Developmental Psych
1/121
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
122 Terms
How to define normal (typical) versus abnormal (atypical)?
1. Normal as absence of disorders
2. Normal as statistical average
3. Normal as an ideal or desired state
4. Normal as successful ‘adaptation’
Normal as absence of disorders
Normal: positive quality of life; function well in different contexts; free of disabling symptoms of psychopathology
Abnormal: negative quality of life; function poorly; symptoms that form a recognizable pattern (syndrome) of psychopathology, fitting a clinical classification
Mental health perspective (P&T)
Normal as statistical average
Normal: behavior that occurs in the majority of the population
Abnormal: behavior that occurs in a minority of the population
Statistical deviance (P&T)
Normal as an ideal or desired state
Normal: meeting social-cultural standards of healthy psychological development
Can be age-related, gender-specific, or culture-relevant expectations
Abnormal: not meeting those standards
Sociocultural norms (P&T)
Normal as successful ‘adaptation’
Adaptation: ability of a person to adapt to his or her environment
Normal: successful adaptation (adequate or optimal); one can deal effectively and flexibly with various possibilities and difficulties that arise in everyday life
Abnormal: poor adaptation
Psychopathology
Refers to intense, frequent, and/or persistent maladaptive patterns of emotion, cognition, and behavior (P&T)
Developmental psychopathology
These maladaptive patterns occur in the context of typical development and result in the current and potential impairment of infants, children, and adolescents (P&T)
Developmental epidemiology
Research into frequencies and patterns of disorders
Prevalence
Proportion of a population with a disorder (number off current cases)
Incidence
The rate at which new cases arise (all new cases in a given time period)
Stigma
Is composed of stereotypes, prejudice and discrimination
Multiple levels: public, personal and self-stigma (or internalized stigma)
Can be harmful, and may prevent seeking help
Do we reach all children that need help?
Of children with problems, only 20% receives formal guidance and 35% support through informal services (teacher etc.), Zwaanswijk Others (2006)
Barriers to mental health care
Perceptions of mental health and child welfare (e.g., lack of confidence in the system, previous negative experiences, stigma)
Perceptions of psychological problems (e.g., denial, beliefs that difficulties resolve over time)
Structural (e.g., long waiting lists, high personal cost)
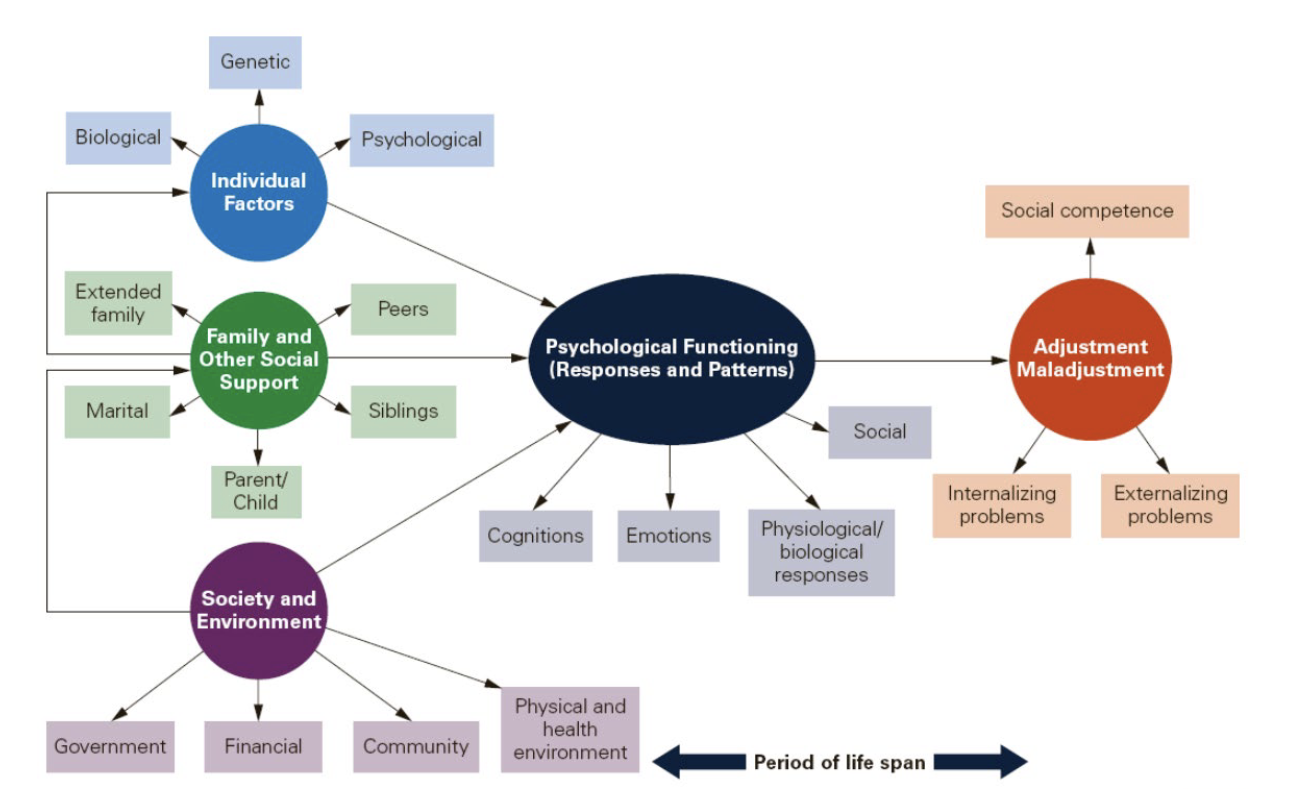
Theoretical explanatory models
Physiological models
Psychodynamic models
Behavioral and cognitive models
Humanistic models
Family or systemic models
Sociocultural models
Physiological models
Physiological (i.e., genetic, structural, biological, or chemical) basis for psychological processes
