NBCOT: Wheelchair seating and mobility
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
Client seated position:
Hands-free sitter
Client is able to maintain a seated position without using hands. The seating system design emphasizes mobility, stability (stable base of support) and comfort.
Client seated position:
Hands-dependent sitter
Client uses one or both hands to maintain a seated position. Pelvic and trunk support is required of the seating system to free the hands for activities.
Client seated position:
Propped sitter
Client lacks the ability to sit without support. Total body support is required of the seating system for posture and repositioning.
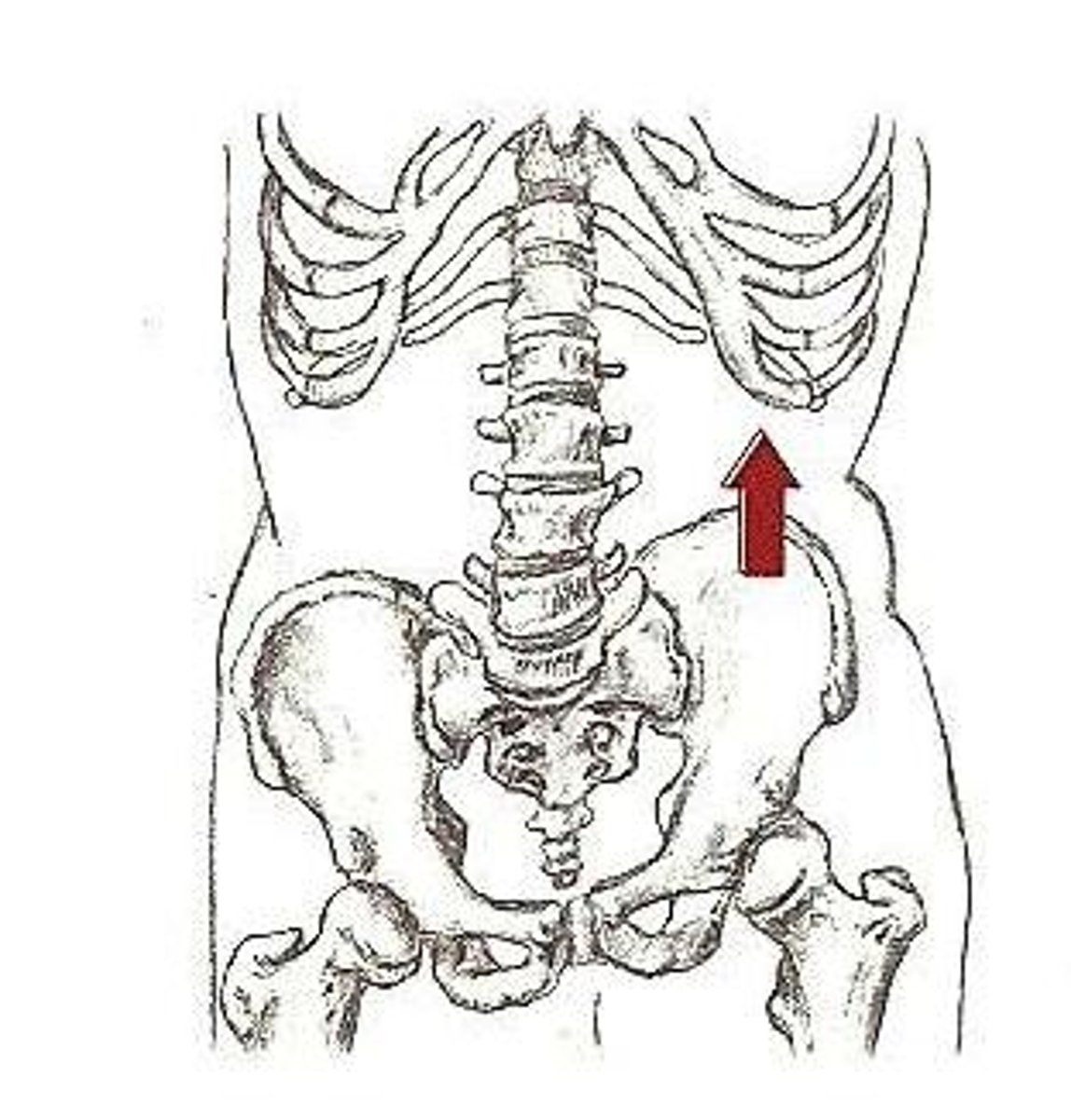
Pelvic obliquity
one side of the pelvis is lower than the other side, which can lead to scoliotic posture and pressure ulcers on the ischial tuberosity
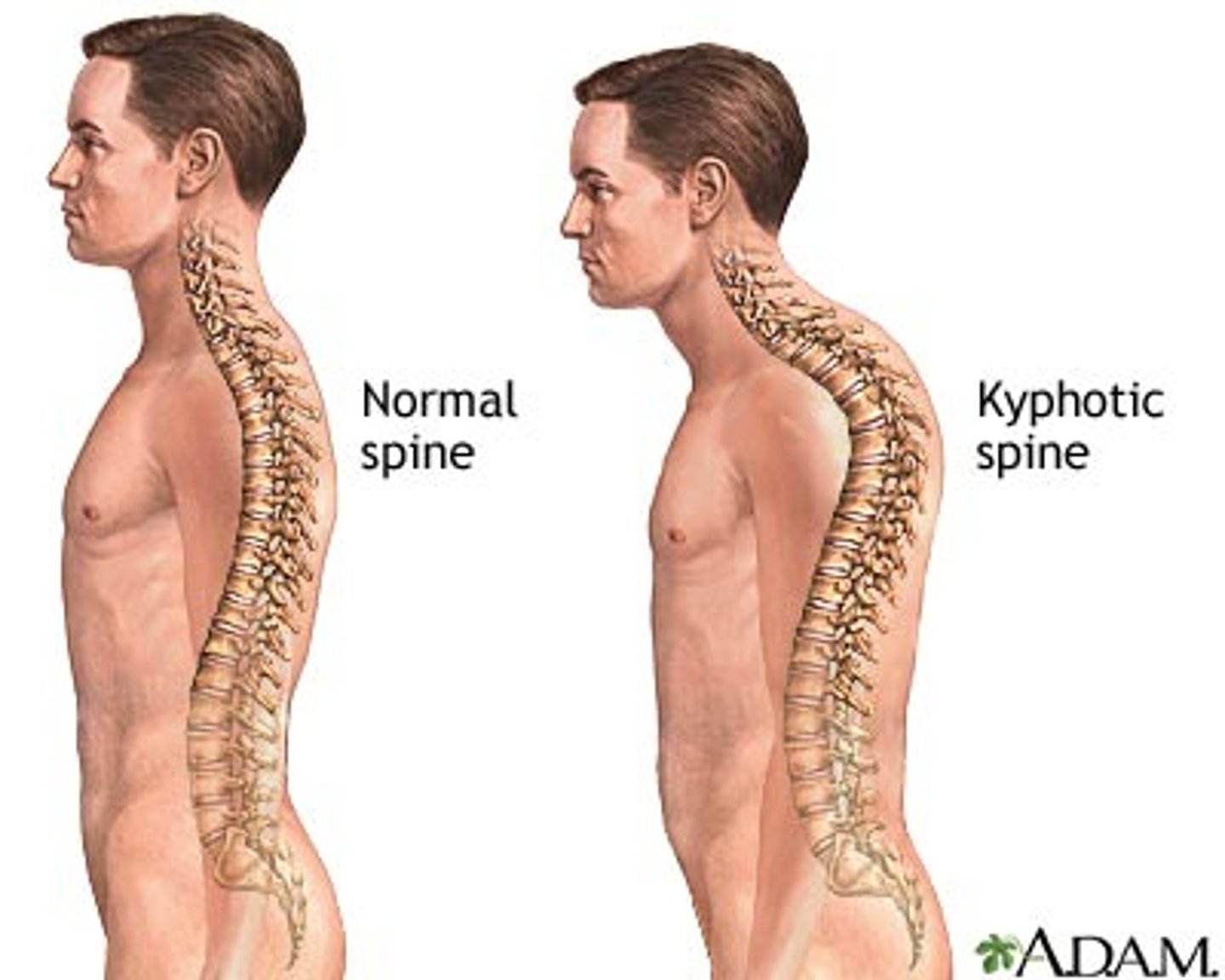
Kyphosis
The pelvis rotates posteriorly, resulting in sacral sitting and flexion of the lumbar spine; clients tend to slide forward in the seat.
