Burn Injuries
1/85
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
what is the largest organ of the body?
the skin
what is the epidermis?
1. top layer
2. protective layer
3. replaced about every 30 days
4. pigment
5. vitamin D synthesis
what is the dermis?
1. 90% of the skin's thickness
2. strength and elasticity
3. contains roots of hair follicles and nerve endings
4. oils and sweat producing glands
5. blood vessels (nutrient delivery to the epidermis)
what is the hypodermis?
1. fatty layer
2. cushions muscle and bones
3. contains CT
4. helps regulate temperature
5. nerves and vessels pass through (both are larger in this layer)
what kinds of problems do you anticipate in patients with burn injuries?
1. inflammation
2. perfusion
3. infection/sepsis
4. clotting (DIC)
5. acid base imbalance
6. e-lyte imbalance
7. nutrition compromise
8. rhabdomyolysis
9. compartment syndrome
10. paralytic ileus
11. ARDS
what do nurses most need to know about burn management?
1. basic understanding of mechanism and classification
2. how to stabilize a patient with burn injury and provide initial emergency management
3. when it is appropriate to transfer a patient to a burn center
when is it appropriate to transfer a patient to a burn center?
how do we classify burns?
1. etiology
2. burn depth
3. TBSA percentages
4. severity
what are the different etiologies of burns?
1. thermal
2. electrical
3. chemical
4. radiation
what are thermal burns?
1. MOST COMMON
2. depends on temp and duration of contact
3. flash, scald, contact
what are electrical burns?
1. LESS COMMON
2. "the grand masquerader"
3. contact points must be identified (multiple organ involvement in the midst of the path)
4. cardiac and/or pulmonary arrest is possible
5. continuous cardiac monitoring for at least 24-48 hrs
6. fluid resuscitation needs will be SIGNIFICANT
7. rhabdomyolysis (myoglobinuria) potential
what is rhabdomyolysis?
death of muscle cells with the release of muscle proteins (myoglobin), which can lead to a pre-renal AKI
what are the signs of rhabdomyolysis?
1. increased CK
2. increased K+ and phosphorus
3. decreased Ca+
4. + urine myoglobin
5. watch BUN/creatinine
6. metabolic acidosis
what is the hallmark sign of rhabdo?
dark, amber urine
what are chemical burns?
1. alkali burns tend to penetrate deep
2. organic compounds can be systemically absorbed (renal and hepatic injury)
3. safety of health care team must be considered (protective equipment, hazmat)
4. early recognition and continuous irrigation
we should irrigate with water for chemical burns until...
1. decrease in pain
2. temperature cannot tolerate
3. transfer to burn unit
what are radiation burns?
1. LEAST COMMON
2. most likely due to sun poisoning
3. prolonged full body exposure to ionization
4. main focus is to HYDRATE
what can prolonged full body exposure to ionization cause?
1. N/V
2. diarrhea
3. fatigue
4. H/A
5. fever
how can we identify the depth of burns?
1. superficial
2. superficial/partial thickness
3. deep partial thickness
4. full thickness
what are superficial burns?
1. mostly sun burns or steam injuries
2. blanchable (adequate blood flow to site)
3. medical management most often NOT needed
4. NO ice to the site
5. pretty painful

what are superficial/partial thickness burns?
