Tibia + fibula #
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
Types of #’s
tibial plataeu #’s
Undisplaced: No separation of bone fragments.
Condylar depression: Articular surface has sunk downwards.
Vertical shear: A vertical split through the condyle.
Comminuted: Bone is broken into multiple pieces.
tibial spine #’s (avulsion # of tibial plateau)
tibia-fibula shaft #’s
What does management of these #’s depend on?
amount of displacement
degree of stabilty
feasibility for surgical fixation
Tibial plateau #’s
common mechanism = valgus/varus force with axial loading
high energy (most common pattern = spilitting) = MVA or sport injuries
low energy = insufficiency fractures, associated w soft tissue injuries (falls in elderly → osteoporosis → typically depressed #’s)
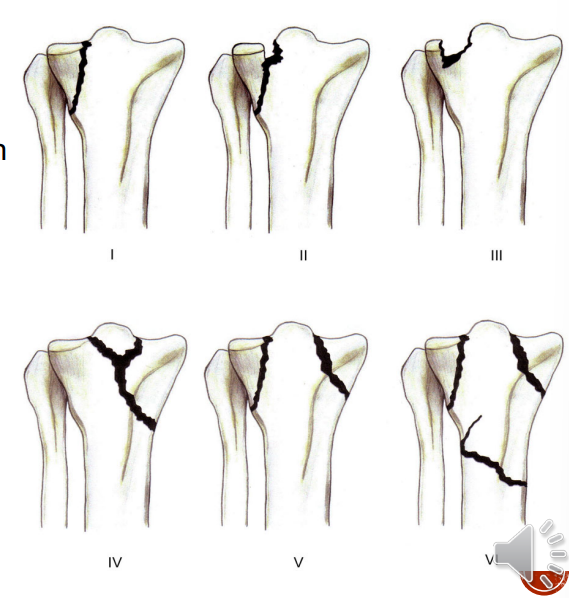
Schatzer’s classification of tibial plataeu #’s:
Schatzker 1 → lateral split
Schatzker 2 → lateral split w depression
Schatzker 3 → lateral depression
Schatzker 4 → medial depression
Schatzker 5 → bicondylar
Schatzker 6 → fracture of both condyles + shaft involvement
Main aims of medical management
Anatomical reduction of the joint surface: Restoring the normal shape of the bone, especially in articular fractures.
Stable osteosynthesis: Securely fixing the bone fragments to allow for early healing and mobilization.
Prevention of complications: Such as joint stiffness, deep vein thrombosis (DVT), and pulmonary embolism (PE).
Conservative management:
full length POP w ankle in neutral (4 weeks)
leg brace allowing knee ROM (4 weeks after)
Management/ Physiotherapy treatment of undisplaced #’s
Main aim of physio:
improve knee joint mvmnt
prevent loss or ROM of joint or stiffness
Treatment (0-4 weeks):
Affected leg:
isometric co-contractions of muscles around the knee + ankle joint
circulation exercises with toes + elevation do leg in extension on bed/chair
hip ROM + strengthening exercises
Maintain/↑ ROM + muscle power of unaffected limbs
bed mobility (one leg bridging, moving side to side)
transfer from lying to sitting
standing + mobs with NWB on affected leg (with appropriate walking aid)
Treatment (4-8 weeks):
knee in brace (allowing knee movement)
start AAROM of knee (flex/ext.)
