8- bone surgery
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
What is bone surgery? Alveolar bone loss caused by periodontitis means? (3)
Procedure to change alveolar bone and fix deformities caused by the periodontal disease or by related factors, such as exostosis and extrusion
Irregular alveolar profile
Infrabony pockets that are difficult to instrument
No periodontal disease control
Why should you do bone recontouring?(3)
Sanitisable gum and alveolar contour
Solve angular defects and craters
Remove furcation defects
Indications for bone surgery?(3)
Changes in bone morphology and contour of gum
Persistent periodontal pockets
7 Considerations when doing bone surgery?
Bone support of each tooth
Destruction of the alveolar process
Prominences and exostoses
Anatomical spaces or compartments
Muscles and attachment level
Arteries (maxillary, lingual, sublingual, facial, etc.)
Nerves (cranial nerve V: maxillary, mandibula
2 types of bone surgery?
Additive osseous surgery - bone regeneration
Resective (subtractive) osseous surgery - bone recontouring/regularisation
What’s an osteoplasty?
Periodontal pocket eliminated
Remodelling of physiologic bone contour and overlying gingiva
Remodelled bone not part of supporting apparatus - no loss of tooth support
What’s a ostectomy?
Excision of part of supporting periodontal bone to eliminate perio pocket and establish gingival contour
Requires some loss of bone support- amount removed important
5 Indications of osteoplasty?
Deep interproximal pockets in posteriors with blunt bone crest, wavy and irregular contour
Pockets on Vb, L/Pt surfaces where bone resorption results from large walls (bi- and trifurcations)
Tipped 2nd molar due to missing 1st molar (deep V-shaped cut)
Pocket removal to prevent recurrent abscesses, even if a raised recession remains
Remove Vb and L concavities for better access for hygiene
3 Indications of ostectomy?
Interproximal bone craters —> the VB + L spines remain, and the interproximal portion disappears
Extremely deep interproximal pockets
Superficial infrabony pockets and those where reattachment attempts have failed
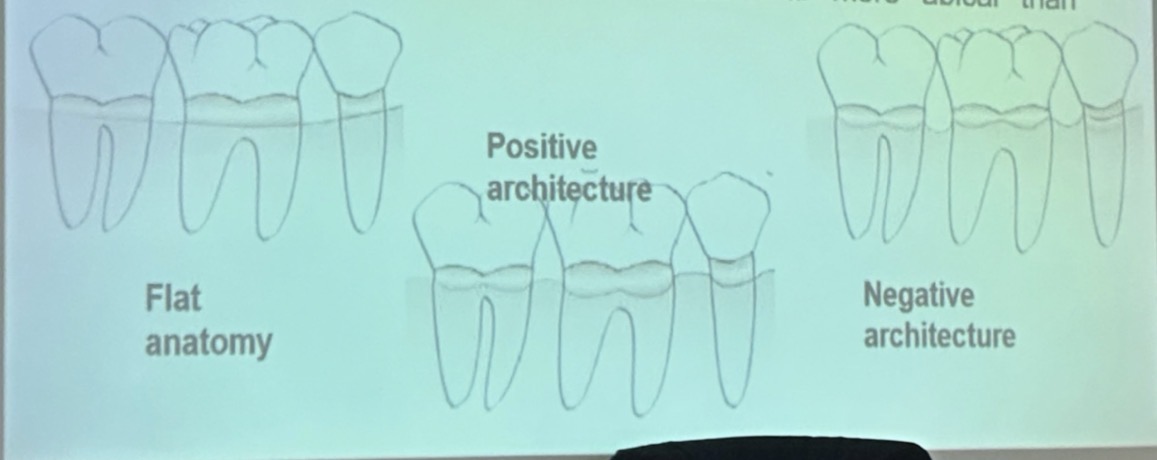
Anatomy of alveolar bone crest - what 4 types?
