Papilloma viruses
1/21
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
22 Terms
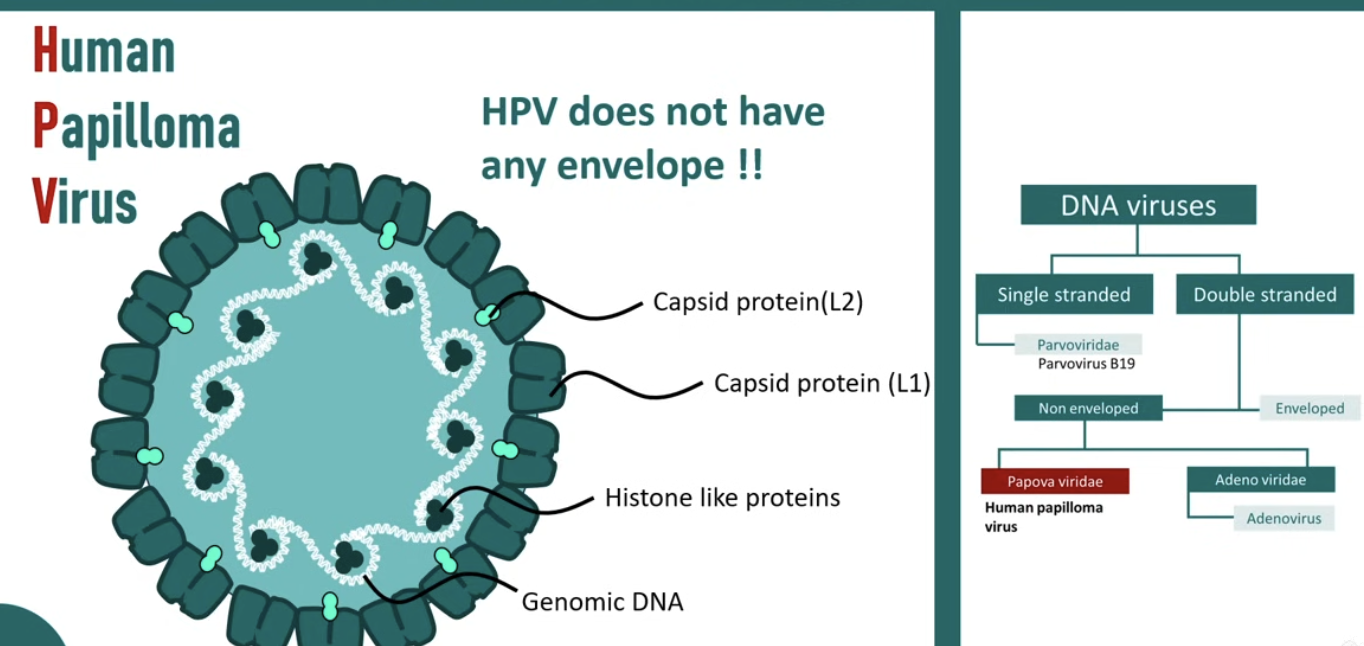
What is the structure of HPVs? (human papilloma viruses)
Small non-enveloped ds-circular DNA viruses
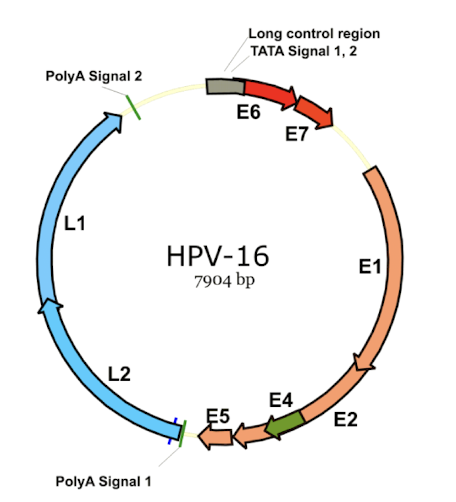
Over 200 genotypes that can infect human epithelial cells, leading to various conditions, including warts and cancers.
