Paramedic Spring Final
1/80
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
81 Terms
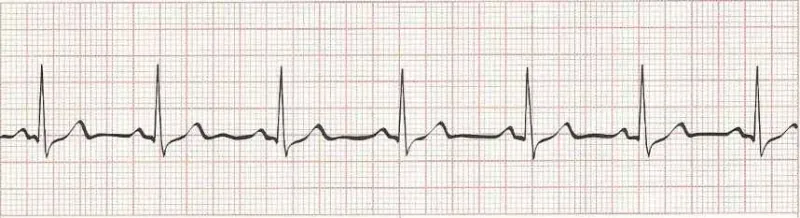
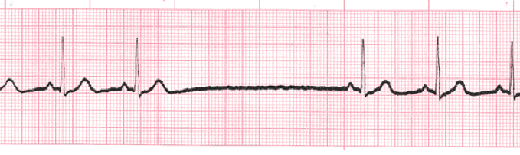
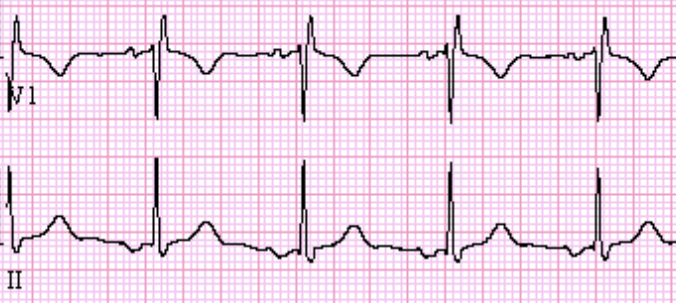
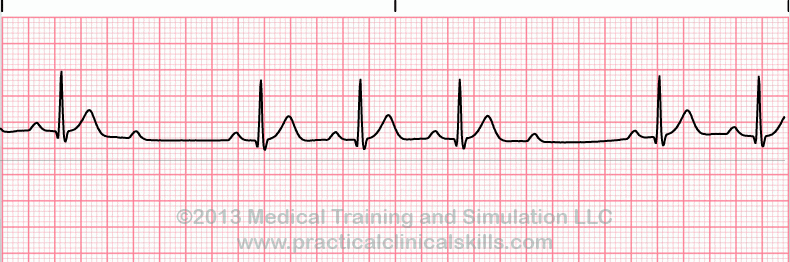
Normal Sinus Rhythm
Rate: 60-100
Rhythm: regular
Sinus Arrhythmia
Rate: 60-100
Regularity: depends on respiration
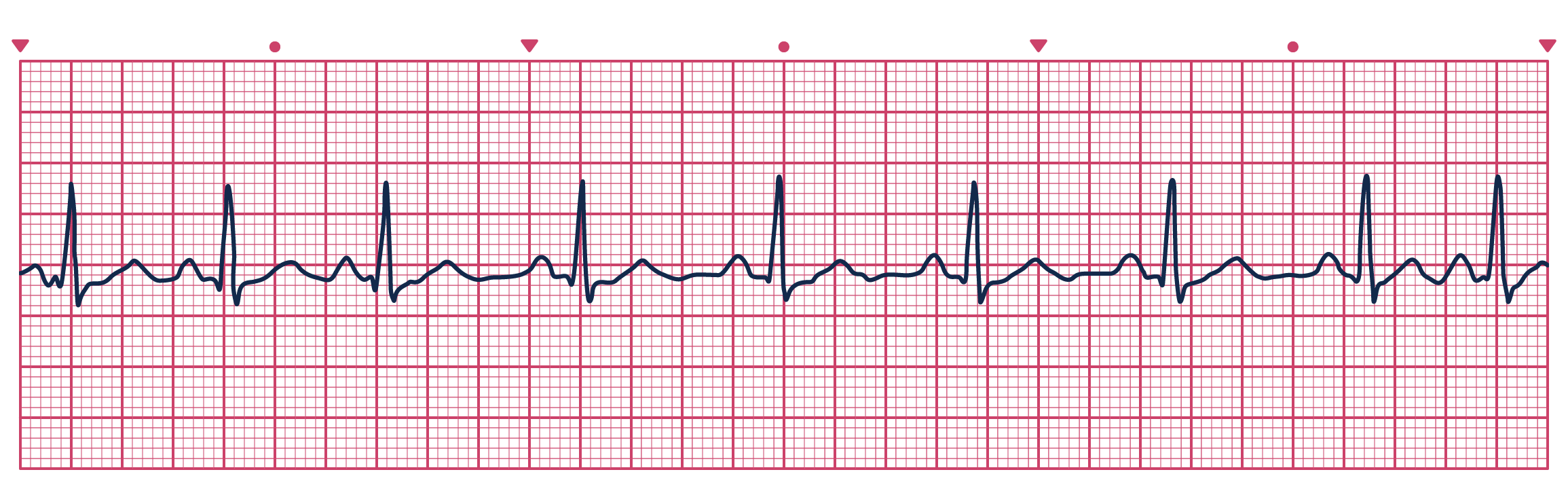
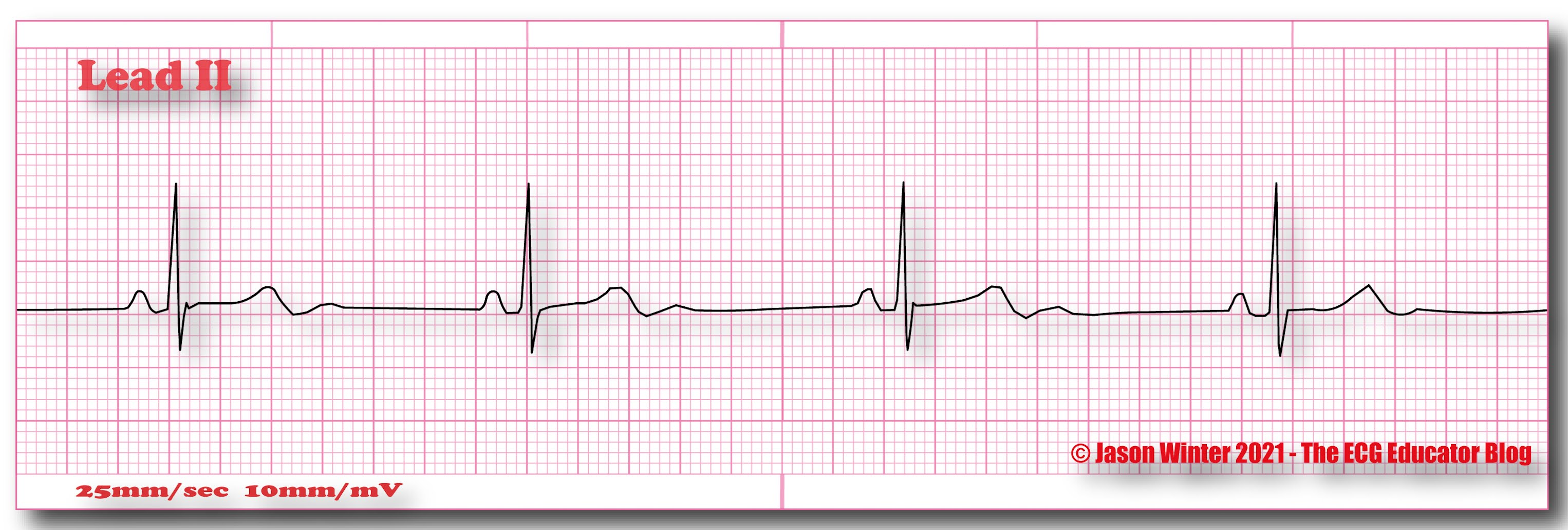
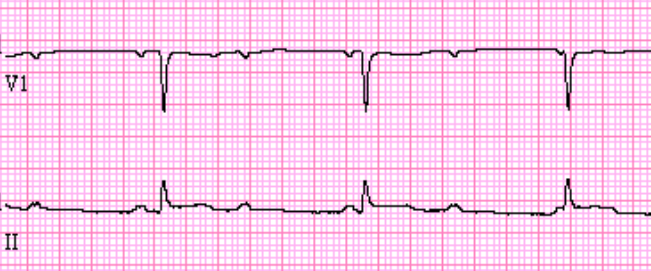
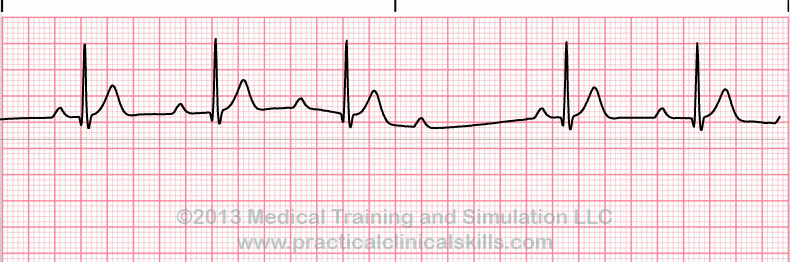
Sinus Bradycardia
Rate: <60
Regularity: regular
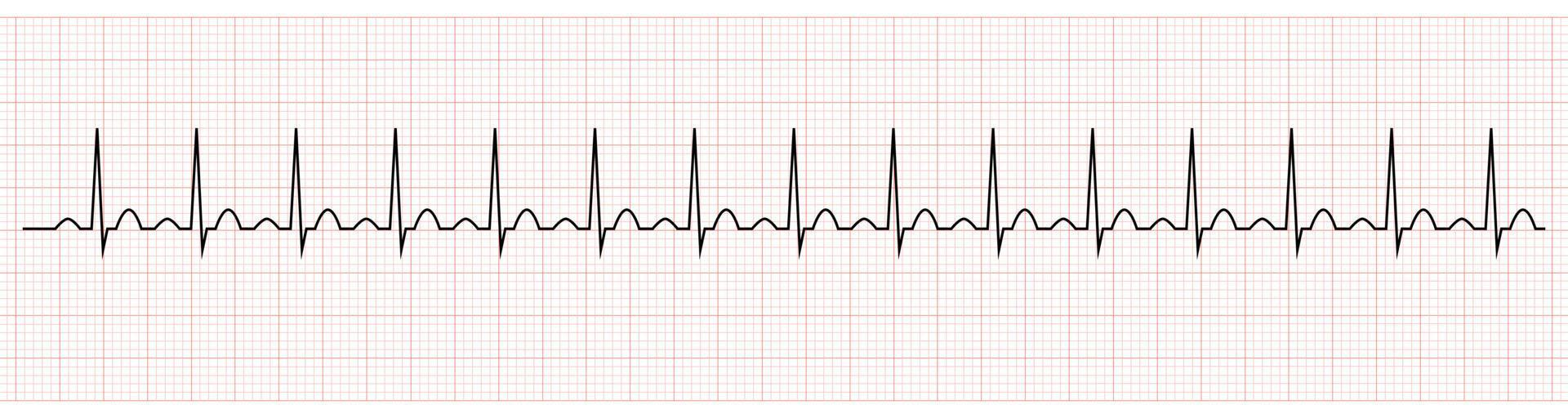
Sinus Tachycardia
Rate: >100
Regularity: regular
Sinus Pause/ Arrest
Rate: varies
Regularity: irregular
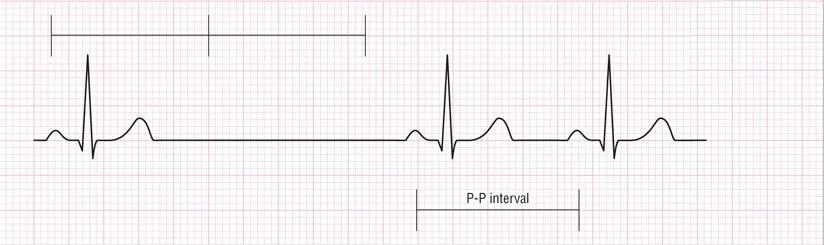
Sinoatrial (SA) Block
Rate: varies
Regularity: irregular
PAC
Rate: depends on underlying rate
Regularity: irregular

Ectopic Atrial Rhythm (EAR)
Rate: <100
Regularity: irregular
P wave morphology is different
Focal Atral Tachycardia (FAT)
Rate: >100
Regularity: irregular
P wave morphology is different

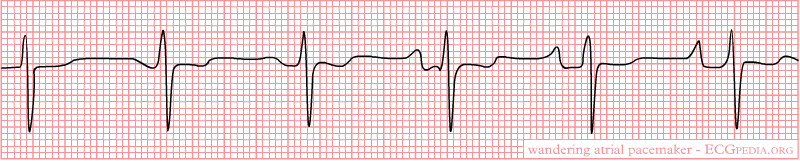
Wandering Atrial Pacemaker (WAP)
Rate: <100
Regularity: irregularly irregular
At least 3 different P wave morphologies
Multifocal Atrial Tachycardia (MAT)
Rate: >100
Regularity: irregularly irregular
At least 3 different P wave morphologies
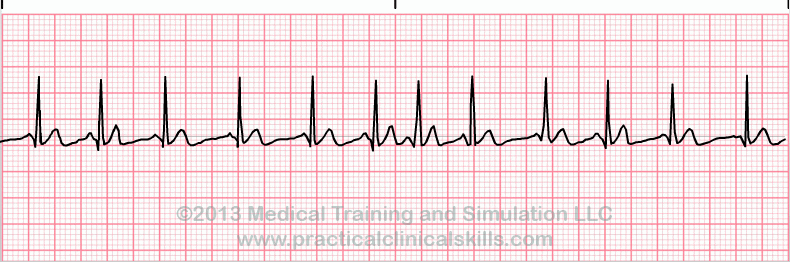
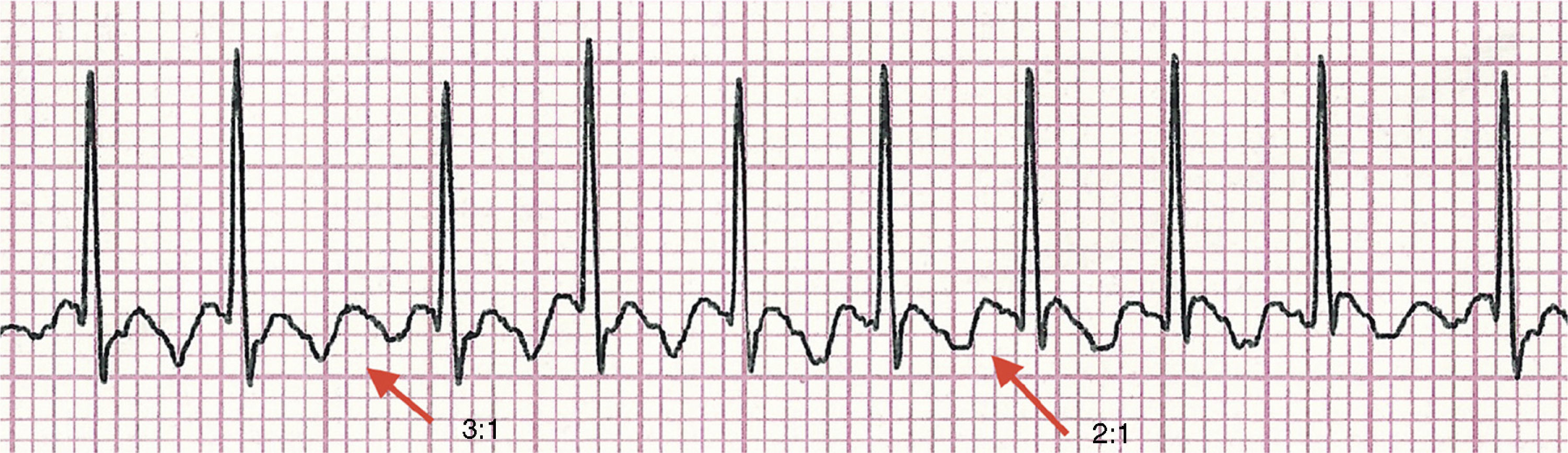
Atrial Flutter (A-Flutter)
Rate: atrial rate ~250-350, ventricular rate ~125-175
Regularity: usually regular, but may be variable
Saw toothed appearance
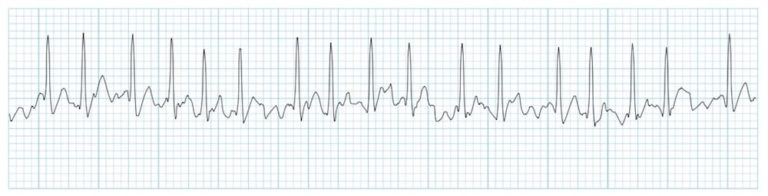
Atrial Fibrillation (A-Fib)
Rate: variable, ventricular response can be fast or slow