Brain development
Pruning: competitive loss of synapses – use it or lose it
Fewer, but stronger and faster pathways
Experience-dependent plasticity
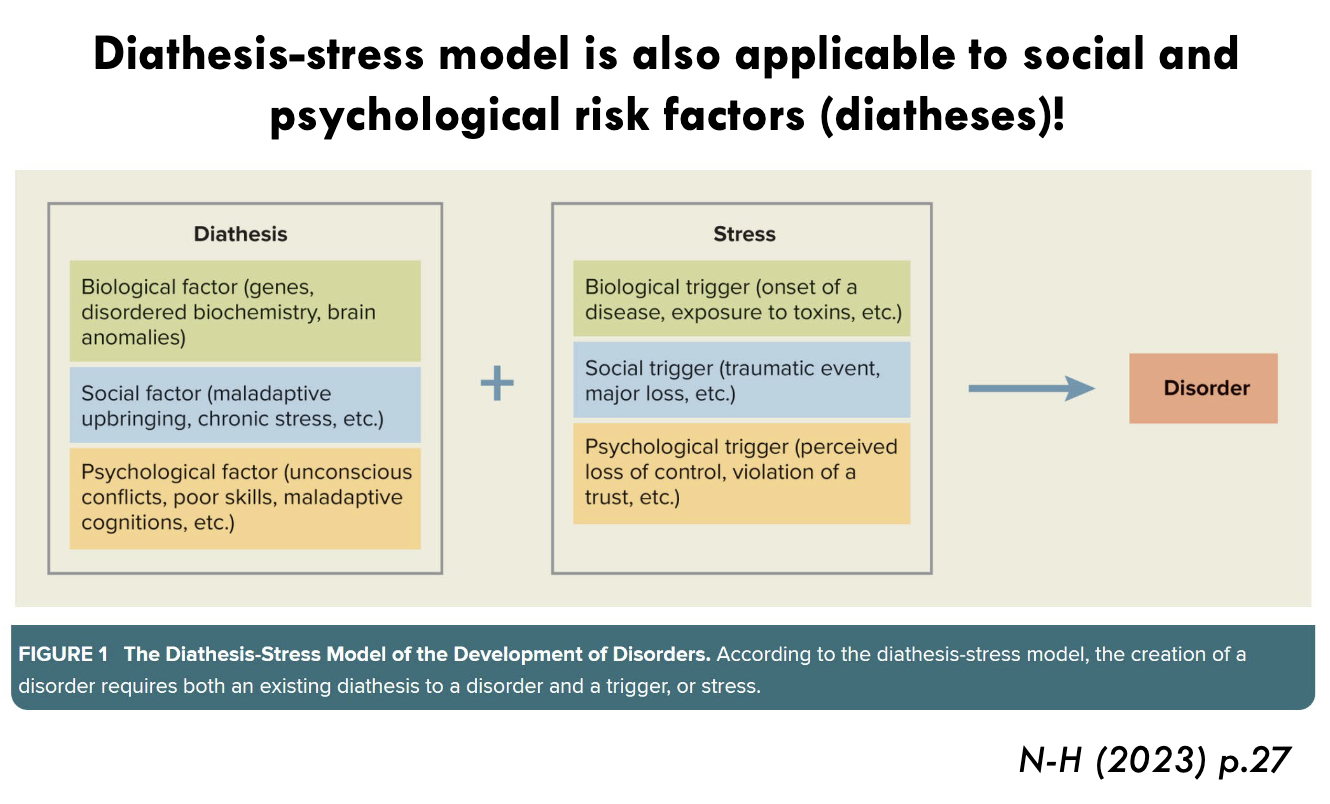
Interactions with environment
Diathesis (predisposition): physiological vulnerabilities (e.g., genetic)
Stress: physiological or environmental
The interaction may lead to the development of a disorder
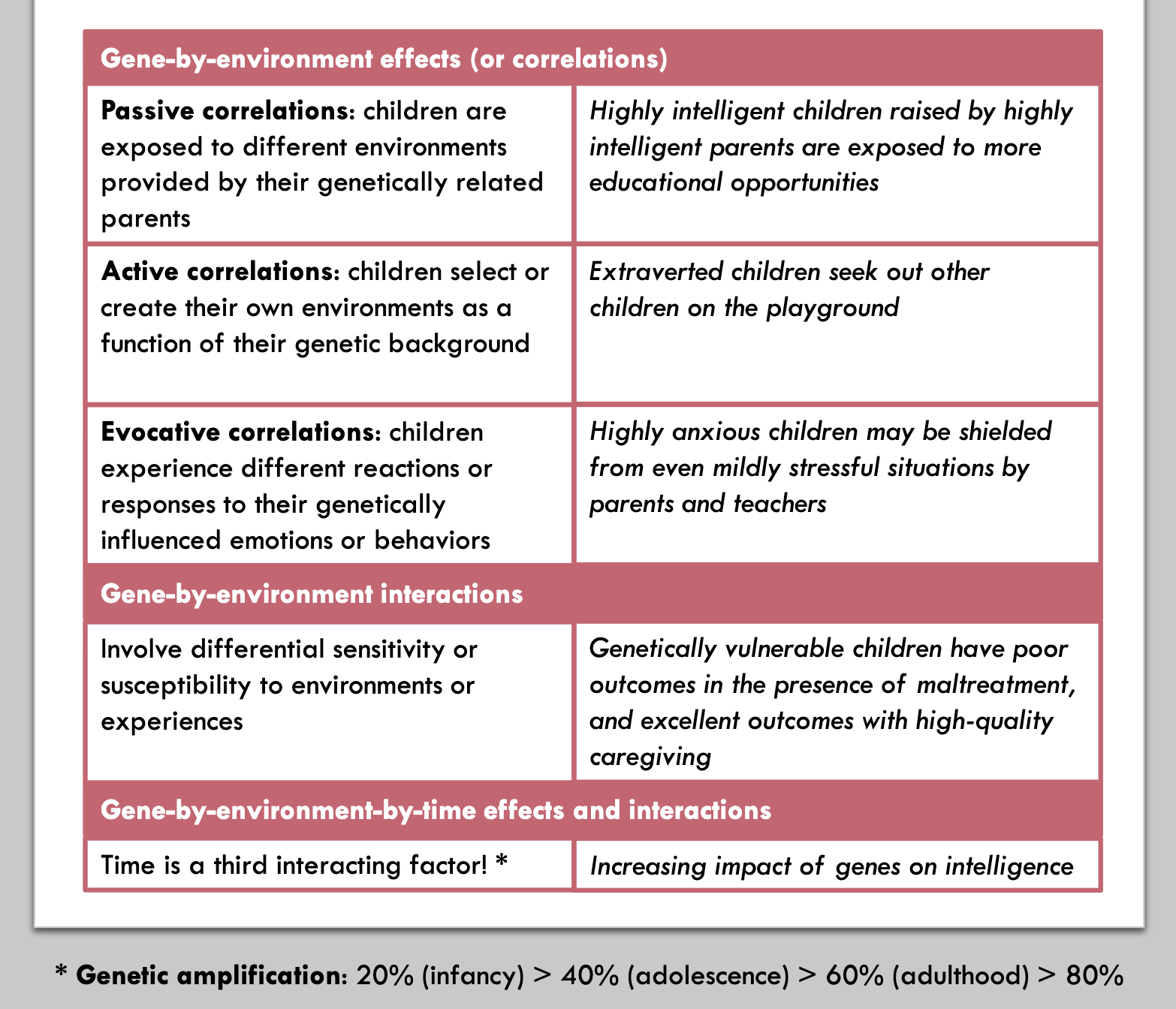
Gene by environment effects and interactions
(1) All psychological traits are genetically influenced
(2) No traits are 100% heritable
(3) Genetic impact is caused by many genes with small effects
(4) Environment matters
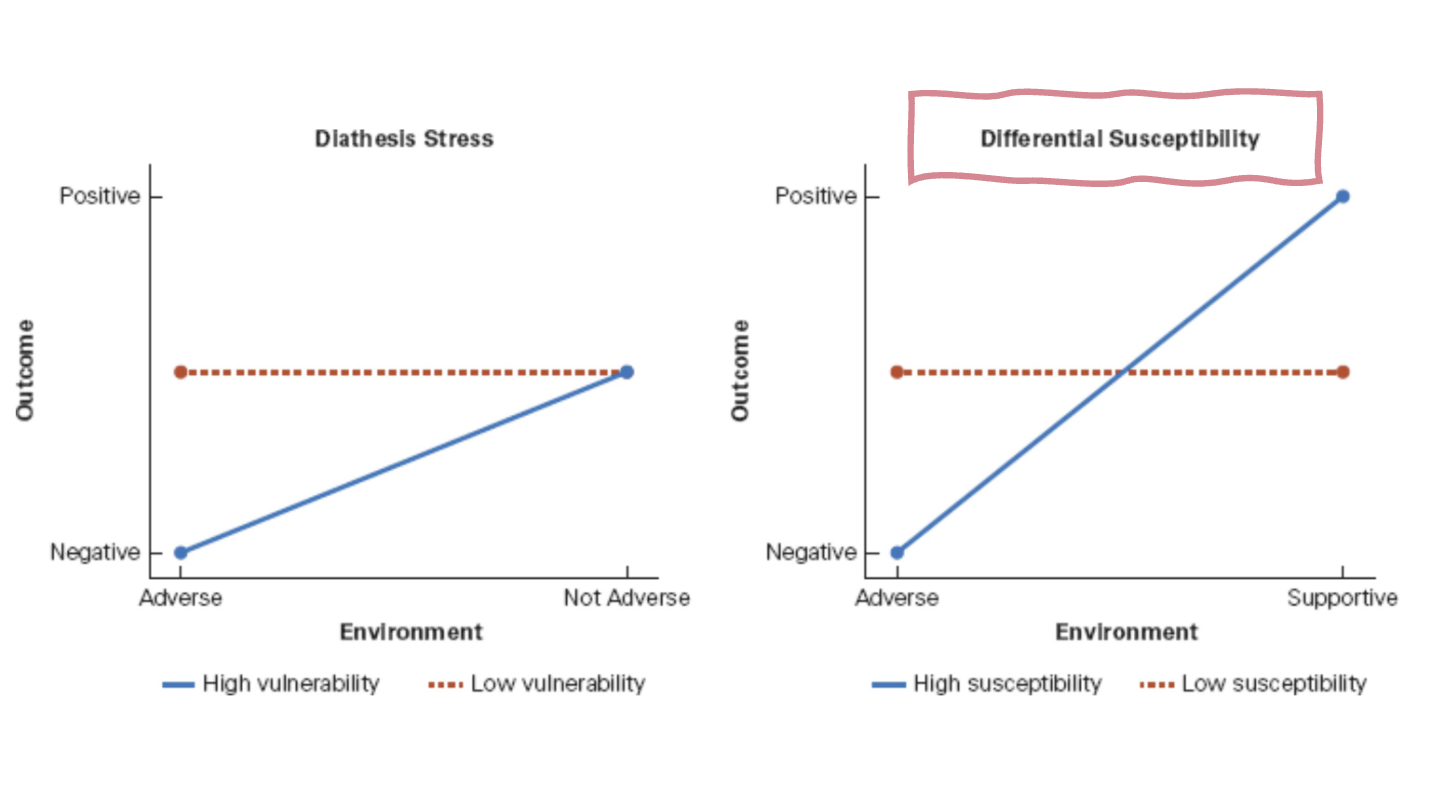
Diathesis-stress model vs. Differential Susceptibility
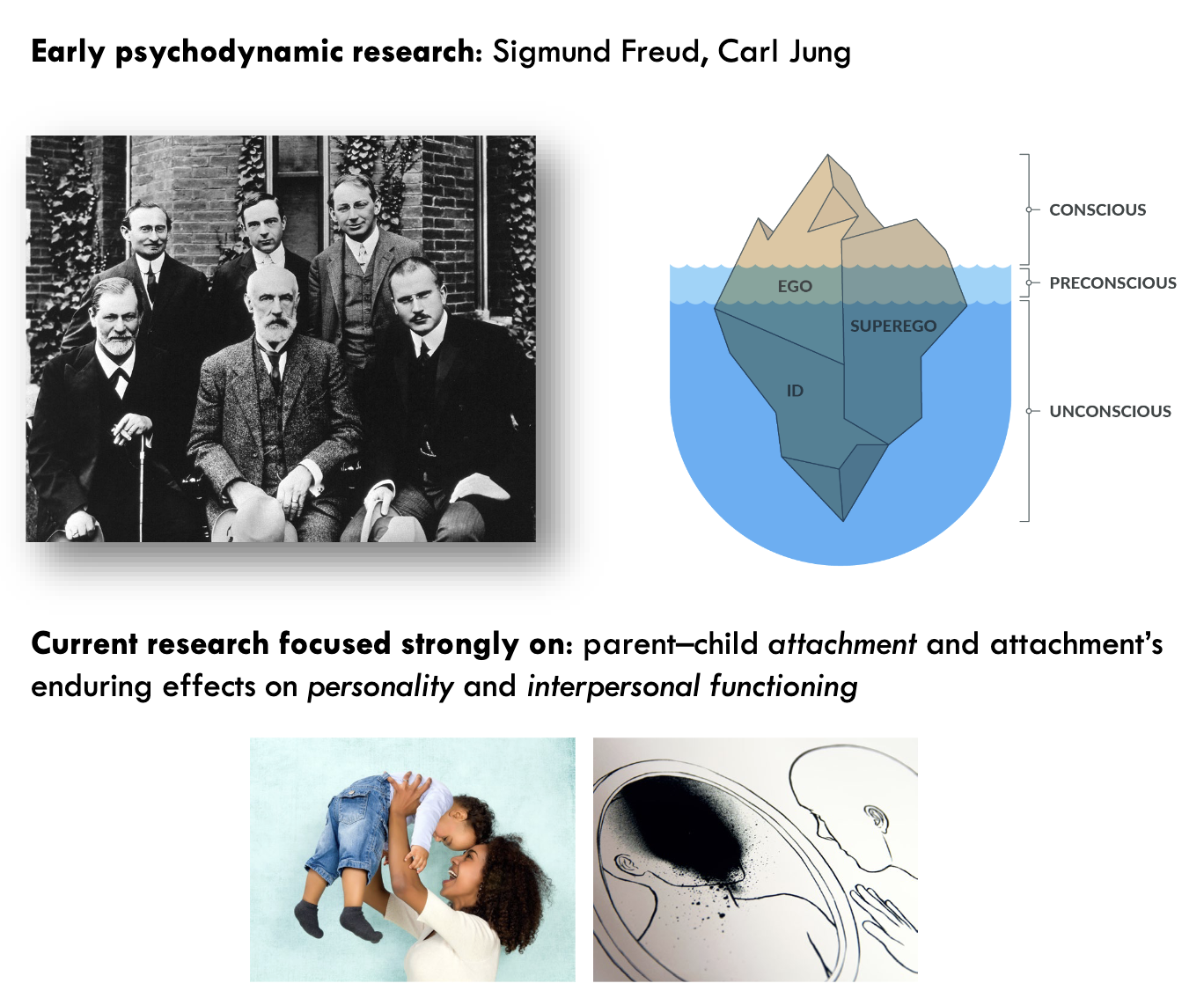
Psychodynamic models
Early psychodynamic models were scientifically dubious…
Contemporary psychodynamic models:
Unconscious processes
Mental representations of self, other and relationships
Subjective experiences
Origins of (a)typical personality in early childhood (developmental challenges)
Behavioral and cognitive models
Behavioral models: environment has powerful effects on development of personality and psychopathology
A(typical) behaviors are acquired via learning processes (e.g. reinforcement)
Cognitive models: focus on processes of the mind and cognitive development (e.g. stages Piaget, Vygotsky)
Cognitive behavioural therapy (CBT): manage problems by changing the way someone thinks and behaves
Humanistic models
Emphasizes personally meaningful experiences, innate motivations for healthy growth, and the child’s purposeful creation of self (e.g. Maslow)
Contrasts with psychodynamic models (conscious versus unconscious, positive versus negative human traits)
Psychopathology: interference / suppression of these needs
Family or systemic models
Understanding of personality and psychopathology of the child based on family dynamics
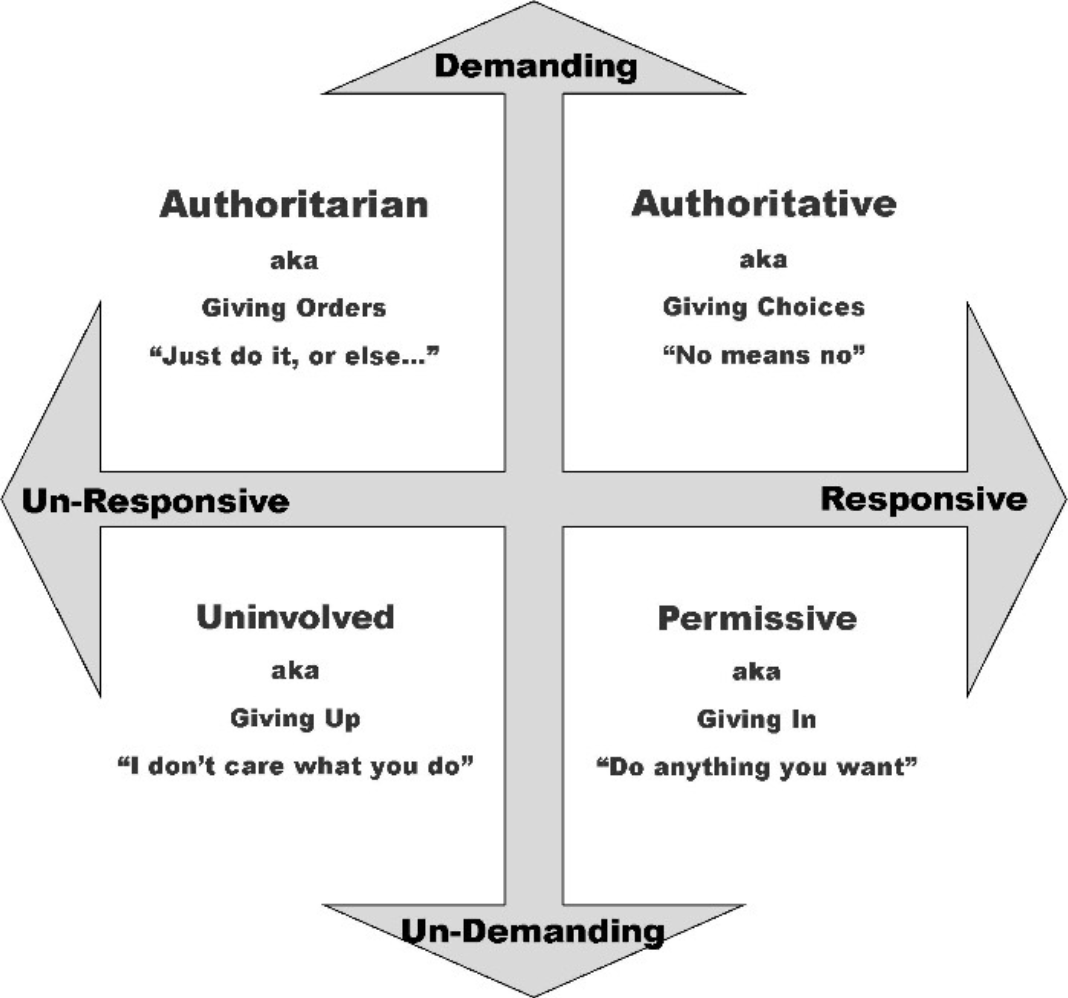
Topics: family type, parenting styles, parent-child relationship, sibling relationship
Shared and nonshared (unique) surroundings of siblings
Diagnostics and therapy focus on the child within the family setting
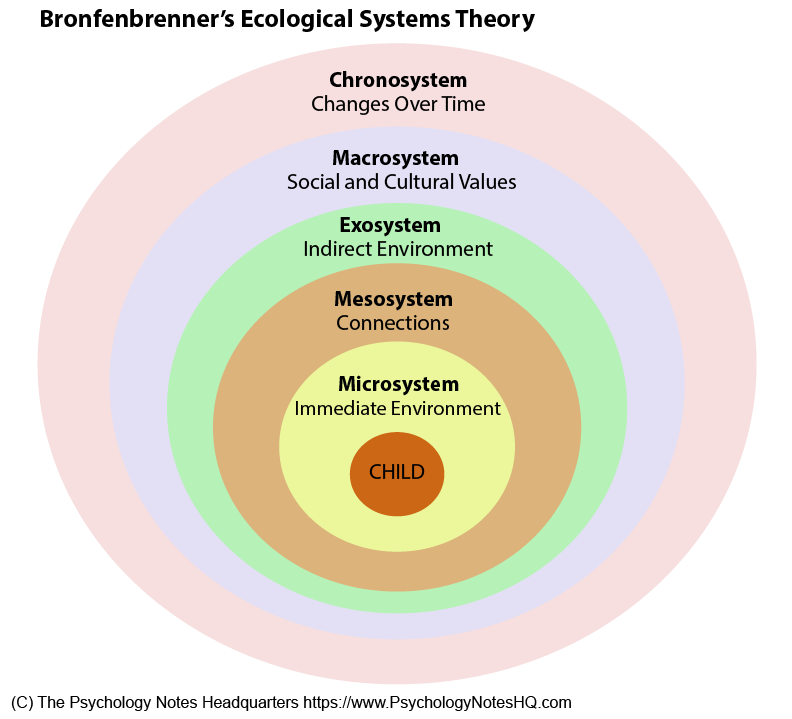
Sociocultural models
Culture is not only the background for development; rather, it is a major influence on development itself
Examples: gender, ethnicity and socioeconomic status
Settings of ecological models include home, classroom, neighborhood (embedded in meso, exo, macro and chrono* systems)
*birth cohort (share key experiences and events)
Developmental psychopathology is not associated with a single point of view or model
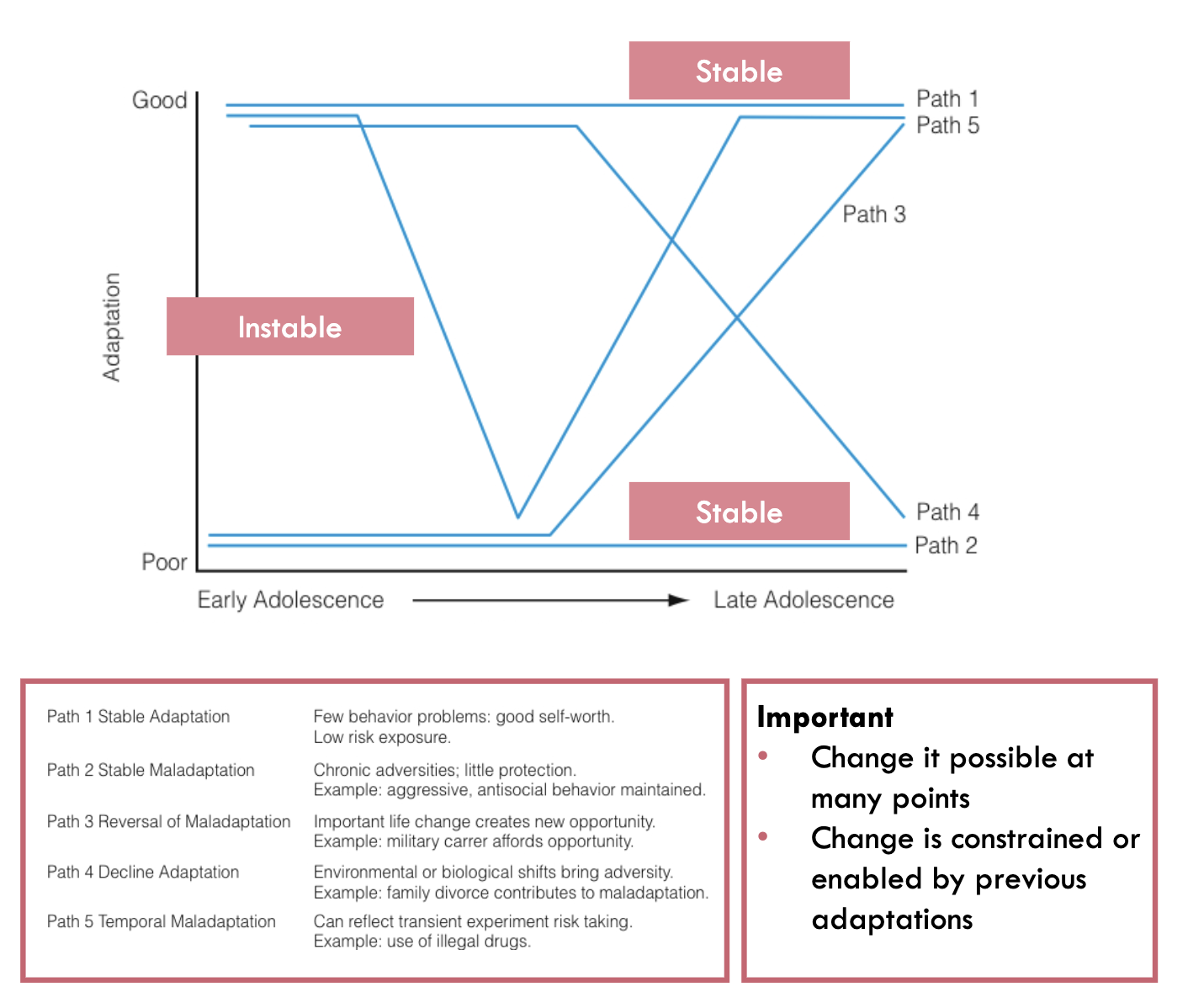
Developmental pathways
Adjustment and maladjustment are points or places along a lifelong map
Some pathways are associated with psychopathology with high probability, others with low probability