Have both early and late capsid e.g. L1 and L2 proteins (E and L)
Have no DNA polymerases
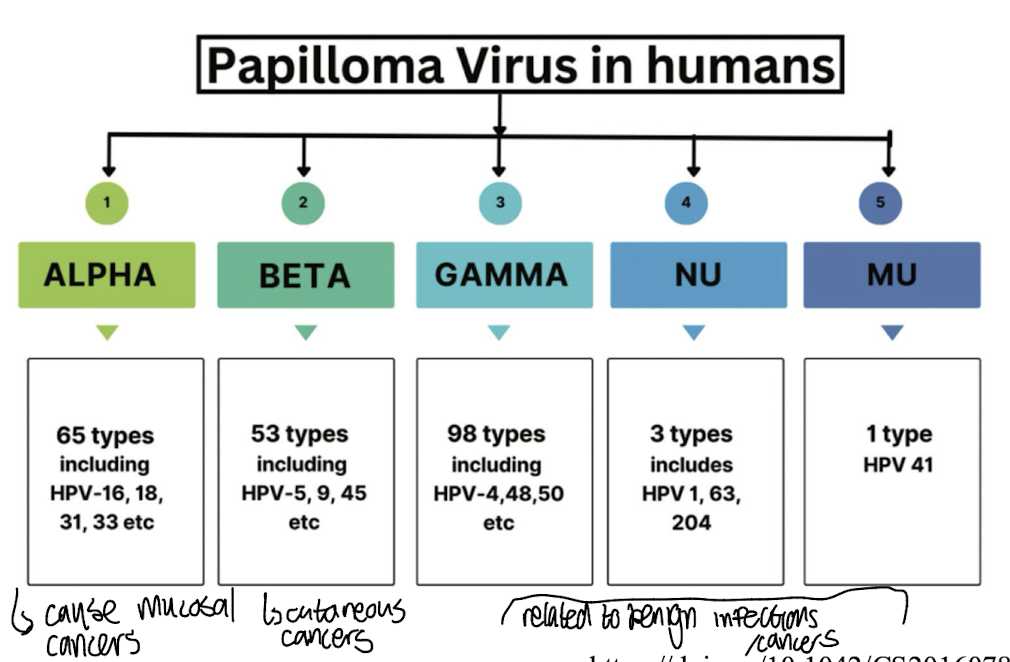
What are the 5 classes of human HPVs?
Classified by Greek lettering:
Alpha → 65 defined types e.g. HPV-16,18,31,33 etc which primarily cause muscosal infections and are associated with cervical and other anogenital cancers.
Beta → 53 types e.g. hpv 5,9,45 etc. mainly linked to skin lesions and cutaneous cancers
Gamma → 98 types associated with non-malignant skin conditions.
Nu→ 3 types including HPV-1, 63, 204
Mu → HPV 41 related to benign lesions of the skin and mucous membranes.
What are the two main clinical manifestations of HPV infection?
Have a tropism for squamous epithelial cells which can be cutaneous or muscosal
Cutaneous→ low cancer risk
Mucosal → high cancer risk
What are the low risk (LR) cutaneous HPV genotypes?
Include HPV-1, 2, 4, 7, and 27.
These types are typically linked to common, benign warts and similar lesions, carrying a low risk of malignancy.
Transmission primarily via fomites, skin-skin contact / dead skin

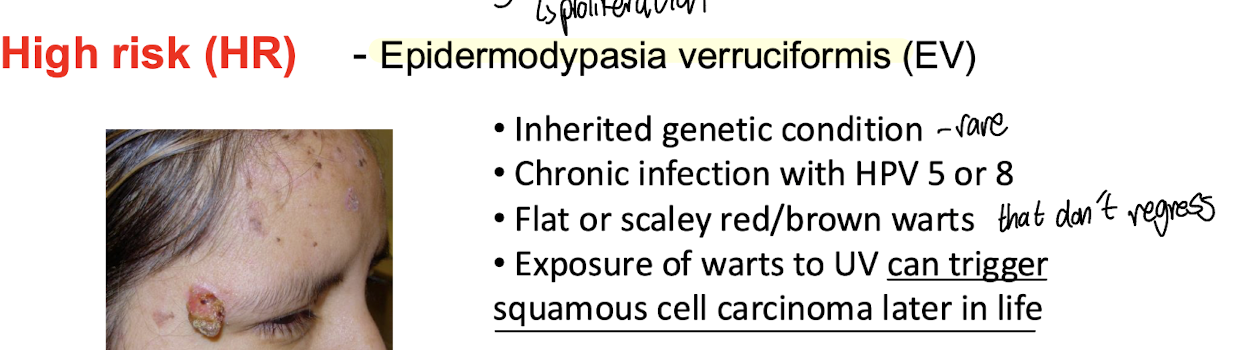
What are the high risk (HR) cutaneous HPV genotypes?
