Quiz 2 Review
1/76
Earn XP
Description and Tags
UT 609B - OB 2
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
77 Terms
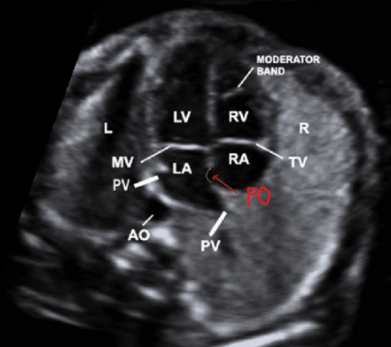
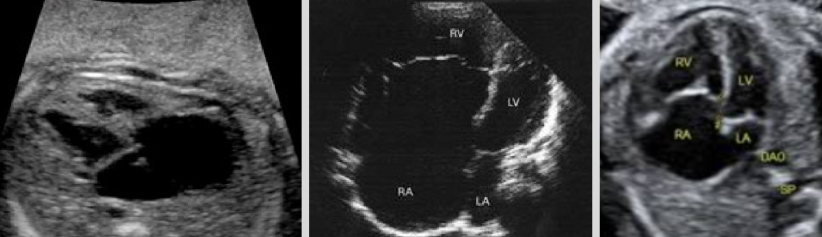
4 chamber (4CH) view
Most important view (many anomalies seen in this view)
Chambers:
RT atrium (RA)
LT atrium (LA)
RT ventricle (RV)
LT ventricle (LV)
Valves:
Tricuspid valve (TV)
Mitral valve (MV)
Tricuspid valve (TV)
Valve between RA and RV
Mitral valve (MV)
Valve between LA and LV
Normal US findings of 4CH view
Heart is in LT chest and fills ~⅓ of chest cavity
Apex points ~45° to LT anterior chest wall
Ventricles are the same size
FO flap opens into LA
Moderator band seen in apex of RV
Valves separating atria and ventricles
Blood in LV extends fully to apex
Which heart chamber is always in front of the aorta?
LA

Anomalies seen in 4CH view
Single ventricle
Hypertrophy, hypoplasia, atresia of chambers
Tricuspid or mitral valve atresia
Atrial/ventricular septal defects
Cardiomyopathy
Endocardial cushion defects
Aortic/pulmonary stenosis - seen better in outflow tract views
Ebstein’s anomaly
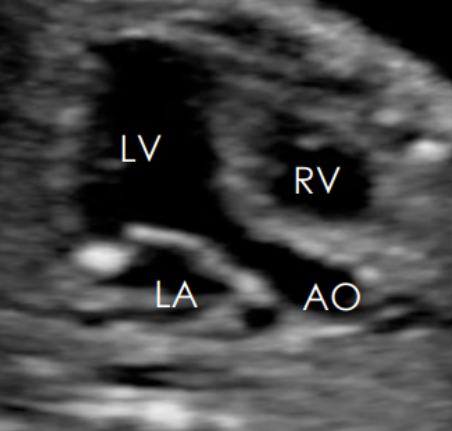
Aortic valve (AV)
Separates LV and aorta
LT ventricular outflow tract (LVOT)
Aortic and LV connection
LA
Aortic root
Aortic valve (AV)
Ventricular septum
RT ventricular outflow tract (RVOT)
Pulmonary artery (PA)
