endo tx for young permanent dentition
1/91
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
92 Terms
pulp cap
tx of an exposed vital pulp by sealing the pulpal wound w a dental material such as calcium hydroxide or MTA to facilitate the formation of reparative dentin and maintenance of vital pulp
direct pulp cap
a dental material placed directly on a mechanical or traumatic vital pulp exposure
indirect pulp cap
a procedure in which a material is placed on a thin portion of remaining carious dentin that, if removed, might expose the pulp in immature permanent teeth
pulpotomy is also refered to as
pulp amputation
pulpotomy
the removal of the coronal portion of a vital pulp as a means of preserving the vitality of the remaining radicular portion
a pulpotomy may be performed as…
emergency procedure for temporary relief of symptoms or therapeutic measure, as in the instance of a Cvek pulpotomy
partial pulpotomy is also referred to as
shallow pulpotomy
cvek pulpotomy
partial pulpotomy
the removal of small portion of the vital coronal pulp as a means of preserving the remaining coronal and radicular pulp tissue
__________ and the __________ are the major factors in tx planning
pupal status; degree of root formation
tx for reversible pulpitis
vital pulp therapy
tx for irreversible pulpitis w a closed apex
RCT
tx for irriversible pulpitis w an open apex
vital pulp therapy OR root end closure + obturation
tx for pulp necrosis w a closed apex
rct
tx for pulp necrosis w an open apex
root end closure and obturation OR regeneration
_______________ is preferable to RCT, if possible, especailly in immature permanent teeth
maintaining a healthy pulp
teeth w open apices have ________ (thin/thick) dentin walls
thin → maintain vitality if possible
types of vital pulp therapies
indirect pulp cap
direct pulp cap
pulpotomy or cvek pulpotomy
success of vital pulp therapy depends on…
status of the pulp before procedure, and proper dx and clinical judgement
technique success depends on the placement of a restoration that precludes bacterial microleakage
indirect pulps caps are recommended in teeth w…
deep carious lesions close the pulp but no signs or symptoms of pulpal pathosis
is this scenario a candidate for an indirect pulp cap:
a tooth w a hx of spontaneous, lingering, or severe pain, or clinical or radiographic evidence of periapical pathosis
NO
indirect pulp caps are used when pulpal inflammation is ________ and complete removal of caries would like result in __________
minimal; pulp exposure
in an indirect pulp cap, the deepest layer of carious dentin is covered w a material to prevent ________ and _________ to the tooth
pulpal exposure; additional trauma
objective of indirect pulp caps is to maintain pulp vitality by… (4)
arresting the carious process
promoting peritubular (sclerotic) dentin, which dec dentin permeability
stimulating the formation of tertiary dentin, which inc the distance between the affected dentin and the pulp
remineralizing the carious dentin
direct pulp capping and pulpotomy involve application of a dressing to…
the exposed pulp in an attempt to preserve its vitality
pulpotomy differs from pulp capping in that…
a portion of the remaining pulp is removed before placing the capping material
what happens to odonotblasts during a pulp exposure
at the site of exposure, odontoblasts will be lost → progenitor cells from the pulp must differentiate into odontoblast-like cells to secrete dentin matrix
