NR507 Advanced Pathophysiology MidTerm With 100% correct answers + rationales 2026
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
Hypersensitivity: Type 1
Type 1: Allergic reaction, Mediated by IgE, Inflammation due to mast cell degranulation
Local symptoms:
-itching
-rash
Systemic symptoms:
-wheezing
Most dangerous = anaphylactic reaction
systemic response of hypotension, severe bronchoconstriction
Main treatment: epinephrine reverses the effects
Hypersensitivity: Type 2
Type 2: Cytotoxic reaction; tissue specific (ex: thyroid tissue)
Macrophages are the primary effectors cells involved
Can cause tissue damage or alter function
Grave's disease (hyperthyroidism) - example of altering thyroid function, but does not destroy thyroid tissue
Incompatible blood type- example of cell/tissue damage that occurs; severe transfusion reaction occurs and the transfused erythrocytes are destroyed by agglutination or complement-mediated lysis.
Type 1 Hypersensitivity VS. Type 2 Hypersensitivity
Type 1 Hypersensitivity
Organ Specific
Antibody binds to the antigen on the cell surface
Type 2 Hypersensitivity
Not Organ Specific
Antibody binds to the soluble antigen outside the cell surface that was released into the blood or body fluids, and the complex is then deposited in the tissues
Hypersensitivity: Type 3 - Examples
Rheumatoid arthritis: Antigen/antibodies are deposited in the joints
Systemic Lupus Erythematosus (SLE)- very closely related to autoimmunity- antigen/antibodies deposit in organs that cause tissue damage
Hypersensitivity: Type 4
Delayed response
Does not involve antigen/antibody complexes like Types 1, 2 and 3
Is T-cell mediated
Differentiating Between the Rash of a Type 1 vs. Type 4 Reaction:
Type 1: Immediate hypersensitivity reactions, termed atopic dermatitis, are usually characterized by widely distributed lesions
Type 4: Contact dermatitis (delayed hypersensitivity) consists of lesions only at the site of contact with the allergen
The key determinant is the timing of the rash:
-Type 1 = Immediate
-Type 4 = Delayed: Several days following contact, ex would be poison ivy
Treatment of Type 4 Rash
A non-severe case of contact dermatitis would be treated with topical corticosteroid.
Why not epinephrine or antihistamines?
-Epinephrine is for emergent Type 1 anaphylactic reactions. Antihistamines act on the H1 receptors. Type 4 does not involve mast cells and H1 receptors.
Antibiotics not appropriate since not an infection
Autoimmunity
Autoimmune disease can be familial, Affected family members may not all develop the same disease, but several members may have different disorders characterized by a variety of hypersensitivity reactions, These include autoimmune and allergic reactions
Associations with particular autoimmune diseases have been identified for a variety of major histocompatibility complex (MHC) alleles or non-MHC genes
Alloimmunity
General term used to describe when an individual's immune system reacts against antigens on the tissues of other members of the same species.
Examples: Neonatal disease where the maternal immune system becomes sensitized against antigens expressed by the fetus, Transplant rejection, Transfusion reaction
Primary Immunodeficiency
Most primary immune deficiencies are result of single gene defects
Something is lacking with the immune system itself.
Example: B-lymphocyte deficiency - one of the most severe forms of a primary immunodeficiency
Secondary Immunodeficiency
Complication of some other physiological condition/disease, Malnutrition one of most common causes worldwide. Example: Pt. with HIV gets pneumocystis carinii
Hematology
Anemias, Involve RBCs, Most of body's iron stores come from the recycling of iron from old RBCs
Iron Deficiency Anemia
Microcytic/Hypochromic Anemia, Caused by disorders of hemoglobin synthesis, particularly iron deficiency, Ferritin is an important measurement that reflects the body's total iron stores, The NP will order a ferritin level to get an idea of the body's total iron stores, Low ferritin reflects anemia
Major Lab Marker for Anemia
Increased RBC distribution width (RDW) is one of the earliest lab markers in developing microcytic or macrocytic anemia
Folate Deficiency
Can cause megaloblastic anemia, Alcoholics can easily get folate deficiency
Ferritin level normal
Hgb low
Hct low
Vitamin B-12 Deficiency
Fatigue, Dyspnea, Peripheral Neuropathy in BLE (numbness and tingling)
Risk Factors: Older adults, H-pylori infection
Affects Vitamin B-12 absorption
Hemolytic Anemia
Who is at risk?
