vert physio - the ECG
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
gap junctions
connections between myocardial cells
contractile myocardial cells
contain abundant actin and myosin; create force of contractions
autorhythmic myocardial cells
non-contractile (“pacemaker”); contain little actin and myosin; unstable resting membrane potentials that cause them to spontaneously generate APs
intrinsic conduction system
connected to autorhythmic cells; population of highly modified myocardial cells that distribute AP to myocardium in coordinated manner, resulting in 3D contraction
cardiac cycle step 1
atrial contraction/ atrial systole; fills ventricles
cardiac cycle step 2
ventricular systole: isovolumetric contraction; pressure begins to mount in ventricles, but not high enough to open semilunar valves
cardiac cycle step 3
ventricular systole part 2: ventricular ejection
cardiac cycle step 4
ventricular diastole: second isovolumetric period: relaxation; pressure drops, blood volume constant
cardiac cycle step 5
ventricular filling; pressure on atrioventricular valves high enough for passive fill
cardiac cycle step 6/1
atrial systole and active filling
sinoatrial node
½ of start of cardiac cycle with concentrated autorhythmic cells in right atrium; depolarizes faster than AV node; drives heart rate; AP causes atria to contract and push blood to ventricles
atrioventricular node
AP carried here from SA node; serves as a regulator (delay in conduction between AV node and AV bundle)
AV bundle
electrical connection between atria and ventricles
AP travel in heart
SA node → AV node → AV bundle → ventricular muscle → L and R bundle branches → Purkinje fibers
ECG Lead I
records activity from upper left and right chest on horizontal axis
ECG Lead II
records activity between upper L chest to lower chest
ECG Lead III
records activity between upper R chest and lower chest
aVR, aVL, and aVF leads
trigonometrically calculated from voltages on leads I-III