Include HPV-5, HPV-8, and HPV-49.
Associated with a higher probability of causing skin cancers and lesions.
Typically manifest clinically as the chronic infection, EV - Epidermodypasia verruciformis → can lead to squamous cell carcinoma due to UV exposure
Contracted primarily due to a genetic disorder that increases susceptibility to HPVs
What are the low risk (LR) mucosal HPV genotypes?
Include HPV-6, 11 as well as 40,42 etc
These types are typically linked to genital warts or benign cervical changes nd similar lesions, carrying a low risk of malignancy.
Transmission primarily via sexual transmission i.e. contact with infected genital skin, mucosal surfaces
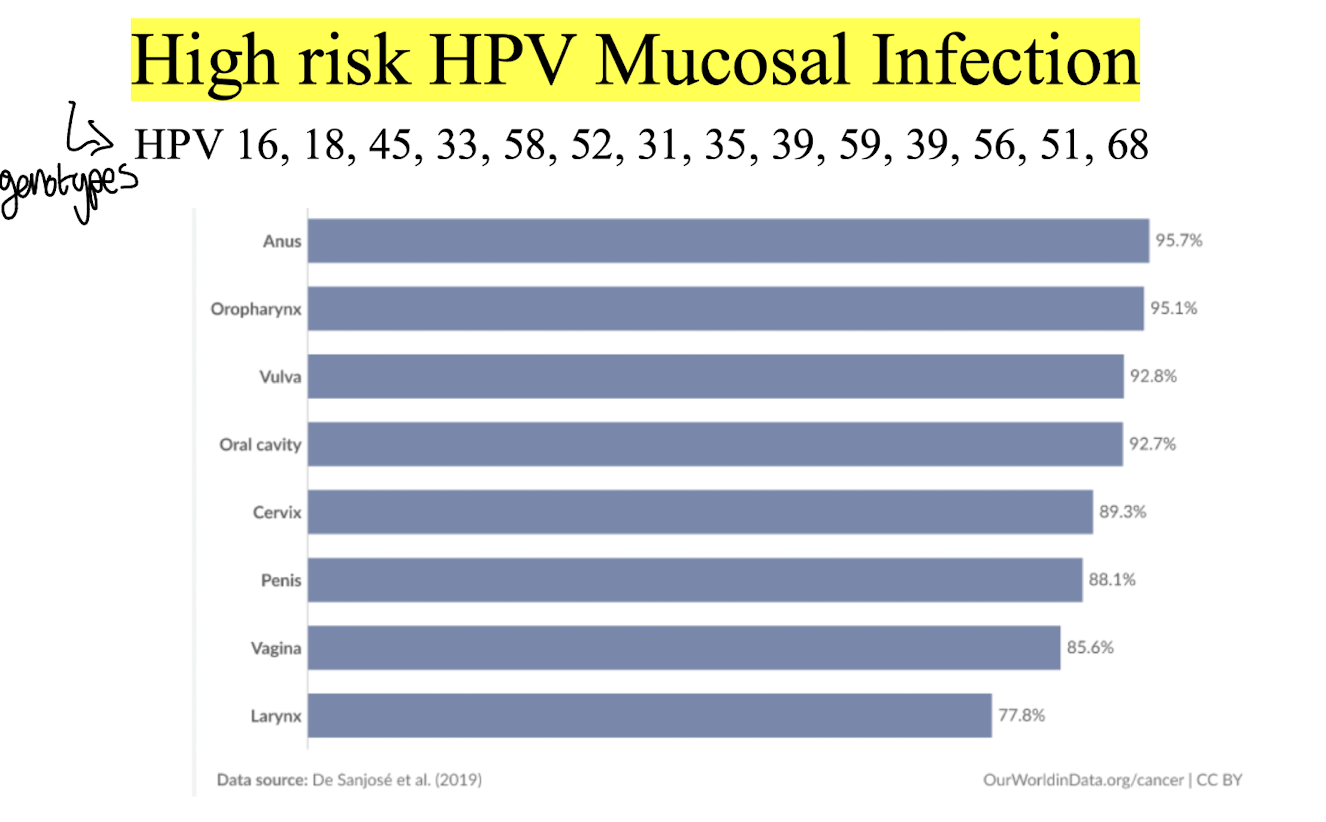
What are the high risk (HR) mucosal HPV genotypes?