RBCs destroyed, Mismatched blood types destroy RBCs.
Autoimmune hemolytic anemia due to autoantibodies against erythrocytes that the immune system perceives as an antigen and then attacks it. Allergic reaction to a drug causes drug-induced hemolytic anemia
Acute Blood Loss Anemia
Trauma victims who are losing blood, GI bleed (Acute)
Aplastic Anemia
Diagnosis made by blood tests and bone marrow biopsy.
AA is suspected if levels of circulating erythrocytes, leukocytes and platelets diminished:
-Granulocyte count less than 500/ uL
-Platelet count less than 20,000/ uL
-Absolute reticulocyte count less than or equal to 40 x 109/ L
Sickle Cell Anemia
Patients encountered who have sickle cell trait, Inherited a normal Hb gene from one parent and an abnormal Hb gene from the other parent
Thalassemia
Inherited blood disorder causing decreased circulating hemoglobin, Many possible genetic mutations
Heart Failure
Pathophysiology (Wk 2 Discussion)
Underlying patho is that there is less cardiac output to meet the body's oxygen demands.
Over time there is decreased contractility, decreased stroke volume, increased left ventricular end-diastolic volume (LVEDV)
When contractility is decreased, stroke volume falls, and LVEDV increases. This causes dilation of the heart and an increase in preload.
Major risk factor is long standing hypertension. Preload = stretch Afterload = resistance
Differentiate between Right and Left Heart Failure
Sometimes right-sided heart failure can occur due to left-sided heart failure due to the back up of fluid from the left side to the right.
Sometimes right-sided heart failure can occur without there being left-sided heart failure; this usually occurs because the person has long standing pulmonary issues (COPD).
Patients will have classic R. sided heart failure symptoms without L. sided heart failure symptoms: Right JVD distention, Peripheral edema, Hepatosplenomegaly
Stages of Heart Failure (ACC/AHA)
-Stage A: patient has risk factors (CAD) but no symptoms; no structural heart damage
-Stage B: patient has structural heart damage (MI), but still has no symptoms
-Stage C: patient is symptomatic with alteration in their daily functions due to dyspnea, swelling, etc. This is where the NYHA functional classifications come into play
-Stage D: end-stage heart-failure - have maximized medications to treat it. May need heart transplant or pacemaker
NYHA Functional Classifications- It's all about the impact on the patient's activity caused by the HF symptoms:
-Stage I: Mild- no limitation of physical activity; Ordinary physical activity does not cause symptoms -Stage II: Mild- slight limitation of physical activity; comfortable at rest; Ordinary physical activity results in fatigue, palpitation, dyspnea or anginal pain.
-Stage III: Moderate- marked decrease in physical activity; marked limitation of physical activity; comfortable at rest. Less than ordinary activity causes fatigue, palpitation, dyspnea or anginal pain. -Stage IV: Severe- inability to carry on any physical activity without discomfort. Symptoms of HF or the anginal syndrome may be present even at rest. If any physical activity undertaken, discomfort is increased.
