3.2.2 The immune system
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
What is primary non-specific defence
The first line of defence that prevents the entry of pathogens. It’s non specific as the response is the same irrespective of the type of pathogen or whether it’s a first or 2nd attack.
NSP - Skin
mechanical
physical, protective barrier
Secretes sebum that contains fatty acids with anti microbial properties
Has anti microbial proteins on surface that change the structure and function of microbial csm
Skin has an outer layer of dead, dry, hardened cells that provide an inhospitable environment for growth of microorganisms.
NSR - Blood clotting
mechanical
blood clotting cascade seals breaks in skin
NSR - mucous membranes
chemical
Lines airways, reproductive systems, gut
Has goblet cells that secrete mucin that forms mucus
Mucus traps pathogens and cilia wafts them back up the trachea to be expelled or swallowed
Mucus also covers ciliated epithelium and prevents trapped pathogens reaching alveoli
Has lysozymes that breakdown cell wall of bacteria
Has phagocytes to destroy bacteria
NSR - HCl
chemical
HCl produced by parietal cells in stomach lining
HCl in stomach kills swallowed pathogens
NSR - tears
chemical
Lysozymes that destroy cell wall of bacteria
NSR - cilia
reflux expulsion - coughing/sneezing
Ciliated epithelium beat and waft trapped pathogens up trachea to be swallowed or expelled
NSR - role of histamines in inflammation
Released by activation of MAST CELLS
vasodilation - more blood flow to wound site - localised heat and redness (higher temp inhibits pathogen reproduction)
Arterioles more leaky - more plasma forced out - more tissue fluid is formed - swelling / pain
What is an inflammatory response
A localised response to pathogens at site of wound that causes redness, pain, odema (swelling) and heat
NSR - role of cytokines in inflammation
Released by mast cells
IL-1 and IL-6 attract phagocytes to wound site - phagocytosis occurs and pathogens engulfed and destroyed
Stimulation of liver to release proteins that bind to surface of bacteria and damaged host cells to promotes phagocytosis by macrophages
NSR - role of serotonin and prostaglandins in inflammation
make arterioles more leaky
Vasodilation
How do fevers help defend against pathogens
many pathogens reproduce at 37 degrees or lower, so higher temp inhibits pathogen reproduction
Specific immune responses work faster at higher temp
3 types of phagocytes
neutrophils
Macrophages
Dendritic cells
Role of neutrophils
circulate in blood plasma
Short lived - die after phagocytosis
Rapid response
Chemicals released by pathogen or infected cell attract neutrophils. (Chemotaxis)
neutrophils have receptor proteins on surface that bind to antibodies attached to antigens on pathogen
once attached, pathogen is engulfed and destroyed
Role of macrophages
long lived
These are monocytes that leave the bloodstream and enter tissues
Process and present antigens to the lymphocytes instead of killing pathogens directly.
Macrophages digests the pathogen and combines the antigens form pathogen’s csm with glycoproteins called major histocompatibility proteins (MHC)
This allows the macrophage to present the pathogens antigens to its surface
Macrophage becomes an antigen presenting cell (APC)
The exposed antigens can be recognised and destroyed by other lymphocytes
Dendritic cells
long processes that increases surface area for the interaction with pathogens + lymphocytes
Once they engulf pathogens they migrate to lymph nodes
Mode of action of phagocytes
pathogen produces toxins
damaged cells releases cytokines
Phagocytes are attracted to cytokines and toxins and travel to site of infection via chemotaxis
Antigens in surface of pathogens recognised as foreign
Receptors on surface of phagocytes bind to antigens on pathogen via opsonins
Phagocytes engulfs the pathogen via endocytosis to form a pseudopodia (where csm extends around pathogen) until the csm fuses with itself again
Phagosome is formed
Phagosome fuses with a lysosome to form a phagolysosome
Lysosomes contain hydrolytic enzymes that digest and destroy pathogens
Harmless products released into cytosol of phagocyte
Role of cytokines in phagocytosis
acts as cell signalling molecules that attract phagocytes to site of infection/inflammation
Increases core body temp - inhibits pathogen reproduction
Stimulates a specific immune response
Role of opsonins in phagocytosis
extracellular proteins that induce phagocytosis
Bind to pathogens and ‘tags’ them so they’re recognised by phagocytes
Phagocytes have receptors on surface that bind to opsonins allowing the pathogen to be engulfed.
