NR 304- Health Assessment II Final Exam
1/244
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
245 Terms
grading pulse
3+ full bounding
2+ normal
1+ weak
0 absent
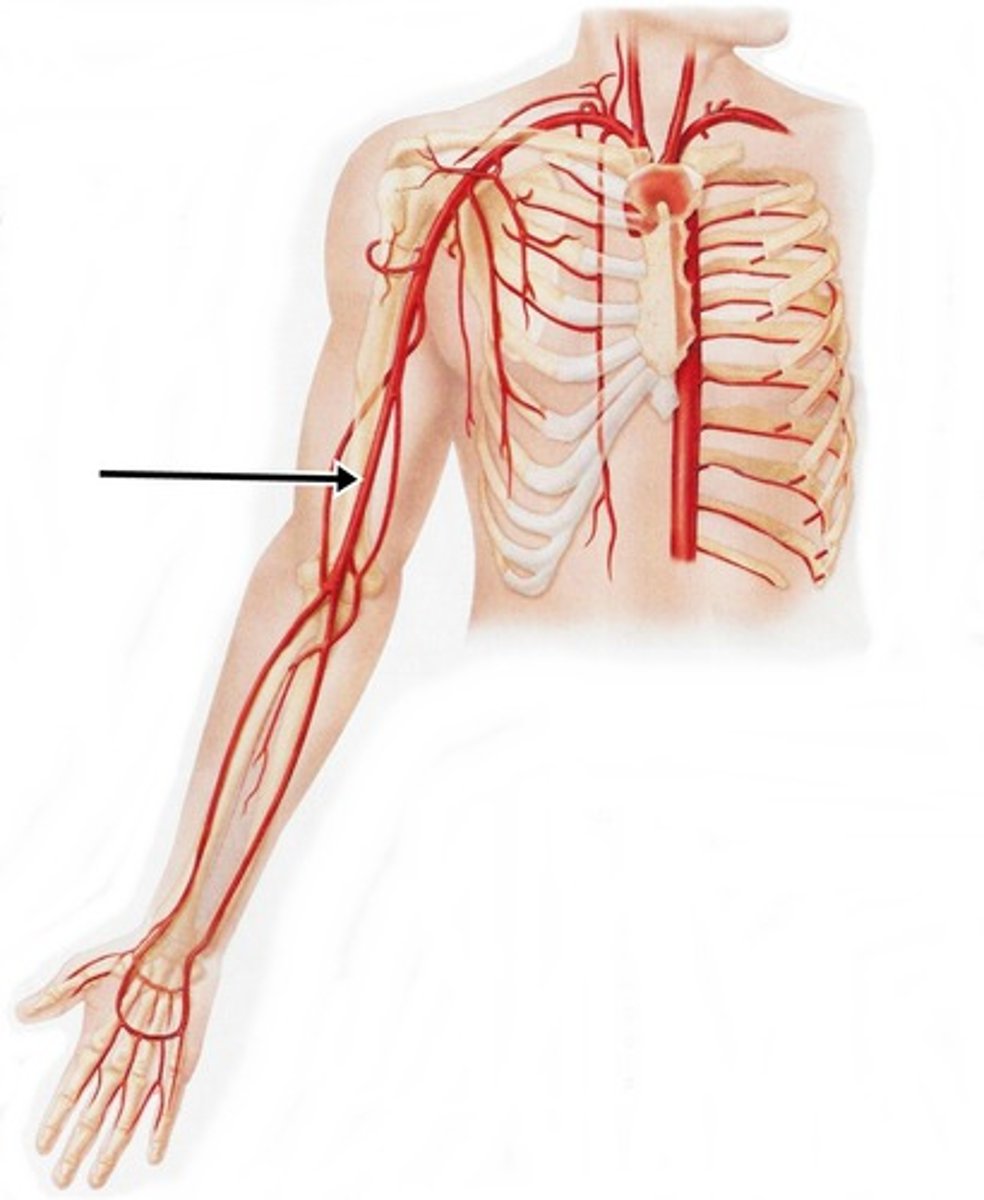
brachial pulse
palpate this pulse if you suspect arterial insufficiency
temporal artery
palpated in front of the ear
carotid artery
palpated in the groove b/t the sternomastoid muscle and the trachea
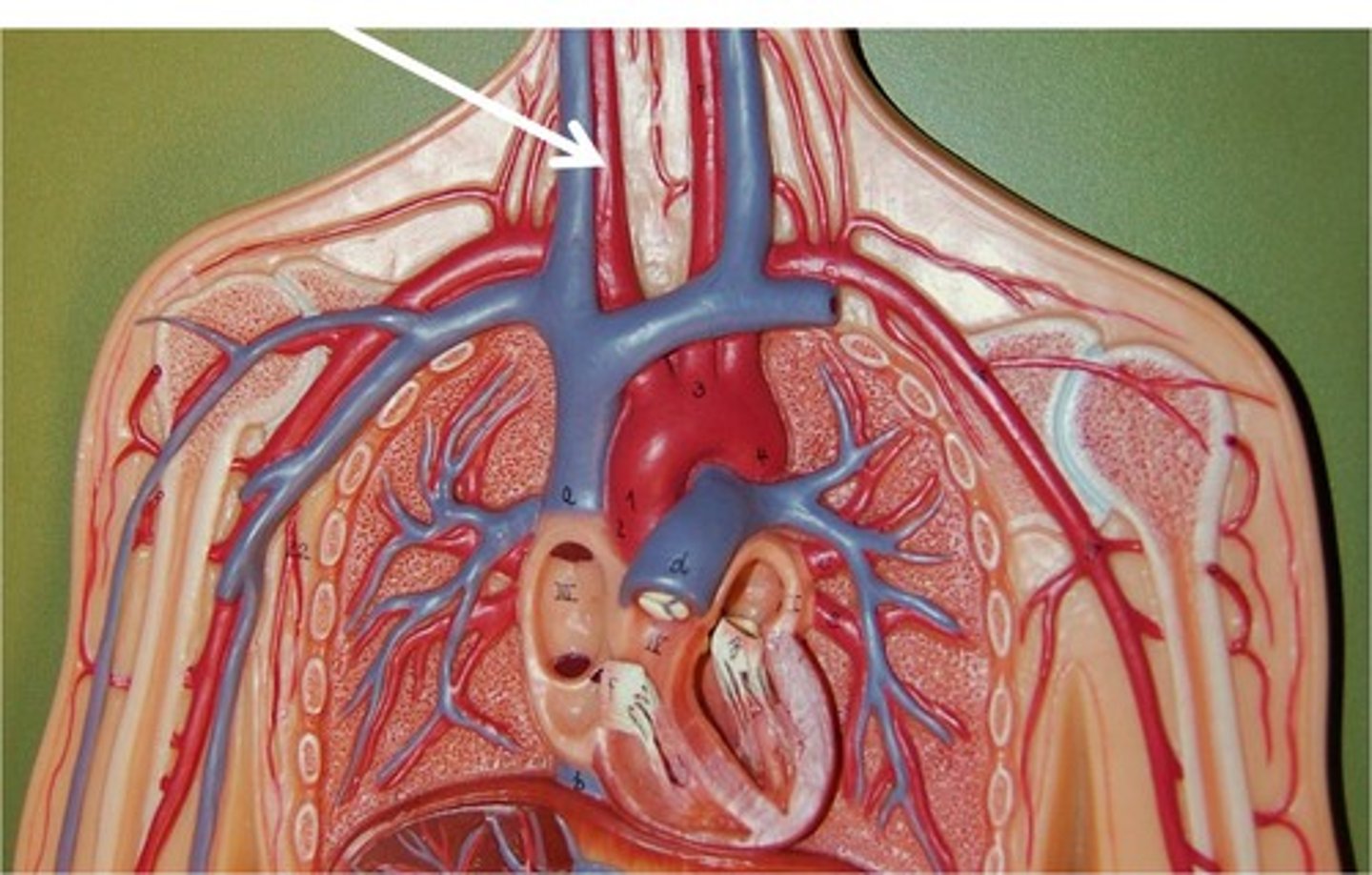
brachial artery
major artery supplying the arm
radial artery
