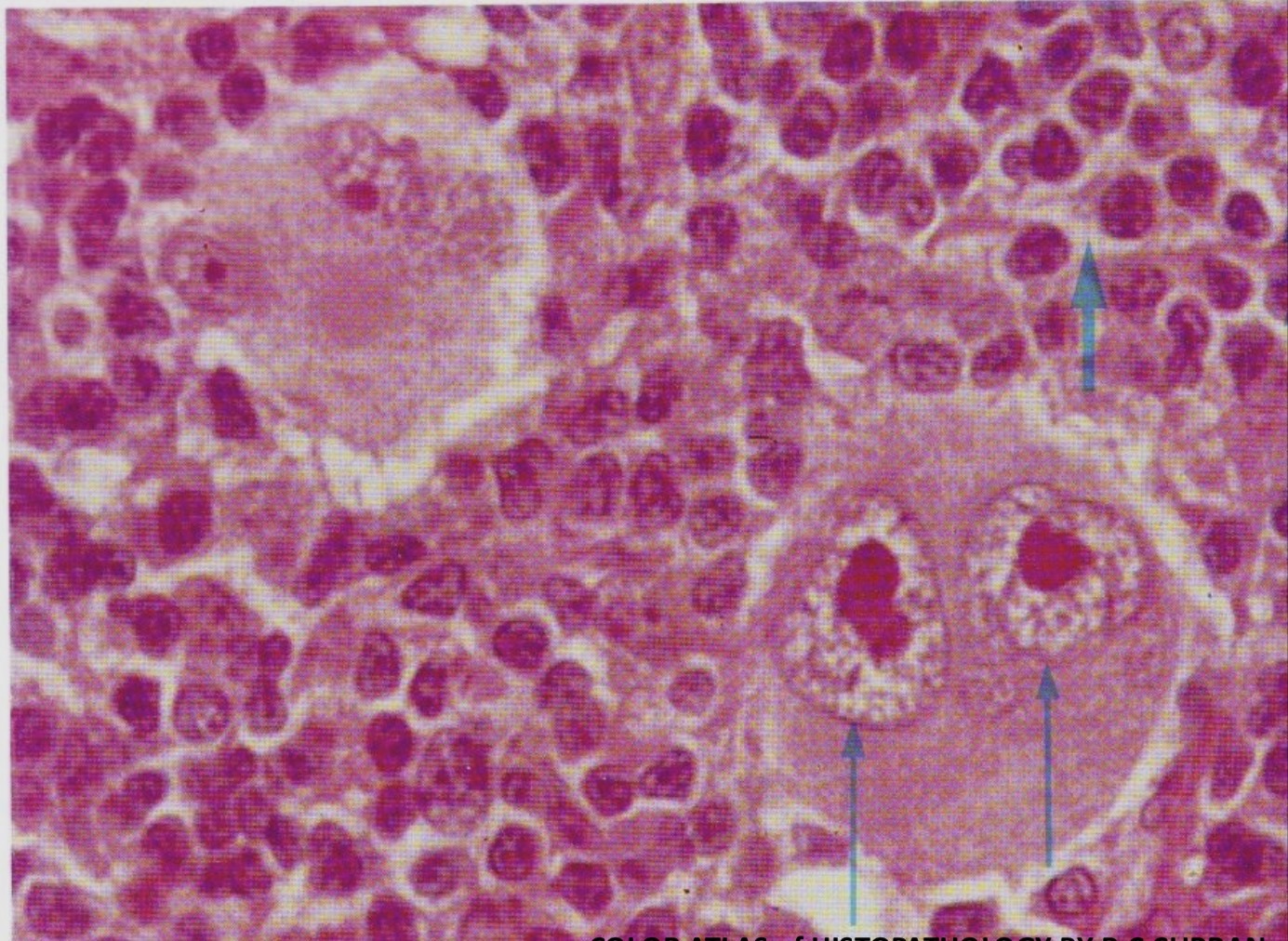
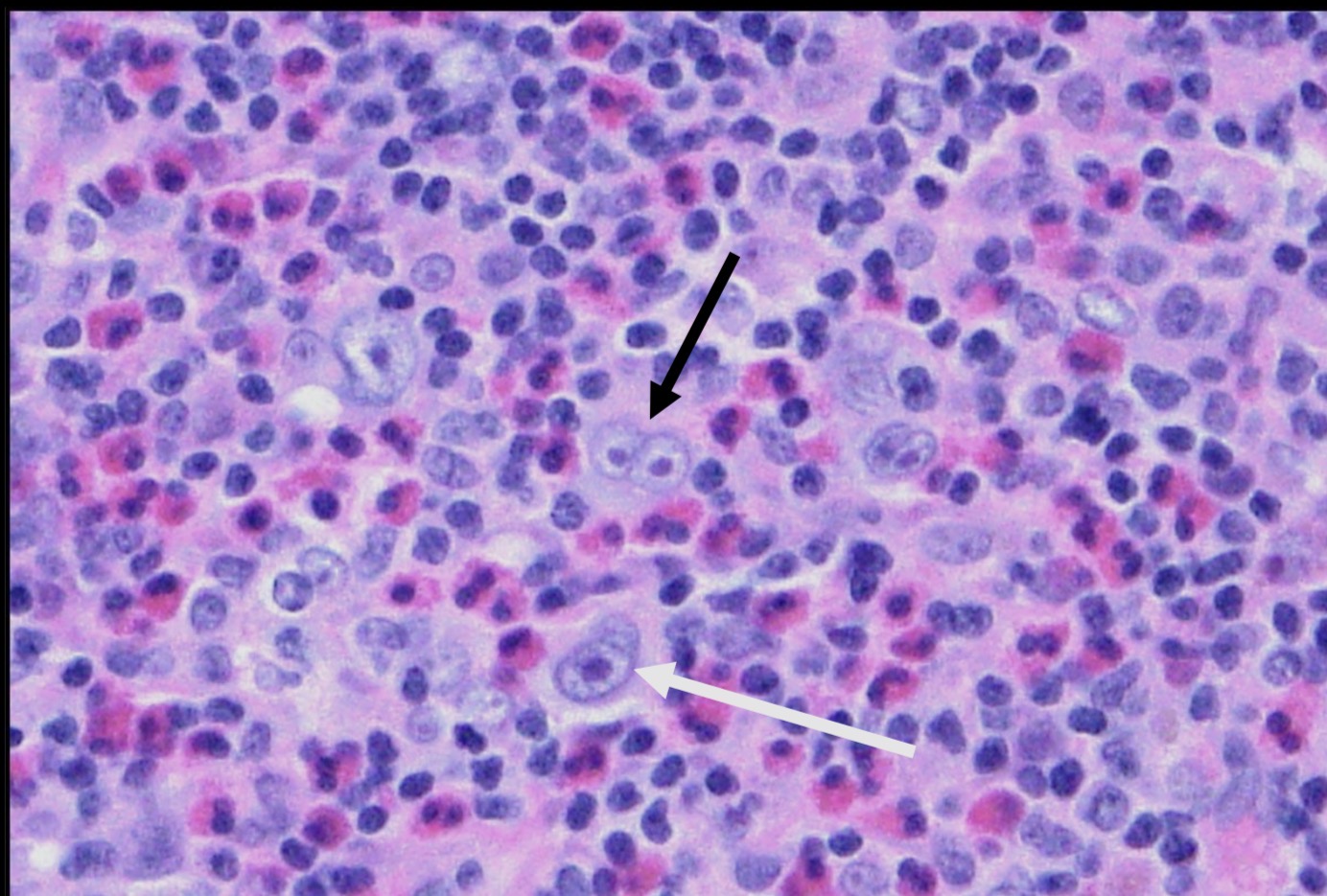
Classical Hodgkin Lymphoma , Lymphocyte Rich- Subtype : Lymph Node
Two classical Reed-Sternberg cells with mirror-image double nuclei are present (thin arrows). Each of the nuclei contains a very prominent eosinophilic nucleolus (owl eye appearance). The background is rich in small lymphocytes (thick arrow)
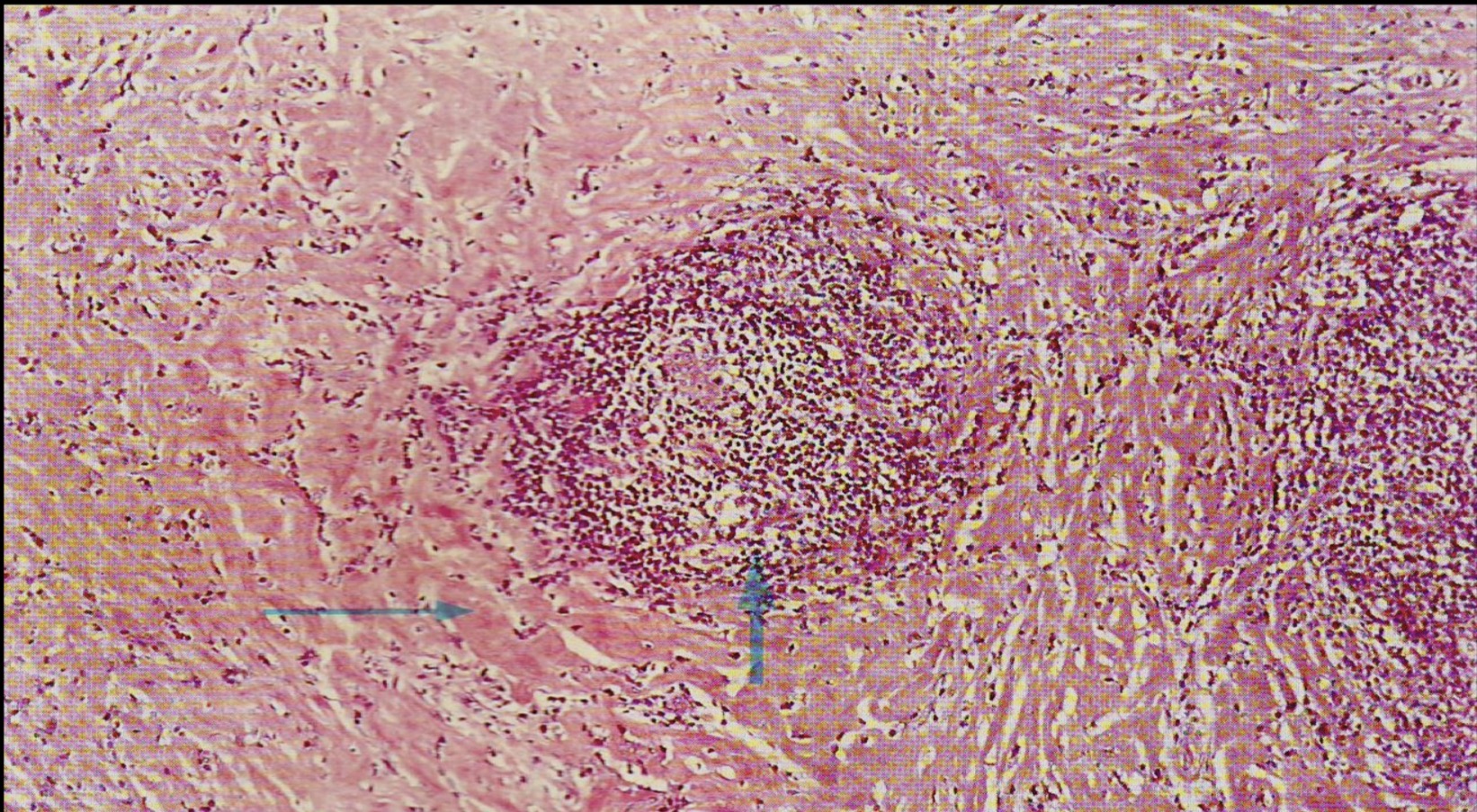
Classical Hodgkin Lymphoma, Nodular Sclerosis- Subtype : Lymph Node
The central nodule of Hodgkin tissue is surrounded by dense band like collagenous fibrous tissue. The edge of another nodule being visible on the right
Classical Hodgkin Lymphoma , Mixed Cellularity- Subtype : Lymph Node
The diagnostic classical Reed-Sternberg cells (black arrow) are easily found within a background of mixed inflammatory cell infiltrates composed of small lymphocytes , eosinophils , plasma cells and neutrophils. Hodgkin cells are also seen (white arrow)