bed mobility (PWB on knee in bridging)
continue with crutch walking NWB → PWB @8wks → FWB @12wks
gradually ↑ WB activities, AROM + strengthening exercises (closed chain) on operated leg from 8 weeks on. → FOCUS ON FUNCTION
Management/ Physiotherapy treatment of displaced #’
Conservative management → skeletal traction (4-6 weeks)
In traction/treatment (0-6 weeks):
active knee movement (work twrd 90 deg knee flex in traction pain dependent)
co-contractions/isometric of muscles around knee joint
circulatory exercises (toes + foot)
maintain ROM + strength of unaffected leg
NB = ROM exercises of knee to mould the developing callus
Treatment (> 6 weeks):
progress ROM of knee + strengthening ecercises of muscles around knee
transfer from lying to sitting
standing + mobs with NWB on affected leg (use appropriate walking aids)
gradually ↑ WB activities, AROM + strengthening exercises (closed chain) on operated leg from 12 weeks on
Management of tibial plateau fractures
Displaced or unstable tibial plateau fractures (especially with condylar depression) require surgical fixation (ORIF), sometimes with bone grafting, and may still need a cast or brace afterwards for additional stability.
Post-op physiotherapy of tibial plateau #’s
early ROM on affected leg to mould callus
CPM (continuous passive movements)
isometrics or co-contractions of muscles around knee
mobilise NWB crutches until union 2-3 months
risk of deformity if early WB
maintain/↑ ROM + muscle power of unaffected limbs
bed mobility
NB = bone graft donor site
Complications of tibial plateau #’s
compartment syndrome
collateral ligamentous tears → risk of unstable knee
common peroneal nerve palsy
late knee instability due to bony collapse + progressive ligament laxity
secondary osteoarthritis
meniscal tears (lat more common than med, associated with schatzker 2, med tear = schatzker 4)
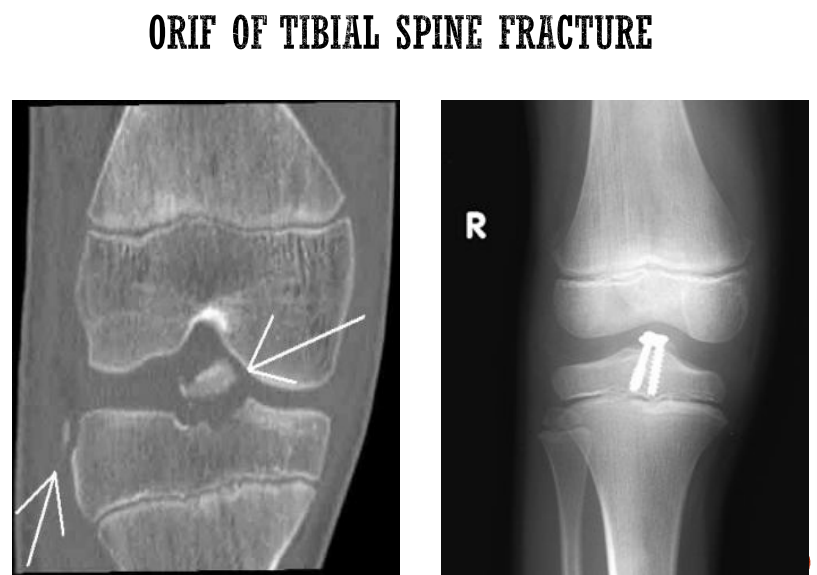
TIbial spine #’s
avulsion # of tibial plateau
caused by twisting, abduction, adduction of knee
pull of ACL or PCL
conservative management → AK POP for 6 weeks
surgical management → if displaced = ORIF, followed by AK POP
Management/ Physiotherapy treatment of tibial spine #’s
Affected leg:
isometric + co-contractions of muscles around knee joint
ROM + muscle power around hip + ankle joints
bed mobility exercises
maintain/improve ROM/muscle power of unaffected limbs
removal of POP → regain ROM/MP of knee joint
Tibia and fibula shaft #’s
tibia is sucutaneous bone therefore open #’s comon
poor muscle coverage + poor vascularity = slow healing + increased risk of infection
compartment syndrome common
twisting force = spiral # at different levels
angular force = transverse or oblique #’s
Open #’s classification:(according to severity fo soft tissue damage)
Type I: Wound <1 cm, clean.
Type II: Wound >1 cm, no major soft tissue damage.
Type IIIA: Extensive soft tissue damage but bone covered.
