FSHN 3620 • Exam 2 SG: Ch. 10/11
1/9
Earn XP
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
10 Terms
Growth and development in early childhood
Growth
Infants: weight 3x in first year
Toddler: ages 1-3 years
Average growth: 3-5 lb, 3-5 in./yr
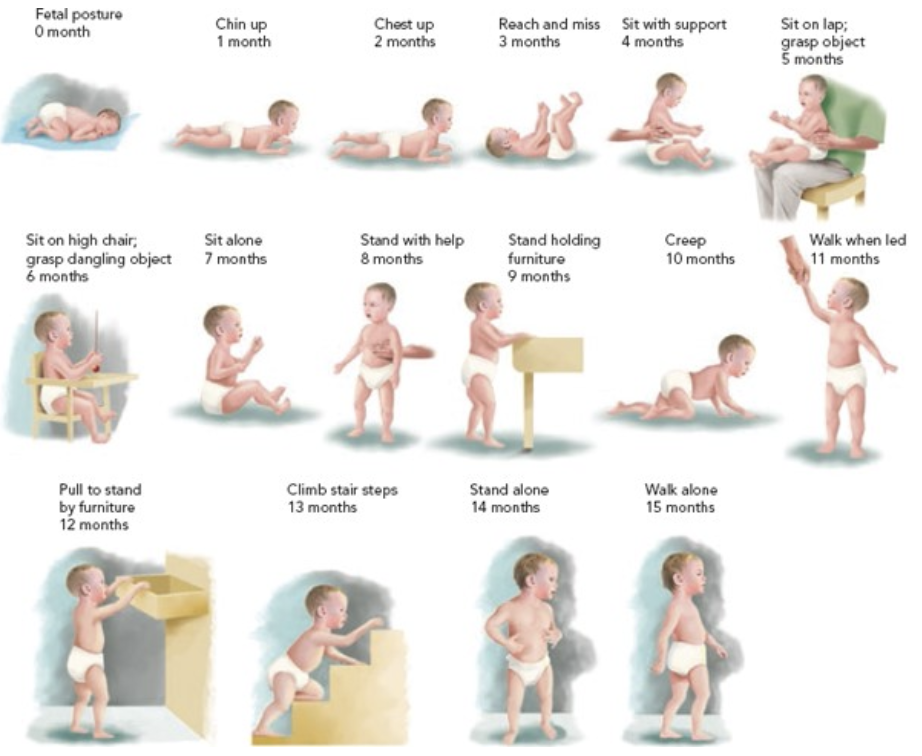
Rapid increase in gross and fine motor skills
Increasing independence, like to explore their environments, language skills develop
Preschool: ages 4-5 yrs
Average growth: 4-6.5 lb, 2.75 in per yr
Increasing autonomy, growing language skills
Expanding behavior control
Physical:
Increase in skull size, jaw widens to accommodate teeth
‘Baby’ fat is lost, Protuberant abdomen by 4th yr
Development
Palmar grasp
Pincer grasp
Protective reflexes
Rooting, ability to suckle, coordinate sucking, swallowing, breathing
State of arousal provides a framework to observe, understand, & interact with infants
Reading and interpreting appropriate growth charts in early childhood
0 – 2 yrs: Use WHO Growth Charts
Standards to identify how children should grow when provided optimal conditions
2 – 19 yrs: Use CDC Growth Charts
Weight, Length/height, head circumference for age, Weight by Length, BMI for age
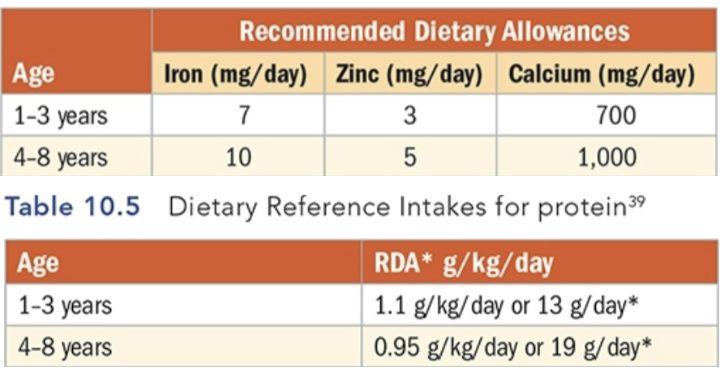
Nutrient needs in early childhood and common nutrient problems
1 Tbsp of food per year of age
Vitamin A
Required for:
Normal functioning of visual system
Maintenance of cell function and growth
Epithelial integrity
Red blood cell production
Immunity and reproduction
Deficiency
Common in lower income countries
Mostly due to low Vitamin A intakes
Deficiency symptoms
Xerophthalmia or dry eyes
Leading preventable cause of blindness in children
Decreased resistance to infection
Iron deficiency in children, milk anemia, and how it is prevented and treated
Iron deficiency anemia
Rapid growth + inadequate intake = common deficiency
Children ages 1–5 yrs should not drink >24 oz/day of goat/cow/soy milk
Screening recommended for children at risk
