visual electrophysiology II
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
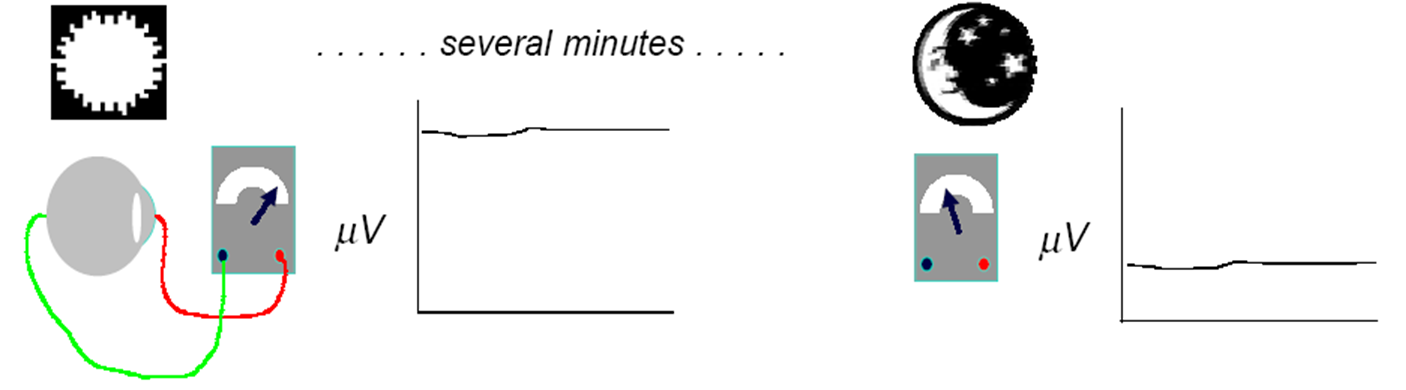
what is EOG - what does it measure (2)
Measures the standing potential (integrity) of the retinal pigment epithelium (RPE)
Standing potential is higher in daylight conditions than it is in dark conditions
how do we measure an EOG (3)
Electrodes are used to monitor eye movements.
Patients observes targets on left and right - 30 degree saccades - swap between L and R
20 minutes in both bright and dark conditions


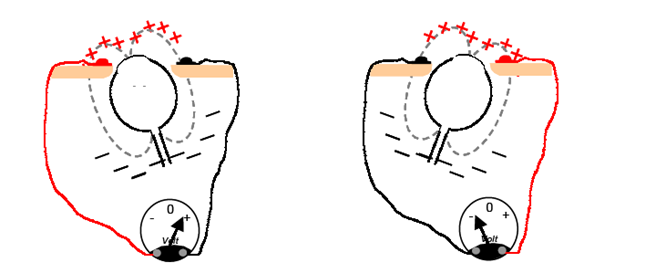
explain why we ask the px to move their eyes from side to side (4)
•The EOG measures the potential that exists between the cornea and Bruch's membrane at the back of the eye (where the RPE is)
•The potential produces a dipole field with the cornea approximately 5 millivolts positive compared to the back of the eye, in a normally illuminated room
