Exam 2 RCA
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
Normal ABG levels
pH 7.35 – 7.45
PaO2 80-100 mmHg
HCO3 22 – 25 mmol/L
SaO2 > 95%
SvO2 65-75%
B.E. + or – 2 mmol/L
Uncompensated Respiratory Acidosis
pH 7.25
PaCO2 65
HCO3 26
PaO2 58
BE +2
Partially compensated respiratory acidosis
pH 7.33
PaCO2 65
HCO3 28
PaO2 58
BE +4
Compensated respiratory acidosis
pH 7.36
PaCO2 65
HCO3 30
PaO2 58
BE +6
Uncompensated Respiratory Alkalosis
pH 7.57
PaCO2 24
HCO3 23
PaO2 88
BE +1
Partially compensated respiratory alkalosis
pH 7.49
PaCO2 24
HCO3 20
PaO2 88
BE -3
Compensated respiratory alkalosis
pH 7.44
PaCO2 24
HCO3 18
PaO2 88
BE -5
Uncompensated Metabolic Acidosis
pH 7.29
PaCO2 40
HCO3 16
PaO2 74
BE -5
Partially compensated metabolic acidosis
pH 7.31
PaCO2 34
HCO3 16
PaO2 80
BE -5
Compensated metabolic acidosis
pH 7.35
PaCO2 30
HCO3 16
PaO2 83
BE -5
Uncompensated Metabolic Alkalosis
pH 7.52
PaCO2 39
HCO3 29
PaO2 92
BE +4
Partially compensated metabolic alkalosis
pH 7.49
PaCO2 46
HCO3 29
PaO2 85
BE +4
Compensated metabolic alkalosis
pH 7.45
PaCO2 49
HCO3 29
PaO2 80
BE +4
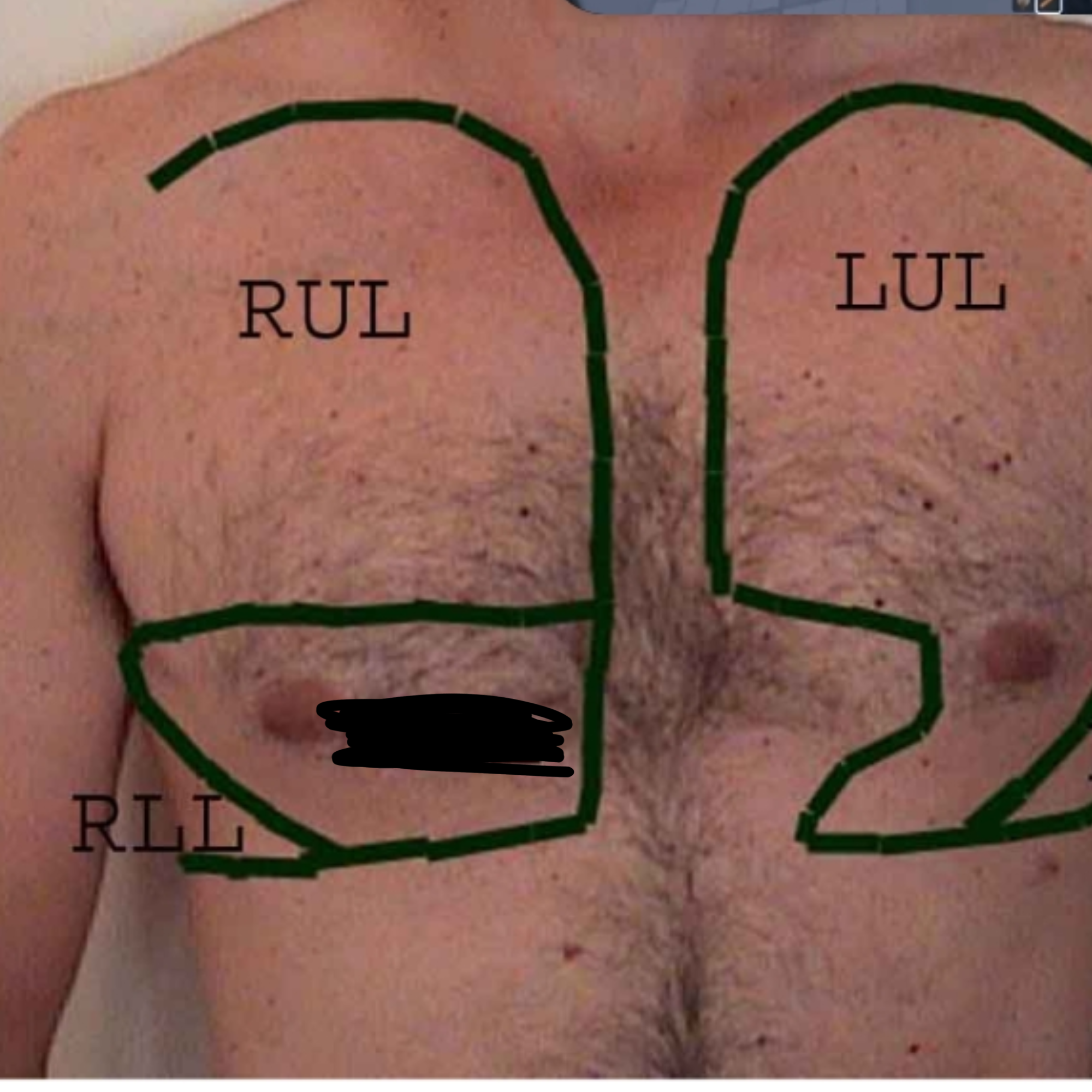
What lobe of the lung is this?