Ideal = interdental bone more coronal interproximally than on B/L + gradual curved slopes between interdental peaks
Flat = interdental and radicular bone at the same height
Positive = interdental bone higher than radicular bone
Negative = interdental bone more apical (lower) than radicular bone
4 Indications for resective bone surgery?
Infrabony pockets where bone removal achieved without sacrificing supporting bone
Deep proximal infrabony pockets requiring bone removal for pocket elimination
Suprabony pockets with irregular bone crest heights- recurrence
Bi- or trifurcations for thorough cleaning
3 Advantages of resective bone surgery
Prevents recurrence of infection and inflammation
Remodels alveolar crest
Restores fibres structure and function
4 Disadvantages/limitations of resective bone surgery?
Buccal recession
Reverse architecture
Sacrifice of Buccal bone
Inadequate interdental space between molars
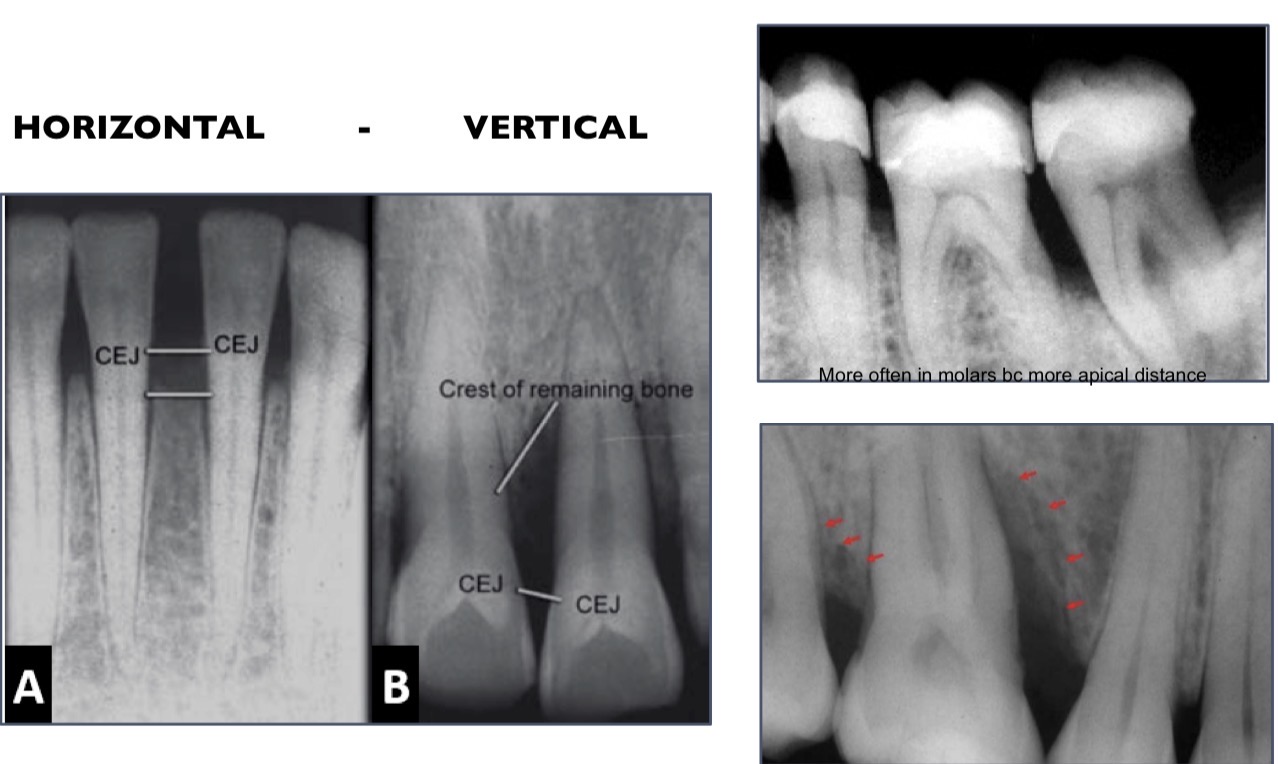
What is an angular defect? Depends on?