•By getting the eye to move from side to side we can measure the variation in the dipole
•Although the origin of the EOG is the pigment epithelium of the retina, the light rise of the potential requires both a normal pigment epithelium and normal mid-retinal function
what does a normal EOG look like (2)
Microvolt level decreases to a minimum level during dark phase
Amplitude Increases during light phase - Called “light rise”
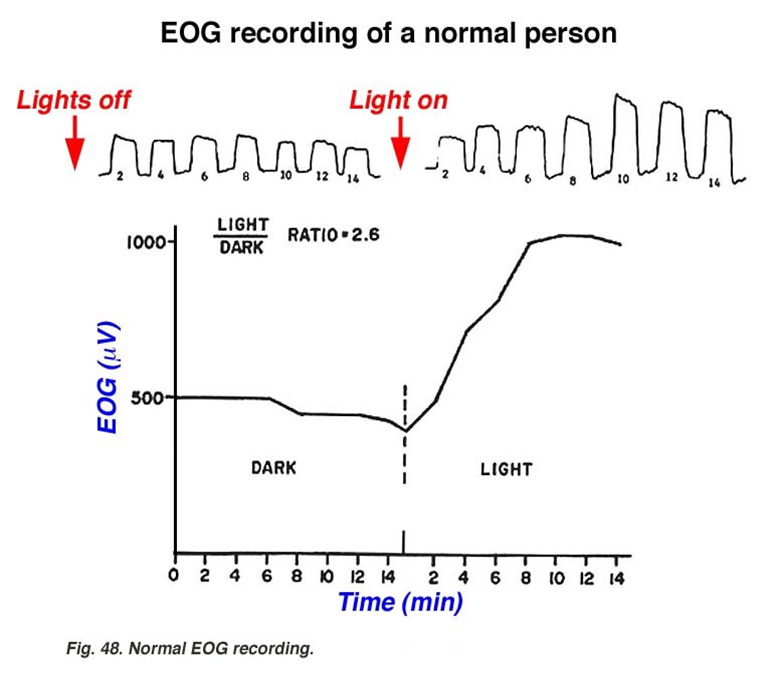
describe how we quantify an EOG (4)
using the Arden ratio
Light peak amplitude /dark peak amplitude = Arden Ratio
Normal range 1.7 up to 4.3 - whatever number you get means that the light peak amplitude is x times greater than the dark peak amplitude
Abnormal result if below 1.7
describe the link between the Arden ratio and age
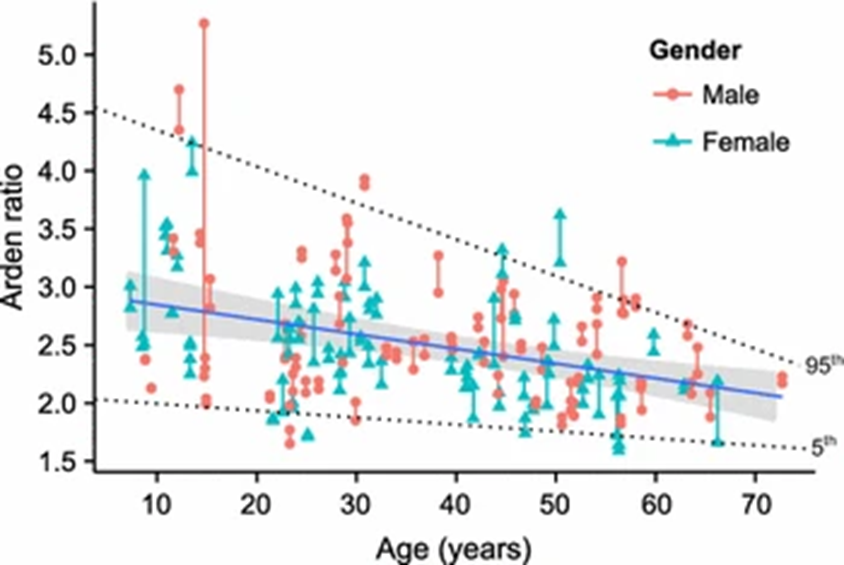
as age increases - Arden ratio tends to decrease in both men and women