direct pulp capping and pulpotomy have been used for ________, ________, and _______ exposure of the pulp
carious; mechanical; traumatic
it is universally accepted that ______________ are the tx of choice for young permanent teeth w open apices
direct pulp caps or pulpotomy
goal of tx young permanent teeth w pulp exposures
maintain pulp vitality and continued root formation
once root formation has been completed, _____________ may be performed, if necessary
RCT
is this a good candidate for a direct pulp cap:
absence of a hx of pain and little/no bleeding at exposure site
YES
there is ____________ (agreement/disagreement) concerning direct pulp capping after a carious exposure in mature permanent teeth
disagreement
bc of normal aging of the dental pulp, chances of successful pulp capping ________ w age
diminish
ideal tx for carious pulp exposures on mature permanent teeth
rct
if rct is unfeasible (or based on clinical judgement), what can be done on a pulp exposure in mature permanent teeth
a direct pulp cap can be attempted → if fails → RCT
is this a good candidate for a direct pulp cap:
permanent teeth w a hx of spontaneous pain, radiographic evidence of pulpal or periapical pathosis, calcification of the pulp chamber or root canals, excessive hemorrhage at the exposure site, or exposures w purulent or serous exudate
NO
how is prognosis affected if there is a larger area of carious exposure
poorer the prognosis → more pulpal tissue is inflamed → greater chance for contamination by microorganisms
why must you be careful removing caries over an exposure site
want to minimize pushing dentin chips or microogranisms into pulp → this would lead to inflammatory rxn that can be severe and cause failure
after mechanical exposure of the pulp, ___________ occurs at the exposure site. but if the initial tissue damage is severe…
acute inflammation; pulp may become chronically inflamed, w eventual pulpal necrosis
prognosis of mechanical exposure vs carious exposures
mechanical better → they lack previous inflammation associated w carious exposures
type of direct pulp cap materials
calcium hydroxide- Ca(OH)2
MTA (mineral trioxide aggregrate)
bioceramics
what happens when Ca(OH)2 is directly applied to pulp tissue
necrosis of adjacent pulp tissue and inflammation of the subadjacent tissue occurs
dentin bridge formation occurs at the junction of the necrotic tissue and the vital inflammed tissue

understanding of mechanisms of Ca(OH)2
not fully understood
ability of Ca(OH)2 to form a dentin bridge is a result from…
a low-grade irritation of the underlying pulp tissue → beneath the region of necrosis, cells of the pulp tissue differentiate into odontoblast-like cells and produce dentin matrix
where does calcium from the dentin bridge come from if Ca(OH)2 was used as the direct pulp cap material
from the blood stream, NOT Ca(OH)2
overall results of using MTA as a direct pulp cap material
excellent results
MTA vs Ca(OH)2 as a direct pulp cap material
MTA produced more dentinal bridging in a shorter period of time w less inflammation
mechanism of MTA as a direct pulp capping material
interacts w synthesis fluid to produce an adherent precipitate w the same composition and structure as hydroxyapatite
Ca from MTA reacts w Ph in tissue fluid → producing hydroxyapatite
sealing ability, biocompatibility, and dentinogenic activity of MTA may occur bc of these rxns
what is the dominant ion released from MTA