1. blisters and peeling typically present
2. MAY need referral to burn center
3. keep it clean and use topical abx
4. VERY painful
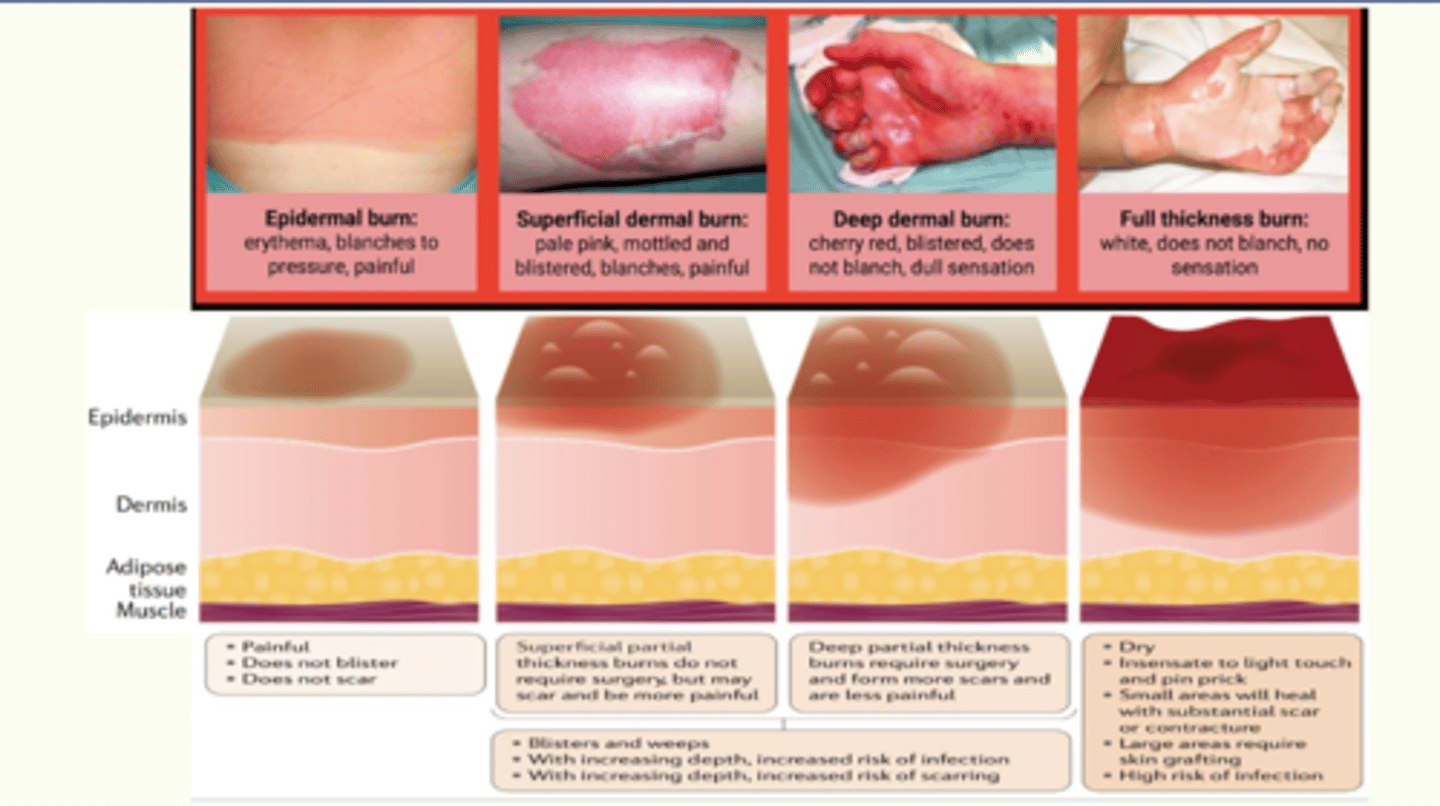
what are deep partial thickness burns?
1. borders may experience hyperemia
2. waxy center
3. sluggish or non-blanching
4. open or closed blisters
5. mottling
6. WILL NEED referral to burn center
7. not as painful or not painful at all (destroyed nerve endings)
what are full thickness burns?
1. dry, leathery, white, brown, black, charred tissue
2. non-blanching (may be contracted if muscle involved)
3. eschar-full thickness burn tissue
4. not as painful or not painful at all
5. WILL NEED referral to burn center
why is it often impossible to determine the exact depth of the burn on the initial inspection?
burns often evolve within the first 24-72 hours (frequent assessment is needed)
what zones do we want to frequently assess in the first 24-72 hours?
1. zone of coagulation
2. zone of stasis
3. zone of hyperemia
what is the zone of coagulation?
most contact, most damage
what is the zone of stasis?
most at risk for conversion
what is the zone of hyperemia?
increased blood flow/delivery of nutrients
what is the MOST important thing to do to promote perfusion in the first 24 hours?
fluid resuscitation
what is the TBSA percentages a guide for?
fluid resuscitation
what are the underestimation of TBSA consequences?
1. shock, renal failure, other organ failure
2. conversion of burns
what are the overestimation of TBSA consequences?