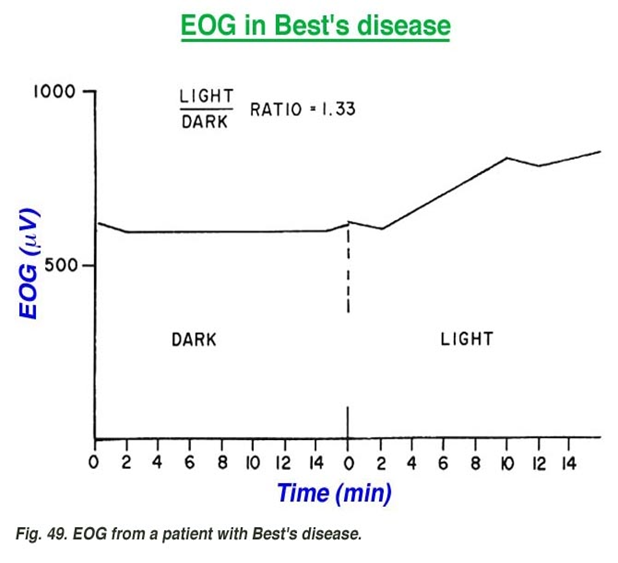
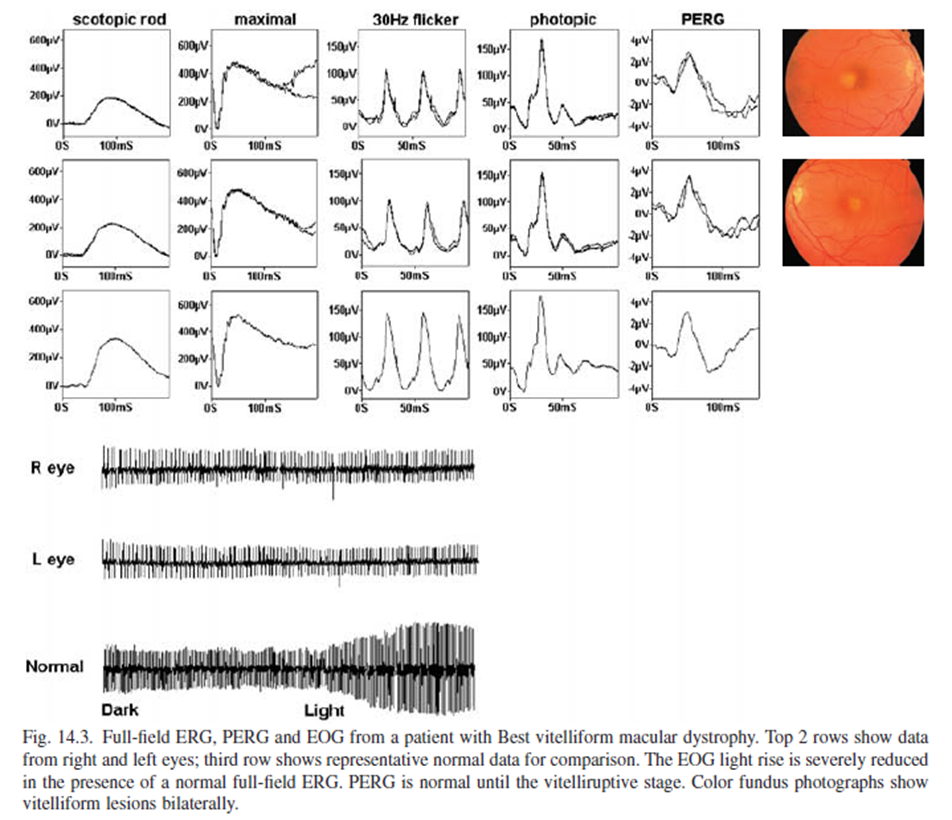
describe how best vitelliform macular dystrophy manifests in an EOG (5)
Integrity of RPE in affected in Best’s - can see in bottom image there is no light rise of RE/LE
Reduced light rise - not as steep as it should be
Therefore we have a reduced Arden ratio
ERGs appear normal in early stages
is an egg yolk appearance of macula - rods, cones and pattern ERG not affected
state what other conditions than an EOG can give us information about (4)
–Retinitis pigmentosa
–Diffuse RPE disease
–Stargardt's diease
–Chloroquine retinal toxicity
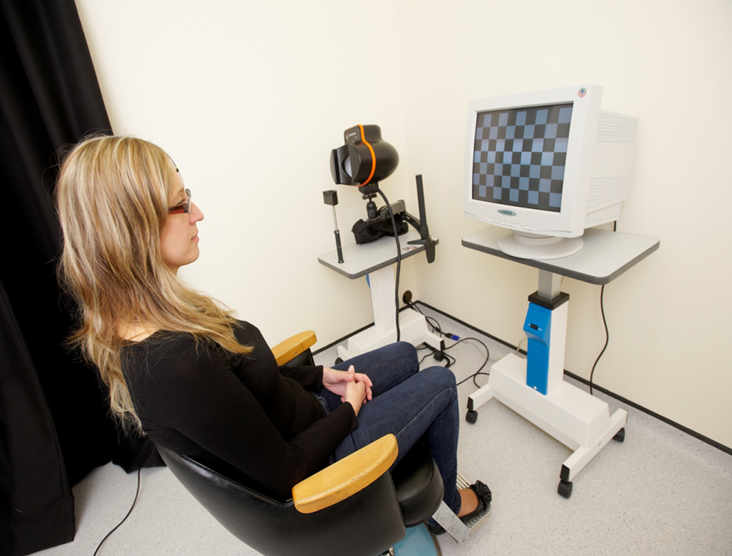
describe how VEPs work - visual evoked potentials (3)
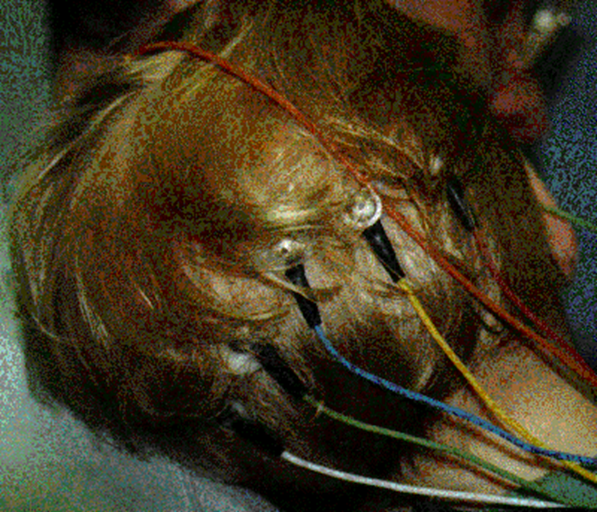
•Electrode is placed on occipital scalp adjacent to primary visual cortex - at the back of the head (unlike in EOG/ERG)
•A reference electrode is placed on a non-visual part of the brain.
