Mass Transport
1/76
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
77 Terms
What are haemoglobins?
A group of chemically similar molecules found in many organisms that have evolved to make them efficient at loading oxygen in a certain set of conditions and unloading them in another.
Describe the structure of haemoglobin
Primary structure made of a specific amino acid sequence in the 4 polypeptide chains, secondary structure where the chains are coiled into a helix, tertiary structure where each chain is folded into a precise shape, and the quaternary structure where the chains are linked to form a spherical molecule, and each chain is associated with a haem group containing a ferrous (Fe2+) ion.
How many oxygen molecules can haemoglobin carry?
Each haem group can carry one, and there are 4 haem groups so 4 molecules can be carried.
What is loading (associating) and unloading (dissociating)?
Loading: process by which haemoglobin binds with oxygen, unloading is the process by which haemoglobin releases its oxygen.
What is partial pressure?
Pressure exerted by one gas in a mixture of gases with the pressure directly related to the concentration of that gas.
What must haemoglobin be able to do to be efficient at oxygen transportation?
Be able to readily associate with oxygen at the surface where gas exchange takes place
Readily dissociate from oxygen at tissues requiring it
What property of haemoglobin allows it to both unload and load oxygen?
It can change its affinity (chemical attraction) for oxygen under different conditions - its shape changes in the presence of certain substances like CO2.
Why do different haemoglobins across species have different oxygen affinities?
Each species produce a haemoglobin with a slightly different amino acid sequence, so each one has a slightly different tertiary and quaternary structure, so different oxygen binding properties - some have high oxygen affinity, some have low.
What does high and low O2 affinity mean?
High: means oxygen can be loaded more easily but released less easily, low: means oxygen cannot be taken up as easily but is released more easily.
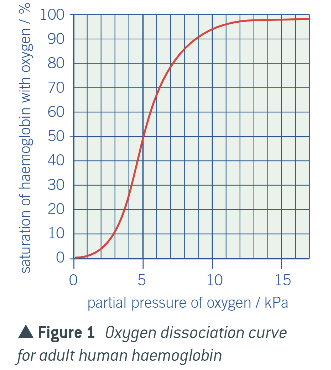
Explain this oxygen dissociation curve:
The shape of the haemoglobin molecule makes it hard for the first O2 molecule to bind to one of its sites as they are closely united, so at low O2 partial pressures little oxygen binds to haemoglobin, so curve is shallow.
When first O2 binds, quaternary structure changes causing it to change shape, making it easier for other subunits to bind to O2 molecule, so first binding induces other subunits to bind.
Takes a smaller increase in O2 conc to bind the second O2 molecule than it did for the first - known as positive cooperativity, and the curve steepens as more haem groups are bound to oxygen so makes it easier for O2 to be picked up.
However when the 4th O2 molecule is reached there is a lower probability that the O2 will find an empty binding site, so the curve reduces.
What does it mean if the oxygen dissociation curve is further to the left or right?
Left means haemoglobin has greater oxygen affinity, so it loads it readily but unloads it less easily, and further to the right means the affinity is lower so loads O2 less easily and unloads it more easily.
What are erothrocytes, and what are their adaptations?
Red blood cells, have biconcave structure which gives a large surface area so O2 can readily be loaded, have many molecules of haemoglobin, and have no nucleus to allow for more O2 to bind.
Give the equation for formation of oxyhaemoglobin:
Hb + 4O2 ⇄ Hb(O2)4
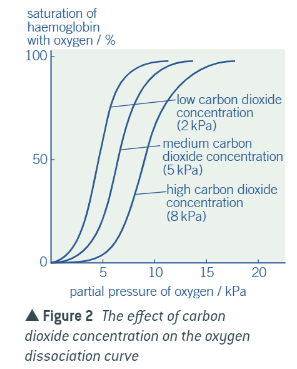
How does the dissociation curve and CO2 conc explain oxygen unloading and loading in different parts of the body?
It is rapidly loaded at higher partial pressures like in the alveoli, so become saturated with O2 to form oxyhaemoglobin. The reduced CO2 concentration means the curve shifts to the left, further increasing affinity for oxygen. However as you enter respiring tissues there is a lower O2 partial pressure, so O2 quickly dissociates to release the oxygen. Increased CO2 concentration shifts O2 dissociation curve to the right.