Pulmonic valve (PV)
RV
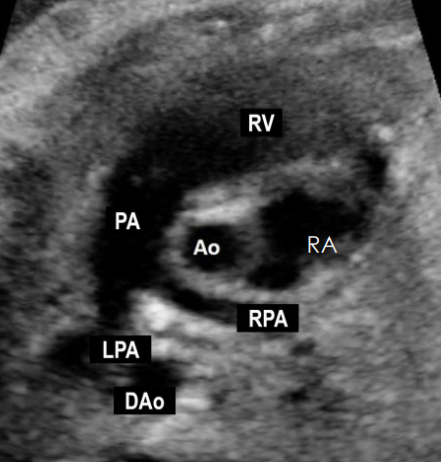
Pulmonic valve (PV)
Separates RV and PA
Anomalies seen on outflow tract views
Transposition of the great vessels
Tetralogy of Fallot
Double-outlet RV
Pulmonary stenosis
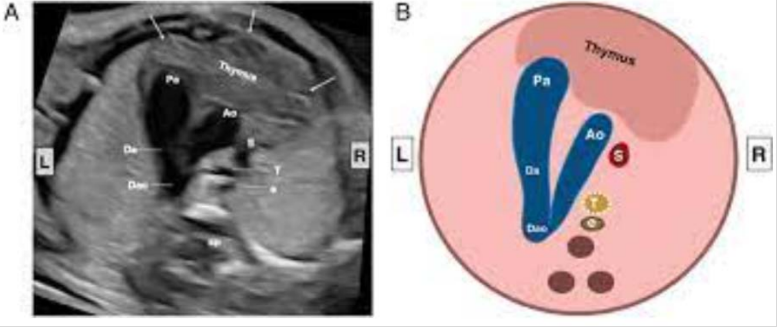
3 vessel heart view (3VV)
Useful for assessing the great vessels
In a straight line from LT ant to RT post, size decreases from LT-RT
Structures
Pulmonary artery (PA)
Aorta (AO)
Superior vena cava (SVC)
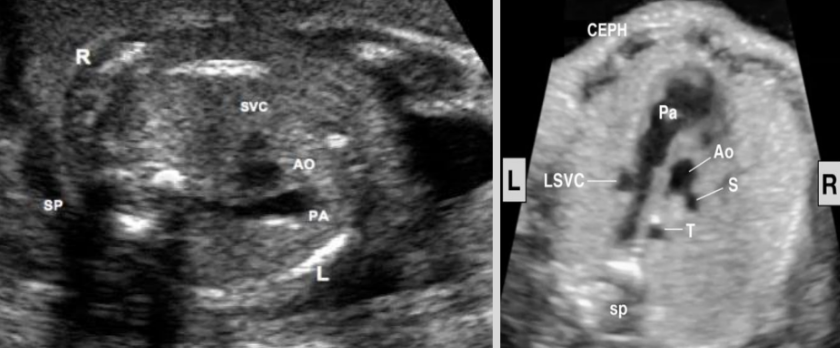
3 vessel trachea view (3VTV)
PA
AO
SVC
Trachea
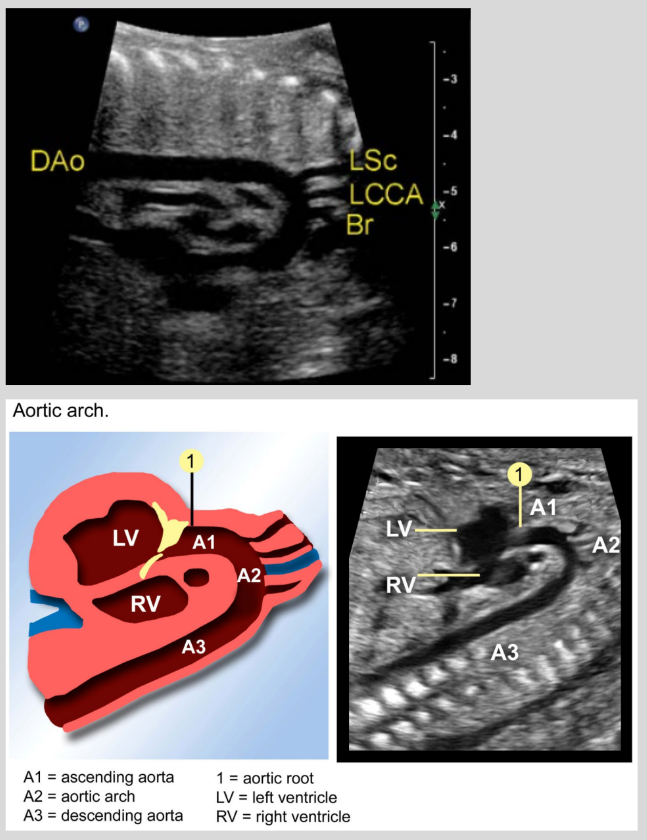
Aortic arch
Turn 90 degrees from 3VV
Vessels coming off to feed the neck/brain
From the center of the heart
Candy cane appearance
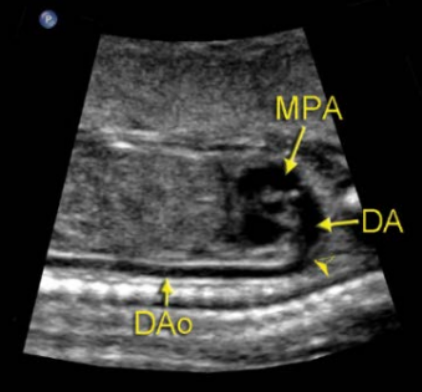
Ductal arch
From the ant chest wall
No vessels coming off to feed the neck/brain
Hockey stick appearance
Cardio system cells (heart, vessels, blood) come from …
Mesodermal layer
Embryology
Cardio system is one of the first systems to appear and function
Blood circulates in embryo by 3rd conceptual/5th menstrual week
Heart begins as cardiogenic cords (paired tubular structures) that fuse on day 22
Embryonic heart forms by beginning of 6th menstrual week → placenta circulation begins
Best time to evaluate heart is at 18-22 weeks
Heart starts beating on day ___
22