•Stimuli - Pattern / Flash / checkerboard (which can be changed in size - helps us determine objective VA)
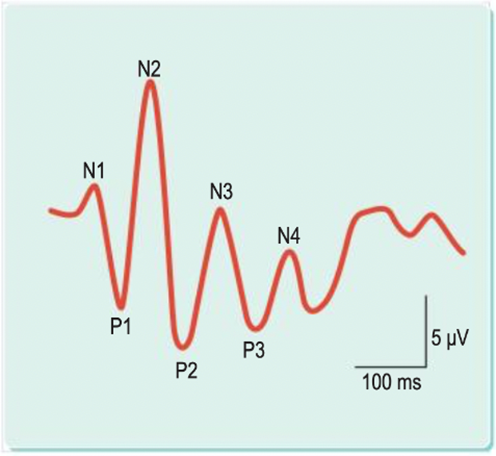
what does a normal flash VEP look like (3)
•Series of negative and positive inflections
•N1, P1 and N2 vary with age
•P2 found in almost all subjects ~120 ms
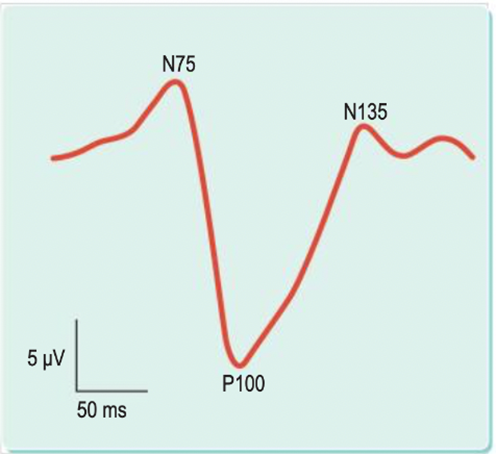
what does a normal pattern VEP look like (3)
•Negative Peak at 75 ms
•Large Positive peak at 100 ms
•Negative peak at 135 ms
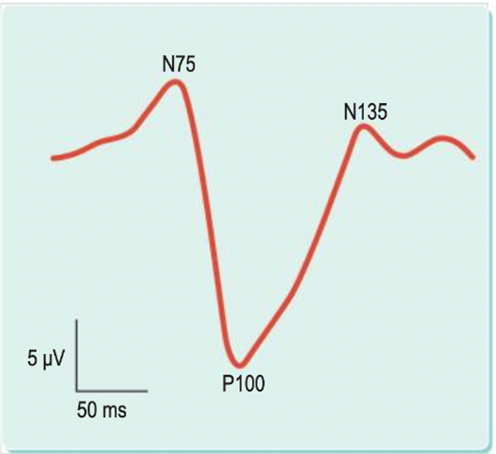
explain the P100 peak and factors that affect it (5)
Important factor as little variation between subjects over time or between eye
Factors that affect P100:
Pattern size
Contrast
Luminanc
Pupil miosis (size)
describe the uses of VEPs (4)
•Understanding the transmission Integrity of the visual pathway - E.g. Multiple Sclerosis
•Monocular stimulation - (one eye at a time and compare)
•Decussation anomalies - E.g Albinism
•Objective assessment of visual acuity - good for infants and px with functional vision loss (px with PTSD - everything is fine physically but something else has affected their vision)
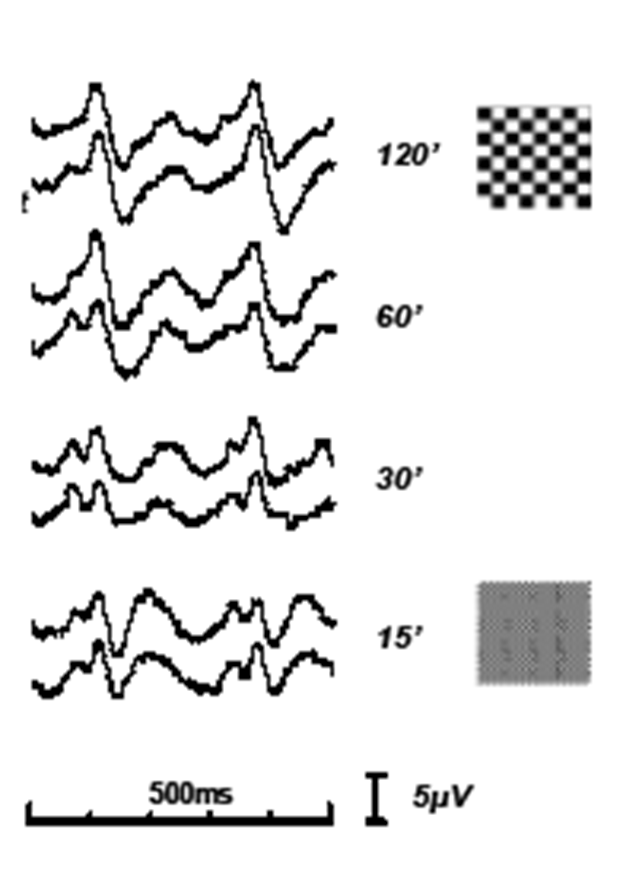
describe the use of VEP in an Objective VA assessment (3)
Can be used in cases of functional vision loss
Pattern has been presented twice over 500 ms - over a number of different checkboard patterns
This patient has good visual acuity - getting characteristic P100 and is = in both eyes - visual system is able to recognise the patterns at all these seconds of arc
