NUR 283 Test 2 Questions and Answers | 2026 Update | 100% Correct-Galen College of Nursing.
1/128
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
129 Terms
Ventricular Tachycardia
CPR, Defibrilate, amiodarone, epi
What is this rhythm and how is it treated?
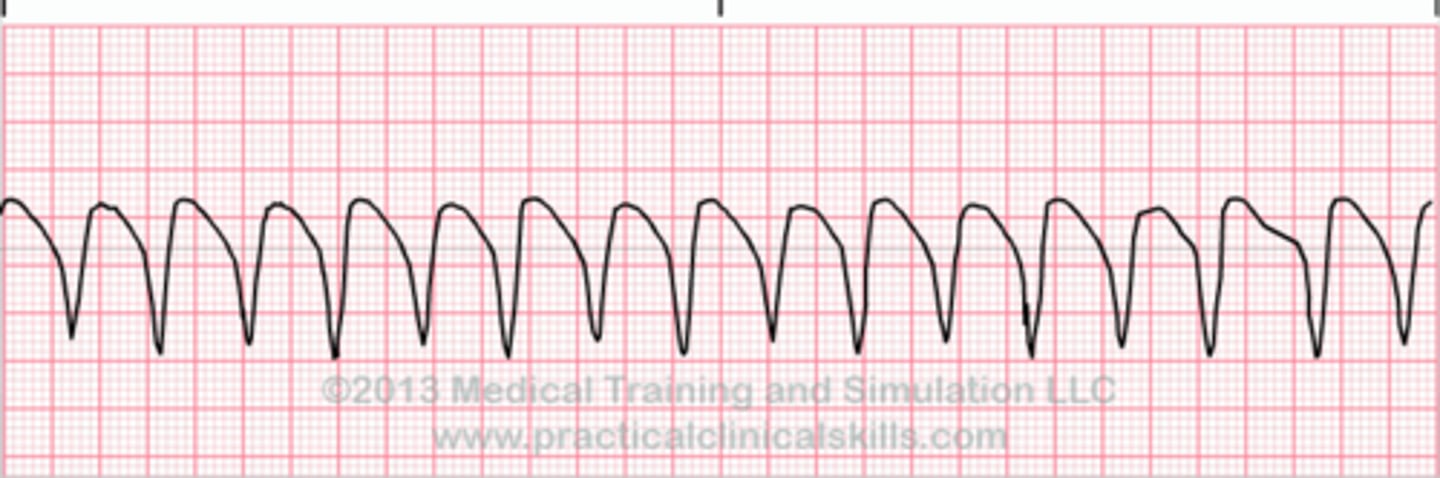
Ventricular fibrillation
CPR, Amiodarone, Defibrilate, Epi
What is this rhythm and how is it treated?

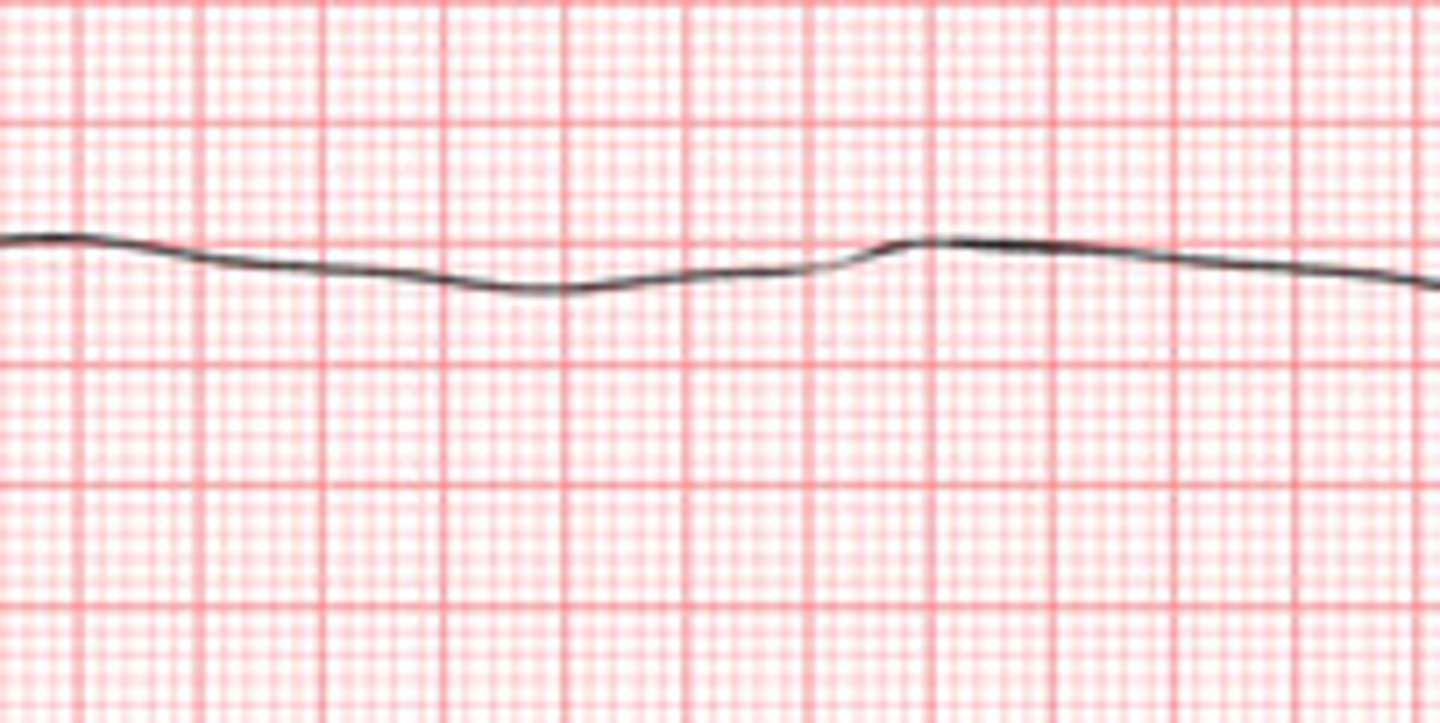
Asystole
CPR & Epinephrine
What is this rhythm? and how is it treated?
PVC or premature ventricular contraction
Treat the underlying cause:
1. hypoxemia (o2)
2. Ischemia (12 lead to confirm)
3. electrolyte imbalance (Mg+ or K+ replacement)
What is this rhythm? and how is it treated?

AFib
"control the rate and anticoagulate"
Synchronized Cardioversion and anticoagulation
What is this rhythm and how is it treated if unstable?

Give an antidysrhythmic (amiodarone)
Cardizem/Diltiazem
We don't defib because we are worried a clot has formed in the appendages which will travel to the brain or lungs when shocked
How is stable Afib treated?
AFib RVR
This is Afib plus tachycardia and it is treated as unstable Afib
Cardiovert
What is this rhythm? and how is it treated?

30%
What percent of cardiac output is lost due to Afib and loss of "atrial kick"?