Continuity and discontinuity refer to the overall group level of a characteristic or behavior
Stability and instability refer to the relative ordering of individuals compared to peers
Coherence: beginnings may be logically linked to outcomes if we carefully evaluate the variables that lead to stability as well as the variables that lead to change
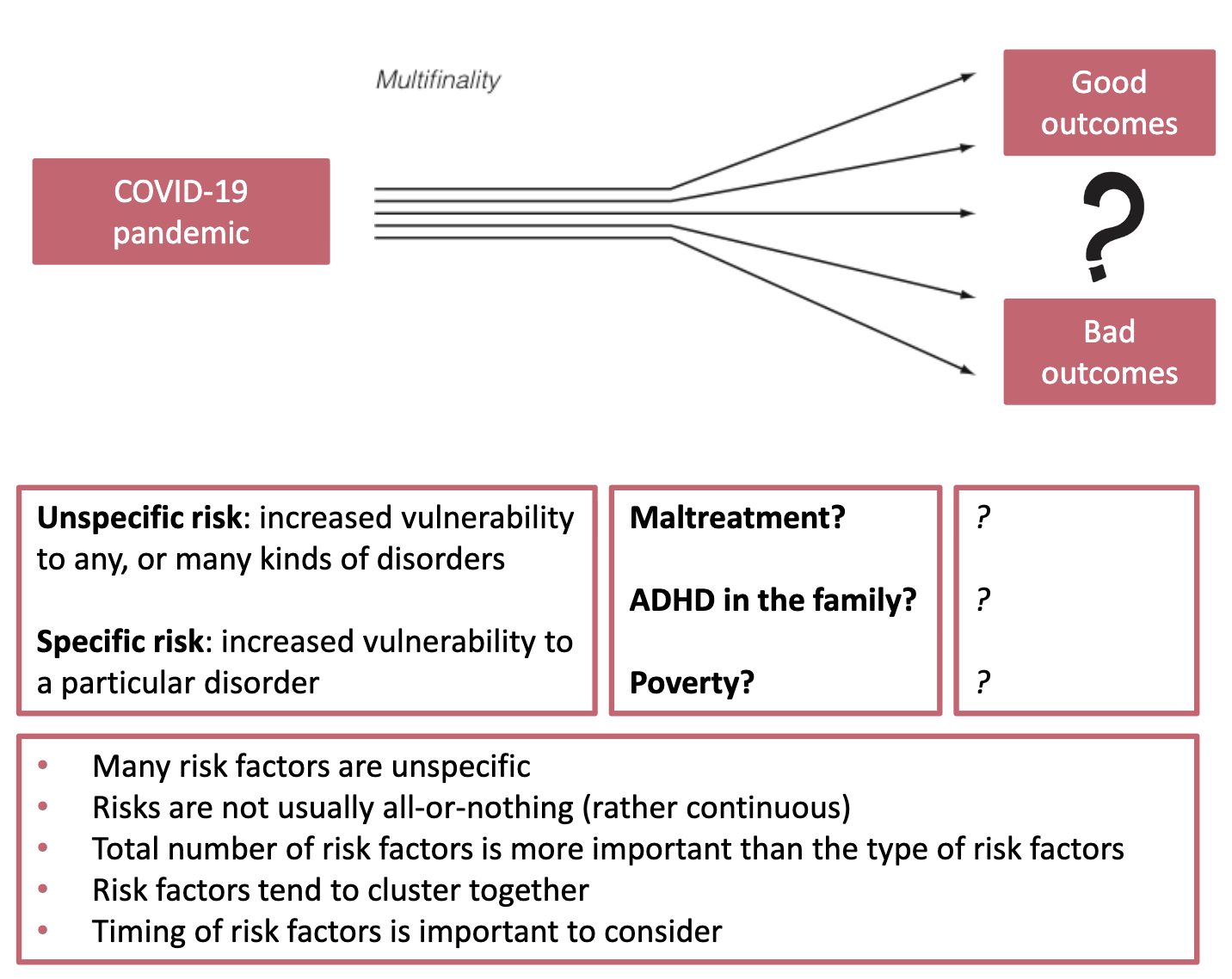
Equifinality and multifinality: same initial conditions lead to various outcomes, and vice versa
Competence and incompetence
Competence: effective functioning in important environments
Similar constructs: arenas of comfort, spaces of relative calm
All children, with and without disorders, display domains of competence and incompetence
Risk and protective factors
Risk: increased vulnerability to disorder
Risk factors: the individual, family, and social characteristics that are associated with this increased vulnerability
Resilience: adaptation (or competence) despite adversity (better-than-expected functioning)
Protective factors: the individual, family, and social characteristics that are associated with this positive adaption
Protective factors influence children’s outcomes by
reducing the impact of risk
reducing the negative chain reactions that follow exposure to risk
serving to establish or maintain self-esteem and self-efficacy
opening up opportunities for improvement or growth
Infant mental health consist of
1. Physiological functioning
2. Temperament
3. Attachment
Physiological functioning: 3 biobehavioral shifts in the first year
1. Rhythmic routines of feeding, dressing, comforting
2. Communicating feelings and intentions through gestures and vocalizations
3. Exploring the environment by crawling, walking etc.
Disturbances
Pica: ingestion of nonfood substances, such as paint, pebbles or dirt
Rumination: repeated regurgitation of food
Avoidant/restrictive food intake disorder: limited appetites, severe selectivity of food, or fear of feeding
Sleep-wake disorders: insomnia, disorders of arousal, nightmare disorder
Physiological functioning: Disturbances with food intake
When is it a problem and when a disorder?
Disorder: inefficient and ineffective feeding pattern
No experience of hunger and relief from hunger*
Developmental delay in feeding routine due to neglect**
Aversive experiences with feeding (e.g., illness, force)
Role of the caregiving environment
Increase in difficulties related to amounts of food, choices of food, and mealtime behaviour that are not solved
Worrying, frustration of the caregiver often increase the feeding problems
Feelings of personal incompetence and anger towards the child increase stress
Possible treatments:
Empirically supported behavioural interventions and also attention for relational issues
Physiological functioning: Disturbances with sleeping
When is it a problem and when a disorder?