Primitive heart changes to 4CH by ___ menstrual weeks
11
Features of fetal circulation
Non-functioning lungs
Blood flows from placenta to heart
Fetal cardio circulation begins at the placenta
Shunts that bypass the liver and lungs
Shunts that bypass the liver and lungs
Placenta
Ductus venosus
Foramen ovale
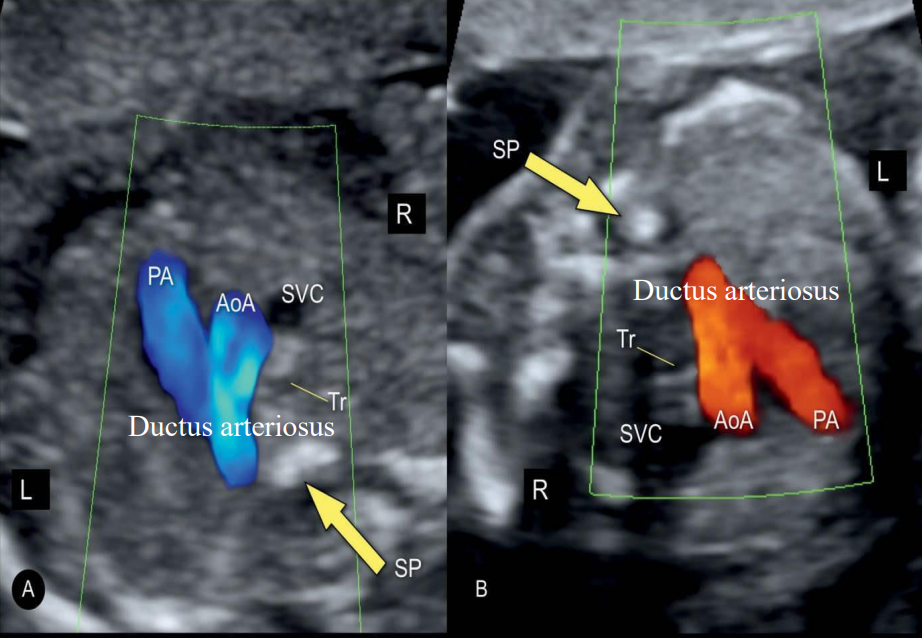
Ductus arteriosus
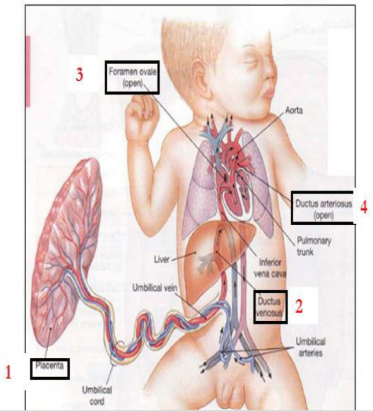
Ductus venosus
Venous connection from the umbilical vein to IVC
Ductus arteriosus
From pulmonary artery into descending aorta
Seals within 24 hrs after birth
Normal fetal HR
100-180 bpm
Transient bradycardia normal in trimester ___ only
2
Tachycardia
Abnormally fast heart rate (180-300 bpm)
Bradycardia
Abnormally slow heart rate (< 100 bpm)
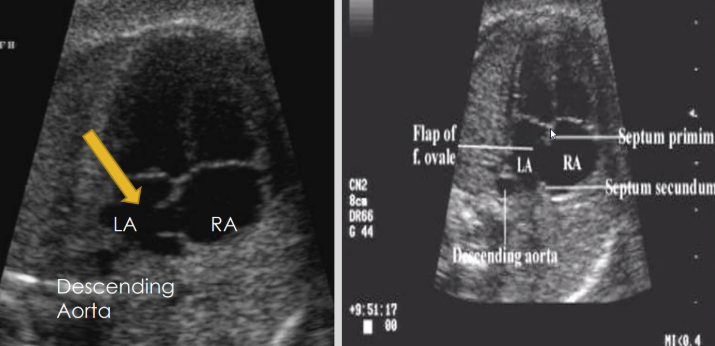
Foramen ovale (FO)
Normal atrial septum opening allowing blood to flow from RA to LA in utero
Septum primum
Septum secundum
~40% of fetal blood flows through FO
Seals within 24 hours after birth
Closes due to
Decreased RT heart pressure and PVR (pulmonary vascular resistance)
Increased LA pressure
Patent foramen ovale (PFO)
Not a true ASD (no septal tissue is missing)
70-75% of PFO close by 2 years old
T/F: Heart abnormalities are some of the most common congenital defects
True
T/F: Ao → LV
True
T/F: PA → RV
True
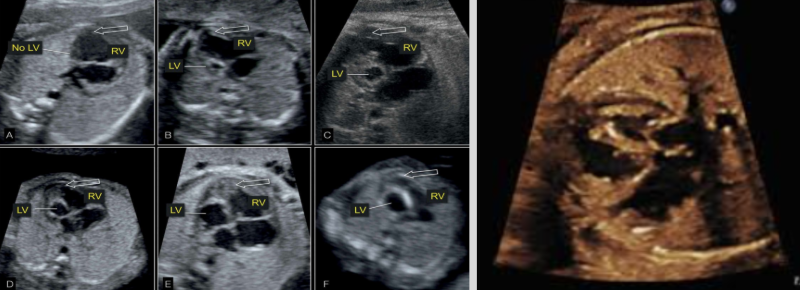
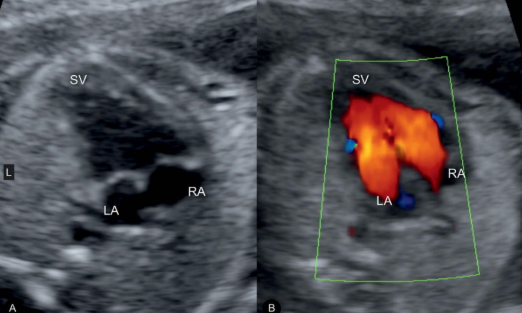