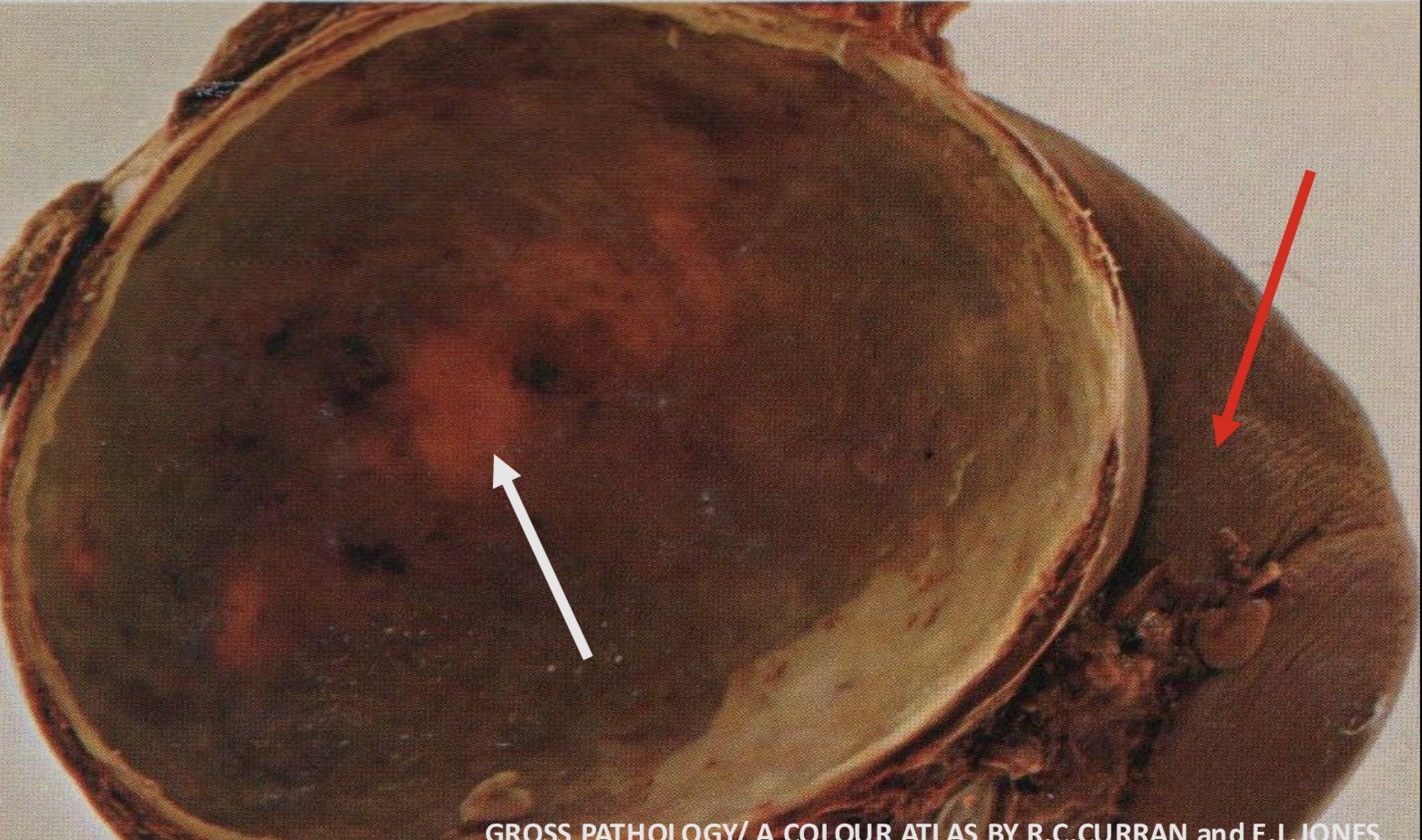
Simple ( Non Parasitic ) Cyst : Spleen
Large spherical cyst with a thick calcified fibrous wall. Its inner surface contains deposits of necrotic yellowish material (white arrow). Part of the spleen is visible on the right (red arrow)
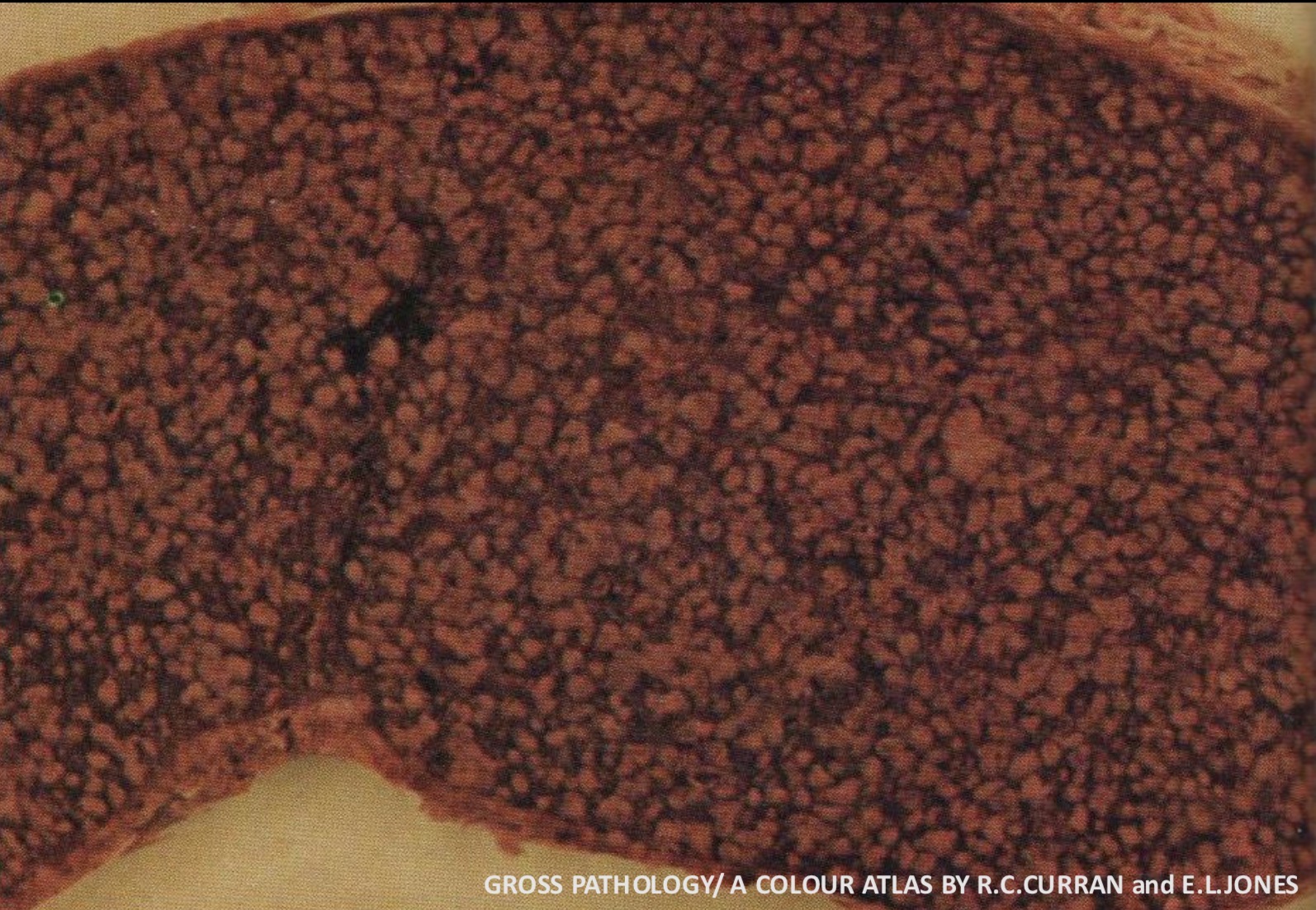
Non Hodgkin Lymphoma : Spleen
The spleen is greatly enlarged. Large numbers of small nodules of Lymphomatous tissue are visible and evenly distributed throughout the spleen
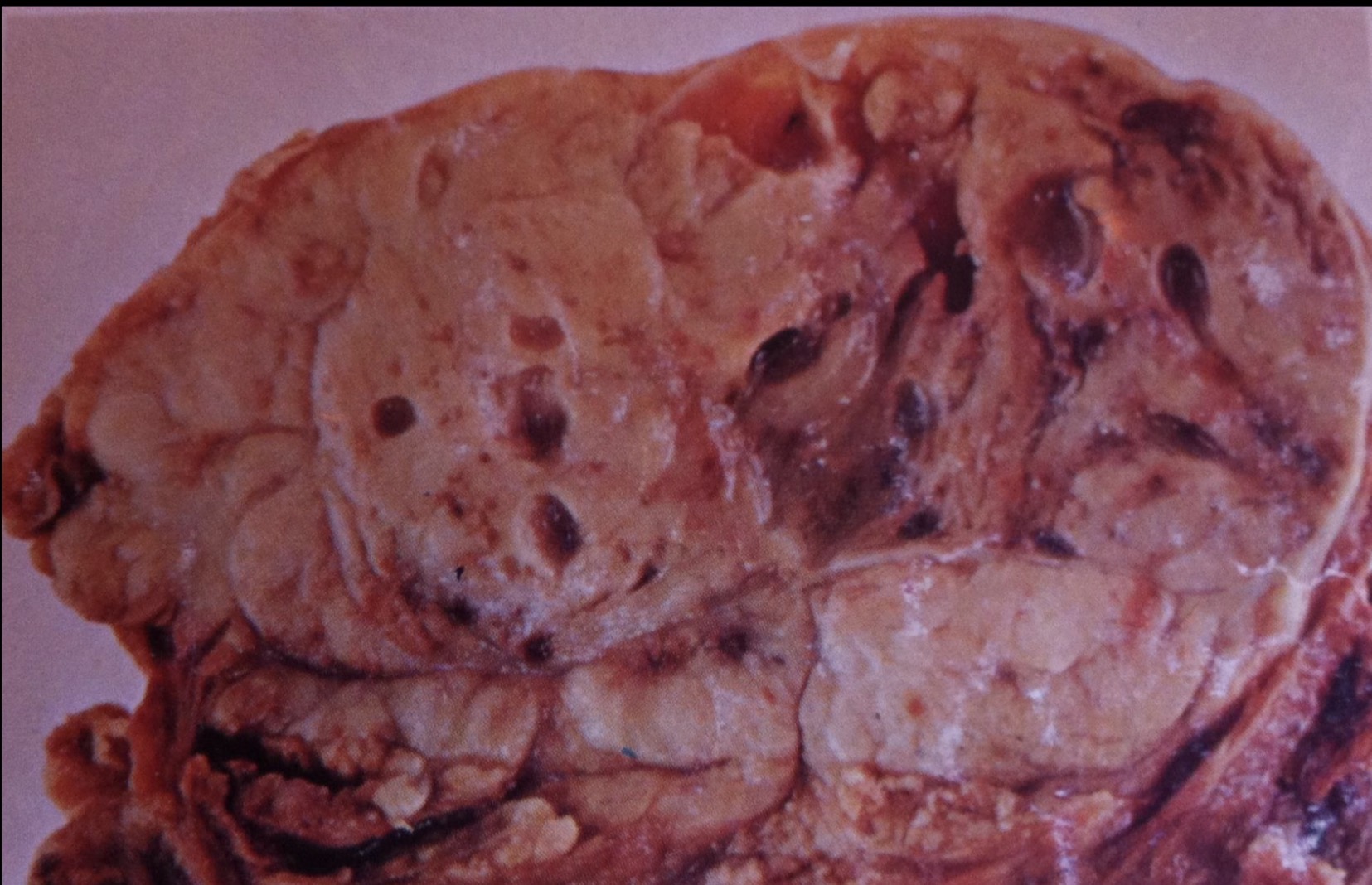
Thymoma : Thymus
Oval tumor mass of the thymus with lobular growth pattern , yellowish-gray in color. Numerous small cystic areas are present
Atherosclerosis : Aorta
Raised yellowish areas that represent atheroma with areas of hemorrhage (red arrow) and thrombosis (white arrow)
