5- relationship with systemic pathologies
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
16 Terms
What are predisposing factors that contribute to periodontal disease?
Any local agent or condition that contributes to biofilm accumulation- dental anatomy, position of the tooth in arch, restorations…
What is a modifying factor?
Any agent or condition that alters the way an individual responds to the presence of biofilm (systemic diseases, smoking, medications...)
Systemic risk factors:
Smoking Hyperglycemia (in diabetic patients)
Reduced intake of antioxidant micronutrients (eg Vit C)
Drugs- system modulators, immunological steroid sex hormones (elevated levels), haematological disorders
What 6 genetic disorders can cause periodontitis as a manifestation?
Diseases associated with immunological disorders- Papillon- Lefevre
Diseases affecting oral mucosa and gingival tissue- epidermolysis bullosa
Diseases affecting connective tissues- Ehler-Danlos Sdr
Metabolic and endocrinological disorders
Diseases with acquired immunodeficiency- HIV
Inflammatory diseases (inflammatory bowel disease)
What diseases/systemic conditions affecting the supporting periodontal tissue can lead to their loss? (Independently of periodontitis)
Neoplasms- squamous cell carcinoma or langerhans cells histocytosis
How do you control risk factors as first step of treating periodontitis?
Stop smoking, control diabetes- increases prevalence, progression and severity of periodontitis
Type 1- lack of insulin due to autoimmune reaction in pancreas
2- insulin resistance associated with chronically high blood sugar
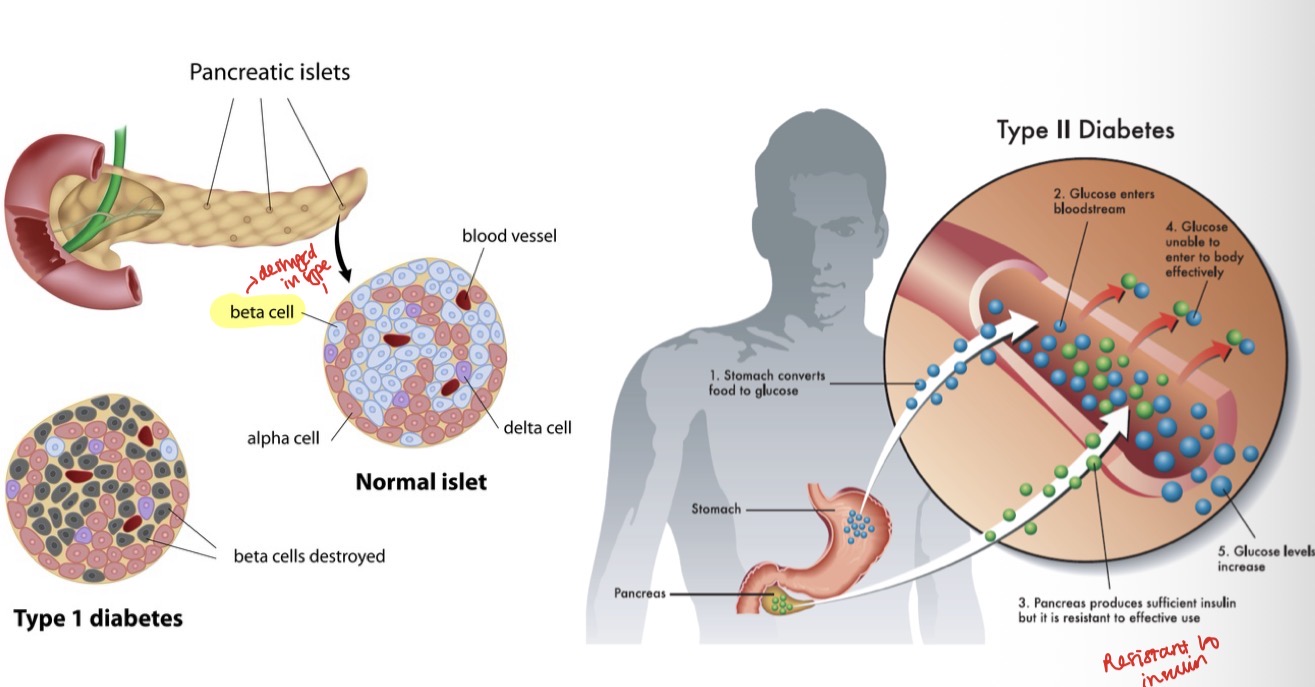
What is the bidirectional relationship between diabetes and periodontal disease?
How periodontal disease affects diabetes-
Worsens glycaemic control
Increases risk of diabetic complications
More common in diabetic patients
How diabetes affects periodontal disease-
Periodontitis is more common and progresses faster, especially if diabetes is poorly controlled
Causes increased inflammatory response in periodontal tissues
How does tobacco affect periodontal disease? Local vs systemic MOA?
Increases risk by 5-20 x
Dose dependent effect
Altered wound healing and microbiota, bad breath, impaired neutrophil function, altered proliferation of T and B lymphocytes
Locally- direct irritant of oral mucous membranes
Systemically- alters immune response and interferes with multiple cellular processes
4 General benefits of quitting smoking?
Decreased risk of myocardial infarction
Decrease in high bp and cholesterol
Increased exercise and lung capacity
Decreased risk of cancer and respiratory tract infections
4 Oral health benefits of quitting smoking?
Decreased risk of oral cancer
Decreased incidence of oral leukoplakia
Better autoimmune reponse and reponse to perio treatment
Increased periodontal vascularisation + prognosis
Which patients may require a more personalised treatment approach?(5)
Moderate (6-15 cig) or severe (more than 16 cig a day)
Have aggressive forms of periodontal disease
Have underlying disease/systemic condition that poses increased risk to patient
Genetic predisposition
Despite repeated attempts at treatment- perio status worsens
What are the 4 main cardiovascular diseases?