1. fluid volume overload
2. pulmonary edema
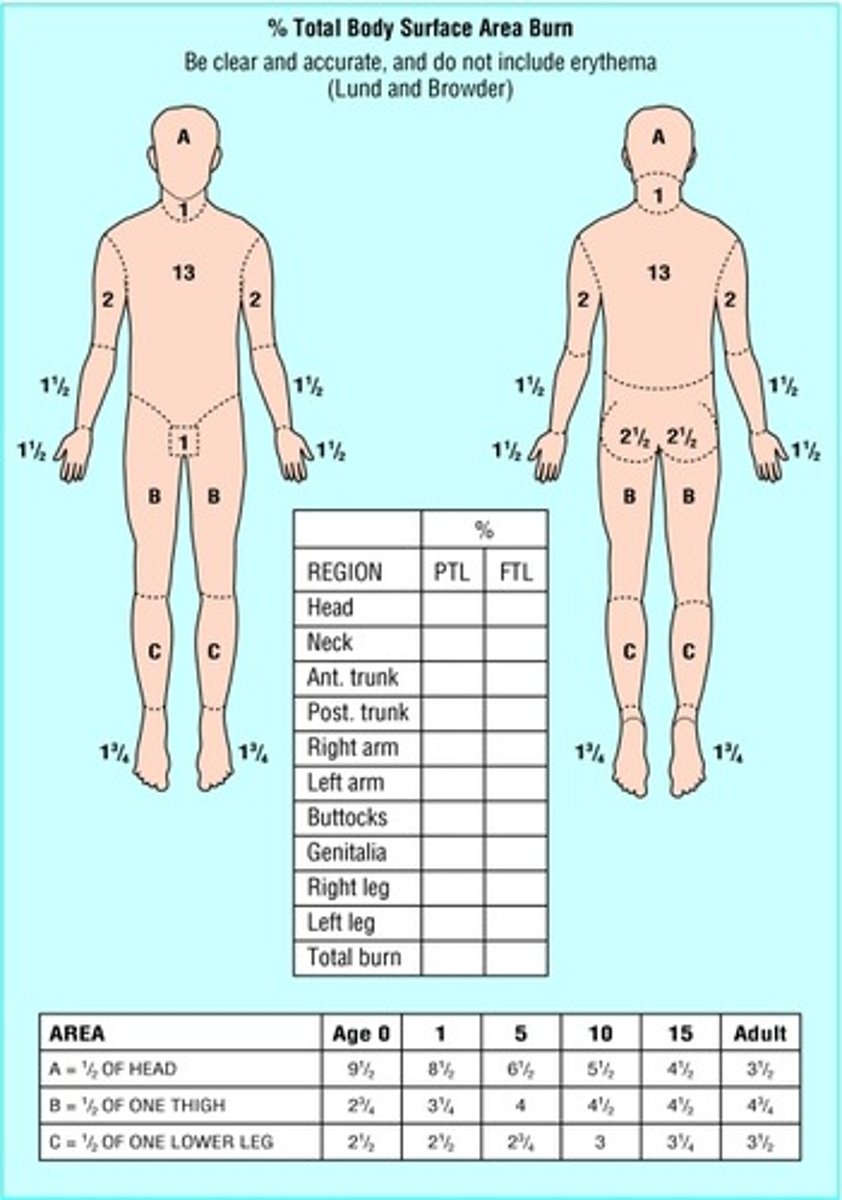
what are the methods for assessing surface area?