Include HPV-16, 18, as well as 31, 33, 45, 52, and 58.
Associated with significant risks of cervical and other anogenital cancers i.e. oropharynx, anus, penile, vulvar and vaginal cancers with HPV-16 and 18 being the most prevalent in cancer cases.
Transmission ALSO primarily via sexual transmission i.e. contact with infected genital skin, mucosal surfaces
What HPV genotypes are responsible for 90% of genital wart cases?
Include HPV-6 and HPV-11.
• Very prevalent in sexually active adults
• Self-limited, regress spontaneously or persist for years
• Difficult to treat in immunosuppressed patients and in pregnant women
• Treatment using Imiquimod; stimulation of innate and acquired immune
response
What HPV genotype is attributed to most cases of oropharyngeal cancers?
• HPV accounts for approx. 70% of all oropharyngeal cancers in the US and 50% in the UK
• 90% of these is caused by HPV16 → most oncogenic
• Linked with oral sexual behaviour → young age of diagnosis
What is the treatment response like for oropharyngeal cancers related to HPV?
• Better response to treatment involving combined surgery and radiation or chemotherapy
• Lower rates of disease relapse and metastasis
• Improved overall survival
What HPV genotypes are attributed to cervical cancer?
HPV 16, 18, 31, 45
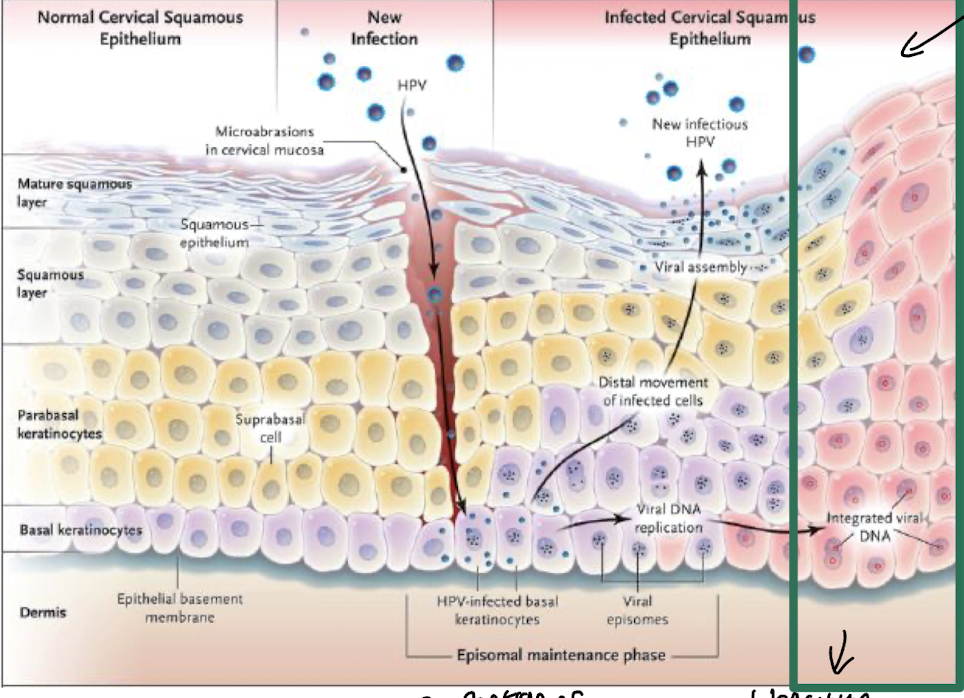
What is the lifecycle like of HPVs linked to cancer development?
Initial infection in the basal layer of squamous epithelial cells, primarily due to micro-abrasions in mucosa i.e. the cervix,
Followed by viral replication i.e. in HPV-infected basal keratinocytes and integration into the host genome.