Disorder: marked and persistent difficulties settling down and falling asleep, as well as maintaining sleep through the night, associated with impaired daily functioning
Insomnia: difficulties falling and staying asleep
Disorders of arousal: sleep terrors or sleepwalking
Nightmare disorder
Problem:
10-30% problems in families with typically developing young children
Risk factors:
Child: individual differences in the ability to self-regulate and self-soothe
difficult temperament
medical condition
insecure attachment
Parents: reinforcing
maladaptive patterns
insensitive caregiving
anxiety/ depression
marital difficulties
Temperament (child)
There are individual differences in:
Reactivity: Infant’s excitability and responsiveness
Regulation: What the infant does to control its reactivity
Temperament traits / big five
Surgency / extraversion: sociability and positive emotionality
Negative affectivity / neuroticism: predispositions to experiences of fear and frustration/anger
Effortful control / conscientiousness attempts to regulate stimulation and response
Well-adjusted: access to the full range of positive and negative emotions as well as mild, moderate and strong intensities of experience
Parenting dimension with large impact on temperament
Warmth: connected to the child’s social and emotional needs
Positive and negative control: connected to the child’s need for autonomy and self-regulation
→ Adding or reducing stress for the child?
If parents react to a stressed child with adding more stress without repairing this, it may result in toxic stress responses, with overactivation of the body’s stress response
Goodness of fit: match and mismatch
Interplay between infant temperament and parenting:
easy-going baby with easy-going parents
or fearful baby with strict parents
Two lessons:
1. In any infant-caregiver pair there are matches and mismatches; growth by ‘match-mismatch-repair’ cycles (shy children benefit from moderate challenges).
2. Extreme mismatches are problematic for children who are more susceptible due to their temperament (differential sensitivity)
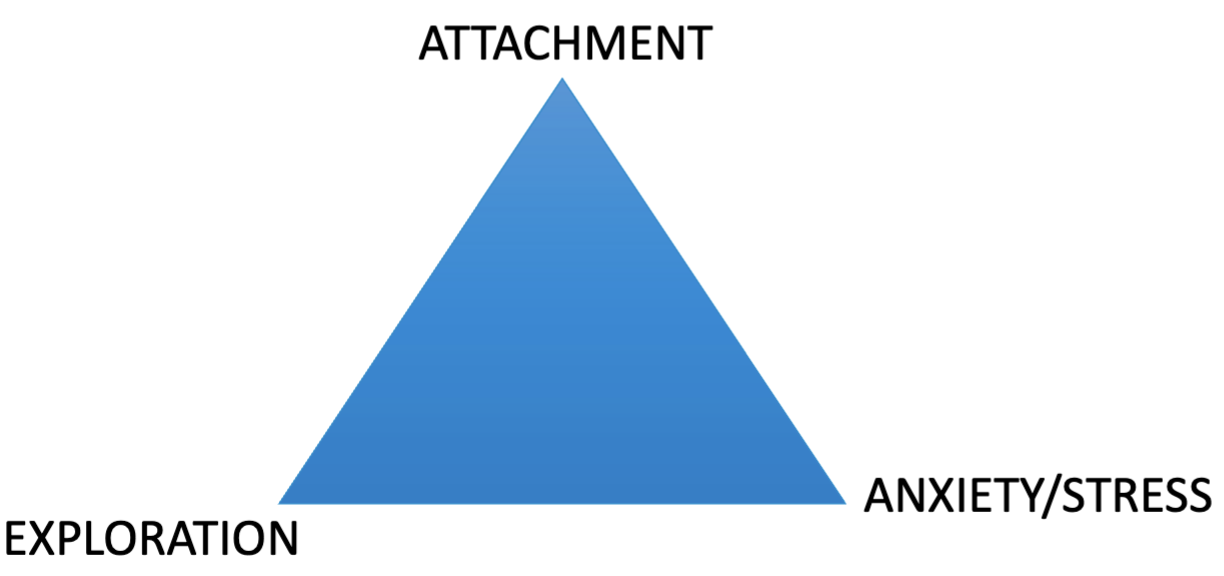
Two central hypotheses of attachment theory
1. Individual differences in the quality of infant-caregiver relationships are largely the product of the history of interaction with the caregiver
2. Variations in attachment quality are the foundation for later individual differences in personality
Problem of continuity over time
Are these different reactions or is there continuity in behavior?
What are (attachment) patterns of emotions, behavior and social interactions in context and over time?
Organisational perspective
Development is characterised as changes in behavioral organisation (including emotion and cognition)
Qualitative differences in behavioural organisation build on previous adjustments
Relations between early development and later outcomes are probabilistic and in continuous interaction with complex developmental processes and systems
Stability/coherence over time vs. changes in support/expectations?
Developmental tasks at the end of first year of life
Development of attachment relationship: experiences of safety, comfort and affection
Development of a rudimentary sense of identity / self: earliest set of cognitions and emotions focused on the infant as a separate being
Basic understanding of others and the world: early ideas about unfamiliar adults and children, along with new situations
4 attachment patterns: Based on behaviour of the child
Secure
1. Secure attachment
Insecure or anxious
Organized:
2. Resistant / anxious / ambivalent attachment
3. Avoidant attachment
Disorganized:
4. Disorganized / disoriented attachment
Secure attachment and caregiving history
The caregiver often responds sensitively, consistently and appropriately to physical, emotional and social needs of the child
More cooperative interactions between parent and child.
Regulation pattern of child
Deeply rooted sense of safety and security
Rudimentary cognitions and emotions, such as:
Self: "I am worthy of care.“; “I am lovable.”
Significant others: "I can trust that you will respond to me in appropriate ways."
World: "The world is safe and pleasant."
Resistant / ambivalent attachment and caregiving history
The caregiver often responds inconsistently or unpredictable to the physical, emotional and social needs of the child
Lower levels of psychological awareness in mothers and developmental lags in infants
Regulation pattern of child
Basic sense of insecurity and uncertainty.
Rudimentary cognitions and emotions, such as:
Self: "I do not know if I am worthy of care/ being loved.“
Significant others: "I cannot trust that you will respond to me in appropriate ways.“
World: "The world is sometimes pleasant and sometimes unpleasant."
Avoidant attachment and caregiving history
The caregiver often responds with inadequate, intrusive or excessively controlling care to the physical, emotional and social needs of the child
“Psychological unavailability” in caregivers.
Regulation pattern of child
Basic sense of insecurity and unfriendliness
Rudimentary cognitions and emotions, such as:
Self: "I'm not worthy of being loved."
Significant others: "I can trust that you usually do not respond."
World: "The world is unfriendly and not responsive."
Cultural differences in attachment patterns
Avoidance is more acceptable in "Western" countries than ambivalence
Situational variations / reactions to novelty (Ambivalent vs. Avoidant)
Ambivalent: difficulty dealing with a novel, complex object; more hesitance; less flexibility; less effective in problem solving
Avoidant: no problems in handling novel objects; close physical and emotional encounters with peers are very challenging
Patterns of behavior:
Ambivalent: seeks help for smaller problems; asks for more nurturance as if they are younger than their actual age
Avoidant: seeks help / contact when stress is over; often disobedient; others often respond instructive and controlling, not nurturant
Disorganised attachment and caregiving history
The caregiver is perceived as frightening, frightened, or malicious
A pattern in which both approach and avoidance is typical
Regulation pattern of child
“Fright without solution": the caregiver is both a source of comfort and a source of anxiety.
Self, significant others, the world:
"The temporary collapse (or absence) of attention-, emotion-, and behavioral strategies when experiencing stressful situations. “
Prevalence: 15% non-clinical groups; 50-80% clinical groups
Disorganised attachment and later outcomes
Longitudinal data until the end of adolescence:
More symptoms and more severe symptoms of psychopathology (e.a. self harm)
Predicts dissociation or psychic collapse
Predicts the development of a conduct disorder
Predicts the development of a borderline personality disorder, sometimes in conjunction with avoidant attachment
Attachment and risk for development of (DSM) psychopathology
Secure attachment pattern:
protective factor: in problematic situations a person has more resilience to deal with them
Insecure-avoidant and insecure-ambivalent patterns:
higher risk for developing problems: not directly related to clinical disorders
Insecure-disorganised pattern:
strong predictor of subsequent psychopathology
Attachment disorders
Reactive attachment disorder (RAD)
lack of organised attachment behaviours, do not seek comfort when distressed and problems with emotion regulation (not easily soothed, excessively timid, hyper-sensitive)
Disinhibited social engagement disorder (DSED)
little if any reticence with unfamiliar others, do not look back to the caregiver while wandering off, social superficiality and attention seeking, sometimes inappropriate physical contact
DSM-5: in Trauma- and Stressor related disorders (with PTSD)
Similarities and contrasts: RAD and DSED
Similarities:
Social deprivation and neglect
Contrasts:
RAD more responsive to enhanced quality of caregiving than DSED
DSED more difficult to treat, "bottomless pit."
Risk factors for attachment disorders
Among other things:
Inadequate, inattentive, inconsistent and intrusive care
Psychopathology in parent
In children: difficult temperament, genetic vulnerability and neurological difficulties
History of extreme insufficient care (DSM-5 C):
1. Social neglect or deprivation
2. Repeated changes of primary caregivers
3. Rearing in settings that limit forming selective attachments
Prevention / intervention for attachment disorders
Preventive support for at-risk children and families:
Enhance positive parenting (STEEP, p. 83)
Attachment and biobehavioural catchup (ABC) (p. 83)
Placement in better caregiving environments (e.g., foster care; p. 81)
Interventions repairing unhealthy parent-child interactions:
Home visits and parenting education/ support (p. 82)
Infant-parent psychotherapy (p. 84)
→ Broad availability and easy accessibility of care
→ Growth towards more attachment security is possible
Historical perspective: Effects of the quality of the parents’ relationship on children
St. Augustine (354-430): "Peace in society depends upon peace in the family."
The family as an enclave; economic unit
Until about 100 years ago, violence against children and other family members was a private matter and was not or hardly considered criminal
Children were the property and responsibility of the father
Importance of adult intimacy for children
Their parent’s relationship is the first model of adult intimacy
From a very young age, children are acutely sensitive to the quality of the interaction of the adults around them.
Not only overt hostility predicts distress in children, but also signs that parents are disengaged or withdrawn from each other.
Appraisal of conflict
Primary appraisal
What is going on: good, bad or neutral?
Secondary appraisal
IF BAD: why is there a conflict, have I done something wrong?
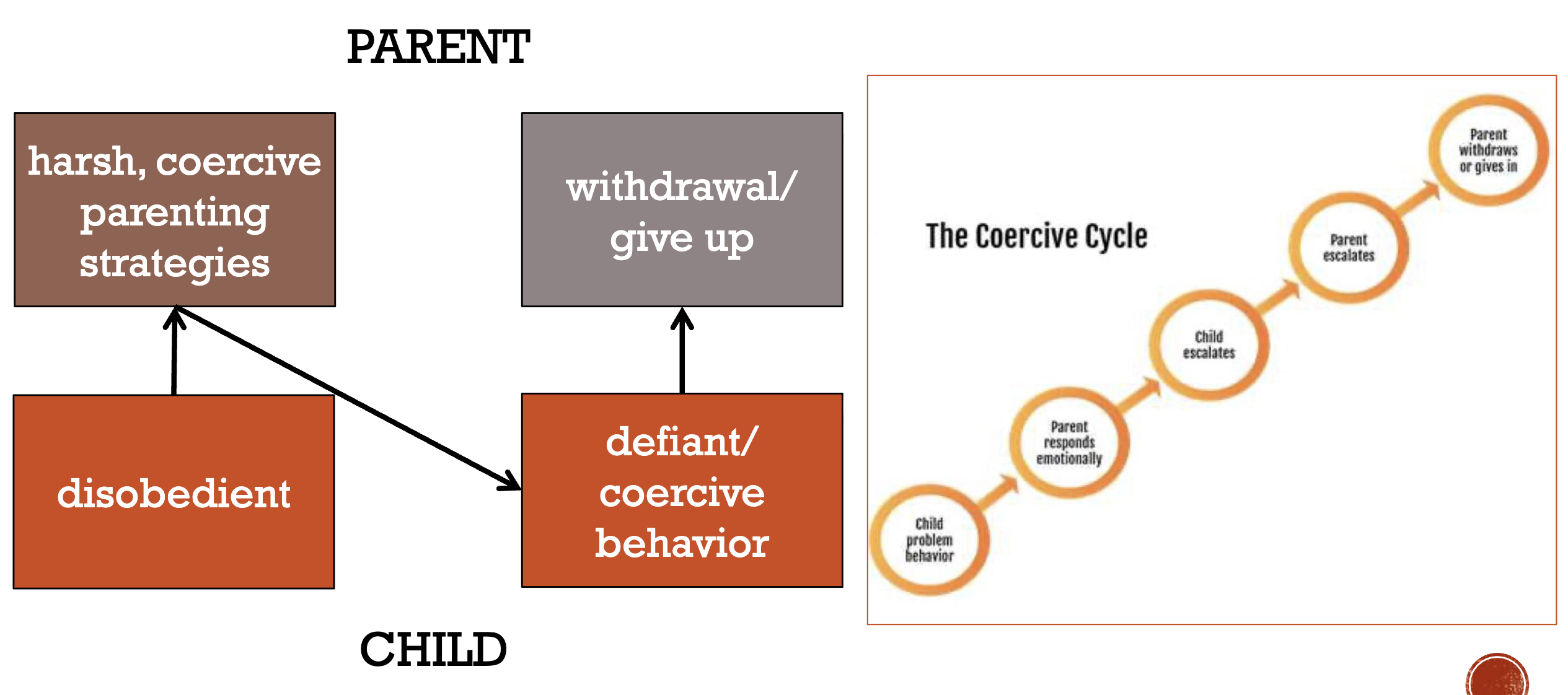
If the child’s behaviour does end the conflict, it will likely be repeated and reinforced → shaping models about attachment and intimacy
Learn how to handle stress within a family
High satisfaction between intimate partners is related to secure parent-child relationship and positive interaction in families
Secure relationship with mother + Many (unresolved) conflicts between partners = Emotional insecurity and stress for the child within the family
Dealing with conflicts between adults
Healthy conflicts between caregivers: resolved successfully
Normal: conflicts take place in each family, these are instructive.
