ceutics renal clearance
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
4 things that determine dose of drug
- clearance
- dosing interval
- target concentration
- route of administration
what happens at the peak of the concentration time curve
in = out (max absorption has already been achieved)
[this is NOT max rate of absorption]
what would the CT graph look like if drug A and drug B had identical properties but CL differs by a factor of 3
absorption side of curve would look the same
elimination side would look different
- drug with bigger clearance would have steeper slope (appear lower) bc its clearing faster
if Drug A has a steeper elimination slope than Drug B, which drug has a larger clearance rate? shorter half life?
Drug A steeper elimination= cleared faster= shorter half life
how do you determine the half life of a drug using the ct curve
its the slope of the elimination side
t/f: elimination is the same as excretion
false. elimination is either excretion or metabolism
t/f: clearance is the same as excretion
false. clearance relates to the rate of drug elimination (so can be metabolism)
t/f: a drug in the urine of the collecting ducts has undergone excretion
false. if it is still in the body, even if its in the urine, then it is not officially excreted. it is excreted when it is completely outside the body
t/f: clearance always refers to the inactivation of drugs
false. prodrugs are activated by metabolism so clearance correlates to activation
t/f: the kidney is capable of both metabolism and excretion
true. has enzymes for metabolism
characteristics of drugs undergoing glomerular filtration
1. drug must be low MW
2. only unbound drugs are filtered
3. un-ionized drugs (ionized= repulsion and static cling)
if the urine is acidic, which drugs can be reabsorbed? trapped?
acidic urine means
- weak acids reabsorbed
- weak bases are ion trapped
why is glomerular filtration unidirectional and passive
afferent arteriole has a wider diameter than the efferent arteriole, forming pressure that pushes blood forward. blood will never go back the other way
what is glomerular ultrafiltrate
fluid that enters the glomerular capsule (tubular fluid)
active secretion vs active reabsorption
secretion= more things put into urine via transporters
reabsorption= things enter back into bloodstream
where in the kidney do active secretion and reabsorption usually occur
proximal tubule
(distal tubule is the last chance before enters the collecting tubule)
will giving a higher dose of a drug change the clearance rate?
no. clearance is a constant. but you will have MORE drug MOLECULES cleared just at the the SAME RATE
how does urine flow affect renal clearance? how doest CT curve change?
slower urine flow allows for a bigger chance for reabsorption of drugs back into blood
- elimination side of curve is elevated
how does gender affect renal clearance
males have faster GFR
the rate of free drug entering urine from the glomerulus is _________ limited
perfusion (how fast can blood enter glomerulus)
t/f: the clearance rate for both free and bound drugs is less than renal blood flow
true
clearance rate for bound drugs
CL= fraction unbound x GFR
(less than renal blood flow)
what will happen to the half life of a drug undergoing active reabsorption?
effect on ct curve?
what will happen to concentration of drug in urine and blood?
increased half life; higher slope on elimination side of graph [remember nothing to do w absorption]
concentration lower in urine, higher in blood
when may we see diffusion back into the urine from the blood
no ion trapping
-> weak acids may diffuse back into acidic urine
in situations with outside glomerular capsule diffusion, CL ___ fraction unbound x GFR
CL _>_ fraction unbound x GFR
theres greater clearance since more of the drug is diffusing into urine, on top of glomerular filtration
compare clearance of free drug, bound drug, active reabsorption, and diffusion
CL= GFR for free drug
CL = GFR * fraction unbound [for bound drugs]
active reabsorption: CL < fu x GFR
diffusion back into urine: CL > fu x GFR
with reabsorption and secretion happening at the same time, who wins?
they cancel out= no real CLINICAL significance
[liver metabolism plays bigger role than renal]
if extraction ratio is reduced from 40% to 20%, what effect would that have
20% more active drug in blood== OD pt
can renal CL ever reach the rate of renal blood flow?