This can lead to the expression of oncogenes, which disrupt normal cell cycle regulation, promoting uncontrolled cell proliferation by cells entering the S phase and potential tumorigenesis.
Cells divide and differentiate as they move up, with distal movement of infected cells ultimately allowing for the release of new infectious HPV particles
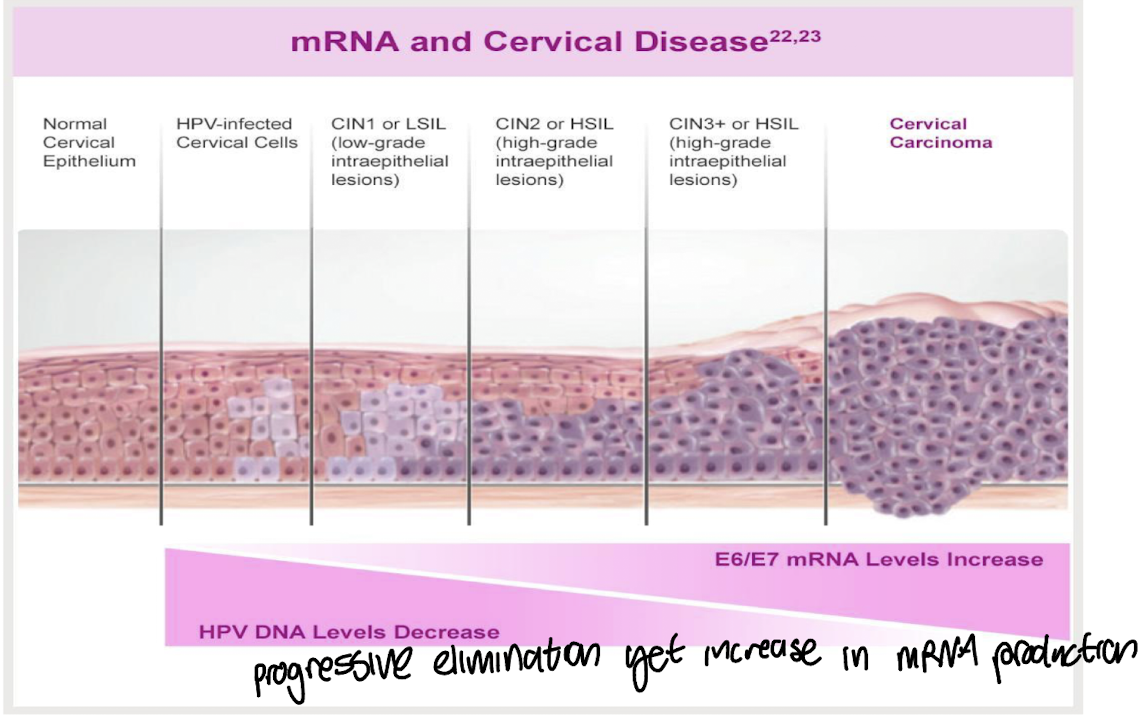
What are cellular events which lead to cervical cancer
Cervical intraepithelium neoplasia (CIN) is a precursor to cervical cancer, characterised by abnormal changes in the cervical cells due to persistent HPV infection.
These cellular changes can progress through stages of CIN 1, CIN 2, and CIN 3, with higher degrees of dysplasia indicating an increased risk for cancer development.