describe use of VEP in Multiple sclerosis (4)
Demyelination - optic neuritis and MS
Compression - thyroid eye disease
Transmission delays - MS slows the response - getting P100 in both eyes - but it is delayed in the LE (as LE is the one with optic neuritis)
Pattern VEP latency changes
what is albinism and state the different types (4)
Hypopigmentation - reduced pigment compared to normal levels
Can either affect: Just the eyes - Ocular albinism
Eyes and skin - Oculocutaneous albinism
Ocular albinism more difficult to diagnose
describe tyrosinase-negative oculocutaneous albinism (4)
Complete albinism
Usually, AR inherited
Incapable of synthesizing any melanin
So px has White hair and very pale skin
what are the ocular signs of Tyrosinase-negative (5)
–VA usually <6/60 (due to foveal hypoplasia)
–Nystagmus – Pendular, Horizontal
–High refractive errors, strabismus, no stereopsis
–Choroidal vessels easily seen due to fundus lacking pigment (melanin)
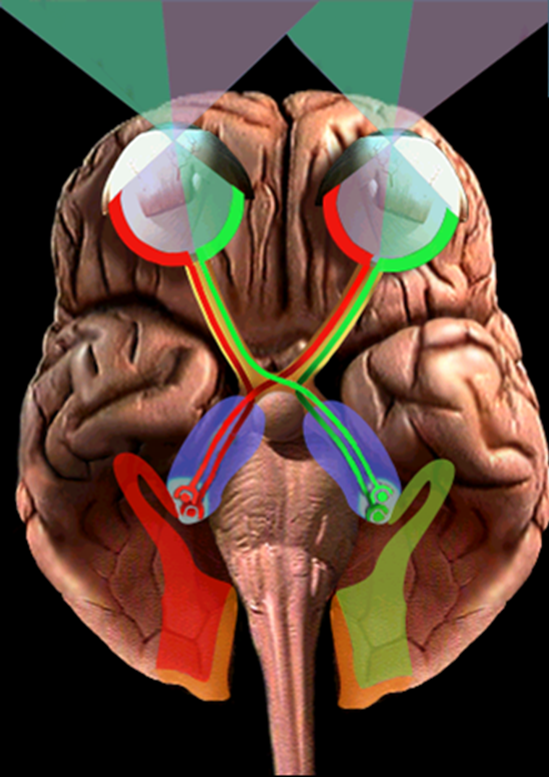
–Optic Chiasm has increased crossing of nerve fibres - This can be detected using Visual Evoked Potentials
describe tyrosinase-positive oculocutaneous albinism (5)
Incomplete albinism
Usually, AR inherited
Capable of synthesizing variable amounts melanin
Patient hair may be white, yellow or red and pale skin at birth, darkens as they get older
this type is more difficult to diagnose as it isn’t as obvious
what are the ocular signs of Tyrosinase-positive (2)
–VA impaired due to foveal hypoplasia.