Explain the Bohr effect at respiring tissues:
CO2 produced at respiring cells
CO2 dissolves into blood plasma, and combines with water to produce carbonic acid
This lowers the pH due to acid dissociating into H+ ions, and this low pH changes the shape of the haemoglobin
Causes them to have a lower affinity for O2, so O2 dissociates more readily so is released to respiring tissues.
Explain the Bohr effect at gas exchange surface:
CO2 is constantly being removed at alveoli
pH is slightly raised due to low CO2 concentration, and this changes haemoglobin shape into one that has higher O2 affinity
Causes it to load oxygen more readily so it can be carried to respiring tissues
What is the Bohr shift?
As CO2 conc increases the dissociation curve is shifted to the right, meaning in high CO2 concentrations oxyhaemoglobin dissociates more readily, so oxygen is released more quickly (has a lower O2 affinity)
What happens when rate of respiration increases in terms of CO2 conc and O2 affinity?
Increase means more CO2 is produced, so pH is lower, so haemoglobin changes shape more, so O2 is more readily unloaded so more O2 is available. Also, lactic acid may be produced which further reduces oxygen affinity.
In practice, do all haemoglobin molecules get loaded with their maximum of 4, and what happens with the number of unloaded molecules in active vs not active tissue?
No, so overall saturation is normally at 75%, and when it reaches tissue with a low respiratory rate, only one of these molecules will be released, so blood returning will be about 75% saturated, but if a tissue is active then all molecules will be unloaded.
What happens to the dissociation curve of foetal haemoglobin?
It has an increased affinity for oxygen, so the curve lies to the left. The haemoglobin operates more effectively at the lower levels of oxygen in foetal blood, the steeper curve means Hb can become quickly saturated with oxygen at lower levels that exist across the placenta, so O2 diffuses from mother to foetus due to concentration gradient.
What happens to the haemoglobin and oxygen dissociation curve of a llama?
It lives at high altitudes, so partial pressure of O2 is lower so Hb has a higher affinity for oxygen, so the curve is shifted to the left
What happens to dissociation curves of active, small, fast respiration rate organisms vs large, slow animals?
Shifted to the right, so that Hb has a lower affinity so that O2 is rapidly delivered to the tissues, whereas large, slow inactive animals will have one shifted to the left.
Explain the dissociation curve of a lugworm?
Live in U shaped burrow, and when the tide goes out the worm cannot circulate a fresh supply of oxygenated water through its burrow, so the water contains progressively less oxygen, so the curve shifts to the left to allow them to load oxygen even at very low partial pressures. Hb with very high oxygen affinity
What factors determine if there is a specialised transport medium, or if it is circulated by a pump?
The surface area to volume ratio, and how active the organism is.
What are some common features of transport systems?
A suitable medium to carry materials, normally a water based liquid.
A form of mass transport where the medium is moved around in bulk over large distances
Closed system of tubular vessels containing the transport medium
Mechanism for moving the medium within vessels
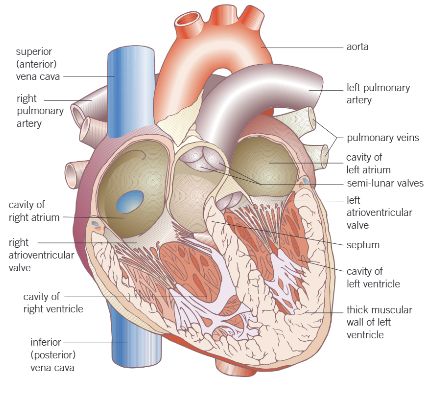
What is the heart, and briefly describe the structure?
Muscular pump located in the chest, made of cardiac muscle. Made of atria which are thin walled and elastic, and the ventricles which are much thicker as they have to contract strongly.
Why do mammals have a double circulatory system?
When blood enters the capillaries there is a very large drop in pressure, so blood flow to the rest of the body would be very slow, so mammals have a system where the blood is returned to the heart to increase its pressure before being distributed to the rest of the body.
Why does the left ventricle have thicker muscular/ elastic wall?
Enables it to contract with enough pressure to pump blood to the rest of the body.
