SLP Exam 3
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
The nervous system
Consists of
•1. The brain
•2. The spinal cord
•3. All associated nerves and sense organs
Nerves, neuron and synapses
Nerves are a collection of neurons
Neurons are the basic unit of your nervous system and have
1. A cell body
2. a single long axon
3. several branching dendrites
Synapse is the space between the axon of one neuron and the dendrite of the next.
central nervous system
•Made up of the brain and the spinal cord.
•Brain –
•Cerebrum – has a right and left hemisphere
•Cerebellum
•Brainstem
the brain
•4 lobes – frontal, parietal, occipital, temporal
•Sensory and motor functions of the cerebrum are contralateral
•In 98% of people the left hemisphere is dominant for receptive & expressive language.
The Cerebellum – the “little Brain
•Coordinates fine motor movement
•Helps maintain muscle tone
•The Cerebellum’s posterior lobe helps with nonmotor processing, including -
•1. executive functioning
•2. working memory
•3. divided attention
•4. affect or emotion
Main types of Aphasia & Areas affected
•Broca’s – frontal – both hemispheres non-fluent, telegraphic speech
•Wernicke’s – left temporal
•Global – large lesions below the brain’s surface
•What may be impaired?
•What to expect from recovery - when is maximum improvement seen?
types of strokes
•Ischemic- most rapid recovery
•Hemorrhagic
•TIA
Hemiparesis
muscle weakness on one side
hemiplegia
paralysis on one side
hemisensory impairment
can not perceive sensory info
hemianopsia
blindness in the right visual filed of each eye
dysphagia
difficulty chewing or swallowing
agnosia
trouble understanding incoming sensory info, auditory or visual
agrammatism
omit grammatical forms, esp little words
How will you assess? How will you intervene?
•Bedside exam- naming things, using visuals
•General guidelines
Assessment for Aphasia
•Case History & Family Interview – oral mech exam, hearing test
•Counsel with the family, as part of the initial assessment process
•Bedside Exams – done a few days in a row, if possible
•Formal receptive and expressive language testing and language samples, once the client has stabilized
RHBD, TBI and cog. impairments
right hemisphere brain disorder
traumatic brain injury
agraphia
trouble writing
Alexia
trouble reading
anomia
trouble naming terms
jargon
speech without meaning, some real words and some made up words
neologism
a newly made up word
paraphrasic
use of a word substitution of a related word
verbal stereotype