Left Upper Lobe

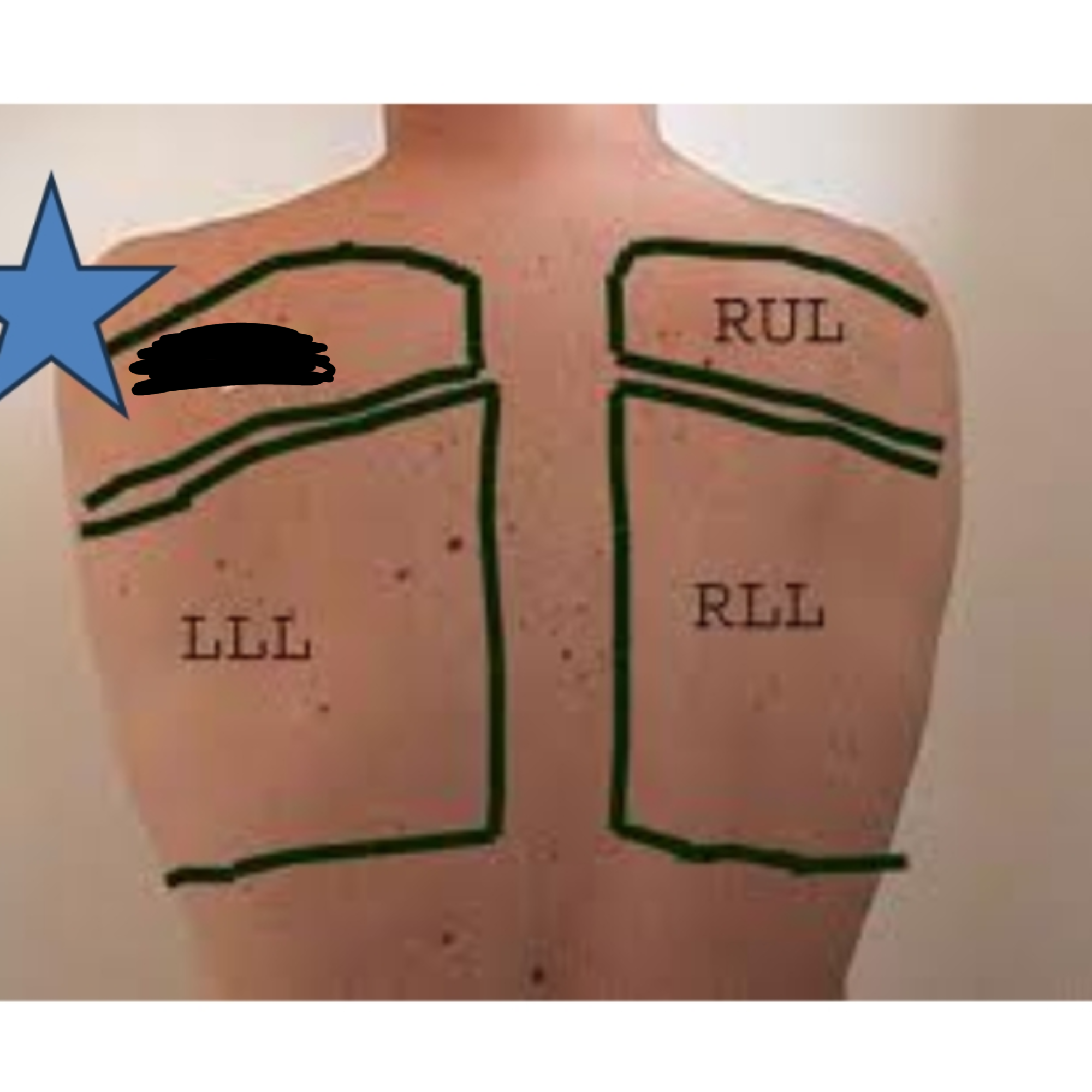
What lobe of the lung is this?