–Iris - May be blue or dark brown with variable translucency - check with retro illumination
describe what ocular albinism is (2)
•Normal skin and hair.
••Usually X-linked inheritance but can be AR in some cases.
what are the ocular signs of albinism (6)
Light iris and/or iris trans-illumination (retro-illumination of fundus)
Foveal Hypoplasia
Nystagmus
Strabismus
Amblyopia
Increased decussation (crossing) of retinal nerve fibres
describe the set up for testing for albinism with VEP (2)
–A range of electrodes are placed across the occipital lobe (including reference electrode placed on non-visual part of brain)
–Lateral and centrally placed
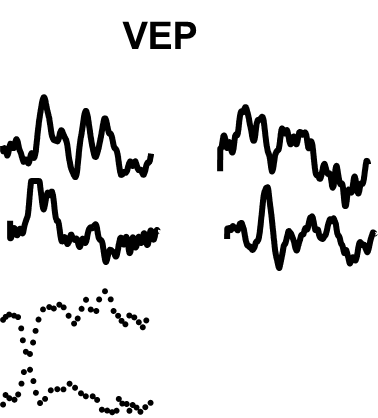
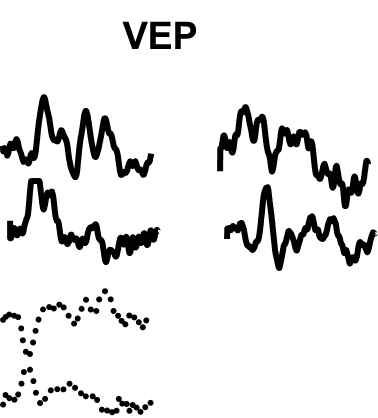
VEP in a normal left + right eye
•One eye is stimulated at a time.
•The response from each hemisphere is measured
•The differences at subtracted
•Should be left with a fairly flat response - should be symmetrical
VEP RE + LE - albinism ()
Stronger Contralateral Response - Earlier signal
Weaker Ipsilateral Response - Later signal
average is no longer flat between the 2 signals
Occurs due to increased crossing of nerve fibres at optic chiasm.
crossed asymmetry - albinism (2)
get a mirror image of the average responses together
asymmetry between the 2 eyes
case history example
Female, age 12, attended with brother
Both with Pigmentary macular changes
ERG and EOG - normal response
Both children very fair and observed to have nystagmus
Marked crossed asymmetry
Probably due to albinism
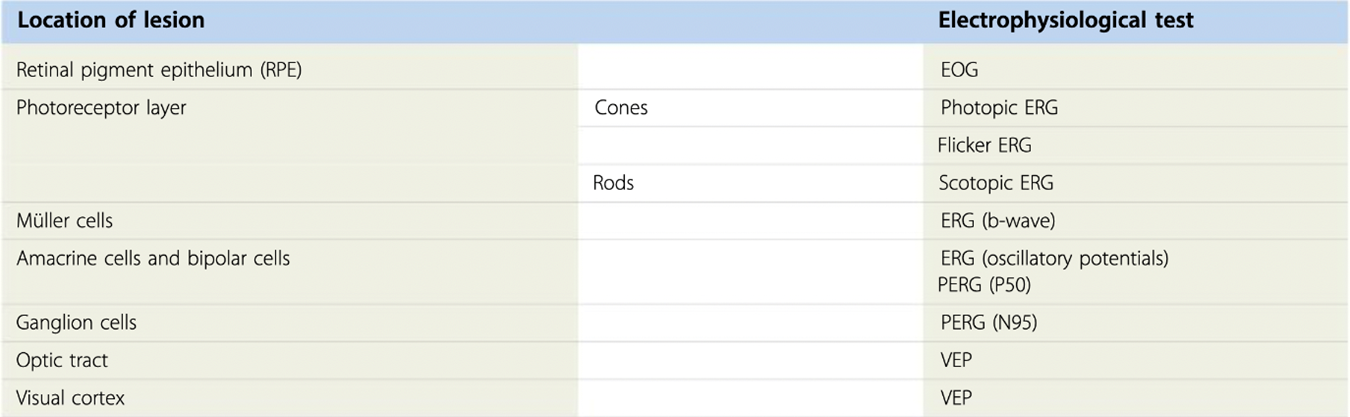
summary table