site of production and maturation of T-lymphocytes/B-lymphocytes
both produced in bone marrow
T = matures in thymus gland
B = matures in bone marrow
Role of T-lymphocytes in SPECIFIC immune response - CELL MEDIATED IMMUNITY
CLONAL SELECTION - T-helper cells have CD4 receptors on their csm that bind complementary to antigens on surface of antigen-presenting cells, which causes t-cells to be activated
CLONAL EXPANSION - activated t-cells proliferate and divide by mitosis to produce many clones (different types of T-cells)
T-HELPER
T-KILLER
T-MEMORY
T-REGULATORY
Role of T-HELPER CELLS
T-helper:
releases interleukins (type of cytokine) that activate B-cells
attract and stimulate macrophages to engulf pathogens
stimulate production of other types of T-lymphocytes
Role of T-Killer cells
recognise foreign antigens on csm of infected host cells and attaches to them
releases toxic chemical PERFORIN which punches holes in csm of infected host cell so it becomes freely permeable and dies via lysis
T-MEMORY CELLS
Long lived cells that remain in blood
if same antigen is recognised again in a secondary attack, t-memory cells rapidly divide by mitosis to produce large numbers of clones of t-killer cells to destroy the pathogens
T-REGULATORY cells
ensure body recognises self-antigens so an autoimmune response isn’t carried out
stops immune response once pathogen is destroyed
B-LYMPHOCYTE specific immune response - HUMOURAL IMMUNITY
CLONAL SELECTION - B-cells are activated by interleukins produced by t-helper cells
CLONAL EXPANSION - activated B cells proliferate and divide by mitosis to form clones
some clones differentiate into B-PLASMA cells and others into B-MEMORY cells
role of B-PLASMA CELLS
PRIMARY IMMUNE RESPONSE
short lived cells
secrete antibodies (immunoglobulins) that are specific to the antigens on csm of pathogen into the plasma
role of B-MEMORY CELLS
SECONDARY IMMUNE RESPONSE
Long lived cells
remain in body after infection to provide immunological memory
if same antigen is encountered again, they divide rapidly by mitosis + differentiate to produce lots of clones of plasma cells so there’s a faster and higher production of Ig (before symptoms appear)
what will plasma cells have more of
ribosomes - increased protein synthesis of Ig
golgi apparatus - more proteins need to be packaged and processed
RER: increased protein synthesis
mitochondria - supply energy for Ig synthesis
why do we get symptoms for disease when first exposed to a pathogen
there’s a delay in the primary immune response if we’re exposed to a new pathogen
it takes time for clonal selection/expansion of T/B-cells to occur
it takes time for antibodies to be produced and released into teh blood
why do we still experience symptoms when re-infected with the same pathogen as before?
some diseases are caused by multiple different strains i.e common cold/flu
each strain has different antigens, so a primary immune response must be carried out each time before immunity is achieved
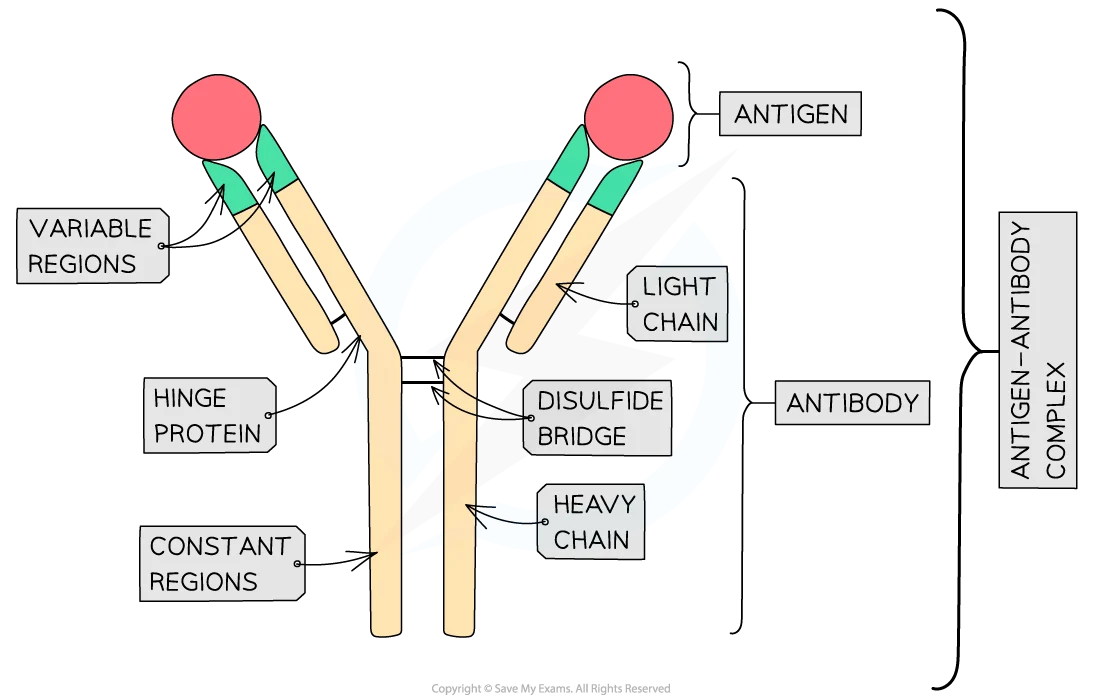
structure of antibodies
Y-shaped globular glycoproteins called immunoglobulins
quaternary structure
2 heavy polypeptide chains bonded to 2 light polypeptide chains via disulphide bonds
hinge region allows flexibility so antibody can bind to the antigens at an angle and bind to more than one antigen at a time
constant region - same for all Ig in the same class (5 classes of antibodies)
variable region - different for each antibody
has an antigen-binding site that’s specific to the epitope (part of antigen that binds to antibody) on an antigen
the antibody binds to the antigen to form an antigen-antibody complex
Function of antibodies
agglutination
opsonins
lysis
anti-toxins
precipitations
role of agglutination
Ig will bind to 2 identical antigens on 2 or more different pathogens
Ig immobilises the pathogen, causing the bacterial cells to clump together
this makes it harder for the bacteria to enter host cells