1. lund and browder classification
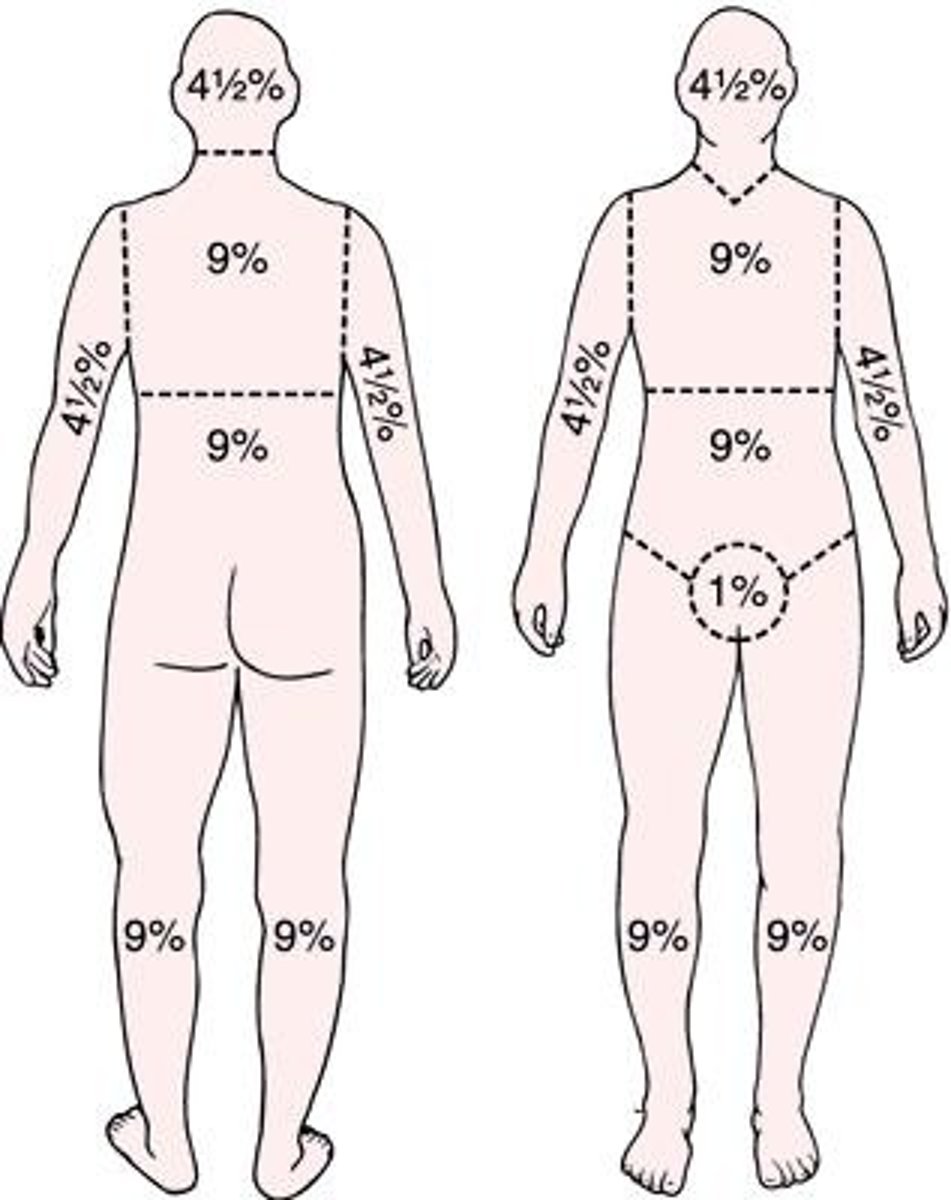
2. rule of palm
3. rule of nines
what is the lund and browder classification?
1. most accurate
2. used in the hospital setting
3. takes time
4. not our first choice
5. completed AFTER full and thorough debridement has been done
what is the rule of palm?
1. least accurate
2. used in the pre-hospital setting
3. quick
what is the rule of nines?
1. most commonly used
2. used in the pre-hospital setting
what should we note regarding the difference between children and infants?
there are different percentages based on age
what are the systemic effects of major burns?
1. burns that involve 20% or less of TBSA - local inflammatory response
2. burns that involve greater than 20% of TBSA - both local and systemic inflammatory effects
how can we determine the severity of the burn injury?
1. presence of inhalation injury (mortality risk is high)
2. patient age and past medical (mortality risk is high)
3. presence of concomitant injury
4. anatomical location of the burns
which locations of the burns trigger referral to a burn center?
1. face
2. hands
3. feet
4. genitalia
5. perineum
6. over major joints (most severe)
what are the initial priorities with a major burn at the scene?
1. stop the burn process
2. manage the airway
3. begin fluid resuscitation
4. prevent hypothermia
what is the top priority in response to a major burn injury?
airway
what is included in airway management?
1. 100% NRB on all patients
2. pulmonary assessment
3. ABGs, sat monitoring
4. assist with intubation if indicated (special care to secure ET tube, trach supplies at the bedside)
5. be aware of ARDS potential
6. assess for possible inhalation injury
7. obtain serum carboxyhemoglobin level (CO level)
when would intubation be indicated?
1. respiratory distress
2. facial burns
3. changes in voice
4. carbon in septum
5. enclosed space during fire (inhalation)
what can make it difficult to know if the patient has an inhalation injury?
