Ch. 6 : Drugs, Addiction, and Reward
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
Drugs
= substance that changes the body’s functioning
Types:
Agonists = pretend to be a neurotransmitter & bind to its receptor
Antagonists = prevent neurotransmitters from bindings to their receptors
Psychoactive drugs = drugs with psych effects (ex. anxiety relief, or hallucinations)
Effects of drugs
Dependence = need to keep taking a drug to avoid withdrawal, NOT just want
physical dependence = body needs it
psych dependence = feelings/thoughts need it (ex. antidepressants)
→ NOT addiction - THUS, u can be dependent & not addicted
Tolerance = more required to produce same effects
can lead to overdoses
Addiction = preoccupation w obtaining a drug, compulsive use, and tendency to relapse after quitting
sorta like OCD
nothing abt dependence or tolerance
Withdrawal = negative reaction when drug use is stopped
usually the opposite of the drugs effect
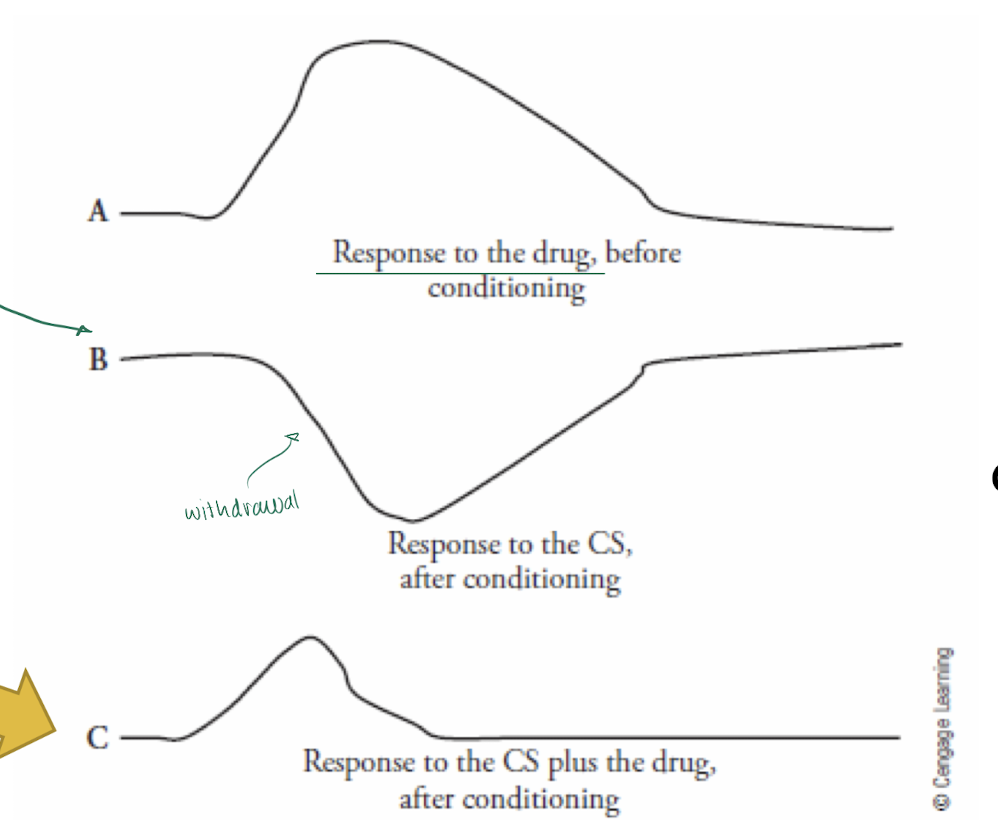
Effect of Drugs: Drug tolerance
if in a new place, withdrawal symptoms/built tolerance doesn’t occur as fast → THUS, drug use is MORE intense bc ur body’s tolerance had been conditioned to a certain environment
→ increased risk of overdoses
Drugs: Opium
1 of the oldest used drugs
strongest natural pain reliever
originally a sleep-aid
“sleep-bringing”
NOTE: tinctures / laudanum (opium dissolved in alcohol) were common in victorian England
Opiate vs. Opiod
Opiate = natural opioid from opium poppy
an opiod
ex. opium, morphine, codeine
Opioid = natural, synthetic, or endogenous peptides (protein made in body) that exert bio effects at the opioid receptors (have similar effects)
ex. opiates, heroin, oxycodone
Opiates & Opioids
→ Heroin = synthesized from morphine
effect: lowers pain, relaxing, euphoria
most notoriously abused opioid
high risk of relapse (lifelong addiction)
1st made in 1800s to be less addictive than morphine (slowly crosses blood-brain barrier)
