SB Practice Exam 2
1/158
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
159 Terms
A patient rehabilitating from a stroke involving the right hemisphere exhibits figure-ground discrimination dysfunction. Which task would likely be the MOST difficult for the patient based on the reported perceptual deficit?
1. Have the patient find his way in the hospital using written directions or a map
2. Have the patient attempt to identify a familiar object when it is placed on its side
3. Have the patient pick forks out of a drawer of disorganized silverware
4. Have the patient point to left and right body parts after receiving verbal instructions
Perception is the mechanism by which the brain interprets sensory information received from the environment. Perception is commonly altered in patients sustaining a stroke involving the right hemisphere.
1. Topographical disorientation involves difficulty comprehending the relationship of one location to another. Having a patient navigate in the hospital using written directions or a map would be an appropriate method to screen for this condition.
2. Form-constancy dysfunction involves difficulty attending to subtle variations or changes in form such as a size variation of the same object. Having a patient attempt to identify a familiar object when it is placed on its side would be an appropriate method to screen for this condition.
3. Figure-ground discrimination dysfunction involves difficulty distinguishing the foreground from the background in a complex visual array. Having the patient pick forks out of a drawer of disorganized silverware would be an appropriate method to screen for this condition.
4. Right-left discrimination dysfunction involves difficulty understanding and using the concepts of right and left. Having the patient point to left and right body parts after receiving verbal instruction would be an appropriate method to screen for this condition.
A physical therapist instructs a patient in a traditional bench press exercise using free weights. Which modification would be the MOST beneficial to limit the amount of stress placed on the anterior capsule of the shoulder?
1. Grasp the bar with a supinated grip with the hands slightly wider than shoulder width apart
2. Ensure that the elbows are fully extended at the conclusion of the upward movement
3. Ensure that the bar does not contact the chest during the downward movement
4. Attempt to slightly raise the head off of the bench during the upward movement
The bench press is a commonly used exercise that functions to strengthen the pectoralis major, anterior deltoid, serratus anterior, pectoralis minor, and triceps brachii. Physical therapists must be able to adapt specific exercises to the unique needs of each patient.
1. The bench press should be performed with a pronated grip rather than a supinated grip. The patient should grasp the bar with the hands slightly wider than shoulder width apart.
2. The elbows are typically fully extended at the conclusion of the upward movement of the bench press. As a result, this action does not serve to limit the amount of stress on the anterior capsule of the shoulder.
3. In a typical bench press the patient is instructed to lower the bar until it touches the chest at approximately nipple level. As a result, ensuring that the bar does not contact the chest serves to reduce the amount of stress on the anterior capsule of the shoulder. Therapists should attempt to avoid instructing patients with known or suspected shoulder pathology in exercises that place the arms and hands behind the plane of the shoulder.
4. The head should remain in contact with the bench at all times during a bench press. Attempting to lift the head is a common substitution pattern that should be avoided since it has the potential to jeopardize patient safety.
A physical therapist works in a hospital with a patient who has methicillin-resistant staphylococcus aureus (MRSA). When treating the patient, which infection control procedures would be the MOST appropriate?
1. Work in the therapy gym, therapist wears gown and gloves
2. Work in the therapy gym, therapist wears gown, gloves, and mask
3. Work in the patient’s room, therapist wears gown and gloves
4. Work in the patient’s room, therapist wears gown, gloves, and mask
Transmission-based precautions are designed to protect health care workers from patients with highly transmissible pathogens that can be spread by direct contact, droplets of moisture or airborne particles. Contact precautions are required when working with a patient with MRSA.
1. When treating a patient with contact precautions, it is necessary to minimize patient transport outside of their room. As a result, it would be more appropriate to treat this patient in their room than in the therapy gym.
2. When treating a patient with contact precautions, it is necessary to minimize patient transport outside of their room. This is also true when treating patients with droplet or airborne precautions.
3. When treating a patient with contact precautions, it is more appropriate to treat the patient in their room than in the therapy gym. To prevent the spread of MRSA, the therapist should don a gown and gloves upon entering the room.
4. While it is appropriate for the therapist to wear a gown and gloves, it would not be necessary to wear a mask when treating a patient with contact precautions. Wearing a mask is only necessary when treating a patient with droplet or airborne precautions.
A physical therapist assesses a patient’s lumbar spine range of motion. The therapist determines that active extension exacerbates the patient’s symptoms and flexion tends to relieve the symptoms. Which medical condition is MOST consistent with the patient’s clinical presentation?
1. Facet joint arthropathy
2. Vascular claudication
3. Piriformis syndrome
4. Disk herniation
Physical therapists can gather valuable information on exacerbating and relieving symptoms through a range of motion screening. The obtained information can assist the therapist to gain a clearer clinical picture of the mechanical and non-mechanical factors contributing to the patient’s current condition.
1. Facet joints (i.e., zygapophyseal joints) are formed by the right and left superior articular facets of one vertebra and the right and left inferior articular facets of an adjacent superior vertebra. Facet joint arthropathy may cause stiffness in the back and increased pain with movement, however, the pain is typically localized to the affected structures and would not radiate down the leg. Flexion tends to result in facet gapping resulting in diminished symptoms.
2. Vascular claudication produces a cramping type pain in the buttock, thighs or calves caused by impaired blood flow often associated with atherosclerosis. Patients with vascular claudication typically experience increased symptoms with activity regardless of the direction of movement and diminished symptoms with rest.
3. Piriformis syndrome refers to a persistent, severe radiating low back and buttock pain spanning from the sacrum to the hip and posterior thigh. The primary symptom is sciatic paresthesia due to nerve entrapment as the sciatic nerve passes under or through the piriformis muscle. Patients with piriformis syndrome often experience increased symptoms with activities that compress the sciatic nerve such as sitting for long periods of time or climbing stairs.
4. A disk herniation results from a tear in the annulus fibrosis of an intervertebral disk allowing the nucleus pulposus to bulge out beyond the damaged outer rings. This often compresses spinal nerve roots and causes radiating symptoms down the leg. Patients with a disk herniation often experience diminished symptoms with extension of the spine since the motion results in the migration of the nucleus pulposus toward the center of the disk.
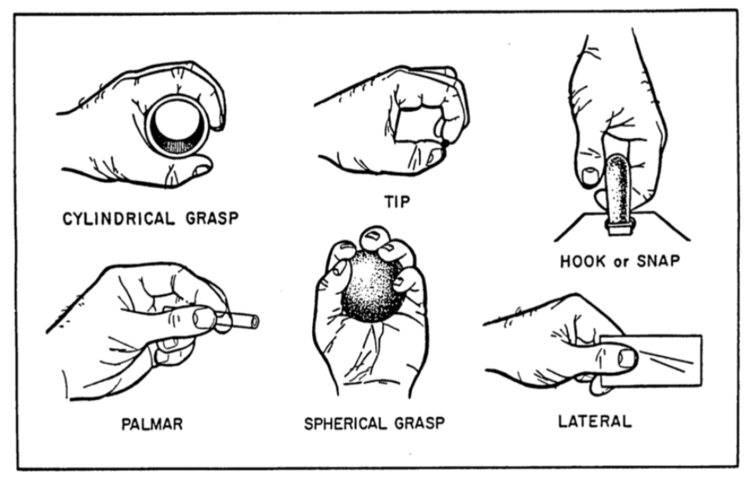
A patient is unable to perform thumb opposition. Which type of grasp would NOT be affected by this deficit?
1. Cylindrical
2. Pad-to-pad prehension
3. Hook grasp
4. Spherical grasp
Opposition involves rotation of the carpometacarpal joint of the thumb in order to align the thumb pad with one or all of the digit pads. Opposition of the thumb is found in most grasp patterns and allows for execution of a variety of activities such as turning a door knob.
1. Cylindrical grasp is used when holding a cylindrically shaped object such as a can of soda or soup. This grasp involves thumb opposition, finger adduction and flexion.
2. Pad-to-pad prehension is used when holding onto a coin. This grasp involves thumb opposition and slight flexion of the thumb joints. It also involves finger flexion at the metacarpophalangeal and proximal interphalangeal joints and either flexion or extension of the distal interphalangeal joints of the fingers.
3. Hook grasp is used when holding onto a briefcase handle or purse. This grasp involves the metacarpophalangeal joints in neutral, with finger flexion at both the proximal and distal interphalangeal joints. The thumb is positioned in extension with this grasp and would not be affected by the inability to perform opposition.
4. Spherical grasp is used when holding onto a round object such as a softball or an apple. This grasp involves thumb opposition and finger flexion and abduction.
VIDEO: Shows patient in supine performing shoulder flexion
After observing the patient perform the action depicted in the video, the physical therapist concludes that the patient has adaptive shortening of the latissimus dorsi. Which observation during testing would BEST support the hypothesis?
1. Increased lumbar lordosis
2. Decreased lumbar lordosis
3. Increased thoracic kyphosis
4. Decreased thoracic kyphosis
The latissimus dorsi originates on the external lip of the iliac crest and inserts on the intertubercular groove of the humerus. Shortening of the latissimus dorsi often results in a limitation of shoulder flexion or abduction. The muscle acts to adduct, extend, and medially rotate the arm. The muscle is innervated by the thoracodorsal nerve.
1. Lordosis refers to an excessive curvature of the spine in an anterior direction, usually identified in the cervical or lumbar spine. Under normal circumstances, a patient should be able to perform complete shoulder flexion without an increase in lumbar lordosis, however, with adaptive shortening of the latissimus dorsi the patient may not have full shoulder flexion and therefore attempts to compensate for the limitation by increasing the amount of lumbar lordosis. Increased lumbar lordosis assists the patient to achieve additional shoulder flexion range due to the insertion of the latissimus dorsi on the external lip of the iliac crest.
2. Decreasing the amount of lumbar lordosis would result in additional shortening of the latissimus dorsi and as a result would exaggerate any observed limitation in shoulder flexion.
3. Kyphosis refers to an excessive curvature of the spine in a posterior direction, usually identified in the thoracic spine. The relative extent of thoracic kyphosis present would not significantly influence the amount of shoulder flexion present in the described testing procedure due to the origin and insertion of the latissimus dorsi.
4. The relative extent of thoracic kyphosis present would not significantly influence the amount of shoulder flexion present in the described testing procedure due to the origin and insertion of the latissimus dorsi.
A physical therapist treating a patient on hemodialysis attempts to measure the intensity of an exercise activity. What is the MOST appropriate method to utilize?
1. Heart rate
2. Blood pressure
3. Respiratory rate
4. Rating of perceived exertion
Hemodialysis is a treatment process for patients with advanced and permanent kidney failure. Kidney failure creates excess toxic waste, increased blood pressure, retention of excess body fluids, and a decrease in red blood cell production. Hemodialysis removes the blood from the body along with waste, excess sodium, and fluids. The process cleanses the blood and returns it to the body. A patient requires this process on average three times per week.
1. The measure of heart rate is highly variable when a patient is receiving hemodialysis secondary to fluid shifts and vascular adaptations to fluid loss during treatment. Autonomic dysfunction can limit heart rate significantly and therefore intensity should be measured using rating of perceived exertion (RPE).
2. Blood pressure will vary in patients on hemodialysis. Hypertension may exist prior to dialysis secondary to fluid retention and hypotension can exist immediately following hemodialysis. Blood pressure, however, is not a direct measure of exercise intensity.
3. Respiratory rate should be monitored to ensure that the patient is not hyperventilating or holding their breath during exercise, however, respiratory rate is not a measure of exercise intensity.
4. RPE is the most appropriate method to measure the intensity of exercise with a patient receiving dialysis. Exercise intensity can vary significantly, however, the patient should work towards approximately 20-30 minutes of low-level exercise using RPE to monitor the intensity of the exercise performed.
During a treatment session, a physical therapist notices that an eight-year-old patient is demonstrating the initial signs of a seizure while lying on a treatment table. What is the MOST appropriate action for the therapist to take during the seizure?
1. Restrain the patient’s movements to decrease the chance of injury
2. Administer cardiopulmonary resuscitation
3. Keep the airway open by placing an object between the patient’s teeth
4. Monitor the patient’s respiratory rate
Physical therapists should be knowledgeable of the appropriate measures to take when a patient is having a seizure to ensure their safety. The objectives are to protect the patient from injury and to protect the patient’s modesty.
1. It is desirable to have the patient in a safe location and position. However, restraining the patient’s movements could actually lead to further injury to the patient and/or therapist.
2. Unless the patient experiences cardiopulmonary arrest, cardiopulmonary resuscitation (CPR) is rarely needed after a seizure. After the seizure has stopped, the therapist should monitor the patient’s pulse and breathing. If the pulse or breathing does not return, the therapist should begin CPR.
3. The therapist should ensure that the patient’s airway remains patent. However, the therapist should not place any objects in the patient’s mouth since the objects may create a choking hazard.
4. It is important for the therapist to monitor the patient’s respiratory rate. If the patient stops breathing for an excessive amount of time following the seizure, the therapist should begin CPR.
A patient is referred to physical therapy after being diagnosed with acute unilateral vestibular hypofunction. Which assessment result would the physical therapist MOST likely use to confirm the diagnosis?
1. Abnormal vestibulo-ocular reflex
2. Abnormal result with an audiogram
3. Magnetic resonance imaging showing recent transient ischemic attack of the brainstem
4. Presence of vertigo with the Dix-Hallpike maneuver
Acute unilateral vestibular hypofunction is the second most common cause of vertigo. Viral infection is a common cause of this condition, usually affecting the vestibular nerve unilaterally. The clinical manifestations of this condition include sudden onset of rotatory vertigo, spontaneous horizontal nystagmus, nausea, and vomiting.
1. The vestibulo-ocular reflex is the connection between the vestibular and visual systems which allows for conjugate movement of the eyes as a result of head movement. When one side of the system is damaged, as in the presence of unilateral vestibular hypofunction, this reflex would be abnormal. When the reflex is abnormal, there is a loss of gaze stabilization with head movement.
2. An audiogram (i.e., test of hearing) typically confirms the presence of low-frequency hearing loss. Hearing loss is not a symptom associated with unilateral vestibular hypofunction, however, it is often associated with a diagnosis of Meniere’s disease.
3. Magnetic resonance imaging can be used when a central cause for vertigo, such as a brainstem lesion, is suspected. Unilateral vestibular hypofunction would be considered a peripheral cause of vertigo.
4. The Dix-Hallpike maneuver is an assessment procedure which uses specific head positions and movements to elicit symptoms of vertigo. This procedure is used to confirm the presence of benign paroxysmal positional vertigo.
VIDEO: Shows patient in sidelying, PT is moving the patients arm (bent at 90) into external rotation
A physical therapist moves a patient’s shoulder as depicted in the video. Which muscle would be placed on stretch with this movement?
1. Subscapularis
2. Posterior deltoid
3. Infraspinatus
4. Teres minor
Passive stretching activities are commonly employed in a rehabilitation program to improve range of motion. A muscle should be stretched in the opposite direction as the muscle’s action in order to increase muscle length.
1. The subscapularis originates on the subscapular fossa of the scapula and inserts on the lesser tubercle of the humerus. The muscle is innervated by the subscapular nerve. The subscapularis acts primarily to medially rotate the shoulder. As a result, passive lateral rotation of the humerus would stretch the subscapularis.
2. The posterior deltoid originates on the inferior lip of the posterior border of the spine of the scapula and inserts on the deltoid tuberosity of the humerus. The muscle is innervated by the axillary nerve. The posterior deltoid acts to extend and laterally rotate the shoulder. As a result, passive lateral rotation of the humerus would not stretch the posterior deltoid.
3. The infraspinatus originates on the medial two-thirds of the infraspinous fossa of the scapula and inserts on the greater tubercle of the humerus and shoulder joint capsule. The muscle is innervated by the suprascapular nerve. The infraspinatus acts to laterally rotate the shoulder joint and stabilize the head of the humerus in the glenoid cavity. As a result, passive lateral rotation of the humerus would not stretch the infraspinatus.
4. The teres minor originates on the upper two-thirds of the dorsal surface of the lateral border of the scapula and inserts on the greater tubercle of the humerus. The muscle is innervated by the axillary nerve. The teres minor acts primarily to laterally rotate the shoulder. As a result, passive lateral rotation of the humerus would not stretch the teres minor.
A physical therapist uses a pan splint as an intervention to diminish spasticity in the wrist flexors. Which position of the wrist would be MOST desirable based on the established therapeutic goal?
1. Wrist in extension to decrease activity of the agonist
2. Wrist in extension to increase activity of the agonist
3. Wrist in flexion to decrease activity of the agonist
4. Wrist in flexion to increase activity of the agonist
A pan splint is used to stabilize the hand in a functional position usually involving slight extension of the wrist. Spasticity refers to an abnormal increase in muscle tone. The condition may be associated with sustained muscle contractions, involuntary muscle spasms, and exaggerated deep tendon reflexes that make movement difficult or uncontrollable. An agonist refers to a contracting muscle that is resisted or counteracted by another muscle termed the antagonist.
1. Positioning the wrist in extension would provide a sustained stretch to the wrist flexors. The position would result in activation of the Golgi tendon organs that serve to reduce spasticity in the agonist and facilitate activity in the antagonist.
2. Positioning the wrist in extension would provide a sustained stretch of the wrist flexors, however, the position would not increase activity of the agonist.
3. Positioning the wrist in flexion would likely increase the amount of spasticity in the wrist flexors. The purpose of the described intervention was to diminish spasticity in the wrist flexors.
4. Positioning the wrist in flexion would likely exacerbate the amount of spasticity in the wrist flexors. The purpose of the described intervention was to diminish spasticity in the wrist flexors.
While greeting a patient in a waiting room, a physical therapist observes that another patient appears anxious, diaphoretic, and dyspneic. When questioned, the patient reports a recent onset of substernal chest pain and nausea that they attribute to severe indigestion. Which medical condition is MOST consistent with the patient's clinical presentation?
1. Myocardial infarction
2. Gastroesophageal reflux disease
3. Spontaneous pneumothorax
4. Pulmonary embolism
A physical therapist must be aware of signs and symptoms associated with emergent conditions. It is the responsibility of the therapist to ensure patient safety, but to also respond to emergent needs of others within the workplace including co-workers and visitors.
1. Crushing chest pain or tightness, which may radiate and is present for greater than 30 minutes, is typically the hallmark symptom of a myocardial infarction (MI). Other signs and symptoms may include anxiety, dyspnea, syncope, nausea, arrhythmia, diaphoresis, and an impending sense of doom.
2. Complaints of dull chest pain or tightness, which may be accompanied by a burning sensation (i.e., heartburn), are often associated with gastroesophageal reflux disease (GERD). GERD, however, does not typically cause diaphoresis or dyspnea.