lies medial to the radius and wrist supplies blood to the hand
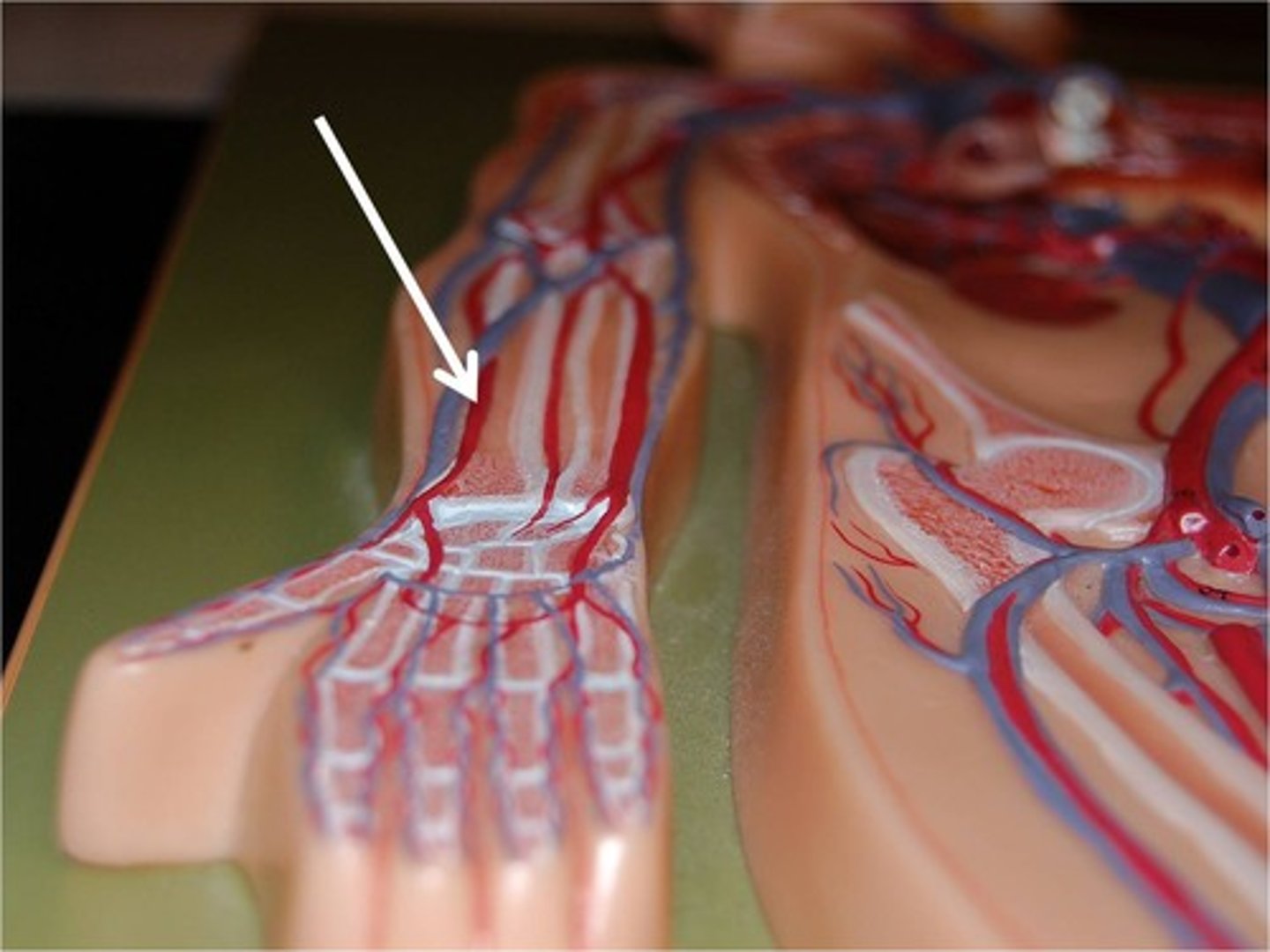
ulnar artery
lies lateral to the ulna. Deeper and often difficult to feel. Supplies blood to the hand
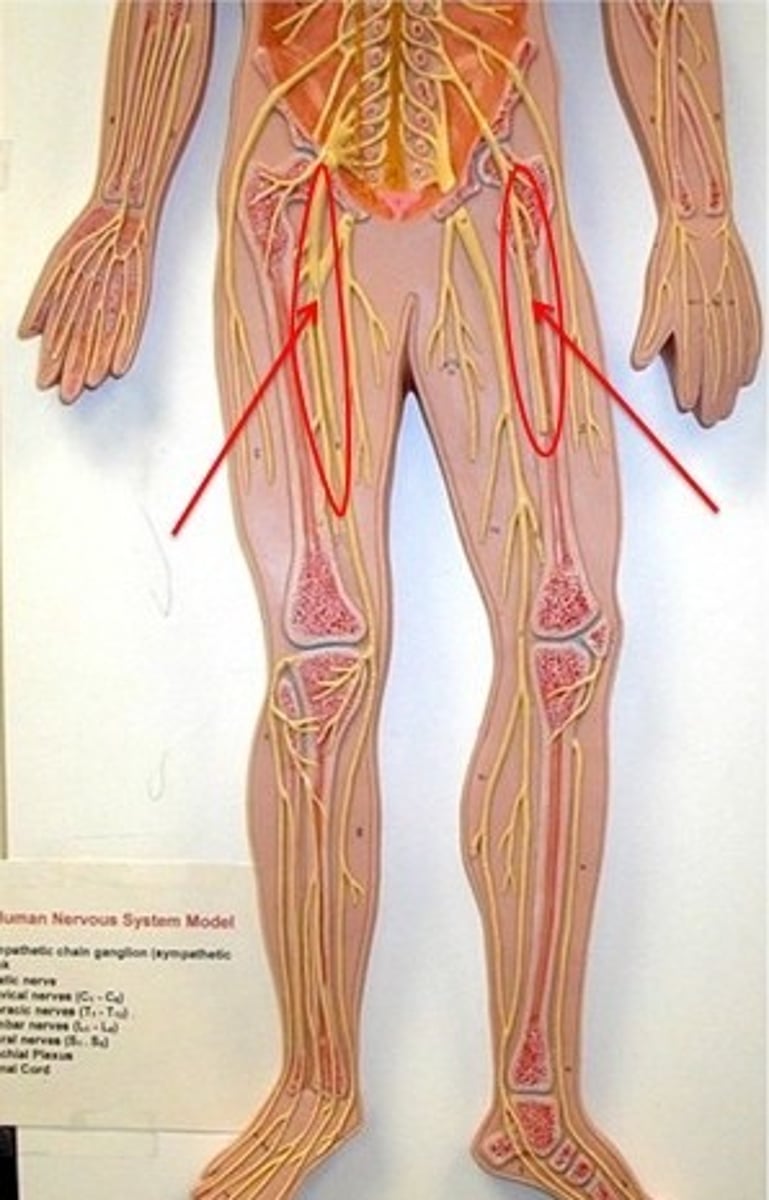
femoral artery
major artery in the leg. Palpated in the inguinal area
popliteal artery
artery in the knee. Located posterior to the patella. Divides into the anterior and posterial tibial artery
anterior tibial
travels down the front of the leg on to the dorsal of the foot becomes the dorsalis pedis.