Regularity: irregularly irregular
No P waves
PJC
Rate: depends on underlying rhythm
Regularity: irregular
P waves are either absent, in QRS, after QRS, or inverted before QRS

Junctional Escape Beat (JEC)
Rate: depends on underlying rhythm
Regularity: irregular
P waves are either absent, in QRS, after QRS, or inverted before QRS
Junctional Rhythm
Rate: 40-60 bpm
Regularity: regular
P waves are either absent, in QRS, after QRS, or inverted before QRS

Accelerated Junctional Rhythm
Rate: 60-100
Regularity: regular
P waves are either absent, in QRS, after QRS, or inverted before QRS

Junctional Tachycardia
Rate: >100-200
Regularity: regular
P waves are either absent, in QRS, after QRS, or inverted before QRS

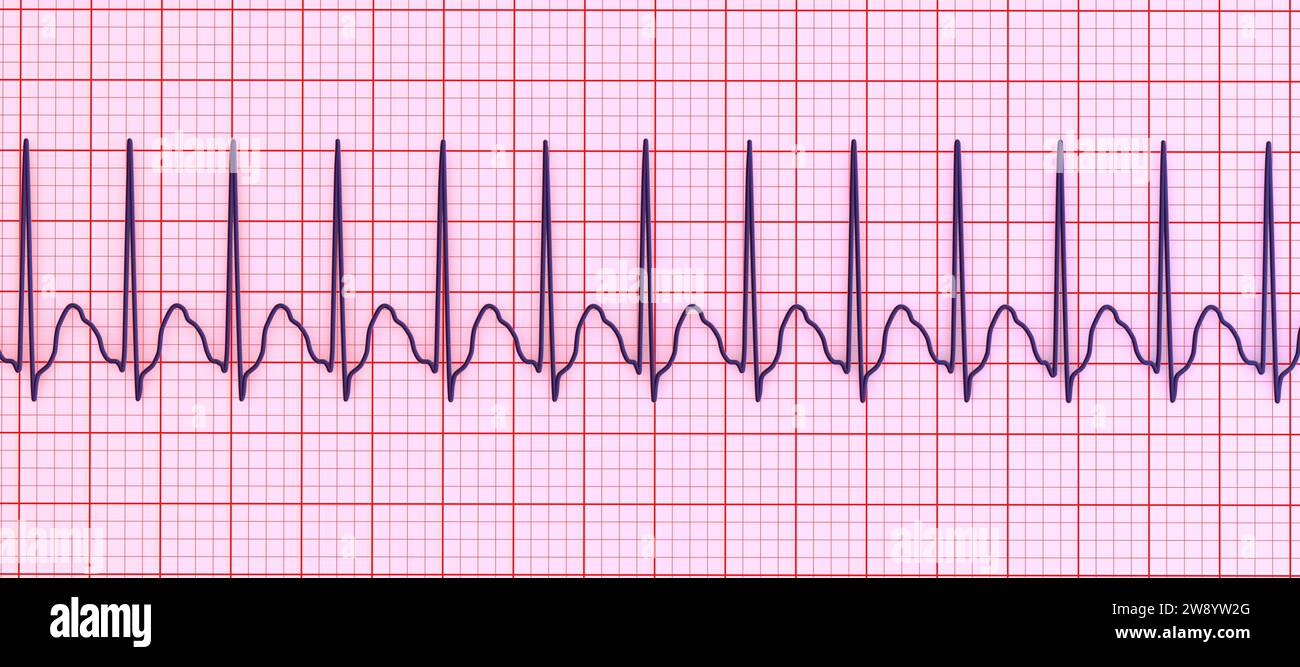
Supraventricular Tachycardia (SVT)
Rate: 180-250
Regularity: regular
Can’t determine P waves
First Degree Heart Block
Rate: depends on underlying rhythm
Regularity: regular
PRI is >0.20 seconds

Second Degree Type 1/ Mobitz 1/ Wenckebach
Rate: depends on underlying rhythm
Regularity: irregularly irregular
Longer, longer, longer, drop
Second Degree Type 2/ Mobitz 2
Rate: depends on underlying rhythm
Regularity: irregularly irregular
If some P’s don’t get through
2:1 AV Block
Rate: depends on the underlying rhythm
Regularity: regular

Third Degree Heart Block
Rate: separate rate for underlying and escape rhythm
Regularity: regular, but P and QRS rates are different
If P’s and Q’s don’t agree

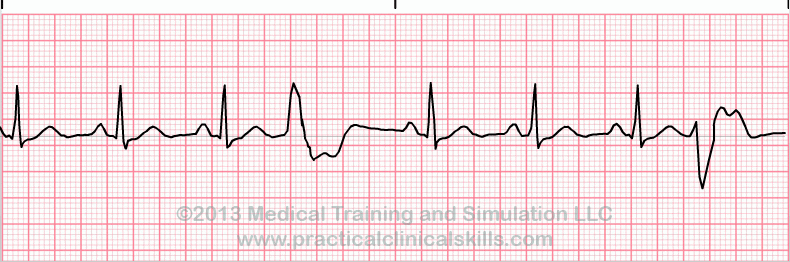
PVC
Rate: depends on underlying rhythm
Regularity: irregular
Ventricular Escape Beat
Rate: depends on underlying rhythm
Regularity: irregular
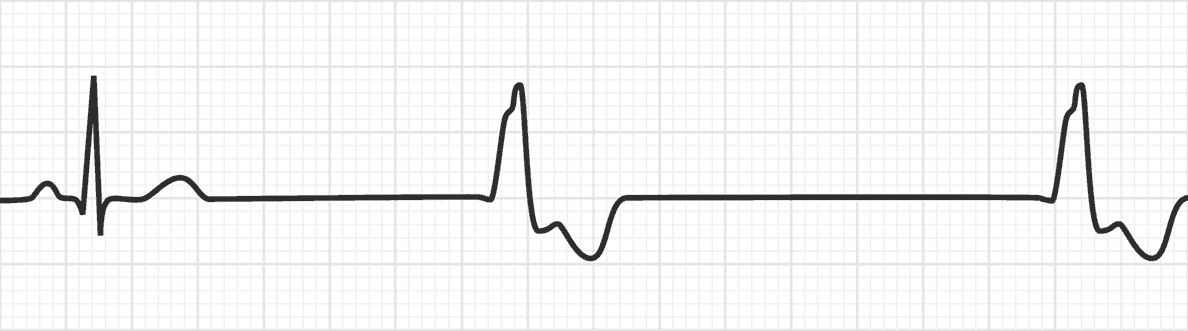
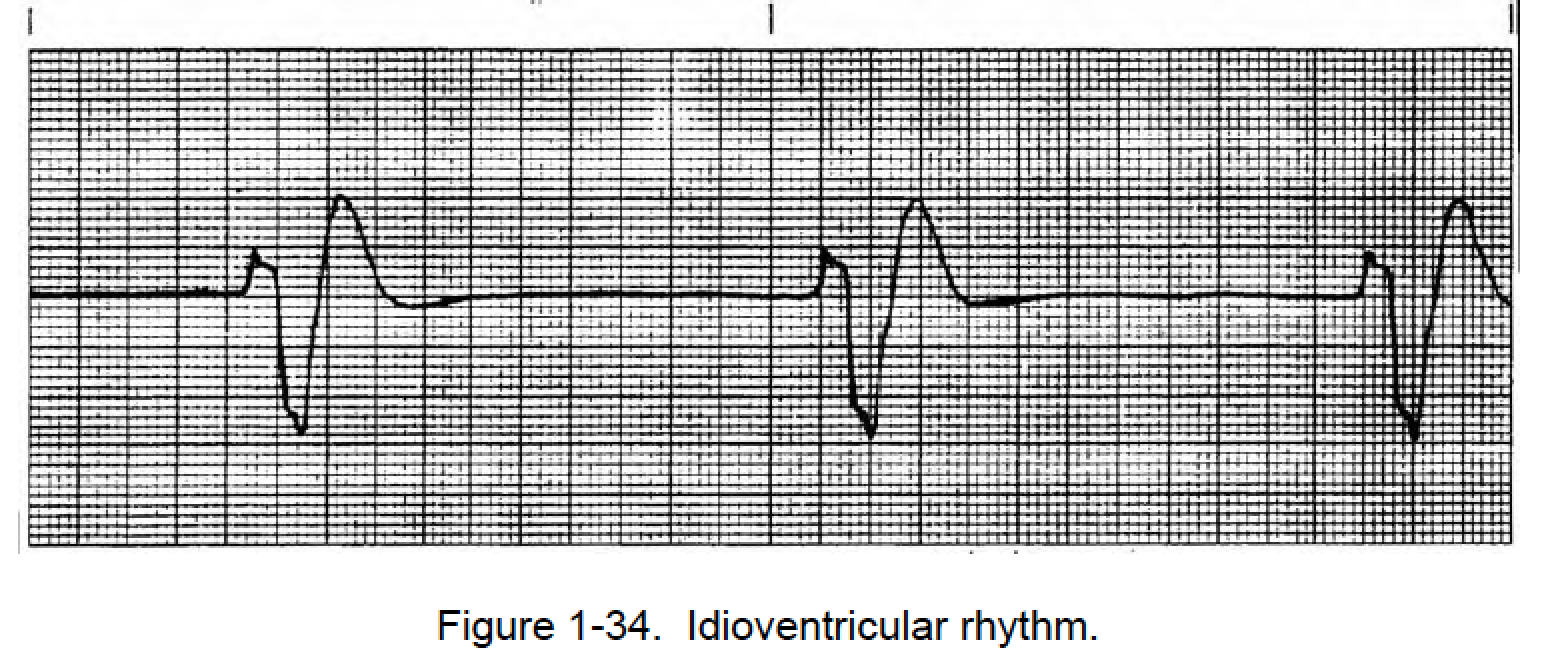