3. Chest pain complaints associated with pneumothorax are typically described as “sharp” or “sudden,” are somewhat localized, and do not present substernally. Dyspnea complaints may be mild to severe depending on the size of the pneumothorax.
4. A pulmonary embolism (PE) of significant size may simulate a MI with common symptoms including chest pain, anxiety, dyspnea, and a sense of doom. A patient with PE would be unlikely to present with vagal related symptoms (e.g., nausea, diaphoresis), however, would commonly exhibit cyanosis.
A patient recently diagnosed with multiple myeloma is treated in physical therapy. Which activities would be MOST important to include in the patient’s plan of care?
1. Decreasing fatigue and fall prevention
2. Decreasing edema and mobility training
3. Decreasing contractures and strengthening
4. Decreasing pain and increasing range of motion
Physical therapists treat patients with multiple myeloma in order to decrease the effects of the cancer. Fatigue is a hallmark of the disease process along with skeletal muscle wasting and risk for pathologic fractures. Therapists play an important role throughout the progression of the disease in order to minimize effects from the cancer and maintain function and strength.
1. The primary symptoms of multiple myeloma include fatigue, bone pain, and muscular weakness. Low-level exercise and fall prevention should be considered the primary focus of physical therapy in order to improve the patient’s overall activity level and avoid pathologic fractures which can be life threatening.
2. Edema is not typically a clinical manifestation of multiple myeloma. Mobility training is appropriate once the patient demonstrates adequate endurance to low-level activity.
3. Contractures are not typically a clinical manifestation of multiple myeloma. Strengthening is appropriate in the form of short duration low-level exercise and can assist with decreasing overall fatigue.
4. Bone pain is a primary symptom of multiple myeloma and can vary in intensity from mild to severe. Pain can decrease with medical management of the cancer, however, subsequent bone destruction increases the risk of pathologic fracture and pain. Range of motion limitation is not typically a clinical manifestation of multiple myeloma.
A physical therapist reviews the results of a patient’s electromyography test. The report notes the presence of brief contractions of single muscle fibers at rest that are not visible through the skin. This description MOST likely characterizes which abnormal potential?
1. Fibrillation potentials
2. Fasciculations
3. Insertional activity
4. Polyphasic potentials
Electromyography (EMG) is the recording of electrical activity of a muscle and its motor unit. The motor unit action potential will be abnormal when there is damage to the nerve or muscle. Types of abnormal potentials include fibrillation potentials, positive sharp waves, fasciculations, and polyphasic potentials.
1. Fibrillation potentials are abnormal spontaneous potentials that occur when the muscle is at rest. They are believed to arise from the spontaneous depolarization of a single muscle fiber. They are not visible through the skin. Fibrillation potentials are often indicative of lower motor neuron disorders and are less commonly seen in myopathic diseases.
2. Fasciculations are spontaneous potentials that occur when the muscle is at rest and are not definitively considered abnormal since they are also found in normal individuals. They are often seen with anterior horn cell degeneration, chronic peripheral nerve lesions, nerve root compression, and muscle spasms or cramps. They are visible through the skin, commonly seen as a small muscular twitch.
3. Insertional activity describes the spontaneous potentials seen on EMG when the needle electrode is inserted into the muscle. These spontaneous potentials are considered normal.
4. Polyphasic potentials are abnormal potentials that are seen during voluntary contraction of a muscle. They are characterized by motor unit potentials that have five or more phases (one to four phases is considered normal). These abnormal potentials are indicative of myopathies, peripheral nerve involvement, and nerve root compression.
A physical therapist assesses a patient’s home to ensure it is accessible. When assessing the stairs, which characteristic would make stair navigation the MOST difficult?
1. Handrails that extend 12 inches past the stairs
2. Steps that are 8.5 inches high
3. Steps that are 12 inches deep
4. Stairs that are carpeted
Examination of the home environment is often an important part of a patient’s discharge process. Environmental intervention strategies may include adaptive or assistive devices (e.g., grab bars, eating utensils), safety devices (e.g., lighting, sensing devices), structural alterations (e.g., widening doors, installing ramps), modification or altered location of objects (e.g., door locks, moving furniture), and task modification (e.g., visual or auditory cueing, energy conservation).
1. All indoor stairwells should have handrails. The handrails should extend a minimum of 12 inches past the top and bottom of the stairs for added safety.
2. Ideally, steps should not be greater than 7 inches in height. Steps that are greater than 7 inches high make stair navigation increasingly difficult for many people with disabilities.
3. Steps should have a minimum depth of 11 inches to allow for adequate foot placement when navigating stairs.
4. Steps should have a nonslip surface to improve traction. Carpeting or the use of abrasive strips on a slippery surface can help to improve traction.
A patient with HIV is being treated in physical therapy for general deconditioning. What is the associated condition MOST likely to increase the risk for opportunistic infection?
1. Neutropenia
2. Anemia
3. Polycythemia
4. Thrombocytopenia
It is important for a physical therapist to be aware of blood values and specifically white blood cell count prior to treatment. Immunocompromised patients are extremely susceptible to opportunistic infections and other medical complications.
1. Neutrophils are a classification of leukocytes (white blood cells) that digest various foreign materials and are referred to as the first line of hematologic defense against invading pathogens. Neutropenia refers to a neutrophil count below normal laboratory reference values. This condition places a patient at risk for developing a serious infection. The longer the neutropenia exists, the more likely the patient is to develop a significant infection.
2. Anemia refers to hemoglobin and hematocrit levels below normal gender specific laboratory reference values. Symptoms may include dyspnea, heart palpitations, and dizziness. Patients who are anemic are advised to change positions slowly, rest frequently during activity, and allow themselves full nights of sleep. This condition does not promote opportunistic infection.
3. Polycythemia is defined as an increase in the number of red blood cells in the body. This condition results in increased blood viscosity and increased blood volume which results in elevated blood pressure measurements. This thickening of the blood can also increase the risk of a stroke or a heart attack. This condition does not promote opportunistic infection.
4. Thrombocytopenia refers to platelet levels below normal reference laboratory values. Patients with thrombocytopenia will bleed and bruise very easily. Precautions include avoiding contact sports, working with or around sharp objects, and tight fitting clothing or accessories. This condition does not promote opportunistic infection.
A physical therapist works on positioning with a 78-year-old female in a skilled nursing facility. Which physiologic change would contribute to an increased incidence of skin breakdown in this population?
1. Increased sensory perception
2. Decreased pain threshold
3. Increased elasticity of the dermis
4. Decreased subcutaneous adipose tissue
Age-related changes begin to occur in a geriatric population that result in a decrease in physical and cognitive functioning. Aging affects all physiologic processes within the body including the integumentary system.
1. As individuals reach an advanced age they experience decreased sensory perception. This results in a larger strength of stimulus being required to be perceived by the individual. This change also impacts awareness of pain, temperature, and body position. As a result, this population is more susceptible to pressure injuries.
2. As individuals reach an advanced age they typically experience an increased pain threshold making it more difficult to detect potential threats to the skin. This lack of sensitivity makes this population more susceptible to pressure injuries.
3. As individuals reach an advanced age they experience a decrease in thickness of the dermal layer and a loss of elasticity causing the skin to wrinkle and sag. This physiologic change makes this population more susceptible to pressure injuries.
4. As individuals reach an advanced age they experience a gradual decrease in subcutaneous adipose tissue. Decreased tissue thickness makes this population more susceptible to pressure injuries.
A physical therapist is treating a patient using neuromuscular electrical stimulation for muscle reeducation. The therapist would like to increase the pulse characteristic called amplitude. Which control should be manipulated on the stimulator?
1. Frequency
2. Ramp time
3. Intensity
4. Phase duration
A waveform is a graphic representation of the shape, direction, amplitude, duration, and pulse frequency of the electrical current being produced. Therapists should be familiar with the various characteristics of a waveform to effectively determine which parameters should be used when administering electrical stimulation.
1. Frequency determines the number of pulses delivered through each channel per second. Frequency controls are often labeled as rate and are expressed in pulses per second or Hertz.
2. A ramp allows current amplitude to gradually increase to a preset maximum and then gradually decrease. Ramp time refers to the amount of time it takes to reach the preset maximum. Ramping is commonly used to make the onset of stimulation more comfortable when performing muscle strengthening.
3. The amplitude of each pulse reflects the magnitude of the current. Amplitude is synonymous with the terms intensity or voltage.
4. The phase duration is the elapsed time between the beginning and end of one phase. With monophasic current it is the time from the initiation of the phase to its end. For biphasic current the pulse duration is determined by the combined phase durations.
A physical therapist uses a measuring device to determine the surface temperature of a wound and the surrounding area. Which variable would MOST heavily influence the obtained temperature reading?
1. Location
2. Sensation
3. Vascularity
4. Surface area
Temperature is often used to gather important information on a disease process or injury. Specifically, temperature can be used as an objective measure of tissue damage and inflammation. There are a variety of instruments that can be used to obtain an accurate recording of surface temperature including thermistors and thermocouples.
1. The location of a wound can influence the obtained temperature, however, the magnitude of the change based on location would be relatively small.
2. Sensation is related to the ability to perceive a stimulus and would not be related to the actual temperature of a wound and the surrounding area. Patients with sensory deficits are at a dramatically increased risk of experiencing a wound.
3. The temperature of a wound is heavily influenced by the amount of blood (i.e., vascularity) circulating through the tissue. Localized erythema or redness is often associated with an increase in temperature, while a reduced temperature is often reflective of diminished vascularity.
4. Surface area refers to the extent or size of an area impacted by a wound. The size of the area affected can influence temperature, however, the magnitude of the change based on the size of the surface area would be relatively small.
A physical therapist administers grade III and IV joint mobilizations to a patient with a capsular restriction of the glenohumeral joint. After returning to therapy later in the week the patient indicates that they experienced mild discomfort in the shoulder the evening after the last session, however, the discomfort had resolved by the next morning. What is the MOST appropriate action?
1. Administer active stretching activities
2. Instruct the patient in passive stretching activities
3. Continue with grade III and IV mobilizations
4. Contact the referring physician
Physical therapists must select the appropriate rate, rhythm, and intensity of mobilization techniques. Graded oscillation techniques using grades III and IV are commonly used to stretch the joint capsule. Physical therapists should carefully assess how patients tolerate treatment and make modifications to the plan of care as needed.
1. Administering active stretching activities would be an acceptable intervention, however, would not likely be as effective as mobilization activities given the presence of a capsular restriction. The absence of current pain or any additional data suggesting the patient did not tolerate the treatment makes it reasonable to continue with mobilization.
2. Instructing the patient in passive stretching activities would be an acceptable intervention, however, would not likely be as effective as mobilization activities given the presence of a capsular restriction. The absence of current pain or any additional data suggesting the patient did not tolerate the treatment makes it reasonable to continue with mobilization.
3. It is not unusual for patients to experience some level of discomfort or pain following grade III and IV mobilizations. The fact that the pain resolved the following day warrants continuing with mobilization.
4. The absence of a “red flag” or a change in medical status makes it unnecessary to contact the referring physician.
A physical therapist is treating a patient who recently received an Unna boot. What is the MOST likely rationale for this intervention?
1. Provide compression and promote healing
2. Provide protection and promote stability
3. Provide absorption and promote oxygen exchange
4. Provide stretch and promote range of motion
An Unna boot is an example of a semirigid compression bandage made of zinc oxide impregnated gauze. The boot is capable of providing a sustained compression force of 35-40 mm Hg.
1. An Unna boot is commonly used to treat venous ulcers that present with edema. The Unna boot consists of impregnated gauze strips that are applied wet and then dry into a non-elastic and non-expandable porous mold. The zinc oxide is indicated since it is used with healing of ulcerations and open wounds.
2. A plaster of Paris or fiberglass cast is an example of a device that is applied to provide protection and promote stability of a body part.
3. Transparent film is an example of a dressing that can provide absorption for minimal amounts of drainage and promote oxygen exchange. Transparent film is highly elastic, conforms to a variety of body contours, and allows for visual inspection of the wound since it is transparent.
4. A dynamic splint is an example of a device that applies a low-load constant stretch in order to improve range of motion or the position of a joint.
A physical therapist working with a three-year-old child diagnosed with an x-linked inherited disease notes that the patient exhibits toe walking and pseudohypertrophy of the gastrocnemius muscle. The mother indicates that the child has a tendency to fall frequently. What medical condition is MOST consistent with the described clinical presentation?
1. Down syndrome
2. Duchenne muscular dystrophy
3. Spinal muscular atrophy
4. Spina bifida
Neuromuscular diseases refer to disorders which affect any part of the motor unit from the anterior horn cell to the muscle itself. These disorders are often characterized by which part of the motor unit is affected (e.g., anterior horn cell, peripheral nerve, neuromuscular junction, muscle). Weakness is a symptom common to all neuromuscular diseases.
1. Down syndrome is a genetic disorder caused by an extra copy of the 21st chromosome. This disorder affects multiple systems of the body, but some of the more common symptoms include delays in physical growth, characteristic facial feature abnormalities, and intellectual disability. Though hypotonia and weakness are symptoms commonly seen with Down syndrome, toe walking and pseudohypertrophy of the calf muscle are not associated with this disorder.
2. Duchenne muscular dystrophy is an x-linked inherited disorder which is characterized by muscle degeneration. The onset of the disease typically occurs between two and five years of age. Early symptoms include falling, difficulty getting up from the floor, toe walking, clumsiness, and an increase in the size of several muscle groups (i.e., pseudohypertrophy).
3. Spinal muscular atrophy (SMA) is an autosomal recessive disorder that results from the loss of anterior horn cells. This disorder can be classified into three different types based on the child’s functional abilities. Symptoms vary widely depending on the type of SMA, but all types are characterized by weakness and mobility impairments. Toe walking and pseudohypertrophy of the calf muscle are not associated with this disorder.
4. Spina bifida is a neural tube birth defect that results in neuromuscular impairments. This condition is characterized by bladder/bowel issues, orthopedic abnormalities (e.g., clubfoot, hip dislocation), hydrocephalus, and leg weakness or paralysis. Toe walking and pseudohypertrophy of the calf muscle are not associated with this condition.
A physical therapist works with a patient in an intensive care unit. During the session the physical therapist hears the low pressure alarm of a mechanical ventilator. Which finding is MOST often associated with activation of the alarm?
1. Change in patient position
2. Pneumothorax
3. Leak in the ventilator circuit
4. Cough
A mechanical ventilator is a device that makes it easier for patients to breathe until they are capable of breathing completely on their own. The device is most commonly used to deliver oxygen, eliminate carbon dioxide, and decrease the work of breathing. Physical therapists must be familiar with the various alarms used on mechanical ventilators to ensure patient safety.
1. A change in patient position would be more likely to cause the high pressure alarm to activate. When the high pressure alarm sounds it indicates that the ventilator has met resistance to deliver the tidal volume and requires more pressure to inflate the lungs.
2. A pneumothorax refers to an abnormal collection of air in the pleural cavity. Pressure from the pneumothorax impedes the lung’s ability to inflate and as a result is more likely to cause the high pressure alarm to activate.
3. The low pressure alarm of a mechanical ventilator is activated when the ventilator has no resistance to inflate the lung. This is most often associated with a patient being disconnected from the ventilator or a leak in the ventilator circuit.
4. Coughing increases intrathoracic pressure and is therefore more likely to cause the high pressure alarm to activate.

A physical therapist examines the foot of a patient diagnosed with plantar fasciitis by performing the Windlass test. What would be the expected response for this test given the patient’s diagnosis?
1. Pain elicited at the base of the great toe
2. Pain elicited at the medial calcaneal tubercle
3. Flattening of the medial longitudinal arch
4. Increased height of the medial longitudinal arch
The plantar fascia is a multilayered fibrous aponeurosis that originates on the medial calcaneal tubercle and splits into five bands that ultimately insert into the bases of the proximal phalanges of the toes.
1. The Windlass test can be used to determine the presence of plantar fasciitis. This test is performed by passively dorsiflexing the great toe with the patient in standing. If the patient has plantar fasciitis, they will likely experience pain at the base of the calcaneus, not at the base of the great toe.
2. A positive Windlass test is indicated by pain elicited at the medial calcaneal tubercle. The Windlass test attempts to mimic the changes experienced by the medial longitudinal arch during the stance phase of gait due to dorsiflexion of the great toe.
3. When the great toe is dorsiflexed, the plantar fascia is lengthened and tightens. As the plantar fascia tightens, the height of the medial longitudinal arch would actually increase, not decrease.
4. During dorsiflexion of the great toe, the plantar fascia winds around the metatarsal head and tightens. This tightening of the plantar fascia shortens the distance between the calcaneus and metatarsal heads (i.e., Windlass mechanism) which elevates the medial longitudinal arch and provides increased support to the foot. Although this phenomenon may be observed during the Windlass test, a positive test is specifically pain elicited at the medial calcaneal tubercle.
The results of a lymphoscintigraphy test reveal that a patient with secondary lymphedema has blockages in the lymph vessels leading to the right lymphatic duct. Given the location of the patient’s blockages, where would the therapist expect to observe swelling?
1. Right elbow
2. Right hip
3. Right abdomen
4. Right foot
Lymph is transported from initial lymph vessels to larger lymph collectors to even larger lymphatic trunks. The two main lymphatic trunks are the right lymphatic duct and the thoracic duct. These vessels empty lymph directly into the venous system via the subclavian veins.
1. The right lymphatic duct is responsible for collecting lymph from the right arm and right side of the head. If there are blockages in the vessels that lead to this duct, swelling may be observed in the right elbow.
2. Because the right hip is drained by lymph vessels that lead to the thoracic duct, swelling in this region would not be expected if the right lymphatic duct was affected.
3. Because the right side of the abdomen is drained by lymph vessels that lead to the thoracic duct, swelling in this region would not be expected if the right lymphatic duct was affected.
4. The thoracic duct collects lymph from all areas of the body except the right arm and right side of the head. Swelling in the right foot would most likely be caused by blockages of lymph vessels that lead to the thoracic duct, not the right lymphatic duct.
A 64-year-old female is referred to physical therapy following a left total hip arthroplasty. The physical therapist notes that the patient demonstrates weakness in the left gluteus medius. Which gait abnormality is MOST likely based on the presented information?
1. Ipsilateral hip hiking
2. Contralateral hip hiking
3. Ipsilateral hip drop
4. Contralateral hip drop
A patient with gluteus medius weakness may demonstrate difficulty with contralateral foot clearance during the midswing phase of gait and attempt to compensate with an excessive ipsilateral trunk lean. The deficit is typically more evident at slower speeds of gait since faster speeds reduce stance time and subsequently the duration of time the muscle has to act as a stabilizer.