carries blood to the anterior compartment of the leg and dorsal surface of the foot
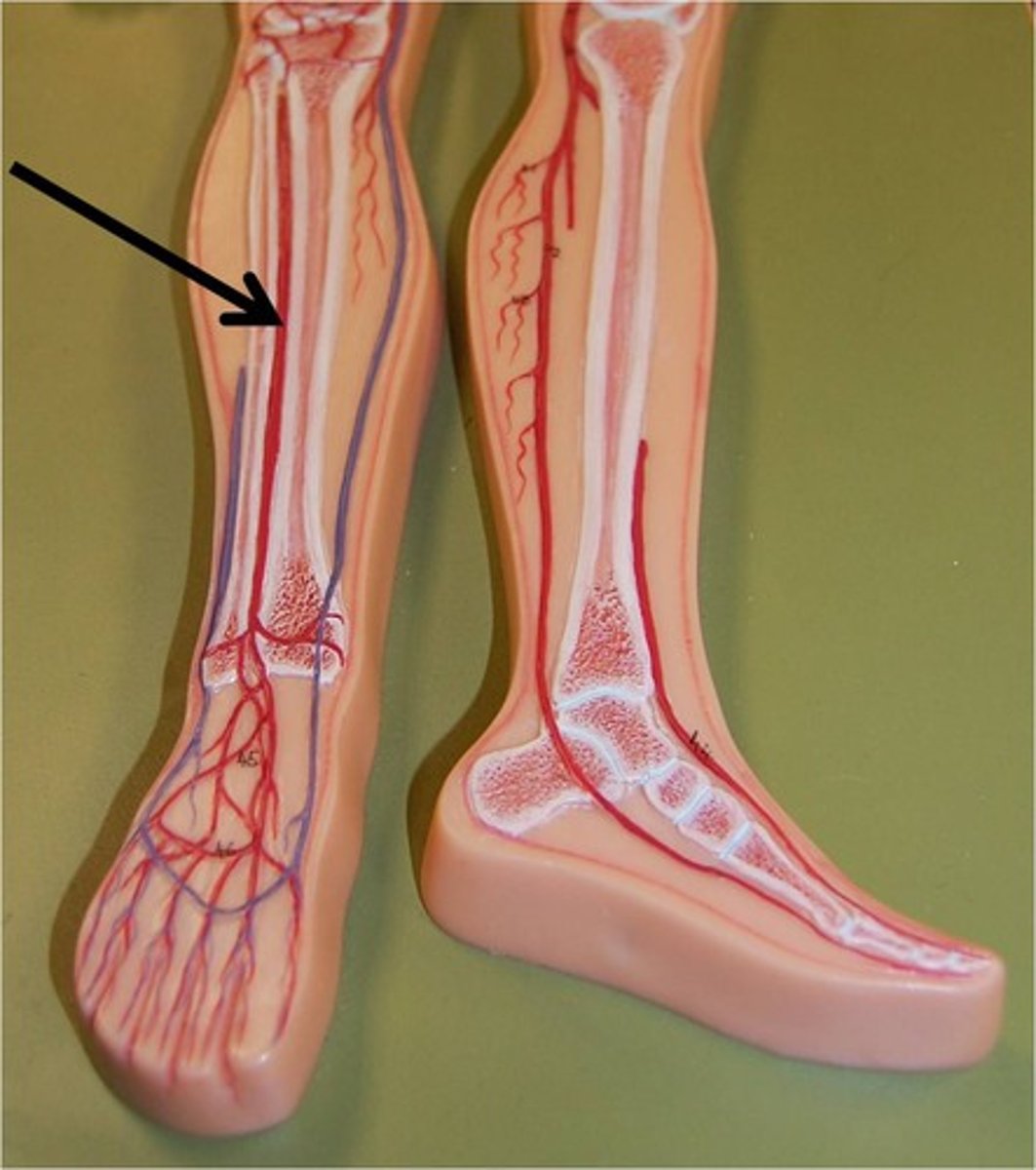
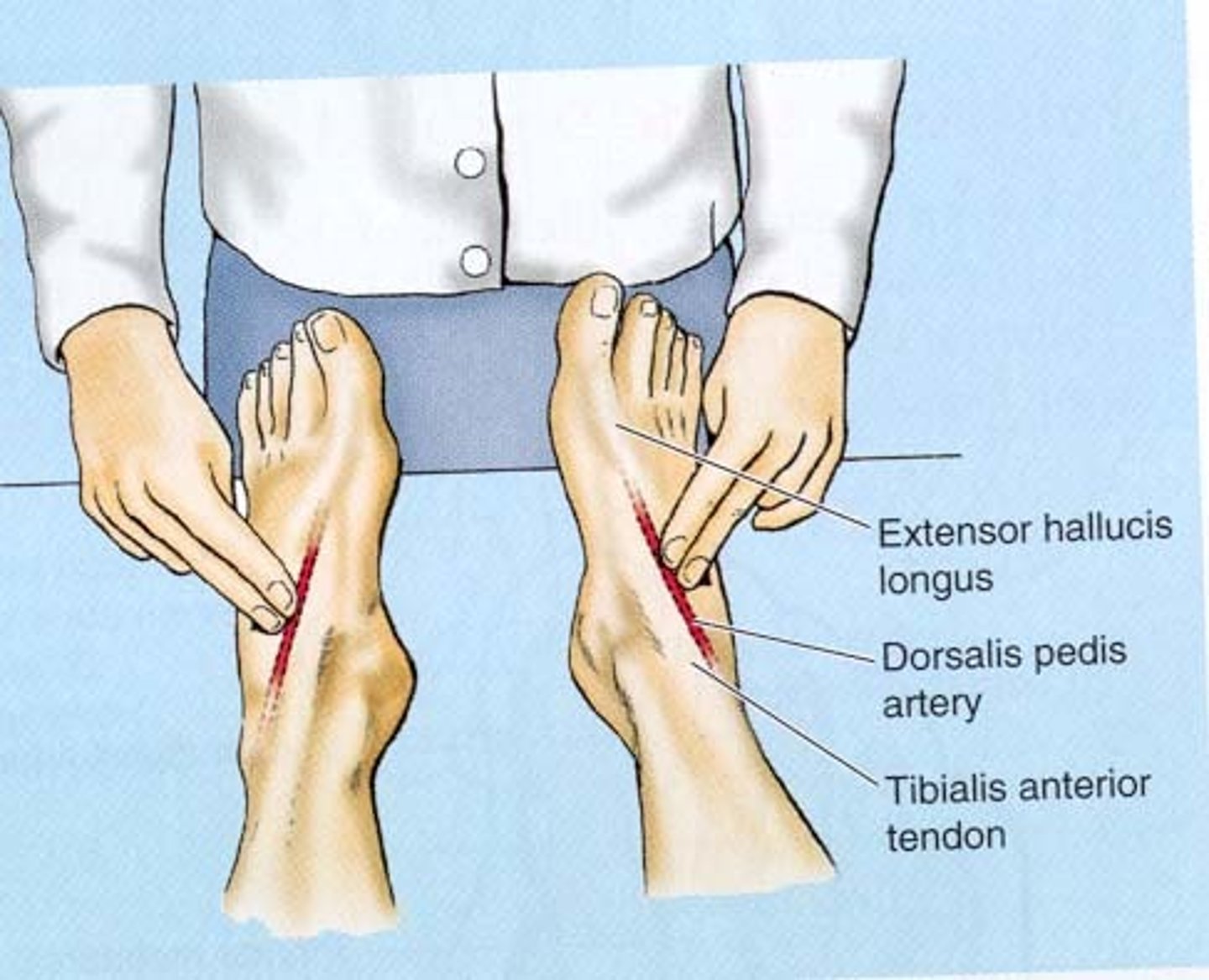
dorsalis pedis
a blood vessel of the lower limb that carries oxygenated blood to the dorsal surface of the foot
claudication distance
the number of blocks walked or stairs climbed to produce pain
peripheral perfusion
checking for capillary refill by blanching the nail beds and noting the time for color return
normal is less than 1-2 seconds
doppler
used if pulses are too weak to detect by palpation, monitor blood pressure in infants or children, measure low blood pressure or blood pressure in the lower extremities
A noninvasive test using sound waves to detect blood flow through blood vessels
ex. competent valves (varicosities)
PVD
circulation disorder in which narrowed blood vessels reduce blood flow to the limbs. Caused by arteriosclerosis (hardening of arteries caused by plaque build up)
Inspect skin for ulcers, temperature and color
lymphedema
swelling in the arms or legs caused by a blockage of the lymphatic system , causes a build up of lymph fluid in tissues
intermittent claudication
a condition in which cramping pain in the leg is induced by exercise, typically caused by obstruction of the arteries
5 P's
Pain
Pulselessness
Pallor
Parasthesia (can't feel)
Paralysis (can't move)
Grading Edema
+1 mild pitting, no swelling
+2 moderate pulling, indentation goes away quickly
+3 deep pitting, swollen
+4 very deep pitting, indentation stays, very swollen
Arterial Occlusion
-5 P's
-Mottling
- Bluish/cyanosis
- decrease capillary refill
- cold temperature
arterial insufficiency
NOT ENOUGH BLOOD TO TISSUES.
Location: Calves, Thighs
skin is cool, pale
-skin is thin and shiny
- no edema
-no hair growth
- decreased pulses
-yellow toenails
