Cognition and Neuro Behaviors Post-Brain Injury
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
Cognition in practice
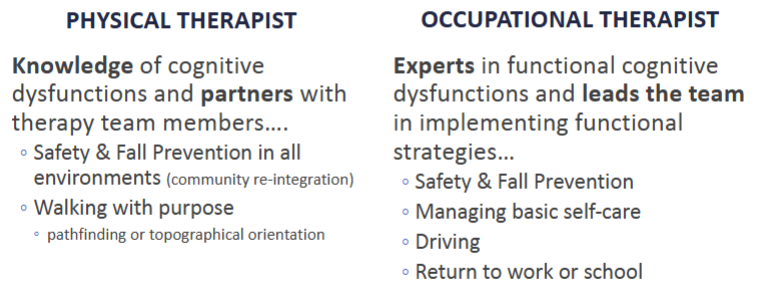
Why should we care?
Cognitive rehabilitation (remediation) vs. compensation for cognition following brain injury:
Improves problem-solving and executive function
Potentially reduces the cost of rehabilitation and lifestyle support following TBI
Impacts how we deliver feedback to the patient
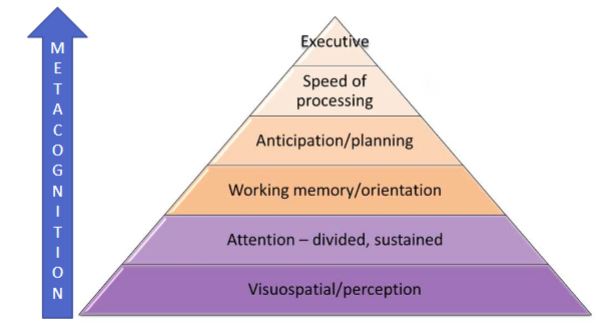
Cognitive skills hierarchy
Damage to temporal lobe
Explicit memory (declarative memory)
Implicit memory deficits (procedural memory)
Explicit memory deficits (declarative)
Retention and retrieval of facts, event, or steps to complete a task
Prospective Memory ability to remember to follow up and anticipate upcoming events, dates, deadlines, etc.
Explicit memory is notably affected during brain injury
Implicit memory deficits (procedural)
“It’s like riding a bike!”
Learned through movement or perception
Accessing implicit memory for learning can be affected due to perceptual and motor disorders as a result of the brain injury
Often utilize procedural memory tasks for remediation
Post-traumatic amnesia (PTA)
Amnesia can occur when there is damage to the medial temporal lobes and the hippocampus
Retrograde Amnesia
Loss of the ability to recall events that occurred immediately before the head injury
Anterograde Amnesia
New events in the immediate memory cannot be transferred into long-term memory; therefore, inability to form new memory (50 First Dates)
Can be retrograde, anterograde, or mixed/transient (unable to remember time and place but remember self)
PTA Recovery
Duration of PTA is an indicator of cognitive and functional deficits
80% of patients with PTA lasting < 2 weeks had good recovery
Classification of TBI due to memory deficits:
Mild TBI: < 24 hours
Moderate: 1-7 days
Severe: 1- 4 weeks
Very severe: > 4 weeks
Damage to prefrontal cortex
Working Memory (attention) deficits
Holding on to small amounts of information and applying it to a cognitive task
Important for learning and the first step in forming memories
Without attention memories cannot be formed
Affected by level of consciousness, arousal, awareness, and motivation
Executive Function deficits
Restraint: judgment, foresight, delay of gratification, inhibiting inappropriate behavior, and self-governance
Initiative: curiosity, drive, creativity, mental flexibility, and personality
Order: planning, abstract reasoning, sequencing, and organization
EF impact on behavior
Emotional control
Inhibition
Shifting
Self-monitoring
Emotional control
the ability to identify and regulate your emotions and respond in a socially tolerable and flexible way and also have a certain level of control over spontaneous reactions
Inhibition
involves being able to control one's attention, behavior, thoughts, and/or emotions to override a strong internal predisposition or external lure, and instead do what's more appropriate or needed
Shifting
involves conscious (not unconscious) change in attention
Self-monitoring
reflects how we understand our behaviors and how we adjust to make changes for the future. Self-monitoring behaviors can include both work-checking behaviors (reviewing mistakes, fixing errors, etc.)