Unbalanced conflicts: without a resolution
As a reaction, children often self-blame if the cause of parents’ behaviour is not identified resulting in:
pulling back, guilt, shame, fear, depressive symptoms.
a desire to intervene/mediate, angry, try to distract attention.
physiological responses (heart rate, blood pressure, skin reactions)
Child does not become accustomed to conflicts between adults.
Negativity between parents remains a stress factor
For the outside world, a child can show indifference
Sensitisation hypothesis
Desensitisation = becoming accustomed to conflicts/ arguments
Sensitisation = becoming increasingly reactive to exposure
A history of conflict reduces the threshold for the child to react negatively and increases reactivity to the conflict:
neuroendocrine system becomes increasingly vulnerable to stress
flight-or-flight response is activated quickly
Siblings: better off with or without?
More sensitivity to differential (parental) treatment and fairness
Development of theory of mind at an earlier age
Development of social competence through experiences of conflict and support to prepare for the complexities of an intimate relationship
What do they learn from siblings?
Negotiation or competition for toys
Playing together
Sharing attention from parents
Differences between siblings and peers
Defining features of friendships with peers:
voluntary
reciprocity
equal status
Consistent research results:
A strong bond with a friend can make up for a weak sibling relationships. Not the other way around!
Effects on social and emotional development:
Motivation for empathy
Shared imaginative play
Broader social network
Expectations about social status: acceptance or rejection from others
Social standing between peers
Sociometric testing = four categories of social standing based on the question to name who they like and dislike within the group.
popular | rejected |
controversial | neglected or socially isolated |
Adolescents and intimate relationships
Early adolescence
Clear distinction between intimate relationships and friendships.
Understanding of intimacy becomes more sophisticated
Often patterns repeat with siblings and friends:
Sroufe c.s.: strong continuity over 20 years (positive and neglected).
Conger c.s.: with supportive parents, also supportive and less hostile in interactions with romantic partners.
Specific experiences can affect the trajectory (e.g., abuse).
Transitions during adulthood
Cohabitation: Four groups of cohabiting couples
Precursor to marriage
Coresidential daters
Trial marriage
Substitute marriage
Parenthood
Early age, or at later age?