Atherosclerosis : Aorta
Advance stage of atherosclerotic plaques at the inner aspect of the aortic wall that show areas of ulceration, hemorrhage and thrombosis (arrows)
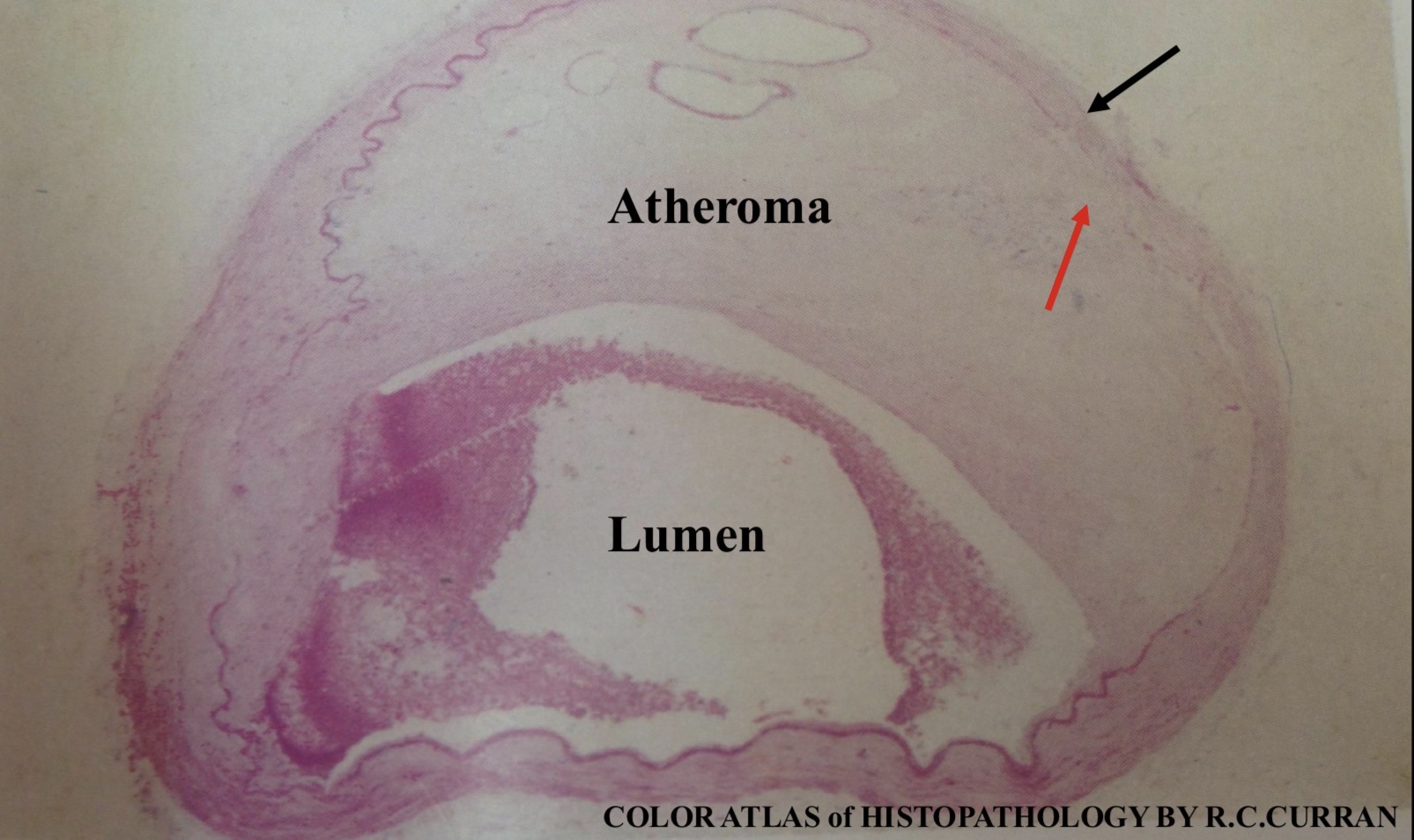
Atherosclerosis: Coronary artery
This cross section of the coronary artery shows severe atherosclerosis that has reduced the lumen. The internal elastic membrane adjacent to the atheroma has disappeared (red arrow) , with atrophy of the media ( black arrow)
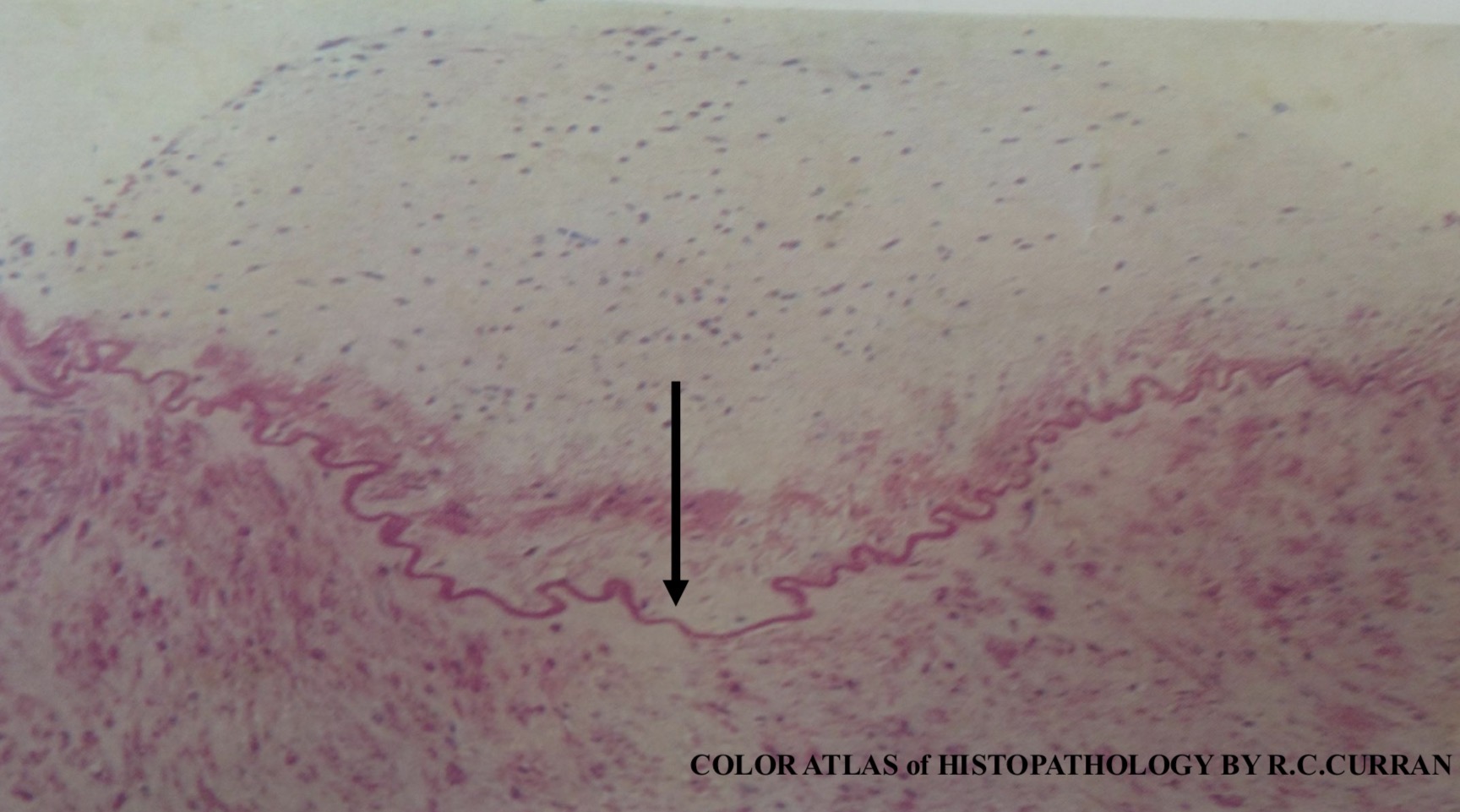
Atherosclerosis: Aorta
This atherosclerotic plaque shows numerous nuclei of macrophages, inflammatory cells and smooth muscle cells and is pale in color due to extracellular fat. The neointima is separated from tunica media by an internal elastic membrane which appears depressed in the center of the lesion (arrow), with slight atrophy of the media