Treat with iron drops and more meat, fish, poultry, & plant sources/Vitamin C to enhance absorption
If anemia and/or iron stores are not improving, there may be other causes
Pica
Consequences of Iron Deficiency
pallor
fast heartbeat
weakness
poor growth
anorexia
impaired immune function
anemia
cognitive disability
Milk Anemia
Ca & casein bind iron in the intestine & hinder absorption
Over consumption of cow’s milk is the leading cause of iron-deficiency anemia in toddlers >1 y/o
AAP rec. No more than 16 oz (2 cups) of cow’s milk/day for 12-24 mo. old
2–5 y/o → 2-3 cups/day
Decreased iron absorption & higher risk of iron deficiency
Increased risk of blood loss from the GI track
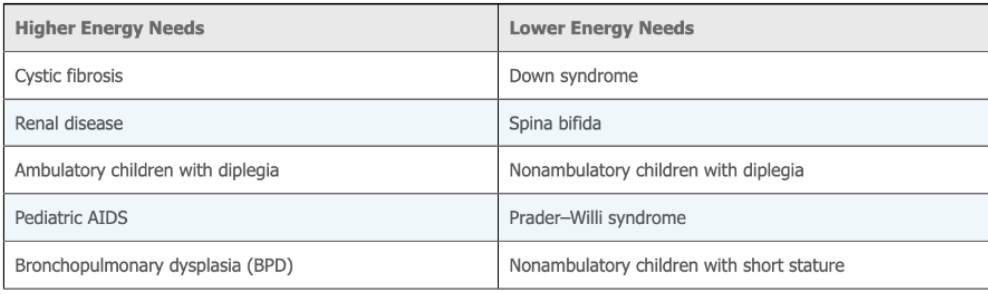
Know how nutrient needs change with special health care needs
Children with Special Health-Care Needs
Broad term for children with, or at risk for, chronic conditions and disabilities
Can be caused by genetic or metabolic disorders, birth defects, preterm birth, infections, prenatal drug exposure, & more
~19.4% of children in the US have special health needs
90% of these children have nutrition-related problems
Feeding problems, both behavioral and neuromuscular, and tube feeding
Behavioral Feeding Problems
Attention deficit hyperactivity disorder (ADHD)
Usually diagnosed in school-age children
Autism spectrum disorder (ASD)
Sensory and environmental preferences & factors can make it uncomfortable & difficult for children with autism to eat a variety of foods
Children with ASD often prefer to eat the same foods over & over
May prefer juices and protein shakes over solid foods
Intervention may include total vitamin & mineral supplementation while SLOWLY introducing food
There is a rise in gluten-free, casein-free, etc. diets for children with autism to improve behavior; the AAP does not recommend these diets unless there is a food allergy or intolerance
Neuromuscular Feeding Problems
Hypertonia: rigid, high muscle tone.