Stressful or well-managed?
Relationship satisfaction and family transitions
Decline in positivity after early stages, less affective expressions between partners
"Our brain is simply wired to take good things for granted." (B&K, p. 488)
Related to transitions of children from one age period to the next
Relationship satisfaction and attachment
Security = balance between autonomy and intimacy
Factors that influence the quality of intimate relationships
Four negative patterns that predict divorce:
criticism
contempt
defensiveness
stonewalling
Intimacy in later life
More older men remarry, women are 3x more likely to be living as a widow
The more disruptions, the less financial security and more risk of hearth disease, esp. for women
Not married in older adulthood does not mean without an intimate relationship
Specific life issues in later life
Mixed blessing of retirement
Widowhood
Loss of health, skills, social relationships, social roles
Relational problems/conflicts with children, partner, brothers/ sisters, others
Increasingly aware of mortality/discuss meaning of life
Timing of issues?
Early onset: arise earlier in life
Late onset: arise in late adulthood
Combination of early and late start
Autonomy in later life: how?
Having a say in matters and being able to keep this up
Active participation and contribution
Freedom of choice and the possibility to shape your own individuality
It is more than being autonomous, independent or in control
→ In later life, about 50% have psychological problems
Depression in later life
First physical symptoms, vague complaints
Subjective memory complaints
Masked by 'smile‘
Often undetected by ascribing the complaints to other potential causes
Potential tips for good (mental) health in later life
Check your blood pressure regularly
Lead a physically and socially active life
Invest in positive relationships (socioemotional selectivity theory):
Break up an unsatisfying relationship
Manage conflicts with more affection and less hostility compared to younger couples and strengthen positive feelings (including sexuality)
More time with close family members and friends
Pioneers in the autism research
Term ‘autism’ used by Bleuler (1911) to describe symptoms of schyzofrenic patients
Grunya Sukhareva (1925): the first psychiatrist to identify and pathologise autism.
Leo Kanner (1943): Autism
Hans Asperger (1944): Asperger’s Sydrome
Autism Spectrum Disorder in the DSM-5 is defined mainly by 2 domains
A. Deficits in social communication and social interaction, including:
Social emotional reciprocity
Nonverbal communication
Relationships
