ANATOMY wk 1 + 2
1/68
Earn XP
Description and Tags
WEEK 1 AND 2
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
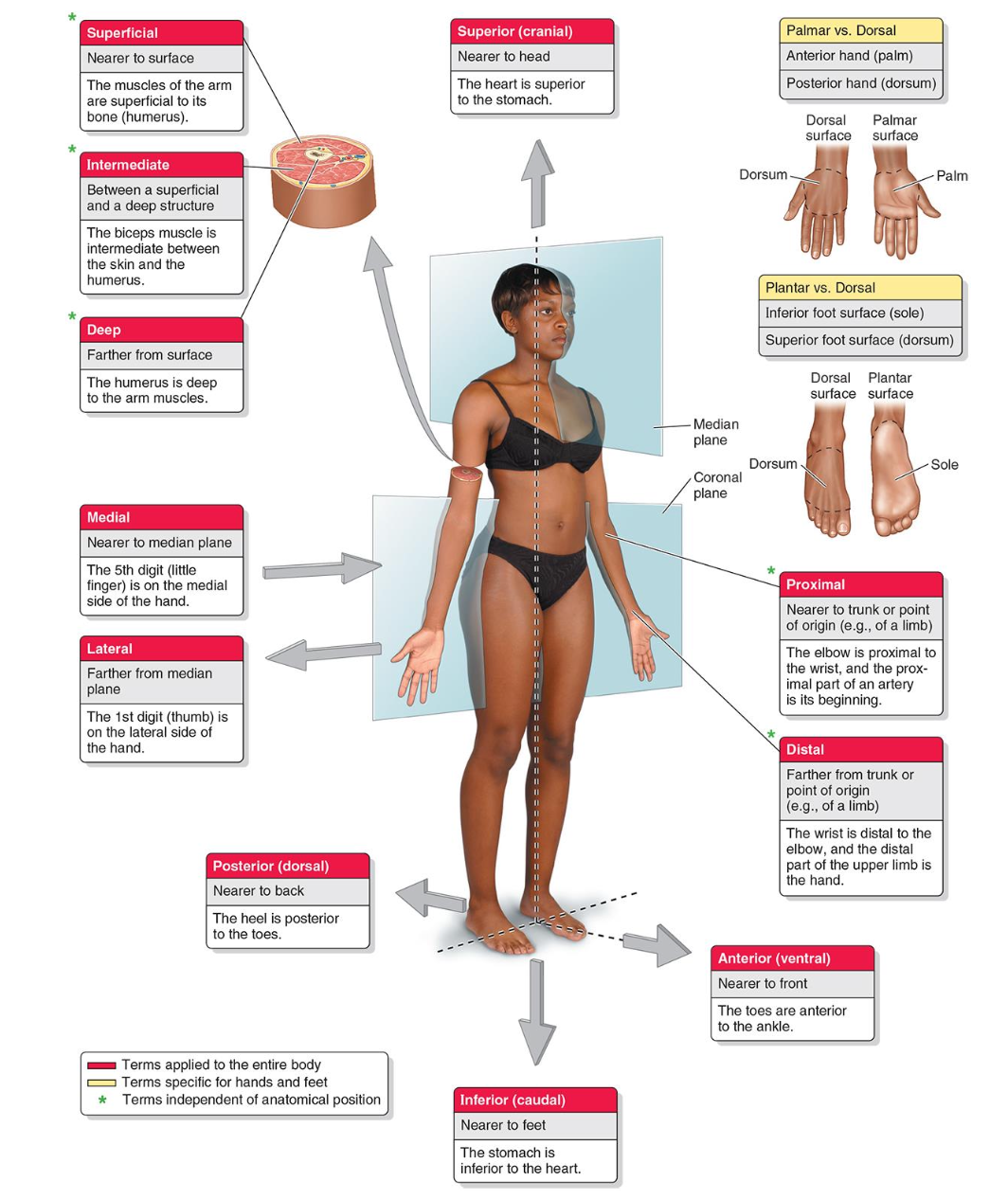
Anatomical terminology, including planes
Anterior (ventral) | Nearer the front. |
Posterior (dorsal) | Nearer the back. |
Superior (cranial) | Upward or nearer the head. |
Inferior (caudal) | Downward or nearer the feet. |
Medial | Toward the midline or median plane. |
Lateral | Farther from the midline or median plane. |
Proximal | Near a reference point. |
Distal | Away from a reference point. |
Superficial | Closer to the surface. |
Deep | Farther from the surface. |
PLANES
Median plane | Divides body into equal right and left halves. |
Midsagittal plane | Median plane |
Sagittal plane | Divides body into unequal right and left halves |
Frontal (coronal) plane | Divides body into equal or unequal anterior and posterior parts. |
Transverse plane | Divides body into equal or unequal superior and inferior parts (cross sections). |
MOVEMENT
Flexion | Decreases the angle between two body parts. |
Extension | Increases the angle between two body parts. |
Abduction | Movement AWAY from the midline. |
Adduction | Movement TOWARD the midline. |
Internal (medial) rotation | Rotation of a limb toward the midline. |
External (lateral) rotation | Rotation of a limb away from the midline. |
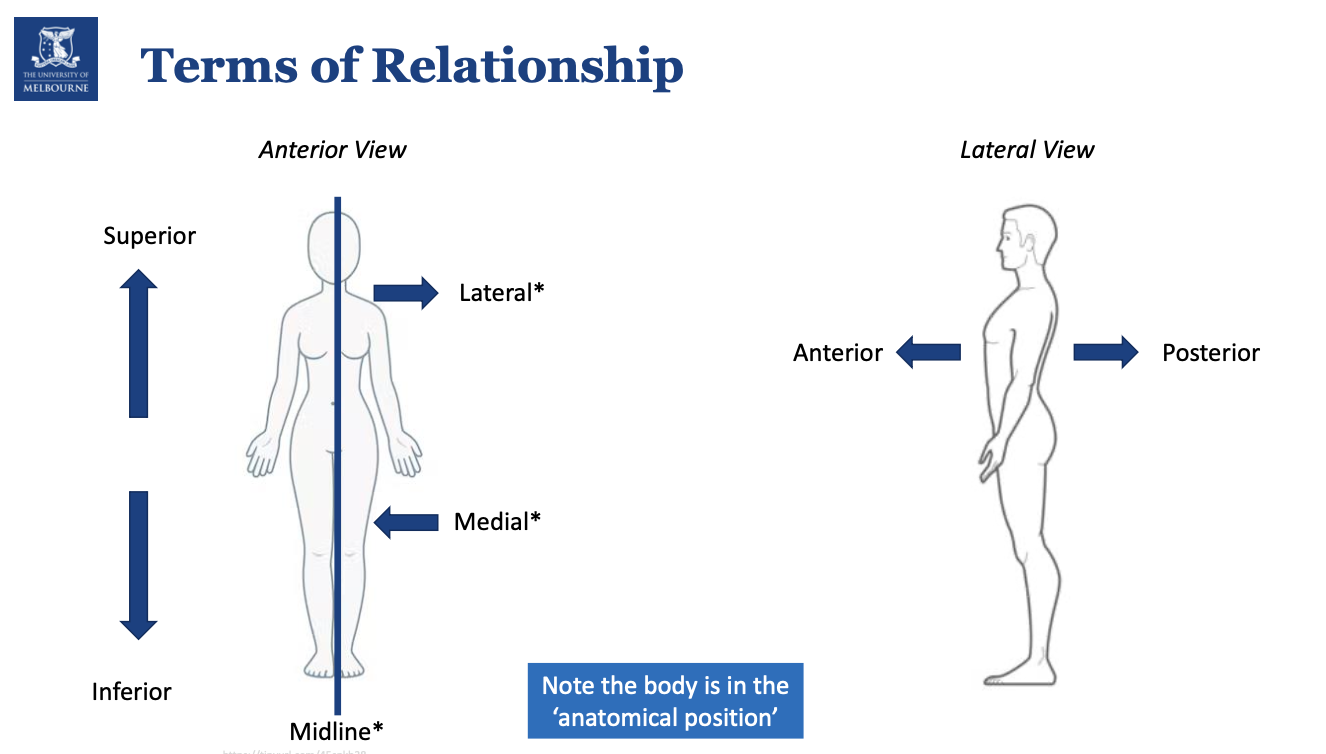
Diagram of common anatomical language
Terms of relationship
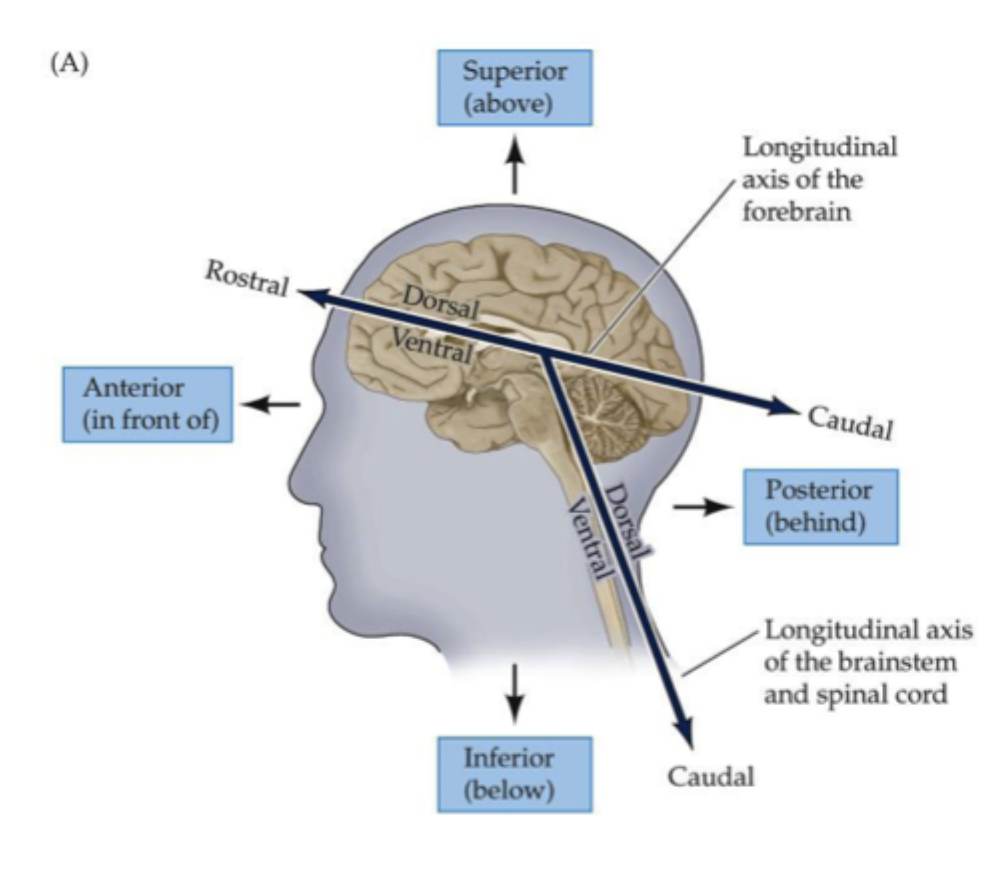
Rostro-caudal meaning?
Rostro-caudal = ‘neuroaxis’
Rostral = toward the beak/nose
Caudal = toward the tail.
*The neuroaxis is essentially vertical in humans but is rotated anteriorly at the rostral end.
