lect 7 - bar type precision attachments
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
16 Terms
splint bar indications
anterior teeth severe resorption of residual ridge
too much vertical space prevents the use of a FPD
esthetic requirements
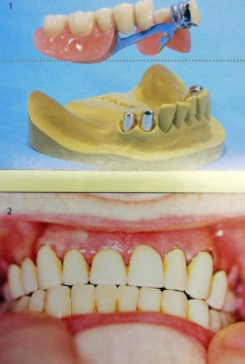
smooth contoured bar resting lightly on the gingival tissues to support the RPD
lower incisors splint together with a splint bar to enhance longevity
tissue surfaces are minimally contacted by the rounded form
floss to clean inferior portion of splint
connecting bar
cast of rigid alloy
soldering not recommended as weaker
available in plastic can be customised for length and cast in metal alloy
internal clip attachements commercially available
cross-section and appearance
Gilmore - oval
Reichenbach - rectangular
Dolder - egg-shaped
diameter shouldn’t exceed 2.35mm
egg-shaped most favourable because it allows the saving of the abutment teeth and retention
most common dimensions :
height - 3mm
width - 2mm
OR
height - 2.2mm
width - 1.46mm
Dolder dimensions
height : 3mm or 2.2mm
width : 2mm or 1.46mm
widest part of the egg shape used in the upper 3rd so the retention minimum 2/3rd is used
clip attachment
longer = better retention
resembles the shape and cross section of the bar, opened from the bottom side and distance between edges is smaller then the widest part of the bar element
can be easily replaced to compensate the subsiding of the denture and facilitate abutments
Wirz
elongating clip attachment x1.5 can double the retentional force
Popoy & Manchev
splint bar made of plastic (polyethene, polypropylene) using element + many chewing cycles friction is increased and can be easily replaced to compensate subsiding of dentur
clip attachment
resilient - withstands from the bar on a distance that is more than the mucosal resilience
rigid - clip attachment in contact with the bar
PD physiologically engages abutment teeth pathophysiologically by bone
3 types of movements of the denture over the egg shaped splint bar
vertical translation
sagittal rotation
frontal rotation
constructional principles
bar must withstand from the gingiva 1-2mm ( to allow flossing)
bar must connect abutments in a straight line
bar must be perpendicular towards the rotational movements
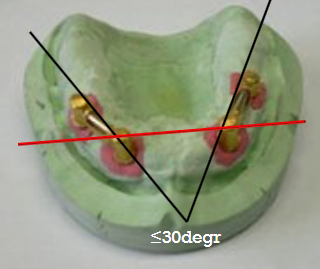
if 2 bars used they must never be bigger than 30o angle one towards another
vestibular flange of denture should be as short as possible (if there is a vacuum here there will be a hypertrophia of the soft tissue under the bar closing the 1-2mm gap under the gingiva)
telescopic crowns
consist of inner and outer telescope or primary/secondary
firmly attached to one another caps
can’t be prefabricated
can be made cylindrical or conical
Bottger
need as much contact between the inner and outer telescope for better retention
Korber
conical telescopic crown
4-8o optimal for friction force of 5-9N
opened telescopic crowns/ring
in cases where the occlusal surface cannot be prepared properly
restricts subsiding of secondary crown
indication for RPD with precision attachments
attachment with 1 direction of movement - rectangular bar
attachments with 2 directions of movement class III and IV
attachments with 3 directions of movement class I and II
contraindication for RPD with precision attachments
abutments with short clinical crowns
parallelism among abutments can’t be achieved
retentive alvolar ridges
abutments with peripheral lesions
abutments with perodontophathia gr. II and III