Left Lower Lobe

What lobe of the lung is this?
Right Upper Lobe

What lobe of the lung is this?
Right Lower Lobe
What lobe of the lung is this?
Right Middle Lobe
Where is the most appropriate place to check for a pulse during a code?
Carotid artery on the neck
What is the normal pulse range and what are the terms for high and low pulse?
60 to 100 beats per minute
Tachycardia greater than 100: anxiety, hypoxemia, exercise, fever, anemia
Bradycardia under than 60: diseased heart, athletes, medication side effect
Apnea
Absence of spontaneous ventilation
Eupena
Normal rate and depth of breathing
Bradycardia
Less than normal rate of breathing
Tachycardia
Rapid rate of breathing
Hypopnea
Decreased depth of breathing
Hyperpnea
Increased depth of breathing with or without an increased rate
Sighing respiration
Normal rate and depth of breathing with periodic deep and audible breaths
Intermittent breathing
Irregular breathing with periods of apnea
Terminology for clinical labs: Erythrocytes, Leukocytes, Thrombocytes
Erythrocytes: Red blood cells
Leukocytes: White blood cells
Thrombocytes: platelets
Terminology for clinical labs: CBC, PT, APTT
CBC: Complete blood count
PT: prothrombin time
APTT: Activated partial thromboplastin time
Terminology for clinical labs: Neutropenia, Anemia, Polycythemia, Coagulation
Neutropenia: a decrease in the neutrophils
Anemia: decrease in the RBCs
Polycythemia: An abnormal increase in the number of circulating RBCs
Coagulation: ability of blood to clot
Terminology for clinical labs: Hemostasis
Ability to prevent hemorrhage, form a blood clot, keep blood flowing in circulation
Terminology for clinical labs: Expectorated Sputum
Preferred method goal is to collect fresh, uncontaminated secretions from tracheobronchial tree. If sputum is needed to look for AFB, THREE samples are needed. Early AM specimens are the best time to obtain. Need 3-5 mL (about 1 teaspoon).
Terminology for clinical labs: Induced sputum
If patient is unable to cough anything up, a sputum induction may be ordered. Hypertonic saline is used via SVN. It is irritating to the airways and may help stimulate a cough.
Terminology for clinical labs: BAL: Bronchoalveolar lavage
Performed via a bronchoscopy by injecting a large volume of fluid into the lungs and then collecting it (sucking it back out) after it mixes with the cells in the lung helps to diagnose interstitial lung disease and the organism causing penumonia
What WBC types and levels of each indicate
Neutrophils: * 50-70% of our WBC most numerous type- our soldiers called into battle to fight infection
Eosinophils: 1-3% of our WBC (accumulate in allergic reactions)
Basophils: 0-1% of our WBC- may also accumulate in allergic reactions
Lymphocytes: 20-40* of WBC- useful in the fight against viral, fungal and TB infections
Monocytes: 2-11% of WBC
What are clinical lab studies for bleeding/coagulation
APTT - Activated Partial Thromboplastin time (APTT)
PT - Prothrombin Time
TCT - Thrombin clotting time
What are the lab studies that evaluate kidney function
BUN: 7 to 20 mg/dL
Creatinine: 0.7- 1.3 mg/dL
GFR: glomerular filtration rate- calculation used to measure kidney function and indicate stage of renal disease.
Urinalysis:
-Urea is a waste product that the kidneys eliminate
-Many kidney diseases result in decreased filtration and increased retention of urea
-BUN will be elevated in other conditions- esp. heart failure
What are CK- MB, troponin, and BNP?
CK-MB- specific for heart damage
Troponin- elevated in heart damage
BNP: (B-type natriuretic peptide) <100 pg/mL, can rule out CHF
how breathing patterns are associated with certain diareses
Bradypnea: Slow breathing (<10–12 breaths/min) often associated with medication-induced respiratory depression (e.g., narcotics) or increased intracranial pressure.
Tachypnea: Fast, shallow breathing (>20–24 breaths/min) associated with pneumonia, pulmonary edema, or anxiety.
Orthopnea: Difficulty breathing while lying flat; associated with congestive heart failure (CHF).