Overview of CNS and PNS
The central nervous system (CNS) comprises the brain and spinal cord. The peripheral nervous system (PNS) is defined as the nerves connecting the central nervous system to the body (the periphery), and includes a number of neuronal clusters (ganglia) at specific locations along these peripheral nerves,
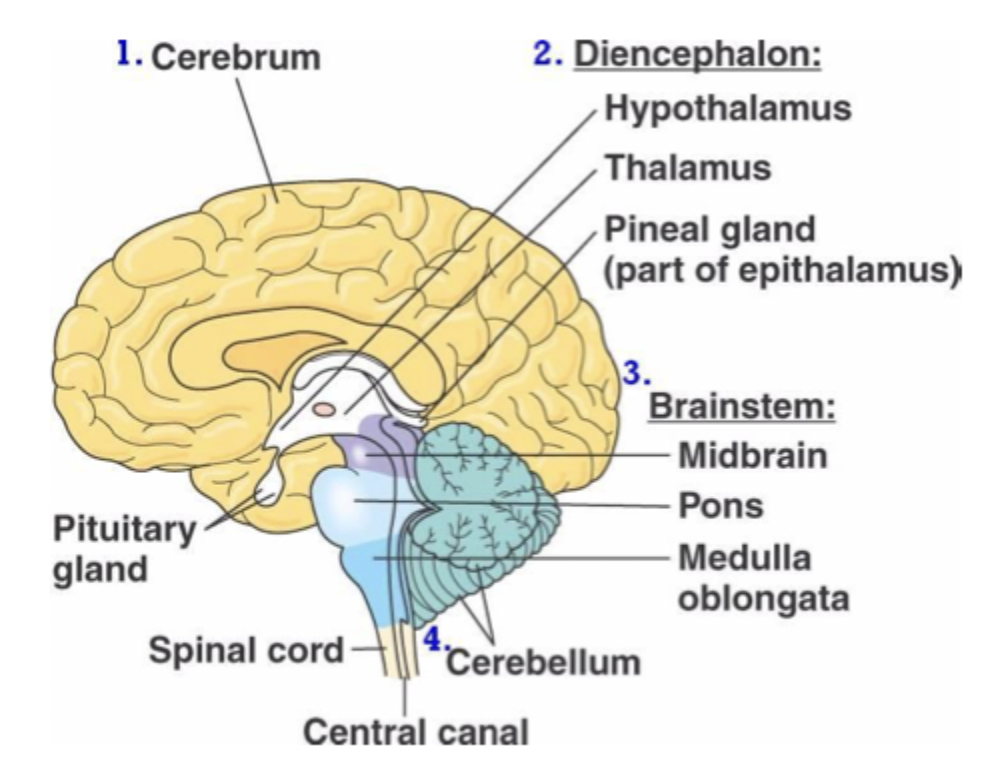
Major parts of the central nervous system (labelled BRAIN)
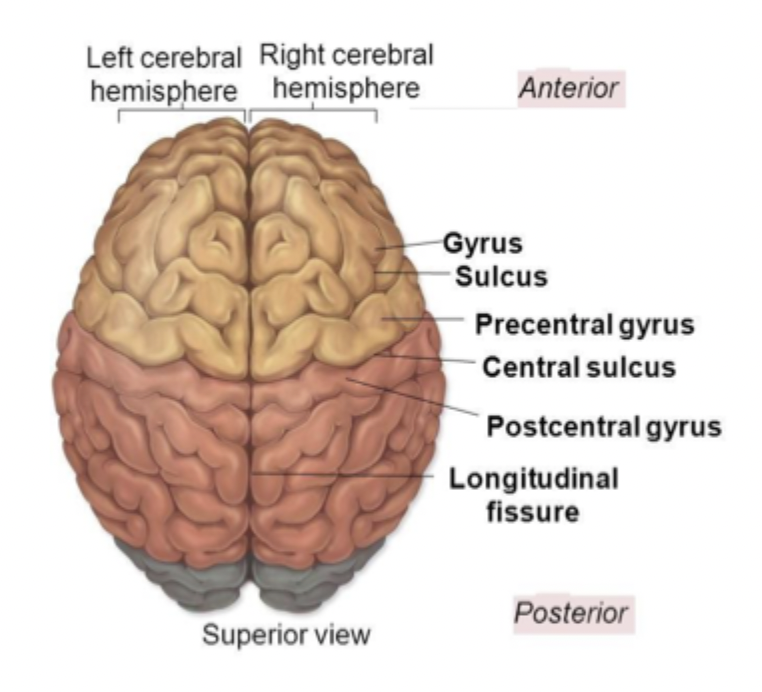
Gyri, sulci, and fissures
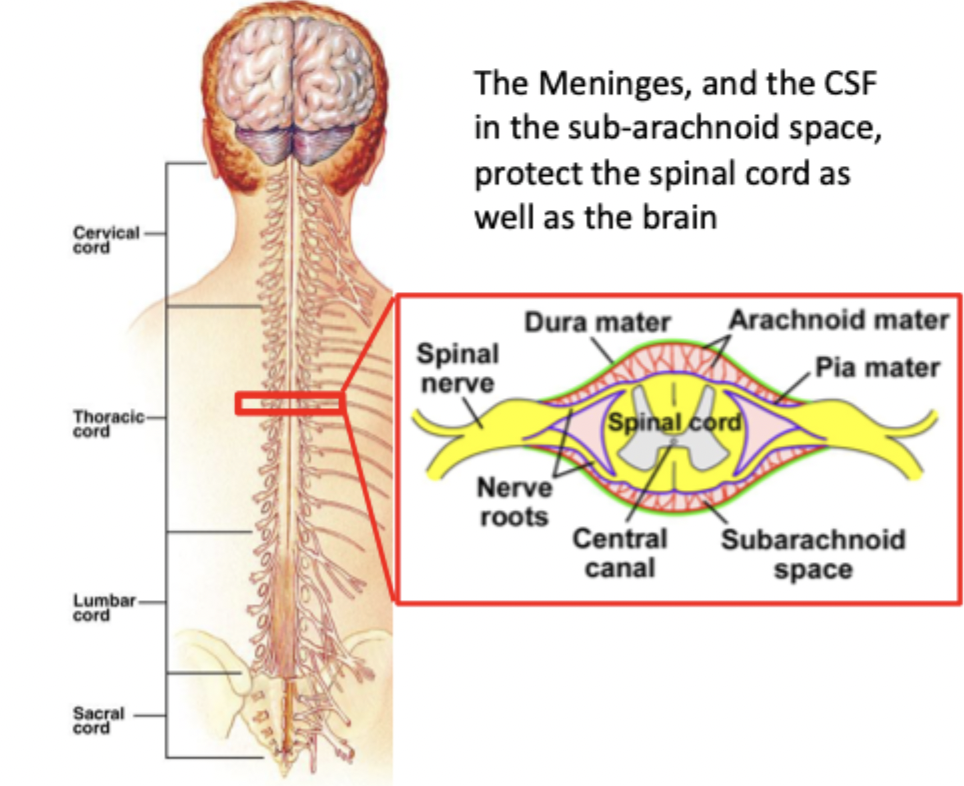
What are the three meninges?
The three meninges are the protective connective-tissue layers that surround the brain and spinal cord. They run from outermost to innermost as dura → arachnoid → pia.
Dura mater?
outermost, toughest layer
Two layers in the cranium: periosteal + meningeal.
Forms dural folds (falx cerebri, tentorium cerebelli) and venous sinuses.
Provides mechanical protection.
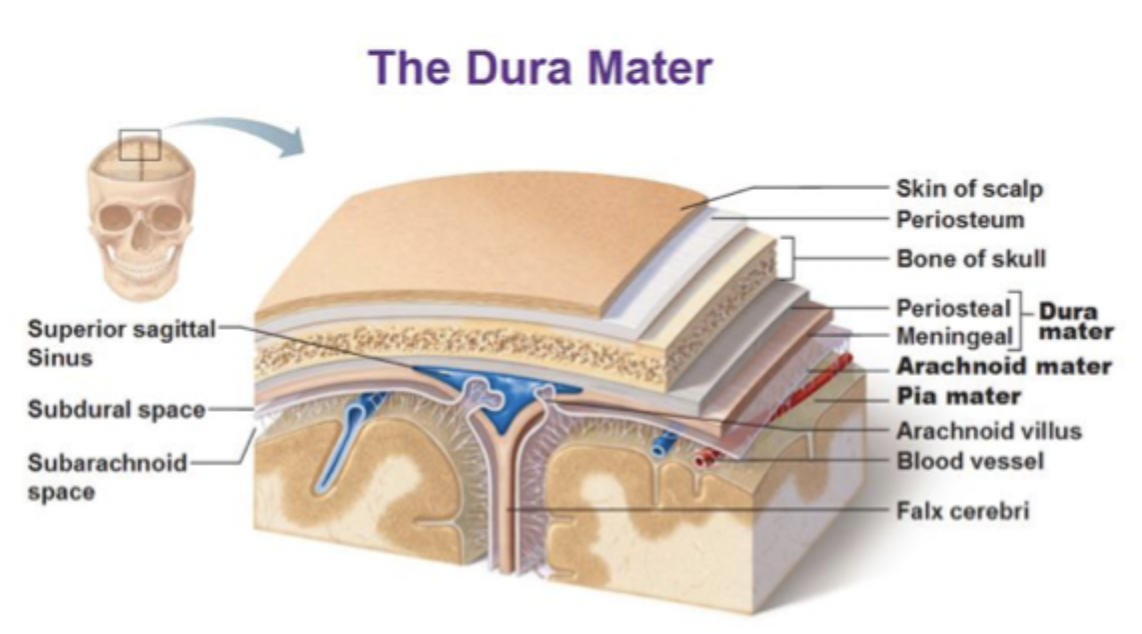
Arachnoid mater?
Middle layer, thin, avascular.
Has arachnoid trabeculae that span to the pia.
Creates the subarachnoid space, which contains CSF and cerebral vessels.
Subdural space lies between dura and arachnoid.
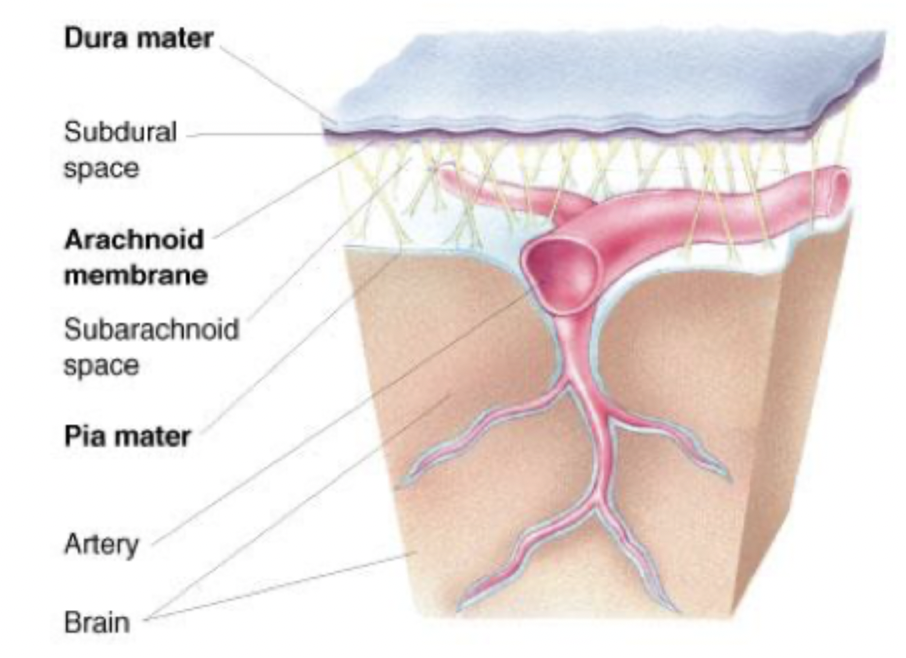
Pia mater
innermost, delicate layer.
Adheres tightly to the brain and spinal cord surface, following every sulcus.
Highly vascular; helps form the choroid plexus with ependymal cells.
Common CNS herniations?
Subfalcine:
Cingulate gyrus herniates under the falx cerebri.
Compression: anterior cerebral artery.
Contralateral leg weakness.
Transtentorial:
medial temporal lobe herniates through the tentorial notch.
Dilate pupil, fatal haemorrhages.
Tonsillar:
cerebellar tonsils herniate through the foramen magnum.
Compression: medulla.
Rapidly fatal respiratory arrest.
Diagram of meninges
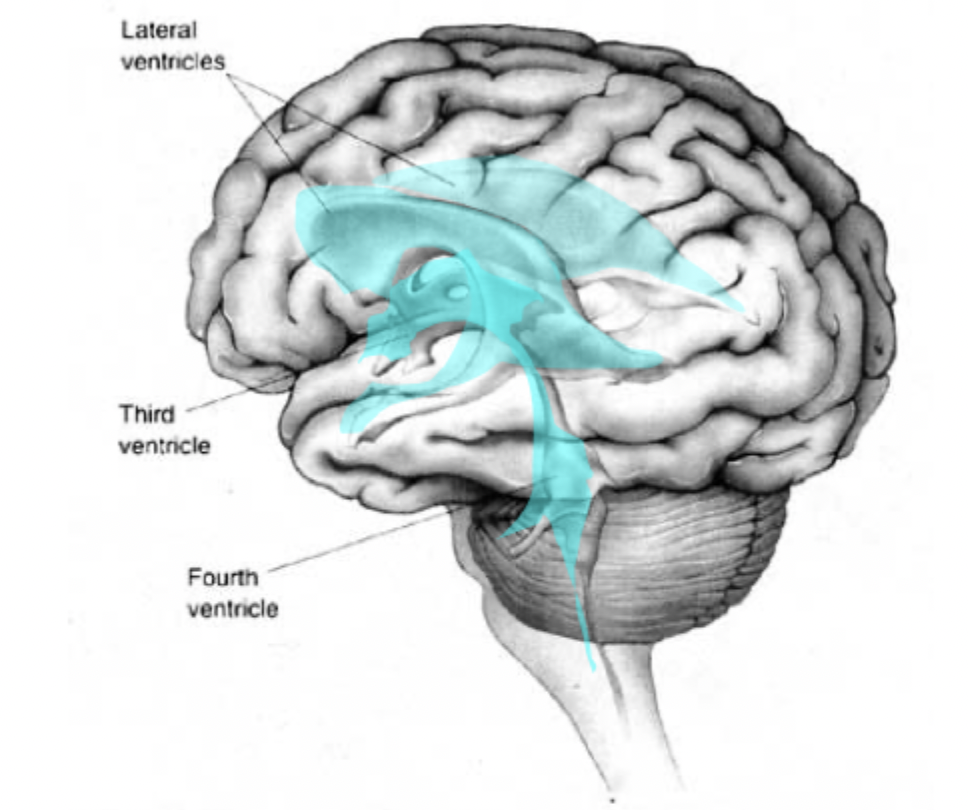
Where does CSF come from?
Cerebrospinal fluid (CSF) is inside the brain (ventricles) and surrounds the brain and spinal cord.
CSF is produced in the choroid plexus in the lateral, third, and fourth ventricles. CSF is reabsorbed by arachnoid granulations into the dural venous sinuses. Minor pathways include spinal nerve roots and lymphatics.
if not drained properly, a catheter is inserted. This drains CSF from the lateral ventricle into the peritoneal cavity to treat hydrocephalus.
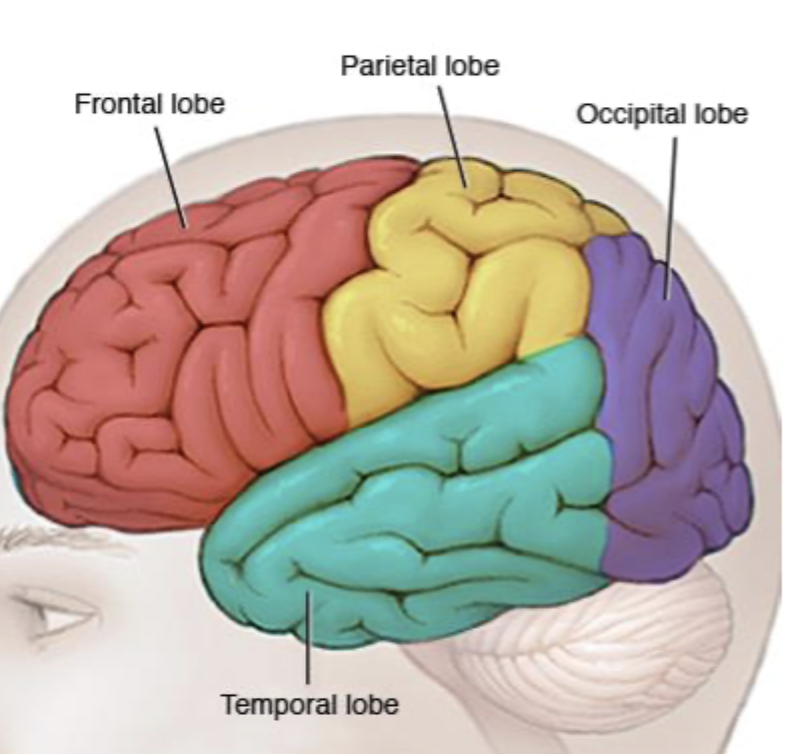
Lobes of the brain
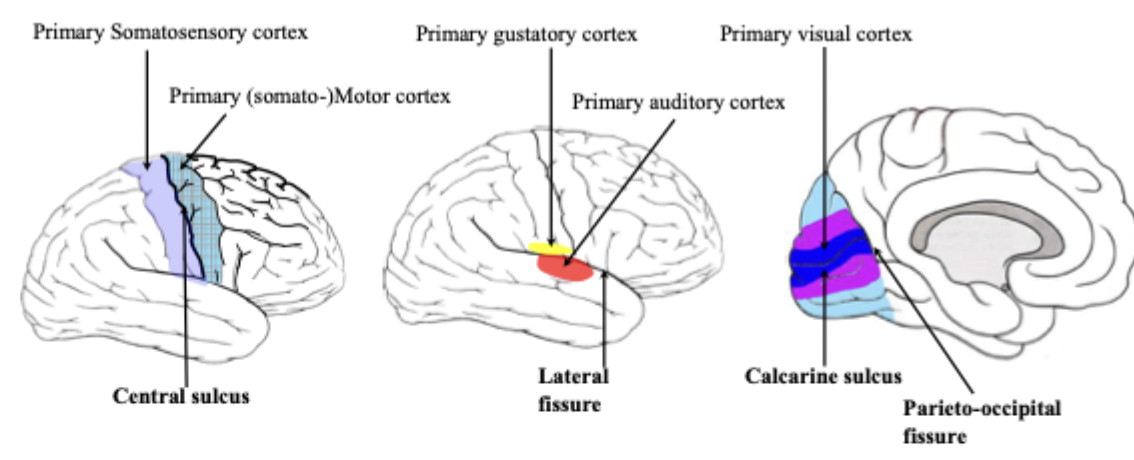
Organisation of the cerebral cortex
Most primary cortices are located around the deepest sulci/fissues such as:
The central sulcus: surrounded by primary somatomotor and somatosensory cortices.