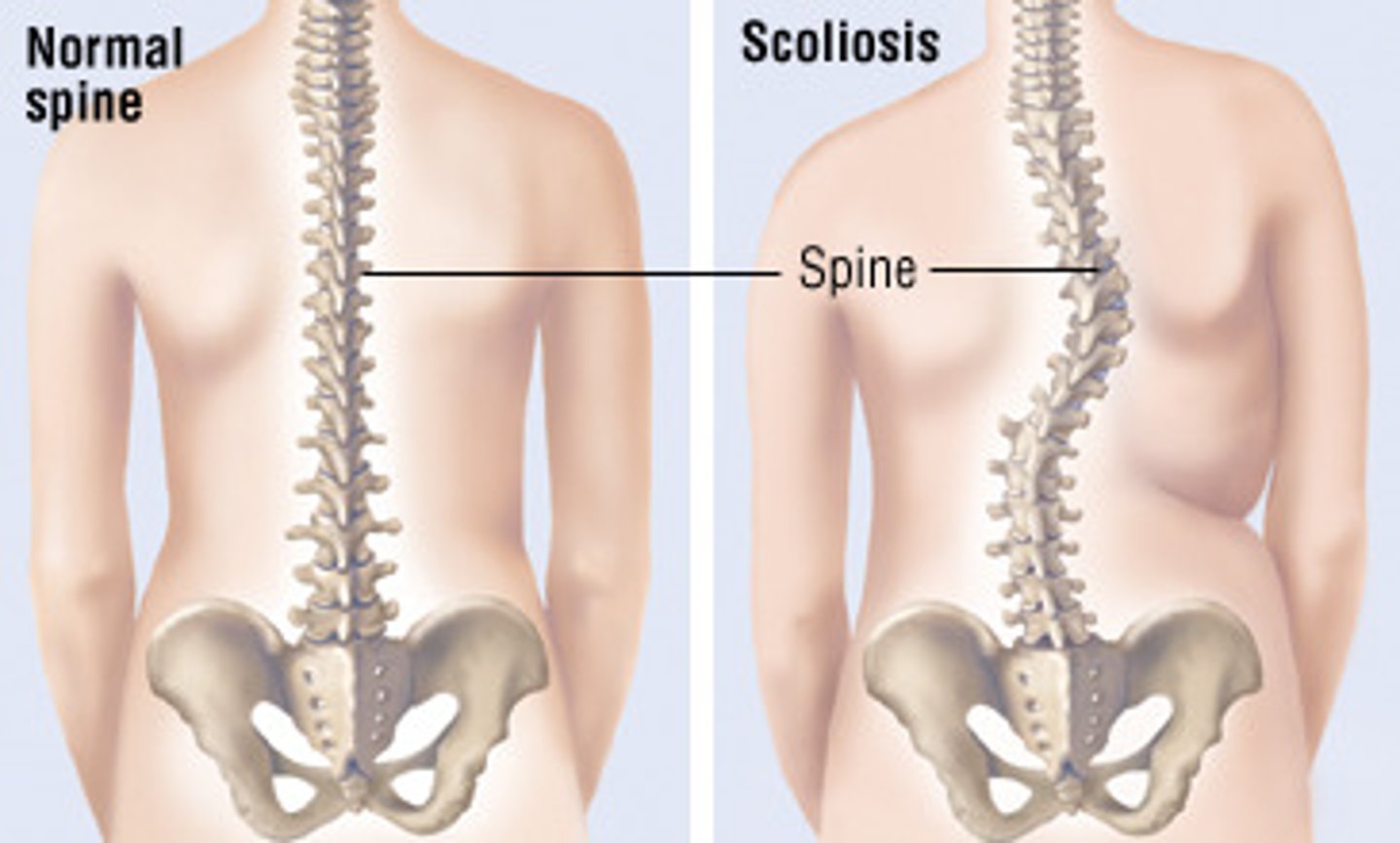
Scoliosis
The pelvis rotates to one side, resulting in the spine and trunk moving to the opposite side
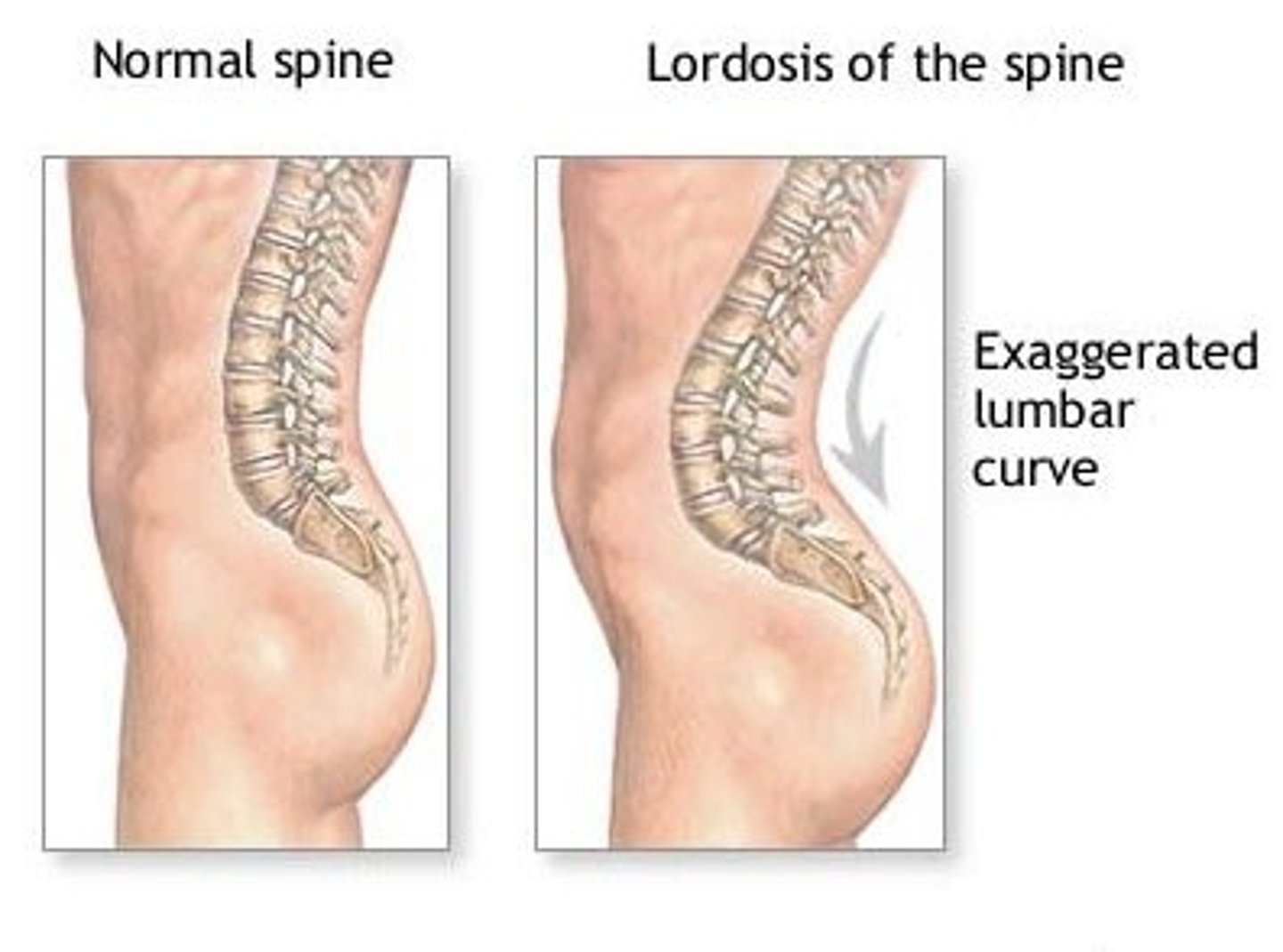
Lordosis
The pelvis rotates anteriorly, increasing the curvature of the lumbar spine; clients tend to use upper extremities for support
Windswept deformity
pelvis rotates laterally, with the thighs moving to the other side

When fitting, always think of pelvis and stabilizing (KT).
When fitting, always think of pelvis and stabilizing (KT).
Seated position
Trunk is upright and in midline position; hips, knees, and ankles are flexed into 90; pelvis is neutral, head is in mid-position, and the arms at the side of the trunk with the elbows flexed to 90.