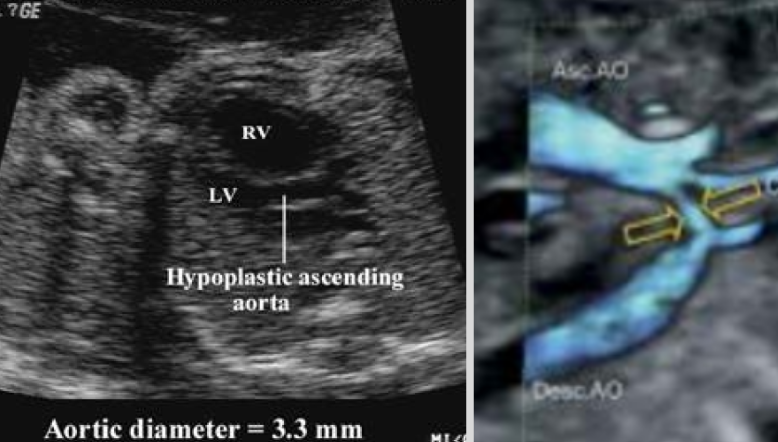
Hypoplastic LT heart
Most severe form of CHDs
Most common cause of death from CHD in early neonatal period
Underdevelopment of LV, MV, Ao, and AV
13% of all CHDs
More common in males
Always lethal
US findings:
Small Ao
Small or absent LV
Cardiomyopathy (CMP)
Abnormally large heart (takes up more than ⅓ of fetal chest)

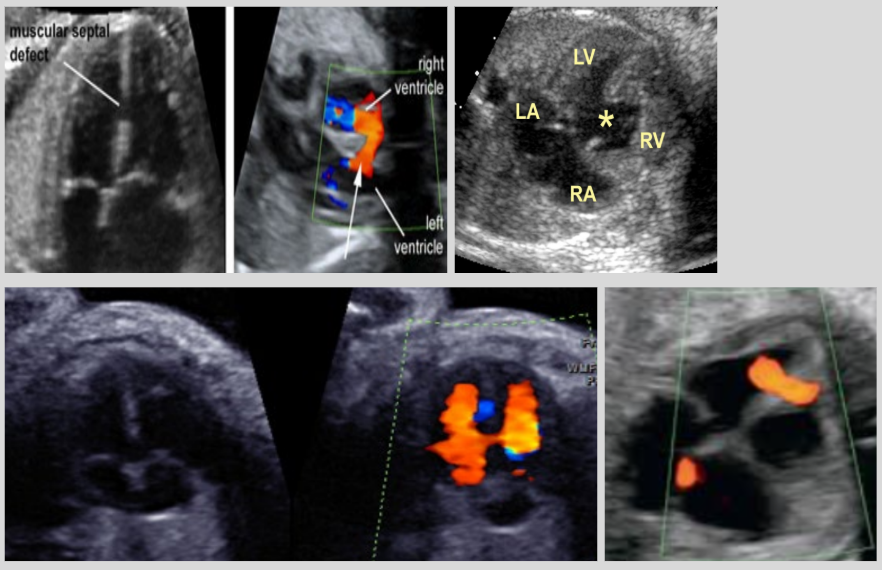
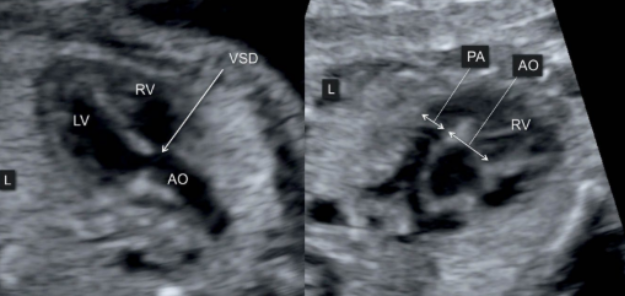
Ventricular septal defect (VSD)
Most common congenital heart defect (1/400 cases)
Abnormal connection between RV and LV
US findings:
Defect in the interventricular septum (IVS)
Blood shunts between ventricles w/ color Doppler
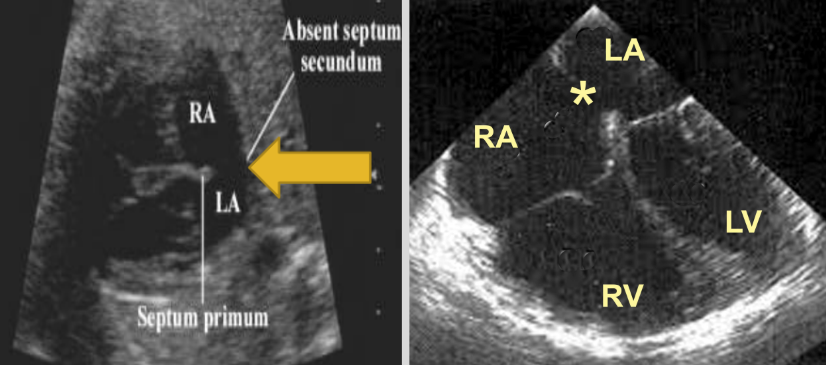
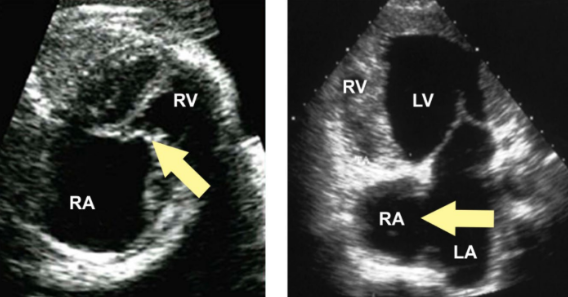
Atrial septal defect (ASD)
Abnormal connection between RA and LA
US findings:
Defect between atriums
Missing septum secundum, septum primum, or both
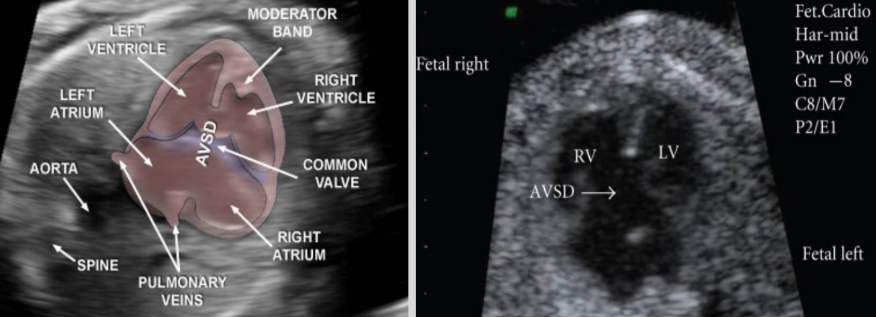
Atrioventricular septal defect (AVSD)
AKA endocardial cushion defect
Fetus has both ASD and VSD
US findings: large defect along cardiac midline
Transposition of the great vessels
PA and Ao are swapped
PA exits from left ventricle
Ao exist from right ventricle
Associations: VSD, patent ductus arteriosus and foramen ovale, and atrial septum defects

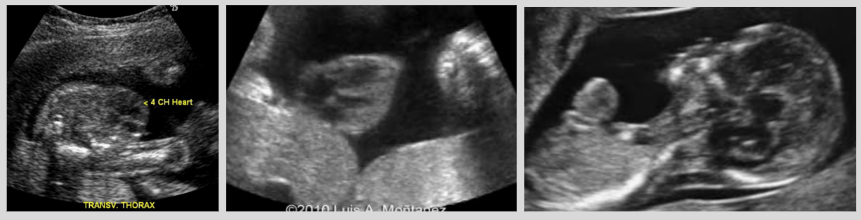