The lateral fissure: surrounded by primary auditory and gustatory cortices.
The calcarine sulcus: surrounded by primary visual cortex.
*The central sulcus separates the frontal lobe from the parietal lobe. The primary somatomotor cortex is located in frontal lobe and is the centre for somatomotor output.
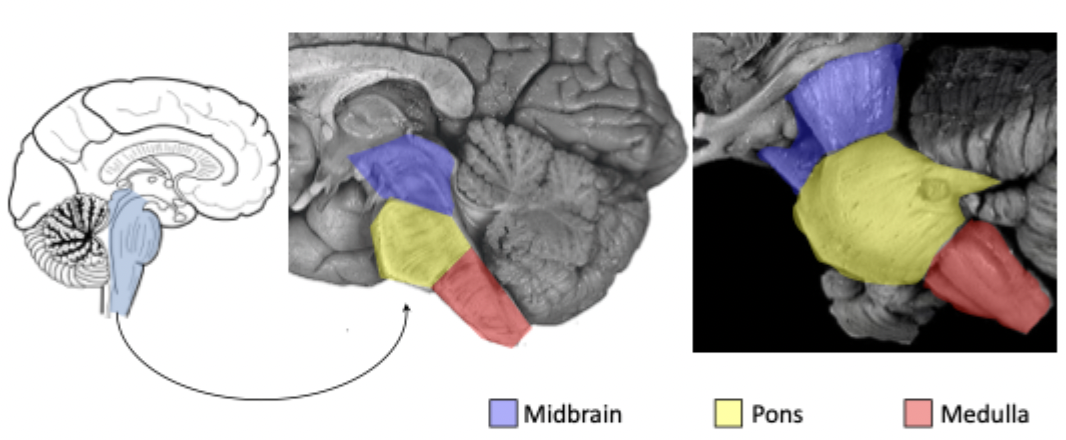
The brainstem?
Is located between the diencephalon (interbrain) and the spinal cord. Is composed of three major divisions:
Midbrain (=mesencephalon)
Pons
Medulla oblongata (=myelencephalon = bulbus)
Oligodendrocytes VS Schwann cells
Oligodendrocytes and Schwann cells both make myelin, but they do it in different nervous systems and with different structural rules.
Oligodendrocytes (CNS myelin)
Found in brain and spinal cord.
Once cell myelinates many axons.
Injury → poor regeneration (CNS cannot repair well).
Involved in multiple sclerosis
Do not have a basal lamina.
Collections = nuclei.
Bundles of axons = tracts.
Schwann cell (PNS myelin)
Found in peripheral nerves.
Once cell myelinates one axon segment.
Injury → good regeneration
Have a basal lamina.
Collections = ganglia.
Bundles of axons = nerves.
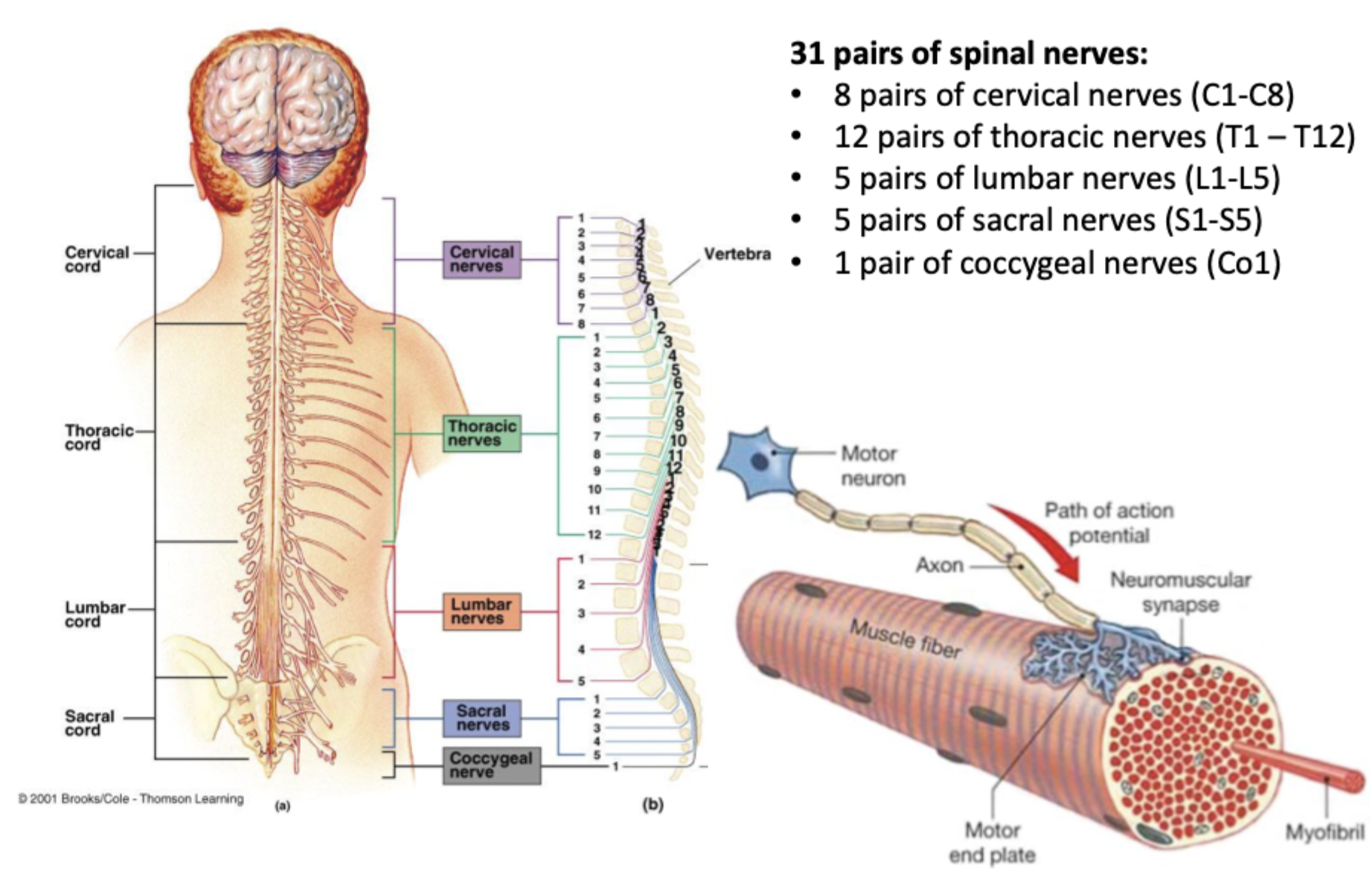
Diagram of the spinal nerves
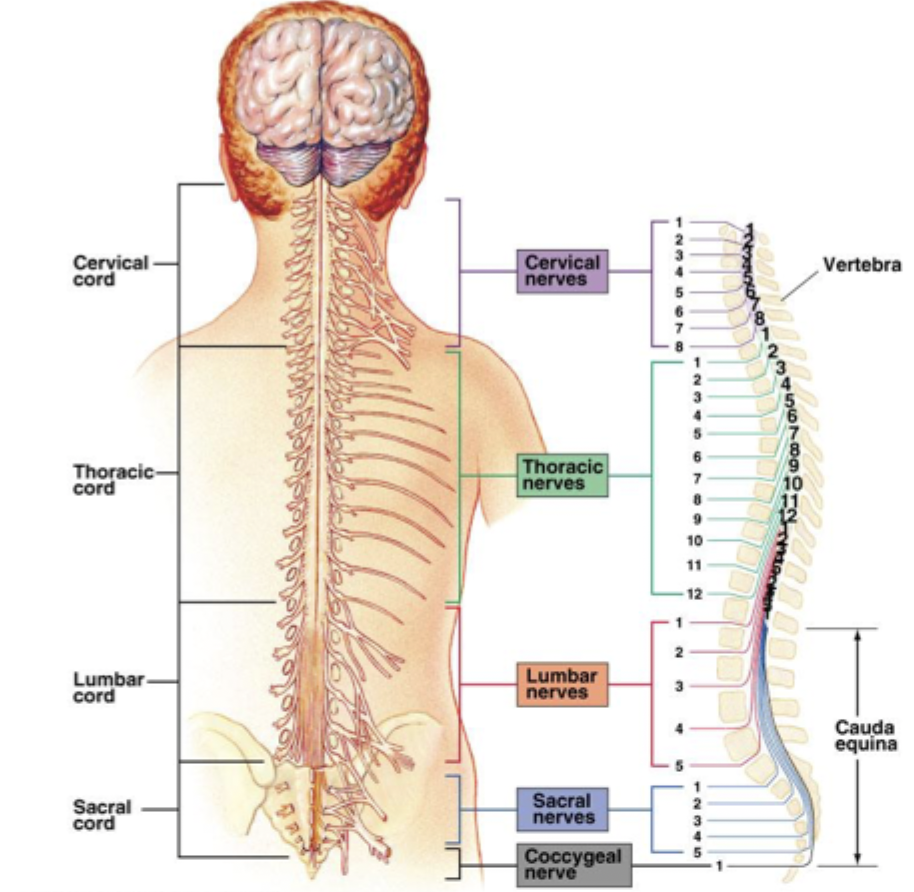
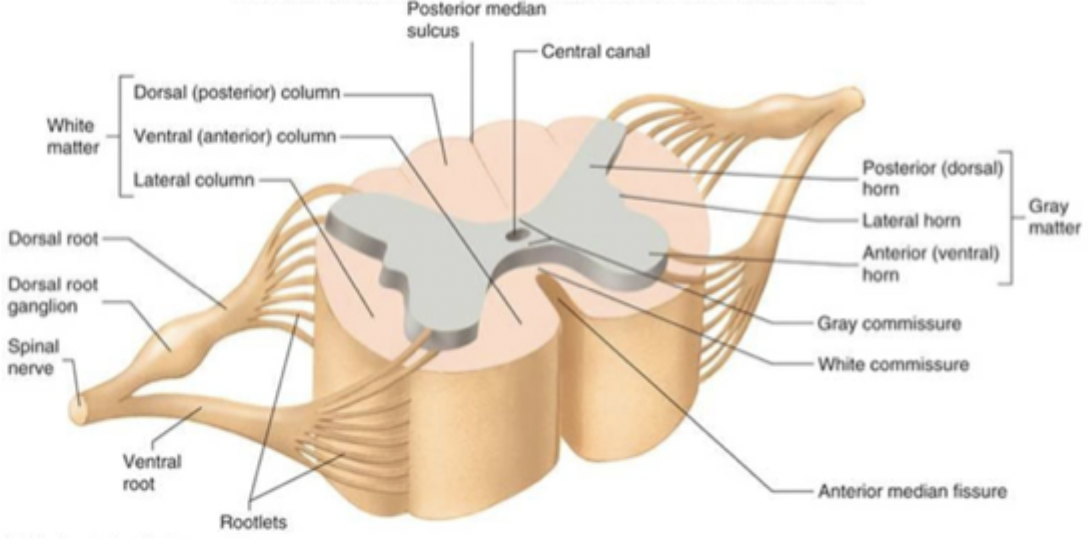
Diagram of one vertebra
*There are cervical (upper limbs) and lumbar (lower limbs) enlargements.