Heart Valve Disorders
Signs and Symptoms (Edapt Scenarios), Murmur Characteristics, Important to know Anatomy
Aortic Stenosis
Blood backed up into left ventricle causing perfusion problems for the rest of the body
Causes:
Bicuspid aortic valve- congenital condition (only two cusps to the aortic valve which usually has three cusps)- the two cusps get damaged quicker because they are doing the work of three
Age related calcification- obstruction/ stenosis
Smoking, High BP, Hypertension, Hyperlipid, Diabetes
Rheumatic Fever
Signs & Symptoms = SAD
S: Syncope
A: Angina
D: Dyspnea
**Fainting
Chest pressure upon exercising
Sustained, laterally displaced apical pulse
Mid-systolic crescendo-decrescendo murmur heard loudest at base and radiating to the neck
S4 gallop present**
Aortic Regurgitation
Blood is coming back from the Aorta into the L. Ventricle through the Aortic Valve
Causes
Widening or aneurysmal change of the aortic annulus (ring of fibrous tissue surrounding the aorta)
Endocarditis
Rheumatic Fever
Signs & Symptoms
Fatigue
Syncope
SOB
Palpitations
Widened Pulse Pressure
L. Ventricular Dilation
Early diastolic murmur along left sternal border
**Shortness of breath that progressively worsens
High pitched early diastolic murmur heard loudest at left lower sternal border
Diastolic rumbling sound at the heart's apex
Systolic crescendo-decrescendo murmur heard at the left upper sternal border
A chest x-ray may show signs of pulmonary edema and cardiomegaly**
Mitral Stenosis
Blood is going to back up into the L. Atrium and Lungs
Causes
Rheumatic Fever / Rheumatic Heart Disease
Endocarditis
Signs & Symptoms
Fatigue
SOB
Exercise intolerance
Cough
L. Atrial enlargement
Pulmonary congestion/edema
Diastolic rumble
Opening snap before Diastolic rumble
**As mitral stenosis progresses, symptoms of decreased CO occur, especially during exertion Shortness of breath on activity
Pounding/racing heart
Associated w/ history of Rheumatic HD
A low-pitched murmur auscultated at the heart's apex
JVD and bilateral crackles in lung bases noted
ECG demonstrates A-FIB and Left Ventricular Hypertrophy**
Mitral Regurgitation
Blood goes from L. Ventricle to L. Atrium and then to the Lungs
Causes - Anything that causes LV dilation
Remodeling process (post MI)
Dilated cardiomyopthathy
Rheumatic Fever/ Rheumatic Heart Disease
Endocarditis
Papillary muscle dysfunction/rupture/ chordae tendinae
Calcification of the valve/around the valve
Signs & Symptoms
Acute
Chronic
**Shortness of breath
JVD, Crackles in bilateral lung bases
Blowing pansystolic murmur heard best at heart's apex and radiates to back and axilla**
Obstructive vs. Restrictive Pulmonary Disease
Obstructive: decreased FEV1 indicates airway obstruction along with low FEV1/FEV ratio 56%
Restrictive: FEV1/FVC ratio above 70%, Review EDapt examples
Asthma
Airways constricted
Intrinsic: triggered by something internal such as anxiety
Extrinsic: triggered by something in outside environment- something in the air (dust mites/pet dander)
In mildest form of asthma (intermittent), short acting beta2-agonist inhalers are prescribed
Mild-persistent asthma will have night symptoms 3-4 days a month
COPD
Diagnosis based on Hx of symptoms, physical exam, chest imaging, pulmonary function tests and blood gas analysis
Pulmonary function testing reveals airway obstruction (decreased FEV1) that is progressive and unresponsive to bronchodilators, Emphysema, Chronic bronchitis
COPD Staging According to GOLD Guidelines- Based on degree of airway limitation
Gold 1: Mild: FEV1≥80% predicted
Gold 2: Moderate: 50% ≤FEV1 <80% predicted
Gold 3: Severe: 30% ≤FEV1 <50% predicted
Gold 4: Very Severe: FEV < 30% predicted
Emphysema
Damage occurs in the alveoli, Impairs gas exchange, Issue is in expiration- they can get air in but cannot get air out
Air trapping, Pursed lip-breathing
Increased A&P diameter, Barrel chest
Chronic Bronchitis
Productive cough with copious amounts of sputum
dyspnea
wheezing
rhonchi and cyanosis of the skin and mucous membranes
Damage occurs in the airway- not the alveoli, Mucous Plugs
Forced Vital Capacity (FVC)
Normal 80-120%
The FVC measures the volume of air in the lungs that can be exhaled.
