Pediatric EOR: Dermatology (Smarty PANCE)
1/141
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
142 Terms
What is the pathophysiology of acne vulgaris?
Follicular hyperkeratinization + Propionibacterium acnes colonization + sebum production + inflammation leading to comedones, papules, pustules
At what age does acne vulgaris typically begin?
Early puberty (ages 10-13) due to increased androgen production stimulating sebaceous gland activity
What are comedonal vs inflammatory acne lesions?
Comedonal: open (blackheads) and closed (whiteheads) comedones; Inflammatory: papules, pustules, nodules, cysts

What is first-line treatment for mild comedonal acne?
Topical retinoids (tretinoin, adapalene) - normalize follicular keratinization and prevent comedone formation
What is first-line treatment for mild to moderate inflammatory acne?
Topical retinoid PLUS topical antibiotic (clindamycin or erythromycin) or benzoyl peroxide
When should oral antibiotics be used for acne?
Moderate to severe inflammatory acne - doxycycline or minocycline (avoid tetracyclines <8 years old)
When should isotretinoin (Accutane) be considered?
Severe nodulocystic acne, acne resistant to other treatments, or acne causing scarring
What are the major side effects and monitoring for isotretinoin?
TERATOGENIC (iPLEDGE program required), dry skin/lips, elevated triglycerides/LFTs, depression - monitor lipids, LFTs, pregnancy tests
What patient education is important for topical retinoids?
Apply at night, expect initial irritation/dryness, use sunscreen (photosensitivity), may worsen before improving (purge period)
What is androgenetic alopecia in pediatric patients?
Rare in children - premature onset typically associated with endocrine disorders, PCOS in females, or genetic syndromes
What pattern of hair loss is seen in androgenetic alopecia?
Males: receding frontal hairline and vertex thinning; Females: diffuse central scalp thinning with preserved frontal hairline
What workup is indicated for pediatric androgenetic alopecia?
Endocrine evaluation (testosterone, DHEA-S, prolactin), thyroid function, consider PCOS workup in females
What is the classic triad of atopic dermatitis?
Eczema, asthma, allergic rhinitis (atopic triad) - often follows “atopic march” progression
What is the age-specific distribution of atopic dermatitis lesions?
Infants (<2 years): face, scalp, extensor surfaces; Children (2-12): flexural areas (antecubital, popliteal fossae), neck, wrists
What are the diagnostic criteria for atopic dermatitis?
Pruritus PLUS ≥3 of: onset <2 years, flexural involvement, dry skin, personal/family atopy, visible eczema

What is the first-line treatment for mild to moderate atopic dermatitis?
Liberal emollients (multiple times daily) + low to mid-potency topical corticosteroids for flares
What is the role of topical calcineurin inhibitors in atopic dermatitis?
Tacrolimus/pimecrolimus - steroid-sparing agents for face/neck, maintenance therapy, or steroid-resistant areas
What triggers should be avoided in atopic dermatitis?
Harsh soaps, hot water, wool clothing, common allergens (dust mites, pet dander), stress, dry environments
What are complications of atopic dermatitis?
Bacterial superinfection (S. aureus), eczema herpeticum (HSV), lichenification, sleep disturbance, psychosocial impact
What is eczema herpeticum and its treatment?