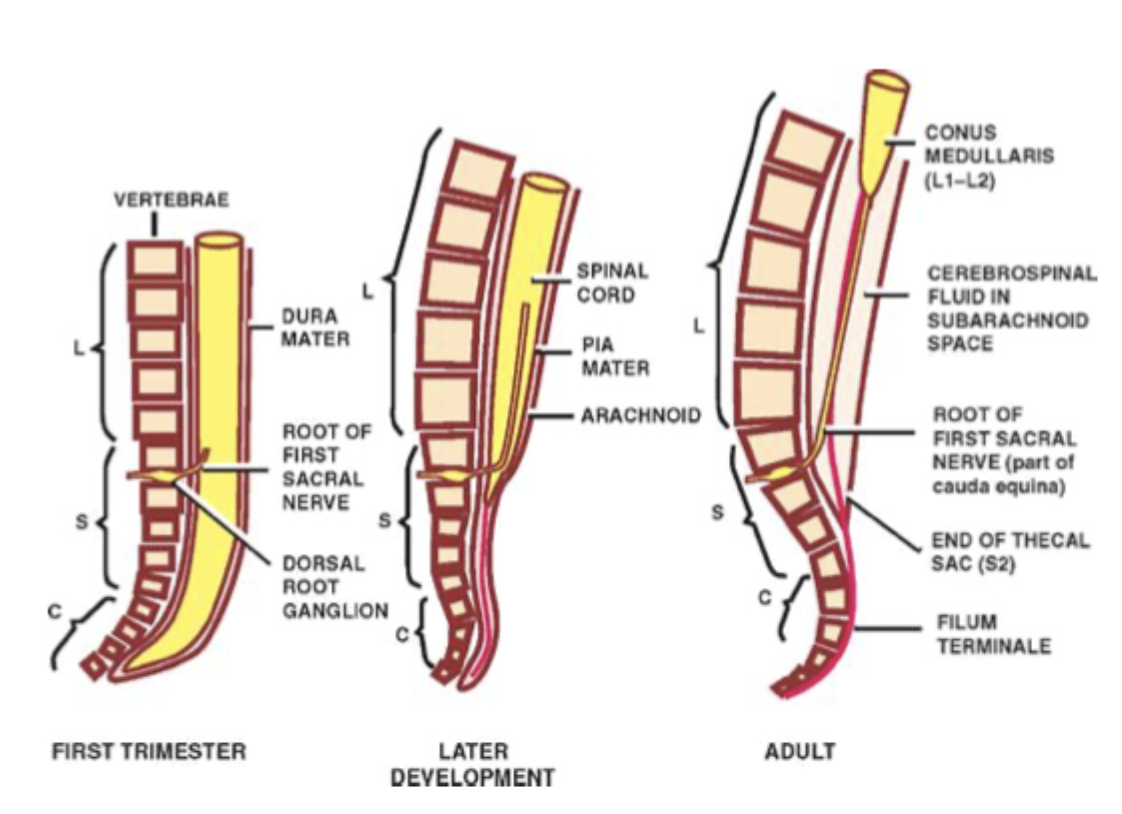
Spinal cord development
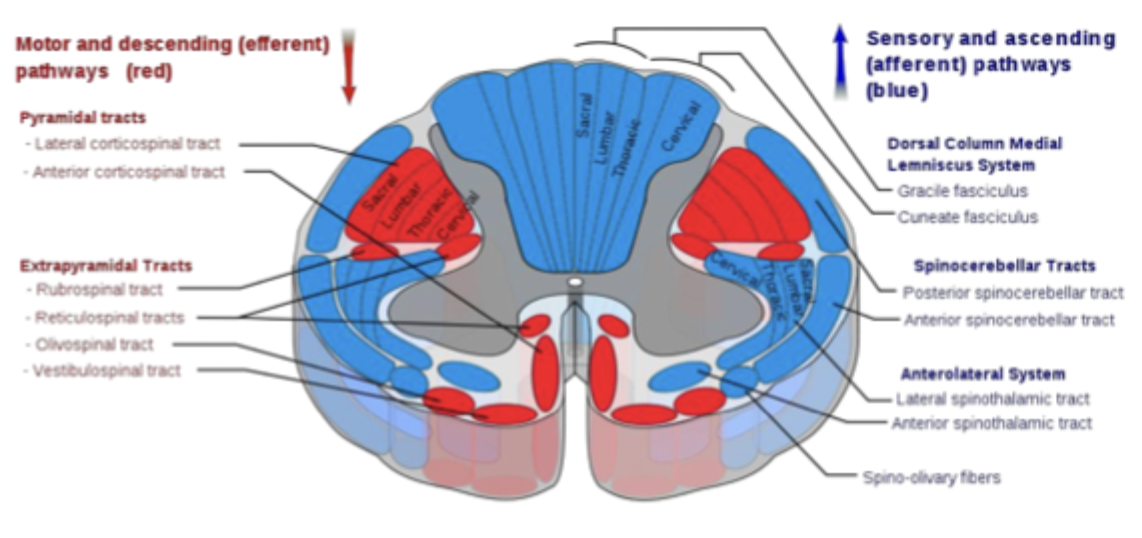
Spinal cord - whiter matter tracts diagram
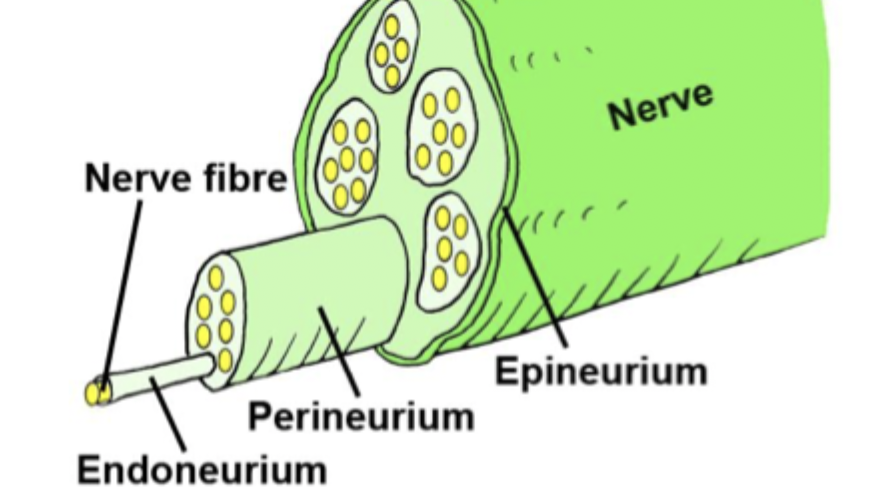
Periphery cluster
Axons in the periphery cluster together to form nerves - collections of thousands of individual axons within a common external connective tissue sheath (epineurium). Within the nerve axons are sub-grouped into fascicles, surrounded by a perineurial sheath.
Peripheral nerve axons can be either efferent (motor) carrying signals from the CNS or afferent (sensory) carrying signals to the CNS.
Separate spinal roots connect efferent and afferent to the CNS.
SENSORY axons join the CNS via a DORSAL (posterior) root.
MOTOR axons join the CNS at a VENTRAL (anterior) root.
Typical spinal segment
Spinal cord and spinal nerves diagram - how many pairs and what are they?
Rami
Rami = branches of a spinal nerve after it exits the intervertebral foramen. They are NOT the same as roots. Roots come into the spinal nerve; rami branch out of it.
Dorsal (posterior) ramus: supplies deep back muscles, facet joints, and skin of the back.
Ventral (anterior) ramus: much larger branch. Supplies limbs, anterolateral trunk, and forms major nerve plexuses: cervical, brachial, lumbar, sacral plexuses. Essentially, all limb innervation comes from ventral rami.
White rami: myelinated, preganglionic sympathetic fibres (T1-L2).
Grey rami: unmyelinated, postganglionic sympathetic fibres (all spinal levels)
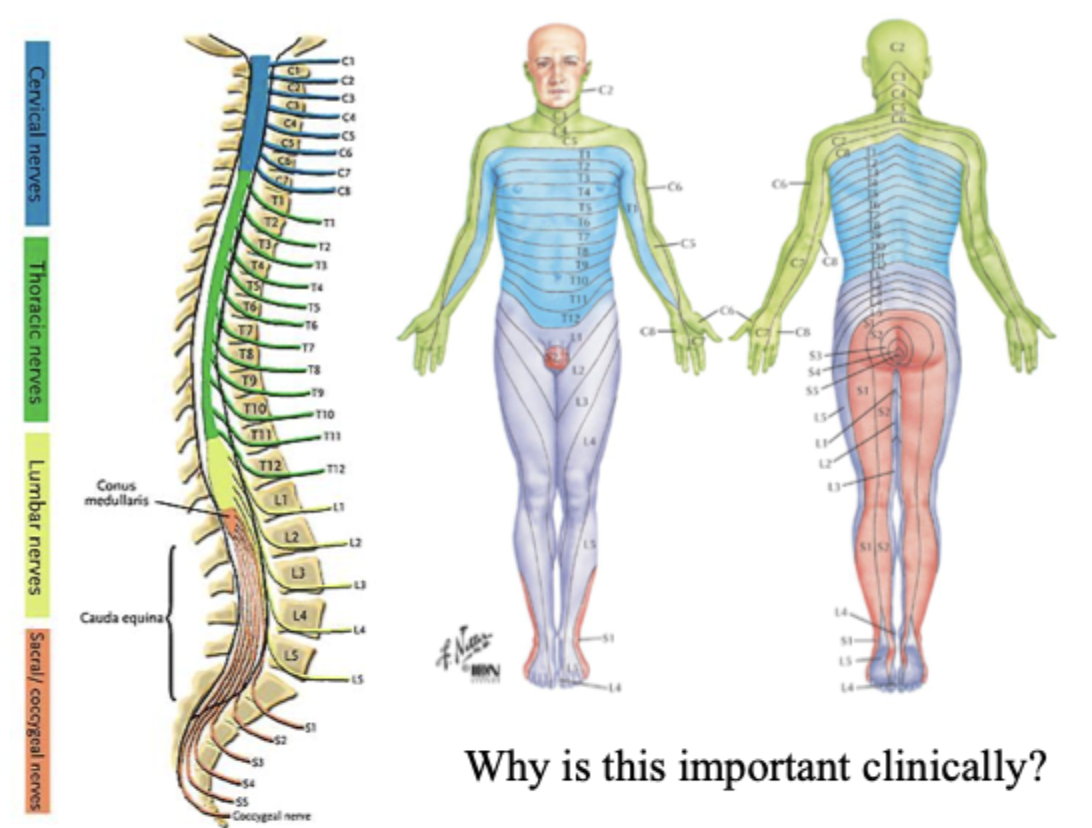
What does segmental innervation refer to?
A dermatome is an area of skin that is mainly supplied by a single spinal nerve. A myotome is the group of muscles that a single spinal nerve innervates.
*NOTE: a peripheral nerve is often comprised of multiple spinal nerves, i.e., several spinal segments contribute axons to a single peripheral nerve.
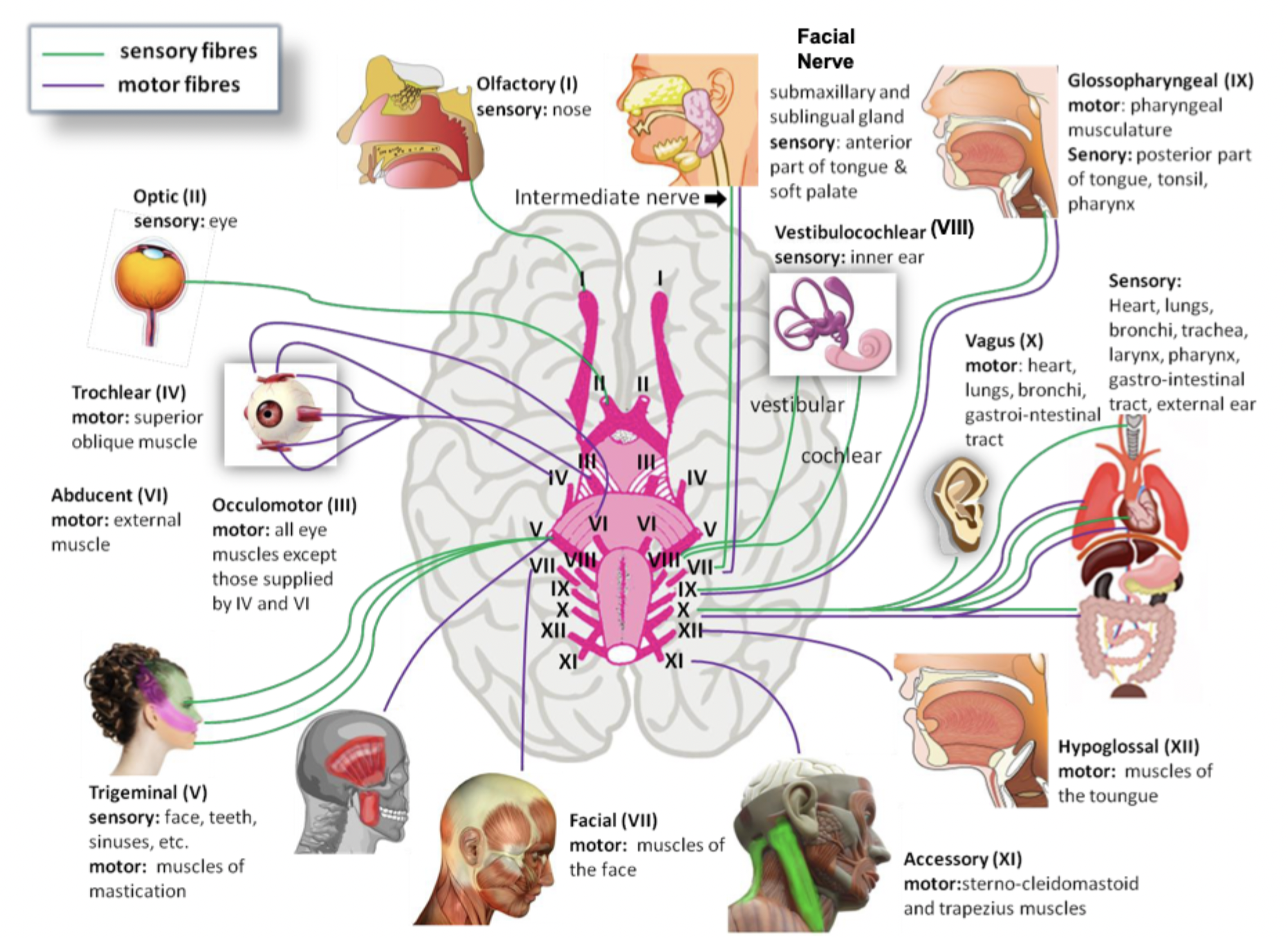
Cranial nerves
Somatic VS autonomic nervous system
Somatic = voluntary, skeletal muscle.
One neuron from CNS → muscle.
Neurotransmitter = ACh.
Receptor = nicotinic.
Effector = skeletal muscle.
Always excitatory.
Heavily myelinated.
Autonomic = involuntary, smooth muscle, cardiac muscle, glands.
Two-neuron chain: preganglionic and postganglionic.
Divided into sympathetic and parasympathetic.
Neurotransmitters: ACh, noradrenaline.
Receptors: muscarinic, adrenergic.
Can be excitatory or inhibitory.
Lightly or unmyelinated postganglionic fibres.
Sympathetic VS parasympathetic
Sympathetic
“fight or flight”
Thoracolumbar (T1-L2).
Short preganglionic, long postganglionic.
Noradrenaline at target.
Parasympathetic
“Rest and digest”
Craniosacral (Oculomotor nerve, facial nerve, glossopharyngeal nerve, vagus nerve).
Long preganglionic, short postganglionic.
ACh at both synapses.
Enteric division of the peripheral nervous system
A vast network of neurons embedded in the walls of the GI tract that controls motility, secretion, blood flow, and absorption. Does this via the myenteric and submucosal plexuses.
“Brain of the gut”
Parasympathetic → stimulates ENS.
Sympathetic → inhibits ENS.
Why study embryology?
Logical framework for understanding adult anatomy.
Provides information about many tissues: reproduction, contraception, stem cells, etc.
Informs about when things go wrong: birth defects, cancer.
Try to think about why each step is happening, to understand the consequence of when it goes wrong.
Periods of human embryology?
Conceptus: fertilisation to end of 2nd week.
Embryo: beginning of 3rd week to end of 8th week.
Foetus: 3rd month to birth.
Ovulation to implantation stages (6 steps)
Ovulation: a secondary oocyte is released from the ovary and swept into the oviduct.
Fertilisation: a single sperm penetrates the secondary oocyte. Eventually, the sperm and egg nuclei will fuse, resulting in a fertilised egg, or zygote.
Cleavage: the zygote soon undergoes rapid mitotic cell divisions as it moves along the oviduct toward the uterus, becoming a pre-embryo that consists of two cells, then four, etc.