Pelvis positioning
Key to stability. Provide a solid base of support by stabilizing the pelvis on a firm surface, which distributes pressure throughout the buttocks and thighs. Support posture with the seat and seat back. Provide cushioning for these surfaces.
pressure mapping
process of measuring pressure by inserting a pressure-sensitive mat between the client and the seating surface
Cushion materials: foam
Cushion materials
variable density, soft and pliable and will mold itself around the buttocks. If it's too soft, client may totally compress it, making it useless for pressure management.
PRO: Lightweight and low cost
CON: Heat and moisture can build up
NOTE: Custom-contoured foam is more expensive and provides better postural control; shearing is reduced, and weight-shifting capability is reduced.
Cushion materials: gel filled
Cushion materials
Conform to the shape of buttocks; they are adequate for postural control, heavy, and sensitive to temperature.
Cushion materials: air filled
Cushion materials
Lightweight, provide even pressure relief BUT have to be properly inflated to perform well. They also reduce postural stability.
Cushion materials: Honeycomb-shaped plastic
Cushion materials
Provide uneven pressure relief and are lightweight
Cushion materials: Alternating pressure
Cushion materials
These cushions provide scheduled pressure relief through alternating levels of inflation and deflation; they also reduce postural stability.
pelvic stabilizer/belt/SubASIS bar
-positioned at the front of the pelvis
-limits pelvic tilt, rotation or obliquity
-pull pelvis at 45 degree angle to base of seat back
thoracic supports wc
-place lateral to trunk, below armpits
-facilitate trunk stability, prevent/slow scoliosis
-anterior trunk supports are placed below the top and above the bottom of the breast bone
thigh supports wc
-lateral or medial to thighs
-control abduction or adduction e.g. windswept deformity
Head rest supports
supports the back of the head and is positioned at the occiput
Wheelchair measurements: Seat width
Pt: Width of hips at widest part
Chair: Add 2 inches to pt measure
Excessive width increases difficulty or reaching drive wheels, getting through doorways.
Too narrow results in pressure on lateral pelvis/thighs. Lateral space should allow for changes in the thickness of clothing.
GOAL: Distribute body weight over as much of the seat as possible
Wheelchair measurements: Seat depth
Pt: Posterior buttock to popliteal fossa
Chair: Subtract 2-3" from pt measurement
Too short fails to support the thigh adequately.
