the kidneys
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
what does urinary excretion allow us to remove from the body 3
excess water, electrolytes and metabolic waste
briefly, how does the kidney form urine
filters blood
reabsorb wanted ions/water
excrete waste/urine
which part of the kidney does blood filtration happen in
what is the specific name for this process
what is the capillary structure called in bowman’s capsule
renal cortex
ultrafiltration
glomerulus
what cells is bowman’s capsule made of
what enters and exits
epithelial cells
afferent - efferent arterioles
what type of capillaries does the kidney have
what does GRF stand for and mean
Kf and σ
fenestrated capillaries (discontinuous endothelium)
glomerular filtration rate (rate of fluid filtration from the renal capillaries into bowman’s space)
filtration coefficient (permeability of capillary to water)
reflection coefficient (how IMpermeable the capillary is to proteins)
what is this the equation for: Kf • [(PGC – PBS) - σ(πGC – πBS)]
what part of the equation is responsible for high filtration rate
what is the secondary barrier in filtration - how
what are the different parts of these cells
GRF
Kf - increased filtration coefficient
podocytes - they wrap round glomerular capillaries to prevent cells and proteins entering
podocyte cell body - primary processes - secondary processes - foot processes
what are the two types of nephrons (extra info)
under a microscope, what is the difference between PCT and DCT
Cortical (superficial) and Juxtamedullary
PCT - brush border of villi (most Na+ absorption), spaced nuclei / DCT - no brush border, dense nuclei
reabsorption:
what are the two routes this can happen by (TC/PC)
what 3 things is it driven by
what 2 types of transport can power transcellular transport against a conc gradient
Transcellular - requires both the luminal and basolateral membrane to be permeable to water or the solute of interest
Paracellular - depends on the tightness of the junction between the cells (tight/leaky)
concentration/ osmosis/ electrical gradients between tubular and interstitial fluids
primary/secondary active transport
reabsorption in PCT:
what is the process called IFR