How can cervical screening be conducted to detect HPV-infected cervical epithelial cells? & what are the treatment options
• Primary screening → positive primary screen indicates inactive viral infection
HPV molecular test for HPV high risk subtypes
25-29yr old every 3 years; 30-65 every 5 years
• Cytology for HPV positive cases
• Colposcopy
Treatment for cervical cancer:
• Surgery, radiotherapy, chemotherapy
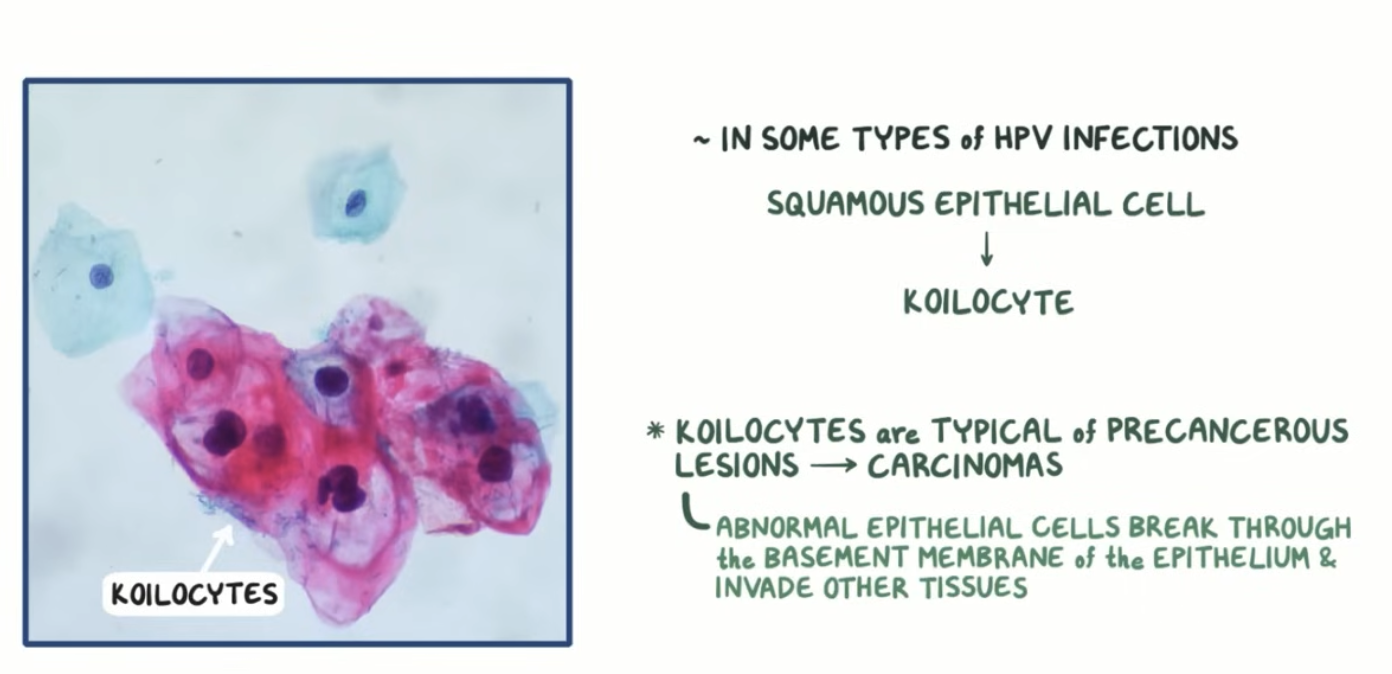
What is a koilocyte and features of it?
= Abnormal squamous epithelium cell as a result of infection with HR HPV
→ Typical of precancerous lesions which can develop into carcinomas
Enlarged nucleus
Clearing “halo” around the nucleus
Condensed chromatin → indicating no active gene expression occurring
Pathogenesis of cervical cancer