-elevated pallor
Pain with walking, relieved by rest (claudification)
venous insufficiency
Location: Lowers legs + Ankles
normal temperature
-normal pulse
-flaky, dry, thick skin
-skin tears easily- friable
-edema
-hyperpigmentation (brown)
- Aching heaviness worse with standing
Nursing priority: Elevate legs
arterial ulcers
-intermittent claudication pain
-no edema
-no pulse or weak pulse
-no drainage
-round smooth sores
-black eschar
-location on toes and feet
venous ulcers
-dull achy pain
-lower leg edema
-pulse present
-drainage
- sores w/ irregular borers
- yellow slough or ruddy skin
-location on ankles

vascular bruit
an audible vascular sound associated w/ turbulent blood flow
heaves
lift, a sustained forceful thrusting of the ventricle during systole. Occurs w/ ventricular hypertrophy as a result of increased workload
right ventricular is seen at the sternal border
left ventricular is seen at the apex
thrill
palpable vibration. Feels like the throat of a purring cat.
Signifies turbulent blood flow and directs you to the location of the origin of loud murmurs
S1
Lub. Closure of the AV valves. Heard at the apex of the heart, correlation w/ the carotid artery, signified that systole is starting
S2
Dub. Heard at the base of the heart. closure of the semilunar valves. Indicates that diastole is starting and systole is ending
AV valves
tricuspid and mitral valves. Close during systole to prevent regurgitation of blood back up into the atria. Filling phase during diastole
Semilunar valves
pulmonic and aortic valve. Opens during systole to allow blood to be ejected from the heart
systole
S1 close of AV valves
S2 openof the semilunar valves
base
top of the heart
apex
bottom of the heart
S3
Lub-dupPA heart murmur, occurs when the ventricles are resistant to filling during the early rapid filling phase.