how does it slow flow and what does this allow
fluid entering loop of henle will be ….
example of 3 things absorbed
isosmotic fluid reabsorption
it reduces volume of fluid - slow - allows more time for exchange in the rest of nephron
isosmotic
HCO3-, aa, glucose
isosmotic reabsorption
how do glucose and amino acids enter blood, what does this drive the uptake of
how is Cl- absorbed
reabsorption of NaCl creates what gradient
what is absorbed as a result and how
transcellular reabsorption, drives Na+ uptake
Cl- enters paracellularly
osmotic gradient
water enters paracellularly - leaky junctions
how is a Net Filtration maintained in glomerulus
how is BP reduced in efferent arteriole
how is colloid osmotic pressure increased
what two pressures favour a net reabsorption of fluid into capillaries
high BP and low colloid (albumin/protein) pressure
filtration of plasma from blood
proteins are retained in smaller plasma volume
low BP, high CP
ENDOCRINE SIGNALS: what effect do these have on reabsorption
anti-diuretic hormone ADH
NORADRENALINE
Aldosterone
^^ water plasma
^^ Na+ plasma
^^ Na+ plasma so — K+ leaves
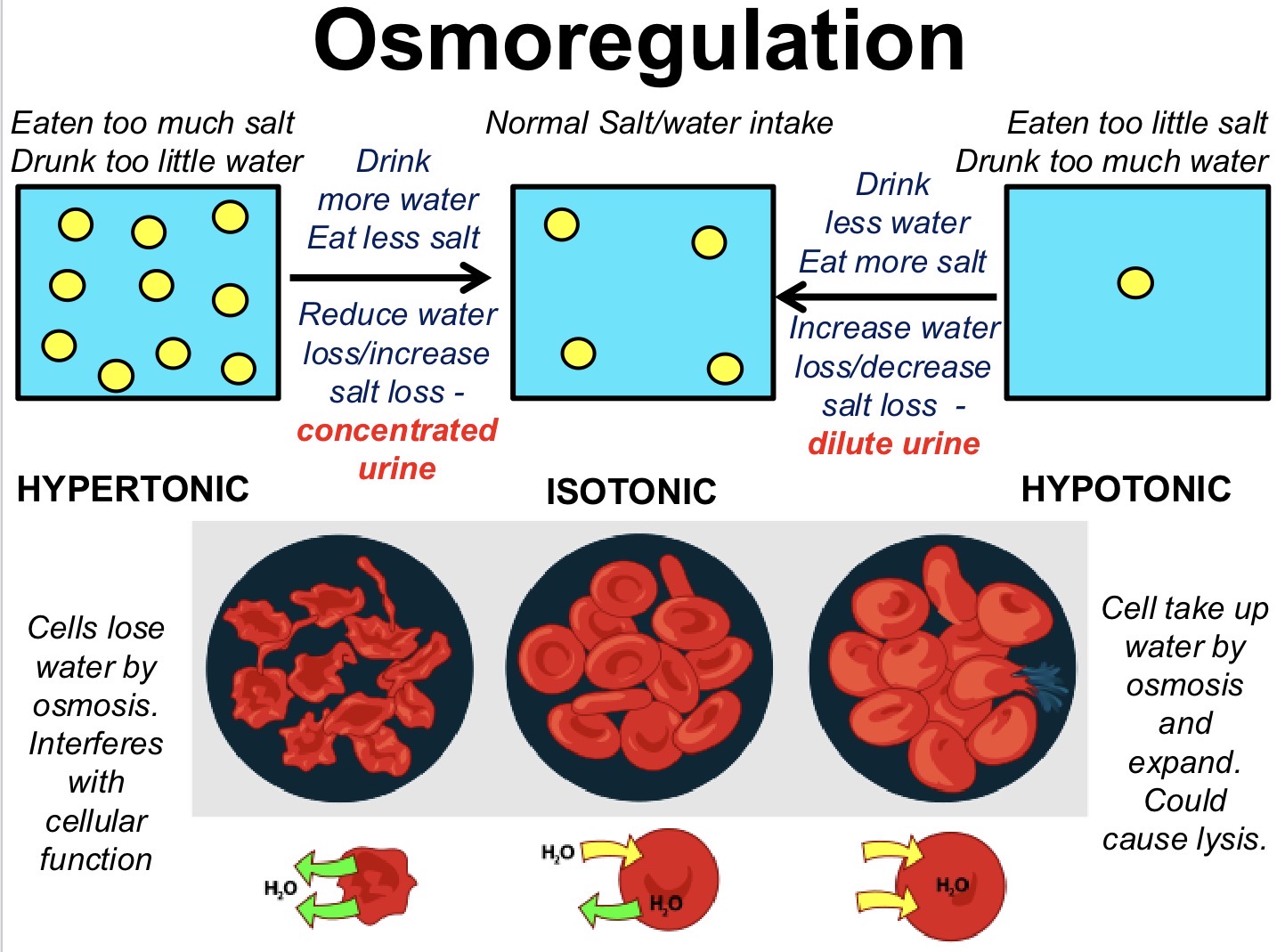
what is osmolarity measured by
mOsmoles/L
state and explain the 3 types of tonic solutions
what can we do to bring it back to normal level
what are the 5 parts of a nephron
what do they each absorb (in the absence of signal)
PCT, thin descending limb, thick ascending limb, DCT, collecting duct
PCT - all aa, sugar, HCO3-, ions, water (isosmotic fluid reabsorption)
TDL - water
TAL - actively reabsorbs NaCl
DCT + collecting duct - NaCl
osmoreceptors:
when plasma is hypertonic, what channels open (S-IIC)
what happens to the cell polarity and what firing is increased
where are signals sent to in the brain
what 2 things are increased as a result of hypertonic plasma
stretch-inhibited ion channels when the cell shrinks
cell depolarises, ^^AP firing
hypothalamus receives signals
increased thirst
increased ADH secretion from posterior pituitary (excrete less urine)
water permeability:
where is water impermeable, what type of junction
where is water permeable, what type of junction
when does transcellular water absorption happen