Widespread HSV infection on eczematous skin - presents with clustered vesicles, punched-out erosions; treat with IV acyclovir

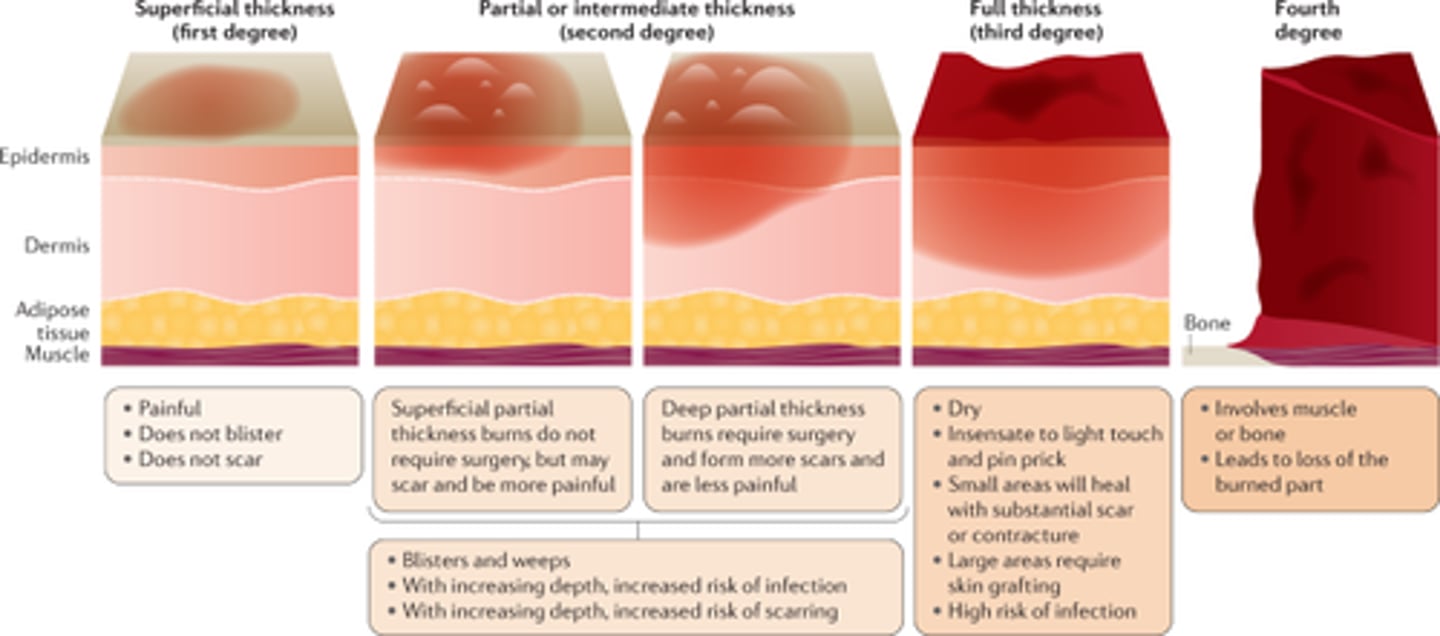
How are pediatric burn depths classified?
Superficial (1st degree): epidermis only; Partial thickness (2nd): dermis involved; Full thickness (3rd): through dermis; 4th: into muscle/bone
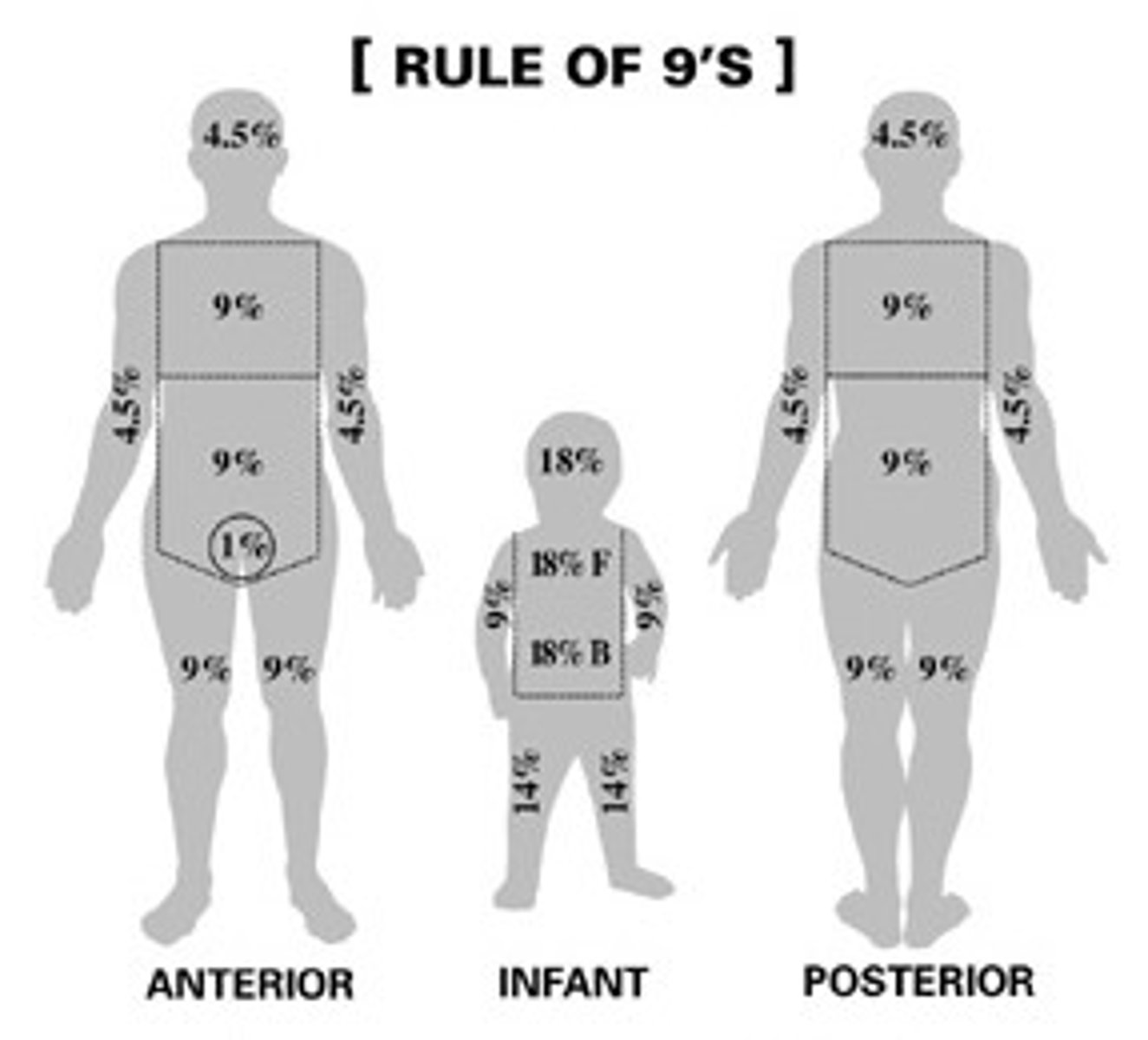
What is the Rule of Nines modification for children?
Head: 18% (vs 9% adult), each leg: 14% (vs 18% adult) - larger head, smaller legs proportionally
What burns require transfer to burn center in children?
>10% TBSA partial thickness, full thickness burns, face/hands/feet/genitals/joints, inhalation injury, electrical/chemical burns
What is the Parkland formula for pediatric burn resuscitation?
4 mL × weight (kg) × %TBSA burned in first 24 hours (give half in first 8 hours, half over next 16 hours)
What are signs of inhalation injury in pediatric burns?
Singed nasal hairs, carbonaceous sputum, hoarseness, stridor, facial burns, history of enclosed space fire
What is the immediate management of minor pediatric burns?
Cool (not ice) water for 10-20 minutes, remove clothing/jewelry, assess depth/extent, clean with soap/water, apply antibiotic ointment
What topical agent is used for burn wound care?
Silver sulfadiazine (avoid in sulfa allergy, <2 months old, pregnancy), or bacitracin for facial burns