Coronary heart disease
Cerebrovascular accidents- ACV or strokes
Congestive heart failure
Peripheral arterial pathologies
What are some non modifiable vs modifiable risk factors of CVD?
Male, elderly, family history
Smoking, diabetes, high bp, obesity, sedentariness
CVD is mainly due to…
Atherosclerosis- thickening of blood vessel wall due to accumulation of lipids and fibrous components
Inflammation- emerging risk factor
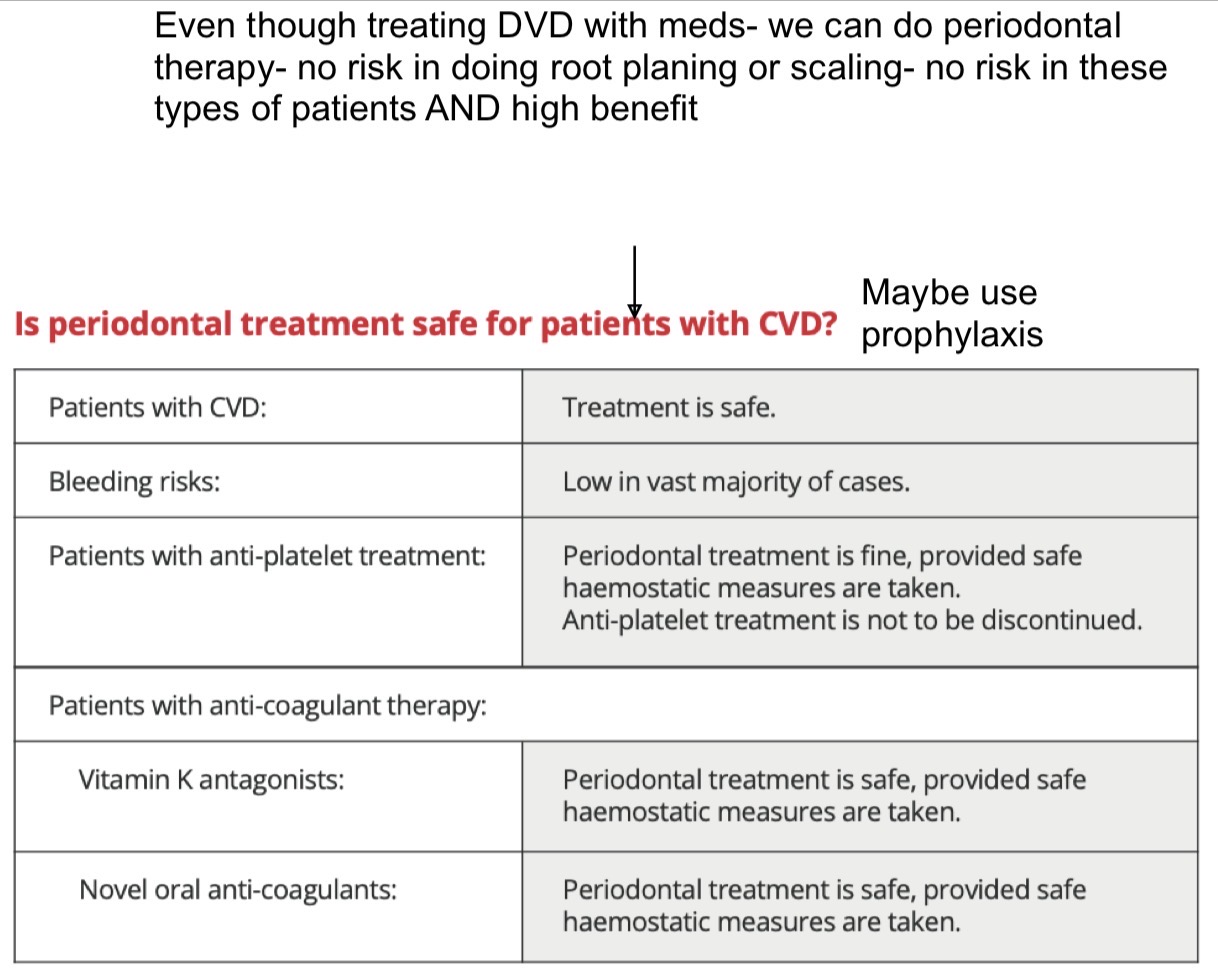
It’s safe to do perio treatment on CVD patients
What hormones increase vascular permeability?
Estrogen and progesterone
What are the main clinical signs of pregnancy gingivitis?
Presence of plaque in the gingival margin- esp anteriors and molars- increased inflammatory response
Increased gingival exudate during 2/3rd trimester
Changes in color and gingival contour
Bop, greater probing depth, max peak of pseudobags in 2nd tri
No insertion loss or bone loss- reversible after childbirth
Scaling can be done safely- but avoid in 1st trimester due to stress for fetus- avoid tetracyclines and metronidazole and perio surgeries
What is a pregnancy (pyogenic) granuloma?
Exophytic growth of pedunculated base
Painful
Located mainly in the anterior sector of maxilla
Due to exaggerated response to irritants (e.g calculus)
Rapid growth
Easy bleeding