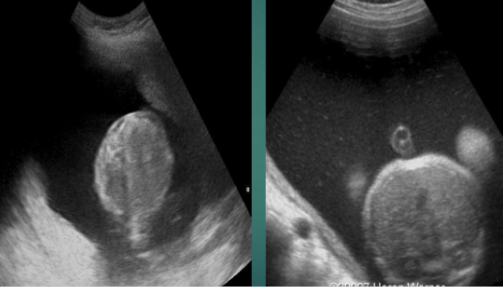
Ectopic cordis
Herniation of heart into amniotic cavity through defect
US findings: heart seen outside of thoracic cavity
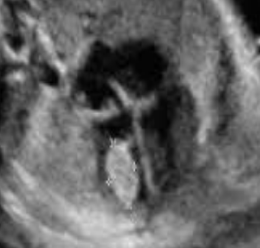
Echogenic intracardiac focus (EIF)
Microcalcification in papillary muscle
Can be in LV or RV
EIF seen in RV is more often associated w/ aneuploidy
Normal variant if seen on its own
If seen w/ other anomalies → increased risk of aneuploidy

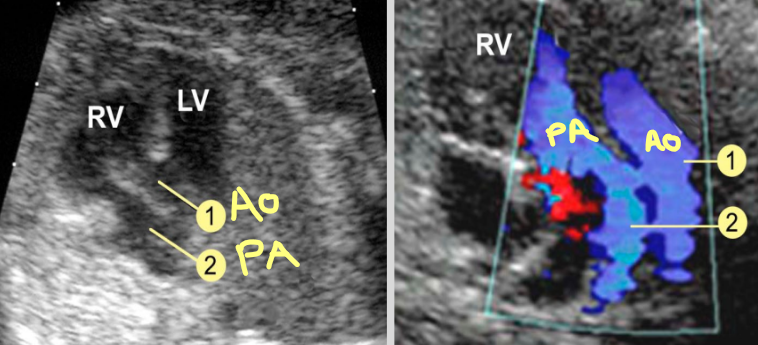
Double outlet RV
Ao and PA arise from the RV
US findings:
VSD almost always present
Linear alignment of Ao and PA
Shared origin of Ao root and PA
Ao is more anterior than PA on 3VV
Tetralogy of Fallot
Y-shaped overriding aorta with outflow from both ventricles
PA stenosis
VSD
RV outflow anomalies
RV hypertrophy
Muscle has to work harder to pump blood through PV
Tricuspid atresia
Failure of the TV and RV to form properly
US findings:
Absent TV, hypoplastic RV and PA, enlarged RA and LV
ASD or VSD
3VV shows small PA
Double inlet LV
LA and RA feed into LV
US findings: single ventricle + 2 atria w/ valves on 4CH
Ebstein’s anomaly
TV displaced inferiorly in RV
US findings:
Enlarged RA (due to displacement), small RV
Inferior displacement of TV
Pericardial effusion
Coarctation of the aorta
Narrowing of aortic lumen
US findings:
Narrowed aortic arc
Disproportionate ventricle sizes
Rhabdomyoma