yes theoretically (all of drug is cleared). you will approach it but never reach it
- all of drug must be unbound
- no reabsorption
- rest of drug is diffused/secreted into urine
given a graph depicting GF and tubular secretion clearance vs fraction unbound, how will you determine whether a drug is highly protein bound?
if greatest elimination rate (highest slope) is active secretion, then the drug is highly protein bound and limited to vasc compartment
if the slope of the GFR clearance was bigger, then the drug is most likely not protein bound
if a drug readily undergoes active secretion, what may this suggest about Vd
undergoing active secretion means the drug is highly protein bound= limited to vasc compartment= low Vd
Drug A is highly acidic
will you expect more of the drug to be in the urine at pH 4.4 or 7.9?
acid will be trapped in base so we would expect more of the drug to be found at pH 7.9
[at pH 4.4 it will probs be in blood]
Drug A is highly basic
will you expect more of the drug to be in the urine at pH 4.4 or 7.9?
base will be trapped in acid so we would expect more of the drug to be found at pH 4.4
[at pH 7.9 it will probs be in blood]
if more of a drug is found in the urine at pH 4.4 than 7.9, is the drug an acid or base?
if more drug is found in the urine when it is acidic, then the drug is a base [ion trapping]
given a graph of amount of drug excreted vs time,
if more drug is excreted (higher slope) when urine is acidic compared to when the urine is basic (lower slope), is the drug a base or acid?
if more drug is excreted in acidic urine, then the drug is a base [ion trapping]
t/f: is less drug is excreted in basic urine then the drug is most likely a weak base
true
would you expect more elimination of salicylic acid at high pH or low pH
weak acid= more elimination at high pH (basic) bc of ion trapping
phenobarbital is excreted in greater amounts in a basic environment. is this a weak base or weak acid
weak acid [ion trapping]
highest density of transporters are found in the renal _________
proximal tubule
t/f: transport systems in the kidney mainly fxn to recycle endogenous compounds such as organic anions, cations, and amino acids
true