B. Restricted, repetitive behaviour and interests (>2):
Stereotypic or repetitive behaviour
Insistence on sameness
High restricted, fixated interest
Hyper- or hypo responsiveness
New in DSM-5 (regarding autism)
Sensory problems
Hyper- or hypo sensitivity
Severity levels
Level 1-requiring support
Level 2-requiring substantial support
Level 3-requiring very substantial support
PDDNOS / Asperger removed
Symptoms must be present in early development but may not fully manifest until later/masked
Prevalence
Prevalence 1-2%
Around 70% normal intelligence
Around 30% experience regression (loss of skills)
Females with Autism
In general: 20% - 25% females
Explanations:
Genes
Symptoms
Compensation
Clinician bias
Savant skills (e.g. Calendric memory)
10% of autistic individuals
Disharmonious IQ profile
Social subtypes (Lorna Wing)
The aloof
The passive
The unusual (odd)
Medical characteristics of autism
Epilepsia (± 25%)
Insomnia and sleep problems (± 60%)
Motor impairments (e.g. poor fine motor skills)
Gastrointestinal symptoms (± 45%)
No empirical evidence of connection between vaccinations and mercury (kwik) → Fraudulent Lancet paper (1998)
Assessment of autism
Current behaviour and Development
Observation
Parent interview
No biomarkers!
Treatment for autism
There is no ‘cure’ for autism
Focus on individual and environment
Customised care, Psychoeducation, Psycho/behavioural therapy, Fysio/speech therapy
Medication
Directed at co-occurring problems (anxiety, hyperactivity, rigidity)
Early intensive interventions (e.g. ABA)
Heated discussion, see recent NAR report
Neurodiversity
People experience and interact with the world around them in many different ways; there is no one "right" way of thinking, learning, and behaving, differences are not viewed as deficits
Medical Model → Social Model
What causes autism?
Short answers:
We don’t know, there is no single cause
We do know, it’s not the mothers fault and its not due to vaccination
Real answer:
Genetics, neurobiology
G x E (sensitivity to exposure)
rGE (liability to exposure)
Heredity of autism
Concordance rate:
Identical (Monozygotic) twins:
80% (100% shared genes, shared uteral environment)
Fraternal (Dizygotic) twins:
31% (50% shared genes, shared uteral environment)
Siblings:
20% (50% shared genes, no shared uteral environment)
Neurobiological explanations of autism
Growth
Abnormal brain growth
Too much growth in early development
Larger head circumference
Chemistry
Neurotransmitters (transmit signal)
Serotonine
Oxytocine
Reward system
Excitation/inhibition balance
Anatomy
No ‘characteristic’ brain structure found yet