Ca
commercially available MTA. products
ProRoot MTA (Dentsply Tulsa Dental) in gray and white versions
MTA is a ____________ cement w a ____________
portland; radiopacifier (bismuth oxide)
MTA hydrates in the presence of…
water formed a colloidal gel that solidifies
main components of MTA
tricalcium silicate
tricalcium aluminate
tricalcium oxide
pH of MTA
~12.5
properties of MTA
low solubility
low compressive strength
biocompatible
seals well
setting of MTA
long setting time → ~4 hrs
sets in the presence of tissue fluid or blood
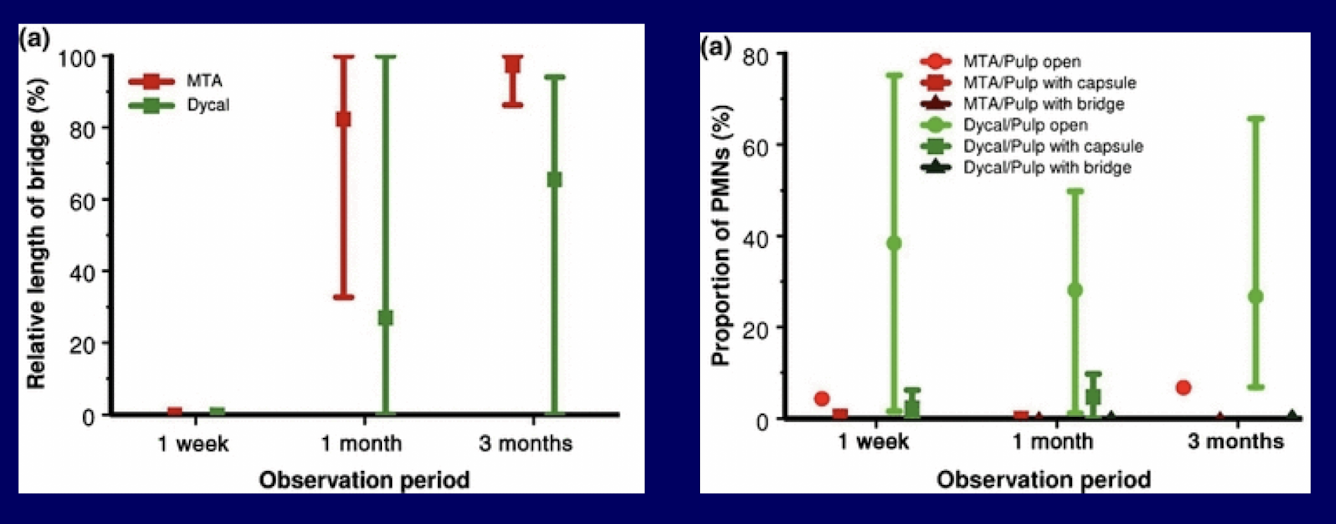
pulpal response to direct pulp capping in healthy human teeth w MTA vs calcium hydroxide cement
MTA resulted in less pulpal inflammation and more predictable hard tissue barrier formation than dycal (calcium hydroxide)
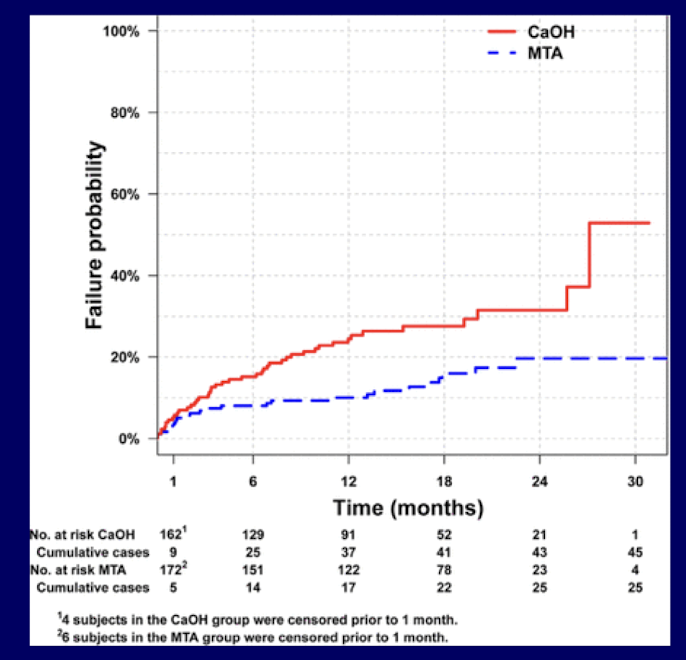
RCT success of direct pulp capping in permanent teeth w MTA vs CaOH
failure at 24 mo:
31.5% for CaOH
19.7% for MTA
large RCT provides confirmatory evidence for superior performance w MTA as a direct-pulp capping agent compared to CaOH when evaluated in a PBRN for up to 2 yrs
direct pulp capping w MTA
direct pulp capping w MTA after pulp exposure during excavation of deep caries could maintain pulp vitality in permanent teeth when a 2-visit tx protocol is observed
pros of MTA
evaluated extensively
biocompatible
sealing ability
clinical outcomes for perforation repairs, vital pulp therapy, root-end fillings, and apical plugs
drawbacks of MTA
long setting time
tooth discoloration
high cost
difficult handling characteristics
new _____________ have been developed to address drawbacks of MTA
bioceramics
difference between pulpotomy and pulp capping
additional tissue is removed form the exposed pulp in a pulpotomy
depth to which tissue is removed in a pulpotomy is determiend by…
clinical judgement → all tissue judged to be inflamed should be removed to place the dressing on healthy, uninflamed pulp tissue
what to do prior to exposing pulp in pulpotomy technique
remove as much carious dentin as possible
traumatic pulp exposures undergoing pulpotomy technique
the pulp has a proliferative response w inflammation extending only a few mm into pulp → when this hyperplastic inflamed tissue removed → healthy pulp tissue is uncovered
carious pulp exposures undergoing pulpotomy technique
it may be necessary to remove pulp tissue to a greater depth, compared to a traumatic pulp exposure, to reach uninflammed tissue
how to remove inflammed pulp tissue in pulpotomy
round carbide bur or diamond bur w high speed and water → creates the least damage to underlying tissue
all tissue coronal to the amputation site must be removed to control hemorrhage
what to do after inflamed pulp has been removed in pulpotomy
tooth is washed w physiologic saline or sterile water to remove debris → dry by vacuum and cotton pellets, NOT air
how to control hemorrhage in pulpotomy technique
cotton pellets slightly moistened w saline placed against the pulp
NaOCl on the cotton pellet can also be used
dry cotton pellets should NOOTTTT be used directly on pulp but will be used over moist pellets w pressure to control
in the pulpotomy technique, hemorrhage should be controlled within __________, and the pellets may need to be changed
several minutes
if hemorrhage continues after several mins, ensure…
all pulp coronal to the amputation site was removed and the site is clean