Most common benign cardiac tumor (prenatally diagnosed)
Associations:
Tuberous sclerosis (60-80%)
Arrhythmias
Valve obstruction
US findings:
Echogenic mass within RV or LV
Fetal pericardial effusion
Accumulation of fluid in the pericardial sac
Normal amount of fluid < 2 mm

Hydrops fetalis
Abnormal amount of fluid build up in 2+ areas of the body
Pericardial effusion
Pleural effusion
Ascites
Cystic hygroma
Skin edema
Two types: immune and nonimmune

Immune hydrops fetalis
Complication of severe form of Rh incompatibility
Mother has Rh negative, fetus has Rh positive
Medication: RhoGAM - prevents mother from making antibodies against baby

Nonimmune hydrops fetalis
Disease or medical condition affects body’s ability to manage fluid
3 main causes: lung/heart problem, severe anemia, genetic/developmental problems
90% of cases

Notes | AFI | MVP | |
Normal | If abdomen wall hits uterine wall on 2 sides, still normal | ? | ? |
AFI: 5-24 cm
MVP: 2-8 cm
Notes | AFI | MVP | |
Polyhydramnios | Abnormally increased amount of amniotic fluid
| ? | ? |
AFI > 24 cm
MVP > 8 cm
Notes | AFI | MVP | |
Oligohydramnios | Abnormally decreased amount of amniotic fluid
| ? | ? |
AFI < 5 cm
MVP < 2 cm
What does D stand for in DRIPP?
Demise
What does R stand for in DRIPP?
Renal abnormalities
What does I stand for in DRIPP?
IUGR
What do the Ps stand for in DRIPP?