1. Ipsilateral hip hiking is typically observed as a compensatory mechanism utilized to assist in clearing the toes during the swing phase of the gait cycle. Hip hiking may be associated with an ipsilateral foot drop or a significant leg length discrepancy.
2. Contralateral hip hiking is often utilized as a strengthening exercise for a weak gluteus medius muscle. A patient may begin the exercise in a gravity-eliminated supine position and progress to standing.
3. An ipsilateral hip drop is not typically associated with muscle weakness, however, may be observed in a patient with a significant leg length discrepancy. With respect to the shorter limb, the ipsilateral hip will typically drop during the stance phase as the contralateral hip hikes allowing that limb to clear the floor as it swings through.
4. During open chain activities the gluteus medius acts as a hip abductor. However, during the stance phase of gait (i.e., closed chain activity), the muscle acts to stabilize the pelvis and prevent contralateral hip drop.
A physical therapist makes footwear recommendations to a patient that include wearing shoes that are wider with a large toe box and a flat heel. Which medical condition would MOST warrant this type of recommendation?
1. Morton’s neuroma
2. Plantar fasciitis
3. Peroneal tenosynovitis
4. Tarsal tunnel syndrome
Footwear can be an important item to assess when treating patients with foot and ankle pathologies. Footwear modifications can redistribute forces, improve stability, relieve pain, and accommodate for deformities and areas of increased pressure.
1. Morton’s neuroma refers to an injury to nerves between the toes which results in thickening and pain. The nerves most commonly affected are located between the third and fourth toes. A common cause of Morton’s neuroma is shoes that are too tight in the forefoot. This problem is made worse with high heels. Shoes with a larger toe box and without a high heel can assist to reduce or potentially alleviate the patient’s symptoms.
2. Plantar fasciitis refers to inflammation of the plantar fascia at the proximal insertion on the medial tubercle of the calcaneus. Plantar fasciitis is often associated with an excessive amount of pronation or prolonged duration of pronation. Possible interventions include orthotics, arch support, heel cup, shock absorbing inserts, night splints, modalities, stretching, and strengthening exercises.
3. Peroneal tenosynovitis refers to inflammation of the peroneal tendons. The peroneus longus and brevis tendons are located posterior to the lateral malleolus and are the structures most commonly affected. This condition is typically associated with activities requiring repetitive ankle motion that result in overuse, trauma or recurrent ankle sprains. Possible interventions include activity management, orthotics, lateral heel wedge, modalities, range of motion, and strengthening exercises.
4. Tarsal tunnel syndrome is a compression neuropathy where the tibial nerve is compressed as it travels through the tarsal tunnel which is located posterior to the medial malleolus. Tarsal tunnel syndrome is commonly associated with “flat feet” or pronation since this increases pressure in the tunnel region often resulting in nerve compression. Possible interventions include orthotics, rigid arch support, and modalities.
A patient in an acute care hospital makes a sexually charged statement during a treatment session that the therapist finds to be offensive. The therapist expresses to the patient that the comment was inappropriate, however, in response the patient gently laughs. What is the MOST appropriate action?
1. Initiate a log detailing any potential future harassment
2. Explain to the patient you are serious and want the behavior to stop
3. Formally report the harassment to the human resource department
4. Request that the patient is reassigned to another therapist
Health care providers should be aware of the physical, emotional, and psychological consequences associated with sexual harassment. Federal and state laws protect health care providers from being harassed by patients who persist in making verbal or physical advances. When harassment is identified, health care providers should take immediate action to protect themselves and stop the harassment.
1. The patient’s reaction (i.e., laughing) indicates that the patient may not fully understand the therapist’s desire to terminate the unacceptable behavior. Although the log detailing any potential future harassment is potentially beneficial, it is more important for the therapist to be clear on the expected patient behavior.
2. Explaining that you are serious and want the behavior to stop builds upon the therapist’s initial comment and reinforces the need to terminate the unacceptable behavior. If the patient does not change their behavior, the action establishes the groundwork for more formal action.
3. Formally reporting the harassment to the human resource department may be slightly premature since the therapist has not yet been explicit in their desire to stop the harassment and there is not yet a pattern of offensive behavior.
4. Requesting that the patient is reassigned to another therapist is a viable strategy if the patient’s behavior persists, however, addressing the topic in a more direct manner should occur first. This action provides the patient with a better opportunity to learn that their behavior is unacceptable.
A physical therapist attends patient care rounds on an inpatient burn unit and learns that a patient has been scheduled for a grafting procedure later that day. Which of the following wounds would be the BEST candidate for the graft?
1. A deep partial-thickness wound that is infected
2. A large superficial partial-thickness wound that is infected
3. A deep partial-thickness wound that has healed 25% in 30 days
4. A large superficial partial-thickness wound that has healed 50% in 10 days
Normal healing times can be predicted based on the depth of tissue injury. These times are considered to be guidelines which may be significantly altered by the onset of infection or an especially large burn area.
1. An infected deep partial-thickness wound may have healing impeded to such an extent that grafting is eventually indicated. However, the graft procedure would not be carried out in the presence of an active infection due to the risk of additional complications.
2. Although an infection may delay wound healing, grafting is not typically indicated for superficial partial-thickness wounds. If well protected, a wound of this depth will typically heal on its own within three weeks without surgical intervention.
3. A deep partial thickness wound will typically heal within three to five weeks. In the absence of infection, however, wounds of this depth that are slow to heal may require grafting to more effectively facilitate wound closure.
4. A large superficial partial-thickness wound can reasonably be expected to require a longer healing time than wounds with smaller surface areas. Given the typical healing times associated with this degree of tissue damage, 50% healing within a 10-day period would be considered favorable and appropriate.
VIDEO: Shows supine bridge with march
A physical therapist has a patient perform a core strengthening exercise using a therapeutic ball as shown in the video. After observing the patient attempt the exercise the therapist determines that the activity is too difficult for the patient. Which observation would BEST support the therapist’s conclusion?
1. The patient is unable to maintain the spine in a neutral position
2. The patient is unable to lift each foot more than three inches off of the floor
3. The patient has increased difficulty lifting the right foot compared to the left
4. The patient experiences rapid fatigue when completing a set of 10 repetitions
Patients often use a therapeutic ball when performing core strengthening exercises. In order to receive maximum benefit from the exercises, patients must maintain proper alignment of the spine and pelvis when performing transitional movements.
1. Core strengthening exercises typically require the spine to be maintained in a neutral position. Patient’s without adequate core strength for a given activity often are unable to maintain the desired position and attempt to substitute by altering the position of the spine.
2. The height of the patient’s foot from the floor is somewhat variable and would not necessarily indicate that the activity is too difficult for the patient. The relative value of the activity is based on the transfer of weight and not the height the foot is lifted from the floor.
3. It is extremely common for patients to experience increased difficulty with a given upper or lower extremity movement when performing bilateral activities that require independent limb movement. Although the patient may experience increased difficulty with a given extremity, this does not necessarily indicate the activity is too difficult.
4. Core abdominal strengthening exercises are demanding exercises that tend to produce rapid fatigue. In addition, many individuals exhibit significant weakness in the core musculature. As a result, a patient experiencing rapid fatigue when completing the activity is relatively common.
A physical therapist assesses a patient’s left hamstrings length by administering the 90-90 straight leg raising test. The therapist begins the testing procedure by positioning the patient as shown in the video. What is the next step when performing this test?
1. Instruct the patient to actively extend the left knee
2. Instruct the patient to actively extend the left knee while flexing the left hip
3. Passively extend the left knee until slight resistance is felt
4. Passively extend the left knee while flexing the left hip until slight resistance is felt
The 90-90 straight leg raising test is a commonly utilized gross assessment of hamstrings length. Normal flexibility of the hamstrings would result in the patient being able to actively extend the knee within 20 degrees of full knee extension.
1. The 90-90 straight leg raising test requires the patient to actively extend the knee as much as possible from the described test position. The therapist can quantify the relative position of the knee by measuring the amount of knee flexion at the end of the active movement.
2. The 90-90 straight leg raising test requires the patient to maintain the hip in 90 degrees of flexion throughout the entire testing procedure. Failure to maintain the hip in the test position would invalidate the obtained results.
3. The 90-90 straight leg raising test is an active assessment of hamstrings length and therefore it would not be necessary for the therapist to passively extend the patient’s knee.
4. The 90-90 straight leg raising test is an active assessment of hamstrings length and therefore it would not be necessary for the therapist to passively extend the patient’s knee. In addition, the testing procedure requires the patient to maintain the hip in 90 degrees of flexion.
A physical therapist enters the room of a patient diagnosed with tuberculosis. Which of the following precautions would be MOST likely?
1. Airborne precautions and a negative pressure room
2. Airborne precautions and a positive pressure room
3. Droplet precautions and a negative pressure room
4. Contact precaution
Tuberculosis is an infectious, inflammatory disease that affects the lungs and can spread to involve lymph nodes and other organs. For patients who have documented or suspected infections that are highly transmissible, transmission-based precautions are in place in addition to the standard precautions used during all patient care activities. Transmission based precautions include contact, airborne, and droplet precautions.
1. Airborne precautions reduce the risk of airborne transmission of infectious agents through evaporated droplets in air or dust particles. A patient with this type of infection will be in a negative pressure room. A negative pressure room includes a ventilation system that generates negative pressure to allow air into the room, but prevents infected air from escaping. Anyone entering the room will wear respiratory protection. Tuberculosis is an example of an infection that is transmitted through an airborne mode.
2. The described patient will most likely be on airborne precautions, but will not be in a positive pressure room. Positive pressure rooms are used for patients with compromised immune systems, such as patients who have HIV. A positive pressure system filters the air before delivery with a HEPA filter and then pumps the air into the isolation room at high pressure which forces air from the isolation room into the hallway.
3. Droplet precautions reduce the risk of droplet transmission of infectious agents through contact of the mucous membranes of the mouth and nose, contact with the conjunctivae, and through coughing, sneezing, talking or suctioning. These infectious agents do not suspend in the air and will travel only three feet or less. A mask should be worn when working within three feet of the patient. Examples of infectious agents transmitted by droplet mode include pneumonia and influenza.
4. Contact precautions reduce the risk of transmission of infectious agents through direct or indirect contact. Examples of infectious agents that can be transmitted through contact include Clostridium difficile, scabies, herpes zoster, and multi-drug resistant bacteria. A physical therapist working with a patient on contact precautions will wear gloves and a gown.
A physical therapist assesses a patient’s shoulder passive range of motion and finds a significant limitation in external rotation with the shoulder abducted to 100 degrees. The therapist classifies the end-feel as firm. Which structure is MOST likely limiting the patient’s motion?
1. Superior glenohumeral ligament
2. Middle glenohumeral ligament
3. Inferior glenohumeral ligament
4. Coracohumeral ligament
1. The superior glenohumeral ligament’s primary role is to limit inferior translation when the shoulder is adducted. It also limits external rotation when the shoulder is in 0-45 degrees of abduction.
2. The middle glenohumeral ligament’s primary role is to limit external rotation when the shoulder is in 45-90 degrees of abduction.
3. The inferior glenohumeral ligament’s primary role is to support the humeral head above 90 degrees of abduction. The ligament is the most important stabilizing structure of the shoulder for patients that engage in overhead activities. The inferior glenohumeral ligament has an anterior and posterior band. The anterior band tightens on lateral rotation and the posterior band tightens on medial rotation. The inferior glenohumeral ligament would most likely be limiting the patient’s range of motion because the shoulder is in 100 degrees of abduction (i.e., over 90 degrees).
4. The coracohumeral ligament’s primary role is to limit inferior translation as well as limit external rotation when the shoulder is in less than 60 degrees of abduction.
A physical therapist attempts to facilitate upper extremity reaching in an eight-month-old infant positioned in supine. The infant presents with a persistent tonic labyrinthine reflex. Which of the following positions would be the MOST likely to eliminate the influence of this reflex while achieving the therapist’s objective?
1. Supine with the upper trunk on a wedge and legs over a bolster
2. Supine with the legs and trunk extended
3. Prone with a pillow under the abdomen
4. Prone with the legs and trunk extended
The tonic labyrinthine reflex results in changes in tone based on head position and the head’s relationship to gravity. This reflex is present at birth and is typically integrated by six months of age. When a child is positioned in supine, the tonic labyrinthine reflex causes an increase in extensor tone, impairing the child’s ability to flex against gravity. Conversely, when the child with a persistent reflex is positioned in prone there is an increase in flexor tone, limiting the child’s ability to lift their head against gravity.
1. The trunk flexion and hip flexion achieved by positioning the child in supine with the upper trunk on a wedge and legs over a bolster counteracts the extensor tone elicited by the tonic labyrinthine reflex. This is the best position for the child to eliminate the influence of the reflex and facilitate upper extremity reaching.
2. Positioning the child in supine with the legs and trunk extended will activate the supine tonic labyrinthine reflex and will increase extensor tone. The increase in extensor tone will inhibit the child from flexing the upper extremity to perform reaching activities.
3. Positioning the child in prone with a pillow under the abdomen will promote an increased flexor tone associated with a persistent prone tonic labyrinthine reflex. This position will not facilitate the child’s ability to participate in upper extremity reaching activities.
4. Positioning the child in prone with the legs and trunk extended will result in increased flexor tone associated with a persistent tonic labyrinthine reflex. This position will not allow the child to participate in reaching activities.
A physical therapist reviews the medical record of a patient that is currently on bed rest secondary to a deep vein thrombosis. What would be the risk factor that is MOST likely to be associated with the deep vein thrombosis?
1. Varicose veins
2. Prolonged liver disease
3. Total hip arthroplasty
4. Tobacco use
A deep vein thrombosis is a blood clot that forms in a vein with the potential to dislodge as an embolism and travel until it blocks an artery. There are various risk factors for acquiring a deep vein thrombosis.
1. Varicose veins are swollen, twisted, and sometimes painful veins near the surface of the skin that have filled with an abnormal collection of blood. Varicose veins have a weak association with acquiring a deep vein thrombosis.
2. Prolonged liver disease can often produce prolonged clotting times, reduced clearance of fibrin degradation products, and thrombocytopenia. It is hypothesized that the impairment of normal hemostasis acts to protect against acquiring a deep vein thrombosis.
3. Major surgery on the hip, knee, leg, calf, abdomen or chest significantly increases the risk of acquiring a deep vein thrombosis. Symptoms of a deep vein thrombosis include swelling of the lower extremity, pain, sensitivity, and warmth over the area of the clot.
4. Tobacco use has a weak association with acquiring a deep vein thrombosis. Other risk factors include advanced age, obesity, infection, and air travel.
A physical therapist documents that the Neer impingement test is positive after a patient reports marked pain during the testing procedure. What is the PRIMARY source of pain when performing this special test?
1. Compression of the greater tuberosity against the anterior acromion
2. Compression of the greater tuberosity against the posterior acromion
3. Compression of the lesser tuberosity against the anterior acromion
4. Compression of the lesser tuberosity against the posterior acromion
The Neer impingement test is performed with the patient positioned in sitting or standing. The therapist positions one hand on the posterior aspect of the patient’s scapula and the other hand stabilizing the elbow. The therapist then elevates the patient’s arm through flexion. A positive test is indicated by a facial grimace or pain and may be indicative of shoulder impingement involving the supraspinatus tendon.
1. When the shoulder is flexed, the humeral head slides posteriorly and rolls anteriorly. The facial grimace or pain associated with a positive Neer impingement test typically results from compression of the greater tuberosity against the anterior acromion during shoulder flexion.
2. When the shoulder is flexed during the Neer impingement test, the humeral head often comes into contact with the acromion, however, the contact tends to occur with the anterior acromion.
3. When the shoulder is flexed during the Neer impingement test, the lesser tuberosity typically is unaffected. The lesser tuberosity can be involved in secondary impingement since it can encroach on the coracoid process.
4. When the shoulder is flexed during the Neer impingement test, the lesser tuberosity typically is unaffected. The lesser tuberosity can be involved in secondary impingement since it can encroach on the coracoid process.
Video Shows: L limb being pushed into abduction, the right leg ADDUCTS towards left leg
A patient status post left CVA works on strengthening the hip abductors and adductors while positioned in supine on a mat. The physical therapist applies resistance as shown in the video and observes the patient’s response. Which term is MOST consistent with the depicted scenario?
1. Limb synergy
2. Souques’ phenomenon
3. Raimiste’s phenomenon
4. Homolateral synkinesis
An associated reaction is an involuntary and automatic movement of a body part as a result of an intentional active or resistive movement in another body part. Neurological impairment allows for such associated reactions.
1. Synergies are considered primitive patterns that occur at the spinal cord level as a result of the hierarchical organization of the central nervous system. Reinforcing synergy patterns is rarely utilized in neurological rehabilitation.
2. Souques’ phenomenon involves raising the involved upper extremity above 100 degrees with elbow extension in order to produce extension and abduction of the fingers.
3. Raimiste’s phenomenon involves facilitating hip abduction or hip adduction of the involved lower extremity with applied resistance to the uninvolved lower extremity in the same direction.
4. Homolateral synkinesis occurs when a flexion pattern of the involved upper extremity facilitates flexion of the involved lower extremity.
A 29-year-old female who recently gave birth to twins is referred to physical therapy for treatment of low back pain. During the session the therapist identifies a four-centimeter separation of the rectus abdominis. The therapist instructs the patient to wrap a sheet around their abdomen while performing an exercise in hooklying. Which of the following exercises would be the MOST appropriate?
1. Lower trunk rotations
2. Head lifts
3. Abdominal curls
4. Diagonal abdominal curls
Diastasis recti is the separation of the rectus abdominis in the midline at the linea alba. Due to the size of the separation (i.e., four centimeters), aggressive abdominal strengthening exercises should be avoided. If the size of the separation is less than two centimeters, more provocative exercises can be attempted. When exercising, the patient should wrap a sheet around the trunk at the level of the separation to approximate the separated muscle.
1. Lower trunk rotation is an exercise performed in hooklying where the patient simultaneously rotates both knees down toward the floor. Exercises involving trunk rotation should be avoided since the rotation may lead to further separation of the rectus abdominis.
2. A head lift in hooklying would be the most appropriate exercise for the patient since the exercise allows for only modest strengthening of the rectus abdominis while minimizing the influence of the obliques (i.e., muscles of rotation). This exercise has the lowest risk of further separating the rectus abdominis, especially if a sheet is used to approximate the muscle.
3. Though abdominal curls focus on strengthening the rectus abdominis while minimizing engagement of the obliques, a full abdominal curl would be too aggressive for a patient with a four-centimeter separation. Once the separation is two centimeters or less, more aggressive exercises may be attempted.