occurs after S2 during rapid filling phase when the AV valves open and atrial blood first pours into the ventricle
(heard at the apex, low pitch, heart failure, heart overload)
S4
fourth heart sound. DaLub-dup. occurs at the end of diastole at pre-systole (before S1) when the ventricle is resistant to filling
A stiff wall (outflow stenosis, HTN, stiff ventricle)
murmurs
turbulent blood flow/ collision current caused by increased blood velocity, decreased blood viscosity and structural defect
varicosities
enlarged, incompentent valves (varicose veins)
reflex grading
0 absent
1 hyporeflexive, diminished
2 normal
3 hyper-reflexive, may indicate disease
4 abnormally reflexive, indicates disease
level of consciousness
a change in the level of consciousness. note person, place time
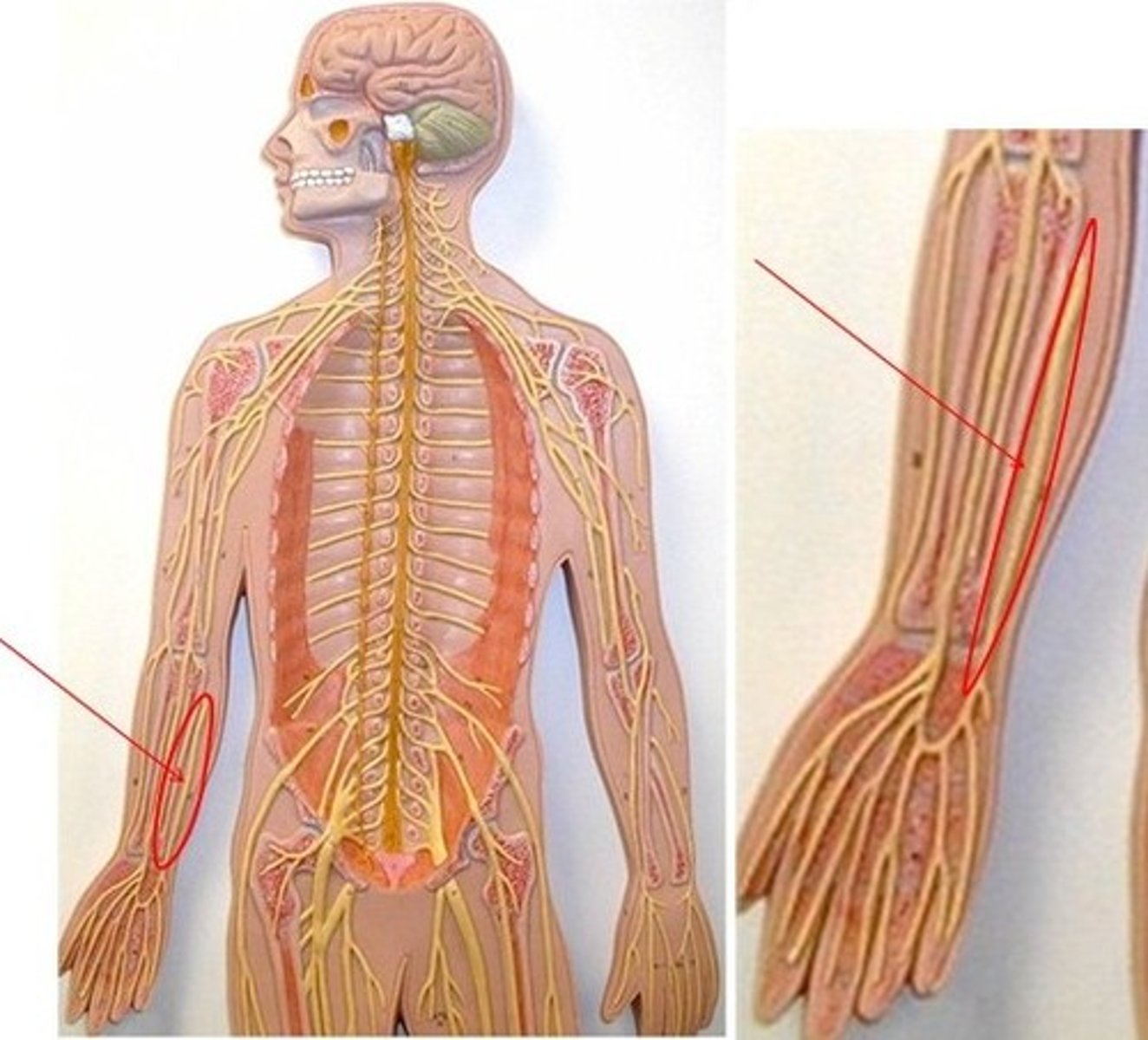
spinothalamic tract
originates in the spinal cord, transmits impulses from the spine to the thalamus on pain, temperature, itch, vibration and crude touch
sensory
lateral spinothalamic tract
pain, temperature
anterior spinothalamic tract
crude touch
posterior (dorsal column) spinothalamic tract
fine touch, sensations of position, vibration
corticospinal tract
conscious control of movement, discrete voluntary skilled movements, such as precise movement of the fingers and toes
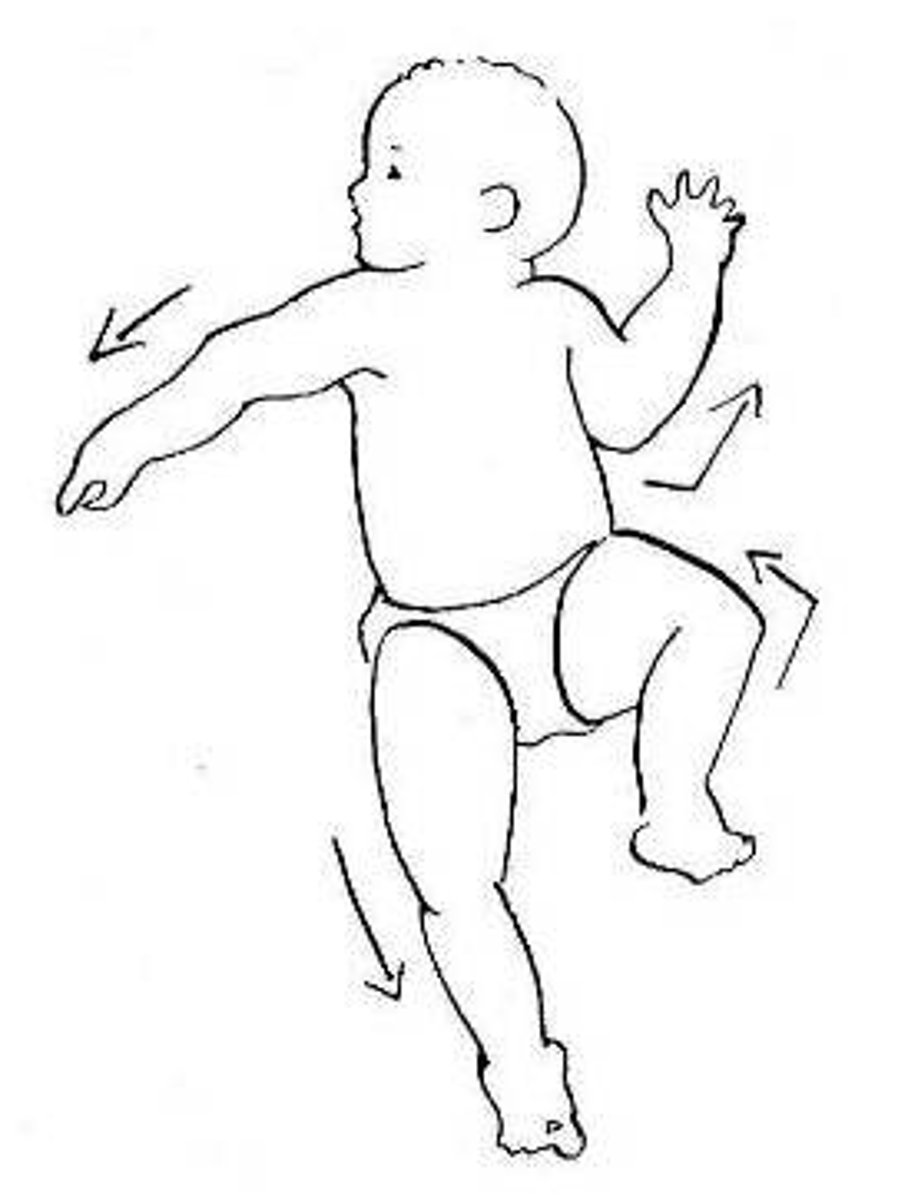
Moro reflex
startling the infant, the baby should look as if its hugging a tree (symmetric abduction and extension of the arms and legs, fanning fingers, curling of the index finger , thumb in C position)
present at 1-4 months
abnormal: absence of reflex or presents after 5 months indicates severe CNS injury

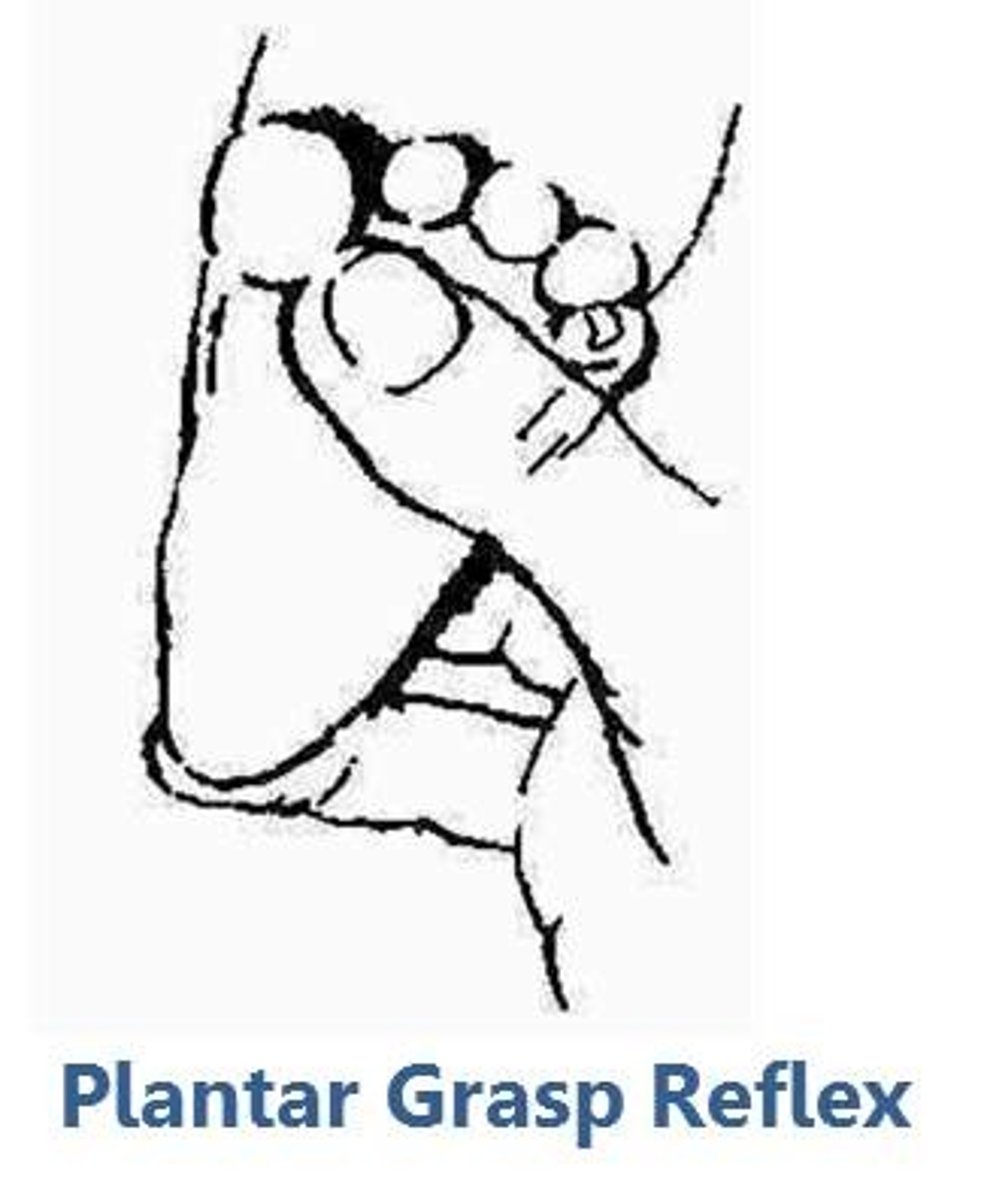
plantar grasp
touch your thumb at the ball of the baby's foot, note the toes curl down tightly, reflex present at birth and disappear at 8-10 months
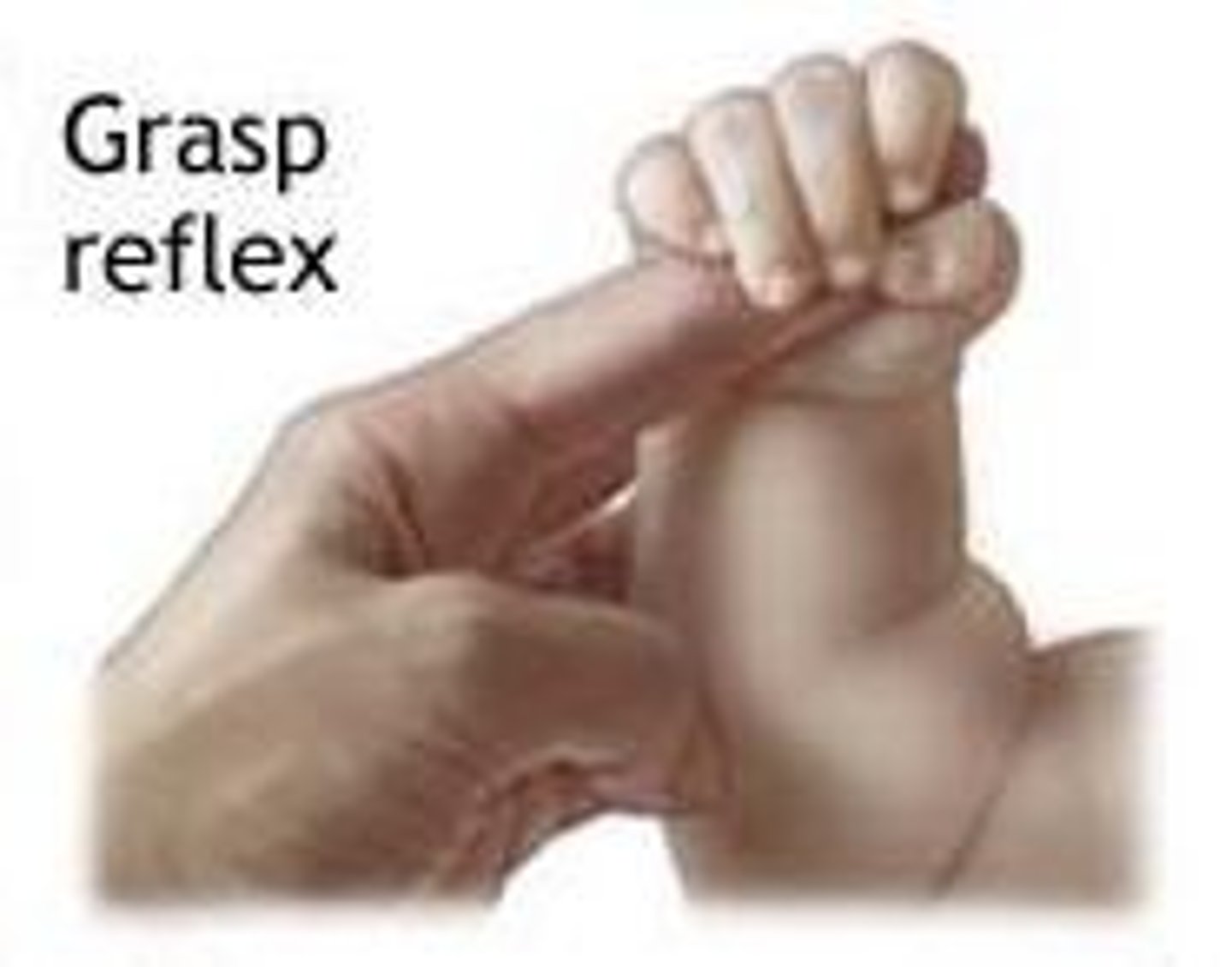
palmar grasp
offer finger from the baby's ulnar side away from the thumb, tight grasp of the baby's fingers