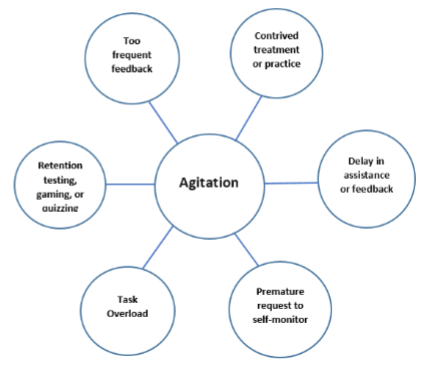
Executive dysfunctions and behavior manifestations
Agitation and aggression are a result of poor executive function skills, especially decreased ability for self-monitoring skills
Inability to establish healthy coping strategies
Important to identify antecedents that trigger maladaptive behaviors
Constantly observing for physical and verbal signs of behavior disruption
Implement healthy coping strategies for the individual
What is behavior?
Actions that are made by a person in conjunction with their environment
Response of the person to various stimuli or input
Neurological Behaviors are those that occur in response to a neurological injury that are dependent on severity of injury, injury location, and psychosocial variables of the individual
We all have behaviors
Etiology of neurological behaviors
Biological/biochemistry
Cellular level (dopamine, serotonin, melatonin, norepinephrine)
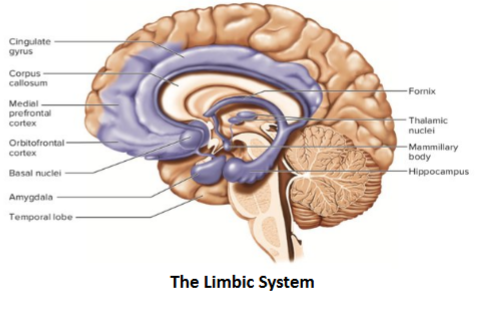
Neuropathology
frontal and temporal damage; unable to
process limbic system information,
cerebellum cognitive-emotional
regulation)
Neurobehavioral
Emotional regulation, Aggression, impulsivity, social withdrawal, compulsive behaviors, disorientation
Inability to adequately use executive function skills
Neurocognitive
Language (receptive and expressive aphasia)
Memory
Problem solving/judgement
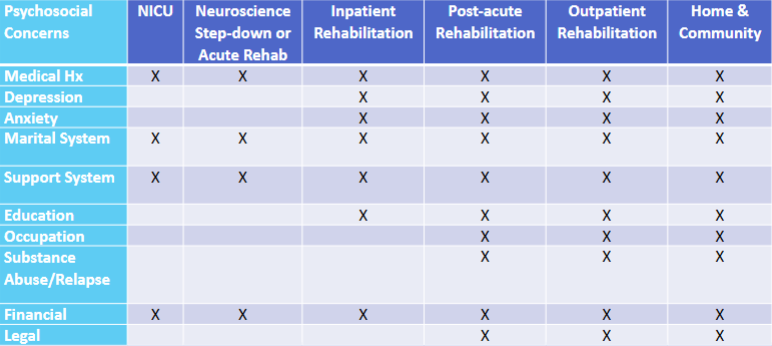
Psychosocial variables
Mental health prior to TBI
Family – culture – dynamic
Education level and achievement
Occupational history
Substance abuse
Financial considerations
Right hemispheric lesions
Agnosia
Inability to recognize the emotions or social cues of others
Inability to initiate an appropriate emotional response
Flat affect
Stunted emotionally
Poor social interaction or socially inappropriate
Impulsive with thoughts, words, actions, etc
They still understand everything going on around them but are limited to making an appropriate emotional connection
Left hemispheric lesions
Aphasia
Frustration with the inability to communicate effectively
Compulsiveness
Frustration when things are out of order or not going the way they want
Compounded with impaired communication
Increased desire for independence/safety
Risky behavior in efforts to not rely on others
Neuroplasticity
The brain’s ability to change and adapt in response to experiences, learning and changes
Whatever the person DOES (or does not do)
is what they are going to continue to do….
Optimal behavior is key!
Negative behaviors
A behavior is typically considered negative when there is a RISK!
These tend to get our attention more than positive behavior…
Negative behaviors tend to be subjective
Verbal outburst
Verbal aggression
Physical aggression
Inappropriate sexual behavior
Elopements – leaving without permission or without someone knowing where they are
Impulsivity
Self-harm
Positive behaviors
Often have no risk, so we tend to overlook these…
Social courtesy – consideration of others
Social skills
Problem-solving
Appropriate requesting
Self-calming or self-regulation
Safety awareness
Acceptance of feedback
THE GOAL: Replace negative behaviors with positive behavior
We need to focus our attention on the positive behaviors by reinforcing them…
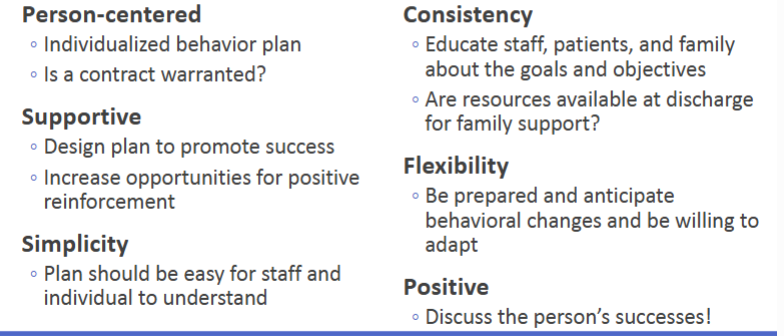
Behavior plan
Structured, collaborative strategy designed to identify, understand, and manage behaviors that interfere with recovery, safety, or quality of life after a brain injury.