Too long may compromise posterior knee circulation or result in kyphotic posture, posterior pelvic tilt, sacral sitting
GOAL: Distribute body weight along as much of the thigh as possible
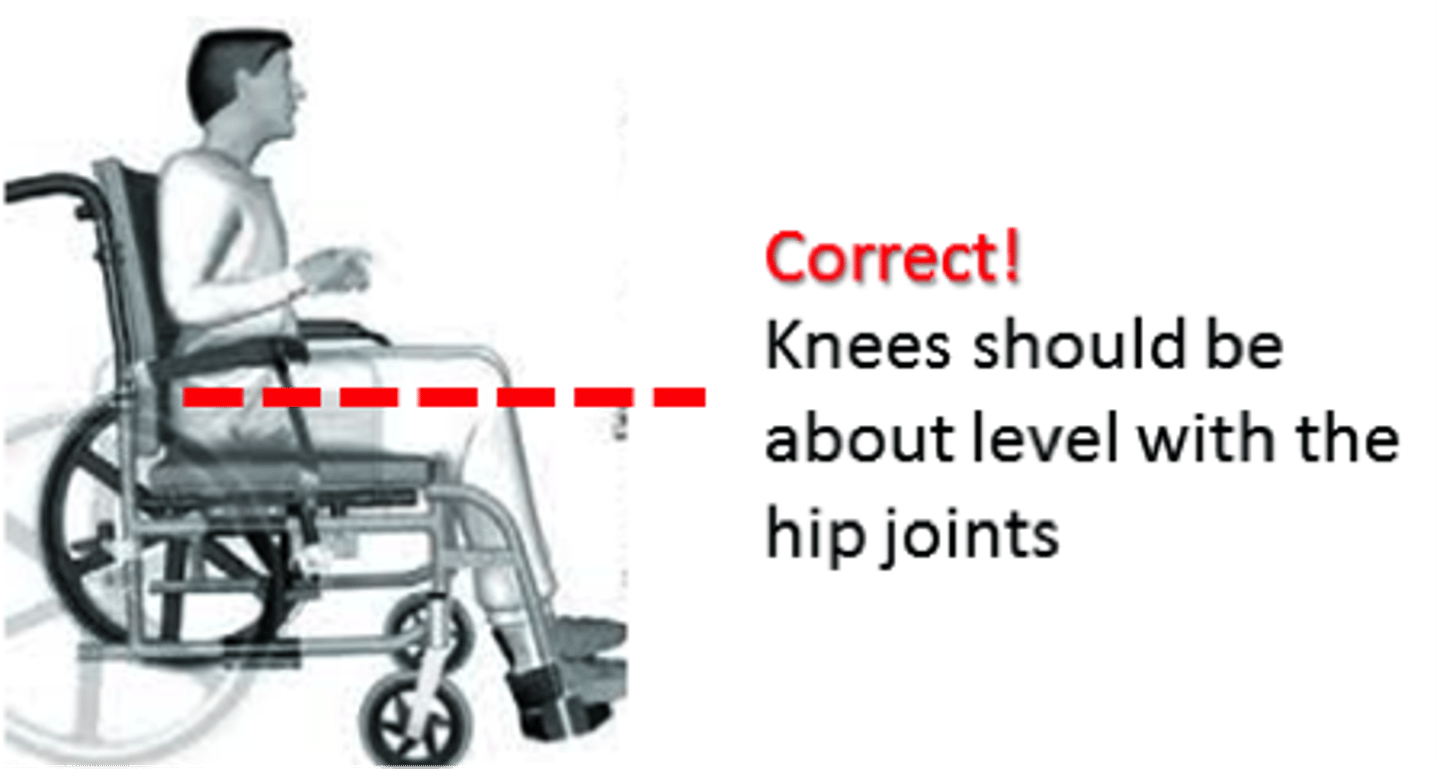
Wheelchair measurements: Seat height
Measure from popliteal space to the bottom of the client's heel.
Footrests should have a 2 inch clearance from the floor
GOAL: Keep thighs parallel to the floor, the feet resting comfortably on the footrests, and the footrests clearing the floor
Wheelchair measurement: Seat back height
A higher back height may be needed if trunk control is poor
For power wheelchairs, back heights to midscapula or the top of the shoulder may be needed to attach upper trunk and head supports
Types of wheelchairs
Transporter chair
Types of wheelchairs
Designed to be pushed by an attendant or caregiver. Smaller rear wheels, making them lighter and easily transportable. Used for short distances or temporary purposes.
Types of wheelchairs
Manual chairs
Types of wheelchairs
Self-propelled or pushed by an attendant or caregiver. Clients need adequate UE strength and endurance to push and brake
Manual STANDARD CHAIR: short term temp use - these chairs fold, the seat and back are sling upholstery, and the rear axle is fixed. They are heavy and have limited adjustability.
Manual LIGHTWEIGHT chair: similar to standard but are lighter in weight. Adj is limited.
Manual ULTRA lightweight chair: available with rigid or folding frames - adj axle and quick release wheels and are customizable
Heavy duty chair: bigger and stronger for clients who are obese or have severe spasticity
Types of wheelchairs
Scooters
Types of wheelchairs
For limited walking, have 3 and 4 wheels and are steered with a tiller. Do not look like wheelchairs and are difficult to steer than power wheelchairs. They have a large turning radius, and the seat swivels, which may make transfers easier. They have limited adjustability.
AOTA: Power wheelchairs provide more postural control with various seating options. Special seating is difficult to attach to a scooter, and it is therefore not recommended for someone with significant postural control challenges.
AOTA: In most instances, scooters require a larger turning radius than power wheelchairs and may have limited ability to maneuver indoors.
AOTA: Scooters are modular and can be disassembled and loaded into and taken out of the trunk of a car more easily than a power wheelchair. The primary disadvantage of power wheelchairs is that they are so large and heavy that they cannot be placed in the trunk of a car and require a special transport system.