Idioventricular Rhythm (IVR)
Rate: 20-40
Regularity: regular
QRS > 0.12
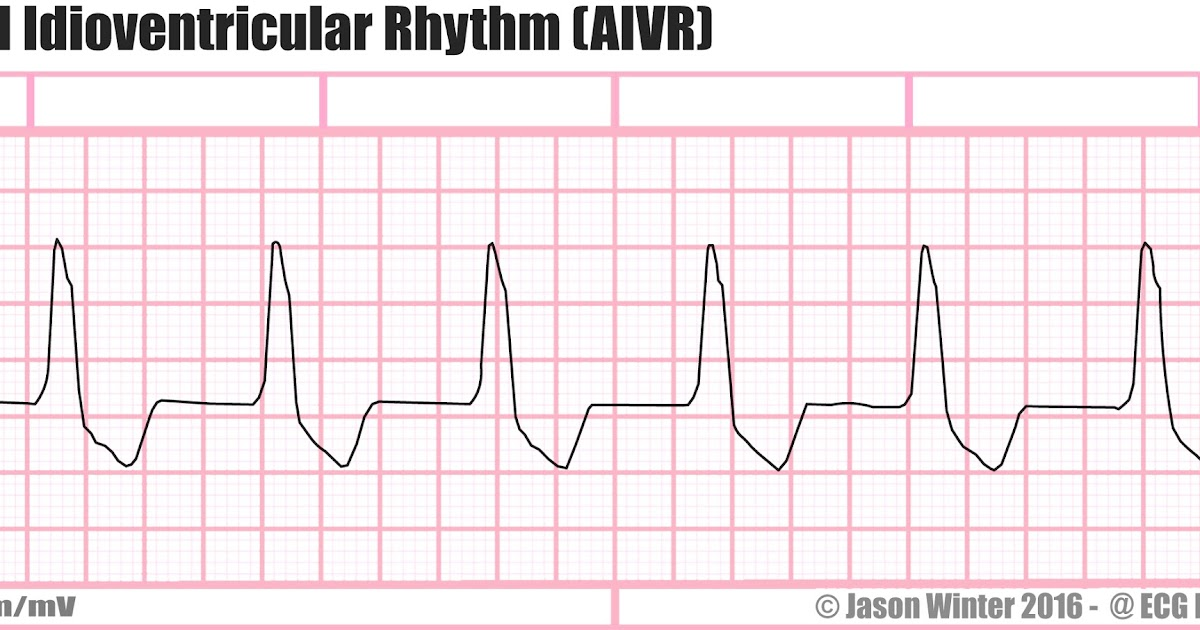
Accelerated Idioventricular Rhythm (AIVR)
Rate: 60-100
Regularity: regular
QRS > 0.12
Ventricular Tachycardia (V-Tach)
Rate: 110-250
Regular: regular
QRS > 0.12

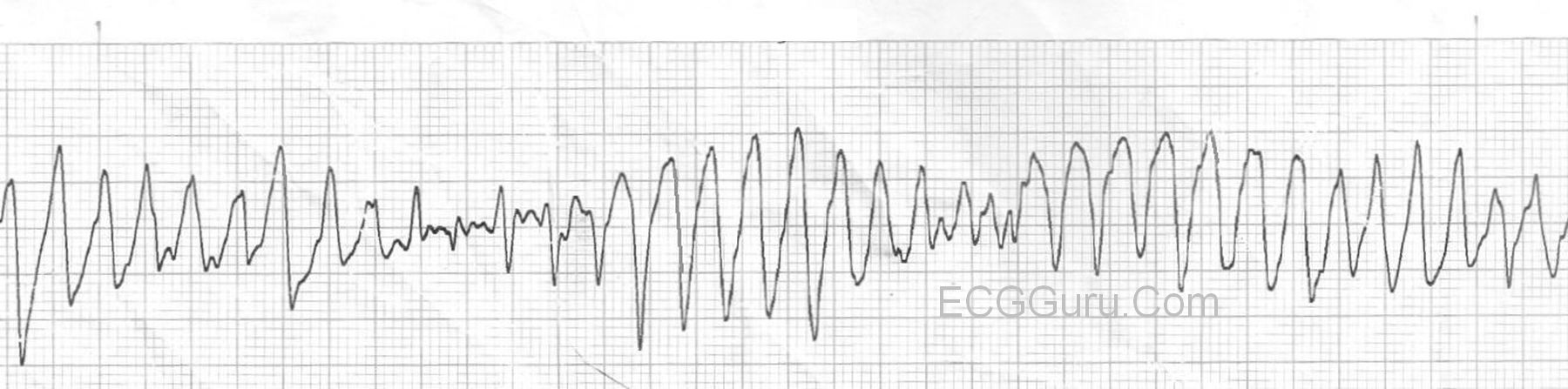
Torsade De Pointes
Rate: 200-250
Regularity: irregular
QRS width is variable
Ventricular Fibrillation (V-Fib)
Rate: indeterminate
Regularity: chaotic rhythm

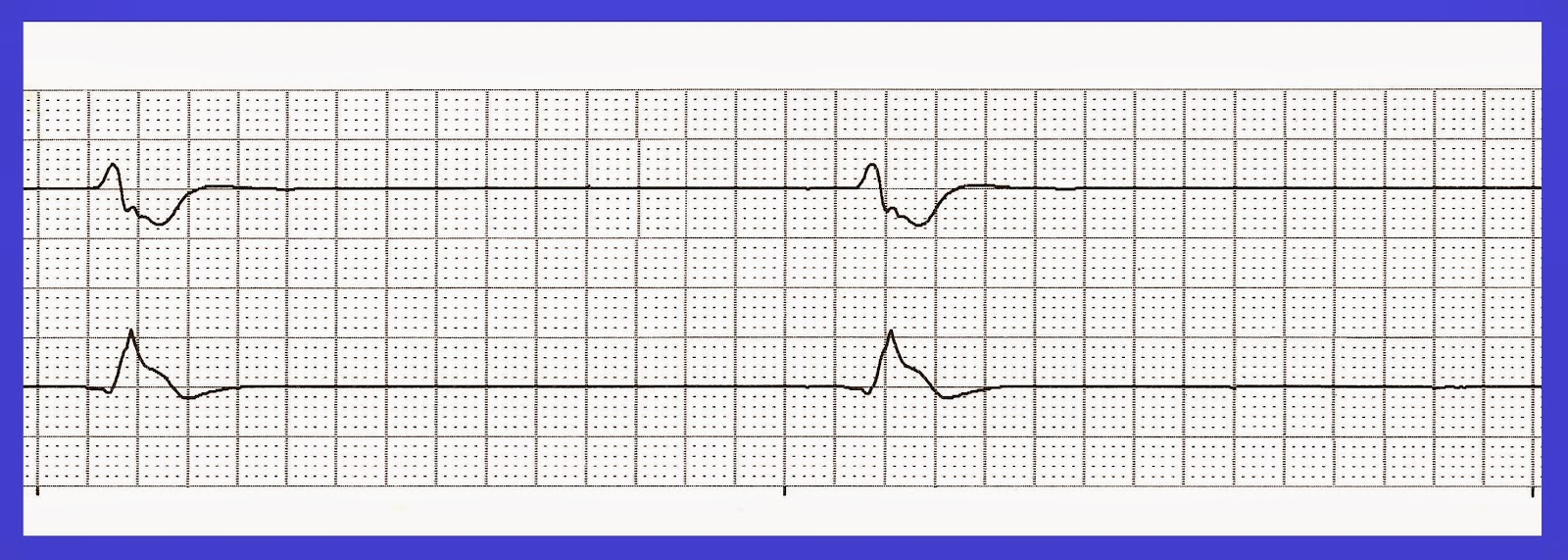
AV Paced Rhythm
Rate and regularity are dependent
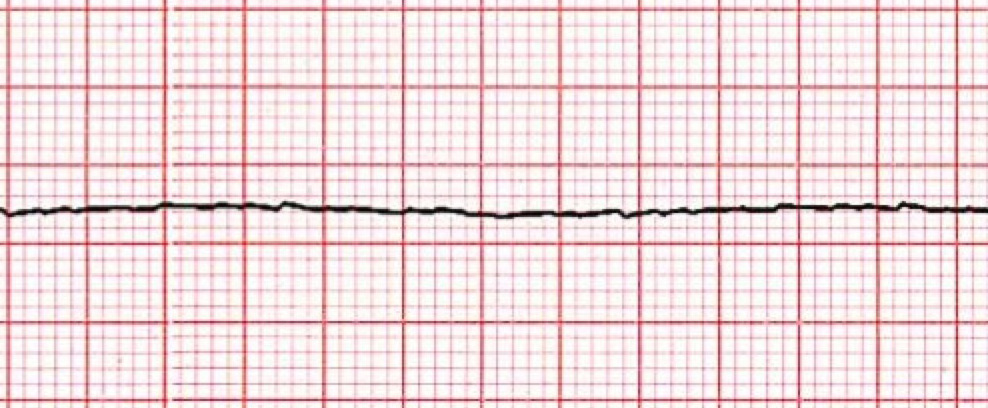
Asystole
not consistent with life
Agonal
Rate: <20
Regularity: irregular
QRS < 0.12
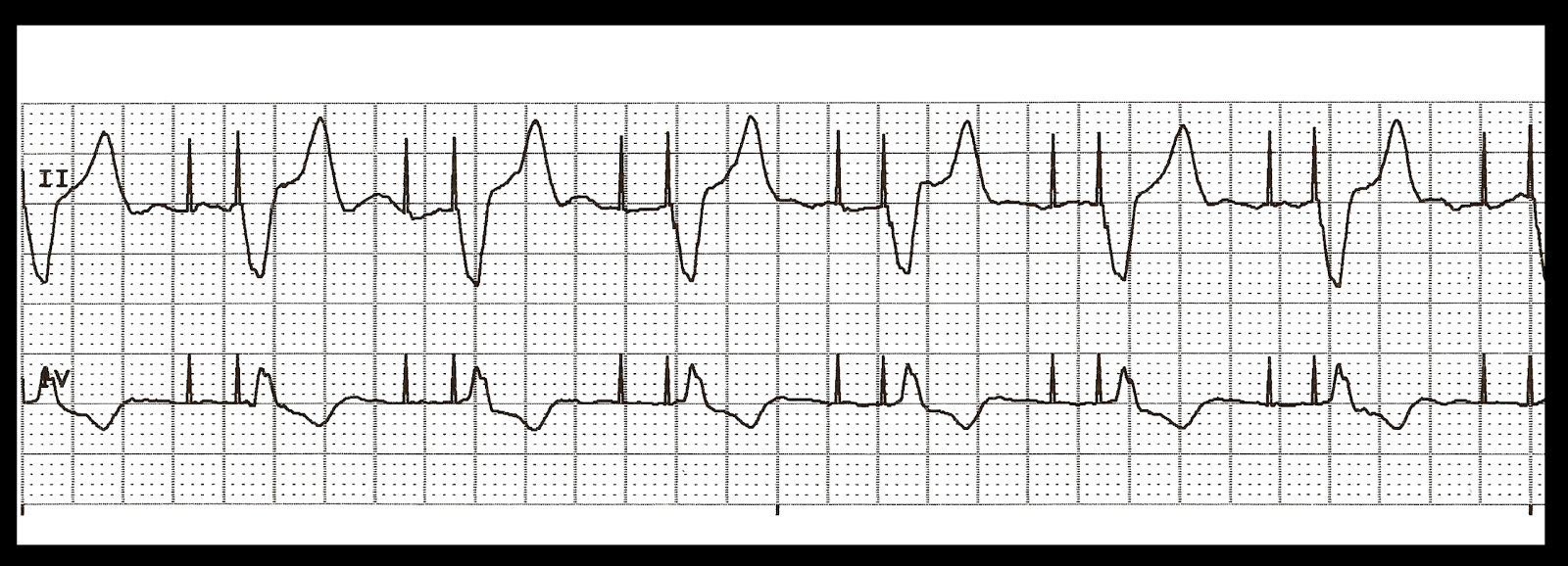
Cardiac Tamponade
Becks Triad: hypotension, JVD, muffled/faint heart sounds
will also see pulsus paradoxus with a manual cuff
ex; hit chest on steering wheel
Non-Compliant HTN uncontrolled
Rapid transport to the hospital
Symptoms of cardiogenic shock
Decreased level of consciousness, tachycardia, hypoxia, cyanosis, pulmonary edema, Hx of MI
Unstable Angina
angina that meets any of the 3:
lasts longer than 20 minutes at rest
new onset
crescendo (more frequent or longer duration)
not readily responding to treatment
Stable Angina
episodic chest discomfort resulting from myocardial ischemia, usually resolve with rest and/or treatment
Prinzmetals Angina
angina resulting from abnormal spasm of coronary arteries
Why is nitro given for CHF/difficulty breathing?
dilates peripheral arteries and veins, reducing preload, afterload, and myocardial oxygen demand; can cause some coronary artery dilation increasing blood flow through the collaterals
Risks for CVD