Chronic infection and integration of viral DNA binding proteins encoded by the E6/E7 genes into cellular DNA; only viral genes expressed in HPV+ cancer cells
E6/E7 expression transforms primary keratinocytes and causes cancer in transgenic animals
Inhibition of E6/E7 inhibits the growth of HPV+ cancer cells and results in senescence
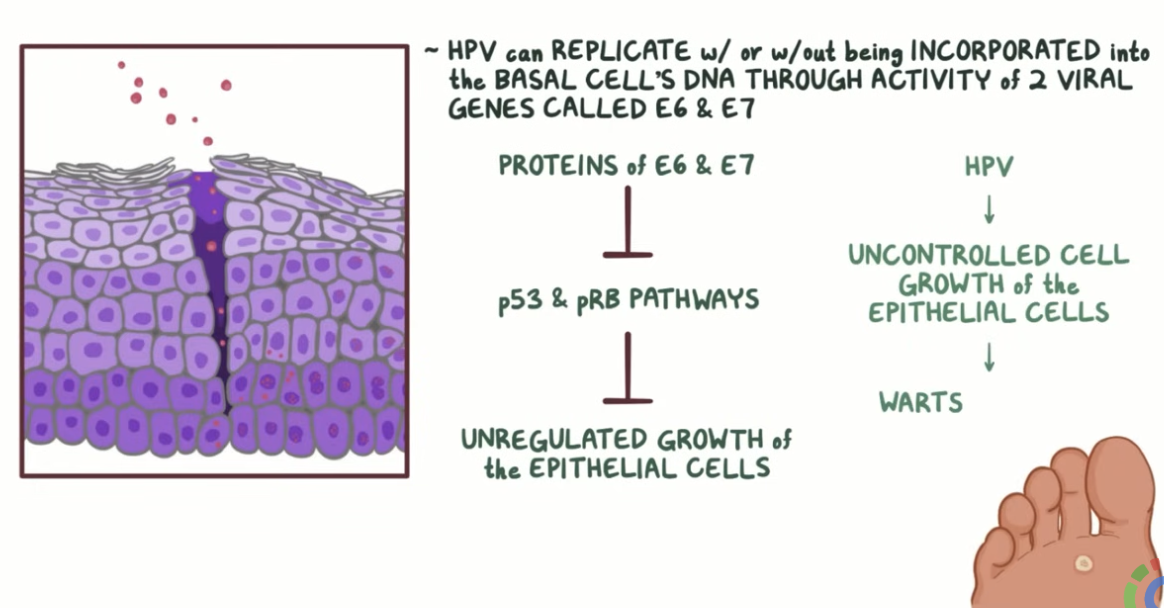
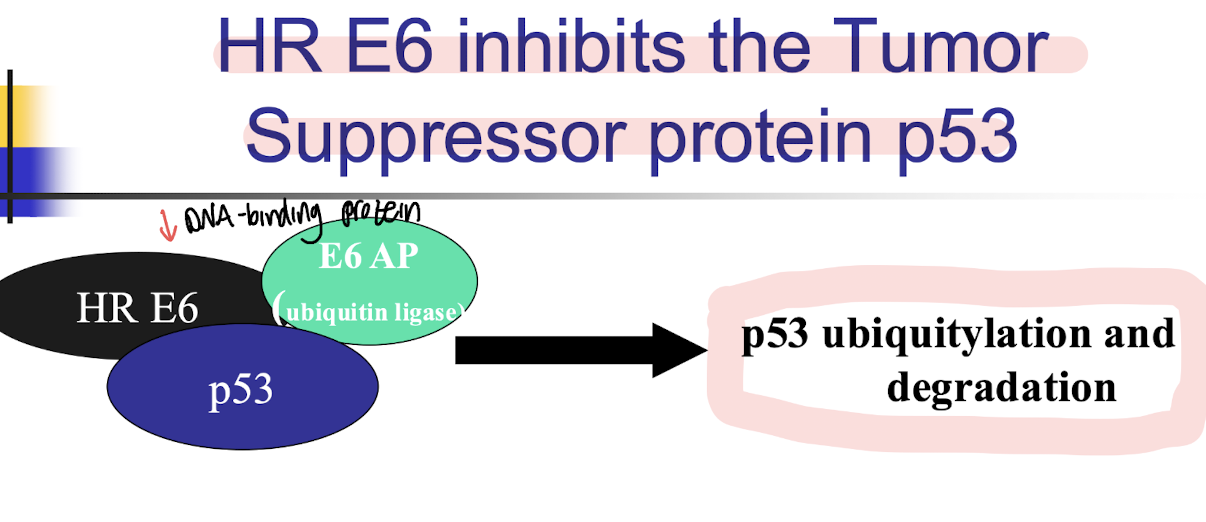
How does high risk E6 DNA binding protein associated with HPV-16 inhibit the tumour suppressor protein p53?
Via p53 ubiquitylation and degradation, leading to cell cycle progression and inhibition of apoptosis.
• p53 is activated by stress to cells eg UV damage → signals for aptosis
• Levels of p53 are lower in HPV positive cells compared to normal cells
Other than p53, what other cellular processes does HR HPV E6 target?