What is the difference between irritant and allergic contact dermatitis?
Irritant: direct chemical injury (immediate, non-immunologic); Allergic: type IV hypersensitivity (delayed 24-72 hours)
What are common causes of pediatric contact dermatitis?
Nickel (jewelry, belt buckles), poison ivy/oak/sumac (urushiol), fragrances, preservatives, rubber accelerators
What is the classic presentation of poison ivy dermatitis?
Linear streaks of erythema, vesicles, and bullae 24-72 hours after exposure with intense pruritus

How is mild contact dermatitis treated?
Avoid allergen/irritant, cool compresses, topical corticosteroids (mid to high potency), oral antihistamines for pruritus
When are systemic corticosteroids indicated for contact dermatitis?
Severe widespread dermatitis, facial/genital involvement - prednisone 1 mg/kg/day (max 60 mg) tapered over 2-3 weeks
What is the most common cause of diaper dermatitis?
Irritant contact dermatitis from prolonged exposure to urine/feces causing maceration and skin breakdown
What differentiates Candida diaper dermatitis from irritant?
Candida: beefy-red with satellite lesions/pustules in inguinal folds; Irritant: spares inguinal folds
How is Candida diaper dermatitis treated?
Topical antifungal (nystatin, clotrimazole) with each diaper change + barrier cream (zinc oxide) + frequent diaper changes
What is perioral dermatitis and who gets it?