4. Diagonal abdominal curls would be an inappropriate exercise for the patient. Not only is an abdominal curl too aggressive, the diagonal abdominal curl is even more advanced since it requires rotation, and thus engagement of the oblique muscles.
A 67-year-old female was recently diagnosed with congestive heart failure. The patient has a lengthy past medical history including renal insufficiency. Which symptom was MOST likely associated with the development of congestive heart failure based on the patient’s past medical history?
1. Left ventricular hypertrophy
2. Fluid overload
3. Pulmonary embolism
4. Valvular stenosis
Congestive heart failure is a progressive condition in which the heart cannot maintain a normal cardiac output to meet the body’s demands for blood and oxygen. Heart failure often develops after other conditions have damaged or weakened the heart. The ventricles weaken and dilate to the point that the heart can’t pump efficiently.
1. Left ventricular hypertrophy often results from increased arterial pressure associated with hypertension. Although hypertension can contribute to the development of congestive heart failure, it is not likely to be the primary symptom given the patient’s past medical history.
2. Fluid overload associated with renal insufficiency often contributes to the development of congestive heart failure. The fact that the medical record includes a history of renal insufficiency makes fluid overload the most relevant symptom.
3. Pulmonary embolism can produce severe hypoxemia impacting the lungs and resulting in elevated pulmonary artery pressures. Although pulmonary embolism can contribute to the development of congestive heart failure, it is not likely to be the primary symptom given the patient’s past medical history.
4. Valvular stenosis or incompetent valves can result in myocardial hypertrophy. Although valvular stenosis can contribute to the development of congestive heart failure, it is not likely to be the primary symptom given the patient’s past medical history.
Setting: Outpatient rehabilitation clinic
Gender: Male
Age: 63 years
Presenting Problem/Current Condition
Parkinson’s disease
Medical History
Diabetes
Other Information
Currently resides with daughter due to mobility concerns
Patient expresses a strong desire to return to his home
Extremely frustrated by freezing episodes and limited ability to perform ADLs
Meds: Recently started taking Sinemet (carbidopa/levodopa)
Physical Therapy Examination(s)
Resting and intention tremors
Festinating gait with stooped posture
Decreased dynamic postural stability
Periodic akinesia and hypokinesia
Physical Therapy Plan of Care
Balance activities
Functional mobility
Postural awareness
Whole-body vibration
Exercise emphasizing rotational and large amplitude movements
Safety awareness
Which parameter of gait would be increased based on the identified gait pattern?
1. Cadence
2. Step length
3. Stride length
4. Walking speed
A festinating gait is characterized by a patient walking on their toes as though pushed. It starts slowly, increases, and may continue until the patient grasps an object in order to stop. The gait pattern is a manifestation of basal ganglia degeneration and the associated decline in the patient’s ability to modulate automatic mobility tasks.
1. Cadence refers to the number of steps an individual will walk over a period of time. The average value for an adult is 110–120 steps per minute. Although slowness of movement is characteristic of this type of gait pattern, cadence would increase due to the small shuffling steps.
2. Step length refers to the distance measured between right heel strike and left heel strike. The average step length for an adult is 28 inches. Step length would decrease in patients exhibiting a Parkinsonian gait pattern.
3. Stride length refers to the distance measured between right heel strike and the following right heel strike. The average stride length for an adult is 56 inches. Stride length would decrease in patients exhibiting a Parkinsonian gait pattern.
4. Walking speed refers to the distance traveled per unit of time and is typically expressed in miles per hour. Walking speed would decrease in patients exhibiting a Parkinsonian gait pattern despite the increased cadence because of the small shuffling steps.
Setting: Outpatient rehabilitation clinic
Gender: Male
Age: 63 years
Presenting Problem/Current Condition
Parkinson’s disease
Medical History
Diabetes
Other Information
Currently resides with daughter due to mobility concerns
Patient expresses a strong desire to return to his home
Extremely frustrated by freezing episodes and limited ability to perform ADLs
Meds: Recently started taking Sinemet (carbidopa/levodopa)
Physical Therapy Examination(s)
Resting and intention tremors
Festinating gait with stooped posture
Decreased dynamic postural stability
Periodic akinesia and hypokinesia
Physical Therapy Plan of Care
Balance activities
Functional mobility
Postural awareness
Whole-body vibration
Exercise emphasizing rotational and large amplitude movements
Safety awareness
Which physical therapy intervention would be MOST affected secondary to the potential negative side effects of the prescribed medication?
1. Balance activities
2. Strengthening activities
3. Range of motion activities
4. Endurance activities
Parkinson’s disease is a primary degenerative disorder and is characterized by a decrease in production of the neurotransmitter dopamine within the substantia nigra of the basal ganglia. Dopamine replacement therapy, such as levodopa (Sinemet), is the most effective treatment in reducing the symptoms of Parkinson’s disease such as movement disorders, bradykinesia, rigidity, and tremor.
1. During the initial use of levodopa, patients regularly experience lightheadedness and orthostatic hypotension. Balance activities would pose the greatest challenge for this patient during this period given the newly prescribed medication. The patient should be monitored closely to ensure safety with activities that challenge their balance.
2. Strengthening activities increase the patient’s overall strength and can include isometric, concentric, and eccentric strengthening. Levodopa does not typically affect strength.
3. Range of motion activities promote adequate mobility at each joint. Levodopa does not affect range of motion. As a result, range of motion activities should not increase in difficulty due to the prescribed medication.
4. Endurance activities improve the aerobic system to meet oxygen demands. Levodopa can initially cause orthostatic hypotension, which can impact the cardiovascular system. However, endurance activities can still be performed without significantly challenging the patient’s balance.
Setting: Outpatient rehabilitation clinic
Gender: Male
Age: 63 years
Presenting Problem/Current Condition
Parkinson’s disease
Medical History
Diabetes
Other Information
Currently resides with daughter due to mobility concerns
Patient expresses a strong desire to return to his home
Extremely frustrated by freezing episodes and limited ability to perform ADLs
Meds: Recently started taking Sinemet (carbidopa/levodopa)
Physical Therapy Examination(s)
Resting and intention tremors
Festinating gait with stooped posture
Decreased dynamic postural stability
Periodic akinesia and hypokinesia
Physical Therapy Plan of Care
Balance activities
Functional mobility
Postural awareness
Whole-body vibration
Exercise emphasizing rotational and large amplitude movements
Safety awareness
Which of the following options will increase the patient's ability to independently resume walking following a freezing episode?
1. Trunk rotation in sitting prior to walking
2. Walking on a treadmill
3. Counting ("one, two, three,...") while attempting to resume walking
4. Practicing walking in a crowded environment
Patients diagnosed with Parkinson’s disease often experience difficulty with gait including small, shuffling steps and freezing episodes. Both auditory and visual stimuli are used to address these difficulties.
1. Trunk rotation will not aid in decreasing the occurrence of freezing episodes. Rotation is more often used to decrease hypertonicity or rigidity. Additionally, performing any strategy prior to a freezing episode will not assist the patient to resume walking during the freezing episode.
2. While walking on a treadmill may assist a patient with their gait pattern, it will not help a patient resume walking during a freezing episode. Additionally, freezing often occurs in a specific context (e.g., walking through a doorway), and a treadmill would be unable to mimic these scenarios.
3. Although it may not decrease the frequency of freezing episodes, auditory cues (e.g., counting “one, two, three”) are useful in assisting a patient to resume walking after a freezing episode. If a patient gets “stuck” in a freezing episode, they can independently use this strategy to continue walking.
4. Walking in a crowded environment may be an appropriate challenge to the patient’s current gait impairments. However, this would not be a specific strategy used to help a patient resume walking during a freezing episode.
Setting: Outpatient rehabilitation clinic
Gender: Male
Age: 63 years
Presenting Problem/Current Condition
Parkinson’s disease
Medical History
Diabetes
Other Information
Currently resides with daughter due to mobility concerns
Patient expresses a strong desire to return to his home
Extremely frustrated by freezing episodes and limited ability to perform ADLs
Meds: Recently started taking Sinemet (carbidopa/levodopa)
Physical Therapy Examination(s)
Resting and intention tremors
Festinating gait with stooped posture
Decreased dynamic postural stability
Periodic akinesia and hypokinesia
Physical Therapy Plan of Care
Balance activities
Functional mobility
Postural awareness
Whole-body vibration
Exercise emphasizing rotational and large amplitude movements
Safety awareness
Which of the following interventions would MOST likely address the patient’s goal of returning home?
1. Core stabilization exercises to maintain a neutral spine
2. Neuromuscular electrical stimulation to reduce atrophy
3. Sensory integration techniques to improve attention
4. Rhythmic auditory stimulation to improve gait activities
Rhythmic movement and auditory cues can be helpful for patients exhibiting akinesia and hypokinesia. These strategies, along with counting to help initiate walking after freezing, would be important to teach family and caregivers.
1. Core stabilization exercises involve activating the deep abdominal muscles (e.g., transverse abdominis) and deep back extensors (e.g., multifidi) to maintain a neutral spine during functional activities. This intervention does not address mobility concerns in returning home.
2. Neuromuscular electrical stimulation (NMES) is a technique used to facilitate skeletal muscle activity. The symptoms of Parkinson’s disease typically include movement disorders such as bradykinesia, rigidity, and tremor. Given the focus of NMES to decrease muscle atrophy, this would not be a primary intervention for a patient with Parkinson’s disease to address mobility issues to return home.
3. Sensory integration techniques are most commonly used for children with learning disorders to help with sensory processing impairments. Sensory integration therapy often involves play activities (e.g., bouncing, spinning) that are believed to help organize the sensory system by providing vestibular, proprioceptive, auditory, and tactile inputs. Given the focus of sensory integration techniques on improving attention, this would not be a primary intervention for a patient with Parkinson’s disease to address mobility issues to return home.
4. Rhythmic auditory stimulation (RAS) typically involves the use of a metronome or a steady beat from a musical device to improve gait or gait-related aspects of movement. Studies have shown RAS to improve gait speed, cadence, and stride length in patients with Parkinson’s disease. This intervention effectively addresses the patient’s mobility concerns and most directly addresses the patient’s goal of returning home.
Setting: Outpatient rehabilitation clinic
Gender: Male
Age: 63 years
Presenting Problem/Current Condition
Parkinson’s disease
Medical History
Diabetes
Other Information
Currently resides with daughter due to mobility concerns
Patient expresses a strong desire to return to his home
Extremely frustrated by freezing episodes and limited ability to perform ADLs
Meds: Recently started taking Sinemet (carbidopa/levodopa)
Physical Therapy Examination(s)
Resting and intention tremors
Festinating gait with stooped posture
Decreased dynamic postural stability
Periodic akinesia and hypokinesia
Physical Therapy Plan of Care
Balance activities
Functional mobility
Postural awareness
Whole-body vibration
Exercise emphasizing rotational and large amplitude movements
Safety awareness
Which patient symptom would provide the BEST justification for the use of whole-body vibration?
1. Dysphagia
2. Tremor
3. Akinesia
4. Cognitive impairment
Whole-body vibration consists of transferring vibration of varying frequencies to the body. Vibration training can be utilized as an intervention to improve muscle strength, power, flexibility, coordination, and to decrease tremors/rigidity. Common medical conditions treated with whole-body vibration include osteoporosis, balance disorders, and Parkinson’s disease.
1. Dysphagia refers to the inability to swallow properly. Treatment of dysphagia does not include whole-body vibration, but rather focuses on proper body positioning and compensatory strategies to avoid aspiration when swallowing. Educational topics include the use of thick liquids and conscious swallowing.
2. Whole-body vibration effectively decreases tremors and rigidity in patients with Parkinson’s disease. Vibratory input to the muscle spindle biases information about muscle length, resulting in more fluid and purposeful movement during memory-guided activity.
3. Akinesia refers to the inability to initiate movement. The decrease in tremor and rigidity associated with vibration can allow for improved gait and increased step length. However, the actual inability to initiate movement is not directly affected by this intervention.
4. Cognitive, memory, and language impairments can be associated with Parkinson’s disease. These impairments most often involve executive functioning within the brain. Cognitive impairments are not affected with the use of whole-body vibration. Adaptive strategies are most commonly utilized to assist with cognitive deficits.
Setting: Outpatient rehabilitation clinic
Gender: Male
Age: 63 years
Presenting Problem/Current Condition
Parkinson’s disease
Medical History
Diabetes
Other Information
Currently resides with daughter due to mobility concerns
Patient expresses a strong desire to return to his home
Extremely frustrated by freezing episodes and limited ability to perform ADLs
Meds: Recently started taking Sinemet (carbidopa/levodopa)
Physical Therapy Examination(s)
Resting and intention tremors
Festinating gait with stooped posture
Decreased dynamic postural stability
Periodic akinesia and hypokinesia
Physical Therapy Plan of Care
Balance activities
Functional mobility
Postural awareness
Whole-body vibration
Exercise emphasizing rotational and large amplitude movements
Safety awareness
When working on controlled mobility with the patient, which of the following would BEST describe the therapist’s objective?
1. Facilitate postural muscle control
2. Promote weight shifting and rotational trunk control
3. Emphasize reciprocal extremity movement
4. Facilitate tone and rigidity
Controlled mobility refers to the ability to move within a weight bearing position or rotate around a long axis. Controlled mobility is one of the four stages of motor control (i.e., mobility, stability, controlled mobility, and skill).
1. Stability refers to the ability to maintain a position or posture through cocontraction and tonic holding around a joint. One example of stability includes unsupported sitting with midline control.
2. Controlled mobility activities should emphasize weight shifting and trunk control with rotation. This type of activity may serve to decrease rigidity and improve the fluidity of gait in a patient with Parkinson’s disease.
3. A patient must possess prerequisite stability and dynamic postural control to perform reciprocal extremity movement. Coordination training often focuses on reciprocal extremity movement.
4. Facilitation techniques are used to increase tone in patients with hypotonia. These techniques are not often used to treat Parkinson’s disease since patients with this condition typically exhibit hypertonia or, in more severe cases, rigidity.
A physical therapist elects to use proprioceptive neuromuscular facilitation (PNF) techniques to help improve a patient’s coordination with movement. Which of the following statements is MOST consistent with the PNF treatment approach?
1. Extremity movement patterns should occur in the cardinal planes.
2. Extremity movement patterns are named for the movement that occurs at the distal joint.
3. PNF patterns consist of unilateral extremity movements only.
4. Rotation is an important component of the movement patterns.
Proprioceptive neuromuscular facilitation (PNF) is a treatment approach developed by Kabat, Knott, and Voss in which movement patterns are diagonal and spiral in nature. It is directed at improving function, performance, and coordinated movement and is commonly used to treat patients with musculoskeletal and/or neuromuscular deficits.
1. The PNF approach uses movement patterns that are diagonal and spiral in nature rather than straight plane (i.e., cardinal plane) movements.
2. When naming the various PNF patterns (e.g., D1 flexion), the pattern is named according to the action that is occurring at the proximal joint.
3. Though many of the PNF patterns are unilateral patterns (e.g., D1 flexion), bilateral patterns and trunk patterns can also be used (e.g., chopping patterns).
4. PNF patterns are diagonal and spiral (i.e., rotational) in nature. For example, the D1 flexion pattern involves external rotation of the shoulder and supination at the forearm.
A physical therapist places a patient in a semi-recumbent position to assess the magnitude of jugular vein distention. Jugular vein distention would MOST likely indicate the presence of which condition?
1. Peripheral arterial disease
2. Congestive heart failure
3. Coronary artery disease
4. Aortic aneurysm
Jugular vein distention results from fluid overload when the heart is unable to pump blood efficiently. As the heart’s ability to pump is compromised, the fluid backs up into the lungs and venous system. Assessing distention of the jugular vein is an effective way to evaluate the functioning of the heart.
1. Peripheral arterial disease is a condition characterized by atherosclerotic plaque build-up in the peripheral arteries that causes occlusion of the blood flow to the extremities. A patient with peripheral arterial disease would experience signs and symptoms of ischemia such as intermittent claudication or skin changes. Jugular vein distention is not typically observed with this condition.
2. Congestive heart failure is a condition characterized by an inability of the heart to effectively pump blood to meet the demands of the body. When the heart can no longer effectively pump blood to the body, fluid backs up into the lungs and venous system. A common sign of this type of fluid accumulation is distention of the jugular vein.
3. Coronary artery disease is a condition characterized by atherosclerotic plaque build-up in the coronary arteries of the heart. Typical signs and symptoms of this condition include angina and myocardial infarction. Jugular vein distention is not typically observed with this condition.
4. Aortic aneurysm is a condition characterized by the permanent dilation of the aortic wall. Due to the blood flow disturbance through the dilated segment of the aorta, the formation of thrombi and emboli can result from this condition. Rupture of the aorta may also result from this condition, leading to uncontrolled hemorrhage and circulatory collapse. Jugular vein distention is not typically observed with this condition.
A physical therapist works with a patient who complains of joint and muscle pain. The therapist reads in the doctor’s note that the patient has a cardiovascular condition that results in damage to the heart valves. Which medical condition is MOST consistent with this description?
1. Pericarditis
2. Coronary artery disease
3. Endocarditis
4. Congestive heart failure
Conditions that affect the heart valves increase the workload of the heart and require the heart to pump harder to maintain adequate blood flow. For patients affected by these conditions, initial symptoms usually involve fatigue. As the condition progresses, symptoms of heart failure (e.g., dyspnea) usually appear.
1. Pericarditis is a condition characterized by inflammation of the pericardium, the layer that covers the outside of the heart. Signs and symptoms of this condition include angina, dyspnea, malaise, and myalgia.
2. Coronary artery disease is a condition characterized by a narrowing or blockage of the coronary arteries which are the vessels that supply blood to the heart. Signs and symptoms of this condition include angina and, if it progresses, myocardial infarction.
3. Endocarditis is a condition characterized by inflammation of the cardiac endothelium, the layer that lines the inside of the heart. This condition may result in damage to the aortic, tricuspid or mitral valve. Signs and symptoms include musculoskeletal symptoms such as arthralgia, arthritis, low back pain, and myalgia.
4. Congestive heart failure is a condition characterized by the heart’s inability to pump enough blood to meet the demands of the body. Signs and symptoms of this condition are dependent upon which side of the heart is affected, but generally include fatigue, dyspnea, and edema.
A physical therapist hypothesizes that a child diagnosed with spina bifida may be exhibiting signs of shunt malfunction. Which signs and symptoms would BEST support the therapist’s hypothesis?
1. Increased irritability and lethargy
2. Decreased tone and deep tendon reflexes
3. Shallow breathing and rapid pulse
4. Skin redness and rash
Hydrocephalus is an increase of cerebrospinal fluid (CSF) within the ventricles of the brain typically due to poor resorption, obstruction of flow or excessive production of CSF. The majority of patients with spina bifida experience hydrocephalus. Successful treatment typically includes surgical placement of a shunt.