Hypotonia: low muscle tone
Both are symptoms of some disabilities that make feeding oneself difficult
Difficulties holding a spoon, swallowing
Very frustrating for the child, & may begin to refuse eating
Tube feeding is required if nutritional needs can't be met my mouth
Tube Feeding
Necessary when nutritional needs cannot be met by mouth
Also utilized when infants and children are at risk for choking or aspirating food or fluids into the trachea and then lungs
Nasogastric (NG) or gastrotomy (G) tubes
Enteral tube feedings (ETF): tube placed into the stomach or SI.
Total parenteral nutrition (TPN): tube inserted into a vein whereby nutrients enter the bloodstream directly.
Food allergies
Basis for allergic reactions is the absorption of intact proteins
Common symptoms are respiratory issues and skin rashes
Children sometimes grow out of allergies
Top 9 food allergenic foods are milk, eggs, fish, crustacean shellfish, tree nuts, peanuts, wheat, soybeans, & sesame
Peanut allergy
Leading cause of death related to food: anaphylaxis
Anaphylaxis: Sudden onset of a reaction with mild to severe symptoms, including a decrease in ability to breathe, wheezing, coughing or tightness in chest, which may be severe enough to cause a coma
Lead poisoning
Elevated blood lead levels
Affects many tissues → including brain, blood, & kidneys
Low-level exposure → decreased IQ, impaired motor, behavioral, & physical abilities
Decrease growth
No safe level
Major sources of exposure → airborne lead, deteriorating paint
Risks → children putting things in their mouths to explore
~25% children living in housing with deteriorated lead-based paint
Tastes sweet, tempting children to consume
Risk factors → young age, poor nutrition, low socioeconomic status, pica
Adequate iron & calcium may decrease lead absorption
Vitamin C may increase lead excretion (not fully understood)
Other nutrition related conditions
Galactosemia – must eliminate galactose from diet
Von Gierke’s disease –provide glucose between meals
Phenylketonuria – must eliminate phenylalanine from diet
Maple Syrup Urine Disease – restriction of branched-chain amino acids
Hartnup disease – provide megadoses of nicotinic acid
Global nutrition and malnutrition concerns such as stunting, wasting, PEM, etc.
Vitamin A Global Prevalence
33.3% of pre-school children in the world (low serum retinol)
0.9% are night blind
Iron
Most common nutritional deficiency worldwide
Anemia caused 50 million years of healthy life lost due to disability in 2019 (WHO)
Children at growing age are at most risk because of increasing blood volume
Reasons for iron deficiency:
Inadequate intake
Impaired absorption
Less bioavailable iron is the only option available
Hemorrhage
Repeated blood losses (parasitic infestation)
Wasting: Child too thin for height due to acute malnutrition.
Not getting enough calories to support nutrition needs and faces an immediate risk of death
Stunting: Failure to grow physically and cognitively due to chronic or recurrent malnutrition.
Effects last throughout the child’s whole life
Protein-Energy Malnutrition (PEM)
PEM: Results when protein or energy are not sufficient in diet.
Primary reason: inadequate food intake
Secondary reason: inadequate nutrient absorption, utilization, increased nutrient utilization and/or losses
Kwashiorkor: protein deficiency, but enough CHO.
Severe protein deficiency but normal caloric intake
Peripheral edema (around abdomen)
Hair changes common – sparse & easily pulled out
Dermatosis, flaky paint appearance of skin
Poor appetite
Reduced subcutaneous fat
Fatty liver common
Worse prognosis
Marasmus: deficiency in all energy – lack both CHO & protein.
Severe deficiency of all nutrients & inadequate caloric intake
Peripheral edema is absent
Hair changes absent
Skin is dry & wrinkled but no dermatosis
Voracious appetite
Absent subcutaneous fat
Fatty liver uncommon
Better prognosis
Lead
Major health concerns here & around the world!
Prevalence: 2.5 % of children 1 – 5 y/o
Young children absorb lead more efficiently (50 vs 10%)
Absorb 4-5x more lead in children than adults