Part 8a - 2026 BRVO, CRVO, hemicentral retinal vein occlusion
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
What is the second most prevalent vascular disease behind diabetic retinopathy seen in clinical practice today?
Retinal vaso-occlusive disease:
BRVO
CRVO
hemicentral rentinal vein occlusion
BRAO
CRAO
hemicentral retinal artery occlusion
How significant is stroke as a cause of mortality in the U.S.?
Stroke is the 4th or 5th leading cause of death in the U.S., reflecting its major public health impact.
What is a transient ischemic attack (TIA), and how often does it precede a stroke?
A TIA is a transient episode of neurologic dysfunction caused by focal ischemia without infarction.
• Occurs before ~10% (or fewer) of strokes.
• Symptoms usually last < 5 minutes, but can persist for hours.
What is the risk of stroke after a TIA?
About 29.5% of patients with TIAs develop a stroke within 1 year.
High early recurrence risk → requires rapid evaluation and treatment.
How does early treatment after a TIA or minor stroke impact future stroke risk?
Treatment initiated within 24 hours reduces the 90‑day stroke risk by ~80%.
This protective effect remains detectable even 10 years later.
What medications are used to treat TIAs and prevent subsequent stroke?
Primary therapy: Antiplatelets
• Aspirin
• Clopidogrel (Plavix)
May also use anticoagulants when indicated:
• Apixaban (Eliquis)
• Rivaroxaban (Xarelto)
What are the sings and symptoms of TIA/Strokes?
Sudden numbness or weakness of face, arm, or leg on 1 side of the body
Temporary problem with speech
Temporary difficulty understanding speech
Temporary loss of vision in 1 eye (amaurosis fugax or transient monocular blindness or TMVL - transient monocular vision loss)
What is the stroke FAST acronym?
Face drooping
Arm may be weak or numb
Speech difficulty
Time to call 911
What is the 2nd most common retinal vascular disease seen in eyecare?
Branch retinal vein occlusion (1st is diabetic retinopathy)
What are the characteristics of BRVO?
incidence rate <2%
Rarely seen in individuals <50, prevalence increases with age
4-5% bilateral
What is BRVO commonly related to?
Hypertension. Other systemic associations include hyperlipidemia, atherosclerosis, and hypercoagulable systemic disorders such as hyperhomocysteinemia and antiphospholipids syndrome.
What is a significant risk factor for BRVO?
Smoking. Not as strong correlation with diabetes, open angle glaucoma
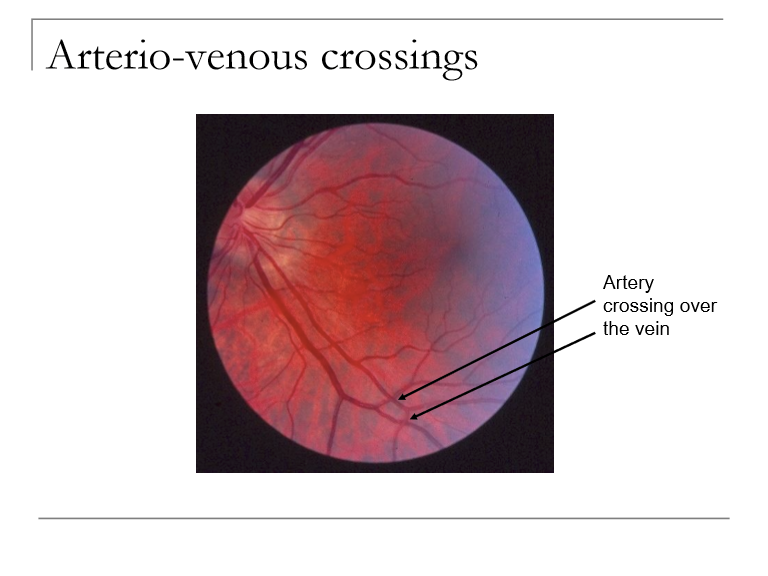
What is the pathophysiology of BRVO?
arteriosclerosis such that an artery compresses a vein at the arterio-venous crossing
Occlusion of vein due to thrombosis
What are the 2 categories of BRVO?
Macular BRVO: probably a blockage of a branch of a branch
Major BRVO: blockage of a major branch
How does the location of a retinal vein occlusion determine the extent of retinal hemorrhage?
The more proximal the occlusion, the greater the area of retina affected:
Small branch → localized area
Major branch → one quadrant
Hemicentral → two quadrants
Central retinal vein → all four quadrants
What retinal involvement pattern is seen in a hemicentral retinal vein occlusion (HRVO)?
HRVO → hemorrhage in TWO quadrants
(usually both superior or both inferior).