1. Physical therapists working with patients with hydrocephalus must be aware of symptoms of the condition as well as shunt malfunction. Immediate medical intervention is often necessary to alleviate the excessive fluid within the brain. Failure to act in a timely manner can result in coma and/or death. Symptoms of potential shunt malfunction include irritability, lethargy, headache, seizures, vomiting, incontinence, and confusion.
2. A lower motor neuron disease is characterized by a lesion that affects nerves or their axons at or below the level of the brainstem, usually within the “final common pathway.” Symptoms include flaccidity or weakness of the involved muscles, decreased tone, fasciculations, muscle atrophy, and decreased or absent reflexes.
3. Shock is caused by insufficient circulating blood volume. In addition to shallow breathing and a rapid pulse, a person can experience altered mental status, decreased urine output, cool and clammy skin, and thirst. Shock is a life threatening condition if not treated in a timely manner.
4. Allergic reactions are sensitivities to allergens that come into contact with the skin, nose, eyes, respiratory tract, and gastrointestinal tract. Common symptoms of a mild allergic reaction include hives, itching, nasal congestion, rashes and red or watering eyes. Anaphylaxis is a sudden and severe life-threatening allergic reaction that occurs within minutes of exposure and requires immediate medical attention.
A physical therapist reviews the medical record of a patient and notes that the patient requires a gluten free diet. What is the MOST likely diagnosis associated with this regimen?
1. Celiac disease
2. Crohn’s disease
3. Diverticulitis
4. Irritable bowel syndrome
Physical therapists must possess an understanding of dietary choices based on specific medical conditions. Patients with diagnoses or comorbidities that relate to the gastrointestinal system may require modification of particular interventions such as positioning, treatment environment, and timing of physical therapy sessions.
1. Celiac disease results from the body’s intolerance of gluten, a protein component of wheat. The condition is characterized by poor nutritional absorption. Signs and symptoms include recurrent diarrhea, abdominal cramping, gas, and signs of malnutrition. Once diagnosed, treatment includes a gluten free diet and vitamin supplements in order to receive adequate nutrition.
2. Crohn’s disease is a specific form of inflammatory bowel disease in which the lining of the gastrointestinal (GI) tract becomes abnormally inflamed. The etiology of Crohn’s disease is idiopathic, but likely the result of an imbalance between anti-inflammatory and pro-inflammatory mediators within the GI tract. Symptoms are typically associated with the inflammatory process or complications such as fibrosis or obstruction most often located in the small bowel or colon.
3. Diverticulitis refers to inflamed or infected diverticula which are pouch-like protrusions within the colon. The exact etiology of diverticulitis is unknown, however, it may be associated with a low fiber diet. Treatment includes an increased amount of daily dietary fiber. Some patients with diverticulitis may develop complications including intestinal fistula, malnutrition, and bowel obstruction.
4. Irritable bowel syndrome consists of recurrent symptoms of the gastrointestinal system that interfere with the normal functioning of the colon. The exact etiology is unknown, but theories include food sensitivities, stress, immune system dysfunction or bacterial infections. Symptoms can include abdominal pain, bloating, nausea, vomiting, and changes in the consistency of stool. Irritable bowel syndrome can typically be controlled by diet, pharmacological intervention, and stress management.
A physical therapist examines several distance and time parameters associated with gait. Which finding would be MOST anticipated when comparing walking in an 18-month-old to walking in an older child (i.e., 7 year old)?
1. An older child would exhibit decreased step length
2. An older child would exhibit decreased stride length
3. An older child would exhibit decreased cadence
4. An older child would exhibit decreased walking velocity
Time and distance parameters are often used to provide a basic description of gait. Commonly used temporal variables include stance time, single limb and double limb support time, cadence, and speed. Commonly used distance variables include stride length, step length, width of base of support, and degrees of toe-out.
1. Step length is defined as the distance measured between right heel strike and left heel strike. The average step length for an 18-month-old is 25 centimeters compared to 48 centimeters for a 7-year-old.
2. Stride length is defined as the distance measured between right heel strike and the following right heel strike. The average stride length for an 18-month-old is 50 centimeters compared to 97 centimeters for a 7-year-old.
3. Cadence is defined as the number of steps an individual will walk over a period of time. The average cadence for an 18-month-old is 171 steps per minute compared to 144 steps per minute for a 7-year-old. The average adult cadence is 110–120 steps per minute. Despite the decrease in cadence, the older child’s walking velocity still increases due to the increase in physical stature (e.g., limb length), enhanced fluidity of movement, and greater muscular force.
4. Walking velocity is defined as the speed of ambulation in a given direction. The average walking velocity for an 18-month-old is 42.6 meters per minute compared to 68.4 meters per minute for a 7-year-old.
A physical therapist attempts to trial the use of an orthosis for a patient with a steppage gait. Which of the following would be MOST appropriate for the therapist to utilize in the trial?
1. Knee-ankle-foot orthosis (KAFO)
2. Hip-knee-ankle-foot orthosis (HKAFO)
3. Ankle-foot orthosis (AFO)
4. Knee immobilize
A steppage gait occurs as a form of compensation for weakness or paralysis of the dorsiflexor muscles. A patient with a steppage gait tends to excessively flex the hip and knee in an effort to clear the foot.
1. A steppage gait involves weakness of the dorsiflexors and therefore would not result in instability at the knee. As a result, the use of a KAFO would not be warranted.
2. A steppage gait involves weakness of the dorsiflexors and therefore would not result in instability at the hip and knee. As a result, the use of a HKAFO would not be warranted.
3. An AFO is the most appropriate intervention to address dorsiflexor weakness and prevent toe drag/foot drop.
4. A knee immobilizer is not indicated for dorsiflexor weakness. Knee immobilizers are often prescribed post-operatively to protect the operated limb until quadriceps strength improves.
A physical therapist palpates a patient’s popliteal artery to monitor their lower extremity circulation. What is the MOST likely reason the therapist used the popliteal artery?
1. The therapist suspects a blockage of the femoral artery
2. The therapist is trying to determine the patient’s ankle-brachial index
3. The popliteal artery is superficial in the popliteal fossa and easy to locate
4. The patient is taking beta-blockers
Peripheral pulses are monitored by palpation with the index and middle finger using light pressure. There are a variety of sites that can be used to monitor pulse including the temporal, carotid, brachial, radial, femoral, popliteal, and dorsalis pedis arteries.
1. If the therapist suspects a blockage in the femoral artery, a distal pulse site should be used (e.g., popliteal artery, dorsalis pedis artery). A weak or absent popliteal pulse may indicate impaired flow or a blockage of a more proximal blood vessel (e.g., femoral artery).
2. When determining a patient’s ankle-brachial index (ABI), the standard procedure is to use a distal pulse site (e.g., dorsalis pedis artery, posterior tibial artery). The popliteal artery is not typically used. Furthermore, ABI is a measure of blood pressure, not pulse rate.
3. The popliteal artery is often difficult to locate due to its deep location in the popliteal fossa. Because of this, the femoral or dorsalis pedis artery is more commonly used to assess lower extremity circulation.
4. Beta-blockers are a category of drug that decreases both resting heart rate and heart rate response to exercise. While taking this medication would affect a patient’s heart rate, it would do so equally across all pulse sites. This alone would not be a reason to use the popliteal artery for monitoring a patient’s pulse.
A physical therapist completes a systems review on a patient status post ankle arthrodesis. Which of the following pieces of information would NOT be documented in the integumentary section of the systems review?
1. Pliability of the scar
2. Level of edema
3. Continuity of skin color
4. Skin integrity
After organizing information obtained from the patient history, a physical therapist should perform a systems review. The systems review is a brief examination of the four main systems of the body (i.e., musculoskeletal, neuromuscular, cardiopulmonary, integumentary) as well as assessment of communication, affect, cognition, and learning style. Information gained from the systems review should inform what tests and measures will be performed.
1. Assessment of scar formation should be documented in the integumentary section of the systems review. Abnormalities in scar formation may include information about the scar’s color, pliability, and texture.
2. Assessment of edema should be documented in the cardiopulmonary section of the systems review. Other cardiopulmonary assessments include heart rate, blood pressure, and respiratory rate.
3. Assessment of skin color should be documented in the integumentary section of the systems review. Abnormalities in skin color may include pallor, redness or bruising.
4. Assessment of skin integrity should be documented in the integumentary section of the systems review. Abnormalities in skin integrity may include small lacerations or the presence of wounds.
A physical therapist reads in the medical record that a patient exhibits asthenia. Which test would be the MOST useful to identify the presence of this condition?
1. Manual resistance to assess muscle strength
2. Marching in place
3. Alternating finger to nose
4. Placing feet on floor markers while walking
There are a variety of tests designed to identify unique coordination deficits. The tests are often included as part of a neurological assessment. Physical therapists should be familiar with how to perform these tests and how to interpret the associated results.
1. Manual resistance to assess muscle strength is often used to test for asthenia. Asthenia refers to generalized weakness, typically secondary to cerebellar pathology.
2. Marching in place is often used to test for a cerebellar movement disorder. A positive test occurs when a patient is unable to follow the rhythm of the cadence.
3. Alternating finger to nose is often used to test for dysdiadochokinesia. Dysdiadochokinesia refers to the inability to perform rapid alternating movements. This condition is a result of damage to the cerebellum.
4. Placing the feet on floor markers while walking is often used to test for dysmetria. Dysmetria refers to the inability to control the range of a movement and the force of muscular activity. This condition is a result of damage to the cerebellum
A note in the medical record indicates a patient is exhibiting signs and symptoms of rhabdomyolysis. Which of the following would be the MOST relevant finding based on this condition?
1. Decreased joint mobility
2. Diminished muscle performance
3. Increased pain
4. Diminished coordination
Rhabdomyolysis is a condition where breakdown of striated muscle fibers leads to the release of myoglobin into the bloodstream. Myoglobin is harmful to the kidneys and can often lead to kidney damage. Rhabdomyolysis occurs with damage to skeletal muscle tissue, particularly following injury.
1. Joint pain and stiffness can occur with rhabdomyolysis, however, joint mobility should not be the most relevant finding since the joint capsule itself is not affected.
2. Diminished muscle performance is associated with rhabdomyolysis due to direct damage to the muscle fibers.
3. Pain, in the form of joint pain and stiffness, can be present with rhabdomyolysis, as well as pain from the precipitating injury, however, it is not the most relevant finding.
4. Coordination relies on an intact neuromuscular system from the motor cortex to the spinal cord. Rhabdomyolysis involves direct damage to the muscle fibers and therefore would not impact coordination to the same extent as muscle performance.
A physical therapist treats a patient who has sustained a gunshot wound to the cervical spine causing an incomplete lesion to the spinal cord. The therapist examines the patient and determines that they no longer can sense pain signals on the right side of the body below the level of the lesion. Which part of the spinal cord was MOST likely affected?
1. Posterior spinal cord on the left
2. Anterior spinal cord on the left
3. Posterior spinal cord on the right
4. Anterior spinal cord on the right
Sensory information is carried to the brain via two ascending pathways: the anterolateral spinothalamic system and the dorsal column-medial lemniscal system. The anterolateral spinothalamic pathway carries nondiscriminative sensations such as pain, temperature, tickle, itch, and sexual sensations. The dorsal column-medial lemniscal pathway carries discriminative sensations such as discriminative touch, stereognosis, tactile pressure, barognosis, graphesthesia, kinesthesia, proprioception, and vibration.
1. The dorsal column-medial lemniscal pathway is located in the posterior portion of the spinal cord, therefore damage to this part of the spinal cord would cause a loss of transmission of the discriminative sensations, which do not include pain signals.
2. The anterolateral spinothalamic pathway is located in the anterolateral portion of the spinal cord, therefore damage to this part of the spinal cord would cause a loss of transmission of the nondiscriminative sensations, which include pain perception (i.e., sharp/dull discrimination). Because this pathway decussates at the level of the spinal cord, lesions to this tract will cause sensory impairments contralateral to the side of the lesion. Therefore, damage to the left side of the spinal cord will cause a loss of pain perception on the right side of the body below the level of the lesion.
3. As stated before, damage to the posterior spinal cord would affect the dorsal column-medial lemniscal pathway, and thus the discriminative sensations only.
4. Though the anterolateral spinothalamic pathway is located anteriorly in the spinal cord, damage to the right side of the spinal cord would cause sensory impairments on the left side of the body.
A physical therapist applies a Semmes-Weinstein monofilament to the sole of a patient’s foot. What monofilament description would indicate that the physical therapist is applying the monofilament correctly during the testing procedure?
1. The monofilament should deform into a “C” shape
2. The monofilament should remain perpendicular to the surface area
3. The monofilament should deform into a “S” shape
4. The monofilament should experience maximal deformation
Monofilament testing is a reliable method of assessing and documenting changes in protective sensation. Monofilament testing kits contain a variety of filament thicknesses which are applied perpendicular to the skin and held in place for approximately one second with enough force to bend the filament into a “C” shape.
1. Monofilaments should deform in a “C” shape. This procedure allows the therapist to know the amount of force, measured in grams. The most common monofilament sizes are 4.17, 5.07 and 6.10 gauge monofilament.
2. If the monofilament remains perpendicular to the surface of the skin it would be impossible to determine the amount of force applied to the patient’s skin by the monofilament.
3. The construction of the monofilament would not permit deforming in an “S” shape.
4. Maximal deformation would require greater force than the force required to bend the monofilament in a “C” shape. As a result, it would be impossible to determine the amount of force applied to the patient’s skin by the monofilament.
A physical therapist treats a patient with cerebellar pathology that exhibits dysdiadochokinesia. Which finding would be LEAST characteristic of this condition when attempting rapid supination and pronation of the forearms?
1. Inability to maintain rhythm
2. Failure to move through full range
3. Rapid onset of fatigue
4. Slowness of movement
Dysdiadochokinesia refers to the inability to perform rapid, alternating movements. This condition results in inappropriate timing of muscle firing and difficulty with cessation of ongoing movement. Common tests for dysdiadochokinesia include rapid supination and pronation of the forearms, alternating finger to nose, and altering the speed and direction of walking.
1. A patient with dysdiadochokinesia may be able to initially maintain rhythm when performing rapid pronation and supination of the forearms, however, this rhythm will quickly deteriorate as the patient has increasing difficulty modulating the movement.
2. A patient with dysdiadochokinesia may exhibit limited range of motion when performing rapid pronation and supination of the forearms in an attempt to successfully complete the activity. Limiting the range of motion decreases the complexity of the task and therefore it is often used as a compensatory strategy by patients with dysdiadochokinesia.
3. A patient with dysdiadochokinesia would not necessarily exhibit a rapid onset of fatigue when performing rapid pronation and supination of the forearms. The condition results from a failure to modulate movement due to the inappropriate timing of muscle firing and not due to muscle fatigue.
4. A patient with dysdiadochokinesia may exhibit slowness of movement when attempting rapid pronation and supination of the forearms in an attempt to successfully complete the activity. More rapid movement results in reduced rhythm, limited range of motion, and less ability to modulate the required sequential movement.
A physical therapist applies a therapeutic modality prior to manually stretching a patient’s plantar fascia. Which modality would be the MOST effective to improve the quality of the stretch?
1. Pulsed ultrasound
2. Moist heat
3. Iontophoresis
4. Ice massage
Numerous therapeutic modalities may be employed to improve both the quality and patient tolerance of a soft tissue stretch. The application of a tissue heating modality (e.g., continuous ultrasound, superficial moist heat) will most directly influence the viscoelasticity of the plantar fascia.
1. Pulsed ultrasound is unlikely to generate the necessary tissue heating required to increase the viscoelasticity of the plantar fascia.
2. Because of the superficial orientation of the plantar fascia, the application of moist heat prior to stretching interventions will positively impact viscoelasticity and improve the overall quality of the stretch.
3. Iontophoresis may be used to assist with pain management when treating plantar fasciitis, however, the intervention will not specifically impact viscoelasticity of the fascia.
4. Ice massage is frequently utilized to reduce the painful symptoms associated with plantar fasciitis, however, it is typically applied following manual interventions and will not improve the viscoelasticity of the fascia.
A physical therapist treats a patient with a pulmonary artery catheter inserted through the subclavian vein. Which range of motion exercise would MOST likely be restricted based on the presence of the catheter?
1. Shoulder flexion
2. Shoulder lateral rotation
3. Shoulder abduction
4. Shoulder extension
A pulmonary artery (Swan-Ganz) catheter is a soft, flexible catheter that is inserted through a vein into the pulmonary artery. The device is used to provide continuous measurements of pulmonary artery pressure. The patient should avoid excessive movement of the head, neck, and extremities to avoid disrupting the line at the insertion site.
1. The subclavian vein is typically accessed under the clavicle on the left side of the upper chest area. As a result, shoulder flexion is typically avoided since contraction of the anterior deltoid and pectoralis major tends to place additional pressure at the catheter’s insertion site.
2. Shoulder lateral rotation is not as likely to be restricted with a pulmonary artery catheter since the teres minor, infraspinatus, and posterior deltoid are not in the immediate area of the catheter’s insertion site.
3. Shoulder abduction is not as likely to be restricted with a pulmonary artery catheter since the middle deltoid and the supraspinatus are not in the immediate area of the catheter’s insertion site.
4. Shoulder extension is not as likely to be restricted with a pulmonary artery catheter since the latissimus dorsi, posterior deltoid, and teres major are not in the immediate area of the catheter’s insertion site.
2. A physical therapist examines a patient with complaints of hip pain. The therapist places the patient in prone and bends their knee to better evaluate the patient’s muscular flexibility. As the patient’s knee bends to end-range, they hike their hip off of the table. Shortening of which muscle would MOST likely be associated with this finding?
1. Iliopsoas
2. Vastus lateralis
3. Rectus femoris
4. Sartorius
Ely’s test is one of many special tests used to determine limitations in muscular flexibility. The testing procedure requires the patient to lie in a prone position while the therapist passively flexes the knee. The test is considered positive if there is limited knee flexion range of motion or if the patient hikes the hip off of the table.
1. The iliopsoas is a one-joint muscle that flexes the hip. Though prone positioning would place this muscle on stretch, knee movement would not affect the muscle’s length since the muscle does not cross the knee joint.
2. The vastus lateralis is a one-joint muscle that extends the knee. Though knee flexion would place this muscle on stretch, the patient would not hike their hip off of the table due to tightness of the muscle since it does not cross the hip joint.
3. The rectus femoris is a two-joint muscle that flexes the hip and extends the knee. The length of this muscle is commonly assessed using Ely’s test since this test places the leg in a position of hip extension and knee flexion, which would maximally stretch the muscle.