Type IIIB: Periosteal stripping, bone exposed, massive contamination.
Type IIIC: Arterial injury requiring repair.
Management of tibia and fibula shaft #’s
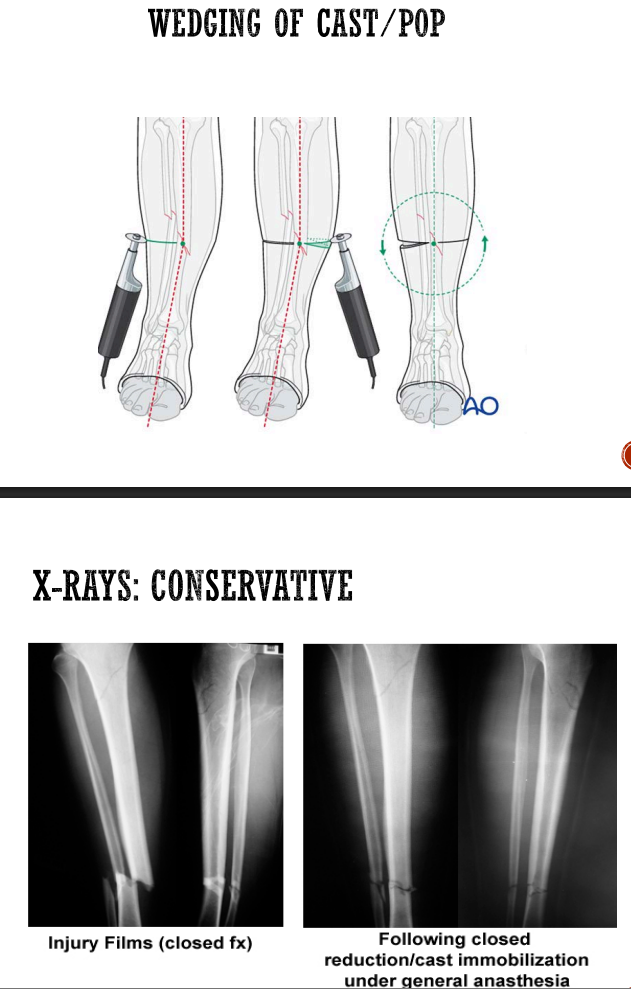
Conservative management:
closed #’s
AKPOP with ankle in plantar grade for 6 weeks
wedging of POP possible to correct residual tilt
calcaneal skeletal traction → when skin viability compromised + massive oedema
once reduction achieved + soft tissue viable → traction converted to POP
Surgical management:
exo-fix
when reduction unlikely to be maintained by POP
compound # (grade 3B)
risk of infection + debridement of wound
ORIF
intramedullary nail of shaft of tibia
plate + screws
fibula refuced w plate + screw if articular involvment
Management/ Physiotherapy treatment of tibia/fibula shaft #’s
affected leg
isometrics + co-contractions around knee + ankle joints
maintain or improve ROM + muscle power around hip joint
unaffected limbs maintain → maintain/↑ ROM + MP
bed mobility
mobilise from lying-sitting-standing w walking aid
NWB mobs w crutches
NB to elevate pt leg when sitting → To reduce post-injury oedema, thereby reducing pain, speeding healing times, and ensuring skin viability over the fracture/surgical site
Physiotherapy after surgical management:
affected limb
aim = regain knee and ankle ROM → observe level of pins in exofix
note surgical approach for intermedullary nail (NB quads)
regain active muecle power → hams, quads, tib ant, gastros, peroneii, tib post
unaffected limbs
maintain/↑ ROM / MP
bed mobility
mobilise NWB for exofix for 6 weeks
FeWB → PWB for ORIF for 6 weeks
if split skin graft → no passive stretching or isotonic / active exercise for 5 days post-graft
once SSG stable → continue with gentle stretching + isometric exercises
Isolated #’s of the fibula
usually secondary to direct blow
symptomatic treatment
NWB bone therefore does not need reduction or fixation unless articular involvement
mobs PWB w crutches until acute pain aubsides
NB strengthening of peroneii
Fracture of the patella
mechanism of injury
direct violence (dashboard + knee → comminuted #)
indirect violence (strong muscle contraction pull off patella → transverse #)
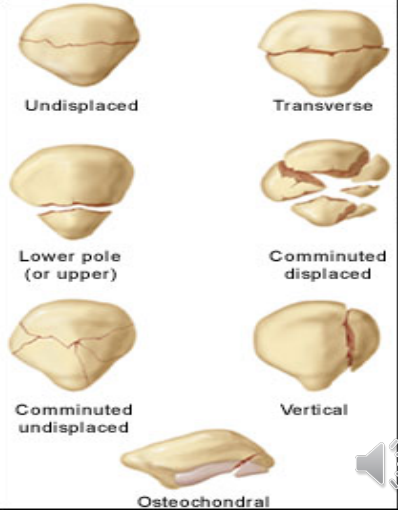
Types of # patterns
comminuted #
transverse #undisplaced #
displaced #
Management / physiotherapy treatment of patella #’s
Undisplaced #
conservative management
AK POP locked in extension for 6 weeks
Physiotherapy:
co-contractions and isometric of muscles around knee
ROM + MP of hip and ankle (above and below!)
mobilise w crutches NWB for 4-6 weeks
bed mobility exercises
maintain ot improve ROm + MP in unaffected limbs
Displaved #’s
associated w rupture of knee extensors (quads)
Surgical management:
ORIF
tension band wiring or K-wire to stabilise # or screw fixation
Dislocations of the patella
patella forced laterally put of groove
May self-reduce or stay displaced.
Atraumatic form more common in females (shallow groove, hypermobility).
Symptoms: Sudden pain/giving way on twisting/jumping, “popping” sensation.
Exam: Apprehension test (+), pain medially & with quadriceps contraction, limited flexion, marked swelling.
X-ray: To rule out fracture.
Management of dislocations of the patella
conservative for both traumatic and atraumatic
closed reduction
cylinder cast → 4-6wks
aim to prevent reccurence
rehab is essential (NB vastus medialis obliquus exercises between 0-15 deg)
Complications of tib-fib #’s
Non‑union: No union by 16 weeks → bone grafting indicated. Smokers at higher risk.
Malunion: Caused by inadequate reduction or failure to maintain reduction.
DVT: Pain on passive ankle dorsiflexion, increased calf swelling, warmth, redness, tender calf squeeze, fever.
Peroneal nerve palsy: Neck of fibula fracture → foot drop; motor weakness + sensory deficit (decreased/absent sensation).
Infection (open fractures): Spiking fever, wound oozing, swelling.
Cause: Increased pressure within a muscle compartment (e.g., proximal third tibia fracture).
Pathophysiology: Oedema → rising pressure → capillary blood flow reduced → ischaemia → necrosis within hours.
Timing: Muscle dies in 6–8 hrs (fibrosis → Volkmann's contracture); nerves die in 2–4 hrs (permanent motor/sensory loss).
5 P's: Pallor, Pain (on passive stretch), Paraesthesia/anaesthesia, Pulses present (late sign), Progressive weakness → Paralysis.
Management: Fasciotomy to reduce pressure
Ankle stiffness complications:
POP must keep ankle in plantigrade (prevents equinus deformity).
Leads to ↓ ROM, ↓ muscle power, gait abnormalities.
Early OA (due to articular damage or malalignment).
Severe disability → osteotomy, arthrodesis, joint replacement.
Popliteal artery occlusion (e.g., proximal tibia # or knee dislocation):
Caused by raised compartment pressure or bony fragment laceration.
Signs: Cyanosed (blue) skin, cold extremity, absent/weak popliteal/DP pulse, numb toes.
Requires immediate arterial repair.