Normal levels of labs ex: glucose, potassium, WBC
Glucose: Normal fasting blood sugar levels range from 70 to 99 mg/dL
Potassium: 3.5 to 5.0 mEq/L
WBC: 4,500 and 11,000
What disorders where unilateral chest movement may occur
pneumothorax
pleural effusion
flail chest
pneumonia
diaphragm paralysis
What is chest expansion and what reduced expansion signifies
Assessing or improving the thoracic cavity's ability to expand during breathing, crucial for optimal lung function
Reduced expansion signifies a decrease in thoracic mobility and lung volume expansion during breathing, indicating underlying pulmonary, pleural, or thoracic musculoskeletal dysfunction.
Where do you used palpation percussion and expansion to diagnose a pneumonia.
the posterior, lateral, and anterior chest wall
What is subcutaneous emphysema
It's when air leaks from the lung into the subcutaneous tissue and fine beads of air make a crackling sound and popping sensation when palpated
Normal Breath Sounds: Vesicular or normal
Pitch: Low
Intensity: Soft
Location: Peripheral lung areas
Normal Breath Sounds: Bronchovesicular
Pitch: Moderate
Intensity: Moderate
Location: Around upper part of sternum, between scapulae
Normal Breath Sounds: Tracheal
Pitch: High
Intensity: Loud
Location: Over trachea
What is vocal fremitus and what does each finding mean
The vibrations created by the vocal cords during phonation
Consolidation/Pneumonia: Air in the alveoli is replaced with fluid, pus, or cells, allowing vibrations to pass through more easily
Lung Tumor/Mass: A solid mass can transmit vibrations more efficiently.
Lung Collapse (Atelectasis): Specifically when the main bronchus is still open.
Fibrosis: Dense tissue acts as a better conductor
What is a D-dimer used for
Is produced as a result of the breakdown of fibrin clots that form in the vasculature
Used often when pulmonary emboli are suspected
What is the significance of abnormal potassium: Hypokalemia
Decreased Potassium Intake
(Low-potassium diet and Alcoholism)
Increased Loss of Potassium
(Gastrointestinal loss, Rental disease, Diuretics)
Extacellular-to-Intracellular Shift of Potassium
(Alkalosis, Increased plasma insulin, Diuretics use)
What is the significance of abnormal potassium: Hyperkalemia
Increased Potassium Intake
(High-potassium diet, Oral potassium supplement, Transfusion of old blood)
Decreased Potassium Excretion
(Rental failure and Hypoalsosteronism)
Intracellular-to-Extracellular Shift of Potassium
(Acidosis, Crush injuries, Tissue hypoxia)
Pseudohyperkalemia
(Hemolysis and Leukocytosis)
What are the 4 components of the physical exam
Inspection
Palpation
Percussion
Auscultation
What is myosis?
Pupil constriction (pontine hemorrhage, narcotics)
JVD is
most common cause of Distended external jugular vein is right-sided heart failure
How can you tell restrictive spine chest
limited lung expansion leading to shortness of breath, chronic back pain, and reduced mobility in the rib cage
How can you tell sternum configurations
Pectus carinatum: Outward sternal protrusion anteriorly
Pectus excavatum: Depression of part or all of the sternum
What does skin turgor help us identify in assessment?
Tells us about hydration status
A good specimen of Sputum Examination will have
few epithelial cells and many leukocytes
A high number of epithelial cells indicate
oral contamination with saliva
What is the Glasgow Coma Scale
Most widely used instrument to quantify neurologic impairment
-Score given for several categories:
Motor response
Verbal response
Poorly suited for patients with impaired verbal response (e.g., aphasia, hearing loss, tracheal intubation)
Eye opening
Issues with the brain stem can affect
regulation of heart rate, blood pressure, and breathing (apneas, hyperventilation, etc)
Phrenic nerves that arise from
C3-C5
Damage to the spinal nerves or above can result
in diaphragmatic paralysis and paralysis of intercostal muscles
In patients with an intact brain stem, the eyes
will move laterally toward the affected ear
In patients with severe brain stem injury, the
gaze will remain at midline
Cheyne-Stokes respiration includes
Intracranial cause * (also hypoxemia, cardiac failure)
Hyperventilation
Apneustic breathing
Ataxic breathing (Biot’s)- severe brainstem issues
Normal ICP includes
10-15mmHg
Declaration of Brain Death includes
Irreversible condition occurring when all perceptible brain activity has seized
Caused by: massive stroke, brain injury, and prolonged cardiac arrest
Establishing brain death will be the grounds used to pronounce a patient dead (even if the heart is still beating) and turn off the ventilator and/or other life-saving measures
A physician and an RT are usually involved in
an “apnea test” which is part of the clinical exam
Looks for an increase in C02 while off
ventilator and the absence of spontaneous breathing
this means that pt. brain is not responding to c02 by breathing