Morula: By day 4, successive divisions produce a morula, a solid ball of cells that enters the uterus.
Blastocyst: by day 6, the pre-embryo becomes a blastocyst, a hollow ball of cells with a fluid-filled cavity. The blastocyst has freed itself from the zona pellucida and can increase in size.
Implantation: the blastocyst attaches to the uterine lining (endometrium) and begins to digest its way inward. The cells of the inner mass begin to form primary germ layers.
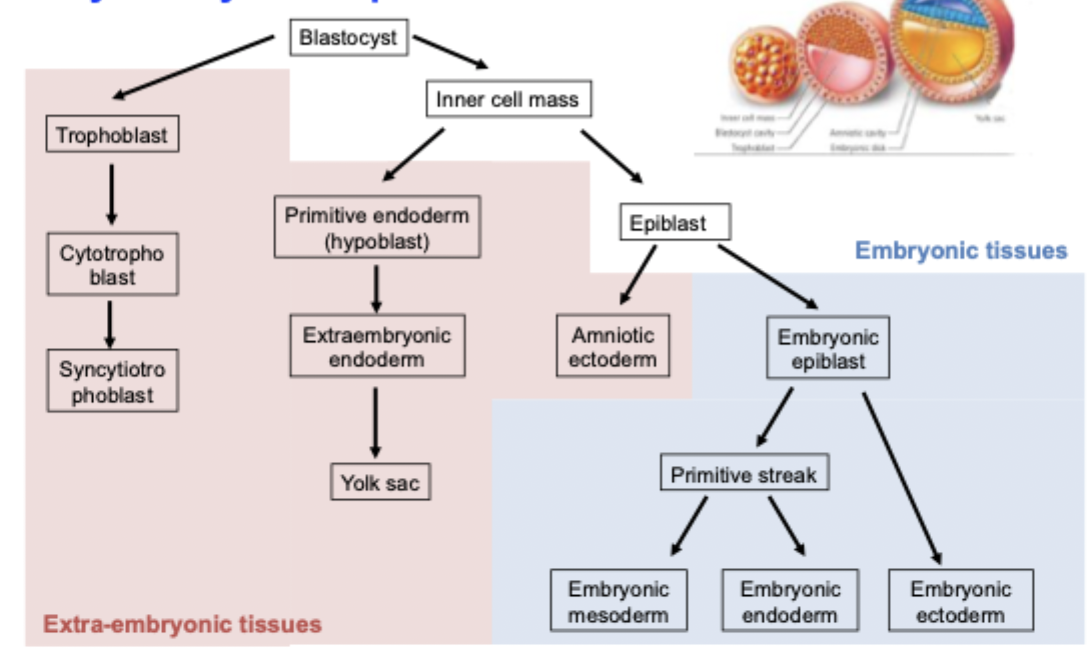
Blastocyst
Cavitation enables two types of cells to be formed:
Outer epithelial layer (trophoblast, will go on to form the extra-embryonic structures).
Inner cell mass (will go on to form the embryo itself.
Between 5-10 days, blastocyst implants into uterine wall.
Two germ layer stage
Morula: solid ball of cells formed as the zygote undergoes cleavage.
Early blastocyst: hollow ball of cells with a fluid-filled cavity.
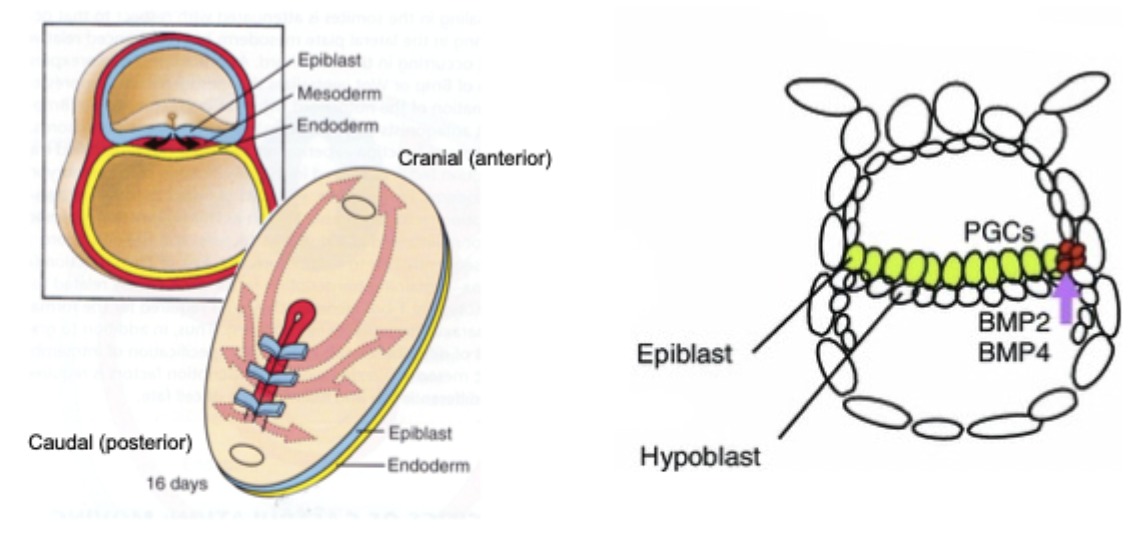
Pre-embryo: with the embryonic disc, two layers of cells that become the embryo proper. Top layer = epiblast (with amniotic cavity in its cavity), bottom layer = hypoblast (with yolk sac in its cavity)
Gastrulation - formation of primitive streak
On the upper surface of the bilaminar disc (on epiblast), a line of thickened cells appear (primitive streak). The primitive streak invaginates to form primitive groove.
Cells of epiblast migrate medially and into primitive groove.
First cells move into hypoblast to form embryonic endoderm.
Later cells move into space between epiblast and endoderm become embryonic mesoderm.
Cells left in epiblast become embryonic ectoderm.
= Three layer stage
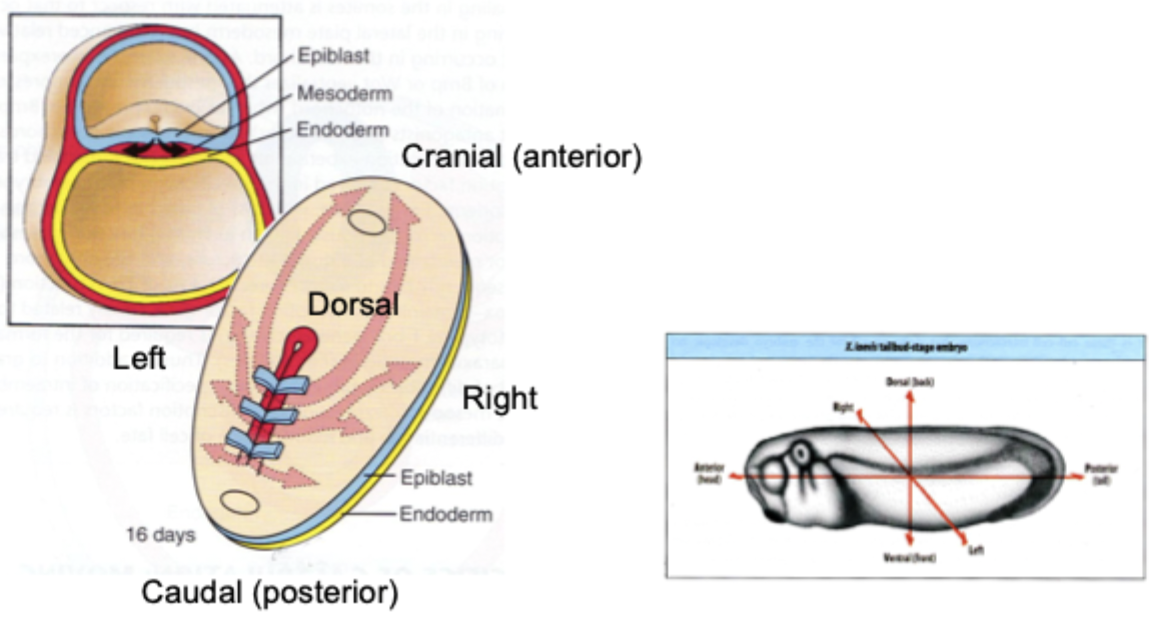
Embryonic body axis
*The node establishes left-right asymmetry, through:
Mechano-sensor.
Cilia on left bend due to fluid moving towards them.
Increased Ca2+ = signal in the cell.
What happens if the node goes wrong?
SITUS INVERTUS
Organs are mirrored from their normal position.
Only some organs or partial: situs ambiguus or heterotaxis.
Often associated with other problem, especially heart defects.
Summary diagram of early development
Notochord formation
A solid rod of mesoderm that forms along the embryo’s midline. It defines the cranial-caudal axis, and induces formation of the neural tube.
Primitive streak forms:
Epiblast cells migrate inward during gastrulation, creating the primitive streak in the dorsal surface.
Cells ingress to form axial mesoderm:
cells move through the primitive node and migrate cranially in the midline.
Notochordal process forms
A hollow tube of mesodermal cells extends forward between ectoderm and endodern.
Notochordal plate forms
The floor of the notochordal process fuses with underlying endoderm → the roof flattens into a plate.
Notochordal plate infolds
The plate folds upward and detaches from the endoderm.
Definitive notochord forms
the infolded plate seals into a solid rod of axial mesoderm - the notochord.
Notochord induces neural tube:
Releases SHH (Sonic hedgehog) → induces overlying ectoderm to form the neural plate, then neural tube.
Notochord patterns ventral surfaces
SHH patterns motor neurons, floor plate, and sclerotome.
Most notochord degenerates
Vertebral bodies form around it; only the nucleus pulposus remains in adults.
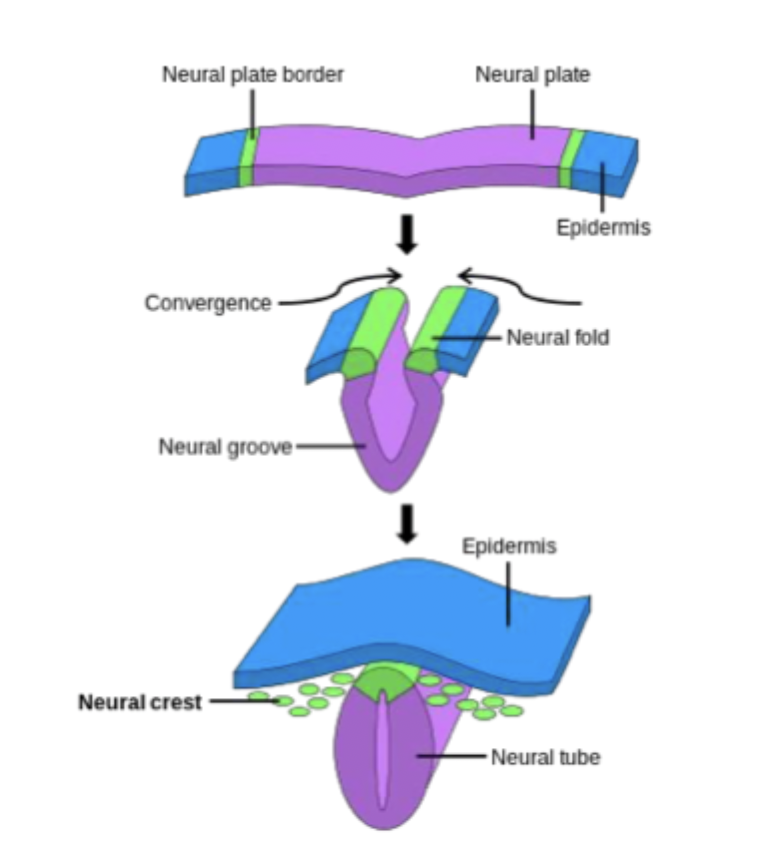
Neural crest cells
Neural crest cells are ectoderm-derived cells that originate at the neural plate-surface ectoderm border. When the neural tube closes, these cells delaminate and migrate along defined pathways.
Give rise to:
Dorsal root ganglia.
Enteric ganglia.
Schwann cells.
Melanocytes.
Sympathetic and parasympathetic ganglia.
Dentine
Segmentation of neural tube
Neural tube initially one cell layer thick and hollow. Cranial end starts to swell, forming vesicles. Vesicles give rise to brain. The remainder gives rise to spinal cord.
Development of skin
Two layers: epidermis and dermis.
Epidermis: from embryonic ectoderm, colonised by melanocytes (neural crest) and Langerhans cells (immune cells from bone marrow).
Dermis: mesodermal (except face: neural crest).
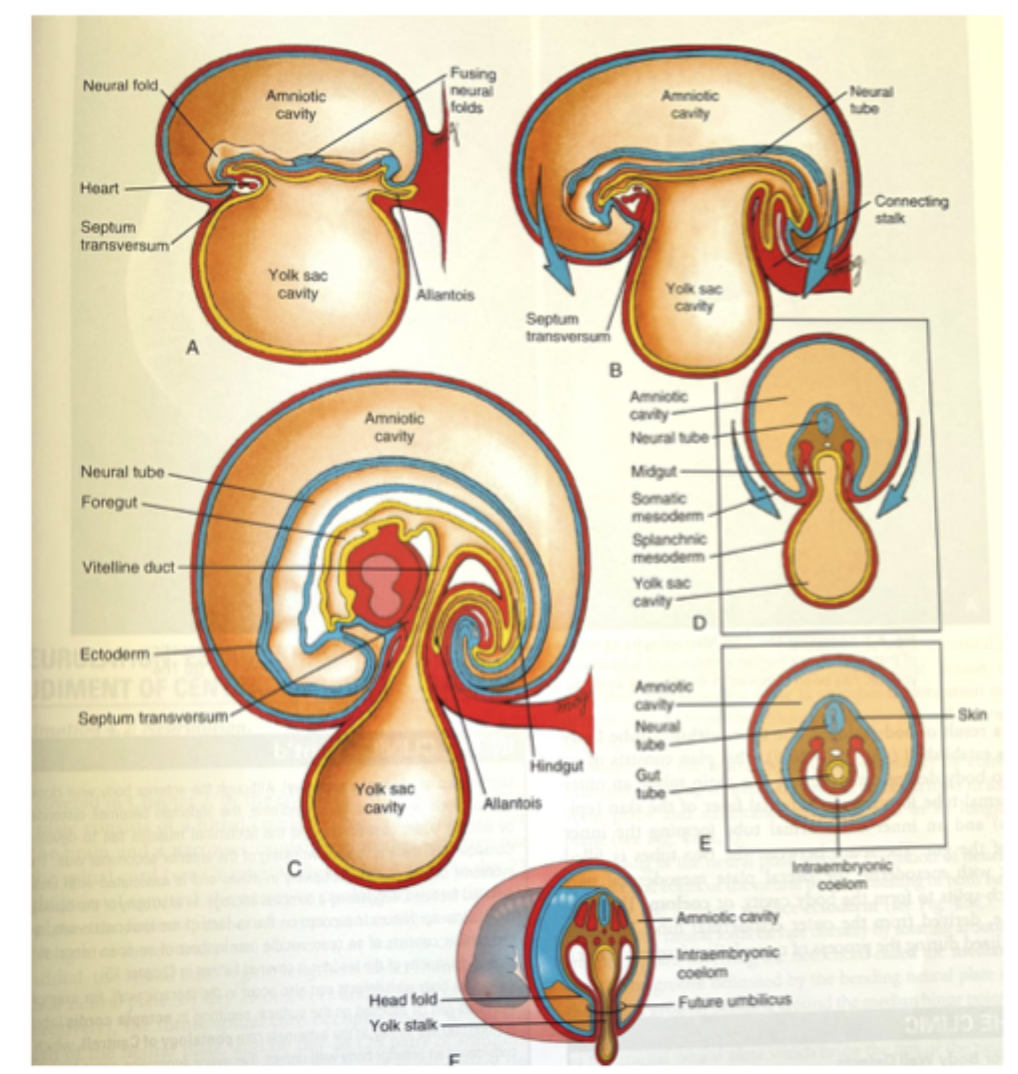
Body folding
End of third week: embryo is flat, ovoid, trilaminar disc (ectoderm, mesoderm, and endoderm).