present at birth, strongest at 1-2 months and disappears at 3-4 months
abnormal- reflex absent w/ brain damage and local muscle or nerve injury, after 4 months indicates frontal lobe lesion
tonic neck reflex
when you turn the baby head to the side and the arms and legs will extend and the opposite will flex. Appears at 2-3 months and disappears at 4-6 months
abnormal- indicates brain damage
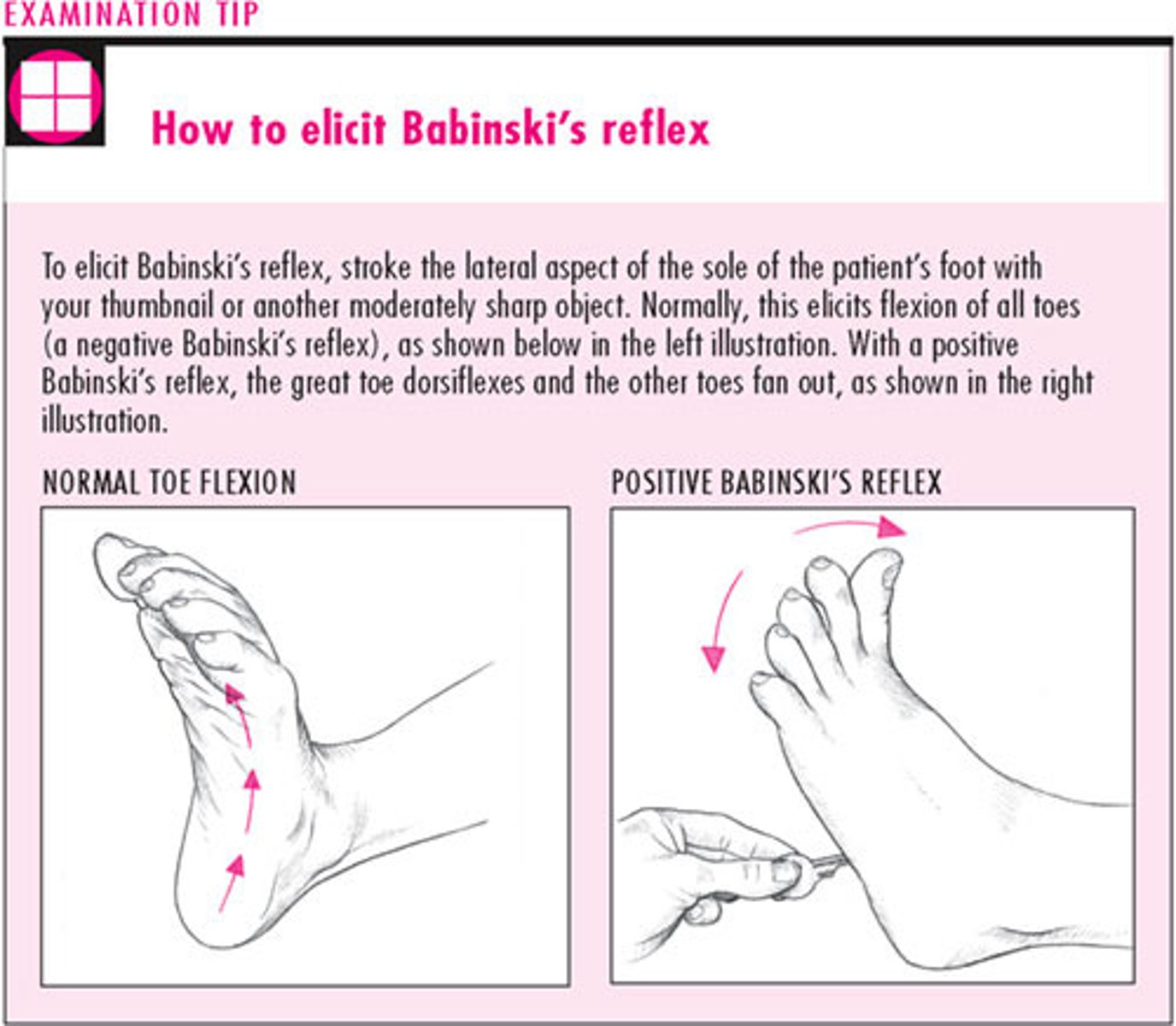
Babinski reflex
take the baby foot and make a upside down J,baby toes should go in a fanning motion (+ test in infants)
present at birth and disappears by 24 months
abnormal- present at 2 years occurs w/ pyramidal tract disease (motor) , in adults

spinothalamic test
pain
light touch
vibration
position (kinesthesia)
tactile discrimination (fine touch)
stereognosis
graphesthesia
two point discrimination
extinction
point location
conscious
promptly and spontaneously to state their name, location, date , time are said to be oriented to self, place and time ability to interact appropriately w/ in the context of the immediate environment
confused
does not respond quickly w info about their name, location and the time
poor attention
delirious
restless
agitated
hallucinations
somnolent
excessive drowsiness, mumbles
obtunded
decreased interest in surrounding, slowed response
stuporous
unresponsive and requires vigorous stimulation (painful) for arousal; once aroused the patient may be confused, agitated, unable to follow commands
comatose
does not make this response to stimuli, have no corneal or gag reflex, and they may have no pupillary response to light
CN I
olfactory nerve, smell
CN II
optic, sensory, visual acuity, pupillary reflex ocular fundus
test: Snellen Chart,
CN III, IV, VI
EOM
-oculomotor (superior rectus, inferior rectus and oblique, medial rectus)
-Trochlear (superior oblique)
-Abducens (lateral rectus)
CN VII
facial, sensory and motor
motor: smile, tightly close eyes, lift eyebrows, puff out cheeks, frown