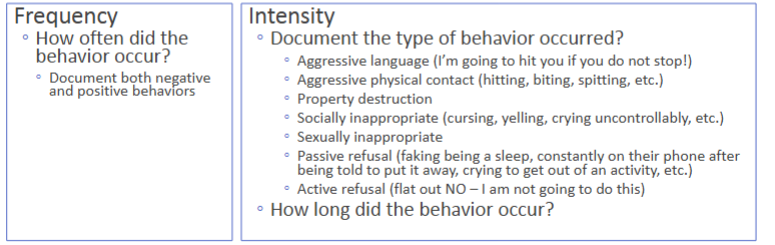
Help to determine the relative frequency and intensity of the behaviors
Both positive and negative behaviors should be measured
Behavior intervention plan (BIP) designed to modify the environment and consequences to shape more functional behaviors.
Are multidisciplinary collaborations that are designed to help the whole team understand behaviors and avoid over medication/sedation
What’s our role in the behavior plan?
Skillfully observe interactions through the different environments and activity demands
Identify and document potential triggers
Redirect/Reinforce as appropriate
Implement the behavior strategies that are deemed successful by the team and document their effectiveness
Guidelines for reducing behavior
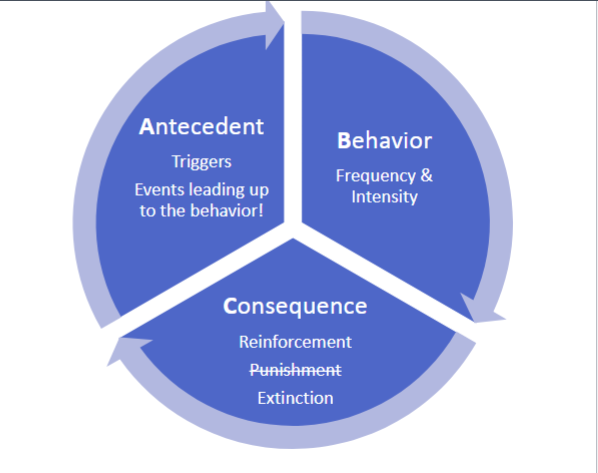
Antecedent
Document all events leading to behavior and possible to triggers:
Do they appear more anxious, angry, tired, etc. than usual?
Was there anything different about their greeting? Was it a typical greeting for this individual?
Consider different triggers. Environmental? Activity? Personal/psychosocial factors?
Behavior
Consequences
Implementation of the behavior plan or strategies agreed upon by the therapy team
Document your response (the chosen strategies) & the person’s response to those strategies:
The individual’s response is usually MOST negative when implementing new strategies
Did the behavior persist, or did extinction occur after using strategies?
Did additional staff have to step in due to escalation?
What strategy seemed to be the most effective? Be prepared to share this with the team.
Behavior plan requirements
Consequences: Strategies for shaping negative behavior
Extinction
“Pivoting” from “junk” or negative behavior
Must use good clinical judgment to determine if negative behavior should persist
Plan for backup staff in near proximity for anticipated escalation of behavior
Redirection to another task or environment
Positive Reinforcement
Praising “desired” or positive behavior
Modeling positive behavior
Praising others in close proximity for their positive participation
You perform the desired task in hopes of their contribution
Substitute negative behaviors
We do NOT want to restrict experiences
We WANT to allow real-life experiences to allow for opportunities to reinforce positive behaviors
Be prepared and have backup!