E6 binds and inhibits a multitude of tumour suppressors via its PDZ binding domain
E6 activates telomerase by up-regulating the expression of the catalytic subunit of human telomerase (hTERT) in infected cells resulting in longer lifespans and immortalisation
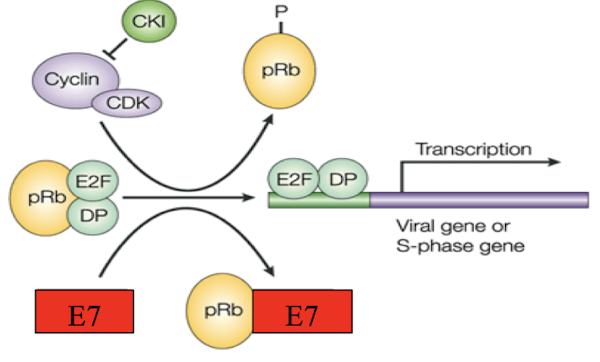
What are the cellular targets of the E7 protein by HR HPV?
Phosphorylation of Rb by E7 releases E2F/DP and promotes cell cycle progression
Hypophosphorylated Retinoblastoma tumor suppressor (pRB) represses G1-S phase transition of cell cycle
E7 binds and inactivates pRB resulting in the activation of the cell cycle
Binds and inactivates CDK inhibitors → resulting in cell growth
Induces cell cycle checkpoint defects e.g. centrosome abnormalities and aneuploidy, contributing to genomic instability along with structural DNA breaks.
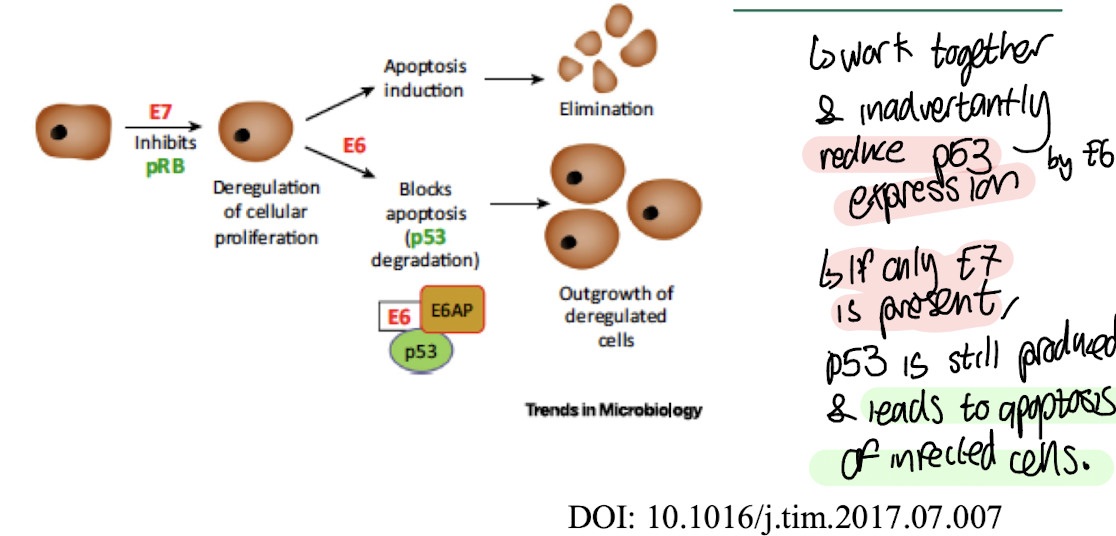
What is an example of how the interaction between HPV’s E6 and E7 proteins is essential for transformation?
An example of the interaction between HPV's E6 and E7 proteins is that E6 promotes the degradation of p53, while E7 inactivates pRB, leading to uncontrolled cell division and transformation
Whereas if only E7 is present, p53 can still activate apoptosis and prevent cell cycle progression.
This cooperative inhibition of both tumour suppressors is crucial for HPV-mediated transformation.
What immune response is generated against HPVs?
Antibody response generated against viral capsid proteins L1 and L2
Anti–L1 antibodies are virus neutralising and type specific
Anti-L2 are generated but not as potent as anti-L1
Specific cell mediated immune response can trigger clearance of natural HPV infection
How does vaccination for HPV help increase the immune response?
• Intramuscular injection allows expression of L1 in vitro leading to the formation of virus like particles with the same conformation dependent neutralizing epitopes as the natural virus
• Strong immune-responses, safe and well tolerated
Vaccines e.g. Gardasil 9 2015 (HPV 6/11/16/18/31/33/45/52/58)
Used in Ireland for girls and boys (2019)
One dose enough in healthy 12-13 yr olds