Fourth week:
Embryo grows rapidly, especially in length.
Process of folding to generate body form.
Main force: differential growth of various tissues.
Embryonic disc and amnion: high growth rate.
Yolk sac: almost no growth.
Developing notochord, neural tube, and somites stiffen dorsal axis.
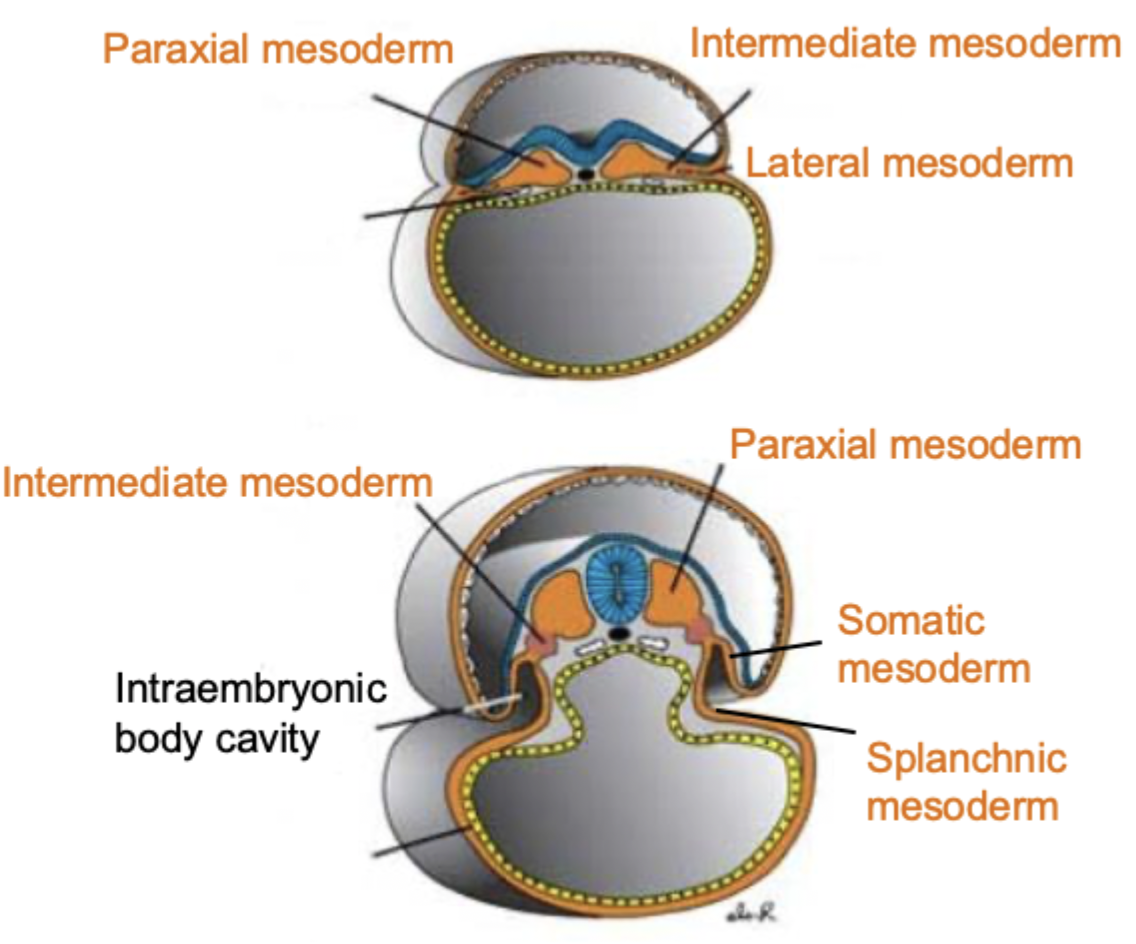
What is the mesoderm subdivided into?
Divided into:
Paraxial mesoderm.
Intermediate mesoderm.
Lateral mesoderm.
Fate of the paraxial mesoderm
IN GENERAL: dermis of skin, axial skeleton, and axial and limb muscles.
In head region form head mesoderm: future muscles of face, jaw, and throat. In trunk region form somites (future muscle, bone, and dermis).
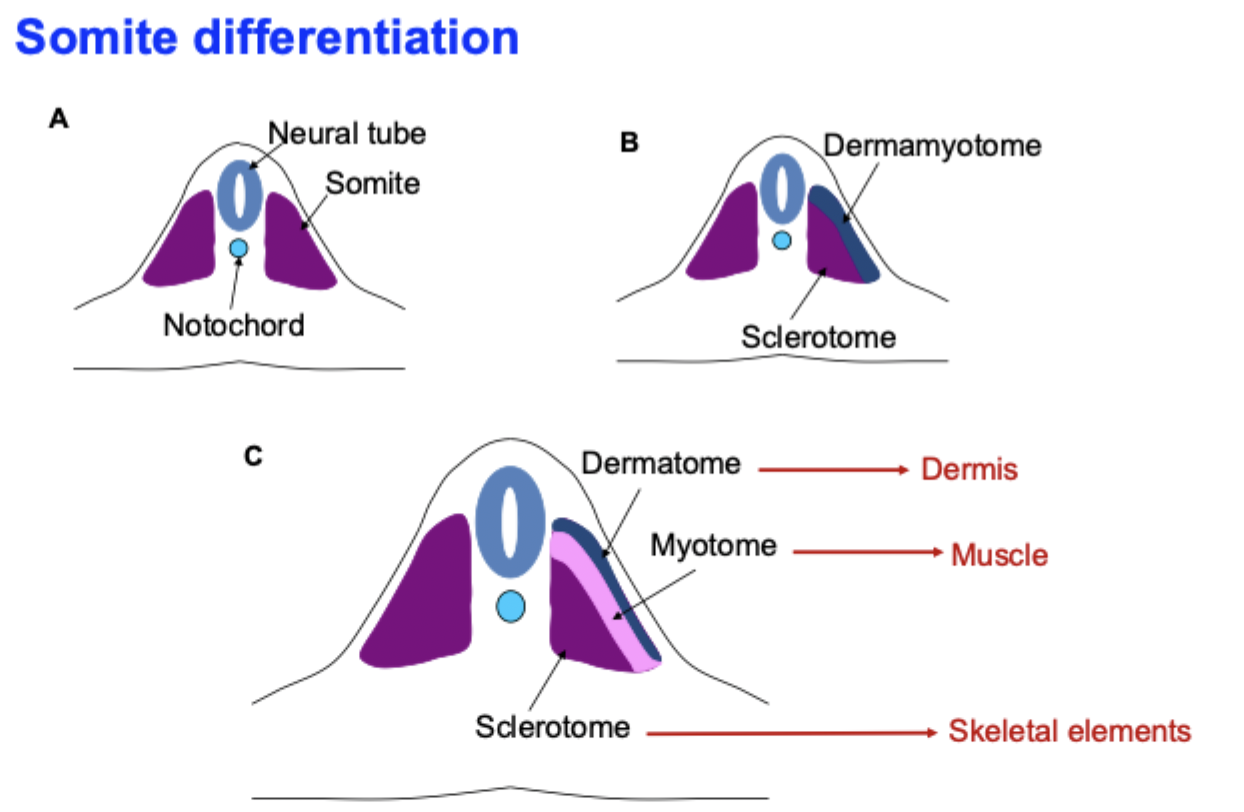
Somitogenesis?
Somitogenesis is the sequential segmentation of paraxial mesoderm into somites along the anterior-posterior axis, providing the template for vertebrae, ribs, skeletal muscle, and dermis.
Formation of paraxial mesoderm from primitive streak:
Gastrulation produces paraxial mesoderm on either side of the notochord and neural tube.
This unsegmented tissue is called presomitic mesoderm.
Establishment of anterior-posterior pattern and gradients.
Cells undergo mesenchymal → epithelial transition (MET) and pinch off as a new somite.
Somite splits into compartments - signals from nearby tissues tell each somite what to become:
Sclerotome → vertebrae and ribs.
Myotome → skeletal muscle.
Dermatome → dermis of the back.
Fate of the intermediate mesoderm?
The urogenital system:
Kidneys, gonads, respective duct systems.
Development of reproduction system and sex determination
The intermediate mesoderm forms a longitudinal ridge, called the urogenital ridge.
CHROMOSOMES DECIDE THE PLAN
XX → No Y → no SRY.
XY → Y present → SRY ON.
Gonads choose the fate. Early embryo has an indifferent gonad (urogenital ridge).
SRY present (XY) → gonad becomes a testis.
No SRY (XX( → gonad becomes an ovary.
Testis make two hormones: AMH and testosterone.
Internal ducts start the same in everyone
Wolffian ducts and Müllerian duct.
If AMH and testosterone present, AMH degrades the Müllerian duct. The testosterone allows the Wolffian duct to survive and develop into epididymis, vas deferens, and seminal vesicles.
If no AMH and no testosterone, the Müllerian duct will stay, allowing it to form into the uterus, fallopian tubes, and the upper vagina. No testosterone degenerates the Wolffian ducts.
Fate of the lateral mesoderm?
Will become the cardiovascular system, smooth muscle, body cavity linings, connective/skeletal tissues.
The lateral mesoderm is divided into the somatic (parietal) and splanchnic (visceral).
SOMATIC: (adjacent to the ectoderm). Will form the body wall, limbs, sternum, parietal serous membranes.
SPLANCHNIC: (adjacent to the endoderm). Will form heart, blood vessels, smooth muscle and connective tissue of the gut wall, visceral serous membranes.
Vasculogenesis
- Formation of new blood vessels from SCRATCH during early embryogenesis.
Mesoderm forms in the embryo.
Mesoderm cells become hemangioblasts.
Hemangioblasts form blood islands (cluster of cells appear in the mesoderm).
Differentiate into angioblasts + blood cells (outer cells → angioblasts, inner cells → primitive blood cells).
Angioblasts line up to form tubes.
Primary plexus remodels into major vessels.
Angiogenesis
Growing from existing vessels.
Existing vessels sense a need for more blood supply (especially VEGF or hypoxia).
Endothelial cells are activated.
Endothelial cells extend buds/sprouts.
Sprouts form new endothelial tubes.
Stabilisation and maturation (pericytes and smooth muscle cells are recruited; basement membrane is laid down).
Network is pruned and remodelled (a refined vascular network).