sensory: taste buds
CN VIII
acoustic, sensory
whisper test, rinne test, weber test, equilibrium (romberg)
corneal light reflec
CN IX
glossopharyngeal, sensory and motor
motor: soft palate and uvual rise in midline, and phonation, swallowing
sensory: gag reflex
CN X
vagus, sensory and motor
motor: phonoation, swallowing, gag reflex
sensory: sensation from the carotid body (lowers heart rate, pharynx, GI secretions)
CN XI
spinal accessory, motor
turn head against resistance, shrug shoulders against resistance
CN XII
hypoglossal (motor)
tongue protrusion, tongue retraction, lingual speech (light, tight, dynamite)
CN V
trigeminal , sensory and motor
sensory: facial sensations, corneal reflex
motor: blinking, clenching teeth, movement of jaw
cerebellar tests
Romberg
Pain
spinothalamic test, sharp and dull
hypoalgesia
decreased pain sensation
analgesia
absent pain sensation
hyperalgesia
increased pain sensation
light touch test
spinothalamic test, apply a wisp of cotton to the skin ask person to say yes when the touch is felt. CN V, VII (if on face, corneal reflex)
hypoesthesia
decreased touch sensation
anesthesia
absent touch sensation
hyperesthesia
increased touch sensation
vibration
spinothalamic test, tests the persons ability to feel vibrations of a tuning fork over bony prominences. Ask pt when the vibrations starts and stops
abnormal- unable to feel vibrations, loss of vibration sense occurs w/ peripheral neuropathy (diabetes, alcoholism)
position (kinesthesia)
tests the persons ability to perceive passive movements of the extremities. move a finger or big toe up and down and ask pt to tell you which way it is moved
abnormal- loss of position sense
tactile discrimination
fine touch test, measured the discrimination ability of the sensory cortex
abnormal: lesions of the sensory cortex or posterior column
stereognosis
tests the persons ability to recognize objects by feeling their forms, size and weights.