t/f: active transporters may move substances both INTO the renal tubule and OUT of the renal tubule
true
t/f: active transporters always follow first order PK
false. active transporters are saturable. not first order. non-linear pharmacokinetics
a cardiac implication that reduces blood flow would ___ CL and ____ half life
lower Cl
increase half life
if a drug has lower affinity for a transporter or the transporter is saturated, how will this effect the CT curve
shift elimination side up bc longer half life
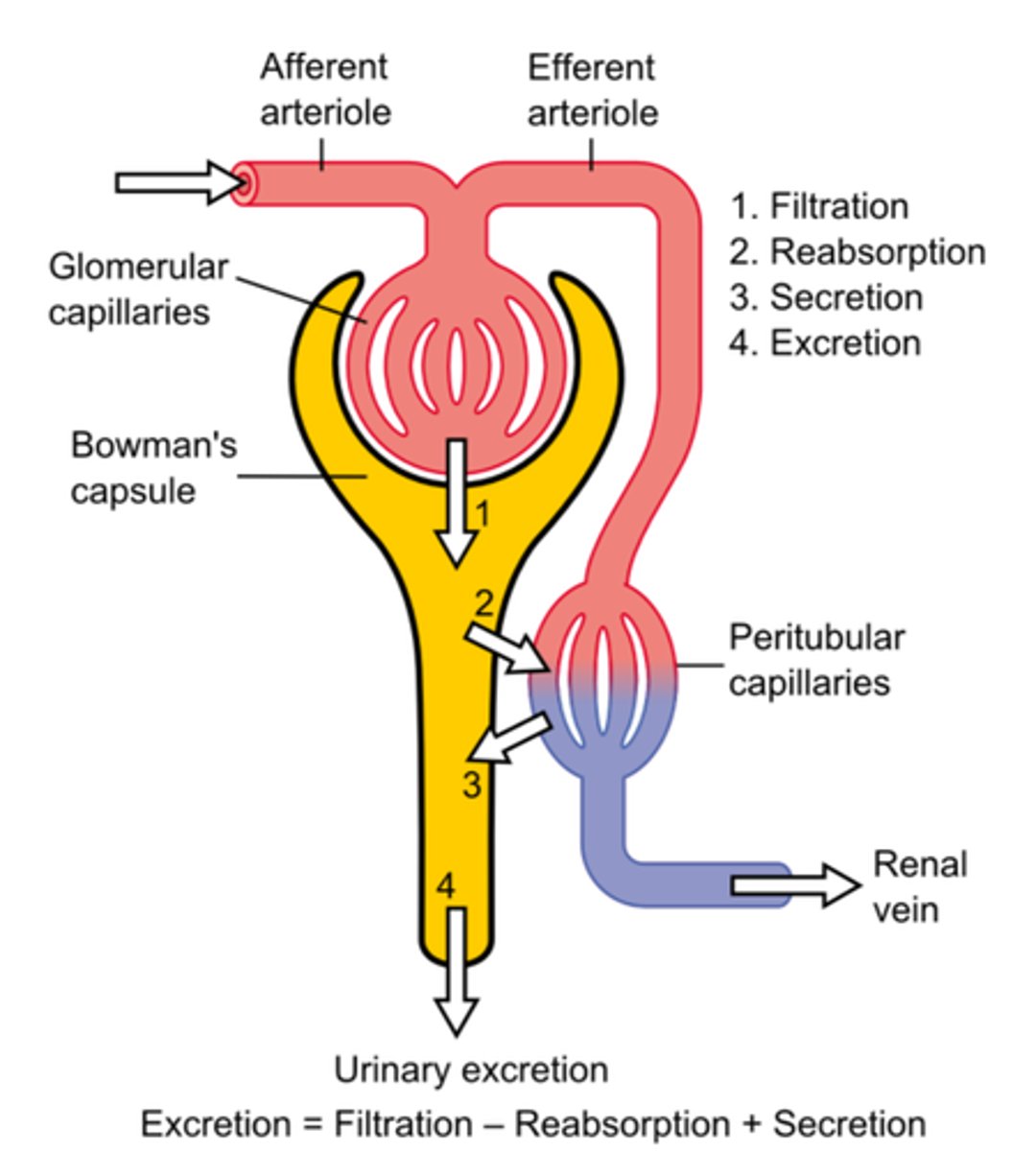
rate of elimination is the sum of which 3 processes
add filtration, secretion
subtract reabsorption
how can urine flow impact clearance
if urine flow is increased, residence time of drug in lumen is lowered= lower chance of reabsorption= increased CL
(so major impact on if drug has significant diffusion/reabsorption)
which will have a greater effect on a drug that is significantly reabsorbed
a. renal blood flow
b. GFR
c. urinary outflow
c. urinary outflow
want to increase flow so it spends less time in lumen
interpret the following excretion ratios
0.5, 1, 2
<1: net reabsorption [more in blood]
1: filtration only (or secretion= reabsorption)
>1: net secretion [more in urine, successfully secreted]
if ER < fu x GFR, is reabsorption due to active transport? what does that depend on
depends on urinary pH
ER < fu × GFR means something is reducing elimination (reabsorption or active transport)
- urinary pH controls how much reabsorption happens by changing the drug's ionization
net reabsorption vs net secretion
what is it?
effect on CT?
net reabsorption= more drug reaching blood. less steep elimination slope
net secretion= less drug in blood (probs protein bound). more steep elimination slope
does GFR depend on concentration?
no. GFR is a constant rate bc renal blood flow is constant. if you increase concentration, you will eliminate MORE molecules but at a CONSTANT rate
ex: drinking more water means you eliminate more water but youre eliminating AT A CONSTANT RATE!!
t/f: half life is determined by CL and Vd
true
what effect would increasing CO have on the plasma clearance of a drug that is highly bound to RBCs
no effect. plasma clearance means free drug in plasma (NOT BOUND TO RBCS)