→ BUT, is actually 3x MORE addictive - bc it quickly crosses the blood-brain barrier
Endorphins = body’s own neurotransmitters for the receptors that opioid drugs act on
endogenous (made in body) - produced in response to pain, increased sympathetic NS, exercise, and/or sex
effect: lowers pain, euphoria
NOTE:
women have more opioid receptors → THUS, require higher opioid doses
men produce more endorphins
Depressants
= reduce CNS activity (brain & spinal cord)
agonists (pretend to be another neurotransmitter)
act as ALL 3 at SAME time:
sedative (calms)
anxiolytic (decreases anxiety)
hypnotic (sleep-inducing)
ex. alcohol, barbiturates, benzodiazepines
→ effect: ALL increase GABA (inhibitory neurotransmitter), thus increase inhibition
Depressants: Alcohol
= from fermented food
effect: calms, lowers anxiety, high doses can induce sleep, euphoria, motor & cognitive impairments, social lubricant (low dose)
@ high doses: decreases activity in brain + at amygdala it increases emotional expression
most commonly used & abused drug
older evidence of abuse than opioids
2 withdrawal Phases:
normal
can experience delirium tremens = severe run to alcohol withdrawal resulting in hallucinations, delusions, confusion, seizures, or death
→ the ONLY withdrawal that can kill u
Depressants: Barbiturates
= in small doses: act selectively on higher cortisol centres involved in inhibiting behaviour → THUS anxiolytics
low dose: anxiolytics
med dose: hypnotic (sleep-inducing for anaesthesia)
high dose: death (low heart rate)
VERY addictive
quickly develop tolerance for calming & anxiolytic effects, BUT NOT for decreased heart rate effect (dangerous)
Depressants: Benzodiazepines
= act at benzodiazepine receptor on GABA
effect: lowered anxiety, sedation, muscle relaxation
safer version of barbs
NOT for anesthesia (bc they dont rly induce sleep)
VERY addictive + develop slightly slower tolerance than barbs
ex. valium, xanax
Depressants: Effect on GABA