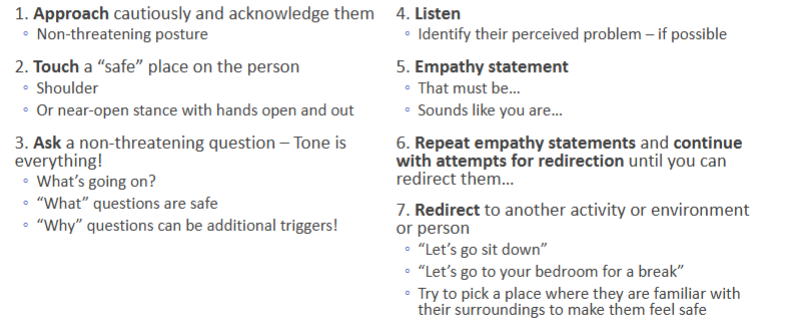
Steps for de-escalation
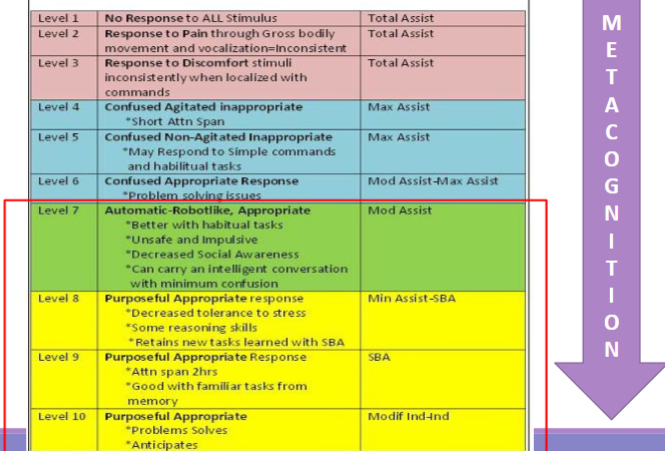
Metacognition
•“thinking about thinking”
•The awareness and regulation of one’s own cognitive processes
•Planning how to approach a task- monitoring comprehension
during the process and evaluating performance afterward.
•Planning, monitoring, evaluating, studying, problem-solving,
preparation.
•Helps learners become more confident and independent.
Choosing an intervention based on metacognitive availability
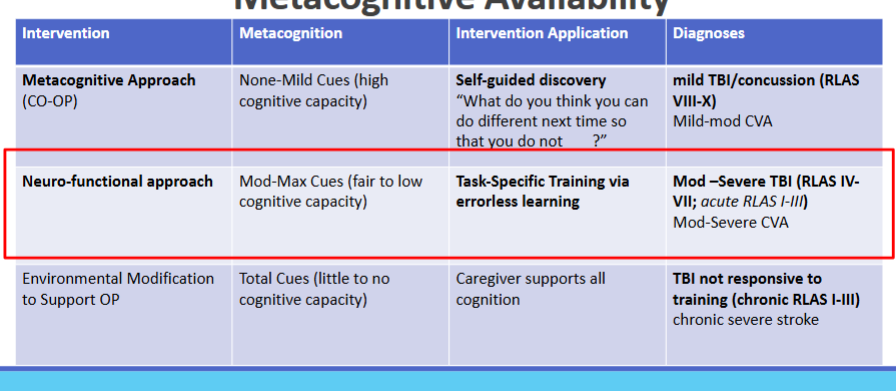
Neuro-functional approach (NFA)
“Learning by doing” through meaningful activities (task-specific training)
Utilize “practice tasks” that have a structured format
Eliminate the required use of executive function
Develop competency and improve self-esteem
Enhances performance and promotes engagement
Goal-setting → positive feedback → motivation
Practice makes perfect
Practice Schedules
Structured daily schedules
Consider the individual’s routine
Blocked Practice vs. Random Practice
Initially blocked practice may be necessary for skill acquisition then transitioning to random practice to facilitate generalization
Trial and error learning
The superior form of learning for people with self-monitoring capabilities
◦ Able to…
1) remember if an error has occurred
2) recognize an error
3) suppress maladaptive behaviors or behaviors
that interfere with the performance
4) replace error-full or maladaptive behavior
with a different or more optimal behavior
Moderate to Mild TBI
Errorless learning
Used with people who have decreased self-monitoring and memory impairments
◦ Unable to…
1) remember if an error has occurred
2) recognize an error
3) suppress maladaptive behaviors or behaviors
that interfere with performance
4) replace error-full or maladaptive behavior
with a different or more optimal behavior
Therapeutic alliance
Emotional bond between client and therapist
Mutual agreement on goals
Mutual agreement on the tasks within the intervention
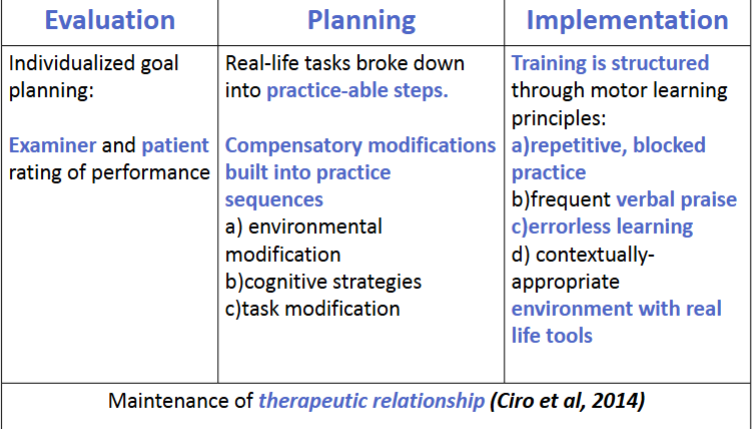
Evaluation, Planning, Implementation
Cognitive strategies examples
Memory & attention aides
◦ Therapy “to-do” or daily check-lists
◦ Daily calendar and orientation logs
◦ Verbal summarization
◦ Visual targets or external cues during pathfinding or activities
◦ Timers (visual timers) and/or alarms for reminders
◦ Grading environment stimuli
Executive Function
◦ Plan and organize in advance or prior to the performance
◦ Time blocking to manage “work” time, scheduling breaks,
etc.