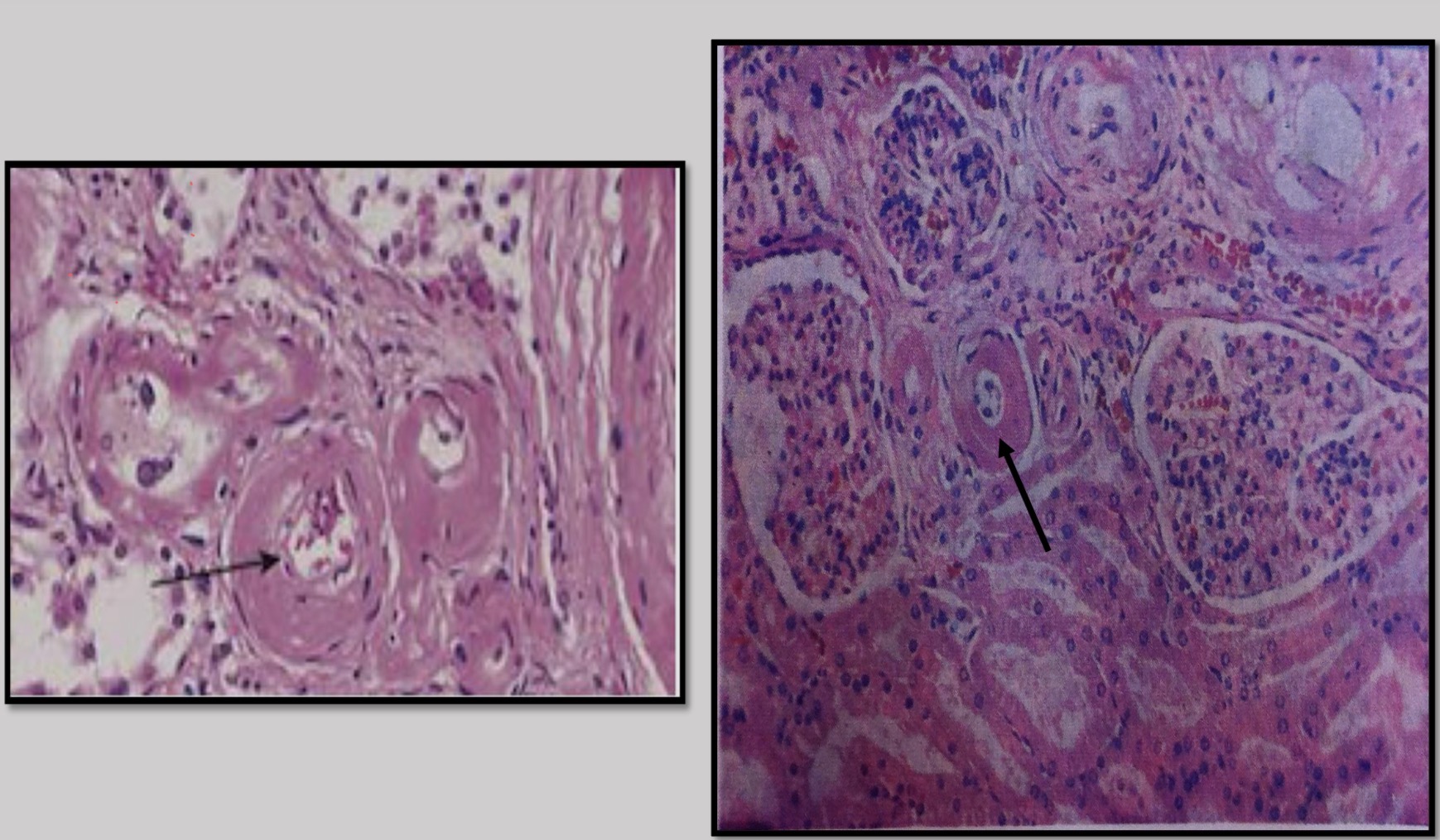
Hyaline arteriolosclerosis (Benign hypertension): Kidney
Homogenous eosinophilic deposition of hyaline material in the walls of blood vessels (arrows), due to benign hypertension
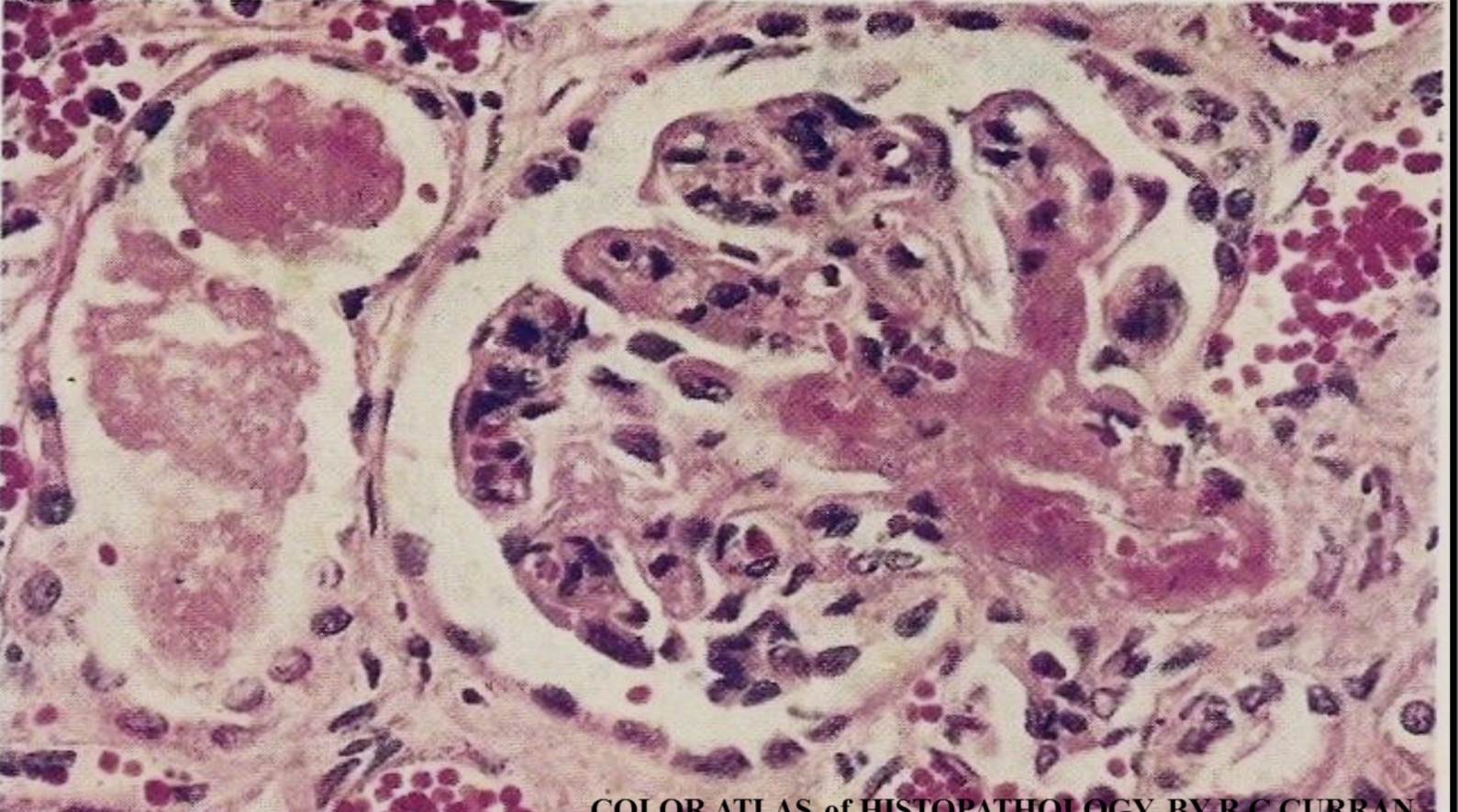
Fibrinoid necrosis (Malignant hypertension): Kidney
Fibrinoid necrosis of the afferent arteriole and part of the glomerulus which appears as bright pink amorphous granular fibrin like material deposit, due to malignant hypertension
Aneurysm : Iliac arteries
Circumferential dilatation of abdominal aorta and both common iliac arteries with atherosclerosis (fusiform aneurysm). Saccular aneurysm of the right internal iliac artery. Prominent atherosclerosis of the left internal iliac artery
Infarction of Myocardium: Heart
Cross section of interventricular septum and left ventricle showing early infarcted area (coagulative necrosis ) with mottled hemorrhagic appearance (arrows)