this is a calcium channel blocker it decreases BP & decreases HR it is often given to help reduce the HR in Afib RVR along with Heparin/Warfarin
What does Cardizem/Diltiazem do?
1. Protamine
2. Vitamin K
3. if there is an active bleed or they are going to need surgery
What is the antidote for heparin?
What is the antidote for Warfarin?
When do we reverse anticoagulation?
1. recognition of sudden cardiac arrest ck for pt responsiveness and breathing
2. Activate the emergency response system (call a code or rapid)
3. CPR if no pulse, and while waiting on the crash cart to arrive. (Remember 30 compressions to 2 breaths)
4. Defibrillate- as soon as possible
what are the steps to BLS CPR?
2 leads ds
How many leads must Asystole be confirmed in?
Vasoconstrictor and (+) Inotrope
what is Epinephrine?
pacer spikes with no P or QRS
Usually a problem with battery or lead in the wrong place. the PM fires but doesn't cause a contraction
use an external pacemaker and call the Dr.
Turn up the the miliamps
What is failure to capture on a pacemaker?
The PM is unable to sense where or when the heart is depolarizing or repolarizing and delivers spikes at an inappropriate time
Pacer rep needs to be called to interrogate the PM
What is failure to sense?
this is called a R on T phenomenon
Causes vtach or torsades de point
What happens if pt is shocked mid repolarization between the S-T?