common expression used repeatedly
Intervention for Aphasia
•Underlying skills – memory & auditory comprehension or specific tasks – naming
•Cross modality – comprehension helps production
•Conversational techniques
•Access language by “bridging” hemispheres- gesture, singing
•AAC
•Cognitive tasks
•Family & caregiver training
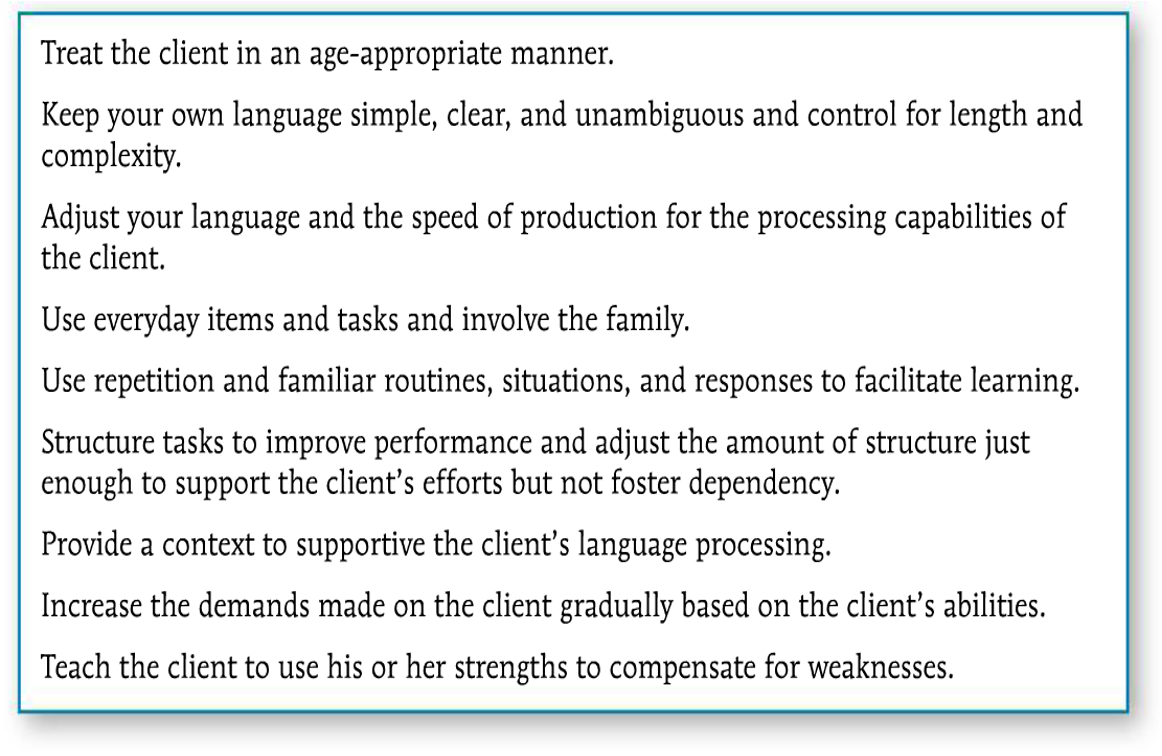
guidelines for intervention
Components of Voice
•Voice production
•Resonance
•Pitch
Loudness
Organic Voice Disorders
•Structural Abnormalities
•Neurological Disorders
vocal nodules (structural abnormalities)
•As a result of forceful adduction (Stemple, Roy, & Klaben, 2014)
•Generally bilateral
•Start off soft, but harden over time
•Usually seen in adult women 20-50 years
•Seen in both male and female in younger children. (Stemple, Roy, & Klaben, 2014)
•Results in hoarseness & breathiness
•Vocal rest, change in vocal behaviors, sometimes surgery
vocal polyps (structural abnormalities)
•Vocal polyps
•As a result of vocal abuse or misuse
•Generally unilateral
•Start off as a ruptured blood vessel, swell and develop a fluid-filled lesion
•Usually larger than nodules and tend to bleed
•Nodules develop over time. Polyps can result from a single traumatic incident, such as Baylor beating TCU 68-51.
•Results in hoarseness, breathiness & diplophonia
•Surgical removal and intervention are usually necessary
laryngitis (structural abnormalities)
•Laryngitis
• Inflammation of the vocal folds as a result from exposure to noxious agents or vocal abuse (Colton, Casper & Leonard, 2011)
•Acute VS Chronic
•Hoarseness - aphonia
•Vocal rest mad changes to voice use (Boone et all, 2010) and lifestyle changes
•Laryngeal papilloma (structural abnormalities)
• Caused by HPV – human papillomavirus
•Usually seen in children under 6 years of age (Boone et al. 2010)
•Exhibit inspiratory stridor, due to narrowing in the airway (Stemple, Roy, & Klaben, 2014)
•Surgically removed – usually more than once
laryngeal cancer (structural abnormalities)
• Linked to cigarette smoking and excessive use of alcohol, as well as HPV, poor nutrition, age, race, family history and GERD – (ACS, 2016)
•Persistent hoarseness
Removal of larynx
Neurologic Voice Disorders
Cause by damage to the Central Nervous System – brain and spinal cord
Or from damage to the Peripheral Nervous System – the 12 cranial nerves
Damage to cranial nerve X (vagus)
•Results in uni or bi lateral vocal fold paralysis, since this nerve controls the laryngeal muscles for phonation.