smoking
advanced age
family Hx of CVD
HTN
hypercholesterolemia
carbohydrate intolerance (DM)
substance abuse
lack of exercise
Synchronized cardioversion
the defibrillator interrupts the QRS cycle and delivers electrical discharge during the R wave
To maintain BP in cardiac arrest:
push hard/fast
Chest contustion Tx
support ventilations, large bore bilateral IV, monitor EKG, rapid transport
Runaway pacemaker
Pacemaker malfunction where it causes rapid ventricular pacing
turn off with a donut magnet
NTG given in CHF patients
Decrease venous return
Synchronized cardioversion
Electrical current through the heart during a specific cardiac cycle (absolute refractory period)
Dropping pulse
Reduced cardiac output
Treatment for MI
Administer NTG
Stroke Volume
Depends on 3 factors: preload, contractility, afterload
venous return most influential to SV
Pediatric Bradycardia Algorithm
Epinephrine 0.01 mg/kg every 3-5 min
Atropine 0.02 mg/kg x1
Consider TCP
heart sounds
S1: “lub” caused by AV valves closing
S2: “dub” caused by closing of semilunar valves
S3: linked the flow of blood into the ventricles “slosh-ing-in” or “ken-tuck-y”
S4: linked with atrial contraction “a-stiff-wall” or “tenn-ess-ee”
After drowning, alveoli collapse is caused from:
Lack of alveolar surfactant
What medication with benefit asthma attacks without negatively affecting a heart attack
Atrovent
Tx for a patient with cyanosis and absent breath sounds
Nebulizer, steroid, BVM, IM Epinephrine, IV access with fluids
Inspiration and Expiration
Depend on changes in the volume of the thoracic cavity
stretch receptors limit inspiration
diffusion
affected by change in concentration of O2 in the alveoli (extending high altitudes)