bone profile lies obliquely to root profile leaving undermined groove along root, esp interdentally
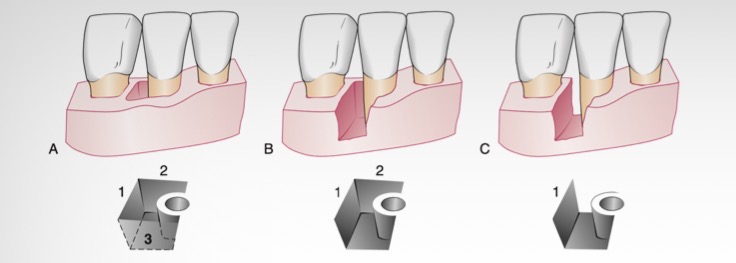
Depend on number of bony walls
3 wall, 2 or 1
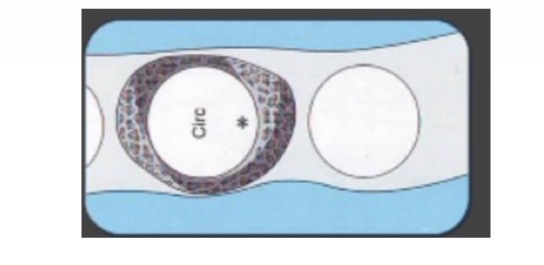
Circumferential defect
Circular wall of destruction
Bone/osseous craters
Concavities in interdental crest confined between B and L walls
2 circular defects connect
Hemiseptal defect
A crater that loses one of its external walls
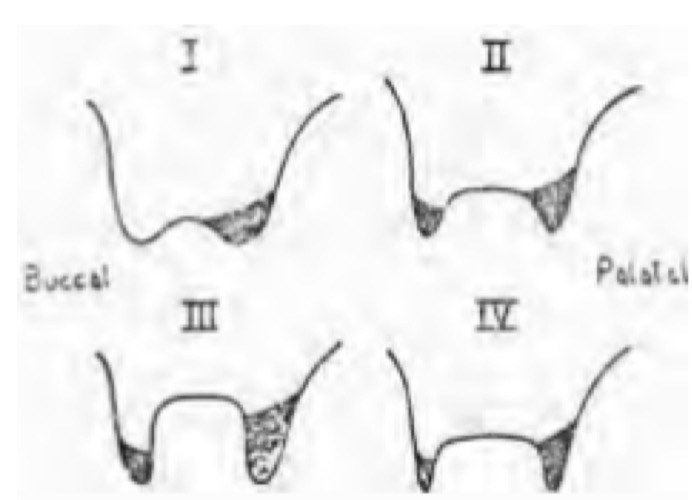
Types of craters
CLASS 1 (2-3 mm): Normal- minimal reduction in PT
CLASS 2 (4-5 mm): Concave- minimal red in PT (2-3mm) and VB
CLASS 3 (6-7 mm): Advanced lesion- minimal red in VB, up to level of PT furcation (sacrifices support)
CLASS 4: Concave with very thin VB and PT walls- red similar to class 3 but with less volume
Root trunk (CEJ-Furcation)
Superficial craters (1-2 mm)—> SHORT trunk: 3 mm max/ 2 mm mand
Medium craters (3-4 mm) —> MEDIUM: 4 mm max/ 3 mm mand