harder for bacteria to spread through blood stream
easier for phagocytosis as phagocyte can engulf multiple pathogens at once
role of antibodies as opsonins
constant region of Ig binds to receptors on csm of phagocyte
variable region of Ig binds to antigens on pathogen/damaged cell
this allows the pathogen to be marked so phagocytes can identify them easier and destroy them
lysis - antibodies
Ig binds to pathogen and attracts complement proteins
these proteins creates holes in csm of pathogens
bacterial cells becomes freely permeable
water moves in via osmosis
bursts (lysis) as cell contents leak out
role of anti-toxins
Ig binds to toxins and neutralises them so they can’t prevent harm
Test for TB
blood test carried out first to determine if person has Ig (if yes, test not needed)
MANTOUX TEST
tuberculin (from mycobacterium tuberculosis) is injected just below skin
If Ig already present, inflamed and red area will appear
Inflamed area is measured:
Big area = strong immunity (or active TB)
Small area = weak immunity - vaccine given
No area = no immunity - vaccine given
Importance of early screening for HIV
important as can lead to early diagnosis so early treatment can be given - people can get counselling/advice about how to limit spread of HIV
Test for HIV
Blood sample
tests for specific antibodies and antigens present in blood
Results in 2-14 days
More accurate test - less false +/-
if +, 3 follow up tests needed before diagnosis
Point of care test
finger prick or mouth swab
Results in 11-28 days
Chance of false +/-
ELISA testing
What does Elisa testing stand for
Enzyme linked immunosolvent assay
When is an ELISA test used and what’s it used for
used to detect the presence of antibodies for a particular pathogen
Used after an immune response has developed and antibodies have been produced
How does ELISA testing work
first coat well with antigen that antibodies would be specific to
Add patients serum and let sit in well for few mins to allow antibodies to bind to antigen - fixed capture molecule
Wash away serum and unbound antibodies
Add enzyme-linked antibody (secondary antibody) which is specific to human Ig
Leave for few mins and wash away unbound secondary antibodies
Add substrate and look for colour change (colour change = +ve result = antibodies specific to substrate)
+ve result = antigen-antibody enzyme linked antibody antibody sandwich
Passive and active immunity differences
PASSIVE:
no immune response
B/T lymphocytes not stimulated - no memory cells
Immediate response
Temporary immunity
ACTIVE:
immune response
B/T lymphocytes activated - memory cells produced
Longer lasting and greater immunity
Time delay - antibody conc. takes time to increase
Passive natural immunity
antibodies received across placenta via breast milk that’s rich in IgA
Infants gut can absorb Ig into blood without being hydrolysed
Only offers protection from diseases mother has had
Passive artificial immunity
injection of Ig from external source
As no memory cells are produced and Ig is eventually broken down by liver, boosters are needed e.g tetanus vaccine - acts as antitoxin and prevents spread of pathogens by preventing viruses from in entering host cells
Active natural immunity
person exposed to live pathogen and gets infected
Produces Ig themselves
Experiences symptoms
Memory cells produced - secondary infection means more Ig produced and at faster rate
Not ok for people with compromised immune systems I.e HIV
Active artificial immunity
antigens received from external source
E.g vaccination
How is an allergic reaction triggered:
person exposed to allergen
Triggers an immune response
IgE produced which binds complementary to receptors on mast cells
Allergy molecules bind to IgE that are attached to the mast cells which triggers histamines to be released via exocytosis
Histamines increase permeability of capillary walls - excess tissue fluid formation - inflammatory response