What is the hallmark distribution of hemorrhage in a central retinal vein occlusion (CRVO)?
CRVO → hemorrhage in ALL FOUR quadrants of the retina.
Represents obstruction of the main central retinal vein → diffuse congestion, venous tortuosity, widespread hemorrhages.
What is the underlying mechanism of branch retinal vein occlusion (BRVO), and why is the superior temporal quadrant most commonly affected?
BRVO results from compression of a branch retinal vein at an arteriovenous (AV) crossing, usually due to arterial sclerosis.
The superior temporal retina is most affected because it has the highest number of AV crossings, increasing the likelihood of venous compression and occlusion.
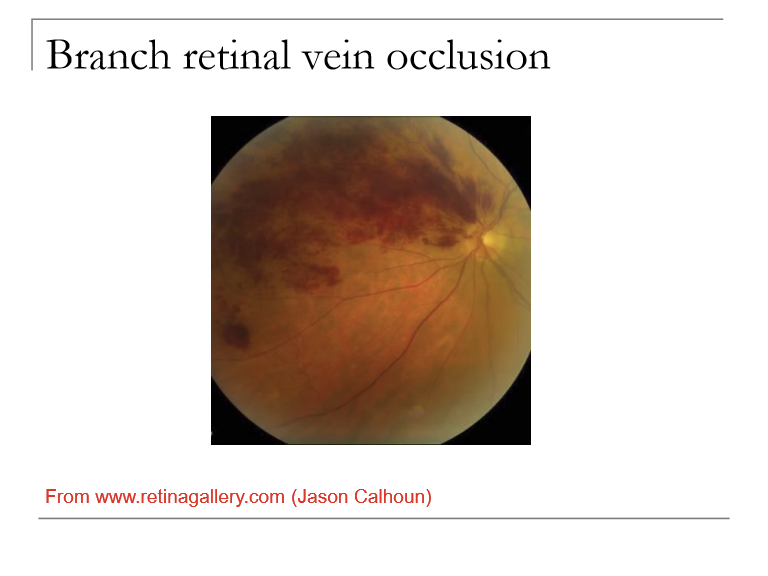
What are the key fundoscopic findings in BRVO?
BRVO shows changes limited to the sector drained by the affected vein, including:
Dilated, tortuous veins
Flame-shaped hemorrhages (primary)
Dot-blot hemorrhages
Sectoral distribution matching the occluded branch
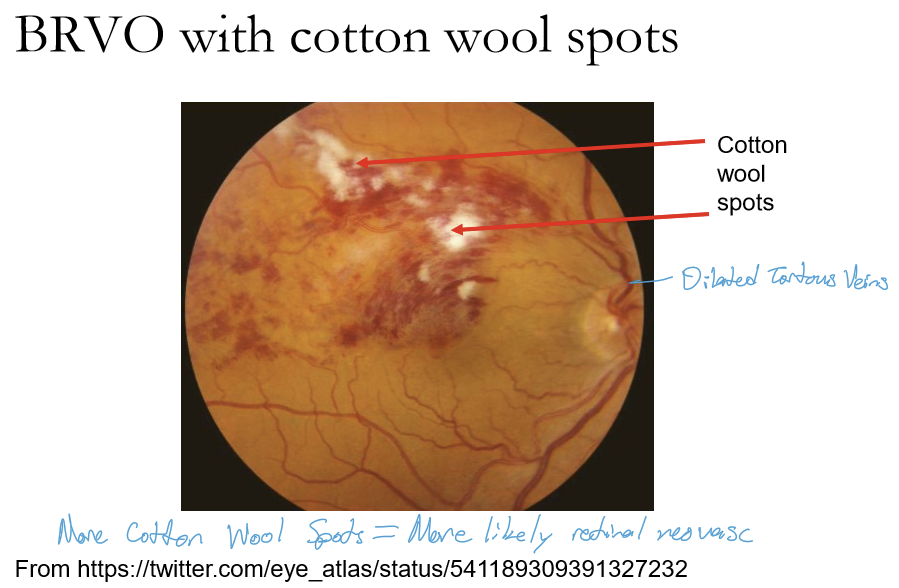
What are potential problems in BRVO?