PROM and post dates
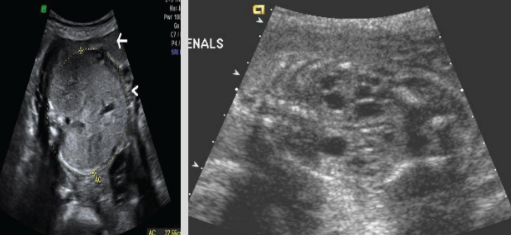
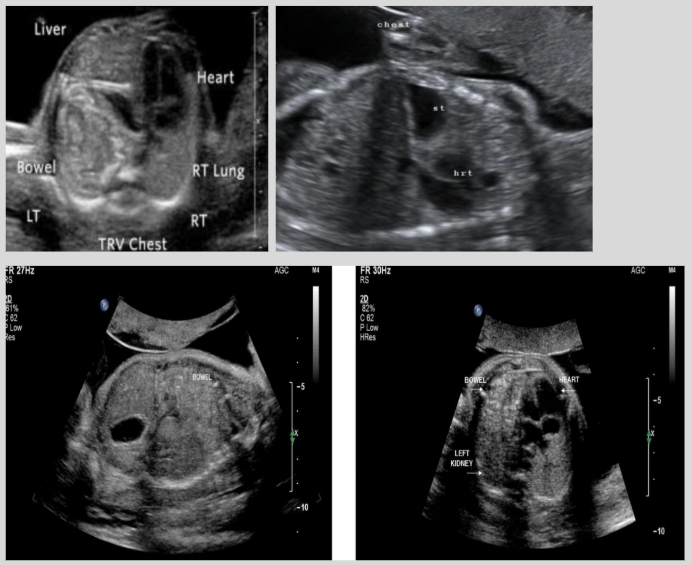
Congenital diaphragmatic hernia (CDH)
Herniation of stomach/bowel/spleen into thoracic cavity through diaphragmatic defect
Result of incomplete fusion of diaphragmatic structure at 6-10 menstrual weeks
Most common: LT-sided herniation (95%)
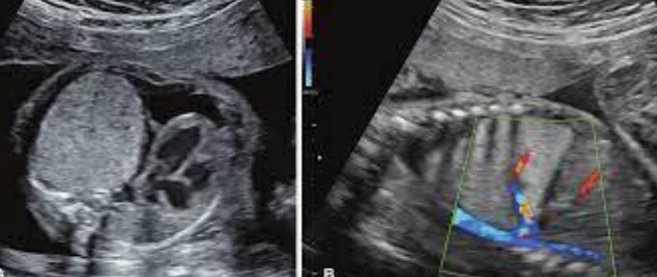
Pulmonary sequestration
Accessory fragment of lung with its own separate arterial circulation
Two types: intralobar and extralobar
Intralobar pulmonary sequestration
Most common, 85% of cases
Closely connected to adjacent normal lung and no separate pleural space
US findings:
Well-defined echogenic mass adjacent to normal lung
Feeder vessel originating from aorta seen w/ color
Extralobar pulmonary sequestration
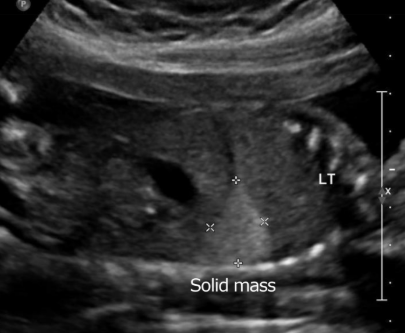
Congenital cystic adenomatoid malformation (CCAM)
Abnormality of lung development where normal lung is replaced by nonfunctioning cystic tissue
Most often unilateral and affects entire lung lobe
Mediastinal shift → increased likelihood of fetal demise
Three forms
Type I CCAM
Most common, 70% of cases
Macrocystic, nonvascular cystic mass in fetal lung

Type II CCAM
Multiple small cysts
Homogeneously echogenic lobes

Type III CCAM
Microcysts or noncystic lesions w/ mediastinal shift
Mediastinal shift + lateral displacement of heart

Tracheal atresia
Lethal condition where trachea fails to form or is obliterated by external compression
Obstruction typically at level of larynx
US findings:
Bilateral enlarged echogenic lungs, fluid-filled trachea, reduced cardiothoracic circumference ratio, polyhydramnios

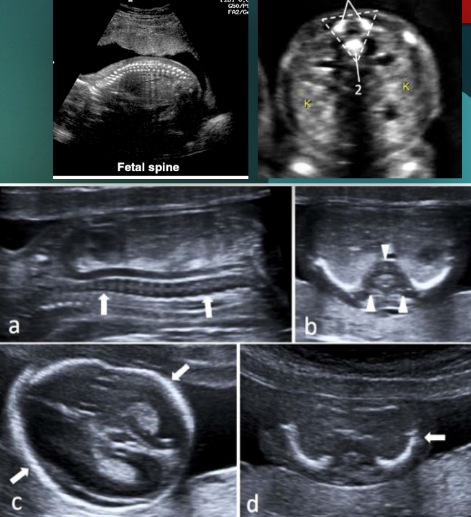
Achondrogenesis
Rare and lethal group of genetic disorders that impair cartilage and bone development
Associated w/ IUGR, cleft soft palate, cystic hygroma, and hydrops fetalis
US findings:
Hypomineralization (absent ossification of vertebral bodies)