if still not controlled: amputation should be performed at a more apical level
what to do in pulpotomy technique once hemorrhaging is controlled
place MTA against the pulp stump
bc MTA takes several hrs to set, what do you do after you place this for a pulpotomy
a moist cotton pellet is placed over MTA and tooth is temporized → pt will return at a later date for removal of cotton and temp restoration so the definitive restoration can be placed
tx for necrotic teeth w open apices can be a challenge. the 3 most used historically and today are:
calcium hydroxide apexification- past
MTA apical barrier- present
regeneration/revascularization- present/future ?
_________ was historically a widely used material to promote apexification
calcium hydroxide
apexification occurs w many material, and had been reported even w/o canal-filling material after removal of necrotic tissue. the most important factors in achieving apexification are:
thorough debridement of the canal (to remove all necrotic pulp tissue)
sealing the tooth coronally (to prevent ingress of bacteria and substrate)
what type of calcified tissue formed a calcium hydroxide apexification
osteoid or cementoid
in calcium hydroxide apexification, deposits are adjacent to…
the filling material- may be short or RG apex
in calcium hydroxide apexification, calcified tissue can be continuous w the ____________
lateral root surfaces → “cap” or “bridge”
characteristic of calcified tissue in calcium hydroxide apexification
porous
calcium hydroxide apexification technique
access, establish WL, debridement, irrigation
fill canal w CaOH paste and seal coronally
recall at 3-6 mo intervals
calcified barrier verified RG and clinically
if barrier not present, repack w CaOH and continue periodic recall
if barrier present, obturate and restore
the total time calcium hydroxide apexification technique takes usually requires…
6-18 mo
calcium hydroxide apexification is _____________ (not/predictable)
is predictable
disadvantages of calcium hydroxide apexification
pt compliance
fractures
long-term CaOH may weaken dentin
alternatives using an artificial apical barrier that allows immediate obturation are…
replacing calcium hydroxide apexification → MTA is the material of choice
MTA apical barrier technique
access, establish WL, debridement, irrigation
resorbable barrier is pushed through the apex to create an extraradicular matrix against which to pack MTA
MTA plug compacted into apical 4-5 mm
wet cotton pellet + seal coronally or immediate filling
entire canal obturated (GP or composite)
restore
regeneration of necrotic pulp has been considered possible only after…
avulsion of an immature permanent tooth
advantages of regeneration
possible further root development and reinforcement of dentin walls → strengthening the root against fx
regeneration technique
if it is possible to create an environment similar to the avulsed tooth, regeneration should occur
if canal is disinfected, matrix into which new tissue can grow is provided, and the coronal access is sealed, regeneration should occur
apexification
a method to induce a calcified barrier in a root w an open apex of continued apical development of an incompletely formed root in teeth w necrotic pulps
apexogenesis
a vital pulp therapy procedure performed to encourage continued physiological development and formation of the root end
frequently used to describe vital pulp therapy performed to encourage the continuation of this process