◦ Grade activity to down or up with summary feedback
◦ Complete part of the task versus all of the task
◦ Allow the person to vocalize successes and areas of improvement or provide this for the person if they are unable to
Overlearning a task
Acquisition of skill beyond the point of mastery
No more performance improvements are observed with practice
Increased ability to maintain skill and reduces performance effort
Increased stability of learned skills and increased self-monitoring skills
Reduces the likelihood of regression as reinforcements are gradually removed
Goal is to achieve optimal, automatic behavior
What’s our goal as therapists?
GENERALIZATION

Behavior change through cognitive approaches
Therapeutic Alliance
patient-therapist trust each other
Neuro-functional Approach (Task-specific Training)
salience will increase motivation and promote participation
Overlearning
the appropriate behavior
Psychosocial & environmental factors
Improving metacognition
Use guided self-discovery – Let them figure it out!
Reshape intended behavior by asking probing questions that requires self-reflection of performance
CO-OP (Cognitive Orientation to daily Occupational Performance)
Signs of metacognition
◦ Spontaneously checks work
◦ Has a good understanding of own personal strengths and weaknesses?
◦ Can easily estimate abilities
◦ Can self monitor during a task— “Am I doing ok? Do I need to change how I am doing this?”
◦ Can monitor the amount of time it is taking to do the task
◦ Can detect errors and change accordingly
Factors that impact prognosis
Age, physical and mental condition, socioeconomic status, & social support
Initial Glasgow Coma Scale and at the time of admission predicts disability and recovery
Longer the duration = poorer outcomes
Severity of the injury; type and location of injury; other injuries and complications; prolonged time before initiation of rehab
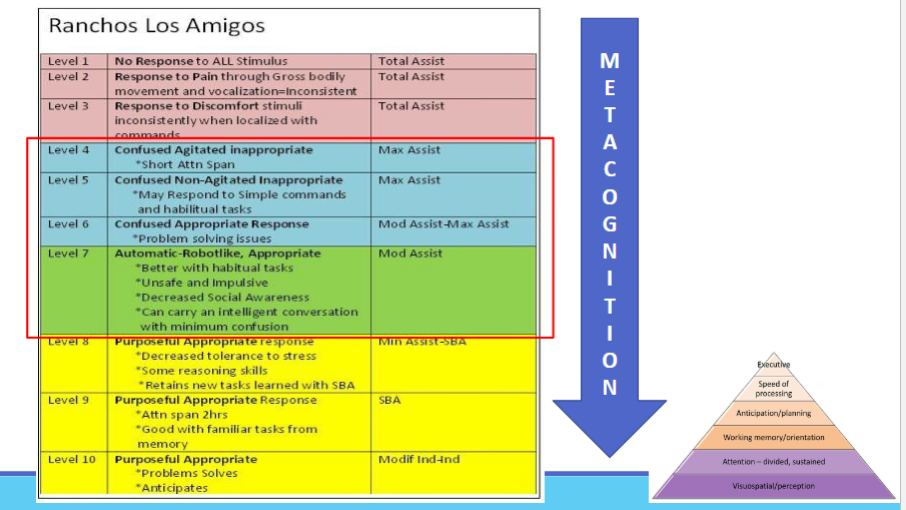
Duration of recovery/time spent at different Rancho Levels
Length of post-traumatic amnesia
Disability Rating Scale - associated with employability and school