Papules/pustules around mouth with perioral sparing - seen in children 6 months-16 years, often after topical steroid use on face
How is perioral dermatitis treated?
STOP topical steroids, oral erythromycin or topical metronidazole, avoid irritants (toothpaste, lip products)
What are the most common drugs causing drug eruptions in children?
Antibiotics (amoxicillin, sulfonamides), anticonvulsants (phenytoin, carbamazepine), NSAIDs
What is the typical presentation of morbilliform drug eruption?
Symmetric erythematous macules/papules starting on trunk, spreading to extremities 7-14 days after drug initiation
What is DRESS syndrome?
Drug Reaction with Eosinophilia and Systemic Symptoms - fever, rash, facial edema, lymphadenopathy, eosinophilia, hepatitis (2-8 weeks after drug)
What drugs most commonly cause DRESS syndrome?
Anticonvulsants (phenytoin, carbamazepine, phenobarbital), allopurinol, sulfonamides, minocycline
When should a drug eruption prompt immediate drug discontinuation?
Mucosal involvement, blistering, facial edema, systemic symptoms (fever, lymphadenopathy), or signs of SJS/TEN
What is the classic target lesion of erythema multiforme?
“Target” or “iris” lesion with three zones: dark red center, pale middle ring, erythematous outer ring
What is the most common trigger for erythema multiforme in children?
HSV infection (most common) followed by Mycoplasma pneumoniae, other viruses (EBV, CMV)
What is the typical distribution of erythema multiforme lesions?
Palms, soles, and extensor surfaces (dorsal hands, elbows, knees) - symmetric distribution
How is erythema multiforme differentiated from Stevens-Johnson syndrome?
EM: <10% BSA, minimal mucosal involvement, target lesions; SJS: >10% BSA, severe mucosal involvement, atypical targets/macules
What is the treatment for erythema multiforme?
Usually self-limited (2-4 weeks) - supportive care, antihistamines, topical steroids; treat underlying infection if identified
What is recurrent erythema multiforme and its treatment?
≥6 episodes per year triggered by HSV - prophylactic acyclovir or valacyclovir can prevent recurrences
What are the classic pediatric viral exanthems?
Measles (rubeola), rubella, roseola (HHV-6), erythema infectiosum (fifth disease/parvovirus B19), varicella
What is the presentation of measles (rubeola)?
Prodrome: 3 Cs (Cough, Coryza, Conjunctivitis) + Koplik spots → maculopapular rash (face to trunk to extremities)
What are Koplik spots in measles?
Small white spots with red halos on buccal mucosa - pathognomonic for measles, appear 2-3 days before rash
What is the classic presentation of roseola infantum?
3-5 days of high fever (39-40°C) that suddenly defervesces, followed by rose-pink maculopapular rash on trunk
What is the “slapped cheek” appearance associated with?
Erythema infectiosum (fifth disease) caused by parvovirus B19 - followed by lacy reticular rash on extremities
What is the classic presentation of rubella (German measles)?
Mild prodrome, postauricular/suboccipital lymphadenopathy, pink maculopapular rash (face downward), resolves in 3 days
What is the presentation of varicella (chickenpox)?
Pruritic vesicles on erythematous base (“dewdrop on rose petal”) in crops, starts on trunk, in various stages of healing

When can children with varicella return to school?
When all lesions are crusted over (no new vesicles) - typically 5-7 days after rash onset
What organism causes impetigo?
Staphylococcus aureus (most common) or Group A Streptococcus (GAS) - can be MRSA in some areas
What are the two types of impetigo?
Non-bullous impetigo (70%): honey-crusted lesions; Bullous impetigo (30%): flaccid bullae that rupture easily
What is the classic appearance of non-bullous impetigo?
Erythematous papules → vesicles → rupture → honey-colored crusts, typically on face (around nose/mouth)

What causes bullous impetigo?
Staphylococcus aureus producing exfoliative toxin - creates flaccid bullae that rupture leaving “collarette of scale”
What is the treatment for localized impetigo?
Topical mupirocin 2% ointment TID for 5-7 days (first-line) or retapamulin ointment
When are oral antibiotics needed for impetigo?