affected by any disease that alters the structure of patency of the alveoli will limit diffusion
pulmonary edema, drowning, inhalation injury, prolonged hypoxia
lung perfusion depends on 3 conditions
adequate blood volume, intact pulmonary capillaries, efficient pumping of blood by the heart
pH falls, O2 becomes easily dissociated from hemoglobin causing O2 to be transported with hemoglobin instead of globin leaving little CO2 bound to hemoglobin
Emphysema
destruction of alveolar walls distal to terminal bronchioles, decrease in alveolar membrane surface area lessening the area available for gas exchange causing an increased ratio of air to lung tissue
commonly prescribed: steroids, Atrovent, betamethasone, metoprolol
S/S for pulmonary edema
SOB, recent Hx of surgery, Hx of asthma
Indications of treatment failure
increased cyanosis
decreased level of consciousness
decreased lung sounds
increased RR (tachypneic)
ARDS (acute respiratory distress syndrome)
commonly called “stiff lungs”
increased fluid in the interstitial space
rapidly progressing, life-threatening
adversely effects gas exchange in lungs causing hypoxia
form of pulmonary edema
Capnography
when perfusion decreases, ETCO2 levels reflect pulmonary blood flow and cardiac output not diffusion
decreased CO2 levels found in shock, cardiac arrest, pulmonary embolism, bronchospasm, and incomplete airway obstruction (mucus plugging)
increased CO2 levels are seen in hypoventilation, respiratory depression, hyperthermia
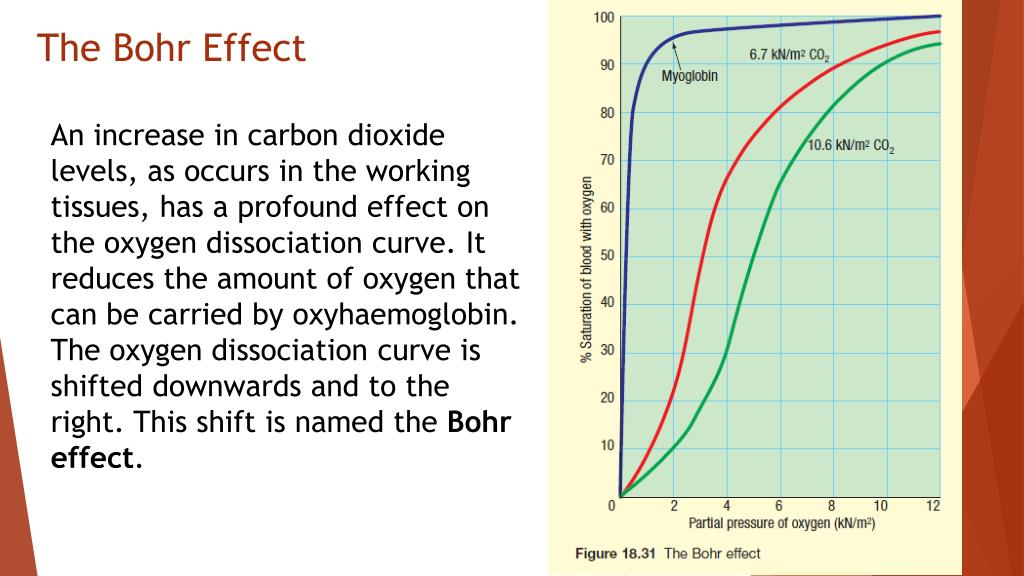
Bohr Effect
changes in body temperature, blood pH, and PCO2 alter the O2 dissociation curve—> within the tissues (as hemoglobin becomes bound with CO2) it loses its affinity for O2 resulting in more O2 being released and available to cells for metabolism