•Voice may be hoarse, breathy, reduced loudness, pitch breaks, diplophonia, also at risk for aspiration.
•Diseases of the Central Nervous System
Parkinson Disease – degeneration of neurons located in the brain stem. Results in muscle rigidity, reduced range of movement and tremor.
This will affect loudness, pitch, breathiness
Voice therapy can be very effective.
Amyotrophic Lateral Sclerosis (ALS)- degenerations of upper and lower motor neurons, ultimately resulting in paralysis.
Will see reduction in volume. Other voice characteristics will vary, due to both flaccid and spastic weakness.
Voice therapy is not recommended.
Functional Voice Disorders
•Muscle Tension Dysphonia – MTD – will see hyper adduction - voice therapy address this specifically
•Conversion Disorders such as Conversion Aphonia – emotional conflict needs to be resolved, rather than voice therapy provided
•Mutational Falsetto – voice therapy and possibly counseling will help
Resonance Disorders
•Often associated with voice disorders involving CNS and PNS
•Often due to structural abnormalities, such as cleft palate
•Velopharyngeal Dysfunction (VPD)
Goals of a Voice Evaluation
1.Determine the presence or absence of a voice disorder
2.Determine the nature of the voice disorder
3.Determine the severity of the disorders
Remember: a medical doctor – preferably an otolaryngologist (ENT doctor) must conduct an examination if a voice disorder is suspected
Vocal Hygiene
•Stay hydrated
•Avoid caffeine and alcohol, tobacco
•Avoid yelling
•Avoid talking in unnatural voices, such as imitating cartoon characters
•Manage allergies, reflux other health issues
•If it is a resonance problem
•Medical management: such as cleft surgery
•Prosthetic devices, such as a palatal obturator
Communicative Competencies
Linguistic Competency
operational competency
social competency
strategic competency
psycho-social competency
Who uses an AAC
Pediatric:
CAS, Down Syndrome, CP, Autism
Adults:
Neurological disease of incident
CP
Anatomical change - Laryngectomy
Core vs fringe words
Core words
•Powerful
•Flexible
•Not nouns
Fringe Words
•Think nouns – cookies, McDonald's, horse
Our Goal with AAC is to augment all communication
•Ability to “generate a novel utterance”
•There are no prerequisites
•I have a 4 year old client. She has Down Syndrome and is very difficult to understand. She has approximately 10 words that can be understood – no, yeah, elp for help... Almost all of her communication attempts are one word utterances.
•I am suggesting she use an AAC device. Why?
An aac device will help her to be able to communicate better, as many of her words can not be understood.
Long term vs Short term use – what do you think?
•I have a client with CAS
•I have a client with CP and severe motor speech disorder
both could use the AAC, for the CAS it would most likely be short term but for CP it will be long term
Motor speech
What will be affected?
Neurological disorders or injuries that affect
•Motor planning
•Programming
•Coordination
•Timing
Execution of movement patterns used for speech production
any part of speech production with adults or children
-respiration
-phonation
-resonation
-articulation
Understand roles of the brain
•Primary Motor Cortex – Found in the frontal lobe. This is where the descending pathway begins. This area is where voluntary motor movements begin. - What happens if there is damage there?
•Pyramidal tract - the direct activation pathway – responsible for volitional movement of limbs and articulators – originates in the motor cortex then to the neurons that activate the muscles.
•Extrapyramidal tract – the indirect activation pathway – regulates reflexes and maintain posture and muscle tone to facilitate movement carried out by the direct activations system.