1. even when no cutaneous burns
2. initial X-rays are often normal (bronchoscopy is needed)
3. be aware of the physical manifestations
what are the physical manifestations of an inhalation injury?
1. facial burns
2. singed nasal/facial hairs
3. carbonaceous sputum (soot), hypersecretion
4. naso or oropharynx erythema
5. excessive agitation/anxiety (hypoxia)
6. tachypnea, retractions, nasal flaring
7. inability to swallow
8. hoarseness, grunting, brassy voice
9. rales, rhonchi, diminished breath sounds
why is a pulse oximeter useless with CO poisoning?
doesn't know what the RBCs are actually saturated with
what are the clinical manifestations of CO poisoning?
1. mild H/A, confused
2. severe H/A, flushing
3. vision changes, disorientation
4. nausea, vomiting
5. irritability, dizziness
6. tachypnea, tachycardia
7. coma, seizures, death
what are the treatment options for CO poisoning?
1. 100% O2
2. possible hyperbaric O2
what is included in fluid resuscitation with major burns?
1. burn shock risk (distributive and hypovolemic)
2. two large bore IVs
3. parkland formula
4. possible inclusion of colloids
5. indwelling urinary catheter to monitor output
6. monitor for myoglobinuria (especially with electrical burns)
7. monitor response to fluid delivery
what is burn shock?
1. fluid shift first 8-36 hours after injury (peak around 24 hours)
2. watch for manifestations of shock
3. with resolution of shock, mobilization of fluid (diuresis)
4. evaporation loss of up to 5 L per day
what should be included with the two large bore IVs?
1. at least 20 G (can go through burn tissue if necessary)
2. IO can be used
3. central line useful
4. administer isotonic fluids
what is the parkland formula?
1. 2-4 mL LR x kg of body weight X TBSA %
2. half of the total volume given within the first 8 hours from when the burn injury occurs
3. remaining half over the next 16 hours
4. with an electrical injury, all ages will receive 4 mL/kg
how can we monitor the response to fluid delivery?
1. UOP - 0.5 mL/kg/hr, 1 mL/kg/hr if myoglobin is present
2. SBP - > 100 mm Hg
3. HR - < 120 bpm
4. CVP - 5-10 mm Hg (higher than normal)
5. pulmonary assessment - sounds clear, pH in range
6. GI assessment - abdomen soft/non-tender, no N/V, no ileus, bladder pressure < 10 mm Hg
7. LOC - A&OX4 (keep narcotic effects in mind)
in what situations would more fluids be needed?
1. inhalation and/or electrical injuries
2. associated trauma
3. alcohol/drug dependency
4. poor health
5. delay in starting fluid resuscitation
how can we prevent hypothermia?
1. keep the patient covered
2. monitor temperature (82-91 F recommended in the room)
3. increase ambient in room temperature
4. other external heat sources (fluid warmer, Baer hugger)
what is NOT the highest priority during the emergent phase?
1. cover with clean, DRY blankets
2. more significant care may be delayed for several hours
3. circumferential burns make wound care a higher priority
why do circumferential burns make wound care a higher priority?
1. possible need for escharotomy or fasciotomy
2. compartment syndrome (extemity)
3. abdominal compartment syndrome
what are we worried about with extremity compartment syndrome?
1. rhabdo/myoglobinuria potential
2. P's of NV compromise
what are the P's of NV compromise?
1. pain
2. paresthesia (earliest warning sign in burn pt)
3. polar
4. pallor (later)
5. pulseless (later)
6. paralysis
what happens to BP with abdominal compartment syndrome?
BP decreases due to fluid shifting from the third spaces into the abdomen AND increased pressure restricts blood flow and CO
what is included in pain management for burns?
1. IV narcotics, avoid IM route
2. possible use of anxiolytic drugs
3. monitor for respiratory depression
why do we want to keep an eye on renal function with burn injuries?
1. decrease in circulating volume/potential perfusion compromise
2. destruction of RBCs leads to free Hgb which can damage tubules
3. muscle damage can lead to myoglobinuria which can damage tubules
(burn patients at risk for an AKI, monitor BUN/CR/GFR/UOP)
what are additional labs of concern with burn injuries?