4. The sartorius is a two-joint muscle that flexes, laterally rotates, and abducts the hip and flexes the knee. Therefore, this muscle would be stretched in a position of hip extension and knee extension. Knee flexion would shorten the muscle and be unlikely to elicit the described response.
A physical therapist teaches a patient to utilize the Valsalva maneuver. Which medical condition would MOST benefit from this type of instruction?
1. Flaccid bladder
2. Congestive heart failure
3. Herniated lumbar disk
4. Peripheral vascular disease
The Valsalva maneuver is a technique characterized by a forcible exhalation with a closed glottis, nose, and mouth. The maneuver results in an increase in intra-thoracic and intra-abdominal pressure and a subsequent decrease in venous return and arterial blood pressure. When the breath is released, there is an exaggerated response to compensate for the drop in blood pressure via a marked increase in heart rate and blood pressure.
1. Flaccid bladder is a condition characterized by an inability of the detrusor muscles to contract when the bladder is full. The Valsalva maneuver causes an increase in intra-thoracic and intra-abdominal pressure and can be effectively used in these patients to assist with bladder emptying.
2. Congestive heart failure is a condition characterized by an inability of the heart to pump enough blood to meet the needs of the body. Due to the significant increase in blood pressure that occurs following the Valsalva maneuver, this technique should be avoided in patients with a cardiac impairment.
3. Herniated disk is a condition characterized by a tear in the outer, fibrous layer (i.e., annulus fibrosus) of the intervertebral disk which allows the inner, softer layer (i.e., nucleus pulposus) to bulge out. Because the Valsalva maneuver increases intrathoracic pressure, the patient’s symptoms could potentially be exacerbated due to the increased pressure on the intervertebral disk and/or spinal nerve.
4. Peripheral vascular disease is a condition characterized by obstruction of the large arterial vessels in the periphery. The use of the Valsalva maneuver would not be beneficial for a patient with peripheral vascular disease since it results in an increase in intra-thoracic and intra-abdominal pressure and a subsequent increase in arterial blood pressure.
A physical therapist identifies the presence of retained secretions in the lungs of a patient with pulmonary disease via auscultation. Which intervention would be the MOST effective to teach the patient to clear the retained secretions?
1. Pursed lip breathing
2. Active cycle of breathing
3. Segmental breathing
4. Inspiratory muscle training
Airway clearance techniques are manual or mechanical techniques used to facilitate clearance of secretions from the airways. These techniques include postural drainage, percussion, vibration, cough techniques, manual hyperinflation, and airway suctioning.
1. Pursed lip breathing is a breathing technique which requires the patient to inhale through the nose and exhale through pursed lips. This technique is used to decrease respiratory rate, increase tidal volume, relieve dyspnea, improve exercise tolerance, and prevent airway collapse. This technique is not used to help clear airway secretions.
2. Active cycle of breathing is a series of maneuvers used by the patient to help clear airway secretions. The maneuvers involve repeated diaphragmatic breathing and thoracic expansion exercises followed by a forced expiratory technique.
3. Segmental breathing (i.e., thoracic expansion exercise) is a technique used to improve regional ventilation in patients with pulmonary disease and to prevent and treat pulmonary complications after surgery. This technique is not used to help clear airway secretions.
4. Inspiratory muscle training is a technique used to increase the strength and endurance of the muscles of inspiration. With this technique, the patient uses a handheld breathing training device to provide resistance to inspiration. This technique is not used to help clear airway secretions.
A physical therapist reads in the medical record that an epidural sensor was used for intracranial monitoring on a patient with an acute head injury. Which unit of measure would MOST likely be utilized with this type of monitoring?
1. Milligrams per deciliter
2. Millimeters of mercury
3. Percent of oxygen saturation
4. Pounds per square inch
Intracranial monitoring is most often utilized on patients with a head injury, brain tumor, cerebral hemorrhage or overproduction of cerebrospinal fluid. An epidural sensor is one of three methods employed to measure the pressure exerted by the brain, blood, and cerebrospinal fluid against the inside of the skull. An epidural sensor is placed through a hole drilled in the skull and inserted between the skull and dural tissue. This type of intracranial monitoring tends to be less accurate than monitoring with an intraventricular catheter or subdural screw.
1. Selected laboratory values such as hematocrit are reported in milligrams per deciliter (mL/dL). Milligrams per deciliter is considered a unit of density.
2. An intracranial pressure monitor reports a value using millimeters of mercury (mm Hg). Normal intracranial pressure is 4-15 mm Hg, however, this value can fluctuate substantially based on patient activity.
3. Percent of oxygen saturation (SaO2) is obtained from an oximeter. The oximeter is usually attached to a patient’s ear or a finger and measures the pulse rate and the percentage of oxygen saturation within the patient’s blood.
4. Pounds per square inch (psi) is a measure of pressure resulting from a force of one pound applied to an area of one square inch. This unit of measure is not used when measuring intracranial pressure.
A physical therapist completes a work site analysis for a patient with T3 paraplegia. The patient is employed in the marketing department of an advertising agency and relies on a wheelchair for daily locomotion. Which of the following is likely to be the MOST significant architectural barrier for the patient?
1. Hardwood floors
2. An entrance ramp with one inch of vertical rise for every six inches of ramp length
3. One-quarter inch thresholds at each door
4. Pedestal type sinks
An entrance ramp that has one inch of vertical rise for every six inches of ramp length would not satisfy the 1:12 (rise:run) minimum ratio identified in the Americans with Disabilities Act (ADA).
1. Hardwood floors allow for easier propulsion, turning, and function with the wheelchair. Floor surfaces must be firm, stable, and slip resistant. A patient would expect increased difficulty using a wheelchair on carpet or outside terrain.
2. An entrance ramp designed with one inch of vertical rise for every six inches of ramp length would be twice as steep as the 1:12 (rise:run) minimum ratio. The 1:12 ratio allows for a maximum ramp grade of 8.3 percent.
3. A threshold of one-quarter inch is an acceptable height as a transition surface. Thresholds with beveled edges up to one-half inch are permissible.
4. Pedestal type sinks would not serve as an architectural barrier since the underside of the sink is open and allows for close wheelchair access. A sink encased with a vanity style cabinet would be more restrictive.
A physical therapist treats a patient diagnosed with a right hemispheric stroke. During the session the therapist instructs the patient to reach for an object with both hands. Which area of the brain is MOST responsible for performing the motor portion of this movement?
1. The prefrontal cortex in the frontal lobe
2. The precentral gyrus in the frontal lobe
3. The postcentral gyrus in the parietal lobe
4. The cingulate gyrus in the limbic lobe
Each hemisphere of the brain is divided into five distinct lobes: the frontal, parietal, temporal, occipital, and limbic lobes. Prominent sulci, such as the central sulcus, help to separate the different lobes. Each lobe of the brain is responsible for distinct brain functions.
1. The prefrontal cortex is located in the anterior portion of the frontal lobe and is responsible for the executive functions, which include memory, reasoning, planning, problem solving, and execution.
2. The precentral gyrus is located anterior to the central sulcus and is considered the primary motor cortex of the brain. It is involved in the initiation of voluntary movements, such as reaching towards an object with both hands.
3. The postcentral gyrus is located posterior to the central sulcus and is considered the primary somatosensory cortex of the brain. It is involved with the cortical processing of tactile and proprioceptive input.
4. The cingulate gyrus is located superior to the corpus callosum and constitutes a portion of the limbic lobe. The limbic lobe is responsible for emotional responses, drive-related behavior, and memory.
A physical therapist treats a 16-year-old male patient with an acute burn injury over his anterior chest. The wound contains dry, leathery eschar and is insensate to touch. Given the wound characteristics, what should be the PRIMARY goal of the therapist’s treatment?
1. Provide an environment which promotes re-epithelialization
2. Control infection to prepare the wound for surgical management
3. Debride blisters to prepare the wound for primary healing
4. Encourage the maintenance of a moist wound surface
Burn management will vary depending on the severity of the injury, which is often determined by the depth of the burn. Full-thickness burns involve damage to the entirety of the epidermis and dermis and are characterized by a dry, firm, leathery eschar which lacks pliability and is insensate to touch.
1. The goal of treatment for a superficial burn is to provide a wound environment which promotes re-epithelialization. This can be accomplished through the application of a moisturizing cream.
2. Full-thickness burns are generally treated in the operating room through surgical excision and skin grafting. Therefore, the goal of the therapist’s treatment is to prepare the wound for surgery by controlling infection. This can be accomplished through the use of antimicrobial topical agents and proper wound cleansing.
3. The goal of treatment for a partial-thickness burn is to prepare the wound for primary healing. This can be accomplished through wound cleansing and debridement of the larger, more fragile blisters.
4. The maintenance of a moist wound surface would be more important for the treatment of superficial and partial-thickness wounds since they heal without surgical intervention. Though maintaining a moist wound surface may be important for full-thickness burns, it does not take precedence over infection control.
A physical therapist treats a patient four weeks following a laminotomy due to impingement on a spinal nerve root. The therapist notices that that the patient’s arm houses a medical device as shown in the image. The medical record indicates that the patient is currently taking vancomycin. What is the MOST likely purpose of the medical device?
1. Administer pain medication to control pain
2. Deliver an antibiotic to combat infection
3. Administer electrical current to promote bone stimulation
4. Administer fluids to prevent dehydration
A laminotomy refers to the partial removal of a lamina. The lamina represents the flat portion of the vertebra originating from the pedicles of the vertebral body. The device shown in the image is a peripherally inserted central catheter (i.e., PICC) line. The device is inserted percutaneously at a peripheral site and extends to the superior vena cava. Vancomycin is an antibiotic used to treat a broad range of bacterial infections.
1. Pain medications to control pain following surgery are most often administered orally or through a traditional intravenous line.
2. A PICC line is often used to deliver antibiotics to combat infection. This type of device is particularly desirable when intravenous medications are administered for a prolonged period of time. The PICC line limits the exposure of distal venous regions to the caustic effects of powerful antibiotic medications and reduces the need for repetitive needle punctures. Other common uses of PICC lines include long chemotherapy regimens or total parenteral nutrition.
3. Bone stimulators utilize pulsed electromagnetic or pulsed low intensity ultrasonic energy to promote bone growth. They are often secured by straps to the affected body part.
4. Fluids to prevent dehydration are most often administered using a traditional intravenous line.
A physical therapist is treating a 45-year-old male who sustained a traumatic injury to his right shoulder while playing basketball one week ago. The patient presents with pain, inflammation, and muscle spasm globally in the shoulder. What is the MOST appropriate intervention?
1. Grade I and II joint mobilizations
2. Bent over rows with a light handweight
3. Doorway stretches for the pectoralis major
4. Proprioceptive neuromuscular facilitation patterns without resistance
The acute stage of healing is characterized by inflammation, pain, edema, muscle spasm, impaired movement, joint effusion, and decreased use of affected areas. The plan of care for this stage of healing should include patient education, control of pain, reduction of muscle spasm, maintenance of joint mobility, reduction of swelling, and maintenance of the function of associated areas.
1. The patient presents with pain, inflammation, and muscle spasm. The most appropriate intervention would be grade I and II joint mobilizations to help control pain by stimulating mechanoreceptors.
2. Bent over rows with a light handweight would be more appropriate for the subacute stage of healing. Strengthening exercises used during the acute stage will likely exacerbate the patient’s symptoms.
3. Doorway stretches for the pectoralis major would be more appropriate for the subacute stage of healing. Stretching exercises used during the acute stage will likely exacerbate the patient’s symptoms. More conservative activities such as pain-free passive range of motion would be more appropriate for the acute stage.
4. Proprioceptive neuromuscular facilitation patterns would be more appropriate for the subacute stage of healing. Active range of motion (AROM) exercises at the site of injury used during the acute stage will likely exacerbate the patient’s symptoms. AROM exercises used at adjacent joints would be an acceptable intervention for the acute stage.
A physical therapist applies a transparent film dressing to a superficial wound on a patient’s lower leg. Which therapeutic objective is LEAST likely based on the type of dressing?
1. Permit autolytic debridement
2. Prohibit entry of bacteria
3. Absorb drainage in the wound bed
4. Reduce friction over bony prominences
Transparent film dressings are thin membranes made from transparent polyurethane with water-resistant adhesives. They are highly elastic, conform to a variety of body contours, and allow for easy visual inspection of the wound since they are transparent.
1. Autolytic debridement refers to the use of the body’s own mechanisms to remove nonviable tissue. Common methods of autolytic debridement include the use of transparent films, hydrocolloids, hydrogels, and alginates. The transparent film helps to establish a moist wound environment that rehydrates necrotic tissue and eschar, facilitating enzymatic digestion of the nonviable tissue.
2. Transparent film dressings are permeable to vapor and oxygen, but are largely impermeable to bacteria and water.
3. Transparent film dressings are nonabsorbent and are therefore not indicated in the presence of significant drainage. Other dressings more appropriate to absorb drainage include alginates and hydrocolloids.
4. Transparent film dressings reduce friction over bony prominences. The dressings form a barrier between the wound bed and therefore serve to resist shearing and frictional forces.
A physical therapist assesses the muscle activity of a patient ambulating on a level surface using electromyography. Which muscle would likely possess the MOST sustained activity throughout the swing phase of gait?
1. Tibialis anterior
2. Gluteus medius
3. Adductor longus
4. Soleus
1. The tibialis anterior is primarily responsible for ankle dorsiflexion and inversion. This muscle sustains its motor activity from toe off through the entire swing phase ending with initial contact. The muscle also continues to be active through the initial portion of the stance phase from initial contact through foot flat.
2. The gluteus medius is primarily responsible for hip abduction and medial rotation. This muscle is active just prior to initial contact and remains active through the first half of the stance phase.
3. The adductor longus is primarily responsible for hip adduction. This muscle is active during the terminal portion of stance phase and remains active through the first half of the swing phase.
4. The soleus is primarily responsible for ankle plantar flexion. This muscle is active for approximately 40% of the stance phase. The muscle becomes active after foot flat and becomes inactive prior to toe off.
A physical therapist treats a patient that has experienced altered serum potassium levels during their current hospitalization. What is the MOST relevant complication for a patient with abnormal potassium levels?
1. Cardiac arrhythmias
2. Water retention
3. Increased blood glucose level
4. Increased oxygen saturation in the blood
Potassium is important for the function of excitable cells such as the heart, nerve, and muscle. Hypokalemia (low serum potassium) or hyperkalemia (high serum potassium) will both place the patient at risk for cardiac arrhythmias. In addition to arrhythmias, potassium imbalance also can produce tetany, muscle weakness, cardiac arrest, muscle pH imbalance, and decreased action potentials.
1. Potassium is an electrolyte found inside cells with normal blood values ranging from 3.5-5.0 mEq/L for an adult. The heart muscle is most susceptible to potassium disturbances with subsequent potential for cardiac arrhythmias or cardiac arrest. Given the alteration in serum potassium levels, the therapist should assess heart rate for a minimum of 60 seconds to ensure that arrhythmias are not present.
2. Water retention would be a predictable complication from an increase in sodium within the blood. Potassium, however, actually assists with decreasing water retention and counters the effects of excessive sodium in the blood stream.
3. Increased blood glucose levels would be a predictable complication from either a decrease in circulating insulin within the blood stream or from ingesting high levels of glucose. A patient with diabetes mellitus is at high risk for significant fluctuation in blood glucose outside of the normal range of 70-110 mg/dl.
4. Increased oxygen saturation is not typically a complication of an electrolyte or blood level imbalance. A patient may exhibit decreased oxygen saturation, however, this is due to ventilatory exchange impairments. Normal oxygen saturation should range from 95-100%.
A physical therapist works with a patient on ascending and descending a ramp in the physical therapy gym. The patient is a 72-year-old female who recently fractured her left tibial plateau and, as a result, is using bilateral axillary crutches. When descending the ramp, where should the therapist stand?
1. In front of the patient toward the right side
2. In front of the patient toward the left side
3. Behind the patient toward the right side
4. Behind the patient toward the left side
Ascending and descending a ramp can be safely performed using axillary crutches, however, a therapist must carefully guard the patient during training.
1. Standing in front of the patient is desirable when descending the ramp, however, the therapist should guard the patient toward the involved side (left side).
2. Standing in front of the patient toward the involved side (left side) is the most desirable position to guard the patient when descending the ramp.
3. The patient is most likely to experience a forward loss of balance when descending a ramp and therefore it is more desirable for the therapist to be positioned in front of the patient. The therapist should guard the patient toward the involved side (left side).
4. The therapist is positioned on the involved side (left side), however, the therapist should also be positioned in front of the patient.
A physician utilizes diagnostic imaging to show motion within a joint through x-ray. What is this type of imaging BEST termed?
1. Computed tomography
2. Fluoroscopy
3. Discography
4. Radionuclide scanning
. Computed tomography is a non-invasive imaging technique that uses cross-sectional images based on x-ray attenuation. Computer enhancement allows the imaging to have significantly better contrast resolution when compared to conventional x-rays.
2. Fluoroscopy refers to examination by means of the fluoroscope. A fluoroscope allows an examiner to observe the actions of joints, organs or entire systems of the body. The instrument requires a specific body segment to be placed between a fluorescent screen and an x-ray tube. X-rays from the tube pass through the body and project images on the screen.
3. Discography is an invasive imaging technique that involves injecting a radiopaque dye into the nucleus pulposus of an intervertebral disc using radiographic guidance. The technique can be used to identify disruptions of the nucleus pulposus or the annulus fibrosus.
4. Radionuclide scanning is an invasive imaging technique that can be used in conjunction with bone scans to identify areas where there is a high level of bone turnover relative to the rest of the bone. The technique requires the intravenous injection of chemicals labeled with isotopes.
A mother indicates that her four-year-old son was diagnosed with a disease during a newborn screening test administered shortly after birth. However, due to the early identification of the disease, the child's condition was effectively treated without any residual impairments. Which medical condition is MOST consistent with the described scenario?
1. Spina bifida
2. Down syndrome
3. Phenylketonuria
4. Tay-Sachs disease
1. Spina bifida is a developmental abnormality due to insufficient closure of the neural tube by the 28th day of gestation. This defect usually occurs in the low thoracic, lumbar or sacral regions. Symptoms are highly variable by type: occulta, meningocele, and myelomeningocele. Spina bifida is detected in utero through blood test and fetal ultrasound. After birth, the condition is confirmed with x-ray, MRI or CT scan. Early identification of spina bifida will not alleviate the residual impairments.