Patient inhales as deep as possible and then exhales as long and as forcefully as possible.
Obstructive: Will be decreased or normal
Restrictive: Will be decreased
Forced Expiratory Volume in 1 second (FEV1)
Normal 80-120%
Amount of air forcefully exhaled from the lungs in the first second.
The patient inhales and forcefully exhales as fast as possible.
Obstructive: Will be decreased
Restrictive: Will be decreased
FEV1/FVC ratio
Determines if the pattern is obstructive, restrictive or normal
Normal is 70% or less than the lower limit of normal for the patient
This is a calculated ratio that represents the proportion of a person's vital capacity that they are able to expire in the first second of forced expiration to the full, forced vital capacity.
Obstructive: Less than 70%
Restrictive: Normal or > 70%
Diffusing capacity
The diffusing capacity is simply how well the lungs are able to exchange gas
Residual volume (RV)
RV is the amount of air that remains in the lungs after a forceful exhalation
Total Lung Capacity (TLC)
RV + FVC = TLC
Normal range is 80-120% of predicted
Obstructive: >120% (represents hyperinflation)
Restrictive: <80%
Microcytic anemia
(MCV<80 fL) describes RBCs that are small.
Iron deficiency
Sideroblastic
Thalassemia
Anemia of chronic disease
Macrocytic anemia
(MCV>100 fL) describes RBCs that are large.
B12 deficiency (pernicious anemia)
Folate deficiency
Normocytic anemia
(MCV 80-99 fL) describes RBCs that are normal in size.
Anemia of inflammation and chronic disease
Hereditary spherocytosis
G6PD deficiency
Paroxysmal nocturnal hemoglobinuria
Hypochromic anemia
RBCs with less hemoglobin than normal. As a result, the RBCs appear pale in color (MCHC is low).
Hyperchromic anemia
RBCs with more hemoglobin than normal. As a result, the RBCs appear a dark hue or red than normal cells (MCHC is high).
Normochromic anemia
RBCs that have a normal amount of hemoglobin. As a result, the RBCs appear neither pale nor dark (MCHC is normal).
Decreased tissue oxygenation from anemia can manifest as signs and symptoms of the following:
Severe fatigue
Pallor
Weakness
Dyspnea
Dizziness
Cardiac Output (CO)
The amount of blood that the heart pumps in 1 minute. CO is also known as cardiac contractility.
CO=heart rate (HR) x stroke volume (SV).
Stroke Volume (SV)
The volume of blood pumped out of the left ventricle during each systolic cardiac contraction.
Afterload
The force, or load, which the heart must contract against in order to pump blood.
Afterload is also known as systemic vascular resistance (SVR).
Preload
The amount of stretch that the cardiac muscle exhibits at the end of ventricular filling.