Deep craters (+5 mm) —> LONG: +5 mm max/ + 4mm mand
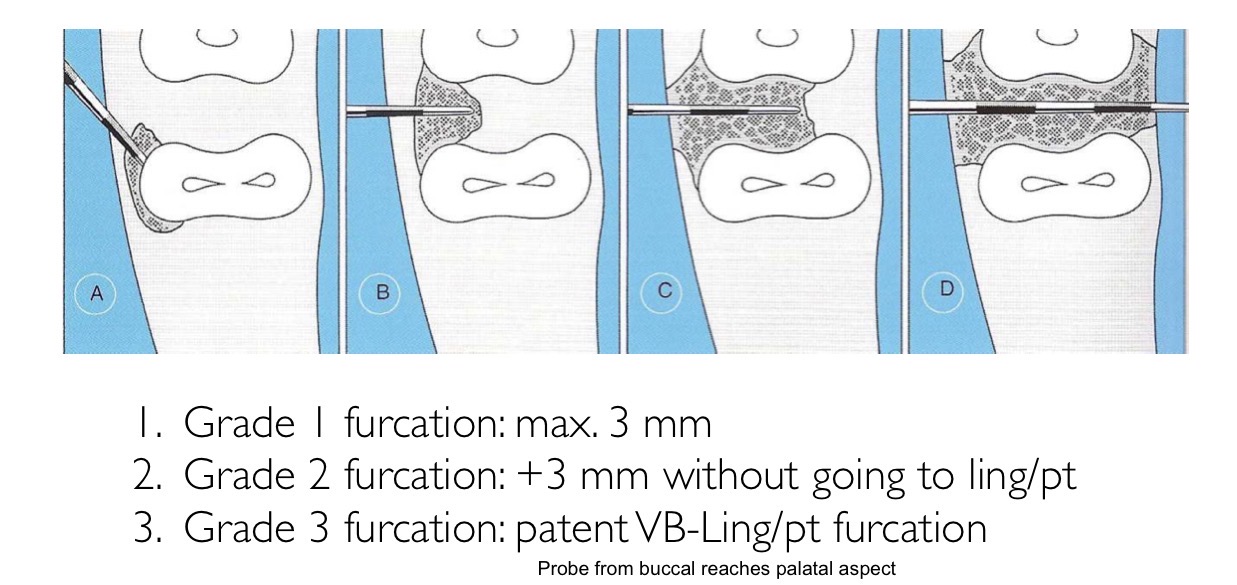
Furcation grades
Grade 1- up to 3mm
2- over 3mm without passing through PT
3- through and through
Furcation Prognostic and contributing factors (4) + 6
Anatomical characteristics
Furcation width
Root trunk length
Root concavities
Cervical enamel projections
Enamel pearls
Dentin and/or cementum bridges
Difficult access for instrumentation
Persistent microflora
Unpredictable results
Treatment grade 1 furcation
SRP
Pocket elimination
Odontoplasty
Treatment furcation grade 2 (5)
Odontoplasty
Tunnelling
Root resection/amputaion
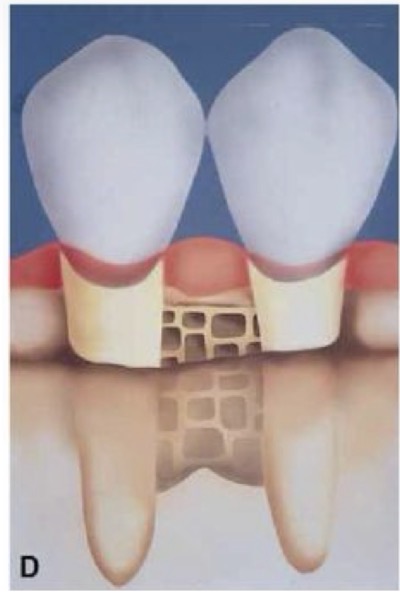
Guided tissue regeneration
Extraction
Treatment furcation grade 3
Tunnelling
Root resection/amputation
Extraction
What factors 8 influence treatment of furcation?
Degree of furcation involvement
Crown-root ratio
Root separation
Strategic value of the tooth
Residual mobility
Oral hygiene options
Long-term prognosis
Implant evaluacion