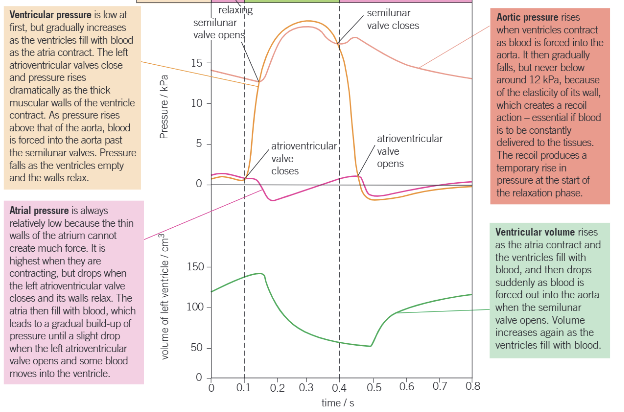
Describe the cardiac cycle:
Deoxygenated blood enters right atrium from vena cava, and oxygenated blood enters the left atrium from pulmonary vein. Walls of the atria contract, increase the blood pressure and force blood into ventricles via the atrioventricular valves opening. Ventricular walls contract so blood pressure increases and when pressure is higher in ventricles than atria, atrioventricular valves shut
How is the heart supplied with oxygen?
Supplied by the coronary arteries, and blockage of them leads to myocardial infarction (heart attack)
Outline the blood vessels of the heart:
Aorta connected to LV and carries oxygenated blood to body
Vena cava connected to RA and brings deoxygenated blood from body
Pulmonary artery connected to RV and carries deoxygenated blood to lungs
Pulmonary vein connected to LA and brings oxygenated blood from lungs
What are the risk factors for cardiovascular disease?
Smoking - produces CO that means blood pressure rises to supply tissues with the same amount of O2. Nicotine raises heart rate
Cholesterol
Diet
High blood pressure from genetics, lack of exercise
What happens in atrial systole?
Deoxygenated blood enters right atrium, oxygenated blood enters left, walls of the atria contract, increasing blood pressure and forcing blood into ventricles via atrioventricular valves opening. At this time ventricles are in ventricular diastole.
What happens in ventricular systole?
After a short delay to allow ventricles to fill with blood, their walls contract, blood pressure increases, forcing atrioventricular valves shut preventing backflow of blood. Valve tendons prevent valves turning inside out, and papillary muscles contract to keep valves taut. Blood pressure is higher in the ventricles than aorta/ pulmonary artery, so semi-lunar valves open and blood is forced into the vessels. Thick muscular walls create the high pressure.
What happens in atrial and ventricular diastole?
Atria and ventricular walls relax. The atria begin to fill again in this stage then will contract (systole). Relaxation of the ventricle wall causes blood pressure to drop below the arteries, so the semi lunar valves shut to prevent backflow of blood
Purpose of pocket valves?
In veins, and ensure that when the veins are squeezed, that blood flows back towards to heart, not away from it.
What is the design of valves?
Made of a number of flaps of tough but flexible fibrous tissue, cusp shaped. When pressure is greater on the convex side rather than the concave side they push apart.
Equation for cardiac output?
cardiac output = heart rate × stroke volume
Heart rate - number of beats per minute
Stroke volume - volume of blood pumped per minute
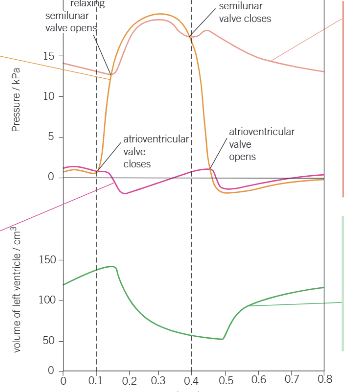
Explain this graph:
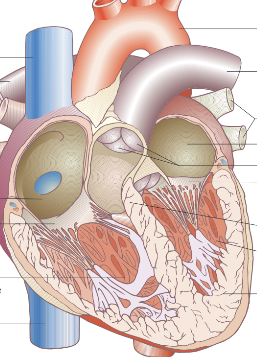
Label this heart diagram:
How is artery structure related to function?
Thick muscular walls which are thick compared to veins so that arteries can be constricted or dilated to control blood flow to certain areas.
Thick elastic tissue thicker than veins that can stretch and recoil to accommodate changes in blood pressure, and maintains high pressure, as well as smooth pressure flow in systole and diastole.
Thick walls to stop bursting under pressure
Small lumen maintains high pressure
Smooth epithelium to reduce friction so less blood clots
No valves as blood is under constant high pressure
Arteriole structure related to function?
Carry blood under lower pressure, and control blood flow between capillaries and arteries.
Muscle layer relatively thicker than in arteries, allowing for lumen constriction so blood flow into the capillaries can be controlled
Elastic tissue is thinner than arteries as blood pressure is lower
Vein structure related to function?
Transport blood slowly under low pressure back to heart.