Infarction of Myocardium: Heart
This is a cross section of the interventricular septum, showing whitish to yellowish area of infarction (coagulative necrosis ), 8-10 days following the infarction (arrow)
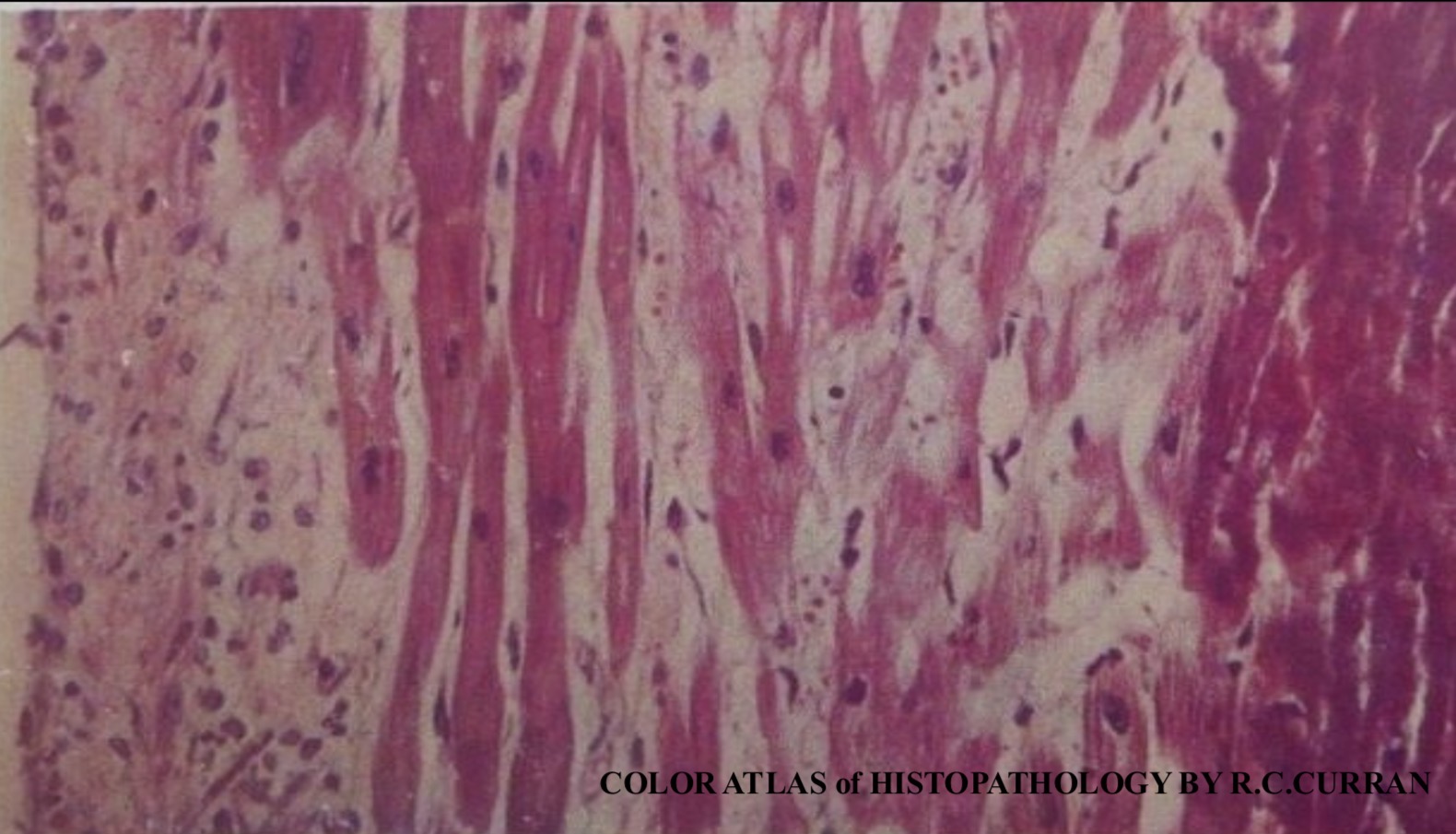
Infarction of Myocardium : Heart
On the left side, the myocardial muscles are normal ,while the myocardial muscles are necrotic or dead on the right side. The dead muscles preserve their architecture ,show deep eosinophilia than the normal muscle with absence of nuclei and the presence of inflammatory cells.
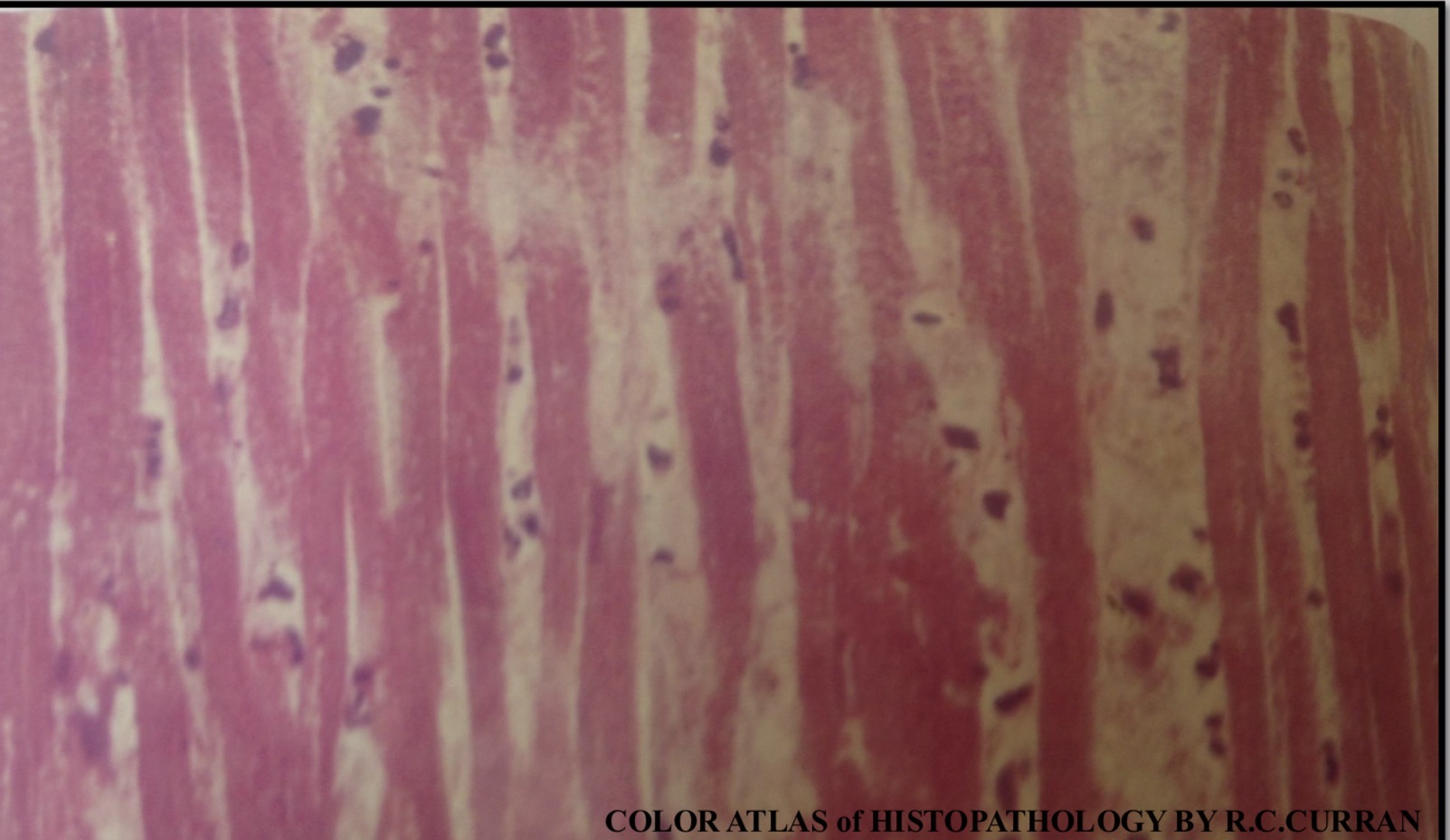
Infarction of Myocardium : Heart
The necrotic myocardial muscles preserve the architecture and are deep eosinophilic than normal ,with loss of nuclei and cross- striation with presence of inflammatory cells within the interstitial tissue.