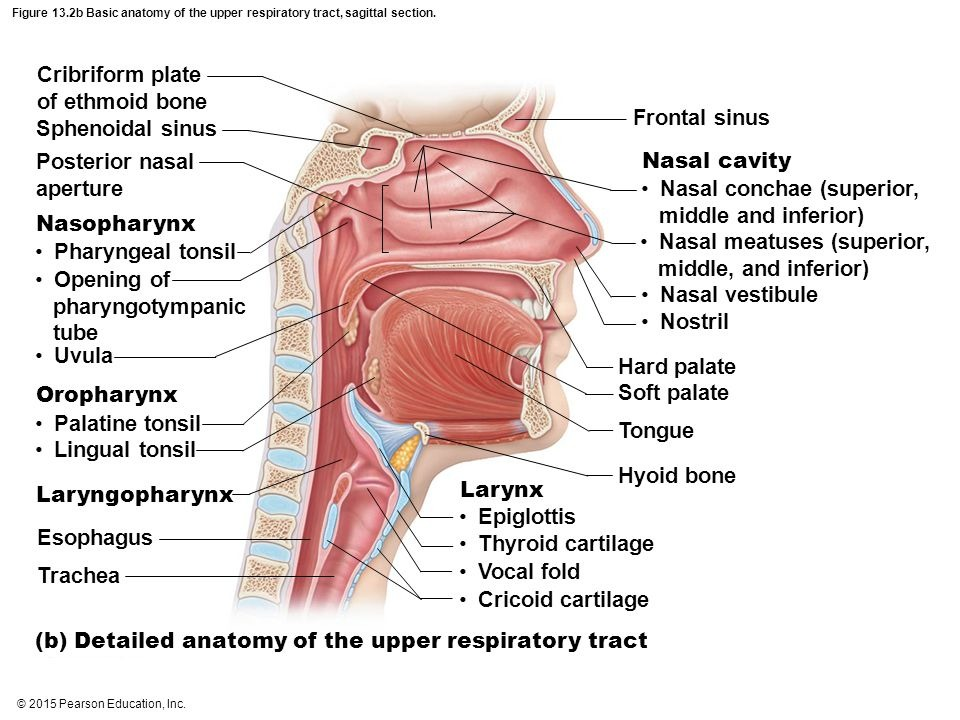
upper airway anatomy
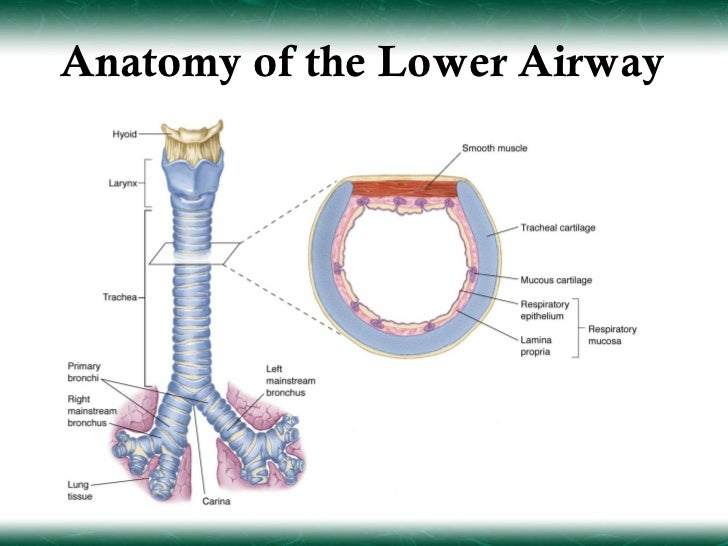
lower airway anatomy
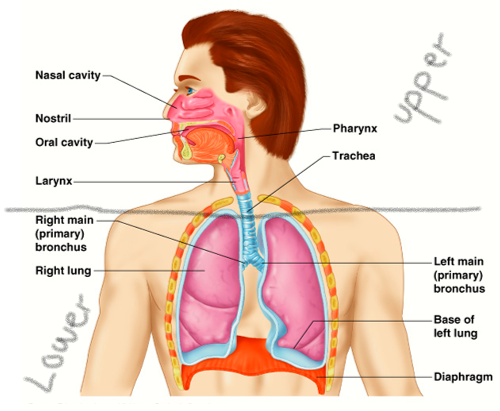
upper and lower airway anatomy
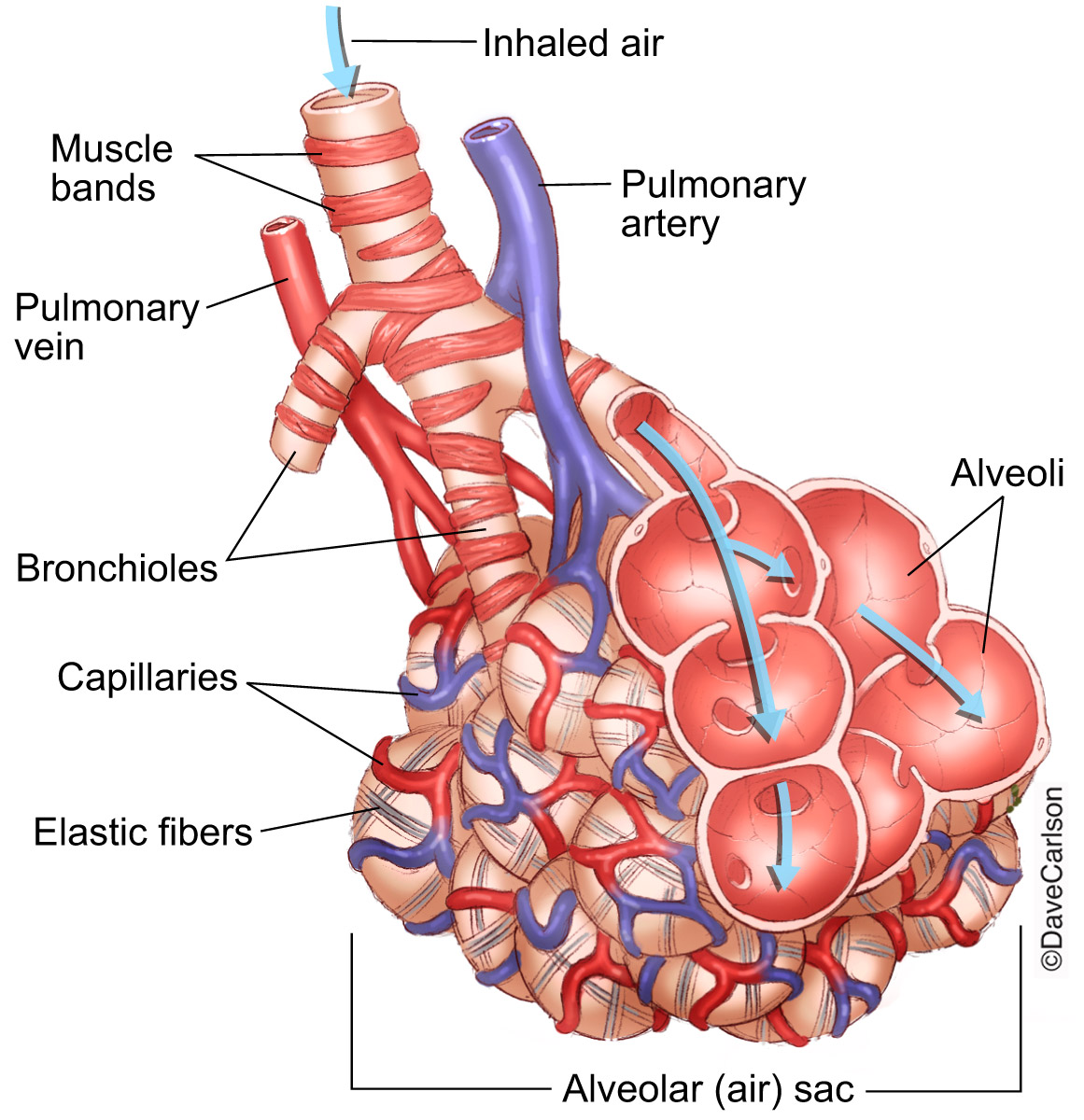
alveoli and pulmonary capillary anatomy
right heart failure
body
heart loses some of its ability to move O2 depleted blood to the lungs to pick up new O2
most often caused by L sided HF- can occur if L side is normal
pitting edema common sign
S/S
peripheral edema
ascites
JVD
cor pulmonale
high diastolic
uncontrolled HTN
left heart failure
lungs
most common type of HF
heart loses some of its ability to pump blood out to your body after it’s been re-oxygenated
usually caused by coronary artery disease
SOB common sign
S/S
O2 sat low
crackles bilaterally
pink, frothy sputum
dyspnea (paroxysmal, nocturnal)
accessory muscle use
Tx of HF
monitor rhythm accordingly
12-lead and IV access
mild- low dose nitro x3-5 mins max
moderate/severe- CPAP, high dose nitro (0.4 SL and 1” paste)
HTN/CHF: 250 mL, Epi infusion (1 mg in 100 mL at 1mL per minute- 60 gtts/min) titrate to SBP of 90 mmHg
Sodium-potassium pump
ships NA+ out of cell and K+ inside the cell against their concentration gradient
3 NA+ out of the cell and 2 K+ inside the cell
ATP drives the energy
from low to high
sodium is the main positive ion in the body
more positive on the outside than the inside at rest to create the squeeze and send more positive in
potassium= depolarization
once it’s all in (+), heart squeezes, it all goes out because it recognizes that it’s not supposed to be in there
Aspirin (ASA)