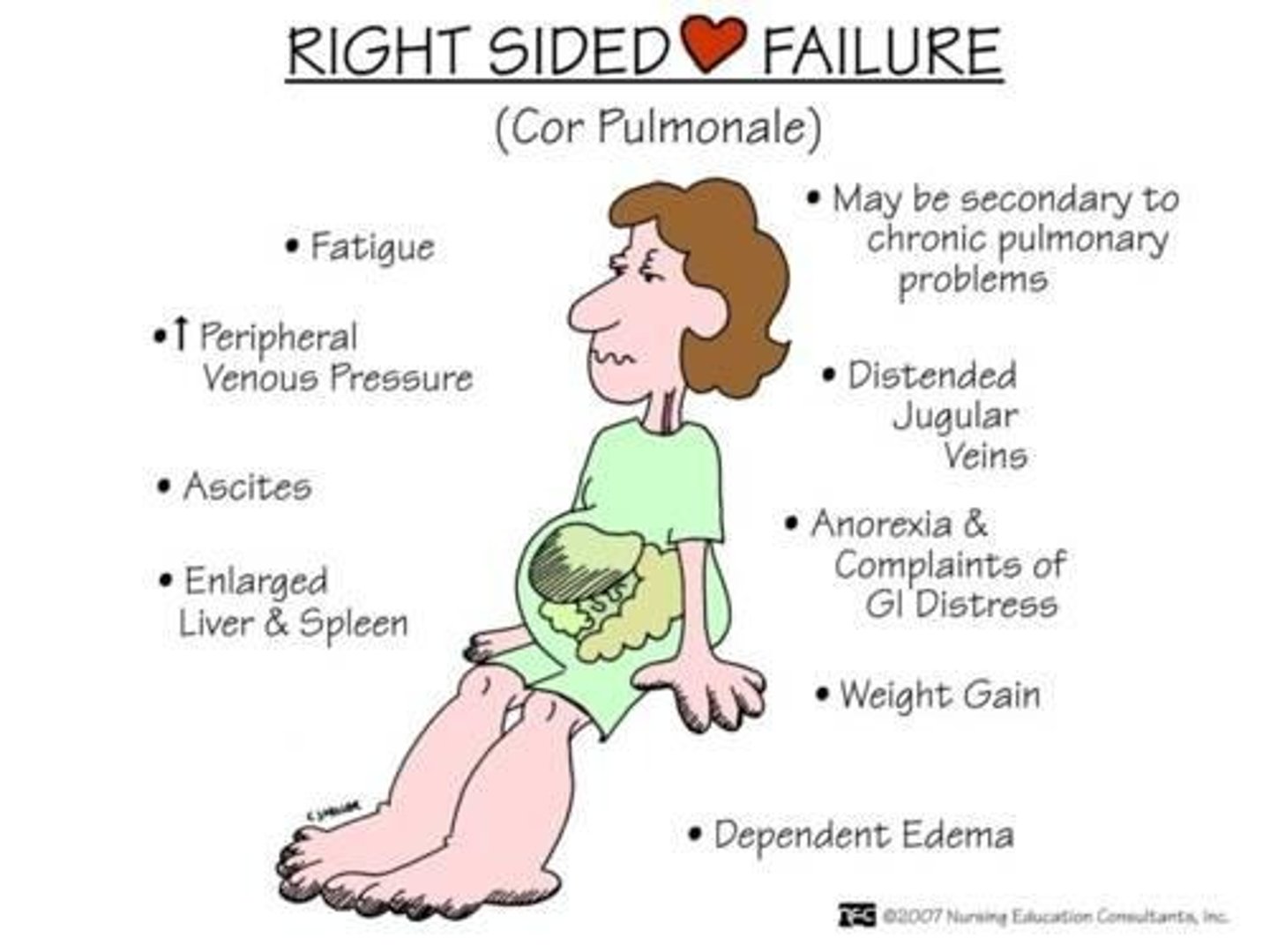
Right-sided Heart Failure
S/Sx:
Jugular vein distention
Hepatosplenomegaly
Peripheral edema
CorPulmonale
Tricuspid valve damage
Right ventricle
superior vena cava (preload)
pulmonary artery (afterload)
Causes of right heart failure include: 1) pulmonary disease that causes pulmonary hypertension. This is the most common cause; 2) right ventricular myocardial infarction (MI), which weakens the cardiac muscle; 3) right ventricular hypertrophy (secondary to cardiac damage); 4) tricuspid valve damage (causing backflow of the blood into the right atrium or right ventricle after ejection); 5) secondary failure as a result of left heart failure due to the build-up of pressure in the damage left ventricle