Narrow thorax
Bone fractures
Micromelia
Micrognathia
Large head w/ slightly decreased ossification of the cranium
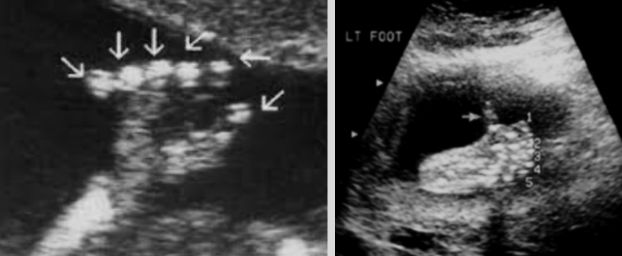
Polydactyly
Presence of extra digits on the fetal hands or feet
One of the most common hand anomalies
Can be an isolated finding or part of a syndrome
Short polydactyly syndrome, asphyxiating thoracic dysplasia, trisomy 13, trisomy 18, and trisomy 21
Rocker bottom foot
Associated with trisomy 13, trisomy 18, and spina bifida

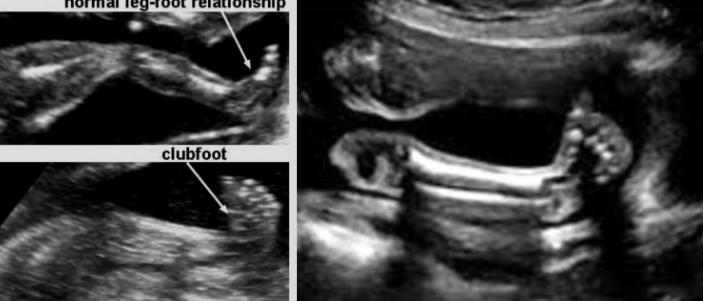
Club foot (AKA talipes equinovarus)
Most common skeletal anomaly seen in routine OB exams
Caused by a shortened Achilles tendon → foot turns in and under
Twice as common in males
Can be an isolated finding or part of a syndrome
Meckel-Gruber, triploidy, Ehlers Danlos, Ellis Van Creveld, Noonan syndrome, trisomy 13, trisomy 18
Treatment - casting and bracing
Syndactyly
Soft tissue or bony fusion of digits

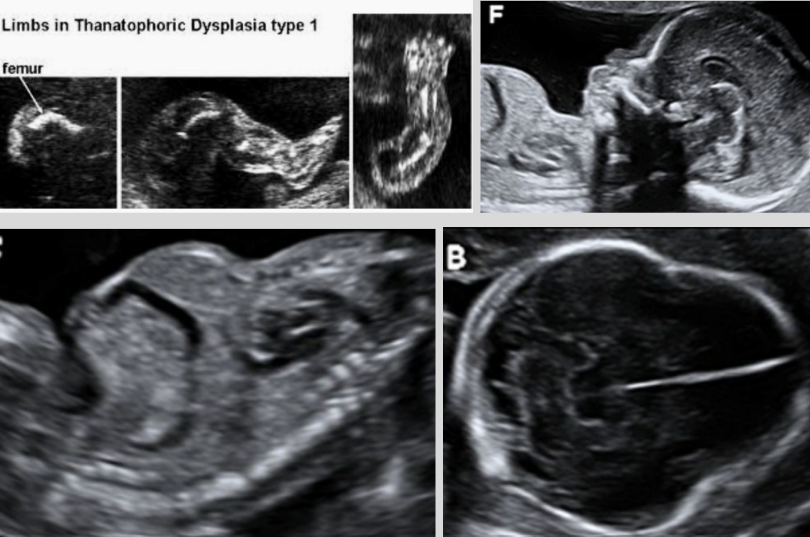
Thanatophoric dysplasia
Severe short-limb dwarfism syndrome that is usually lethal in perinatal period
Most common form of lethal skeletal dysplasia due to breathing difficulties that lead to respiratory failure
Thanatophoric - Greek for “death bearing”
Poor prognosis, still birth, or death after birth due to pulmonary hypoplasia
More common in males
Etiology - autosomal dominant inheritance of FGFR3 gene
Two types
Associated w/ macrocephaly, hydrocephalus, patent ductus arteriosus, ASD, horseshoe kidney, hydronephrosis, and imperforate anus
US findings:
Frontal bossing (clover-leaf skull)
Hypoplastic thorax (small thorax w/ normal trunk)
Bell-shaped chest
Curved long bones
Hypomineralization
Macrocephaly
Fetal bones are normal
Rhizomelia
Proximal segment of a limb is shortened (humerus or femur)
Micromelia
Proximal and distal segments of all limbs are shortened
Mesomelia
Distal segment of a limb is shortened (radius/ulna or tib/fib)
Amelia
Absence of an extremity