CO= HR x SV
What is the cardiac output formula?
CO- 4-6
pink warm and dry
>30 ml/hr UO
SBP >90
AOx4
MAP >60
Skin perusing cap refill <2second
What are signs and symptoms that cardiac output is good?
CVP 2-6 mmHg
Hypo/hypervolemic
What is the range for CVP?
signs of hyper/hypovolemia
hypovolemic=
skin tenting & dry mucous membranes
decreased CVP < 2
Hypervolemic=
Fluid overload/edema
increased CVP >6
What are signs and symptoms of a preload problem?
- if hypovolemic give fluids, albumin, blood
-if hypervolemic give a diuretic
How are CO problems related to Preload/SV treated?
1. is CO low?
2. Did the HR change?
3. Preload: What is CVP? hypo/hypervolemic s/s?
If normal move on...
4. Afterload, what is their BP? High or low?
if normal must be contractility...
5. (+) inotrope needed to increase contractility
What are the steps to determine the cause of low cardiac output?
BP over 140
BP below 90
If preload is fine and HR is fine it may be an afterload problem. What changes do you look for in an SV/afterload problem?
you need to reduce the BP, administer any kind of antihypertensive medication
ACE, ARB, BB, CCB
If SV BP is over 140 what treatment is expected?
You need to increase the BP administer a vasopressor/vasoconstrictor
Epi, Neo, dopamine, vasopressin, norepi
If SV BP is under 90 what treatment is expected?
Poor contractility
Administer a (+) inotrope
Epi
Digoxin
dobutamine
milronone
If both afterload and preload have been ruled out as the cause of low cardiac output what is the likely cause of low CO? and how is it treated?
>90
Stable BP
>60
Stable MAP
2-6
CVP
4-6
CO
0.5-2.0 ng/dl
Therapeutic range for Digoxin
15 or less
Normal ICP
We are looking for changes from baseline this is how you know if a person is getting worse or improving.
Why is a baseline assessment so important in Neuro?
Vagus nerve
10th cranial nerve
what nerve is responsible for the regulation of internal organ functions, such as digestion, heart rate, and respiratory rate, as well as vasomotor activity, and certain reflex actions, such as coughing, sneezing, swallowing, and vomiting
Balance
Eyes
Face
Arms
Speech
Time
BE FAST
Ischemic Stroke
What type of stroke that occurs when the flow of blood to the brain is blocked?
Hemorrhagic Stroke
What kind of stroke is caused when a blood vessel in the brain leaks or ruptures; also known as a bleed in the brain?
60 mins
What is the door to needle (TPA) time for a ischemic stroke?
They are looking for bleeding on the scan. If bleeding is found TPA is contraindicated. The patient will instead be taken directly to the OR to stop the bleeding?
Why is a CT w/out contrast done when a stroke is suspected?
Hemorrhagic Stroke
A patient comes the ED and c/o of the worst headache of there life. What do you suspect?
-hemorrhagic stroke will show up right away
-ischemic stroke will not show up right away it takes several hours in order to show on a scan.
What shows up on a CT depending on kind of stroke?
4.5 hrs
What is the maximum amount of time that can have elapsed since stroke symptoms started to administer TPA?
excessive bleeding, after administration of TPA ischemic strokes, can become hemorrhagic. This is why TPA is contraindicated in hemorrhagic strokes it will cause additional bleeding.
Neurological improvements
After administration of TPA what do you need to monitor for in your patient?
TIA (transient ischemic attack)
This is usually a sign that a bigger stroke has the potential to happen and is often a warning sign
If a patient has symptoms of stroke that occur but resolve in less than 24 hours, what kind of stroke did they most likely have?
This patient is ok to have a elevated BP and allowed to be hypertensive intentionally. The increased BP allows or helps to increase blood flow to go past the blockage and keep brain perfused preventing brain tissue death
What do we want the patient's BP to be at if they have suffered an ischemic stroke?
we don't want their BP to be high, so we either keep it in a normal range or below normal. If their BP is high they will continue to bleed into their brain and may cause worsened ICP.
If a patient suffers from a hemorrhagic stroke what is different about how we manager their BP?
High dose statins to prevent atherosclerosis
What medication class is often prescribed post stroke to patients after or during recovery?