Thin muscle layer as their constriction and dilation cannot control blood flow to tissues
Thin elastic layer as low pressure of blood will not cause bursting
Thin wall to allow for easy flattening and there is no risk of bursting.
Valves at regular intervals to prevent backflow of blood. Skeletal muscles near the veins compresses them and forces blood along - valves ensure this is towards the heart.
What are similarities between arteries veins and arterioles?
All have tough fibrous outer layer, muscle layer, elastic layer, smooth endothelium, and a lumen.
Capillary structure related to function:
Exchange metabolic materials like oxygen, CO2 and glucose.
Walls are extremely thin and only are 1 cell thick (endothelial cells), shortens the diffusion distance and increases rate of diffusion.
Highly branched increasing surface area
Narrow diameter and so permeate tissues, so no cell is far from a capillary and there is a short diffusion distance
Very narrow lumen so red cells are squeezed flat, bringing them closer to the cells so reducing diffusion distance
Permeable so oxygen and glucose diffuse into tissues and waste products diffuse into blood.
Spaces between endothelial cells so white blood cells can escape to deal with infection.
What is tissue fluid?
A watery intercellular liquid formed when substances leave the capillaries, and cells exchange substances with this fluid. Most of it returns to blood, and some enters the lymphatic system. It is the immediate environment of cells, and formed from blood plasma.
How is tissue fluid formed?
Hydrostatic pressure from the heart pumping (ventricular systole) is created at the arterial end of the capillaries, which causes tissue fluid to move out of the blood plasma - this includes water and small molecules, not plasma proteins. This pressure is opposed by hydrostatic pressure of tissue fluid outside capillaries, resisting outward liquid movement, and the lower water potential of blood due to plasma proteins, so some water moves into capillaries by osmosis. However the overall effect is to create a pressure pushing tissue fluid out of capillaries
Why do plasma proteins/ large molecules not leave the blood?
A collagen basement membrane around capillaries prevents such large molecules from leaving, called ultrafiltration.
How is tissue fluid returned to circulatory system?
Once it has exchanged metabolic materials it is returned mostly directly to capillaries.
Loss of tissue fluid from capillaries and friction between capillary walls reduces hydrostatic pressure inside them, so by the time blood reaches venous end its hydrostatic pressure is lower than tissue fluid around, causing tissue fluid to be forced back into capillaries by the higher hydrostatic pressure.
Blood plasma also has a very low water potential as it has lost water but still has plasma proteins, so water leaves tissue fluid by osmosis down a water potential gradient
Tissue fluid lost O2 and glucose but has now gained CO2 and other waste which diffuses into blood down a diffusion gradient.
How are contents of the lymphatic system moved?
Hydrostatic pressure of tissue fluid that has left capillaries, and contraction of body muscles that squeeze lymph vessels to ensure fluid moves towards the heart as well as valves being present, and returns to blood at the sub-clavian vein via thoracic duct at the base of the neck.
How is lymph formed?
Excess tissue fluid drains into lymphatic vessels and becomes lymph which is a straw coloured fluid.
how is blood flow in aorta smoothed
Elastic recoil
What is transpiration?
Loss of water from the leaves of plants by evaporation. This is a passive process as energy is provided by the Sun.
How does water leave air spaces around the stomata and enter the atmosphere?
Humidity of the atmosphere is less than the air spaces next to stomata, so there is a water potential gradient from the air spaces through the stomata to the air. Water molecules diffuse out of the air spaces into the surrounding air. Water lost by diffusion from air spaces is replaced by water evaporation from cell walls of mesophyll cells.
How is xylem tissue adapted to transport water?
It is composed of dead cells that join to form long empty tubes, there are no cell contents which maximises space for water transport.
Lack of cytoplasm means they are hollow so water flow is not restricted.
They have no end cell wall, or end cell walls with many holes, so less restriction of water flow.
Xylem is strengthened by lignin which occurs in rings, making the vessels very strong, so resist high tension and negative pressure, so do not collapse.
How does water move up the stem in the xylem?
Water moves by mass flow, and the driving force is transpiration, causing low pressure in leaves so water is pulled up.
Energy from the Sun causes water to evaporate from the leaves via the stomata
This establishes a water potential gradient across the mesophyll cells so water leaves the xylem.
Cohesive forces due to hydrogen bonding means that water molecules tend to stick to each other (cohesion), so other water molecules are pulled upwards to replace those leaving. This creates tension in the xylem.