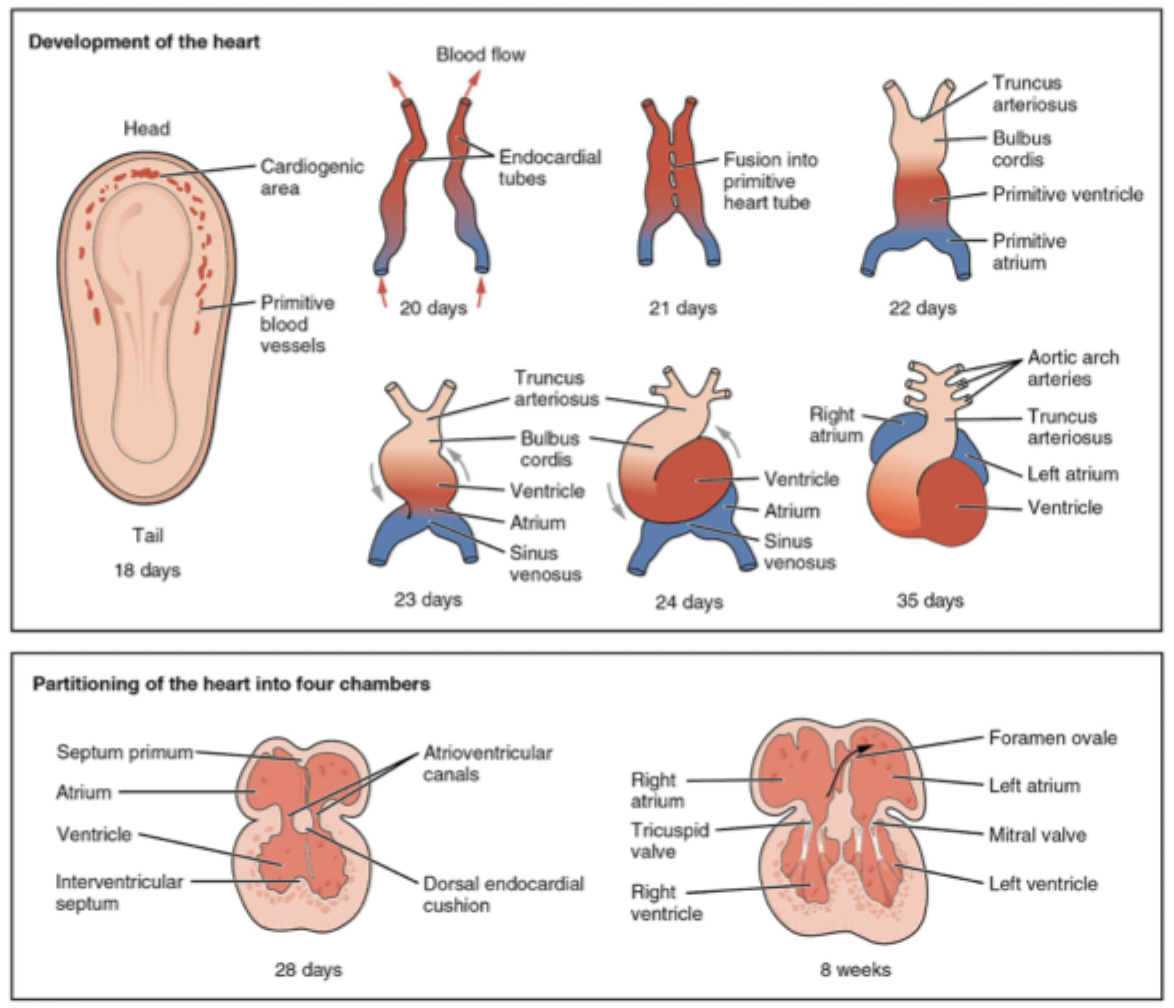
Development of the heart
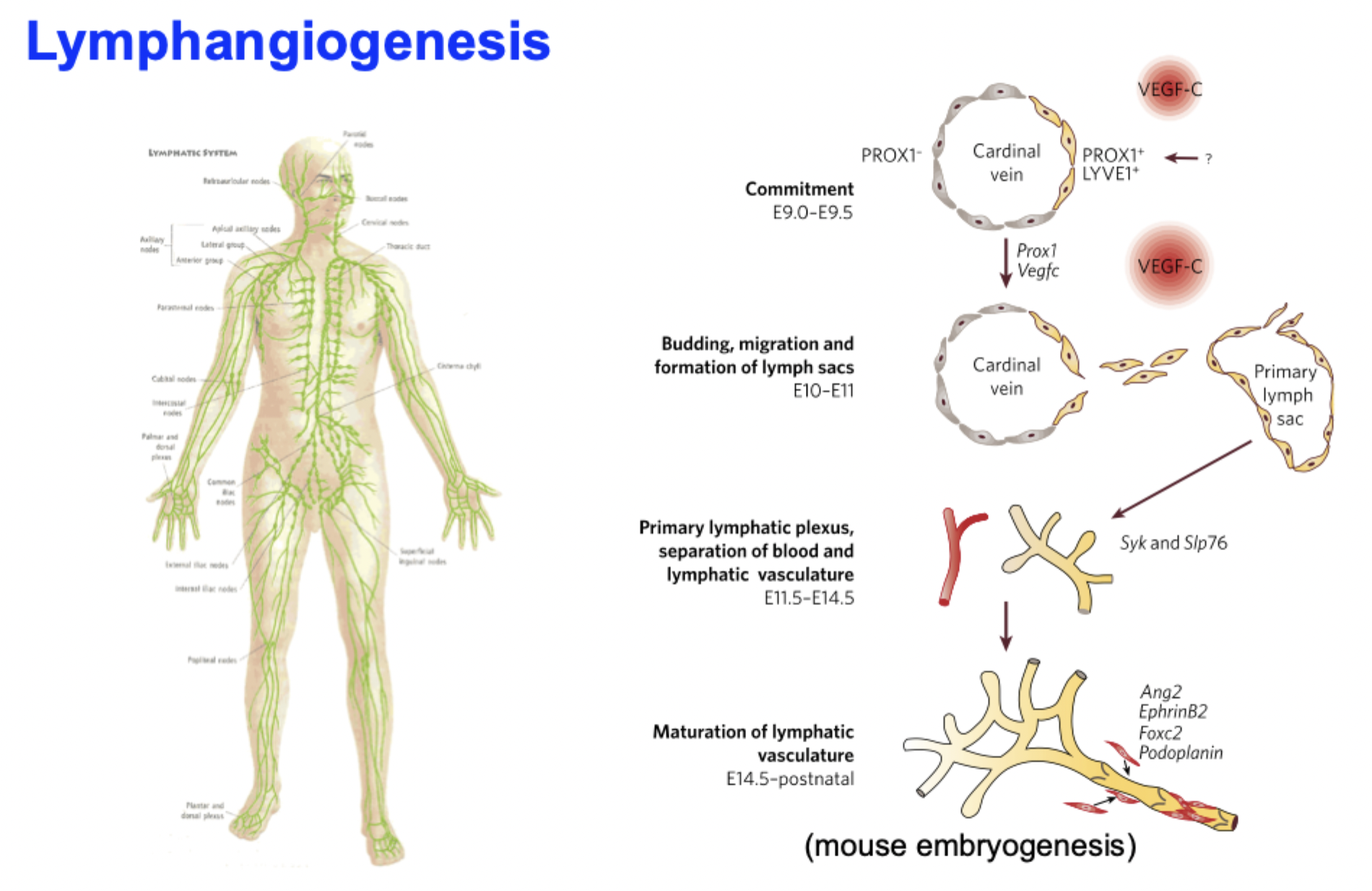
Lymphangiogenesis
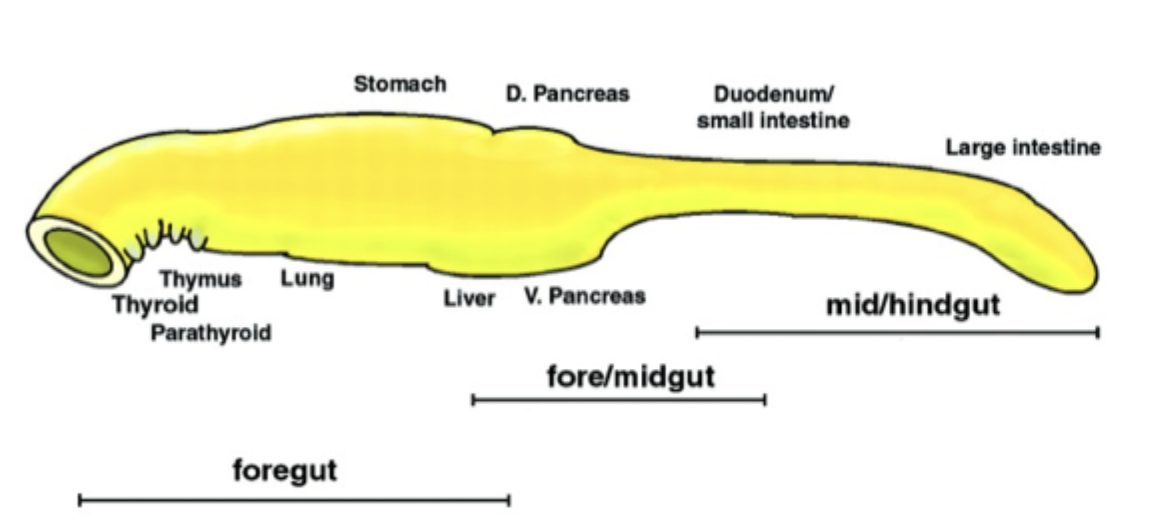
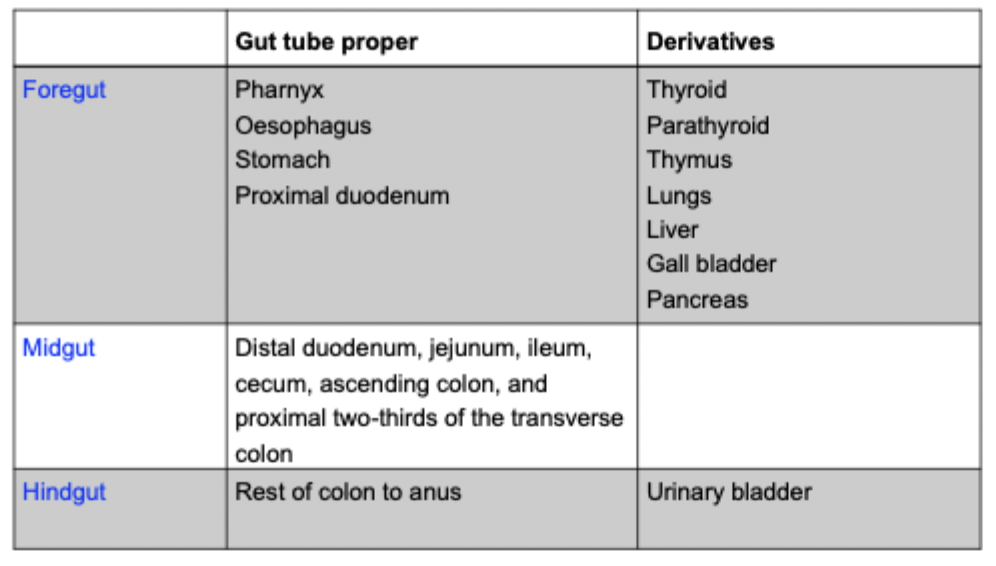
What does the endoderm become?
Important for inducing formation of mesodermal organs (e.g., heart, blood vessels).
forms lining of digestive tract.
Digestive tract = whole length of the body.
Buds off liver, gall bladder, pancreas, lungs.
Cranial part (anterior of lungs): pharynx.
Epithelial pockets of pharynx: thyroid, thymus, and parathyroid.
What occurs during embryo folding?
End of third week: embryo is flat, ovoid, trilaminar discs (ectoderm, mesoderm, endoderm).
Fourth week:
Embryo grows rapidly, especially in length.
Process of folding to generate body form.
Main force: differential growth of various tissues:
Embryonic disc and amnion: high growth rate.
Yolk sac: almost no growth.
Developing notochord, neural tube, and somites stiffen dorsal axis.
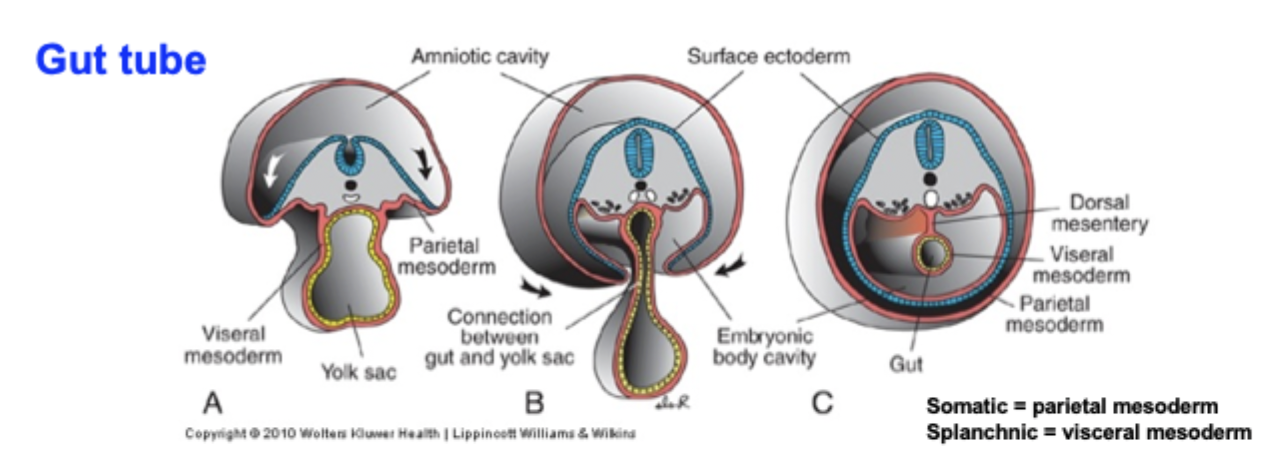
Gut tube formation?
Lateral folding of the embryo completes the gut tube. With lateral folding, mesoderm is recruited to gut wall. Mesodermal layer of the gut tube from splanchnic mesoderm. Somatic mesoderm lines body cavity.
start with the trilaminar embryo: after gastrulation, you have endoderm (inside), mesoderm, and ectoderm (outside). The endoderm will form the epithelium of the gut and its derivatives.
Embryo folds in the median (head-tail) plane: Cranial (head) folding bends the cardiogenic region and endoderm into a blind-ended tube (creates the foregut). Caudal (tail) folding does the same at the caudal end (forms the hindgut).
Lateral folding closes the ventral body wall: the embryo folds from both sides towards the midline. The endodermal sheet is rolled into a tube, and the yolk sac is pinched, leaving a narrow connection.
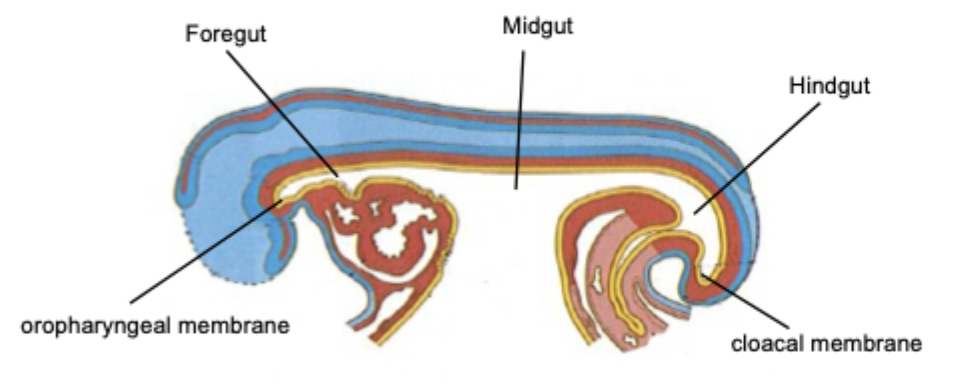
Continuous primitive gut tube is formed: the endoderm now forms a single continuous tube from cranial to caudal: foregut (cranial), midgut (open to yolk sac), hindgut (caudal).
Mesoderm invests the tube: splanchnic mesoderm surrounds the endodermal tube → forms gut wall connective tissue, smooth muscle, and visceral peritoneum. Somatic mesoderm lines the body wall → parietal peritoneum. The space between becomes the peritoneal cavity.
Regional patterning of the gut tube: signalling gradients (e.g., HOX) specify regions.
The breakdown of both ends of the tube = future mouth and anus.
Allantois
Begins as an endodermal outpouching (week 3).
The allantois forms a small diverticulum from the hindgut endoderm.
It grows into the connecting stalk (future umbilical cord).
Early function: blood formation + vessel development.
In early embryos, the allantois helps with blood formation (haematopoiesis) and the formation of umbilical arteries and veins.
Becomes the urachus as the embryo grows: as the bladder develops from the urogenital sinus, the allantois becomes a fibrous tube connecting the bladder apex and umbilicus. This tube is called the urachus.
Final adult remnant: median umbilical ligament - after birth, the urachus obliterates and becomes the median umbilical ligament. This is a midline structure running from the bladder to the umbilicus.
*Simpler: the urachus connects the foetal bladder to yolk sac.
Development of the gut?
Primitive gut develops at beginning of fourth week. It is closed at the cranial end: oropharyngeal membrane, and closed at the caudal end: cloacal membrane.