depressants ALL act on GABA receptors, but DIFFERENTLY, bc they bind at different sites → diff effects
GABA receptor = inhibitory ion channel
Cl- enters making cell MORE (-) → hyper polarization
requires 2 GABA’s binding to open
HOWEVER
→ 1 depressant + 1 GABA binding can open channel EASIER
NOTE: barbs are so dangerous bc @ high [barb] it can open the receptor BY ITSELF
![<ul><li><p>depressants ALL act on GABA receptors, but DIFFERENTLY, bc they bind at different sites → diff effects </p></li></ul><p></p><p>GABA receptor = inhibitory ion channel</p><ul><li><p>Cl- enters making cell MORE (-) → hyper polarization </p></li><li><p>requires 2 GABA’s binding to open</p></li></ul><p> HOWEVER</p><p> → 1 depressant + 1 GABA binding can open channel EASIER</p><p></p><p><span style="color: red;">NOTE: barbs are so dangerous bc @ high [barb] it can open the receptor BY ITSELF</span></p><p></p>](https://assets.knowt.com/user-attachments/80a7e82d-cbb4-4fea-965e-97501703d176.png)
Stimulants
= activate CNS
effect: produce arousal, increased alertness & elevated mood, decreased appetite
ex. cocaine, amphetamines, nicotine, caffeine
Stimulants: Cocaine
= from coca plant
effect: euphoria, lowered appetite, increased alertness & relieves fatigue
how: prevents reuptake of dopamine - thus its an antagonist (blocks)
usually comorbid abuse
pretty mild withdrawals
CAN be used as a local anesthetic or cough suppressant
ex, crack-cocaine (smoked or inhale vapours), powder, pure cocaine (smoke freebase)
Stimulants: Amphetamines
= synthetic
effect: euphoria, increased confidence & concentration
how: prevents reuptake of dopamine + increases release of dopamine
legal/nonlegal
longterm use : decreased grey matter (cell bodies in cortex)
ex. meth (fast-acting), Vyvanse (for ADHD)
Stimulants: Bath salts
= variety of synthetic drugs related to cathinone from khat plant
changed frequently, thus can be very dangerous
Stimulants: Nicotine
= primary psychoactive & addictive agent in tobacco