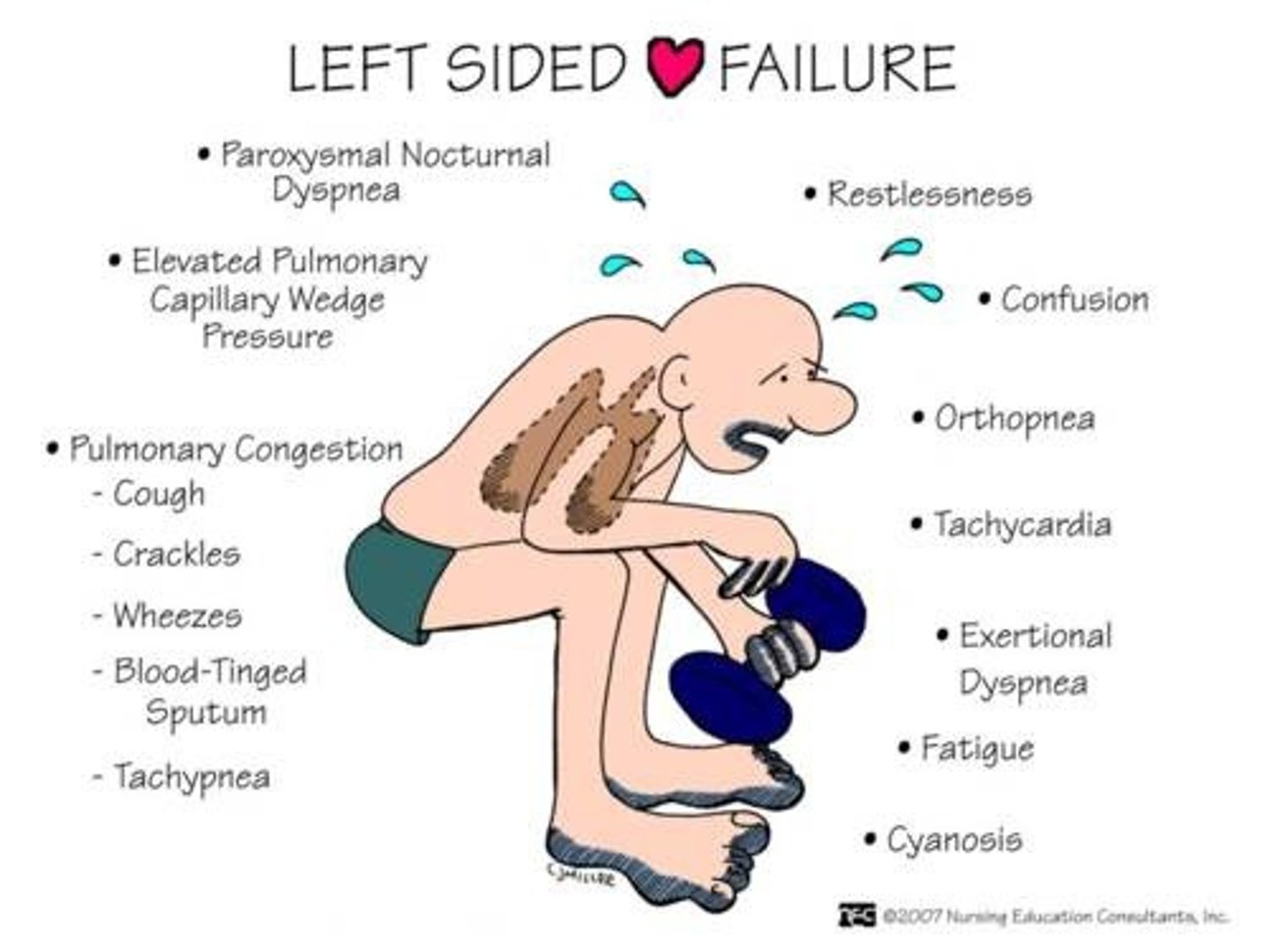
Left-Sided Heart Failure
S/Sx:
Increased left ventricular afterload
Decreased ejection fraction
Increased left ventricular preload
Pulmonary edema
Dyspnea
Left ventricle
Pulmonary vein (preload)
Aorta (afterload)
This increased pressure will force fluid from the pulmonary capillaries into the pulmonary tissues, which essentially floods those areas. The result is pulmonary edema and dyspnea. If left ventricular heart failure is unresolved, volume and pressure will continue to build until it reaches the right side of the heart, contributing to right heart failure as well