Types of wheelchairs
Power wheelchairs
Types of wheelchairs
For those who cannot propel a manual or for who propelling is contraindicated
Movement controlled through joystick or alternative control type (breath, head, chin, eye, tongue). Multiple seating options are available ranging from automotive-type captain's seats to seats that tilt, recline, elevate the leg rests, or stand
Chairs that recline and tilt
For clients that have hip contractures, need to recline to reduce pressure or manage fatigue, or cannot reposition themselves independently or are unable to maintain an upright seated position. They assist in managing ROM, muscle tone, orthostasis, catheterization, and head control and in enabling visual contact.
Tilt - seat-to-back angle is fixed
AOTA NBCOT question: Transferring tips
An anterior pelvic tilt moves the center of mass over the center of the client's body. Heels should point toward the surface to which the client is transferring for easier pivot. Pushing up from the wheelchair armrest assists in the transfer
Four basic measurements:
Seat width, seat depth, seat height, seat-back height
Wheelchair propulsion INITIAL training (NBCOT question)
The initial stage of wheelchair propulsion training should occur inside the therapy clinic because the client can learn how to maneuver the wheelchair on a smooth, uncluttered surface.
NBCOT question
An OTR® and a Level II Fieldwork student at a long-term care facility observe a new resident moving his wheelchair forward by gripping the front of the pushrim and giving it multiple tiny pushes. The OTR® asks the student, "Why do you think he is pushing his wheelchair that way?" The student observes a bit longer and responds:
*Is the seat back too low or too high?
Seat back is too high: When the seat back height is above the lower angle of the scapula, it can prevent adequate shoulder extension, which is necessary for contacting the pushrim.
A, B: If the seat back of the chair was too low, the client would able to extend his shoulders and get a proper grip on the pushrim; if the chair was too wide, the client would only reach the top of the pushrim.
D: If the armrests were too low, the client would have a greater ability to reach the top of the pushrim.
Dependent transfer
The ______________________ transfer is designed for use with the client who has minimal to no functional ability. It is important to encourage maximum independence, and this client should not be require dependent transfers.
Bent pivot
____________ transfers are used when the client cannot initiate or maintain a standing position but can bear some weight; with lower-extremity paralysis, however, the client cannot bear weight.
Stand pivot transfers
______________ are used when the client can take small steps toward the transfer surface. This client is unable to bear weight.
Sliding board transfers
____________ are the most functional way to transfer for a client who cannot bear weight through the lower extremities but can use the upper extremities to assist with the transfer.
Rule of thumb for the client's ability to sit upright.
Minimal hip flexion of 90°, The ability to achieve 90° of hip flexion is necessary for postural stability when sitting upright without support.. Hip flexion less than 90° will put the client in a partially reclined position, increasing pressure on the sacral area.
NBCOT: An adolescent client who has muscular dystrophy uses a manual wheelchair that has a backrest cushion and a gel seat insert. The client reports a recent onset of shoulder pain while propelling the wheelchair over a carpeted surface. The OTR® observes that the wheelchair has a backrest cushion that positions the client's pelvis beyond the rear wheel axle. Which wheelchair modification should the OTR® recommend to reduce the client's shoulder pain?
Remove the backrest cushion: Removing the backrest cushion will position the client's pelvis directly over the rear wheel axle, which will make propulsion easier.
NBCOT: An OTR® is addressing meal preparation with a client who recently sustained a fracture of the left humerus and is currently in a splint and sling. The client uses a straight cane for functional mobility. How should the OTR instruct the client to remove items from the oven during meal preparation?
Stand to the left of the oven, open the door, reach in with the right arm, pull out the food, and place it on top of the oven. - Standing to the left of the oven allows the client to open the door easily with the right hand and remain as close as possible to the food item being retrieved when pulling it out of the oven. Standing to the right of the oven would require the client to rotate to get the right arm in a position in which lifting the food item would be possible. Standing directly in front of the oven creates a bigger space between the client and the food item being retrieved, which means the client would have to bend farther forward, creating a bigger risk of falling.
NBCOT: Although fitted with an ultra lightweight wheelchair (K0005), a client with bilateral above-the-knee amputations is prone to losing sitting balance and falling forward when propelling the chair. The position of the axle is in front of the pelvis. The OTR® needs to find a balance between stability and the effectiveness of arm propulsion. Because the chair is a K0005, which solution will the OTR® MOST likely suggest?