effect: lowers anxiety, calming, lowered appetite
how: increases acetylcholine (excitatory neurotransmitter) @its nicotine receptor → increasing activity
Stimulants: Caffeine
= active ingredient in coffee and tea
effect: arousal, increased alertness, lowered sleepiness
some health benefits
CAN overdose
Psychedelic Drugs
= cause perceptual distortions
serotonergic = increase serotonin (get sensory distortions)
ex. LSD, magic mushrooms
catecholaminergic = increase acetylcholine, THUS increase stimulants (get perceptual distortions + stimulants)
ex. ecstacy, molly, MDMA
NMDA receptor agonists (blocking) = inhibit glutamate (an excitatory neurotransmitter) → get extreme hallucinations similar to schizo
Designer drugs = synthetic from chemicals
Psychedelic Drugs: serotonergic
= increase serotonin
result: sensory distortions
ex. LSD, magic mushrooms
Psychedelic Drugs: catecholaminergic
= increase acetylcholine, THUS increase stimulants
result: perceptual distortions + stimulants
ex. ecstacy, molly, MDMA
Psychedelic Drugs: NMDA receptor agonists (blocking)
=inhibit glutamate (an excitatory neurotransmitter)
result: extreme hallucinations similar to schizo
Psychedelic Drugs: Designer drugs
= synthetic from chemicals
Marijuana
= from plant cannabis sativa
natural one doesn’t kill from consumptions alone, but synthetic one is lethal
Cannabinoid = compounds made by our bodies (endogenous)
Addiction: Reward Circuit
2 theories of addiction:
they like the reward
to avoid withdrawal symptoms
→ neither explain it fully
Reward = positive effect and object/condition has on user
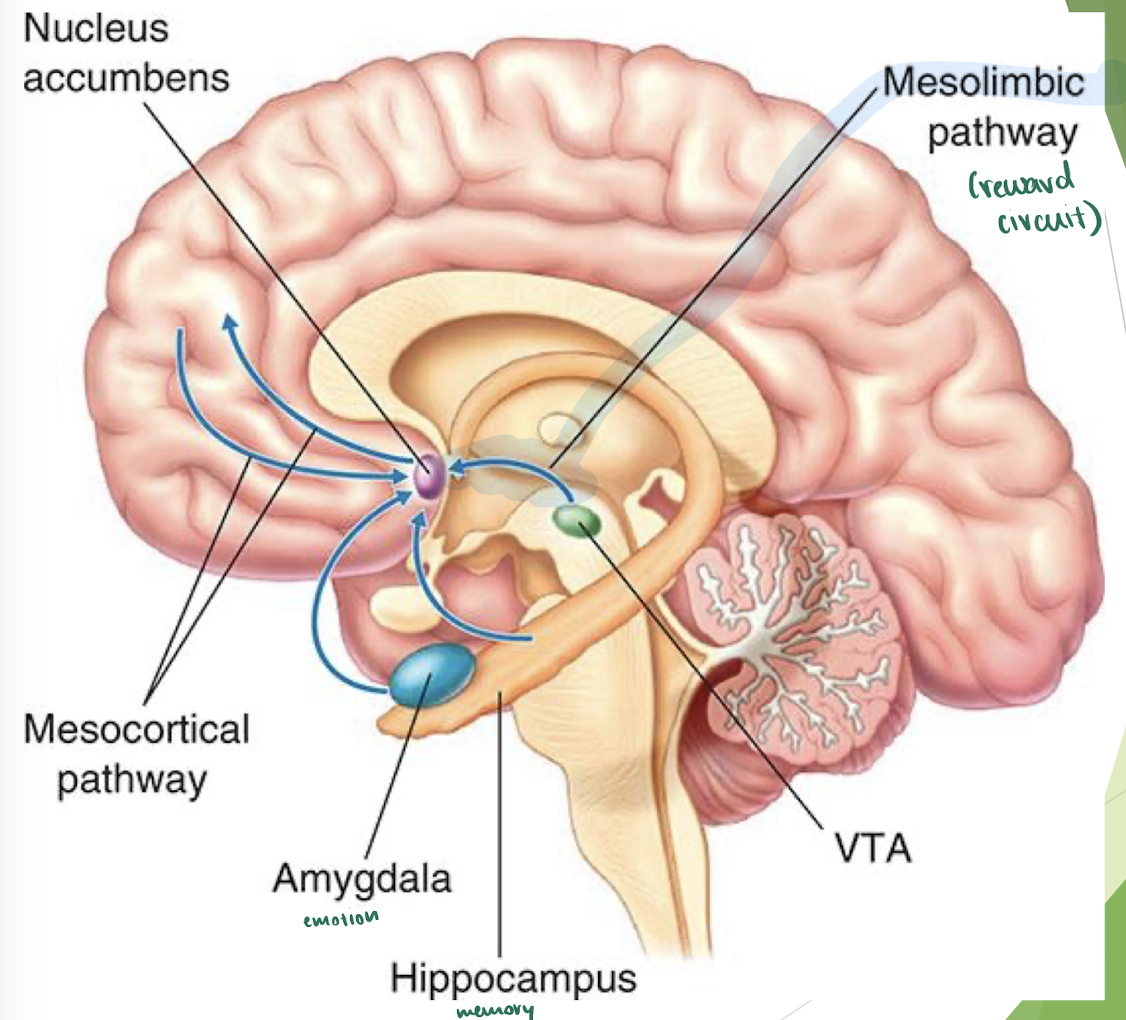
Mesolimbic Pathway = reward circuit
2 parts:
ventral tegmental area (VTA) = sends dopamine to nucleus accumbens → feel happy
ALL addictive drugs increase the dopamine sent
nucleus accumbens
stops activating
sends & receives info from frontal lobe
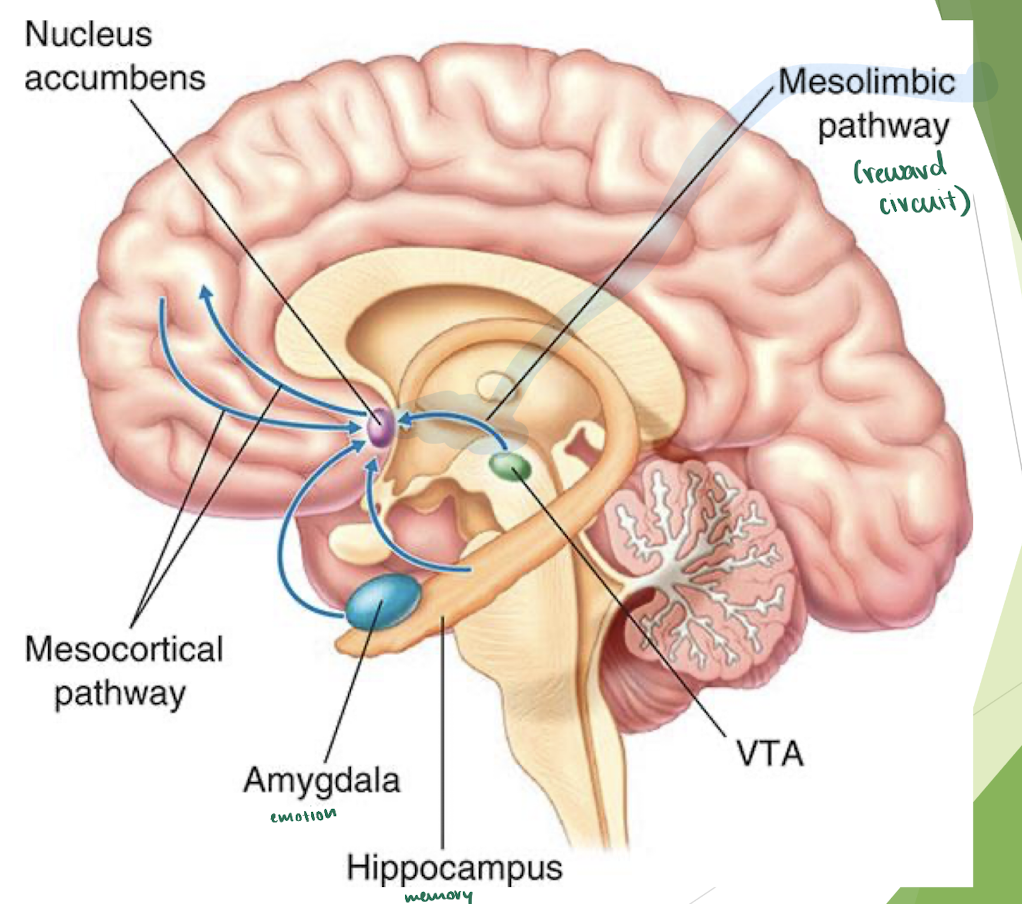
Addiction: Mesocortiocolimbic dopamine system