Einothoven’s triangle
arrangements of leads
P wave
atrial systole - contraction of atrial muscle following depolarization; last 100ms
flat line following P wave
PR interval; time when L and R atria both completely depolarized (isoelectric, systole); R and L atrial contraction
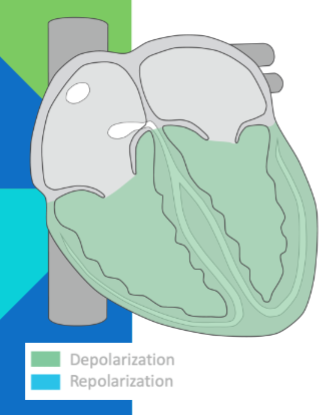
QRS complex
ventricular systole; contraction of ventricles following rapid depolarization; finish before T wave begins; lasts 270 ms
T wave
repolarization of ventricles
normal sinus rhythm (NSR)
normal state with SA node as lead pacer; 60-100 BPM
sinus bradycardia
same as NSR but rate <60 BPM; vagal stimulation leading to nodal slowing, or medicine; conditioned athletes
sinus tachycardia
same as NSR, but rate >100 BPM; medications, exercise, etc
asystole
when heart’s electrical system ceases functioning; heart stops
atrial fibrillation
chaotic firing of numerous intrinsic conduction cells in atria in haphazard fashion; no discernible P waves, QRS complexes irregular
atrial flutter
from short circuit in heart, electrical current circulates through R atrium quickly
first degree AV block
from prolonged block in signal conduction to AV node; medication, vagal stimulation, disease, etc.; PR interval > 0.2 seconds
junctional rhythm
SA node is non-functional and cannot initiate normal pace making; HR becomes firing rate of AV node; no interval between P wave and QRS; 40-60 BPM
ventricle tachycardia
very fast ventricular rate with wide QRS complex; similar to atrial flutter, but fast ventricle firing; 100-200 BPM
ventricular fibrillation
“cardiac chaos”; ventricular pacers firing at own pace with no organized contraction
premature atrial contraction
when some pacemaker cell in atria fires before SA node; complex that comes sooner than expected
premature ventricular contraction
premature firing of ventricular cell, before normal SA node
isovolumetric relaxation
ventricular diastole: relaxation of ventricles; 50mL blood into each ventricle; semilunar and AV valves closed