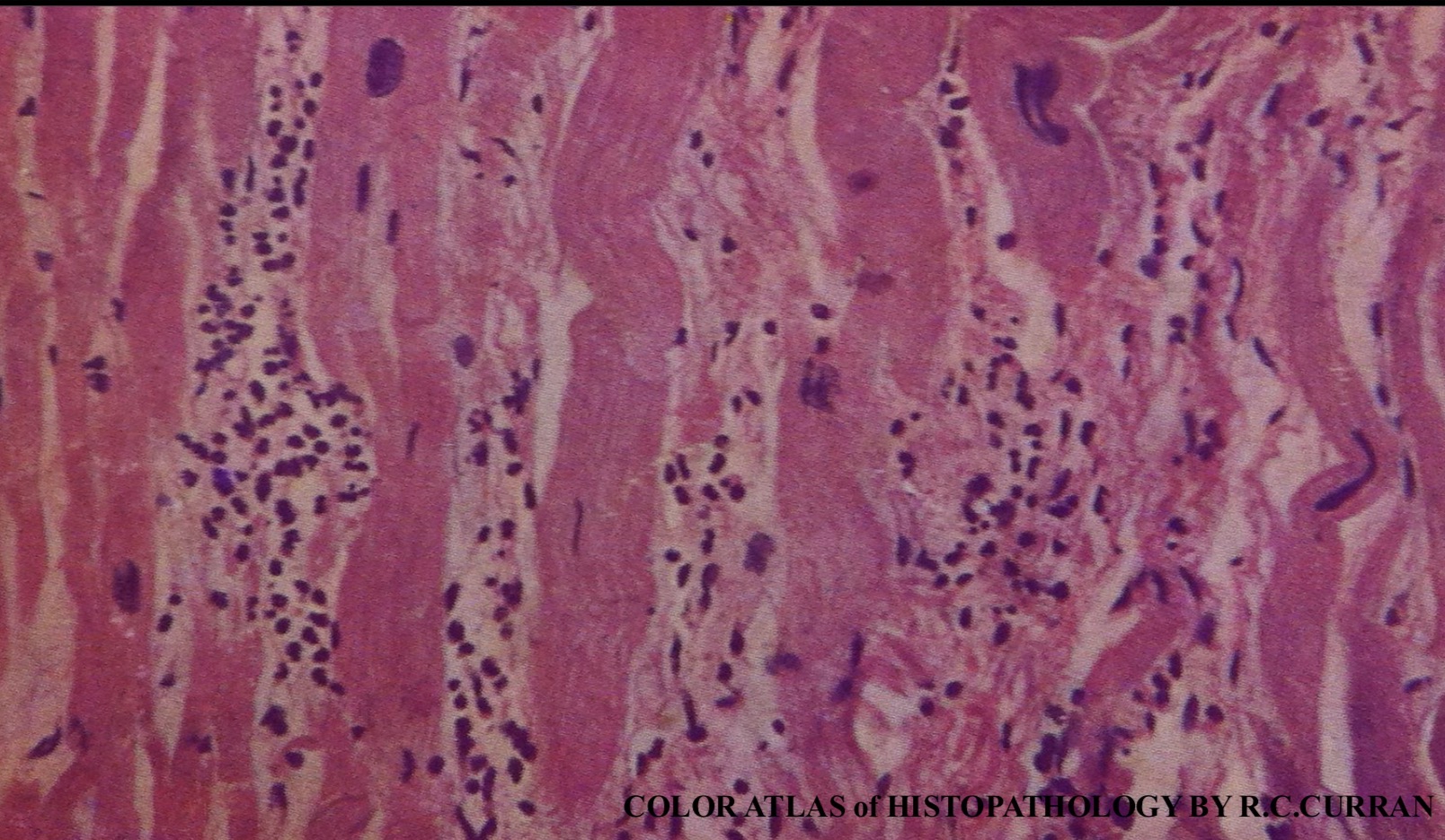
Viral myocarditis: Heart
Some of the myocardial muscle fibers are swollen with infiltration by lymphocytes and neutrophils
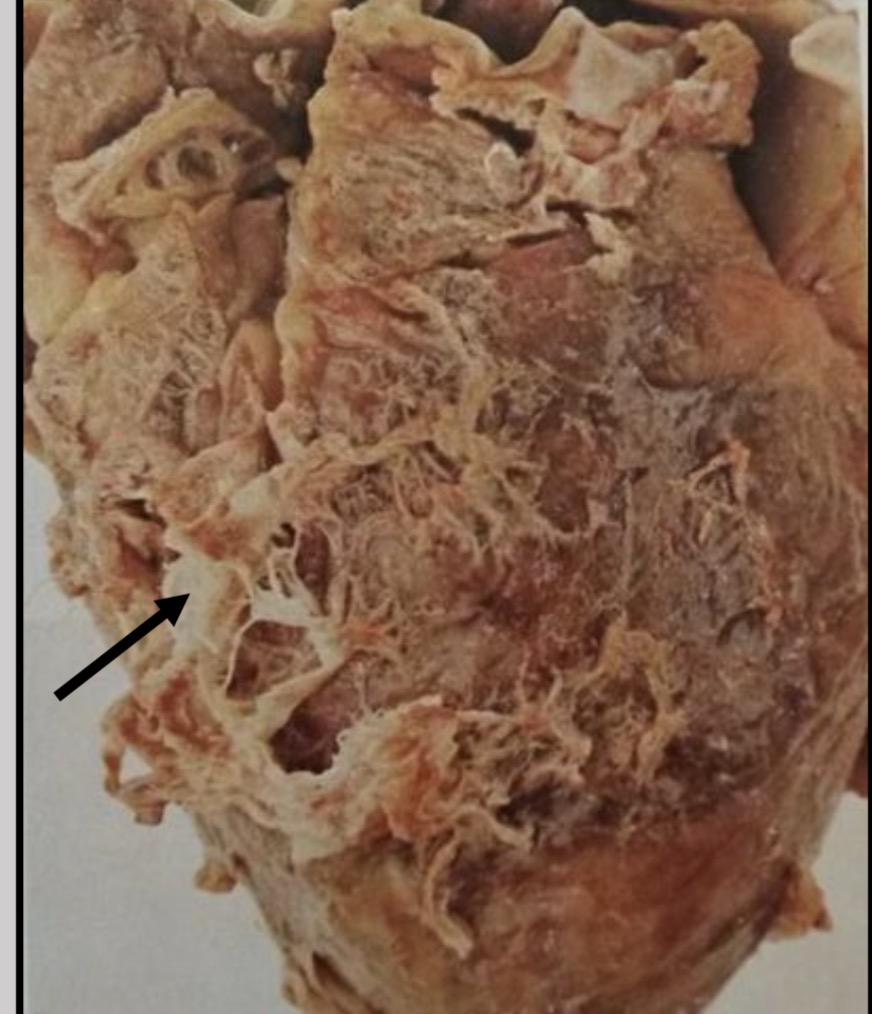
Fibrinous (uremic) pericarditis :Heart (bread and butter appearance)
-The epicardial surface is covered with a mesh of gray- white strands of fibrin giving bread and butter appearance with organization of some fibrin strands which appear whitish in color (arrow
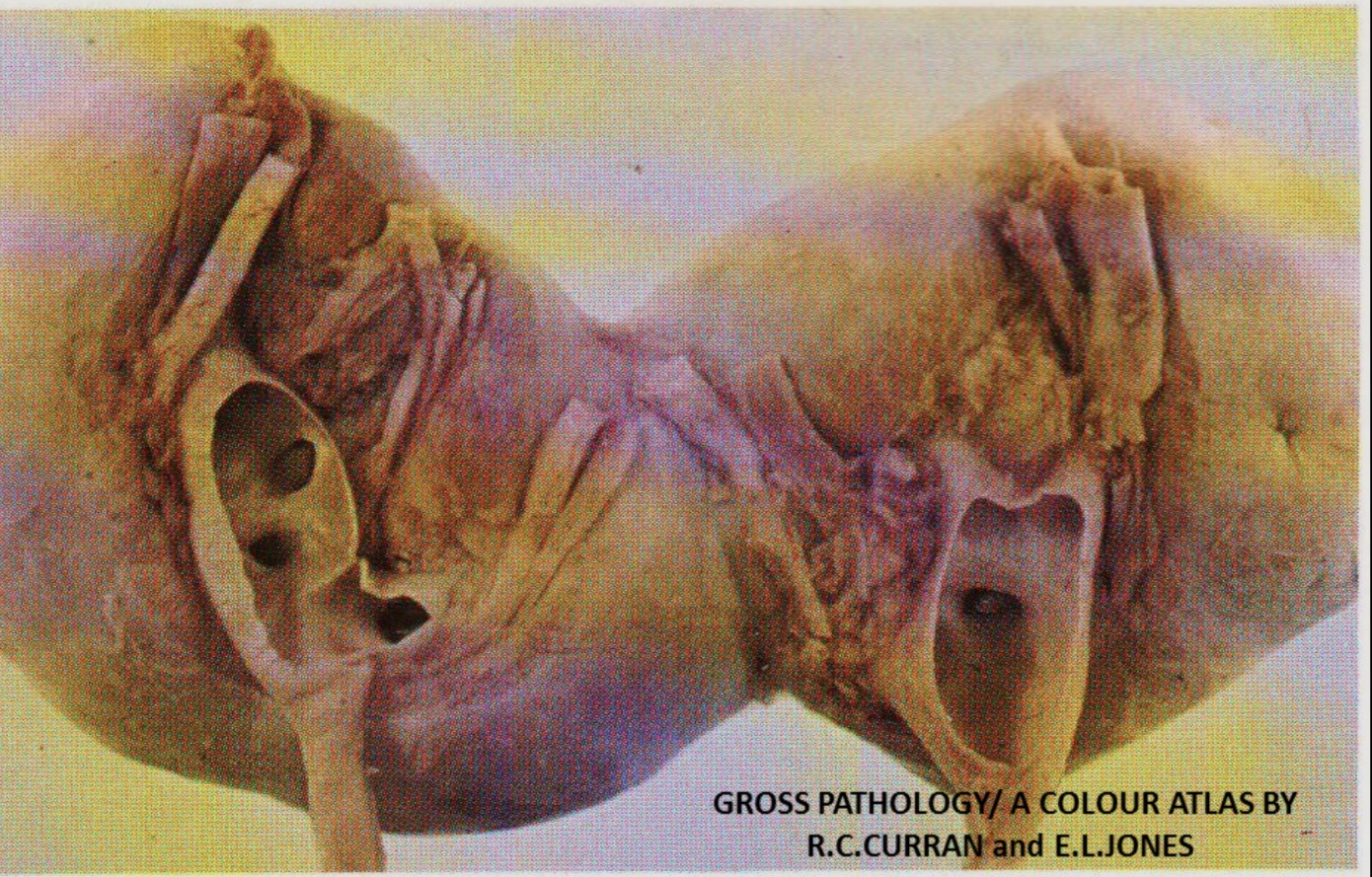