Mesocortiocolimbic dopamine system = consists of the VTA + brain regions receiving its dopaminergic projections (nucleus accumnbens, prefrontal cortex, amygdala, & hippocampus)
influences whether we’re rewarded
NOTE: addiction creates functional + structural changes in the brain that persist long after stopping drug use
Addition: Hypofrontality
w addiction:
hypofrontality = reduced activity in frontal regions that control working memory, behavioural inhibition & response to environment
doesn’t return fully after addiction
changes occur regardless of the type of addiction
NOTE: cravings persist after years of drug abstinence
Treating Drug Addiction
want to treat everything at once, thus consider comorbidity
→ addiction is often accompanied by mental or emotional personality disorders
Treating Drug Addiction: Treatments
Agonist treatments = replace drug with less severe drugs with a similar effect
ex. Methadone - a synthetic opioid to treat opioid addiction
gives a little opioid response + addicted drug cant bind since the spots already taken
NOT strong + less addictive
Antagonist treatments = using drugs that block the addicted drugs effects
NO opioid effect
ex. naltrexone/naloxone
Aversive Treatments = cause negative run if u taken the addicted drug
Antidrug vaccines = attach to drug & cause immune system to make antibodies that degrade the drug
works short-term for some ppl
Addiction: Roles of Genes
→ addiction is heritable
Study: heritability of addiction was 1st established w alcoholism
falsely said there were type 1 and 2 alcoholics
Type 1 = cautious & emotionally dependent ppl → alcoholics after 20 (environmental)
Type 2 = uninhibited ppl → early alcoholics (genetic)
genetics influence how drugs are metabolized, neurotransmitter/receptor levels + other risk factors
drugs also impact genetic function
→ Methylation = attach a methyl group to DNA → suppresses a genes activity
most commonly thru smoking + CAN be passed down genetically