1. Eye opening
2. response to verbal
3. Motor response
What is measured by the Glasgow coma scale?
Max score- 15
worst score- 3
comatose- 8
Glascow coma scale general numbers
they are allowed to sleep but they need to be woke up q1hr to do quick neuro checks
-LOC
What instructions are given to a patient with a head injury d/c home?
-racoon eyes
-battle sign (bruising behind ear)
1. Sniffing and swallowing alot
What are symptoms of a basilar skull fracture? what are symptoms of a possible CSF leak with this kind of fracture?
must catch or collect some to send for glucose testing to confirm CSF leak
A halo sign can be another clue but not complete confirmation
If a patient has a basilar skull fracture with suspected CSF leak how is this confirmed?
1. Widening pulse pressure
2. Cheyne Stokes Respirations
3. Bradycardia
What are the symptoms of Cushing's triad?
This is a in stage 4 brain herniation. and is permanent damage as the brain matter and brain stem have been squeezed through the foramen magna.
What is suspected if you find your neuro patient with ipsilateral pupil dilation?

-episodes of confusion
-NV
-pupils equal and reactive
-breathing normal
-BP normal or high
-pulse normal or high
-temp varies
Intervention in this stage carries the best patient outcomes
What are the patient neuro symptoms in stage 2 compensation? Intervention?
-beginning in ability to stay awake progressively deeper coma
-pupils small reactive progressively slowing response to light
-respirations may begin slowing
-pulse pressure begins to widen
-pulse bounding but slowing
Surgical or medical intervention needed now or patient will herniate
What symptoms are seen in stage three neuro decompensation?
-coma
-ipsilateral pupil dilation and fixation
-wide pulse pressure
-bradycardia slight irregularity
-cheynes stokes respirations to central neurological hyperventilation
Usually surgical or medical intervention is futile at this point
What neuro symptoms are seen during stage 4 herniation?
1. Mannitol - decrease ICP by removing fluids
2. Decadron (dexamethasone)- decrease ICP by reducing inflammation and swelling
3. Ventilator- protects airway
What are some medical interventions for a brain injury?
Allow CO2 to be lower and allow pt to blow off CO2 because it helps to decrease the pressure in the brain
What is unique about the CO2 level for a neuro patient in the ICU?
1. quiet room
2. dark room
3. decrease stimulation
4. drama free zone
5. HOB 30 degrees
6. no hip flexion above 90 degrees
7. log roll
8. no unnecessary suction, reduce sneeze, cough, vomiting's ect
9. keep fever down
10. coordinating care to decrease the number of room interruptions
What are nursing interventions for neuro injury in ICU?
patient urine output has increased
How do we know if mannitol is working?
electrolyte imbalance Na+
What do we watch for during mannitol administration?
when it lasts over 5 min it becomes a status epilepticus
When does a seizure become an emergency?
benzodiazepines usually Ativan
What is the rescue medication for seizures?
10-20
Dilantin therapeutic level
-dextrose
-filter tubing
-cardiac collapse
What can you never give Dilantin with? What kind of tubing is needed for administration? What happens if you administer it too fast?
headache,
nausea,
vomiting,
constipation,
dizziness,
spinning sensation,
drowsiness,
slurred speech,
loss of balance or coordination,
swollen or tender gums,
sleep problems (insomnia),
nervousness,
tremors, or
rash.
What are the side effects of Dilantin?
Gingeval hyperplasia
What oral side effect can Dilantin cause?
-never hold down pt
-loosen clothing or restraint
-nothing in mouth
-protect airway
-suction (wait until seizure over to suction or do oral care)
-protect from injury
-do not leave pt
-time seizure
-ok to turn on side if appropriate
seizure precautions
there is reduced glucose in the CSF because bacteria love glucose
How do we know if the meningitis is bacterial?
- nuchal rigidity
-bruzinski sign
-kernig sign
-HA
-photosensitivity
S/S of meningitis?
Fetal position
What is the safest position to be in for a LP to check for meningitis?