Water is pulled up in a column across the mesophyll cells and down the xylem
Adhesive forces between water molecules and the walls helps maintain the column
What is cohesion tension?
The upward pulling force acting on water in the xylem can be so great that the water is under tension, exerting an inward pull on the walls of the xylem vessels
What is transpiration stream?
Column of water being pulled up the xylem as a result of transpiration.
How and why does the diameter of the tree change during the day?
Water evaporates from leaves, and rate of transpiration increases as the light intensity increases due to increased rate of photosynthesis.
Water loss reduces water potential in cells, and water is drawn out of the xylem
Water molecules are cohesive from H bonding, which creates more tension and more negative pressure.
This pulls the wall of the xylem vessels inwards and so the trunk shrinks.
At night when transpiration is lowest there is less tension so the diameter of the trunk increases.
What is evidence to support the cohesion-tension theory?
Changes in tree trunk diameter
If the xylem vessel is broken and air enters it, the tree cannot draw up water, as the continuous column is broken and water molecules cannot stick together.
When a xylem vessel is broken water does not leak out, but air is drawn up which is consistent with it being under tension
What is a mass potometer used for?
Measure change in mass of a plant as a result of transpiration (loss of mass as water evaporates).
Outline the process of using a capillary potometer?
Leafy shoot is cut under water.
Potometer is filled completely with water so there are no air bubbles.
Rubber tube is used to fit the leafy shoot to the potometer
An air bubble is introduced to the capillary tube, and the distance it moves in a given time is measured multiple times and a mean is calculated.
Volume of water lost is calculated and plotted against time on a graph
Limitations of a potometer:
Water loss from air tight seal
Water loss from capillary tube
Water could be used in photosynthesis
Water may be used to maintain turgidity
How does temperature affect rate of transpiration?
High temperature increases the rate of evaporation of water from the surface of spongy cells because it increases the kinetic energy of water molecules. Raises water potential in the sub-stomatal air space so molecules are moving faster, so transpiration increases.
How does humidity, air movements, and light affect rate of transpiration?
Humidity - high humidity means a higher water potential in the air surrounding the stomata, so lower water potential gradient between sub-stomatal air space and the air outside, so less evaporation.
Air movements - wind removes boundary layer of water molecules outside the leaf which increases water potential gradient between inside and outside which causes increased transpiration rate.
Light stimulates plants to open their stomata to allow gas exchange for photosynthesis, which increases rate of transpiration.
What is translocation?
Process by which organic molecules (amino acids, sucrose) and some mineral ions (K+, Cl-, Mg2+) are transported from one part of the plant to another.
What is phloem tissue comprised of?
Made of sieve tube cells which form long columns with perforations in the end walls called sieve plates. The cells are alive but have no nuclei and other organelles, cytoplasm is reduced to strands around the edge, and these strands pass through holes in the sieve plates to form a continuous filaments. Each sieve tube cell is associated with one or more companion cells that are connected by plasmodesmata and provide proteins, ATP etc.
What are sources and sinks?
Sources: sites of production of sugars from photosynthesis
Sinks: Places in the plant where the sugars will used, and the phloem transports from source to sink
What is mass flow theory?
The idea that translocation is driven by mass flow, which is then driven by a combination of active transport and evaporation (energy from the Sun).
How is sucrose transferred into sieve elements from photosynthesising tissue?
Sucrose is manufactured from the products of photosynthesis in cells with chloroplasts
Sucrose diffuses down a conc gradient by facilitated diffusion from photosynthesising cells to cell spaces. Hydrogen ions are actively transported from companion cells into spaces within cell walls using ATP
These ions diffuse down a conc gradient through carrier proteins into companion cells. Sucrose molecules are transported along with the ions via co-transport.
Sucrose then diffuses into the sieve element via plasmodesmata
How is sucrose transported through sieve elements to the sink?
The sucrose moves into the sieve tube elements, causing them to have a lower water potential, xylem has a higher water potential so water moves down the concentration gradient from xylem to phloem creating a high hydrostatic pressure.
This causes movement of sucrose to the sink where hydrostatic pressure is lower.
At the sink sucrose is used up in respiration or converted to starch. Cells have a low sucrose concentration so sucrose is actively transported from sieve tubes to cells, lowering water potential.
Water also moves into cells by osmosis due to lower water potential. This lowers hydrostatic pressure, so establishes a pressure gradient so that phloem contents move from high (source) hydrostatic pressure to lower (sink) pressure.
What is evidence for and against the mass flow hypothesis?