Less neurons in lymbic system (amygdala, hippocampus) and
Cerebellum (movement, cognition)
Evidence: MRI, postmortem and animal studies
Activity
EEG: Brain waves (oscillations) → Some evidence for atypical activity during in specific regions during: perception faces, emotions, perspective taking
Need for studies on real-time interactions
Psychological explanations of autism
Central Coherence
Natural tendency to see connection between stimuli
Weak central coherence: focus on detail
Strong central coherence: focus on whole
Executive Functioning
Cognitive functions that regulate goal directed behaviour
e.g.: Mental flexibility, Planning, Working memory, Inhibition, Initiative
Emotional competence
Theory of Mind
‘The ability to ascribe mental states to people and to explain and predict behaviour in terms of underlying mental states’
e.g.: Perspective taking, Empathy, Reciprocity
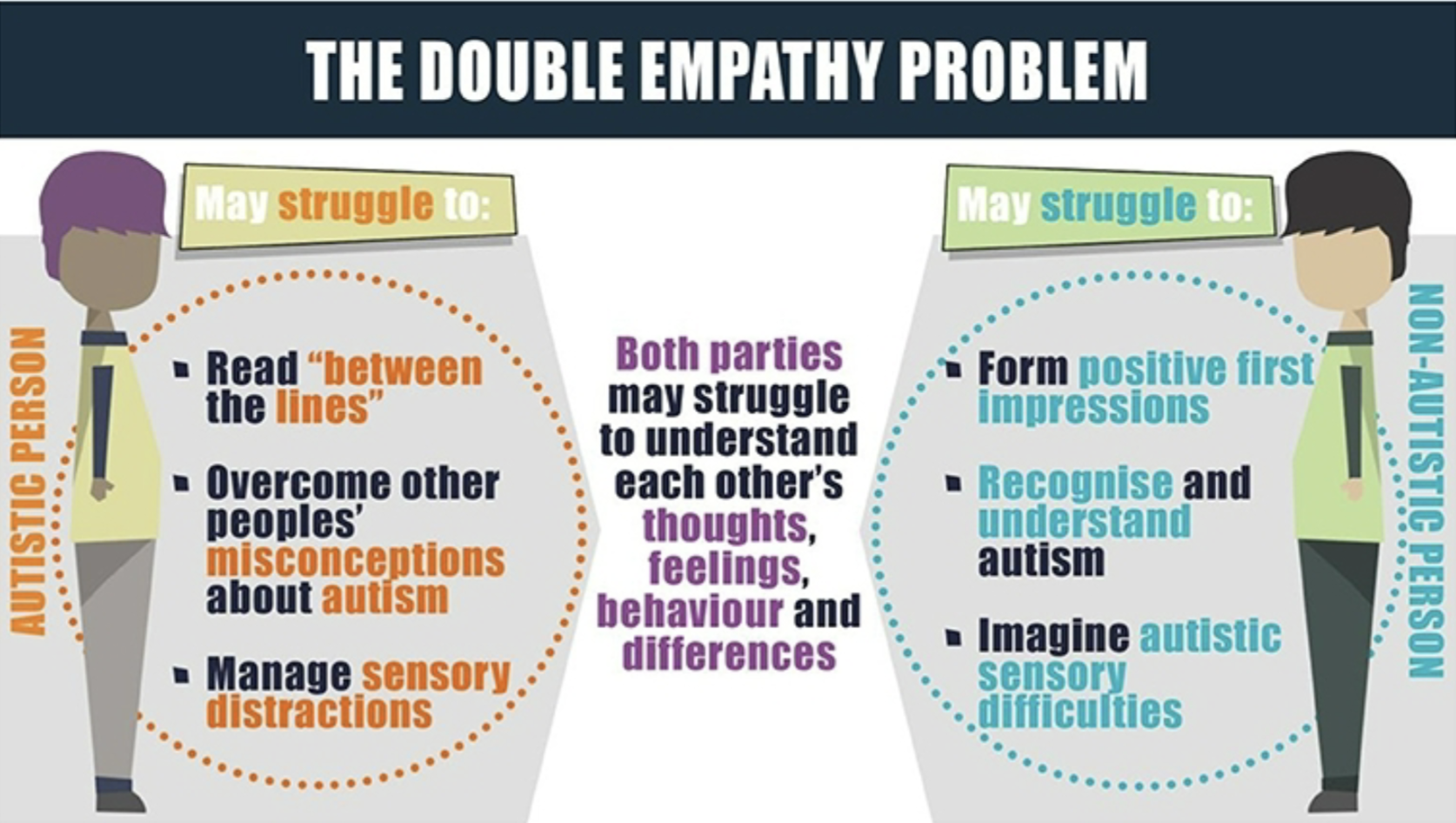
Double Empathy
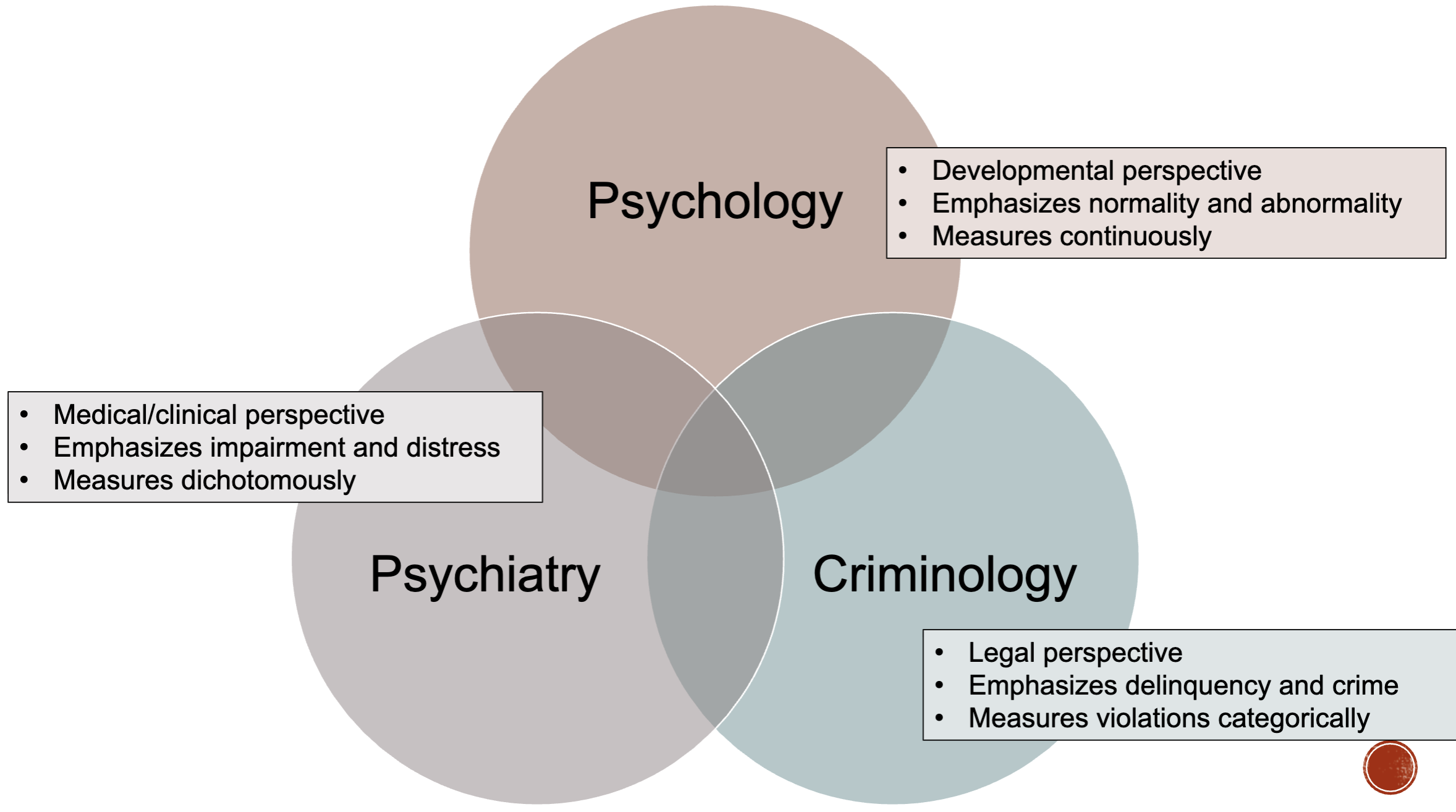
Psychology vs. Criminology vs. Psychiatry
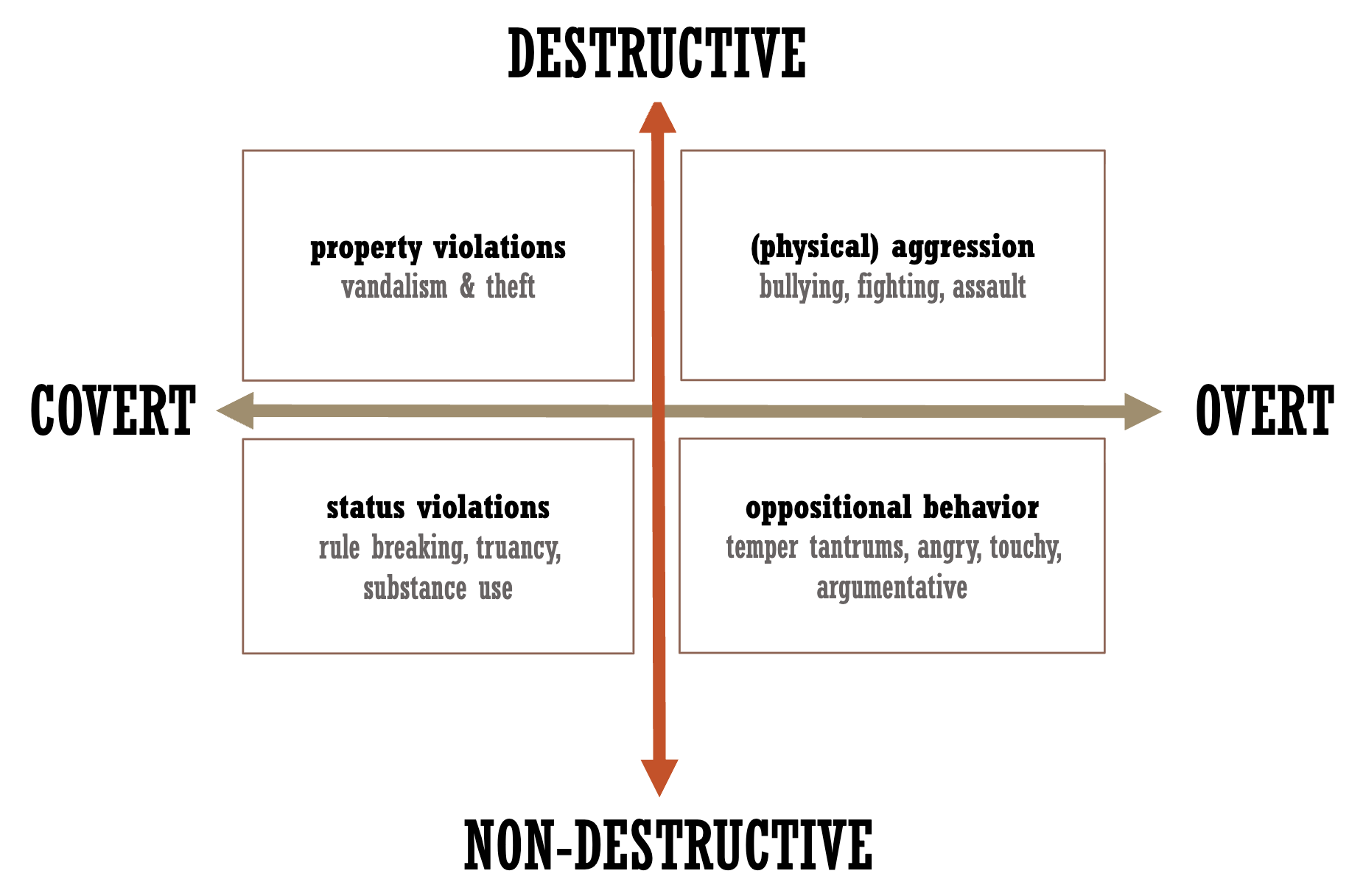
Typology of antisocial behaviour (Frick, 1993)
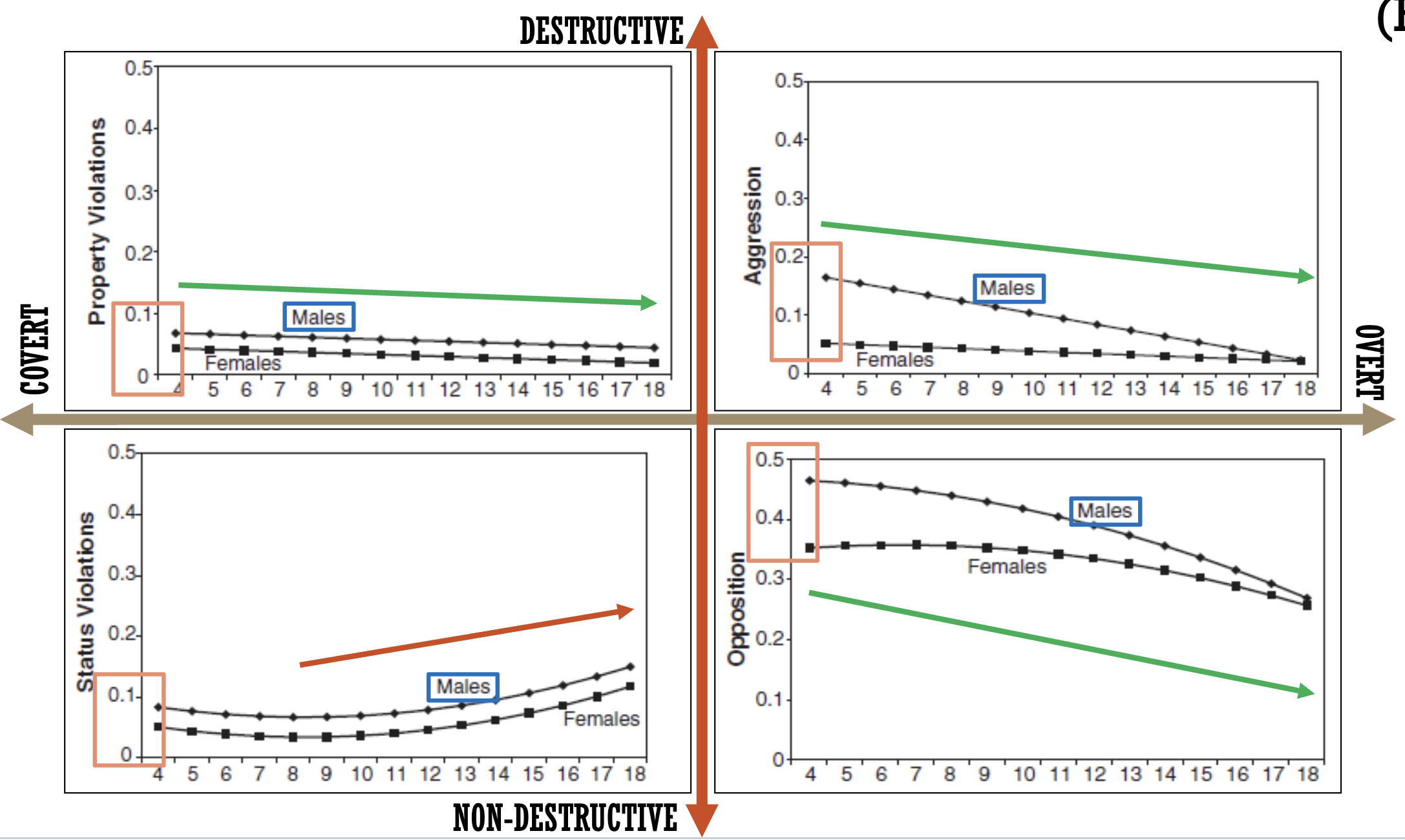
Normal course of antisocial behaviour (Bongers, 2004)
Normal course of delinquency
Highest between 15 and 25
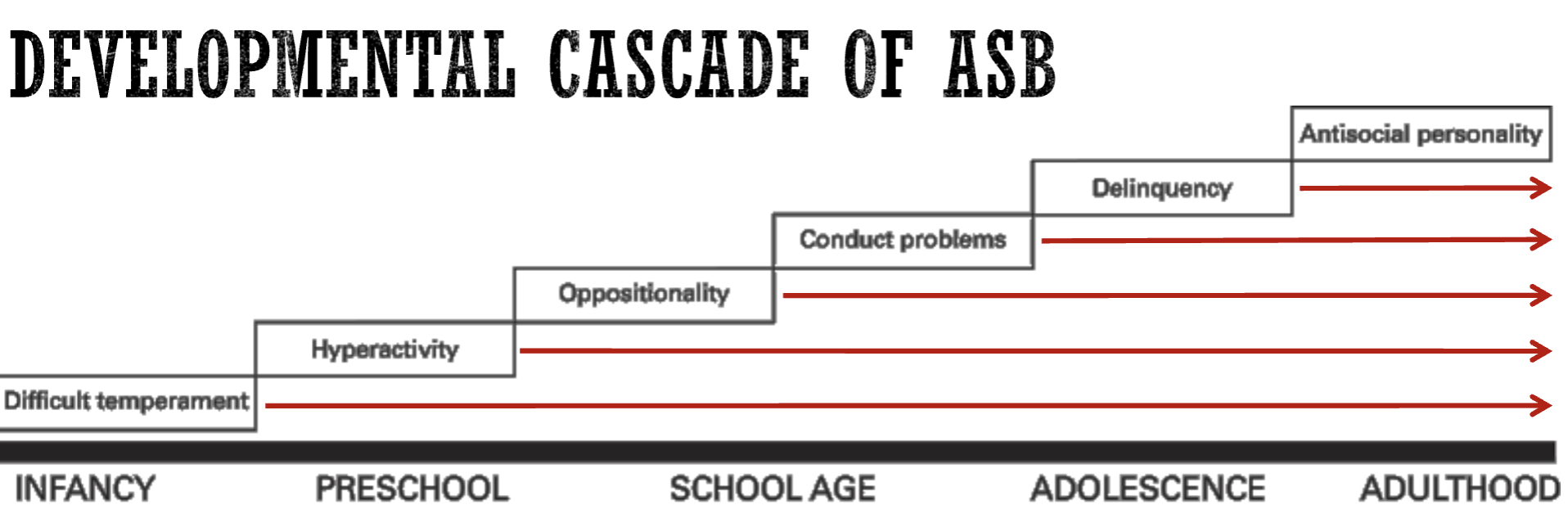
Adolescence-limited vs. Life-long persistent ASD (Moffit, 1993)
Adolescence-limited: quite normative for the age period, spikes during teenage years and rapidly declines when people enter adulthood
Life-long persistent: starts in pre-school age, stays at the same level throughout life
Disruptive, impulse-control, conduct disorder
Conditions involving impaired self-control of emotions and behaviours, SUCH THAT:
these problems violate the rights of others, and/or
bring the individual into significant conflict with authority figures
Disruptive behaviour disorders
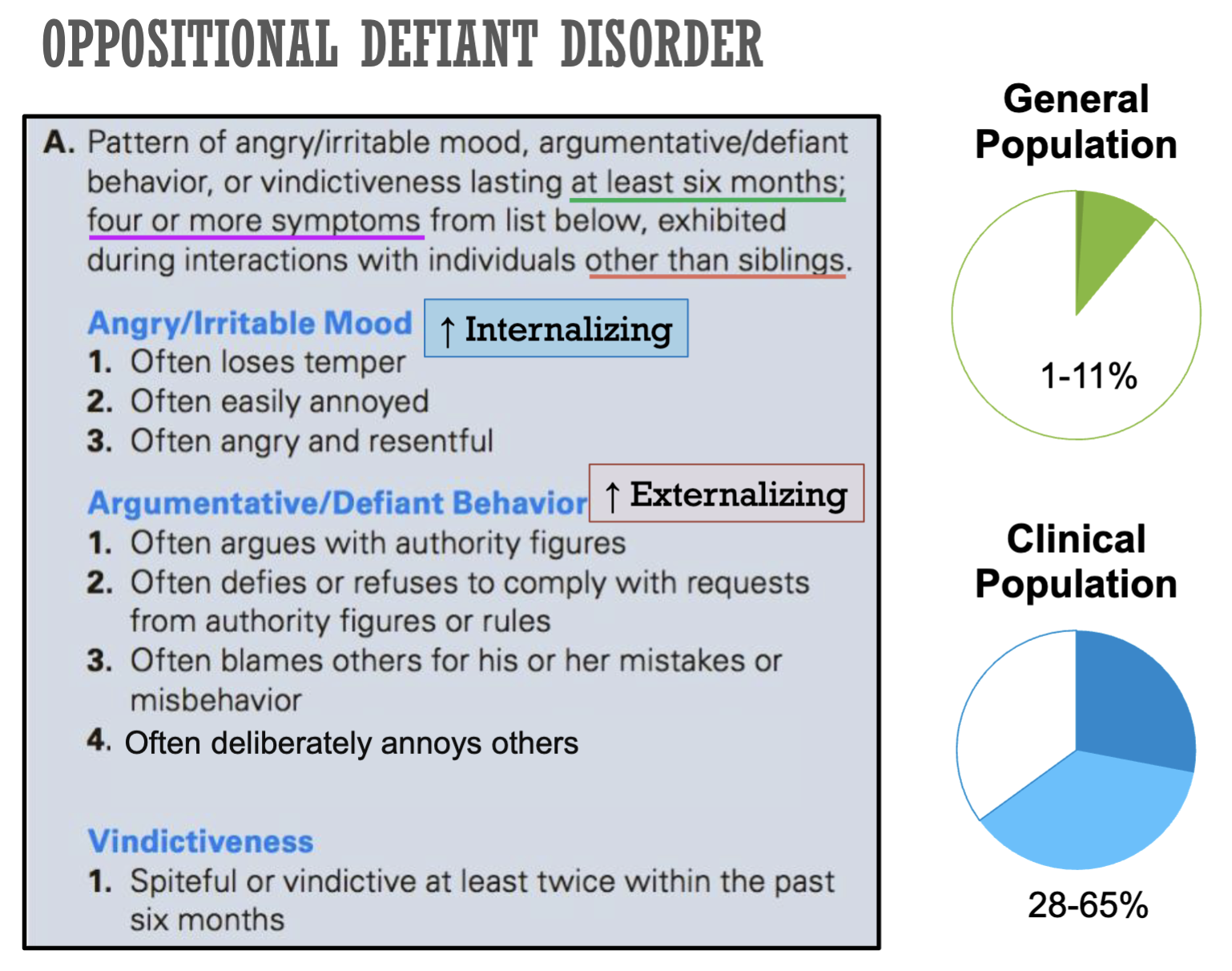
Oppositional Defiant Disorder (ODD)*
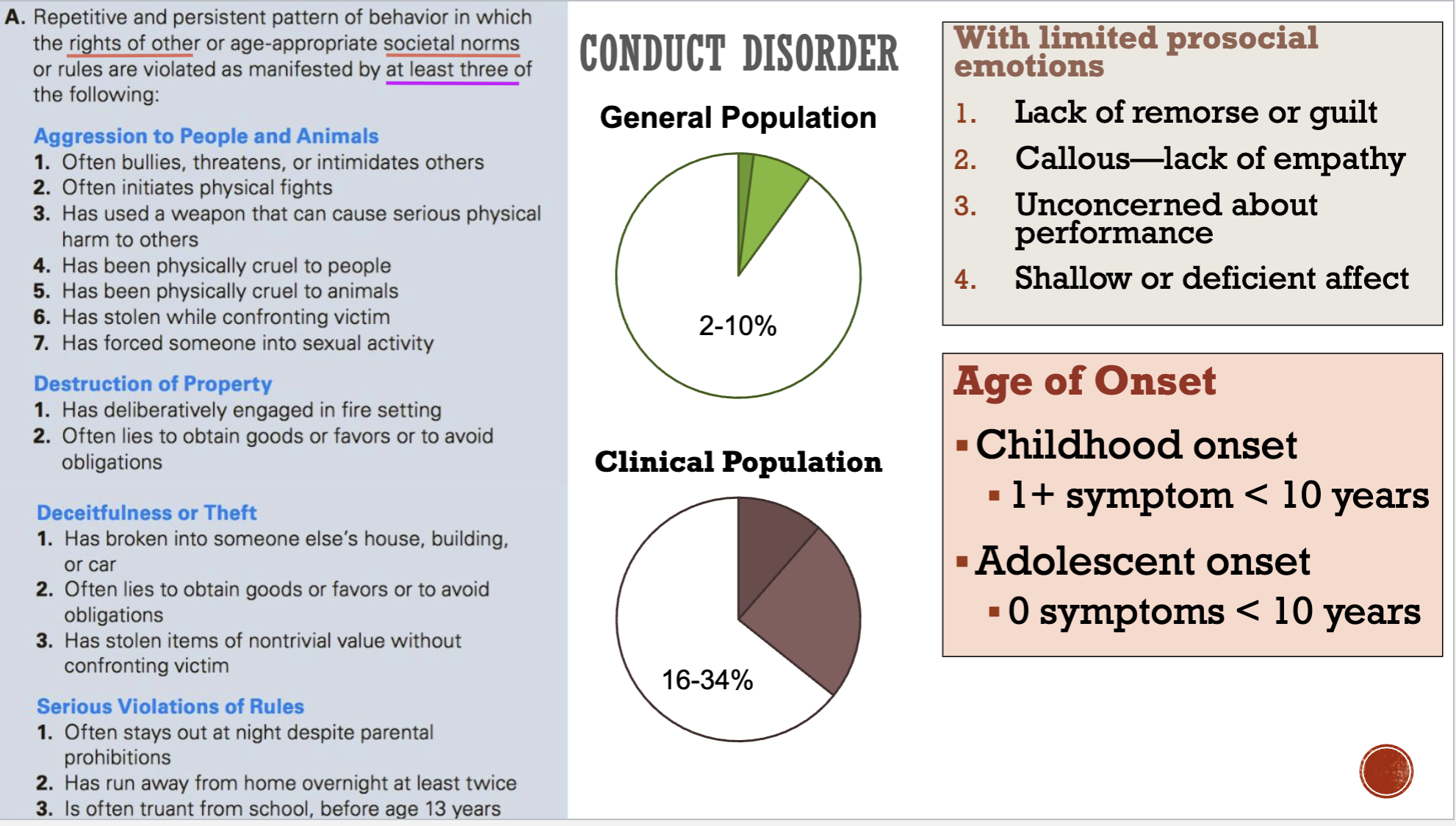
Conduct Disorder (CD)*
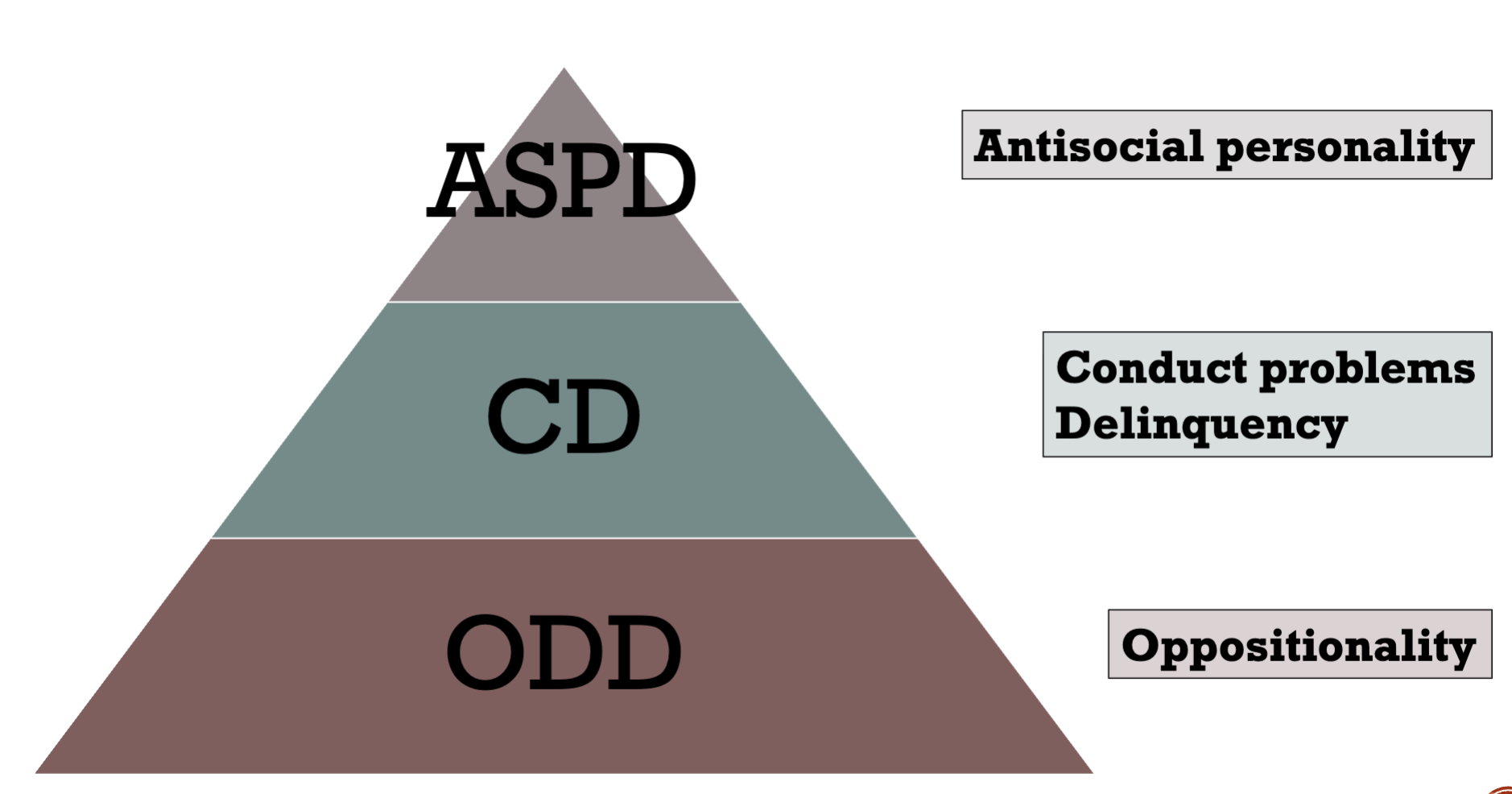
Antisocial Personality Disorder (ASPD)
Intermittent Explosive Disorder (IED)
Pyromania
Kleptomania
Oppositional Defiant Disorder (ODD)
Conduct Disorder (CD)
Developmental cascade of ASB
Pyramide of ASB
Factors that affect the development of ASD
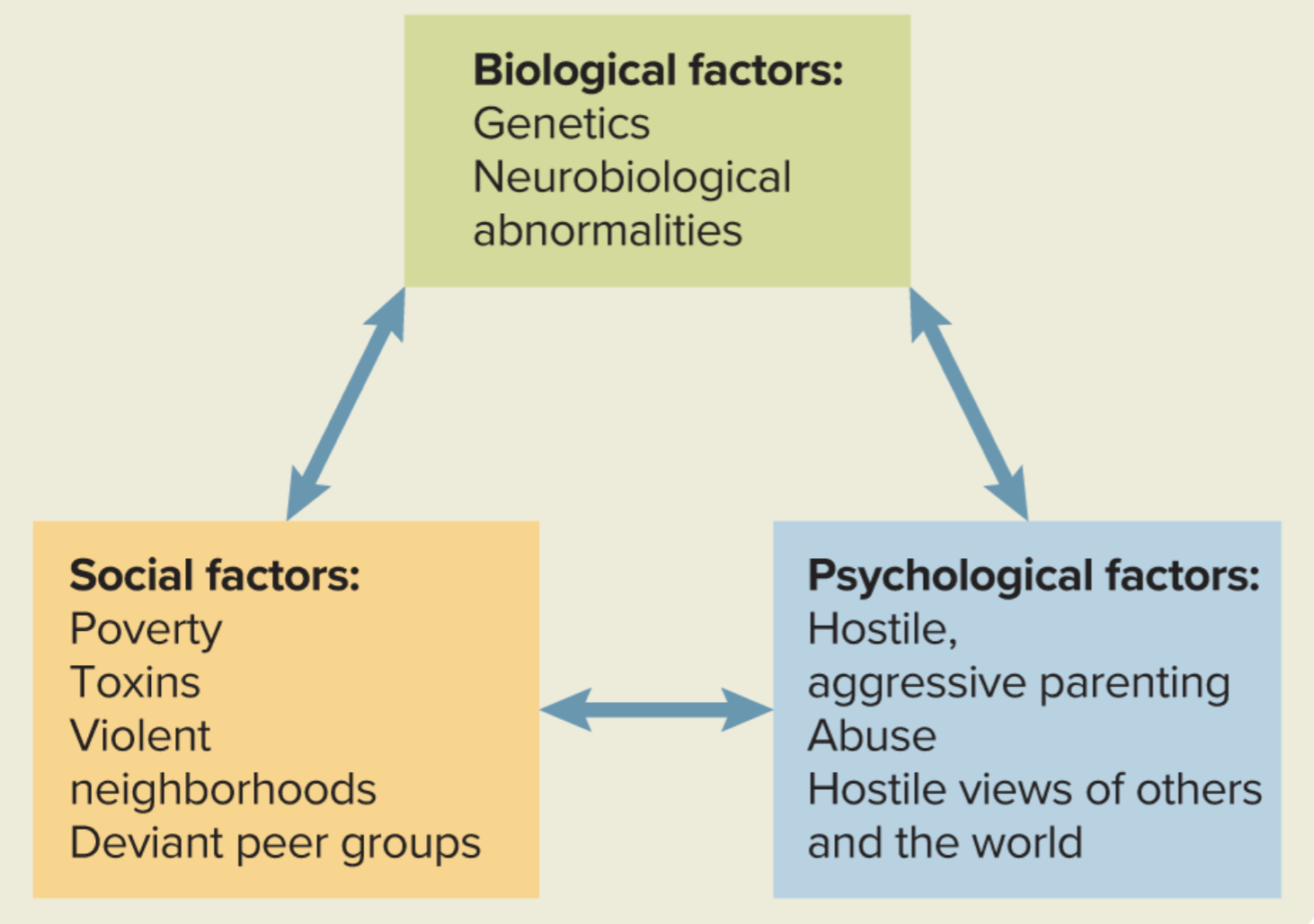
Genetic Vulnerability for ASD
FOXP2 (speech, language, et al.)
Prenatal risk factors
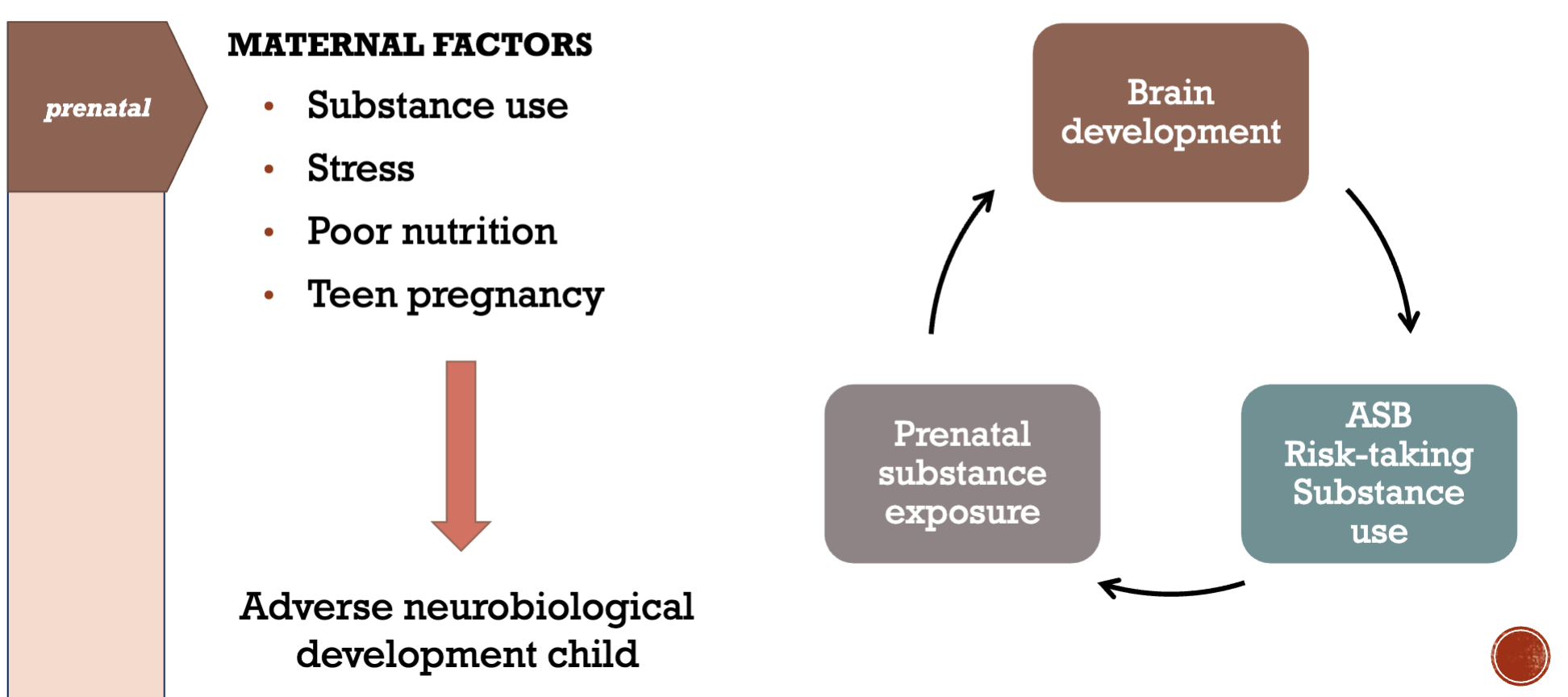
Factors in inadequate parenting (Belsky, 1984)
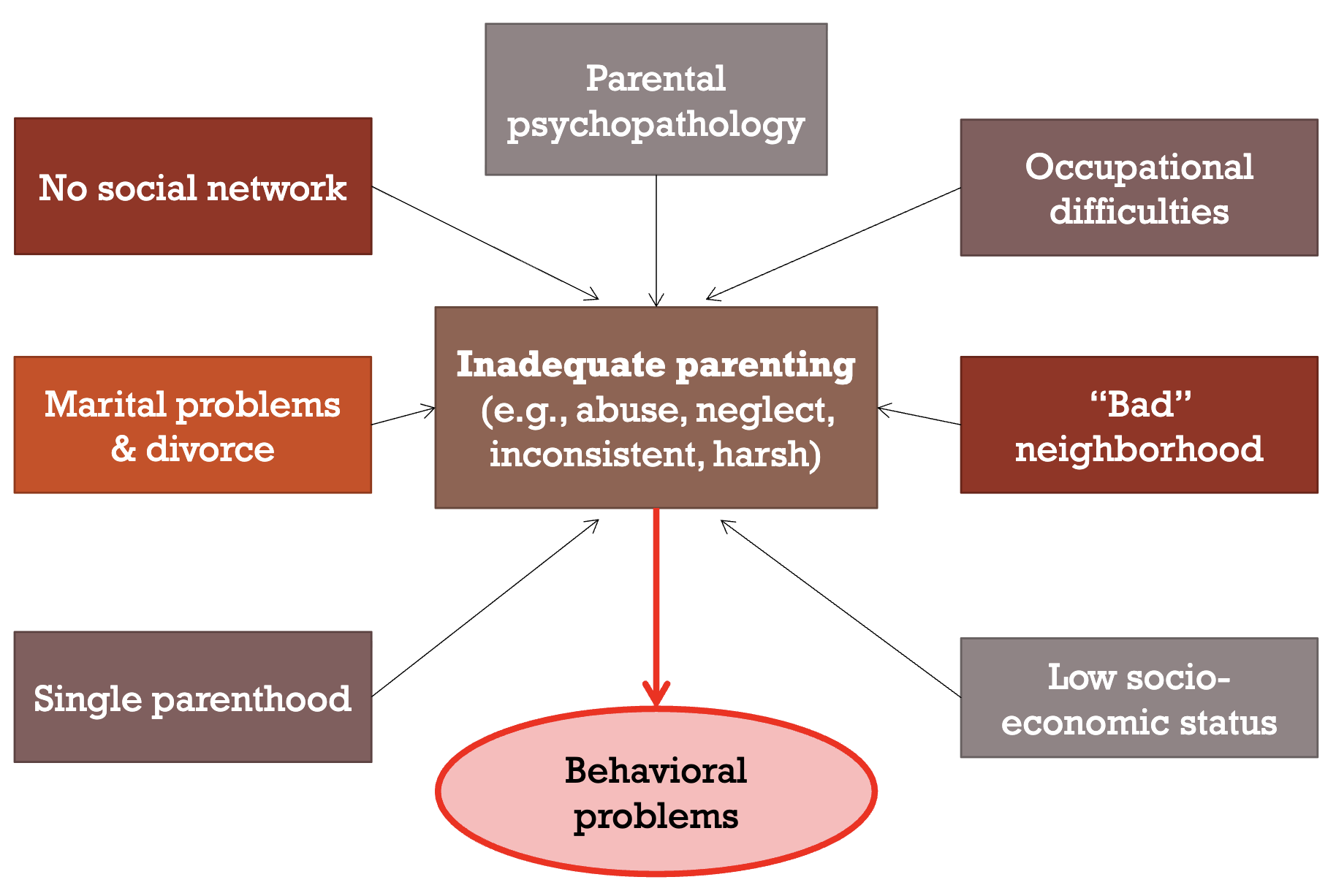
Types of inadequate parenting
Parent-child interaction & ASD