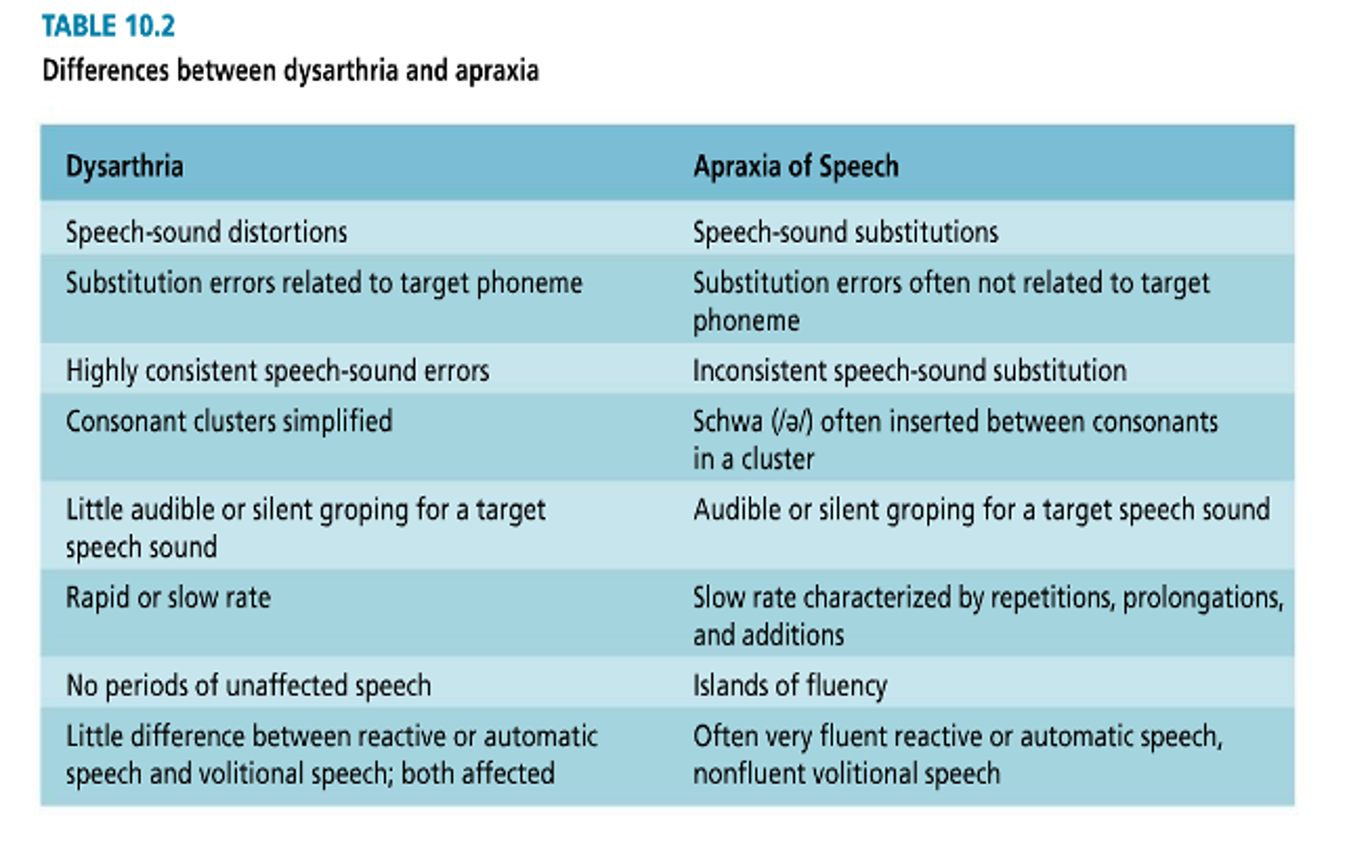
Dysarthria vs apraxia
Types of dysarthria
•Flaccid
•Spastic
•Ataxic
•Hypokinetic
•Hyperkinetic
•Mixed
Types of
CP
Spastic CP – 60% of individuals with CP
• Spasticity - resistance to passive stretch
• Increased muscle tone
Athetoid CP – 30% of individuals with CP
• slow involuntary writhing
• disorganized and uncoordinated movement
Ataxic CP – 10 % of individuals with CP
•clumsy and awkward movement
•problems with balance
Remember RAC and give examples
-restore
-adjust
-compensate