2. Down syndrome (trisomy 21) is a genetic abnormality consisting of an extra twenty-first chromosome due to an error in cell division. Symptoms of this syndrome include intellectual disability, hypotonia, joint hypermobility, flattened nasal bridge, narrow eyelids with epicanthal folds, flat feet, scoliosis, congenital heart disease, and visual and hearing loss. Down syndrome is detected in utero through a combination of tests that may include blood test, fetal ultrasound, and amniocentesis. After birth, the condition is confirmed with a chromosomal karyotype. Early identification of Down syndrome will not alleviate the residual impairments.
3. Phenylketonuria is an autosomal recessive condition in which a mutation occurs in a gene responsible for breaking down the amino acid phenylalanine. Symptoms will typically present within a few months of birth as the phenylalanine accumulates. If left untreated, severe intellectual disability will occur. Phenylketonuria is treated through dietary restriction of phenylalanine throughout the person's lifetime. Adequate prevention will avoid all manifestations of the disease. Phenylketonuria is detected through a required screening for all newborns. If the initial screening is positive, further blood and urine tests are required to confirm the diagnosis.
4. Tay-Sachs disease is an autosomal recessive inherited trait characterized by the absence or deficiency of hexosaminidase A. At approximately six months of age, the child will start to miss developmental milestones and will continue to deteriorate in motor and cognitive skills. As symptoms progress, the patient develops significant intellectual disability and paralysis, and will usually die by the age of five. Tay-Sachs disease is typically carried out when both parents cannot be ruled out as carriers. The disease is detected in utero through a combination of tests that may include detecting hexosaminidase A, chorionic villus sampling, and amniocentesis.
A physical therapist performs pulmonary function testing on an otherwise healthy 80-year-old male status post humeral fracture. Which pulmonary value would the physical therapist expect to remain MOST stable over the patient’s lifespan?
1. Tidal volume
2. Residual volume
3. Forced vital capacity
4. Inspiratory capacity
1. Tidal volume, or the amount of air in a normal resting breath, tends to remain stable over time. Typically, tidal volume is 500 mL (i.e., half of a liter).
2. As a result of the aging process, residual volume can increase by 30-50% due to the loss of alveoli and increasing stiffness of the rib cage.
3. As a result of the aging process, forced vital capacity can decrease by 40-50% due to the loss of alveoli and increasing stiffness of the rib cage. Forced vital capacity includes the inspiratory reserve volume, expiratory reserve volume, and tidal volume.
4. Inspiratory capacity is the combination of inspiratory reserve volume and tidal volume. As a result of the aging process, there is a decrease in the inspiratory reserve volume resulting in a decreased inspiratory capacity.
A physical therapist administers a special test to a patient with a lower extremity injury. Which special test would NOT be initiated with the patient in prone and the knee flexed to 90 degrees?
1. Apley’s test
2. Craig’s test
3. Peroneal tendon dislocation test
4. Thompson test
1. Apley’s test is performed with the patient positioned in prone with the test knee flexed to 90 degrees. The therapist stabilizes the patient’s femur using one hand and places the other hand on the patient’s heel. The therapist medially and laterally rotates the tibia while applying a compressive force through the tibia. A positive test is indicated by pain or clicking and may be indicative of a meniscal lesion.
2. Craig’s test is performed with the patient positioned in prone with the test knee flexed to 90 degrees. The therapist palpates the posterior aspect of the greater trochanter and medially and laterally rotates the hip until the greater trochanter is parallel with the table. The degree of femoral anteversion corresponds to the angle formed by the lower leg with the perpendicular axis of the table. Normal anteversion for an adult is 8-15 degrees.
3. The peroneal tendon dislocation test is performed with the patient in prone with the knee flexed to 90 degrees. The patient is asked to actively dorsiflex and plantar flex the ankle along with eversion against the therapist’s resistance. If the tendon subluxes from behind the lateral malleolus, the test is considered positive. The test can also be performed with the patient in prone, although is classically performed with the patient in prone with the knee flexed to 90 degrees.
4. The Thompson test is performed with the patient positioned in prone with the feet extended over the edge of a table. The therapist asks the patient to relax and proceeds to squeeze the muscle belly of the gastrocnemius and soleus muscles. A positive test is indicated by the absence of plantar flexion and may be indicative of a ruptured Achilles tendon.
A physical therapist comes into the clinic in the morning and notices that the hot pack machine was unplugged overnight. Which guideline would be the MOST appropriate after plugging in the hot pack unit?
1. Wait to use a hot pack for a minimum of one hour
2. Wait to use a hot pack until the following day
3. Wait to use a hot pack until the water in the unit reaches 160 degrees Fahrenheit
4. Wait to use a hot pack until the unit is formally inspected by a qualified individual
1. Waiting a minimum of one hour to use the hot pack would be an insufficient amount of time for the water in the hot pack unit to reach the necessary temperature. As a result, the hot pack would not be able to deliver the necessary amount of heat to accomplish the therapeutic objective.
2. Waiting until the following day would likely be unnecessary since typically a hot pack unit will reach the necessary temperature (158 and 167 degrees Fahrenheit) within a two hour period.
3. Waiting until the hot pack unit reaches the necessary temperature would best signify that the hot pack possesses the appropriate amount of heat. The amount of time needed to reach this temperature will be somewhat variable based on the intrinsic properties of each hot pack unit and therefore the temperature of the water offers the best guideline.
4. The current unavailability of the hot pack unit resulted from the device being unplugged. As a result, inspection of the unit by a qualified individual would not be necessary prior to using a hot pack.
A therapist measures a patient’s blood pressure at the beginning of a therapy visit and notes that the resting blood pressure is significantly lower than normal. What is the MOST logical explanation for this objective finding?
1. The therapist used a blood pressure cuff that is too small
2. The patient exercised just prior to the therapy visit
3. The therapist took the measurement with the patient’s arm at their side while seated
4. The patient has been nauseous and vomiting over the past two days
1. The blood pressure cuff must be the proper size to obtain an accurate measurement. A blood pressure cuff that is too narrow in relation to the patient’s arm circumference will result in a reading that is inaccurately high.
2. Exercise results in an increase in systolic blood pressure. Blood pressure should drop to its normal resting value within three to five minutes after termination of exercise. Though more than five minutes has likely elapsed between the patient’s physical activity and the therapy visit, the recent exercise would not result in a decrease in blood pressure.
3. Arm positioning may affect a blood pressure reading. When sitting or standing, the patient’s arm should be resting at the level of the fourth intercostal space. Having the arm below this position (e.g., at the patient’s side) would result in an increase in the blood pressure value.
4. The patient is likely dehydrated from vomiting over the course of the past two days. Dehydration (i.e., low blood volume) results in a decrease in resting blood pressure.
A physical therapist treats a patient that presents with a chronic inflammatory disorder limited to the mucosa and submucosa layers of the colon and rectum. A chart review reveals that the affected area is restricted to the colon and presents as a continuous lesion with involvement of the inner lining progressing to the rectum. The patient experiences chronic diarrhea and rectal bleeding. Which medical condition is MOST consistent with the described scenario?
1. Crohn’s disease
2. Irritable bowel syndrome
3. Ulcerative colitis
4. Transmural inflammatory disease
1. Crohn’s disease is a form of inflammatory bowel disease with a chronic and unpredictable course. It typically affects all layers of the intestinal wall and is characterized by diseased areas separated by normal, unaffected tissue (unlike ulcerative colitis that presents with continuous, uniform involvement of only the mucosa and submucosa layers). Crohn’s disease can affect any segment of the intestinal tract, unlike ulcerative colitis that is restricted to the colon and rectum. Fissures and fistulas are also common with Crohn’s disease.
2. Irritable bowel syndrome (IBS) refers to a chronic condition that is non-inflammatory and can occur anywhere within the intestines. IBS is characterized by abnormal intestinal contractions and an exaggerated gastrocolic reflex resulting from impaired motility, stress, visceral hypersensitivity, and abnormal processing of the nervous system.
3. Ulcerative colitis can occur at any age but is most common between 10 to 40 years of age. Inflammation of the mucosa results in small erosions and subsequent ulceration. Diarrhea is often severe and chronic, however, unlike Crohn’s disease, ulcerative colitis does not present with fissures or fistulas.
4. Transmural inflammatory disease is characterized by inflammation that encompasses all layers of the intestinal wall. This inflammatory process is discontinuous where inflamed areas are separated by normal, unaffected tissue.
A physical therapist works on improving the range of motion of a patient four weeks after total hip arthroplasty using a posterolateral approach. The patient is having difficulty reaching their feet to don and doff their shoes independently. Which of the following motions should be emphasized to achieve improved independence with this skill?
1. Hip flexion
2. Hip medial rotation
3. Knee extension
4. Hip lateral rotation
A total hip arthroplasty is performed as a result of progressive and severe osteoarthritis or other hip pathology that produces pain and disability. A posterolateral approach leaves the abductor muscles intact, however, it penetrates the posterior capsule resulting in post-operative joint instability. In order to prevent dislocation of the femoral head component, the patient should avoid excessive hip flexion greater than 90 degrees, hip adduction, and hip medial rotation.
1. Hip flexion should be avoided at angles greater than 90 degrees since this results in stress on the weakened posterior capsule of the hip joint and increases the risk for hip dislocation. This patient should not bend over in a sitting position to don and doff their shoes since this would increase hip flexion past 90 degrees.
2. Hip medial rotation should be avoided since this motion places stress on the weakened posterior capsule and results in the femoral head component assuming a position where it may dislocate. Hip medial rotation would not assist this patient to independently don and doff their shoes.
3. Knee extension is not a precaution for this patient, however, if the knee was extended the patient would have to flex the hip greater than 90 degrees to reach their feet.
4. Hip lateral rotation places the femoral head component in a stable position following a posterolateral approach. Improved range of motion into lateral rotation should be emphasized in order to maximize function for this patient. The patient can laterally rotate their hip and place their foot on their opposite knee with the hip flexed less than 90 degrees in order to safely don and doff their shoes.
A physical therapist administers the slump test to a patient being treated in physical therapy with low back pain. The patient notes pain in the posterior knee when the knee is extended and ankle is dorsiflexed. The therapist then has the patient slump and flex their neck while plantar flexing the ankle. The patient indicates that this positional change makes the pain disappear. What can the therapist conclude from this test?
1. The patient has tight musculature in the posterior leg
2. The patient is experiencing neural tension of the sciatic nerve
3. The patient has a lumbar disk herniation
4. The patient is likely malingering
The slump test is a neural provocation test performed with the patient in sitting. It consists of a series of progressive active and passive movements including cervical flexion, trunk flexion, knee extension, and ankle dorsiflexion. With each movement, the therapist asks the patient if they are experiencing symptoms (e.g., radicular pain, numbness, tingling). If symptoms are not produced, the therapist proceeds to the next movement to increase the amount of dural stretch.
1. Having the knee extended and ankle dorsiflexed would increase dural stretch on the sciatic nerve, though this position would also place stretch on the posterior musculature of the leg (i.e., hamstrings and calf muscles). Having the patient plantar flex the ankle would release the tension/stretch on all of these structures, though having the patient slump and flex the neck would increase the tension on the nerve without increasing the stretch on the muscles. Because this resulted in a decrease in the patient’s pain, the original pain can likely be attributed to tight musculature.
2. The position of knee extension and ankle dorsiflexion would increase tension on the sciatic nerve. By plantar flexing the ankle, tension would be decreased, though slumping and flexing the neck would counteract this decrease in tension and maintain dural stretch. Because the patient reported a decrease in symptoms, it is unlikely that they were experiencing tension on the sciatic nerve with the original test position.
3. The slump test is not necessarily designed to diagnose the exact cause of the patient’s symptoms, though disk herniation is one of the possible causes. As stated previously, the patient is more likely experiencing symptoms related to muscular tension as opposed to neural tension.
4. The slump test is not typically used to determine the presence of malingering and there is no information in the scenario that would lead one to believe that the patient is malingering. The described position would lead to an increase in the stretch on the posterior musculature of the leg and would explain the patient’s reported pain.
A physical therapist measures the blood pressure of a patient sitting upright over the edge of a plinth. Based on the presented image, what is the GREATEST source of measurement error?
1. Positioning of the upper extremity
2. Positioning of the sphygmomanometer
3. Positioning of the diaphragm of the stethoscope
4. Positioning of the inflation bulb
Accurately measuring blood pressure is a critical skill for physical therapists. There are many factors that can influence a blood pressure reading including the position of the patient, size of the sphygmomanometer, amount of pressure used to occlude the artery, the rate of pressure release, and placement of the sphygmomanometer.
1. Blood pressure readings can vary as much as 20 mm Hg by altering the position of the upper extremity. Ideally, the patient should be placed in sitting with the arm in a relative horizontal supported position at the level of the heart. This patient’s position depicted in the image would allow for an accurate blood pressure measurement.
2. The sphygmomanometer (i.e., blood pressure cuff) appears to correctly fit the circumference of the patient’s arm and is positioned appropriately at one and one-half fingers width above the antecubital fossa.
3. The diaphragm of the stethoscope should be placed over the brachial artery’s pulse point in order to auscultate Korotkoff’s sounds. The brachial artery pulse point is located slightly above and medial to the antecubital fossa. The presented image shows the diaphragm placed well below the antecubital fossa and below the pulse point of the brachial artery. The position of the diaphragm would make it extremely difficult to accurately complete the blood pressure measurement.
4. The inflation bulb that is attached to the sphygmomanometer pumps air into the bladder of the cuff. The accuracy of the blood pressure measurement is not influenced by the position of the inflation bulb.
A physical therapist prepares to select a dressing for a patient with a lower extremity arterial insufficiency ulcer. The wound measures two centimeters in diameter with a depth of one-half centimeter. Considering the typical characteristics of an arterial insufficiency ulcer, which dressing would be the MOST desirable to maintain an appropriate moisture balance in the wound bed?
1. Hydrogel
2. Transparent film
3. Wet-to-dry gauze
4. Calcium alginate
1. A hydrogel is a moisture retentive primary dressing that provides a moist environment for wound healing. An arterial insufficiency ulcer typically produces minimal drainage, therefore the use of a hydrogel is appropriate to assist in preventing the wound from dehydrating and impeding the healing process.
2. A transparent film dressing may assist in maintaining a moist wound environment with a minimally draining wound, however, this dressing is typically recommended for superficial partial-thickness wounds that will heal by primary intention. A wound with the dimensions described would be considered a full-thickness wound that will require intervention to heal by secondary intention.
3. A wet-to-dry gauze dressing provides some moisture to the wound bed on initial application, however, as the dressing dries, the wound bed will typically dehydrate. This inconsistency in wound bed moisture balance is undesirable and typically impedes wound healing.
4. A calcium alginate dressing is highly absorptive and is typically utilized with wounds that produce moderate to heavy exudate. A wound producing minimal exudate is unlikely to saturate the alginate to the extent necessary for it to form a beneficial hydrophilic gel.
Setting: Outpatient rehabilitation
Gender: Male
Age: 74 years
Presenting Problem/Current Condition
Right hemisphere stroke
Medical History
Transient ischemic attack
Diabetes
Other Information
Lives with spouse in a retirement community
Physical Therapy Examination(s)
Left neglect and diminished proprioception
Ambulates with a large base quad cane
Difficulty focusing and frequently perseverates
Spasticity assessment: left upper extremity can still be easily moved throughout the range of motion despite marked tone
Cognition assessment: Unable to count from one to twenty-five by increments of three
Physical Therapy Plan of Care
Formal cognitive assessment
Balance training
Fall prevention
Maximize independence with ADLs
Discharge planning
Which of the following actions is the MOST appropriate to ensure patient safety when walking?
1. Provide continuous verbal cues
2. Utilize visual cues and demonstration
3. Provide manual assistance on the left side
4. Provide manual assistance on the right side
A physical therapist must carefully consider a patient’s current limitations and identify remedial strategies to assist the patient to achieve established goals. The presence of left neglect and diminished proprioception requires the therapist to take formal action to avoid jeopardizing patient safety.
1. Verbal cues may be beneficial for the patient. However, without concurrent manual assistance, the patient would likely still have increased difficulty with ambulation and may be at increased risk for a fall.
2. Visual cues and demonstration prior to practice are important. However, this type of educational strategy would not directly address the left neglect and diminished proprioception.
3. The physical therapist should offer manual assistance on the patient’s left side during ambulation activities. The manual assistance can facilitate motor activity and weight bearing, as well as proprioception on the affected side. Manual contact significantly reduces the risk of fall or injury.
4. The patient presents with left neglect. As a result, manual assistance would not typically be necessary on the right side of the body.
Setting: Outpatient rehabilitation
Gender: Male
Age: 74 years
Presenting Problem/Current Condition
Right hemisphere stroke
Medical History
Transient ischemic attack
Diabetes
Other Information
Lives with spouse in a retirement community
Physical Therapy Examination(s)
Left neglect and diminished proprioception
Ambulates with a large base quad cane
Difficulty focusing and frequently perseverates
Spasticity assessment: left upper extremity can still be easily moved throughout the range of motion despite marked tone
Cognition assessment: Unable to count from one to twenty-five by increments of three
Physical Therapy Plan of Care
Formal cognitive assessment
Balance training
Fall prevention
Maximize independence with ADLs
Discharge planning
Which of the following would likely be utilized when conducting a spasticity assessment?
1. Strength testing
2. Deep tendon reflex testing
3. Active range of motion
4. Passive range of motion
Spasticity is a condition in which there is an abnormal increase in muscle tone or stiffness of muscle, which often interferes with movement. Spasticity is usually caused by damage to nerve pathways within the brain or spinal cord that control muscular movement. The Modified Ashworth Scale (MAS) is an instrument that is used to assess muscle spasticity. The MAS uses ordinal scoring, with a grade of “0” indicating the absence of spasticity and a grade of “4” indicating the presence of rigidity.
1. Strength testing may be used for patients who have had a stroke to determine which muscles have been affected as a result of the neurological damage. However, strength testing would not provide valuable information to assess spasticity, which requires a passive assessment.
2. Deep tendon reflex testing may be used for patients who have had a stroke to determine if the patient has hyporeflexia or hyperreflexia as a result of the neurological damage. However, deep tendon reflex testing would not provide valuable information to assess spasticity, which requires a passive assessment.
3. Active range of motion may be used for patients who have had a stroke to determine the patient’s functional use of their extremities. However, active range of motion would not provide valuable information to assess spasticity, which requires a passive assessment.
4. The MAS is an assessment tool that is used to grade spasticity. Spasticity refers to an increased resistance to passive stretch that is velocity-dependent. Therefore, passive range of motion would be the most appropriate method for measuring spasticity.