Move the axle back so the client's center of gravity is over the axle and add antitippers - by moving the axle backward, compromised stability will be offset by the antitippers, but movement efficiency will be increased during propulsion and the client's center of gravity will no longer be at the front of the wheelchair, thus reducing the risk of falling forward. ALSO - antitippers ALONE are used to prevent falls backward and the client has been falling FORWARD.
NBCOT: An OTR® is creating an intervention plan for a client who was recently in a car accident and has multiple fractures. The client is currently not driving but has verbalized the desire to drive again in the future. What is the appropriate hierarchy of skill building to restore competence in mobility for this client?
HEIRARCHY for this client:
1. Start with functional ambulation for ADLs
2. then move to car transfers
3. then to functional ambulation for community mobility
4. end with driving.
Considering the hierarchy of skills for each mobility task and their demands, functional ambulation for community mobility is considered more complex than car transfers and therefore should not be addressed before car transfers.
NBCOT: The topic of the February 7, 2013, newsletter MLN Matters, published by the Medicare Learning Network under the Centers for Medicare and Medicaid Services, was related to changes in the criteria for mobility assistive equipment and mobility-related ADLs (MRADLs), which OTR®s working with positioning, seating, and wheelchairs need to know for reimbursement. Which of the following is NOT an MRADL specifically cited by Medicare?
A: Cooking | Explanation: Cooking is not specifically cited by Medicare; Medicare regulations state that beneficiaries must have significant limitations in tasks such as "toileting, feeding, dressing, grooming, or bathing."
NBCOT question: An OTR® is teaching a client how to pop a wheelie in a manual chair so that the client can negotiate curbs. What instructions would the OTR give this client?
Grasp the hand rims posteriorly and pull them forward forcefully and abruptly, throwing the head back forcefully, if needed. - To elevate onto the large rear tire, it is necessary to grasp the hand rim as far posteriorly as possible and quickly pull forward.
Other answers/reasons:
B: Grasping the hand rims anteriorly and pulling forward would push the wheel farther into the ground, not allowing the wheelchair to elevate.
C: Grasping the hand rims in the center would make it difficult to get enough force to elevate the large rear tire.
D: Grasping the hand rims in the center and pulling them backward would not allow for enough force and would push the wheels in the wrong direction.
NBCOT: A new client is unable to sit up on the edge of the bed or stand without assistance. The OTR® has decided to address bridging in bed. Why is this a functional activity for an OTR to address?
Bridging is used to assist with LB dressing in bed. - Bridging is a movement strategy used to complete functional activities in bed, such as using a bed pan or pulling pants over the hips.
NBCOT: A client's family purchased an ultra lightweight wheelchair (K0005) for the client. It has the correct seat height, seat width, and seat depth, but the client has difficulty propelling it. The OTR® asks the client to demonstrate moving the chair forward. What two potential problems would the OTR® FIRST focus on?
Location of the axle in relation to the client's center of gravity, seat-back height
NBCOT: An OTR® works at a skilled nursing facility that provides wheelchairs for clients who need them. As a result, the facility has a room full of wheelchairs of various sizes. The OTR is often expected to find the wheelchair that best fits each new client, which requires determining whether the seat depth is appropriate for that client. Where should the front edge of the wheelchair seat be in relation to the client's hamstrings?
1-2 inches proximal to the posterior side of the bent knee | Having the seat of the wheelchair very close to the bent knee without touching it allows for the client's body weight to be evenly distributed, which prevents pressure sores, while still allowing for knee clearance from the edge of the seat upholstery
NBCOT: A client reports having difficulty with lower-extremity mobility in relation to getting into and out of bed. What piece of adaptive equipment is MOST appropriate to recommend to this client?
A leg lifter: A leg lifter is a device for moving one leg at a time. It can be used to allow the client to manually move the legs over the side of the bed or manually lift the legs into bed.
B: A bed ladder is a device on which a person pulls with one or both upper extremities, using each rung in progression until his or her trunk is at the desired position. It does not assist with moving the legs.
C: A bed rail can assist with rolling or moving in bed, but does not help move the legs.
D: An overhead trapeze bar assists with rolling over, lifting the hips up, scooting the body in bed, or obtaining a long-leg seated position in bed. However, it does not help move the legs.