class: NSAID/ platelet inhibitor
indications: suspect ACD and/or STEMI
contraindications: allergy, patients who took a full dose prior to EMS arrival
dose: 324 mg (4×81mg chewable)
Nitroglycerin (NTG)
class: vasodilator
indications: angina, CHF, acute pulmonary edema
contraindications: allergy, peds <13y, pulmonary HTN or ED meds in the past 24 hrs., asymptomatic HTN, SBP <90, HR <60 or >150, inferior STEMIS
dose:
chest pain= 0.4 mg SL repeat x2 every 3-5 minutes, max dose 1.2 mg
pulmonary edema or CHF= low dose 0.4 mg SL, repeat 3-5 mins, max dose 1.2 mg; high dose x1 0.4 mg SL and 1” paste, x1 0.8 mg SL, continue 0.8 to achieve 20% reduction in SBP
NTG paste: 1” for adults
Adenosine
class: antiarrhythmic
indications: slow rate of narrow complex tachycardia, only effective in SVT, stable/wide complex tachycardia (possible VT) for pediatrics with caution
contraindications: allergy, Hx of moderate to severe asthma or active bronchospasm, polymorphic or irregular wide complex tachycardia
dose: adult 0.6 mg rapid IVP bolus followed by flus, give 12 mg if no response within 2 mins, give 12 mg if no response after another 2 mins; pediatrics 0.1 mg/kg rapid IVP/IO, max initial dose of 6 mg, 2nd and 3rd doses 0.2 mg/kg, max additional dose of 12 mg
Atropine
class: anticholinergic
indications: symptomatic bradycardia if pacing is ineffective
contraindications: known allergy, dysrhythmias in which enhancement of conduction may accelerate ventricular rate and cause < cardiac output (A-Fib, A-flutter, PAT with block)
risk/benefit contraindications: AV block at His- Purkinje level (Mobitz II or 3rd degree), suspected AMI/ ischemia, glaucoma
Epinephrine
class: sympathomimetic
indications: medical cardiac arrest/ peds trauma arrest