Setting: Outpatient rehabilitation
Gender: Male
Age: 74 years
Presenting Problem/Current Condition
Right hemisphere stroke
Medical History
Transient ischemic attack
Diabetes
Other Information
Lives with spouse in a retirement community
Physical Therapy Examination(s)
Left neglect and diminished proprioception
Ambulates with a large base quad cane
Difficulty focusing and frequently perseverates
Spasticity assessment: left upper extremity can still be easily moved throughout the range of motion despite marked tone
Cognition assessment: Unable to count from one to twenty-five by increments of three
Physical Therapy Plan of Care
Formal cognitive assessment
Balance training
Fall prevention
Maximize independence with ADLs
Discharge planning
Using the Modified Ashworth Scale, which grade of spasticity would be the MOST accurate for this patient?
1. 1
2. 1+
3. 2
4. 3
The Modified Ashworth Scale (MAS) is an instrument that is used to assess muscle spasticity. The MAS uses ordinal scoring, with a grade of “0” indicating the absence of spasticity and a grade of “4” indicating the presence of rigidity.
1. A grade of “1” on the MAS is described as a slight increase in tone. This increase in tone may manifest as a “catch and release” or may be characterized by an increase in tone at the end of the range of motion.
2. A grade of “1+” on the MAS is described as a slight increase in tone. This grade differs from a grade of “1” in that the “catch” is followed by minimal resistance throughout the rest of the range of motion, which is usually less than half of the total range.
3. A grade of “2” on the MAS is described as a marked increase in tone throughout most of the range of motion. Despite the increase in tone, the affected part can still be easily moved through the range of motion.
4. A grade of “3” on the MAS is described as a considerable increase in tone. This grade differs from the previous grade in that the affected part is not easily moved through the range of motion.
Setting: Outpatient rehabilitation
Gender: Male
Age: 74 years
Presenting Problem/Current Condition
Right hemisphere stroke
Medical History
Transient ischemic attack
Diabetes
Other Information
Lives with spouse in a retirement community
Physical Therapy Examination(s)
Left neglect and diminished proprioception
Ambulates with a large base quad cane
Difficulty focusing and frequently perseverates
Spasticity assessment: left upper extremity can still be easily moved throughout the range of motion despite marked tone
Cognition assessment: Unable to count from one to twenty-five by increments of three
Physical Therapy Plan of Care
Formal cognitive assessment
Balance training
Fall prevention
Maximize independence with ADLs
Discharge planning
Which cognitive function was documented as being problematic for this patient?
1. Attention
2. Constructional ability
3. Abstract ability
4. Orientation
Attention is defined as the capacity of the brain to process information from the environment or from long-term memory. The complexity and familiarity of the task determines the degree of attention required to complete the task.
1. Attention can be assessed by asking a patient to count from one to twenty- five by increments of three. The task should be relatively easy for most individuals. However, it requires the person to exert a sustained, consistent effort. Attention deficits are common with many neurological disorders, including brain injury, stroke, and dementia.
2. Constructional ability can be assessed by asking a person to copy figures consisting of varying sizes and shapes or to draw a known item, such as a clock.
3. Abstract ability can be assessed by asking a person to interpret a common proverb or to describe similarities or differences between two objects.
4. Orientation can be assessed by asking a person to identify time (e.g., day, month, season), person (e.g., name), and place (e.g., city, state).
Setting: Outpatient rehabilitation
Gender: Male
Age: 74 years
Presenting Problem/Current Condition
Right hemisphere stroke
Medical History
Transient ischemic attack
Diabetes
Other Information
Lives with spouse in a retirement community
Physical Therapy Examination(s)
Left neglect and diminished proprioception
Ambulates with a large base quad cane
Difficulty focusing and frequently perseverates
Spasticity assessment: left upper extremity can still be easily moved throughout the range of motion despite marked tone
Cognition assessment: Unable to count from one to twenty-five by increments of three
Physical Therapy Plan of Care
Formal cognitive assessment
Balance training
Fall prevention
Maximize independence with ADLs
Discharge planning
Which physical therapist action would be the MOST effective to refocus the patient during periods of perseveration?
1. Focus on the topic of perseveration for a short period of time in order to appease the patient
2. Guide the patient into an interesting new activity and reward successful completion of the task
3. Take the patient back to their room for quiet time and attempt to resume therapy once they have stopped perseverating
4. Continue with repetitive verbal cues to cease perseveration
Perseveration is the continued repetition of a word, phrase or movement. Patients with a lesion in the premotor or prefrontal cortex often exhibit perseveration.
1. It is not necessary to attempt to appease the patient since the patient cannot independently move beyond whatever they are perseverating on. Staying with the topic will not assist in moving forward.
2. Since the patient typically continues the repetition of a word, phrase or movement after the cessation of the original stimulus, the best intervention would be to redirect the patient away from the current activity.
3. The patient will not benefit from “quiet time” since the patient is not perseverating due to a behavioral issue. Redirecting the patient may successfully allow the patient to move forward and continue with therapy without interruption.
4. Verbal cueing is not an effective technique to cease perseveration. The patient typically requires a redirection of their attention to another activity or environment.
A physical therapist working in a neonatal intensive care unit reviews a patient’s medical record and observes that the infant’s APGAR score was recorded as 7 and 9 for the first and fifth minutes, respectively. Which observation would warrant a score of less than 2 in its respective category?
1. The infant is crying
2. The infant’s heart rate is 85 beats per minute
3. The infant is actively moving their arms and legs
4. The infant sneezes
The APGAR scale is a scoring system used to evaluate the physical condition of a newborn infant after delivery. Each of the five signs (i.e., heart rate, respiratory effort, muscle tone, reflex irritability, color) is scored on a 0-2 scale for a total possible score of 10 points. Scores are usually reported in the first and fifth minutes after delivery. A score of 8-10 is considered normal indicating that the infant does not require resuscitation.
1. The infant crying is an indication of a good respiratory effort and would receive a score of 2. A slow, irregular respiratory effort would receive a score of 1, while the absence of breathing would receive a score of 0.
2. A heart rate less than 100 beats per minute would receive a score of 1. A heart rate greater than 100 beats per minute would receive a score of 2, while the absence of a heart rate would receive a score of 0.
3. Active movement of the arms and legs is an indication of muscle tone and would receive a score of 2. Some flexion of the extremities would receive a score of 1, while limp or flaccid appearing extremities would receive a score of 0.
4. The infant sneezing in response to stimulation (e.g., suctioning with a syringe after delivery to clear the airway) is an indication of reflex irritability and would receive a score of 2. A grimace would receive a score of 1 and no response would receive a score of 0.
A physical therapist uses therapeutic ultrasound for deep heating of the left piriformis muscle prior to soft tissue mobilization and stretching. Which of the following would be the MOST appropriate treatment parameters?
1. 3 MHz, 1.0 W/cm2, 100% duty cycle, for 12 minutes
2. 1 MHz, 1.0 W/cm2, 100% duty cycle, for 12 minutes
3. 3 MHz, 1.5 W/cm2, 100% duty cycle, for 8 minutes
4. 1 MHz, 1.5 W/cm2, 100% duty cycle, for 8 minutes
A physical therapist should be able to select specific therapeutic modality parameters based on the desired therapeutic outcome. Parameters of ultrasound include the frequency, duty cycle, intensity, and duration. A 100% duty cycle (i.e., continuous ultrasound) is used when the treatment objective is to heat the tissue.
1. The frequency of ultrasound is chosen based on the depth of tissue to be treated. The piriformis is a relatively deep structure and therefore a frequency of 1 MHz should be used. Additionally, 12 minutes is more time than is needed to sonate over the piriformis muscle.
2. A frequency of 1 MHz should be used since the piriformis is a deep structure. However, when using 1 MHz, the intensity needs to be between 1.5 and 2.0 W/cm2 to produce tissue heating. Additionally, 12 minutes is more time than is needed to sonate over the piriformis muscle.
3. When using ultrasound, an area twice the size of the sound head can be effectively treated in a 5 minute period. As a result, 8 minutes would be adequate to sonate over the piriformis muscle. A frequency of 3 MHz would not provide the necessary depth to adequately sonate the piriformis muscle.
4. A frequency of 1 MHz should be used since the piriformis is a deep structure. When using 1 MHz, the intensity should be between 1.5 and 2.0 W/cm2 to produce tissue heating. 8 minutes would be adequate to sonate over the piriformis muscle.
A physical therapist begins to suspect that a patient may have compartment syndrome secondary to significant lower leg swelling and a decreased dorsalis pedis pulse. If compartment syndrome is present, which nerve would MOST likely be affected?
1. Tibial nerve
2. Sural nerve
3. Deep peroneal nerve
4. Superficial peroneal nerve
Compartment syndrome is a condition associated with increased tissue pressure in a specific muscular compartment. The condition is most commonly seen in the lower leg, especially in the anterior compartment. Compartment syndrome is characterized by pain with exertion, swelling, decreased sensation, and diminished pulses.
1. The tibial nerve is a branch of the sciatic nerve that is located in the posterior lower leg. The nerve primarily innervates the plantar flexors of the ankle. Compartment syndrome would be unlikely to affect the structures in the posterior compartment.
2. The sural nerve is a sensory branch of the tibial nerve. As stated previously, this nerve is located posteriorly in the lower leg and would not likely be affected by compartment syndrome.
3. The deep peroneal nerve is a branch of the common peroneal nerve, located in the anterior lower leg. Because of its location, this nerve is commonly affected with compartment syndrome. Compression of this nerve can result in a steppage gait due to difficulty performing dorsiflexion.
4. The superficial peroneal nerve is a branch of the common peroneal nerve, located in the lateral lower leg. Lateral compartment syndrome does exist, although it is relatively rare.
During a family meeting in an acute rehabilitation hospital a 26-year-old male with complete C7 tetraplegia asks a variety of questions about self care and mobility expectations. With an uncomplicated recovery, the patient can expect lower extremity dressing to be performed with what level of assist in bed?
1. Dependent
2. Minimal assist
3. Modified independence
4. Independent
Following a complete spinal cord injury, patients are likely to express anxiety and concern regarding their significantly altered level of functional independence. In order to appropriately address a patient’s questions, it is essential for the physical therapist to possess knowledge of the anticipated functional outcomes associated with each level of injury.
1. Patients diagnosed with higher levels of tetraplegia (e.g., C1-C5) are typically dependent on the assistance of a caregiver for both upper and lower body dressing. Patients who are not cognitively impaired should be encouraged to participate in the activity by offering verbal direction.
2. Patients diagnosed with mid-level tetraplegia (e.g., C6) are typically able to perform lower extremity dressing in bed with minimal assistance from a caregiver. Upper extremity dressing in bed is typically performed with modified independence (e.g., use of a reacher).
3. Patients diagnosed with lower levels of tetraplegia (e.g., C7-C8) are typically able to perform both upper and lower extremity dressing tasks in bed with modified independence (e.g., use of a shoehorn).
4. Depending on the level of injury, patients diagnosed with paraplegia (e.g., T1 or lower) may demonstrate modified independent or independent upper and lower extremity dressing abilities either in bed or seated.
A physical therapist receives a referral from a physician that states a patient has pes anserine tendinitis. Which of the following muscles is MOST likely affected by this condition?
1. Adductor longus
2. Semimembranosus
3. Biceps femoris
4. Sartorius
The pes anserine is a grouping of three conjoined tendons that all insert on the anteromedial surface of the proximal tibia. Overuse injuries are common in this area and may lead to pes anserine tendinitis or bursitis.
1. The adductor longus originates on the superior ramus of the pubis and inserts on the medial third of the linea aspera of the femur. This muscle does not cross the knee joint and therefore is not part of the pes anserine.
2. The semimembranosus originates on the ischial tuberosity and inserts on the medial condyle of the tibia. Though it does insert on the medial tibia, its tendon is not one of the three tendons that make up the pes anserine.
3. The biceps femoris originates on the ischial tuberosity, sacrotuberous ligament, and along the shaft of the femur and inserts on the fibular head and lateral condyle of the tibia. This muscle is located in the lateral thigh and therefore is not part of the pes anserine.
4. The sartorius originates on the anterosuperior iliac spine of the pelvis and inserts on the anteromedial proximal tibia. It is one of the three tendons of the pes anserine, along with the gracilis and semitendinosus.
A physical therapist assesses the vital signs of a newborn baby prior to the start of the therapy session. Which of the following measurements would be considered abnormal for this patient?
1. Body temperature of 99 degrees Fahrenheit
2. Resting heart rate of 150 beats per minute
3. Resting respiratory rate of 40 breaths per minute
4. Resting blood pressure of 150/100 mm Hg
Physical therapists should be aware of the anticipated changes in vital signs from infancy to adulthood. Although there is consensus on the general direction of the change, the magnitude of the change is highly variable depending on the resource consulted.
1. As a person moves from infancy to adulthood, body temperature values remain relatively constant.
2. As a person moves from infancy to adulthood, heart rate values will generally decrease. Therefore, a newborn’s heart rate will be higher than an adult’s heart rate.
3. As a person moves from infancy to adulthood, respiratory rate values will generally decrease. Therefore, a newborn’s respiratory rate will be higher than an adult’s respiratory rate.
4. As a person moves from infancy to adulthood, blood pressure values will generally increase. Therefore, a newborn’s blood pressure will be lower than, not higher than, an adult’s blood pressure.c
A patient being treated in an acute care hospital complains of excessive thirst on several different occasions during a treatment session. Which electrolyte imbalance would MOST likely be associated with this scenario?
1. Hypercalcemia
2. Hyperkalemia
3. Hypermagnesemia
4. Hypernatremia
Electrolytes play a critical role in maintaining homeostasis within the body. Examples of critical roles played by electrolytes include regulating cardiac function, fluid balance, acid-base balance, and neurologic activity. The most serious electrolyte imbalances involve abnormalities in the level of calcium, potassium, and sodium.
1. Hypercalcemia refers to an excessive level of calcium in the blood. Normal serum calcium is 8.4-10.2 mg/dL. The condition is most commonly associated with hyperparathyroidism since excessive parathyroid hormone raises the level of circulating calcium above normal. Symptoms typically include constipation, pain, nausea, and vomiting.
2. Hyperkalemia refers to an excessive level of potassium in the blood. Normal serum potassium is 3.5-5.0 mEq/L. Levels higher than 7 mEq/L can have significant hemodynamic and neurologic consequences, while levels exceeding 8.5 mEq/L can cause respiratory paralysis or cardiac arrest. Symptoms typically are related to abnormalities in muscular or cardiac function.
3. Hypermagnesemia refers to an excessive level of magnesium in the blood. Normal serum magnesium is 1.5-2.0 mEq/L. This condition is relatively rare since the kidneys are able to eliminate excess magnesium by rapidly reducing its tubular absorption. Hypermagnesemia is most often caused by renal failure. Symptoms typically include hypotension and respiratory depression.
4. Hypernatremia refers to an excessive level of sodium in the blood. Normal serum sodium is 135-145 mEq/L. The condition results when there is a net water loss or a sodium gain and reflects too little water in relation to total body sodium and potassium. Hypernatremia is most often caused by impaired thirst or restricted access to water and can be facilitated by pathologic conditions with increased fluid loss. The primary symptom of this condition is thirst.
A physical therapist treats a patient with stage II breast cancer who presents with neck and shoulder pain. Which intervention would be inappropriate to incorporate into the plan of care?
1. Ultrasound to the pectoralis major insertion
2. Cold pack application to the shoulder
3. Suboccipital release techniques
4. Taping application to assist with postural awareness
Staging is the process of describing the extent to which a cancer has developed by spreading. Stage II cancer is characterized by an increased risk of metastasis due to the size of the tumor. When treating a patient with cancer, it is important for therapists to be aware of modalities and physical agents that have the ability to cause cancer to further metastasize.
1. The use of any deep heating agent (e.g., diathermy, ultrasound) is contraindicated over the site of a tumor in a patient with cancer. Deep heating agents increase blood flow and have the potential to increase the spread of cancer. The relative proximity of the pectoralis major to the active site of cancer makes applying ultrasound an inappropriate intervention.
2. Active cancer is not a contraindication for the use of cryotherapy. In patients who are undergoing radiation therapy, however, the therapist should use caution to avoid applying the cold pack over dysvascular tissue or insensate skin.
3. Soft tissue manipulation over a malignant tumor should be avoided due to the potential for metastasis of the cancer. However, the suboccipital muscles are far enough away from the active site of cancer that these techniques are unlikely to result in metastasis. Additionally, the suboccipital release technique uses a relatively low level of force so that there would not be a significant increase in blood flow.
4. Taping techniques can be used in patients with shoulder pain to assist them with postural awareness. Active cancer is not a contraindication to the use of taping.
A physical therapist treats a patient using grade III and IV oscillations. Which examination findings would BEST support this type of intervention?
1. Decreased active range of motion and decreased passive range of motion
2. Decreased active range of motion and normal passive range of motion
3. Normal active range of motion and decreased passive range of motion
4. Decreased active range of motion and increased passive range of motion
The results of the physical therapy examination should provide the physical therapist with the necessary information to generate a problem list and develop an appropriate plan of care. Interventions incorporated into the plan of care should be appropriate to accomplish the established therapeutic goals. Oscillatory techniques can be graded on a 5-point scale. Grade I and II mobilizations are performed at the beginning of the available motion without actually reaching the limit of motion. Grade III and IV mobilizations are performed up to or past the limit of available motion. Grade V oscillatory techniques are termed manipulations.
1. Grade III and IV joint mobilizations are performed primarily to stretch the joint capsule due to a capsular restriction. A restriction in the joint capsule would result in decreased active and passive range of motion.
2. Decreased active range of motion and normal passive range of motion would more commonly be associated with muscle weakness.
3. Normal active range of motion and decreased passive range of motion would be relatively uncommon. Passive range of motion is often greater than or equal to the active range of motion.
4. Decreased active range of motion and increased passive range of motion is not uncommon since passive range of motion is often greater than active range of motion. If the decrease in active range of motion was associated with a capsular restriction, the patient would also exhibit a decrease in passive range of motion.
A physical therapist administers ultrasound to a patient diagnosed with right patella tendinopathy. Based on the patient's medical diagnosis what is the MOST appropriate output frequency?
1. 1 W/cm2
2. 1 MHz
3. 3 W/cm2
4. 3 MHz
The frequency used for ultrasound is either 1 MHz or 3 MHz and is determined based on the depth of tissue to be treated. For tissue up to 5 centimeters deep, 1 MHz is used. For tissue 1-2 centimeters deep, 3 MHz is used.
1. The unit “W/cm2” is a measurement of intensity, not frequency.
2. A frequency of 1 MHz would be used for treating deeper structures (up to 5 centimeters deep). However, the patella tendon is a superficial structure.
3. The unit “W/cm2” is a measurement of intensity, not frequency.
4. A frequency of 3 MHz would be used for superficial structures (1-2 centimeters deep). This would be the appropriate parameter to use since the patellar tendon is a superficial structure.