There are 3 parts:
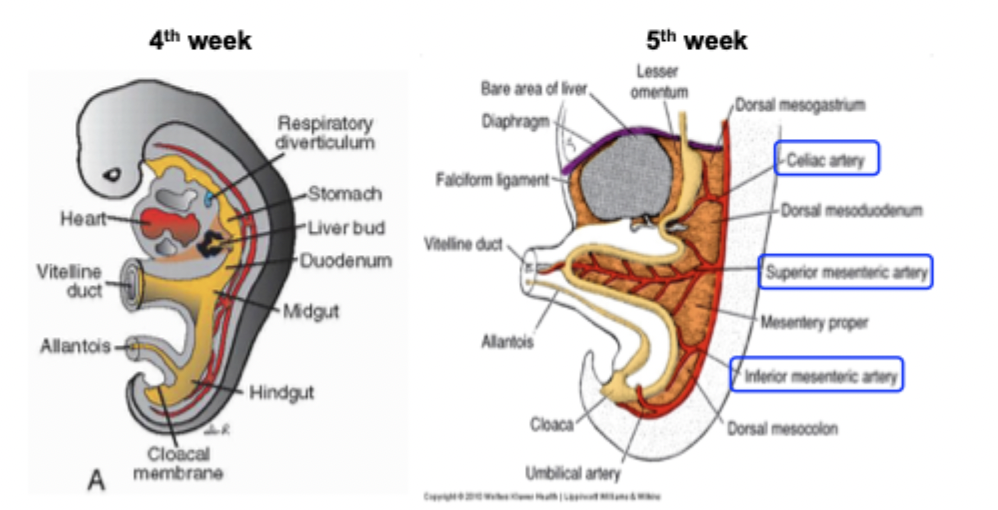
Blood supply to each segment of the gut?
Foregut: from celiac artery.
Midgut: from superior mesenteric artery.
Hindgut: from inferior mesenteric artery.
Regional patterning of the gut diagram
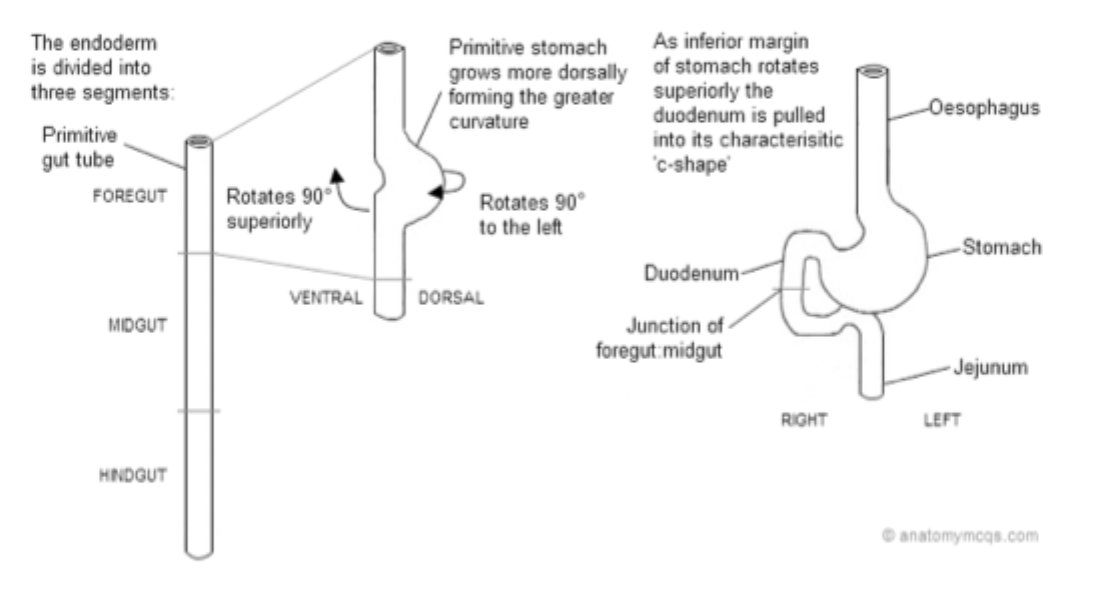
Development of stomach
Distal part of foregut, around middle of fourth week, slight dilatation.
Enlarges and broadens ventro-dorsally.
Dorsal part grows faster than ventral part: greater curvature of stomach.
While growing: rotation 90 degrees clockwise.
Ventral border (smaller curvature) moves to right, dorsal border (greater curvature) to left.
Rotation superiorly bends duodenum into C-shape.
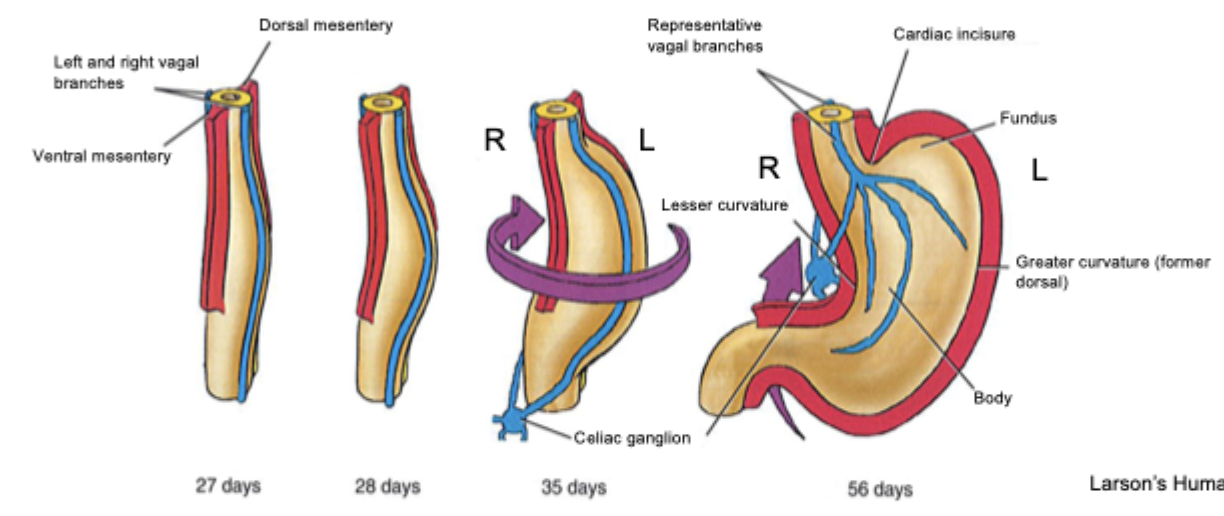
Diagram of the development of the stomach
GENERAL development of other endodermal organs
Endodermal thickening.
Cells proliferate to form bud.
Continuous lengthening and bifurcation/branching.
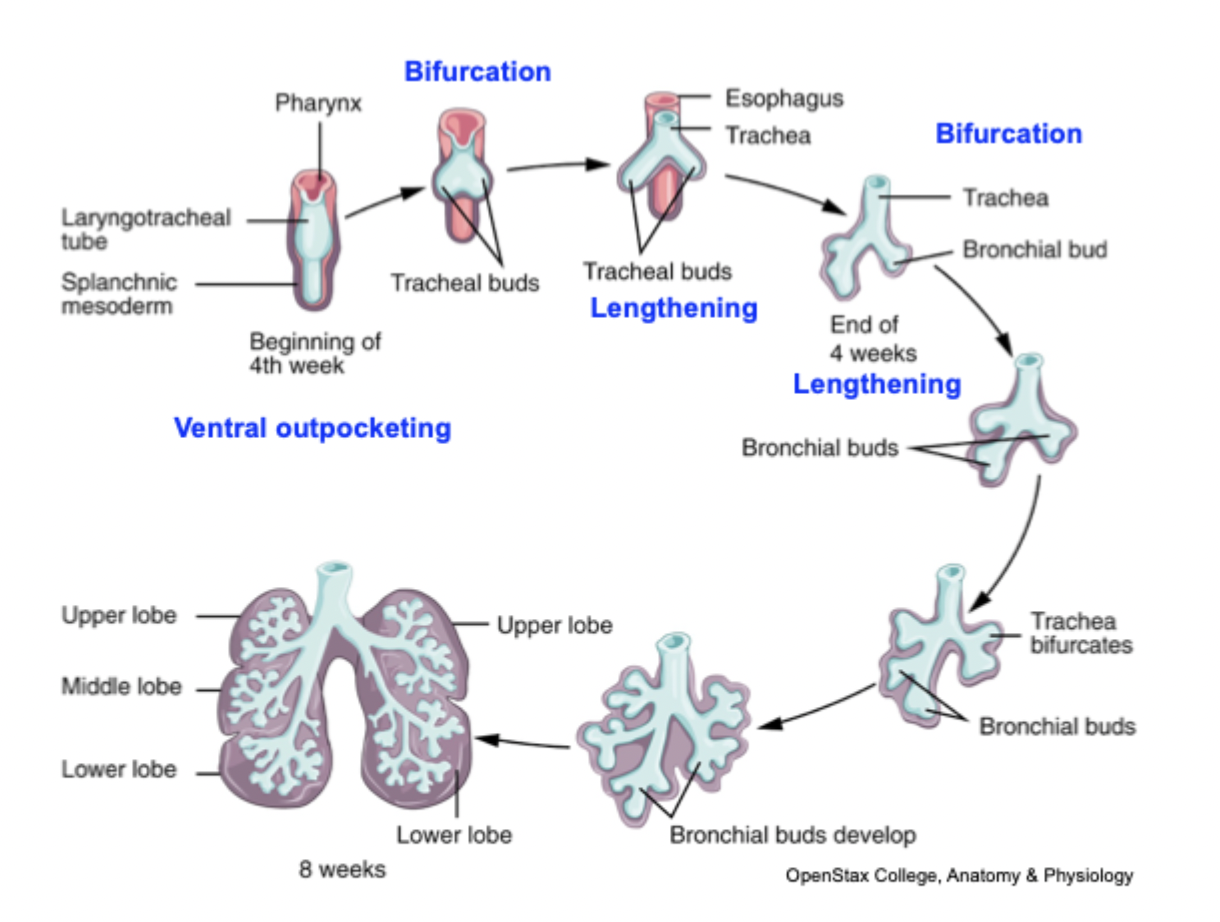
Development of lungs
Lung bud forms from foregut endoderm (week 4).
A respiratory diverticulum buds off the ventral foregut.
This will form the trachea and lung primordia.
Separation of trachea and oesophagus.
Tracheoesophageal folds grow and fuse → tracheoesophageal septum.
Ventral tube → trachea + lung buds; dorsal tube → oesophagus.
Primary lung buds (3 on right, 2 on left) branch into bronchi
the lung bud divides into right and left primary bronchial buds.
Primary buds → secondary bronchi (lobar) → tertiary bronchi (segmental).
Branching continues → terminal bronchioles form. No respiratory bronchioles or alveoli yet → gas exchange not possible.
14 more branchings → terminal bronchioles.
The gut and its derivatives (TABLE)
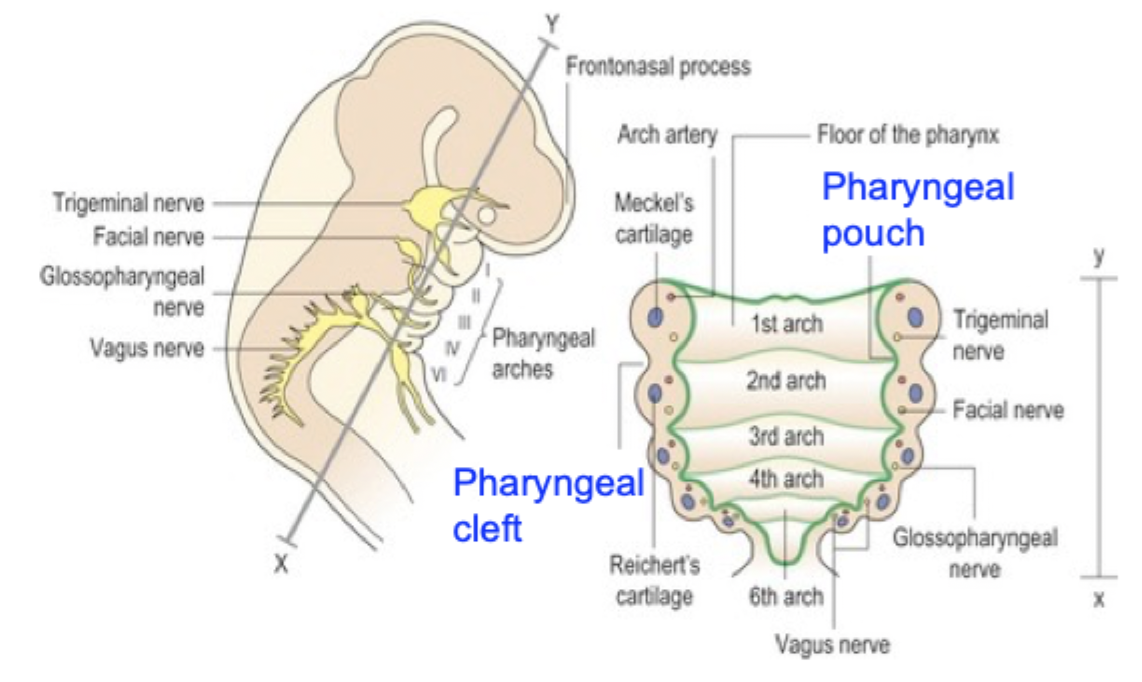
Human face development: pharyngeal arches
Also called branchial arches:
Outer covering of ectoderm.
Mesenchymal core derived from mesoderm as well as neural crest cells.
Lined inside with endoderm.
EACH pharyngeal arch contains:
central cartilagionous skeletal element (derived from neural crest).
Striated muscle rudiment (derived from head mesoderm).
Arch-specific cranial nerve.
Aortic arch artery (endothelial cells derived from mesoderm).
Primordial germ cells and PGC migration
PGC are precursors of sperm and egg. They are specified early in development, embryonic disc with two layers. They are specified by inductive signalling from surrounding cells.
PGCs are specified in the epiblast early, then move to the yolk sac wall near the allantois.
Entry into embryo through hindgut: as the embryo folds, PGCs re-enter the embryo by migrating into the endoderm of the hindgut.
Migration along dorsal mesentery: from the hindgut, PGCs move cranially along the dorsal mesentery of the gut.
Arrival at genital ridges: they finally reach the gonadal ridges on the posterior abdominal wall, where they populate the developing testes or ovaries.
Proliferation and differentiation: once in the gonad, PGCs proliferate and later differentiate into spermatogonia or oogonia, depending on sex.
*Mesentery = double layer of peritoneum that suspends the intestines from the posterior abdominal wall and carries their blood vessels, nerves, and lymphatics.