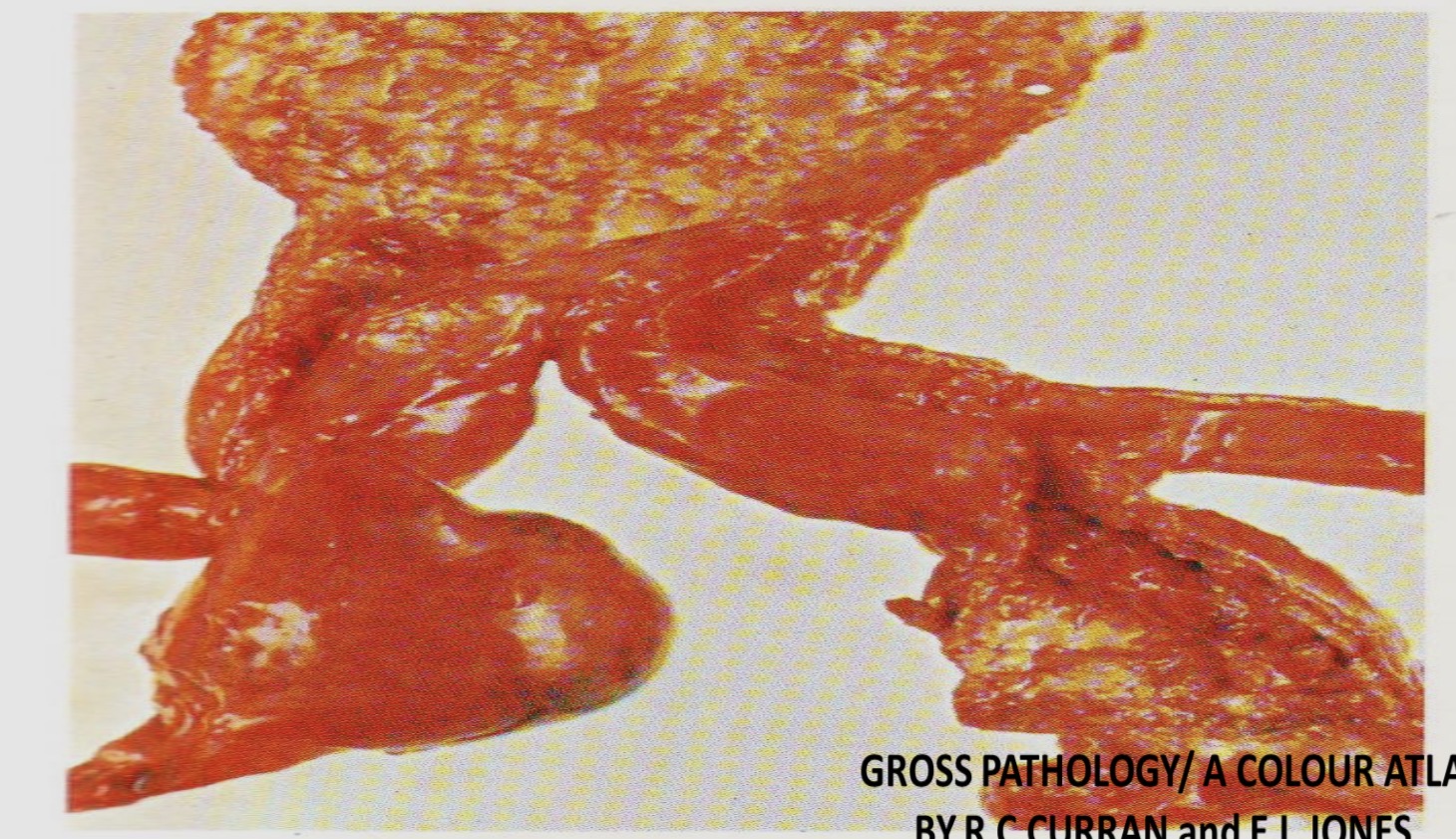
ongenital Fusion (Horseshoe) Kidney
Congenital fusion of the lower poles of both kidneys which are connected by fibrous band or by renal tissue that has given rise to a horseshoe appearance. Each kidney has its own separate pelvis and ureter
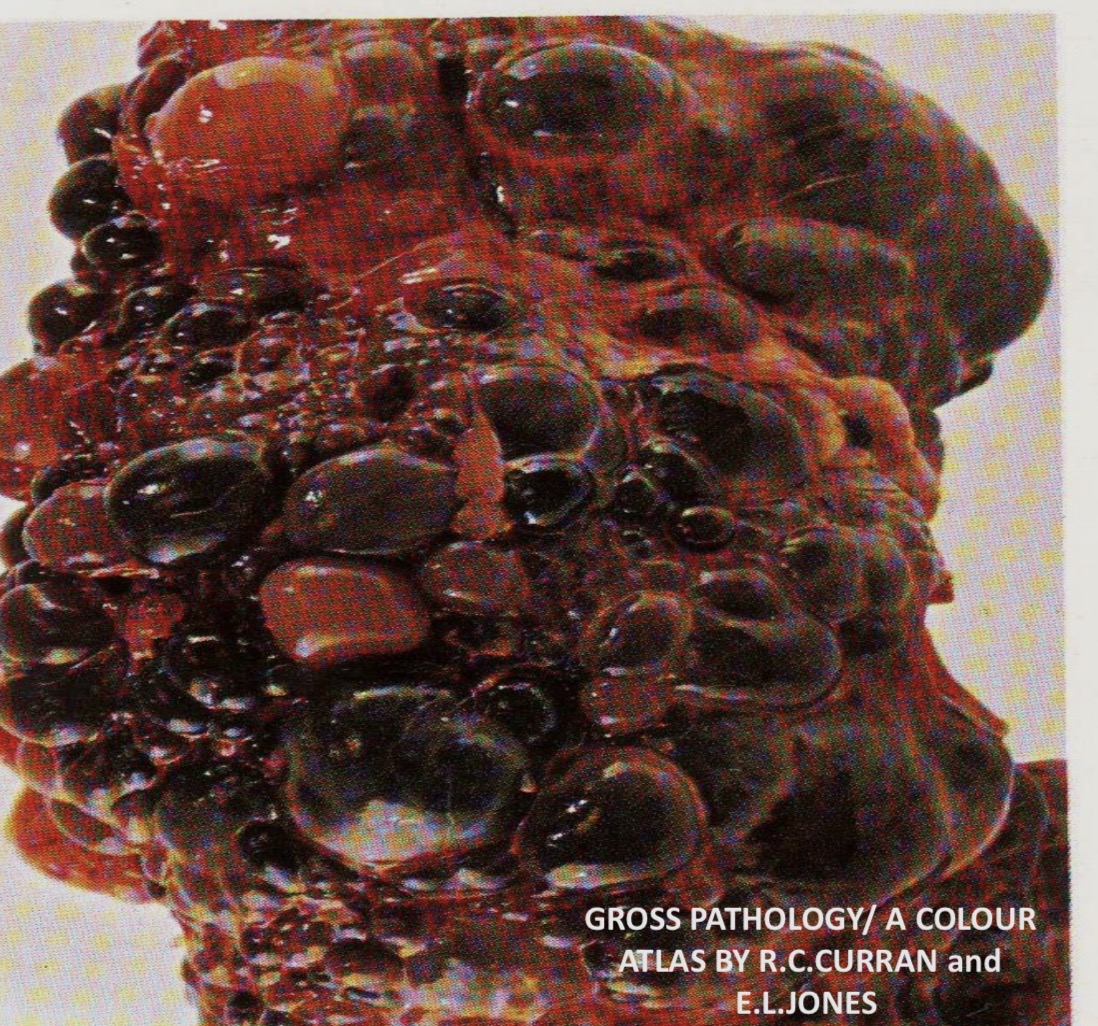
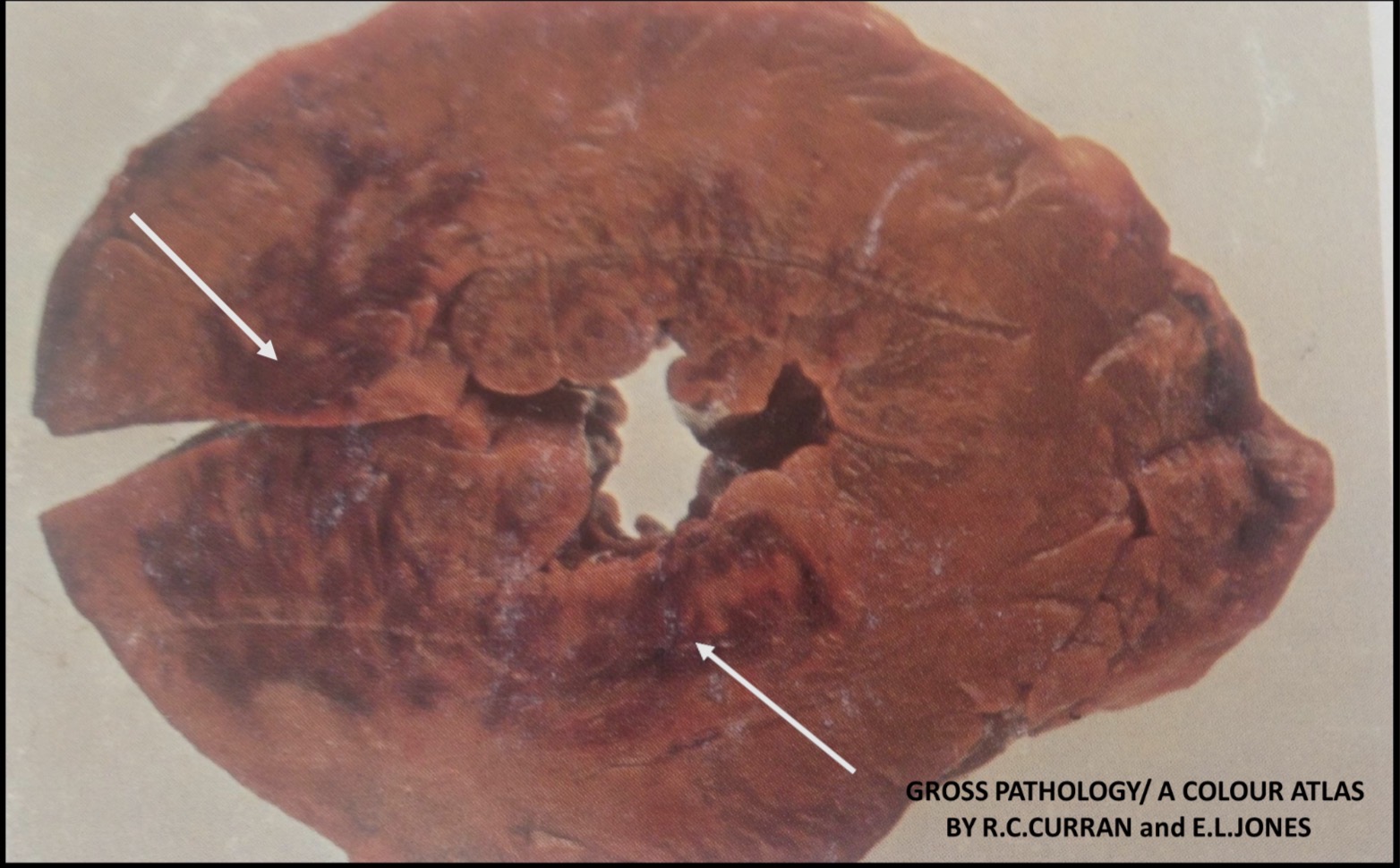
Polycystic Kidney ( Adult Type )
The kidney is enlarged and consists of small and large cysts bulging through the capsule. The