Extensive disease (>5 lesions), multiple sites, poor response to topical therapy, or systemic symptoms
What oral antibiotics are used for impetigo?
Cephalexin or dicloxacillin for 7 days; clindamycin or trimethoprim-sulfamethoxazole if MRSA suspected
What is ecthyma?
Deep form of impetigo with ulceration extending into dermis - “punched out” appearance with thick adherent crust

What complications can occur from untreated GAS impetigo?
Post-streptococcal glomerulonephritis (not prevented by antibiotics), cellulitis, lymphangitis, scarring
What are the three types of human lice?
Head lice (Pediculus humanus capitis), body lice (P. humanus corporis), pubic lice (Phthirus pubis/crabs)
What is the most common age group for head lice infestation?
School-age children 3-11 years old, more common in girls (sharing hair accessories, close contact)
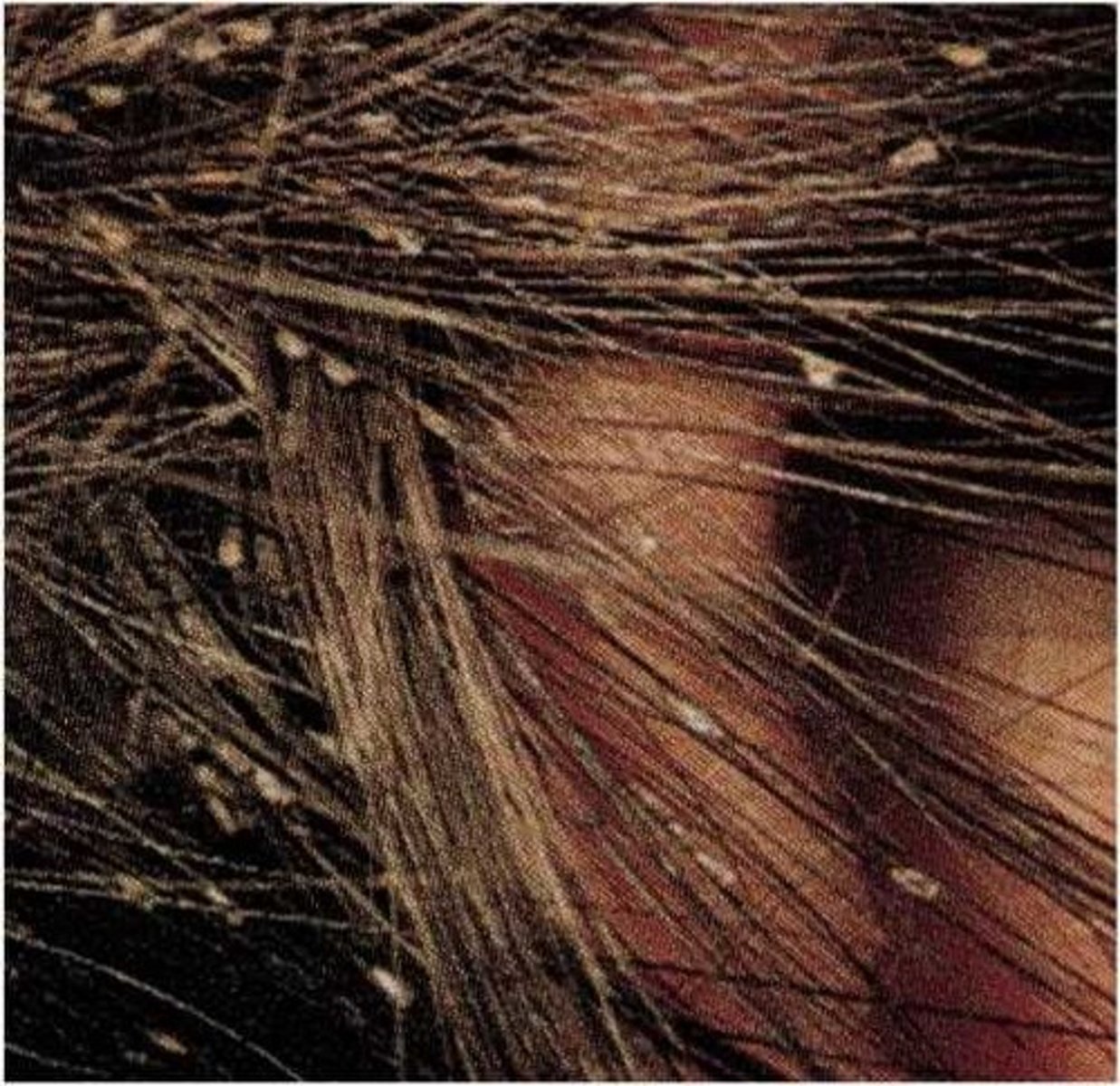
What is the definitive diagnostic finding for head lice?