Hypoxia with potential for retinal neovascularization (~8% of BRVO patients develop retinal neovascularization which may be hidden by hemorrhage)
Microaneurysms appear, can leak, creating retinal edema which can include macular edema
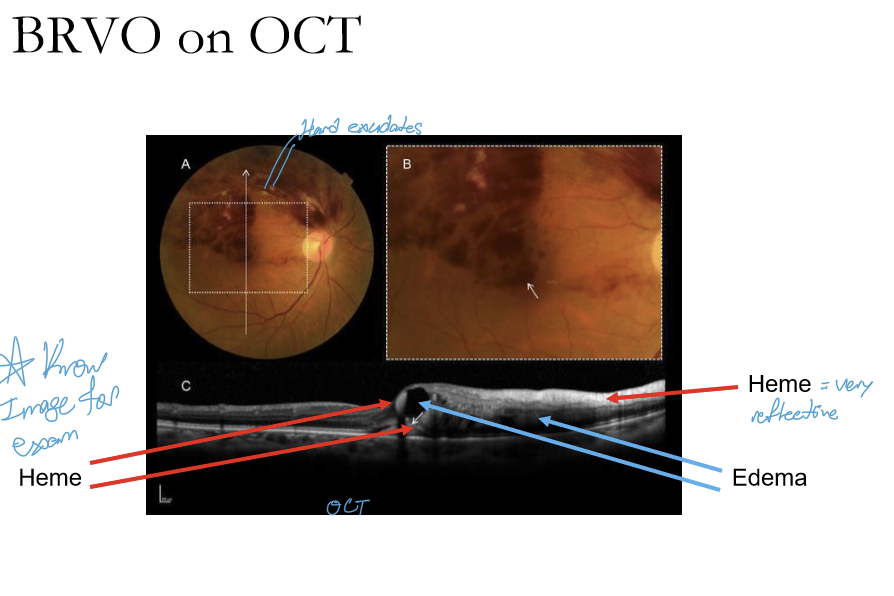
How does BRVO appear on OCT?
Heme is hyperreflective with pockets of edema
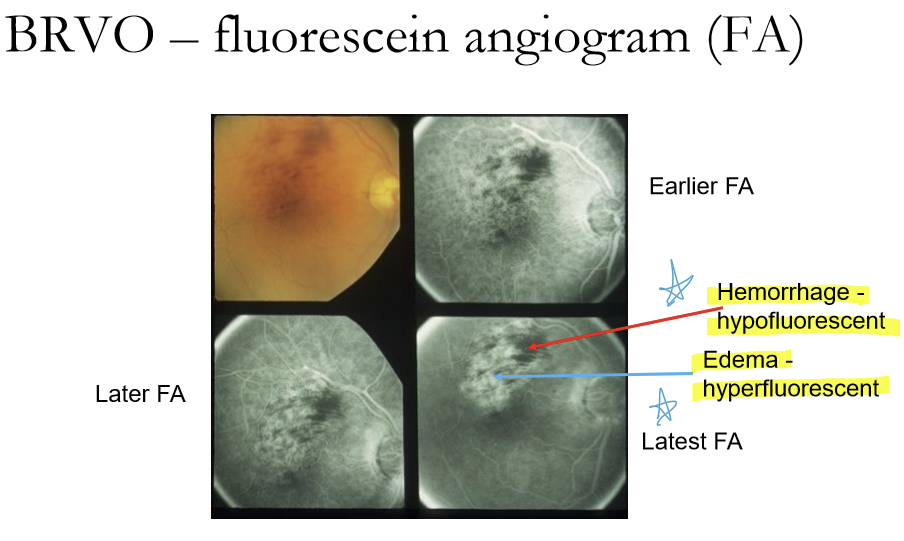
How does BRVO appear on FA?
Hemorrhage are hypofluorescen. Edema are hyperfluorescent.
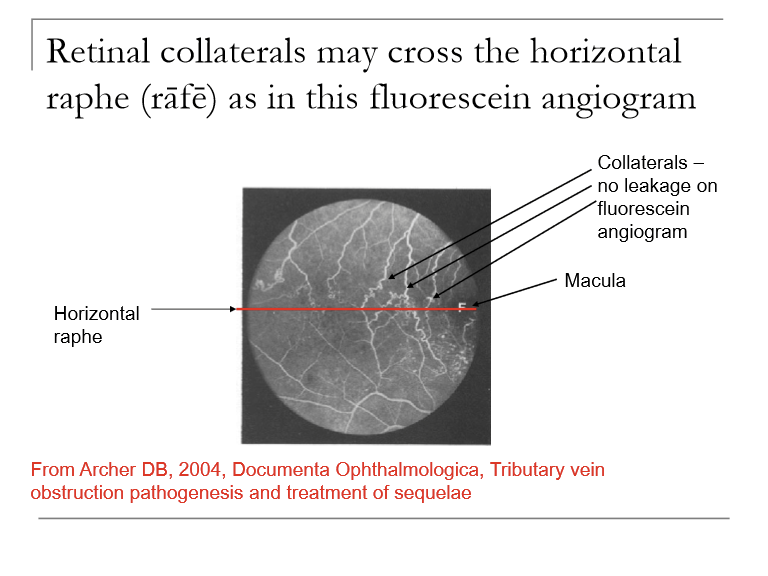
What are some findings after BRVO?