tight junction - found everywhere after PCT
leaky junctions - found in PCT, paracellular water movement (water is also permeable in the thin descending limb and collecting duct (variable))
with aquaporins (need both luminal and basolateral channels)
what is countercurrent multiplication
what is high osmolarity and what is its trend going down to the medulla
what does high osmolarity mean for collecting ducts
high NaCl conc from the ascending limb in the medulla so water can leave the descending limb
how concentrated solution is with solute, increased down to medulla
water is drawn out from collecting ducts as conc urine leaves by osmosis
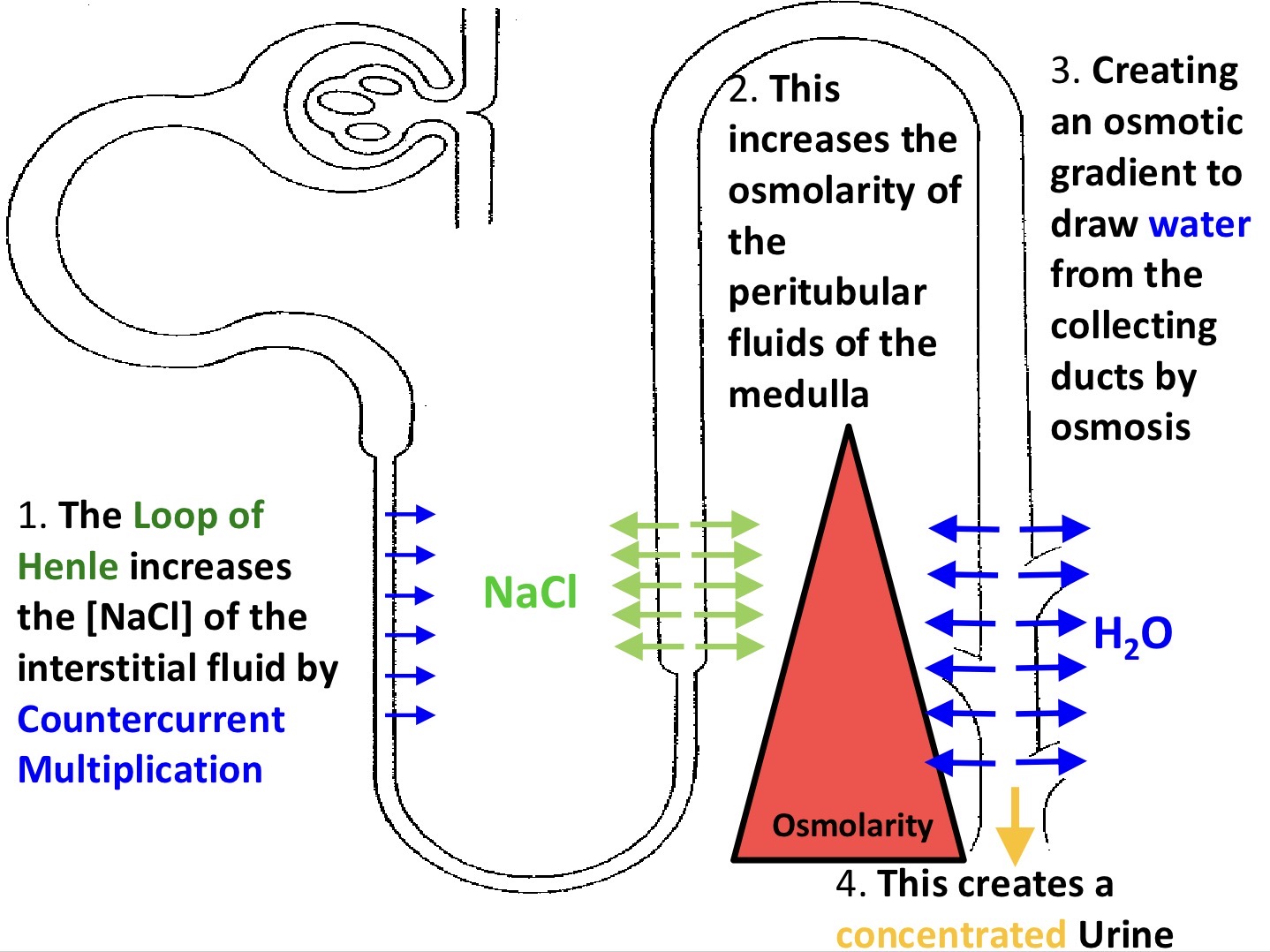
countercurrent multiplication
characteristic of PCT fluid
what does the TDL have to make it permeable to water
what does the TAL do with NaCl, effect on interstitial fluid
what happens to NaCl conc of tubular fluid
what happens to NaCl in ascending limb
characteristic of tubular fluid leaving loop of henle
isosmotic to plasma
expresses aquaporin 1
actively pumps out NaCl to mame interstitial fluid hyperosmotic to plasma (osmotic gradient created for TDL)
increased salt conc in tube - preconcentrated tubular fluid
so it gets actively transported out - water and salt gets semi balanced
hyposmotic to blood plasma, more NaCl reabsorbed compared to water back to blood
without ADH, what happens to collecting duct and urine concentration
how does ADH work
effect on urine and blood osmolarity
collecting duct is impermeable to water, dilute urine
binds to receptor on CD, causes exocytosis of vesicles containing aquaporin 2 on tubule lumen
create conc urine, water reabsorbed into blood - lower blood osmolarity
diabetes insipidus DI:
what is it
2 things it can lead to if untreated
what is polyuria and polydipsia
2 causes
Caused by lack of antidiuretic hormone (ADH/vasopressin) or kidney resistance to it, affecting water retention - not related to blood sugar (produce very dilute urine and very thirsty)
potentially leading to hypotension (low BP), hypernatraemia (high blood Na+) if untreated
PU - excessive urination, PD - excessive thirst
A failure of ADH secretion or A failure of the collecting duct to respond to ADH