contraindications: HTN, preexisting tachydysrhythmias with a pulse (ventricular and supraventricular), IVP Epi should not be administered to any patient with a pulse
dose: PEA/asystole (0.1 mg/mL) 1 mg IVP every 4 mins, max dose 4 for initial arrest, 2 more for rearrest; VF/VT (pulseless) single dose (0.1 mg/mL) 1mg IVP/IO following initial dose of amiodarone, 1 more dose for rearrest, peds get max 4 initial and 2 for rearrest
Amiodarone
class: class III antiarrhythmic
indications: prevent recurrence of VF/VT after defibbing and conversion to SVT rhythm, VF, VT, A-fib, A-flutter with aberrancy (wide QRS), HR >130 and SBP >100
contraindications: seconds or third-degree AV block, allergy, idioventricular escape rhythm, accelerated idioventricular rhythm, sinus brady, block, or arrest, hypotension, cardiogenic shock, ventricular conduction defects, iodine hypersensitivity
dose: adult with pulse (A-fib or A-flutter with aberrancy) 150 mg IV/IO over 10 min mixed with 50-100 mL dilute, repeat x1; adult without pulse VF/VT (torsade after mag) 300 mg repeat x1 with 150 mg IV/IO; peds with a pulse 5 mg/kg IV/IO over 20 mins in 50-100 mL dilute; peds without pulse 5 mg/kg max single dose 300 mg repeat twice to max dose of 15 mg/kg
Esomolol
class: class II antiarrhythmic
indications: persistent VF or pulseless VT after the second dose of amiodarone
contraindications: allergy
dose: adult (>13y) 0.5 mg/kg IV/IO over 1-2 min no repeat; peds not indicated
Diltiazem (Cardizem)
class: calcium channel blocker
dose: 0.25 mg/kg (max 20 mg) IV bolus slow over 2 mins, if response not adequate repeat 15 mins of 0.35 mg/kg (max 25) over 2 mins; 50y or older, borderline BP (SBP 100-12