place a familiar object in the person hand and ask pt to identify it.
abnormal: asterognosis
asterognosis
inability to identify object correctly occurs in sensory cortex lesions (stroke)
graphesthesia
the ability to "read" a number by having it traced on the skin. A good measure of sensory loss if the person cannot make the hand movements needed for sterognosis
two point discrimination
tests the persons ability to distinguish the separation of two simultaneous pin point on the skin.
Apply two point of an opened paper clip to the skin note the distance which the person no longer perceives two separate points
mental status exam
measures appearance, behavior, thought process and cognition
parathesia
numbness, losing ability to feel
cerebellar test
-rapid alternating movements (RAM)
-finger to finger test
-finger to nose test
-heel to shin test
-gait
-Romberg test
-heel to toe (tandem walking)
rapid alternating test
cerebellar test, ask the person to pat the knees w/ both hand and turn over and pat knees . should be done with equal turning and a quick, rhythmic pace
abnormal- lack of coordination, slow, clumsy and sloppy response
finger to finger
w/ persons eyes open, ask the he or she use the index finger to touch your finger and this their own finger should be smooth and accurate
abnormal- lack of coordination, dysmetria, past pointing
dysmetria
clumsy movement w/ overshooting the mark and ccurs w/ cerebellar disorders or acute alcoholism
past pointing
a constant deviation to one side
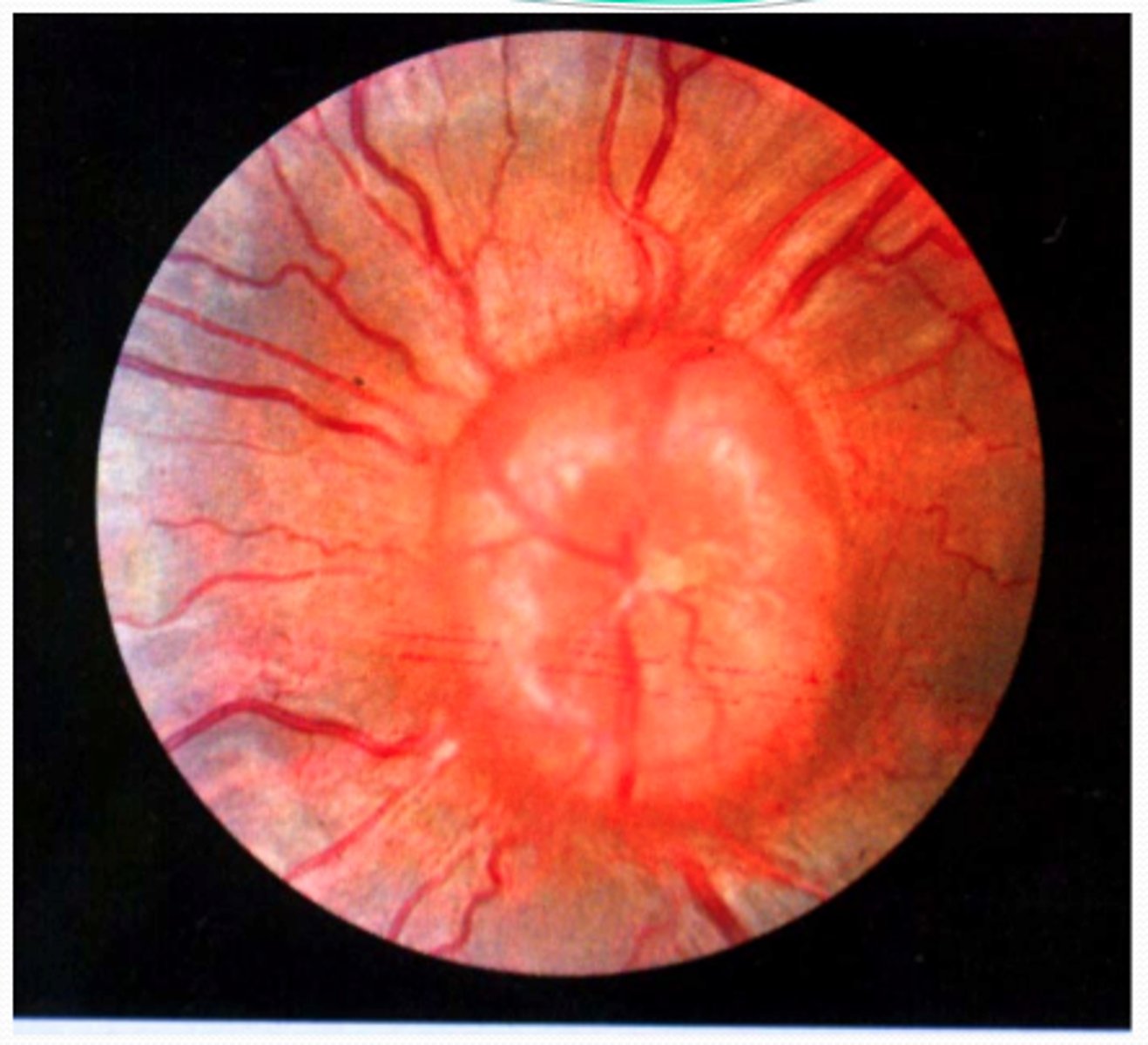
papilledema
abnormal CN II inspection increased intracranial pressure
Babinski adults
abnormal plantar reflex test. Dorsiflexion of the big toe and fanning of the toes
cerebrovascular accident (CVA)
stroke, occurs when the blood flow is interrupted to a part of the brain
ischemic stroke
most common, occurring when a blood clot blocks a blood vessel in the brain
hemorrhagic stroke
less common stroke, occurs when a blood vessel in the brain ruptures and causes bleeding
symptoms of a stroke
-weakness or numbness in the face, arms or legs
-confusion
-changes in vision
-trouble walking, dizziness, loss of balance, coordination
-severe headache w/ no reason or explanation
recognition of a stroke
Face- are they equal on both sides (facial droop)
Arms- can client raise both arms equallt (arm drift)
Speech- slurred speech or inappropriate words or mute
Time- EMERGENCY
Parkinson's disease
death of dopamine generating cells in midbrain
symptoms of Parkinson's disease
-slow rigid movement
-dementia
-stoop posture
-shuffling gait
-pill rolling
-tremors
-bradykinesia
-rigidity
-impaired balance
-small handwriting