ventricular filling
75% of ventricular filling occurs as blood flows through atria and AV valves; all chambers relaxed
myocardial contractile cells
majority of cells in atria and ventricles; responsible for contraction
myocardial conducting cells
autorhythmic cells that form conduction system; similar to neurons
intercalated discs
at junctions between cells
gap junctions
channel between muscle fibers for passage of cations and spread of APs
desmosome
anchors muscle fibers together
sinoatrial node
myocardial conducting cells; superior and posterior right atrium; highest inherent rate of depolarization; initiates sinus rhythm
internodal pathways
conduct signal from SA node to AV and atrial mocardia
Bachmann’s bundle/ interatrial band
conducts from R to L atrium
atrioventricular node
myocardial conductive cells on inferior right atrium; impulse must pass through AV node before ventricles; slow transmission - small diameter
atrioventricular bundle
travels from AV node to interventricular septum
atrioventricular bundle branches
travel to L and R
Purkinje fibers
extend from the apex and spread impulse to myocardial contractile cells
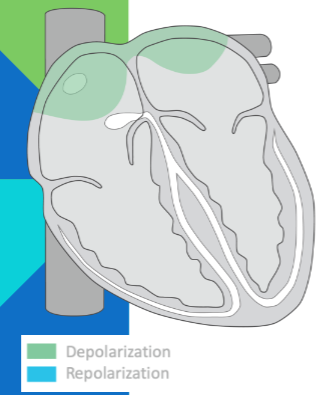
P wave: atrial depolarization

isoelectric: atrial depolarization complete; atria contract; impulse delayed at AV node

QRS complex: impulse to heart apex; ventricular depolarization; atrial repolarization (obscured by QRS)
isoelectric; ventricular depolarization complete; ventricles contract
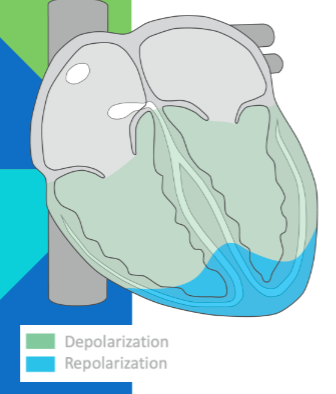
T wave; ventricular repolarization
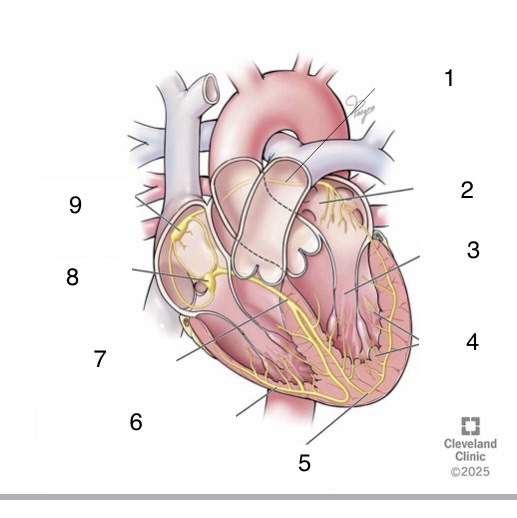
1
Bachmann’s bundle
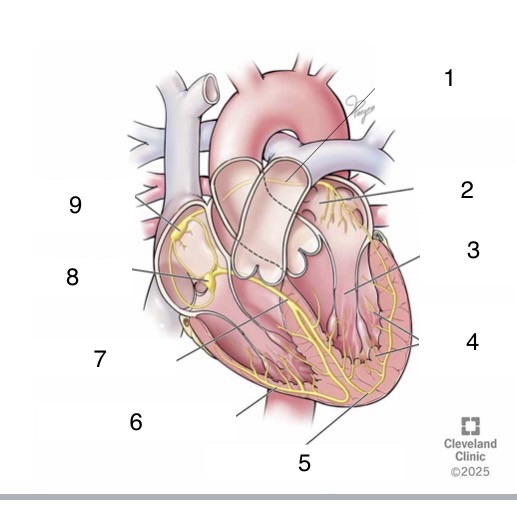
4
Purkinje fibers
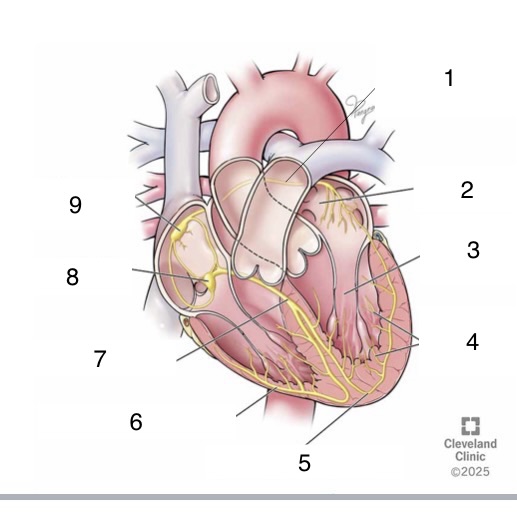
5
left bundle branch
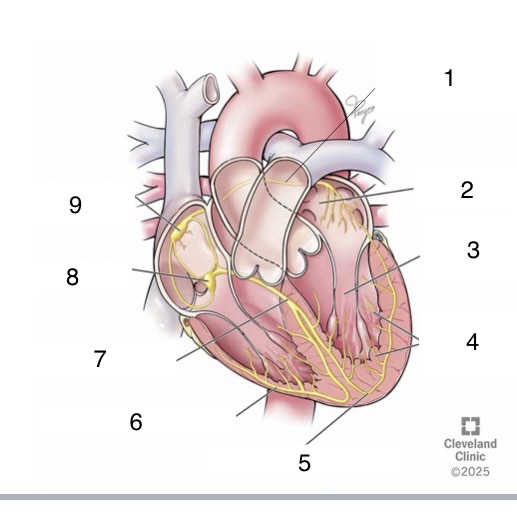
6
right bundle branch
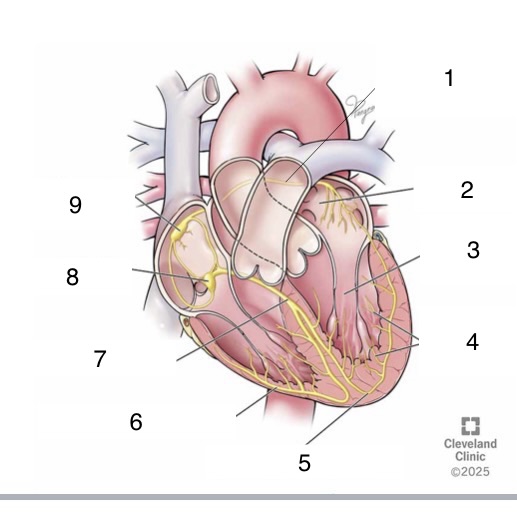
7
bundle of His
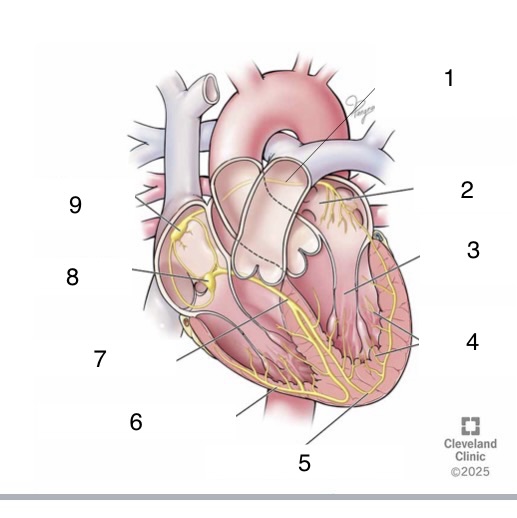
8
AV node
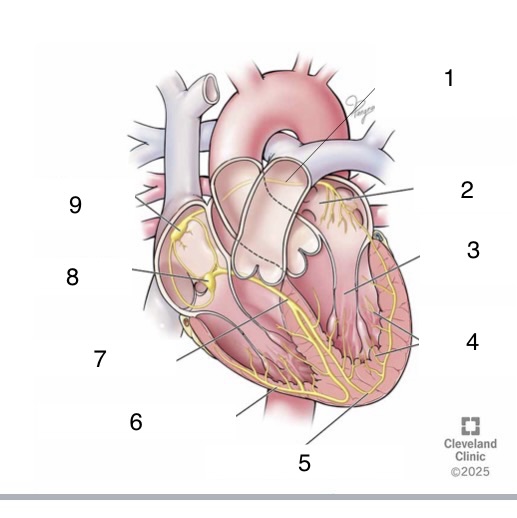
9
SA node