1. CBC (H/H, WBCs with differential) - WBC elevated d/t inflammation (not necessarily infection)
2. BG - increased d/t the stress response
3. DIC profile
4. electrolytes - Na+ decreased with fluid loss, K+ increased d/t acidosis and cell lysis
5. serum proteins - lose proteins with fluid shifting (NEEDS PROTEIN TO HELP WITH HEALING)
6. ABGs
what do the ABG changes look like with burn injuries?
1. metabolic acidosis
2. respiratory acidosis
3. mixed acidosis
what should be assessed with electrical burns?
1. 12 lead ekg
2. tropnin
3. CK-MB
what are the priorities in the intermediate phase of care?
1. wound healing and closure
2. pain management
3. ensuring optimal nutrition
4. continued infection prevention
what is super important about GI tract health and nutritional needs in the intermediate phase of care?
1. increased metabolic needs
2. decrease in nutrient absorption and motility (ileus potential)
3. use of prokinetic medications (metoclopramide, erythromycin)
4. medications for GI protection (PPIs, H2 blockers)
5. NGT
6. dobhoff tube may be placed
7. supplemental vitamins and minerals
8. assessment of nutritional status
because the patient has a decrease in nutrient absorption and motility, what should be done ASAP?
tube feeding or PO to replenish nutrients (dob hoff much preferred over TPN, want to use the gut)
what are the symptoms of an ileus?
1. abd distention
2. decreased bowel sounds
3. decreased passing gas
4. N/V
what are examples of PPIs?
protonix, nexium
what are examples of H2 blockers?
famotidine, tagamet
why can an NGT be used?
1. initially to relieve gastric distention, N/V (rest and decompress the gut)
2. prefer a dob hoff because it decreases the risk of aspiration
3. want to know if they can tolerate and prevent aspiration
how can we prevent aspiration with an NGT?
1. increase the HOB
2. check placement
3. check residuals and place back (should not have more than a few hours worth of residual)
what is included in wound care during the intermediate phase of care?
1. with pre-medication or in the OR
2. topical treatment/dressings
3. wrap fingers/toes individually (to avoid adhering to each other)
4. mechanical and enzymatic debridement
5. surgical debridement and closure grafting (autograft, prefer the patient's own skin)
what can be done to maintain autograft integrity?
1. constant contact
2. immobilization
3. vascular supply
4. skin care
5. monitor for infection
what area of graft placement poses the greatest risk for infection?
perineal grafts
what can be done to decrease the risk of infection for a perineal graft that has the potential to come into contact with stool or urine?
1. foley cath
2. rectal tube
what is the most common cause of death after the emergent phase?
infection leading to sepsis
what is included in infection and sepsis prevention in the intermediate phase of care?
1. infection control practices vary (some implement contact precautions)
2. teach patient and family infection control and unit policies
3. abx based on cultures (they are not automatically placed on antibiotics for prophylaxis)
4. standard sepsis screening NOT useful in the burn patient
why is standard sepsis screening not useful in the burn patient?
1. burn patient may demonstrate all the criteria for sepsis without actually having an infection or being septic
2. sepsis is burn patients, " a change in the burn patient that triggers the concern for infection "
when should sepsis be considered for a burn patient?
when three or more of the following criteria are met
what is included in the septic criteria for a burn patient?
1. <36.5 C or > 39 C
2. > 110 bpm
3. > 25 breaths per minute (not ventilated)
4. > 12 L/min minute ventilation (ventilated)
5. thrombocytopenia < 100,000
6. hyperglycemia w/out DM ( > 200 untreated plasma glucose, > 7 units of insulin/hr, > 25% increase in insulin requirements over 24 hr)
7. inability to continue enteral feedings > 24 hrs
what would indicate that the patient is unable to continue enteral feedings past 24 hours?
1. abdominal distention
2. high gastric residual (2x feeding rate)
3. uncontrollable diarrhea (> 2500 mL/day)
when does the rehabilitation phase of care begin?
when the patient is admitted and may last for several years
what is included in the rehabilitation phase of care?
1. emotional/psychological health (PTSD potential)
2. emotional/psychological health of the family
3. contracture prevention (joint splinting, PT, ROM)
4. prevention of hypertrophic scars (steroids, laser)
5. promotion of mobility, flexibility, comfort, psychosocial health
6. continued monitoring for infection, nutritional status, pain
7. community resources