Lipid inflitrates after ~2 months
Collateral channels open to shunt blood around the occluded zone (can cross horizontal raphe)
Venous sheathing
Vascular tortuosity
What initial systemic evaluation is recommended for patients with new or old BRVO?
Perform a physical exam + targeted blood tests to evaluate vascular risk factors.
Common labs: BP measurement, fasting glucose/A1c, lipid profile, CBC, ESR, CRP, and sometimes hypercoagulability testing in young patients.
Goal: identify systemic contributors (e.g., HTN, diabetes, hyperlipidemia).
What determines the ocular management approach in BRVO?
Treatment depends on whether the patient has:
Macular edema, and/or
Retinal neovascularization
These findings guide use of anti‑VEGF therapy, focal/grid laser, and panretinal photocoagulation (PRP) if needed.
What is the prognosis of BRVO?
50-60% have final VA of 20/40 or better even without Tx
Prognosis correlates well with initial VA
Poorer prognosis if chronic macular edema or macular ischemia/capillary nonperfusion
Five DD or more of capillary nonperfusion is a major risk factor for development of retinal neovascularization
What are the Tx for macular edema in BRVO?
Grid laser helps macular edema mildly after branch vein occlusion according Branch Vein occlusion Study (BVOS).
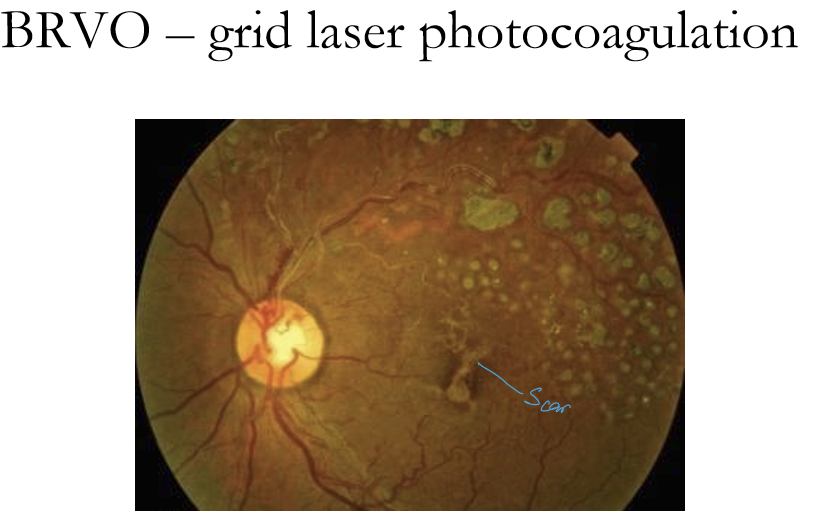
What is the management for macular edema in BRVO?
BVOS: grid laser photocoagulation recommended if:
VA 20/40 or worse
BRVO of 3 months duration shows no foveal hemorrhage or macular ischemia
SCORE study compared laser photocoagulation to intravitreal steroid injections: laser remains the standard of care due to SE of steroids
What are the treatments for macular edema in BRVO?
standard of care/first-line tx are now intravitreal anti-VEGF injections
primary poof of efficacy for this comes from BRAVO study and follow-up studies
Laser photocoagulation may help
How common are retinal vs. iris neovascularization after BRVO?
Retinal neovascularization (NVD/NVE): ~8% of BRVO cases
Iris neovascularization (rubeosis iridis): ~2–3%
Both are driven by retinal ischemia → VEGF release and increase risk of vitreous hemorrhage or neovascular glaucoma.
When must an optometrist urgently refer a patient with BRVO?
Refer within 2–3 days if macular edema or retinal/iris neovascularization is present.
These findings require ophthalmologic management (e.g., anti‑VEGF, laser) and are outside optometric treatment scope.
What is the appropriate optometric follow‑up schedule for BRVO if referral is not immediately performed?
Daily Amsler grid monitoring by the patient
Dilated fundus exam (DFE) + OCT every 1–2 months for the first ~4 months
→ evaluate for new macular edema or neovascularizationThen every ~6 months afterward for stability
What systemic medical steps should optometrists take for patients with BRVO?
Patients must receive a systemic vascular work‑up, or if already managed, the physician must be notified within 3-5 days.
Conditions to evaluate: hypertension, diabetes, hyperlipidemia, cardiovascular risk.
What lifestyle counseling should optometrists provide to BRVO patients (even if referred)?
Discuss:
Smoking cessation
Healthy weight maintenance
Blood glucose control
These reduce risk of recurrent or bilateral retinal vascular events.