Live louse on scalp (2-3mm, moves quickly) - nits (eggs) alone don’t confirm active infestation
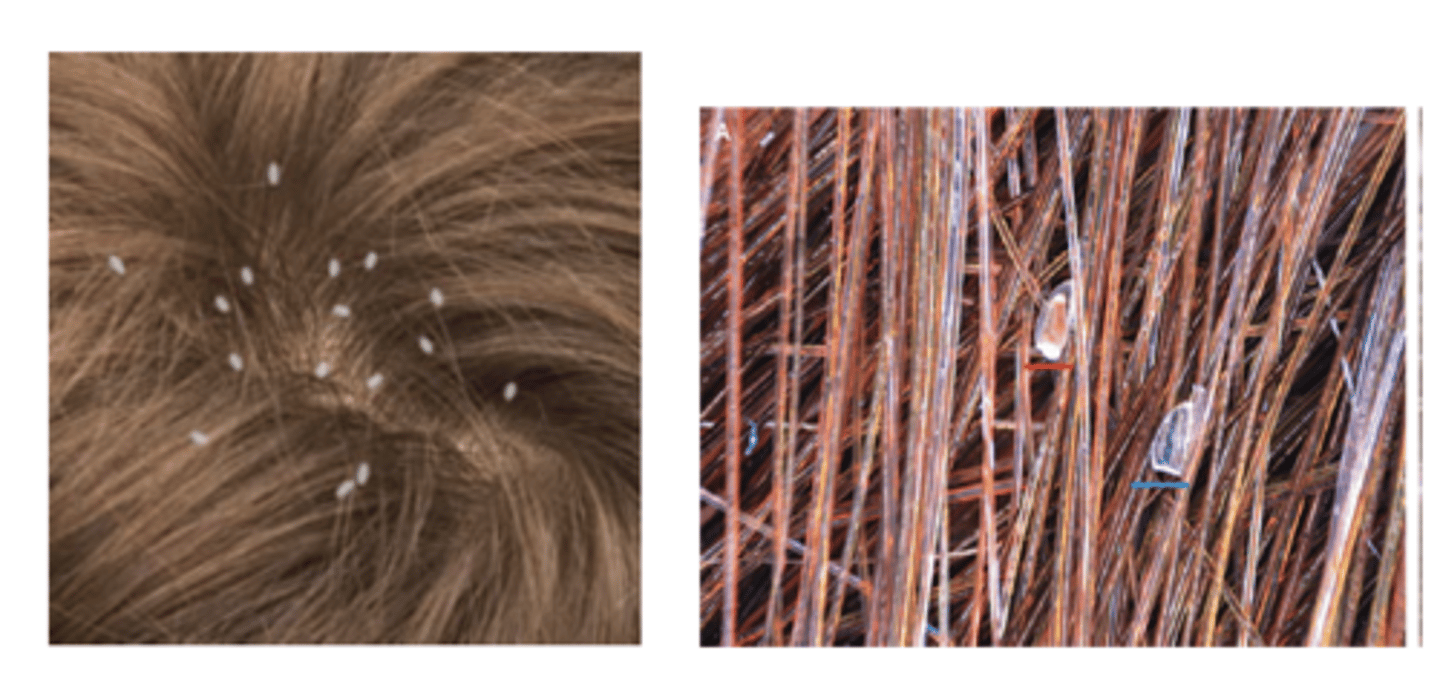
Where are nits typically found on the hair shaft?
Within 6mm of scalp (nits >6mm from scalp are likely old/hatched and don’t indicate active infestation)
What is first-line treatment for head lice?
Permethrin 1% cream rinse (OTC) or malathion 0.5% lotion - apply to dry hair, leave 10 minutes, rinse, repeat in 7-10 days
What treatment is used for permethrin-resistant head lice?