dark bluish-black cysts contain altered blood and the lighter cysts contain urine

Polycystic Kidney (Infantile Type)
The kidney is enlarged . The cut surface is sponge-like due to the presence of numerous small cysts in the medulla
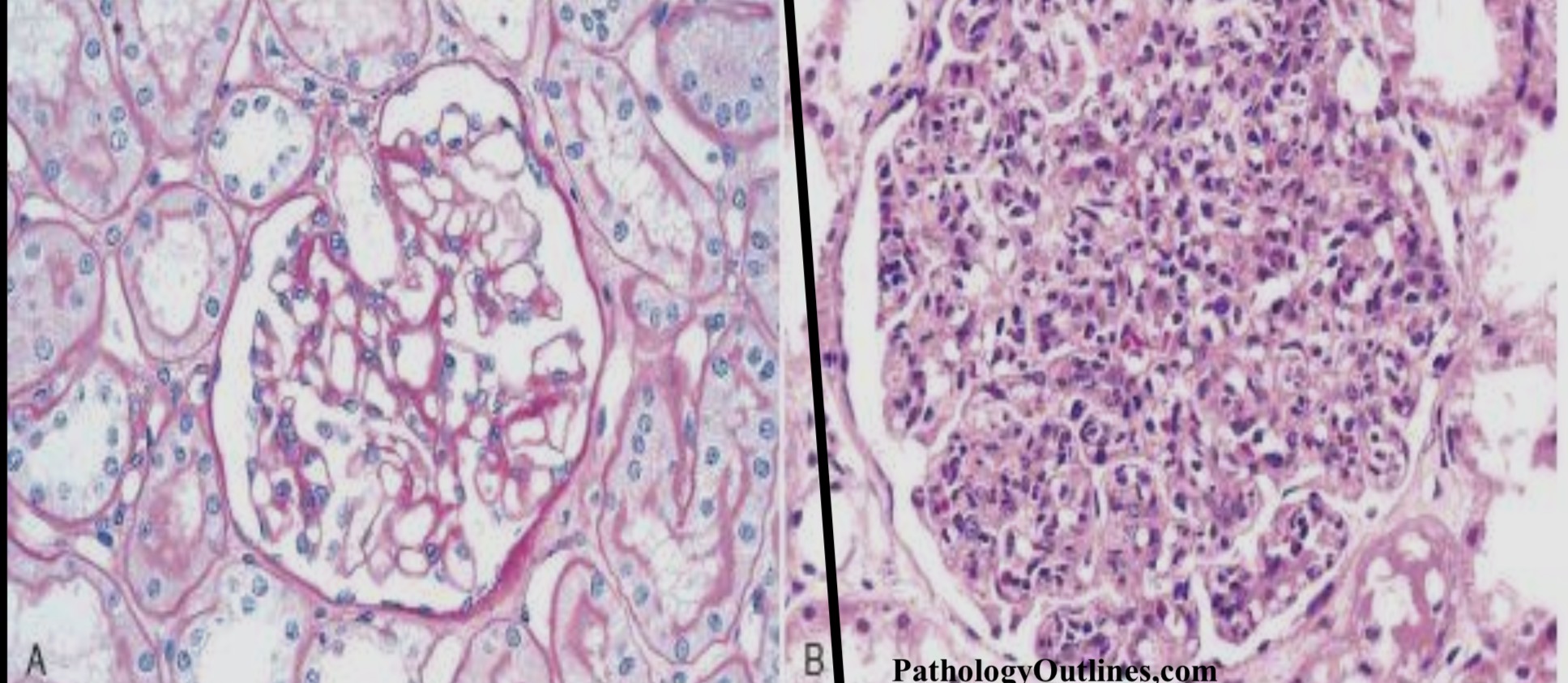
Normal glomerulus on the left compared with glomerulus in ADPGN (acute diffuse proliferative glomerulonephritis) on the right. The glomerulus is swollen and enlarged due to marked increase in glomerular cellularity in ADPGN