"Dry inside"
fluid is lost in excess leaving behind the Na+
this means high blood serum osmolarity and low osmolarity in urine
causing decreased specific gravity below 1.005 and increased Na+ above 145
These patients are dehydrated and need fluid replacement and desmopressin to stop loss of fluids through excessive urination
Diabetes Insipidus
"Wet Inside"
This patient has too much fluid inside
low blood serum osmolarity and more concentrated urine
Causing increased specific gravity above 1.030 and Na+ below 135
These patients need a diuretic to get rid of the excess fluids
SIADH (syndrome of inappropriate anti-diuretic hormone)
When a pt has lost brain function the organs start to shut down and begin to deteriorate
What is unique about brain death and organ donation?
-no spontaneous respirations
-absent reflexes
-EEG will be flat
-perfusion studies so decreased or no perfusion
-cold caloric test is negative
-Dolls eyes is negative
What criteria is used to determine brain death?
test the ocular vestibular nerve by shooting ice cold water in the ears. A normal result would be the eyes should turn towards the ear that has the ice water in it.
what is a cold caloric test?
(-) open eyes move side to side and eyes stay fixed
(+) open eyes move head side to side and the eye move opposite to the head movement
A negative result is indicative of brain death
What is a dolls eyes test?
Patient will not be able to breath on their own they will need a mechanical ventilator
What is unique about a spinal cord injury around the C4 or above area?
They are considered a quadriplegic or tetraplegic
What is a patient considered if they have a spinal injury between T6 and C5?
They are considered a paraplegic
If a spinal injury occurs below T6 what are they considered?
-nutrition
-bowel and bladder training
-skin breakdown
-preventing muscle atrophy and contractures
-preventing aspiration
-maximizing ADL's
What care is focused on if a patient has suffered a spinal injury?
Active range of motion is carried out by the patient themselves and cannot be utilized by patients that have paralysis. Passive range of motion is carried out with the help of a physiotherapist, nurse, or mechanical device
What is the difference between active and passive range of motion?
fear the fracture will become a spinal cord injury
What are we worried about with a vertebral fracture?
-Cspine immobilization
-xray to look for bone fragment near the cord
What do we do if we suspect a vertebral fracture?
temporary paralysis that can last for up to 1 year
What is spinal cord shock?
T6 injury and above can cause this
What kind of injury can cause autonomic dysreflexia/ hyperreflexia?
this is a life threatening emergency and is caused by a stimulus below the spinal cord injury that the autonomic nervous system doesn't know how to interpret.
Causing
-Extreme HTN
-Diaphoresis
-Bradycardia
-JVD
What is autonomic dysreflexia/hyperreflexia?
Find the cause and fix it....
1. elevate HOB
2. loosen sheets, clothing anything constrictive, look for foley kink or cap in bed (anything causing pressure)
3. treat BP with fast-acting medication to lower BP
What are the interventions for autonomic dysreflexia?
Green (walking wounded)
Black (deceased)
Red (immediate care needed)
Yellow (injured but can wait to be seen)
What are the mass casualty color codes for triage?
RR > 30
Cap refill > 2 seconds
No radial pulse
decreased LOC
What qualifies a person for Red tag in mass casualty triage?
Green (walking wounded)
Anyone that can walk to leave the casualty scene independently is considered what color?
Open airway if not breathing move on
When determining if black or red what does you check?
Redness is superficial - it is the top most layer (epidermis)
Treatment is cool water immersion No ice this causes tissue necrosis
What is a first degree burn?
Partial thickness burn- dermis is affected and blisters are open or closed
These burns require wound care and they are very painful
What is a second degree burn?/
Full thickness burns that affect the subq layers muscle, bone and organs.
This patient will require a skin graft
What is a third degree burn?
Check Airway
Step 1- burn ID them
determine if they need to go to a special burn unit
Step 2- Fluid replacement
Large bore IV's at least 2
What are the initial steps when treating a burn victim?
Urine output is between 30-60 mL/hr
When do we know if fluid replacement has been adequate on a burn victim?
1. burn ID (rule of 9)
2. manage airway -look for signs of burn hair, soot ect
3. IV access
4. fluid replacement
5. pain control
6. electrolyte replacement
What treatment is done in the phase 1 emergent phase of burn treatment?
Diuresis phase kidney's suddenly start releasing a lot of fluid this is a good sign.
maintain oxygenation
replace nutrition
wound care
mobility exercises
infection prevention
What care takes place during the acute phase 2 of burn care?