Ivermectin lotion 0.5%, spinosad suspension, or oral ivermectin (if >15kg)
What environmental measures are needed for head lice?
Wash bedding/clothing in hot water, vacuum furniture/carpets, soak combs/brushes in hot water; no need to treat entire house
When can children return to school after head lice treatment?
After first treatment application (AAP recommends no “no-nit” policies) - education about avoiding head-to-head contact
What is the classic presentation of lichen planus? Use the 6 Ps
Purple, Polygonal, Planar (flat-topped), Pruritic Papules, Plaques

Where are lichen planus lesions typically distributed?
Flexor surfaces (wrists, ankles), lower back, genitals; oral mucosa (Wickham striae)
What are Wickham striae?
White lacy lines on buccal mucosa - pathognomonic for oral lichen planus

What is the typical age of onset for lichen planus?
Rare in children - when it occurs, usually in children >5 years old
What is the treatment for lichen planus?
High-potency topical corticosteroids, oral antihistamines for pruritus; oral lesions may require topical tacrolimus
What is the herald patch in pityriasis rosea?
Single large (2-5cm) oval salmon-colored patch with collarette scale appearing 1-2 weeks before generalized eruption

What is the classic distribution of pityriasis rosea?
“Christmas tree” pattern on trunk - oval lesions following skin cleavage lines (lines of Blaschko)
What is the typical age group for pityriasis rosea?
Children and young adults 10-35 years old, possible viral trigger (HHV-6, HHV-7)
How is pityriasis rosea differentiated from secondary syphilis?
Pityriasis: herald patch, spares palms/soles; Secondary syphilis: includes palms/soles, no herald patch, positive RPR/VDRL
What is the treatment for pityriasis rosea?
Self-limited (resolves in 6-8 weeks) - symptomatic treatment with emollients, antihistamines, low-potency topical steroids if pruritic
What triggers should be avoided in pityriasis rosea?
Hot showers/baths (worsens pruritus), vigorous exercise (heat exacerbates), harsh soaps
What organism causes scabies?
Sarcoptes scabiei var. hominis (human itch mite) - obligate human parasite
What is the classic symptom of scabies?
Intense pruritus that worsens at night (due to mite activity) affecting multiple family members
Where are scabies burrows typically found in infants/children?
Infants: palms, soles, face, scalp; Older children: finger webs, wrists, axillae, waistline, genitals
What is the pathognomonic finding for scabies?
Linear or S-shaped burrows (tunnels) - often with papules, vesicles, or excoriations at ends
How is scabies diagnosed?
Scrape burrow with mineral oil, examine under microscopy for mites, eggs, or fecal pellets (scybala)
What is first-line treatment for scabies?
Permethrin 5% cream - apply neck down (include head/neck in infants), leave 8-14 hours, rinse, repeat in 1 week
What alternative treatment is used for scabies?
Oral ivermectin (for children >15kg or >5 years) - give 200 mcg/kg, repeat in 2 weeks
What household measures are needed for scabies?
Treat all household members simultaneously, wash bedding/clothing in hot water, seal non-washables in plastic bag for 72 hours
What is post-scabies pruritus?
Persistent itching for 2-4 weeks after successful treatment due to hypersensitivity to dead mites - treat with antihistamines, topical steroids
What is Stevens-Johnson syndrome (SJS)?
Severe mucocutaneous reaction with epidermal detachment affecting <10% BSA - medical emergency
What medications most commonly cause SJS in children?
Sulfonamides, anticonvulsants (lamotrigine, phenytoin, carbamazepine), allopurinol, NSAIDs
What is the prodrome of SJS?
1-3 days of fever, malaise, upper respiratory symptoms before mucocutaneous eruption develops
What are the characteristic skin lesions of SJS?
Dusky red/purple macules with atypical targets, vesicles, bullae, confluent erythema with epidermal detachment
What is the mucosal involvement in SJS?
Severe involvement of ≥2 mucosal surfaces (eyes, mouth, genitals) - erosions, hemorrhagic crusting, conjunctivitis
What is Nikolsky sign and its significance?
Lateral pressure on apparently normal skin causes epidermis to separate - positive in SJS/TEN
What is the immediate management of SJS?
Stop causative drug, admit to ICU/burn unit, supportive care (fluids, wound care, pain control, nutrition), ophthalmology consult